

DISFAGIA E RGE: VALUTAZIONE E TRATTAMENTO€¢ Gastric compliance ... =>gravi alterazioni anatomiche...
79
Ospedale dei Bambini “V. Buzzi” Milano SC di Chirurgia Pediatrica SC di Chirurgia Pediatrica (Direttore dott. G. Riccipetitoni) (Direttore dott. G. Riccipetitoni) SS di Chirurgia Pediatrica Gastroenterologica SS di Chirurgia Pediatrica Gastroenterologica (Responsabile dott. L. Maestri) (Responsabile dott. L. Maestri) Servizio di Endoscopia Digestiva Servizio di Endoscopia Digestiva (Referente dott. G. Fava) (Referente dott. G. Fava) DISFAGIA E RGE: DISFAGIA E RGE: VALUTAZIONE E TRATTAMENTO VALUTAZIONE E TRATTAMENTO Congresso intersocietario SIMFER Congresso intersocietario SIMFER-SINPIA SINPIA Bosisio Parini, 8 Bosisio Parini, 8-9-10 ottobre 2008 10 ottobre 2008
Transcript of DISFAGIA E RGE: VALUTAZIONE E TRATTAMENTO€¢ Gastric compliance ... =>gravi alterazioni anatomiche...

Ospedale dei Bambini “V. Buzzi” Milano
SC di Chirurgia PediatricaSC di Chirurgia Pediatrica
(Direttore dott. G. Riccipetitoni)(Direttore dott. G. Riccipetitoni)SS di Chirurgia Pediatrica GastroenterologicaSS di Chirurgia Pediatrica Gastroenterologica
(Responsabile dott. L. Maestri)(Responsabile dott. L. Maestri)Servizio di Endoscopia DigestivaServizio di Endoscopia Digestiva
(Referente dott. G. Fava)(Referente dott. G. Fava)
DISFAGIA E RGE: DISFAGIA E RGE:
VALUTAZIONE E TRATTAMENTOVALUTAZIONE E TRATTAMENTO
Congresso intersocietario SIMFERCongresso intersocietario SIMFER--SINPIASINPIA
Bosisio Parini, 8Bosisio Parini, 8--99--10 ottobre 200810 ottobre 2008
Chirurgo pediatra e SIMFER-SINPIA? Che
c’azzecca?

THE NERVOUS SYSTEM AND GASTROINTESTINAL THE NERVOUS SYSTEM AND GASTROINTESTINAL FUNCTIONFUNCTION
M.A. Altaf and M.R. Sood DEV DISABIL RES REV, 2008
GASTROINTESTINAL DISORDERS IN CHILDREN WITH GASTROINTESTINAL DISORDERS IN CHILDREN WITH NEURODEVELOPMENTAL DISABILITIESNEURODEVELOPMENTAL DISABILITIES
P.B. Sullivan DEV DISABIL RES REV, 2008

ORAL- MOTOR IMPAIRMENT
Symptoms from oral-motor impairment include feeding
problems, drooling and gagging as well as
dysarthria. Uncoordinated swallowing increases the
rysk of pulmonary aspiration, which may or may not
heralded by recurrent coughing and choking with
feeds.
P.B. Sullivan, 2008

ORAL- MOTOR IMPAIRMENT
Feeding problems can easily lead to malnutrition in children with CP
and seriously adversely effect the quality of life of theirs mothers.
Those children with the severest general motor deficit are also
those with the most severe degree of oral-motor impairment. This
is because development of oral-motor skills mirrors general
neurological maturation.
P.B. Sullivan, 2008
ORAL- MOTOR IMPAIRMENT
This development requires the coordination of the movement of a
total of 31 pairs of striated muscles in the mouth, pharyng and
oesophagus by six cranial nerves, the brain stem and the
cerebral cortex. When the central control of this mass of
musculature is severly impaired there is little chance of getting
sufficient quantities of food and drink safely into the
esophagus
P.B. Sullivan, 2008
GER
The high incidence of GER (15-75%) in neurologically
impaired children is well recognized. Several reasons have
been proposed to account for this high incidence…including
hiatus hernia, adoption of a prolonged supine position,
and increased intrabdominal pressure secondary to
spasticity, scoliosis or seizuresP.B. Sullivan, 2008

GER
Nevertheless, CNS dysfunction is likely to be the prime cause
of GER. As a result of neuromuscolar incoordination, the
antireflux function of LES mechanism and esophageal
motility are significantly impaired.
Thus, food and acid and pepsin reflux rostrally from the
stomach into the esophagus
P.B. Sullivan, 2008
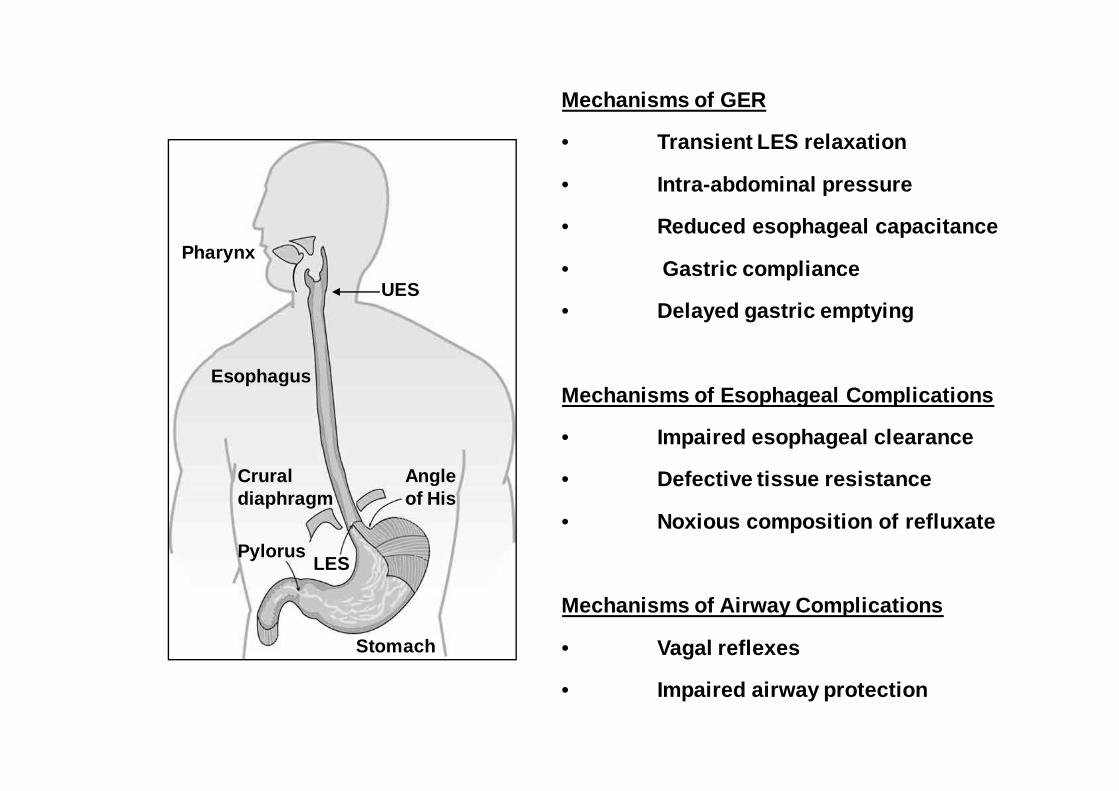
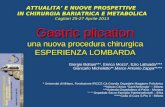
Esophagus
LES
Cruraldiaphragm
Pylorus
Stomach
Angle of His
Pharynx
UES
Mechanisms of GER
• Transient LES relaxation
• Intra-abdominal pressure
• Reduced esophageal capacitance
• Gastric compliance
• Delayed gastric emptying
Mechanisms of Esophageal Complications
• Impaired esophageal clearance
• Defective tissue resistance
• Noxious composition of refluxate
Mechanisms of Airway Complications
• Vagal reflexes
• Impaired airway protection

GERD
GER is a pathological process and GERD refers to the symptom
complex that arises as a result of that process.
It is ironic that the learning deficit that usually accompanies
neurological impairement also impairs the ability of the affected
individual to communicate the main symptom of GERD which is
pain
P.B. Sullivan, 2008

GERD
Chronic peptic esophagitis=>mucosal ulceration=>stricture
formation
Pain=>irritability and crying=>distonic movement of face and neck
Chronic dysphagia=>behavioral food avoidance or aversion
Vomiting, hematemesis, anemia, rumination and regurgitation
Dental problem
P.B. Sullivan, 2008

RESPIRATORY CONSEGUENCE OF GERD
The association between GERD
and respiratory complications
(apnea, laryngitis,
asthma/wheezing, chronic cogh,
chronic pulmonary aspiration,
recurrent pneumonia and
progressive lung injury) has
been recognized for decadesP.B. Sullivan, 2008
ORAL-MOTOR
IMPAIRMENT
GERD

La diagnosiLa diagnosi
=>=> pHmetria esofageapHmetria esofagea
=> pasto baritato=> pasto baritato
=> esofagogastroduodenoscopia=> esofagogastroduodenoscopia
=> Manometria esofagea=> Manometria esofagea
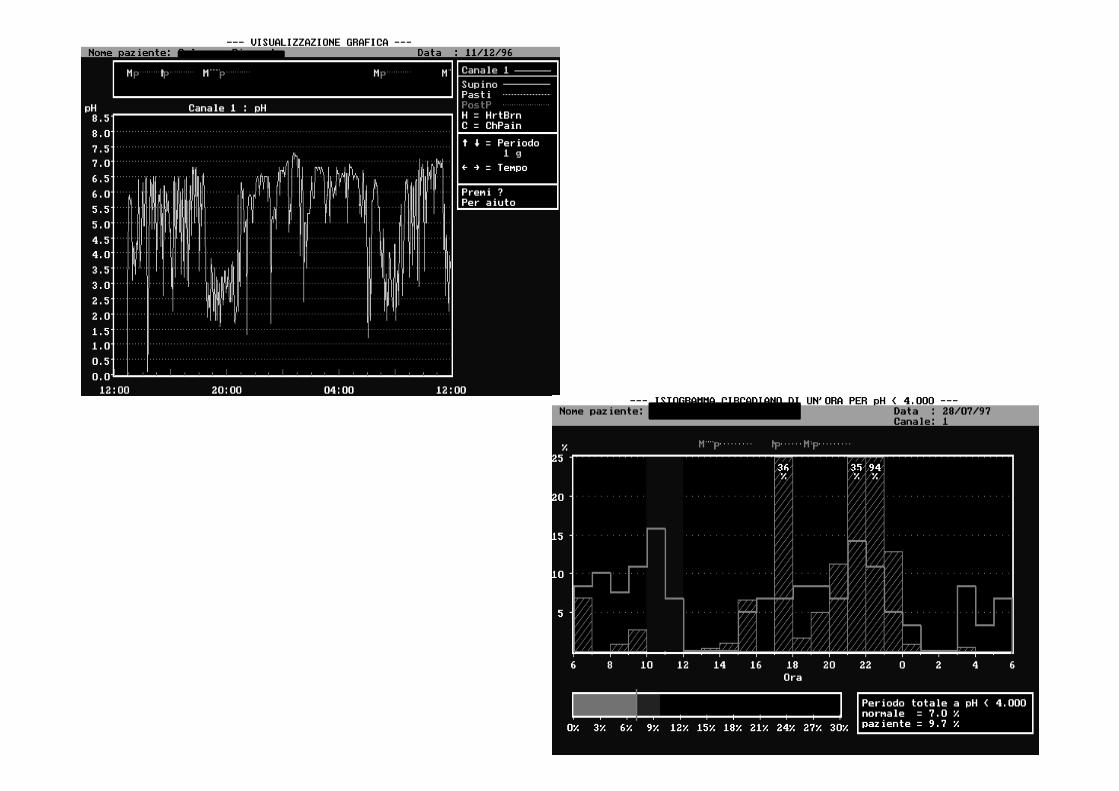
pHmetria esofageapHmetria esofagea
Monitoraggio prolungato del pH esofageoMonitoraggio prolungato del pH esofageo
dimostradimostra
••per quanto tempo vi è acido nell’esofago (IR in %)per quanto tempo vi è acido nell’esofago (IR in %)
••relazione tra i sintomi e l’evento RGErelazione tra i sintomi e l’evento RGE
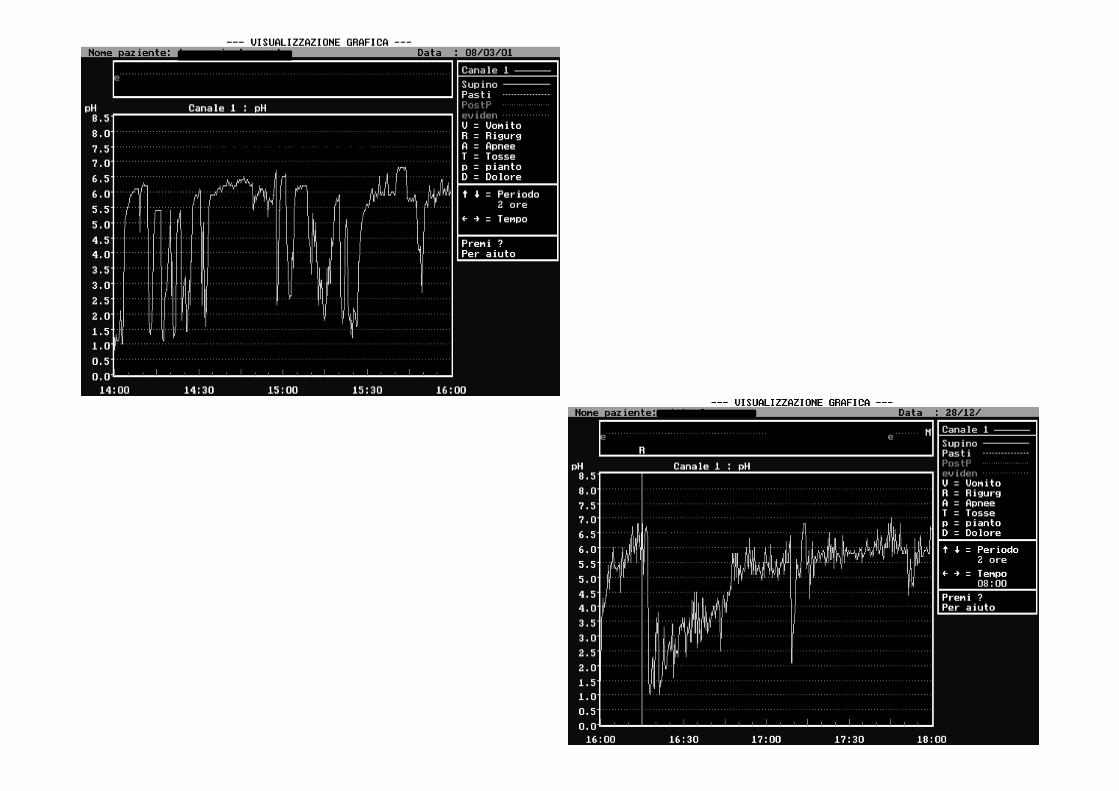
accessi di tosseaccessi di tosse
FKT
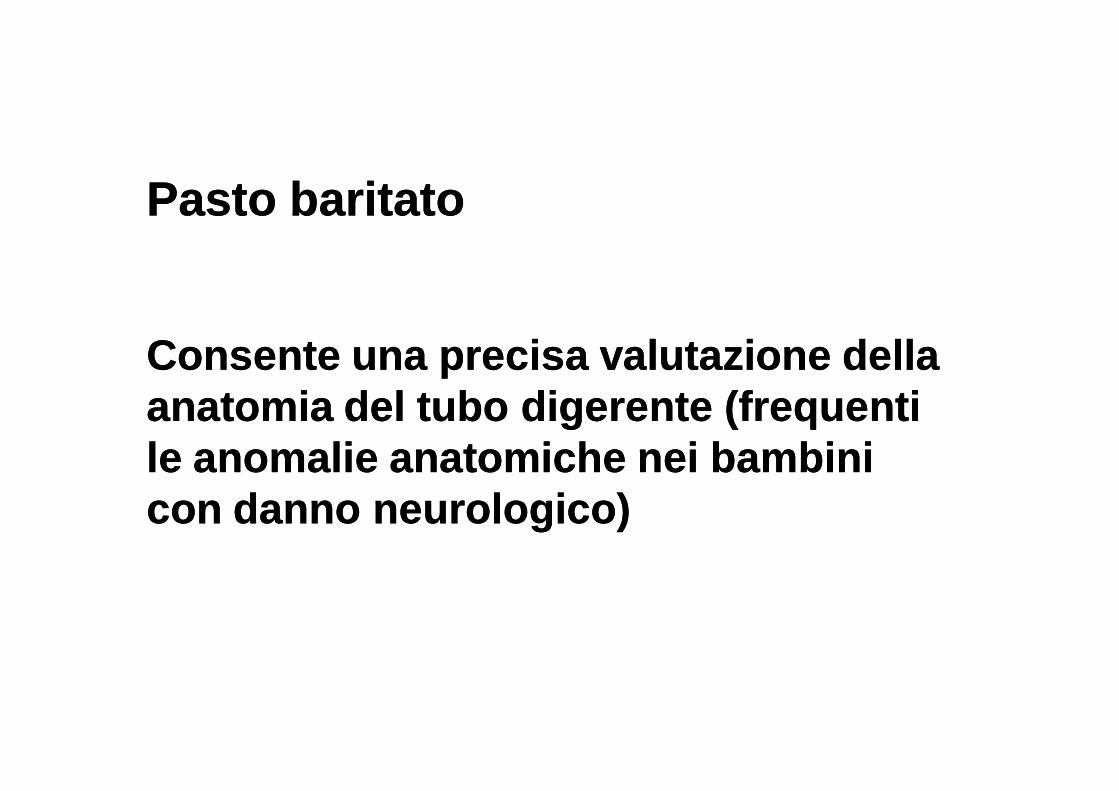
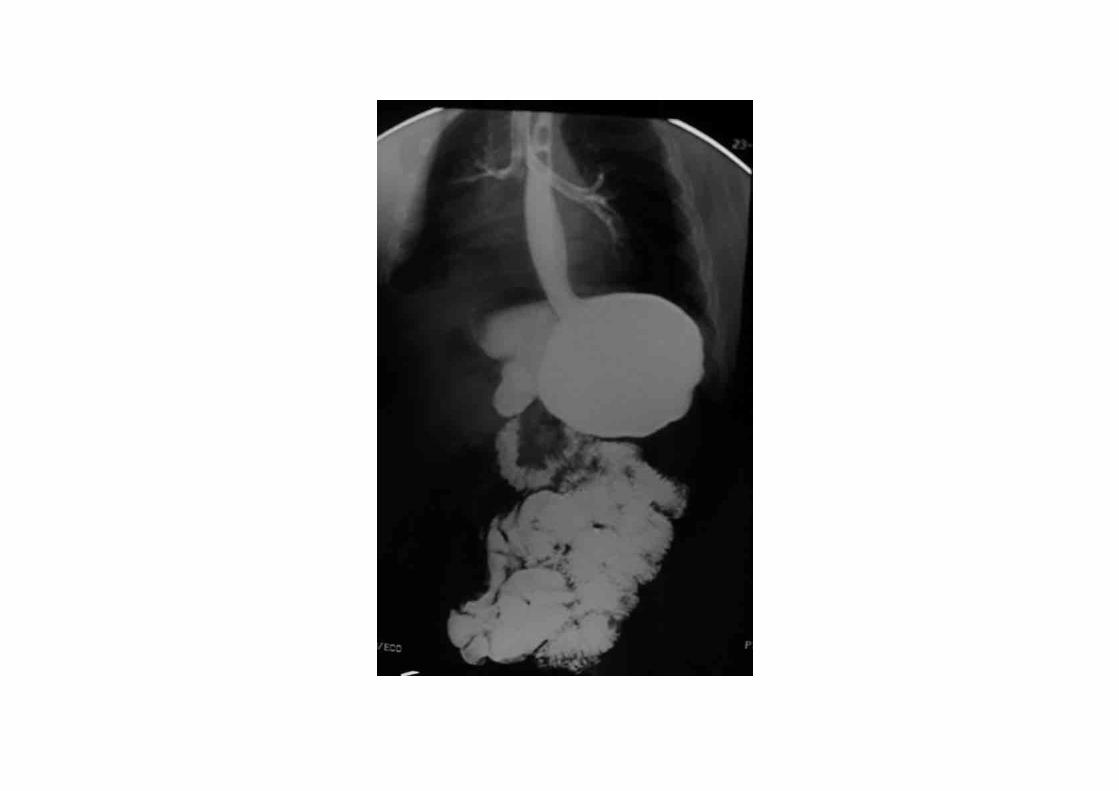
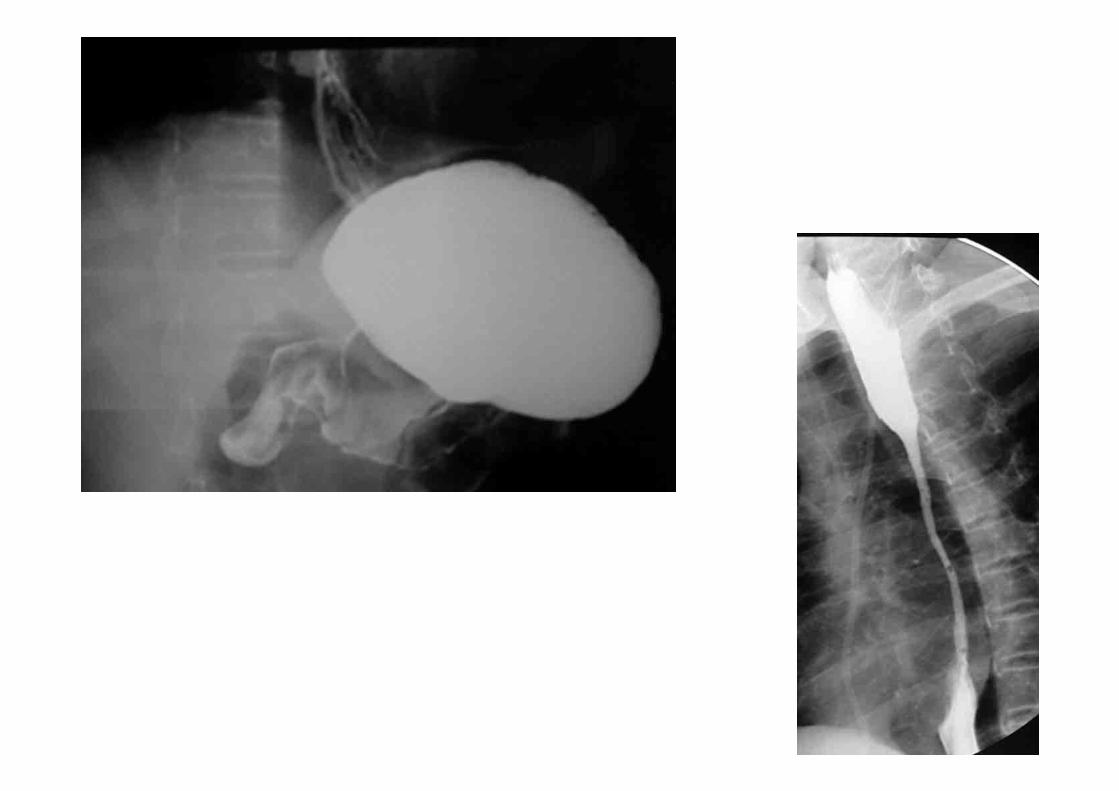
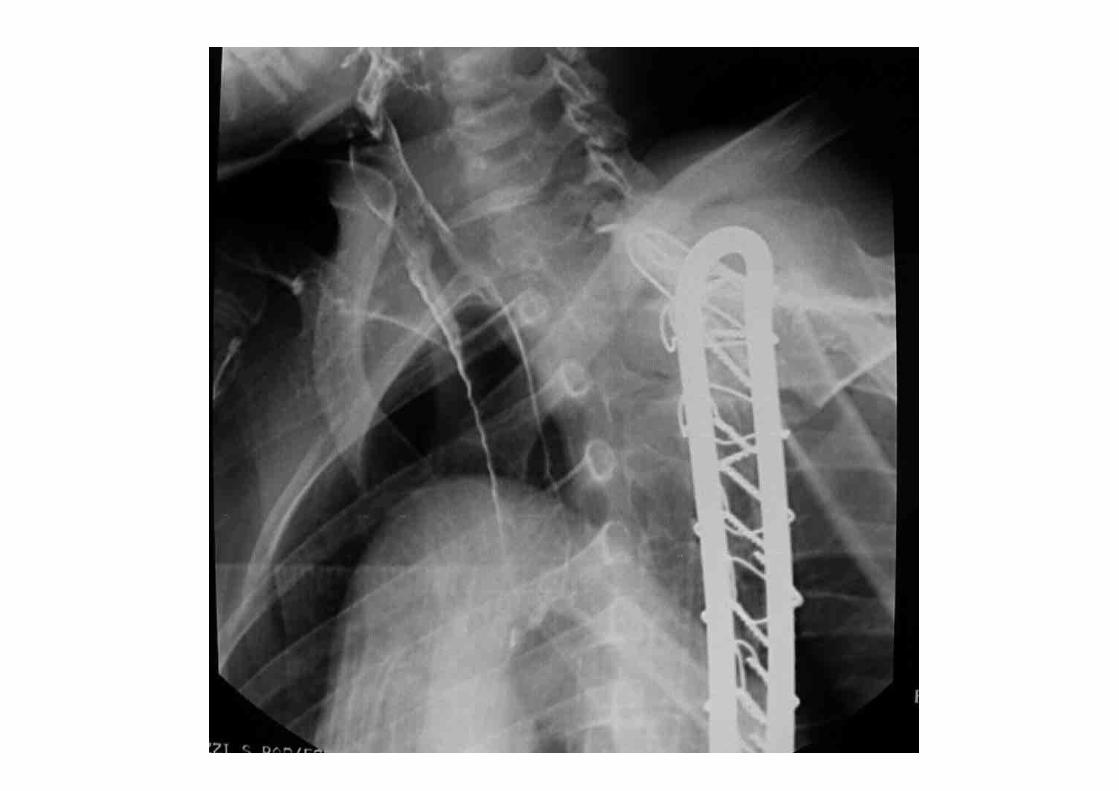
Pasto baritatoPasto baritato
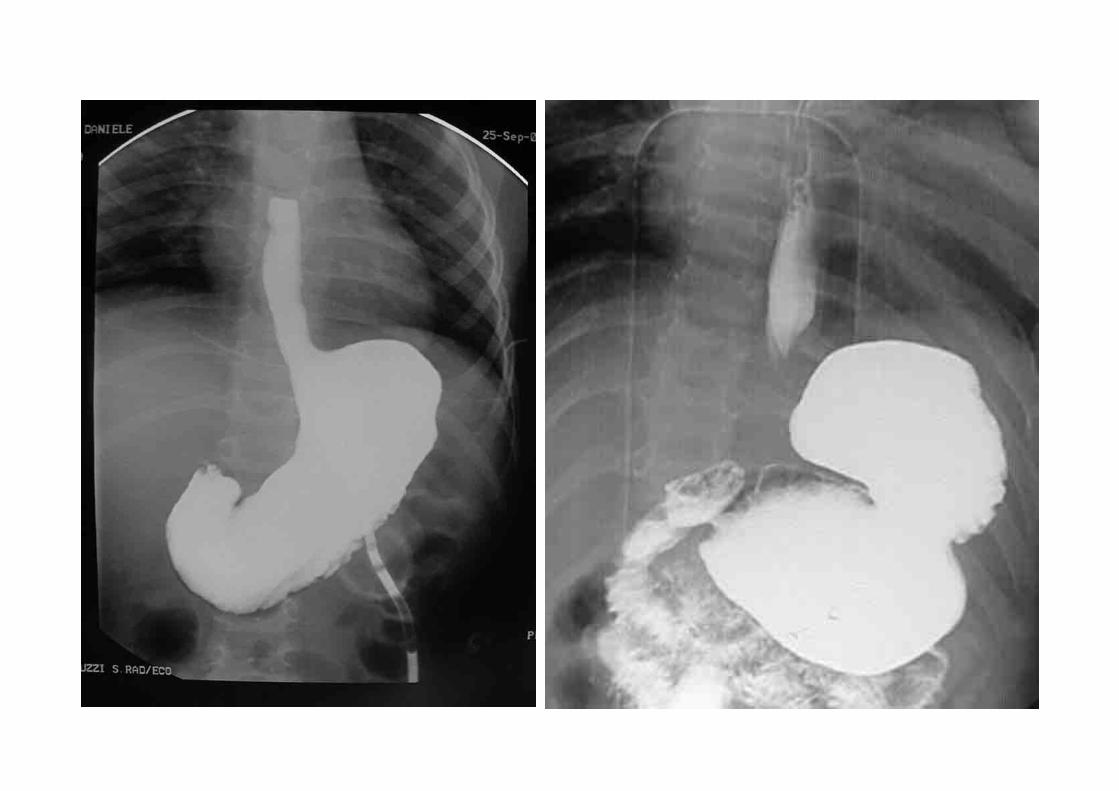
Consente una precisa valutazione della Consente una precisa valutazione della anatomia del tubo digerente (frequenti anatomia del tubo digerente (frequenti le anomalie anatomiche nei bambini le anomalie anatomiche nei bambini con danno neurologico)con danno neurologico)




Pasto baritatoPasto baritato
Consente una valutazione (grossolana) della funzione di Consente una valutazione (grossolana) della funzione di
deglutizione che, tuttavia,viene meglio studiata condeglutizione che, tuttavia,viene meglio studiata con
=> Videofluoroscopia=> Videofluoroscopia
=> Valutazione logopedica=> Valutazione logopedica
=> Valutazione foniatrica=> Valutazione foniatrica



In casi selezionati, la funzione di deglutizione viene studiata dal punto di vista manometrico
Deglutizioni secche Deglutizioni umide

EsofagogastroduodenoscopiaEsofagogastroduodenoscopia
Valuta le condizioni della mucosa esofagea, Valuta le condizioni della mucosa esofagea,
permettendo di diagnosticare la presenza di permettendo di diagnosticare la presenza di
lesioni esofagitiche più o meno gravilesioni esofagitiche più o meno gravi

Terapia medicaTerapia medica
Risultati spesso deludentiRisultati spesso deludenti
=> procinetici (domperidone)=> procinetici (domperidone)
=> antiacidi (idrossido di MG e Al)=> antiacidi (idrossido di MG e Al)
=> acido alginico=> acido alginico
=> antisecretivi (ranitidina, omeprazolo, => antisecretivi (ranitidina, omeprazolo, esomeprazolo)esomeprazolo)

In pediatria va seguito lo schema “step up”“step up”(dal farmaco più maneggevole e con minor effetti collaterali al farmaco meno maneggevole e con più effetti collaterali)
procinetico
PPI
Ac. alginico
antiH2
Domperidone: 0.2 mg/Kg/dose 4 volte/die, 20’ prima dei pasti
Ac. Alginico: 0.5 ml/Kg/dose 4 volte al giorno. 20’ dopo i pasti
Ranitidina: 10 mg/Kg in 2 dosi al giorno
PPI: 1-2 mg/Kg al giorno alla mattina
Terapia medicaTerapia medica
Farmaci “non gastroenterologici”Farmaci “non gastroenterologici”
=> baclofen=> baclofen
=> ondansetron=> ondansetron
Effect of baclofen on emesis and 24 hour Effect of baclofen on emesis and 24 hour esophageal pH in NI children with GEResophageal pH in NI children with GER
The GABA type B receptor agonistThe GABA type B receptor agonist baclofen baclofen was was recently reported to reduce reflux in adult recently reported to reduce reflux in adult patients with GERD reducing the incidence ofpatients with GERD reducing the incidence oftransient lowertransient lower esophageal sphincter relaxationsesophageal sphincter relaxations
8 NI children with GER was studied.8 NI children with GER was studied. BaclofenBaclofen(0.7(0.7 mg/Kg/die)mg/Kg/die) was administered…in 3 divided was administered…in 3 divided doses 30’ before meals for 7 daysdoses 30’ before meals for 7 days
J Pediatr Gastroenterol Nutr. 2004 Mar; 38(3):317J Pediatr Gastroenterol Nutr. 2004 Mar; 38(3):317
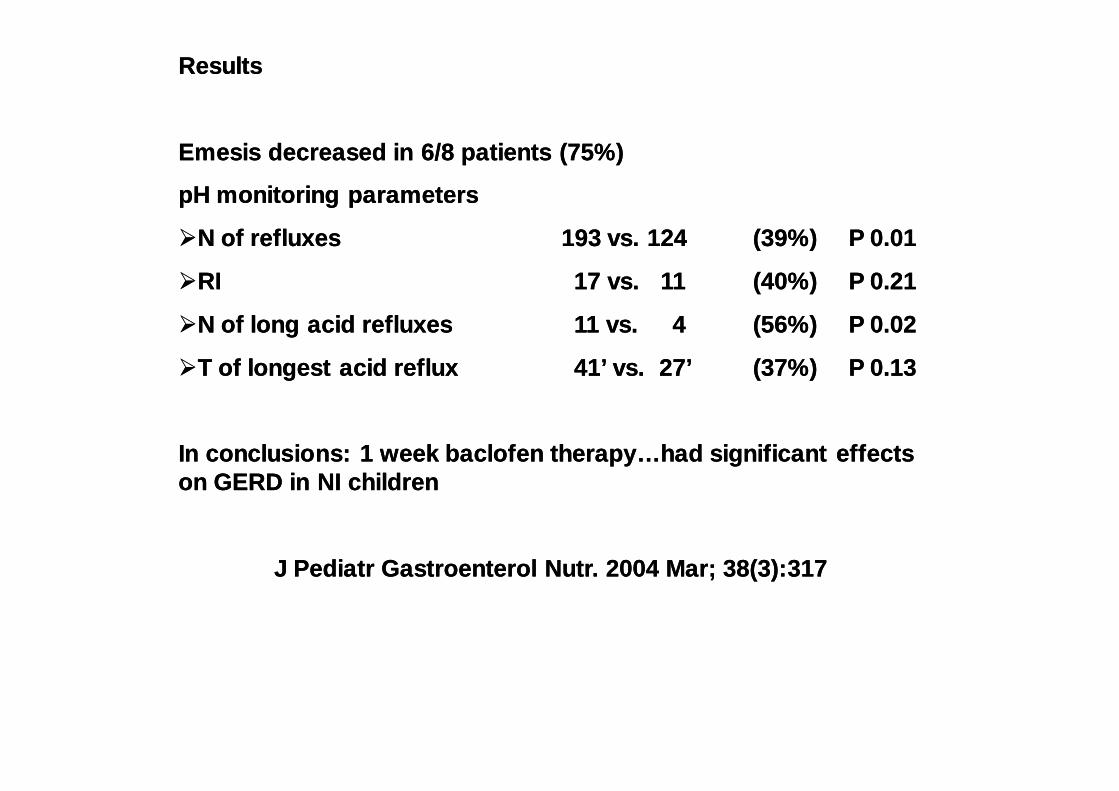
ResultsResults
Emesis decreased in 6/8 patients (75%)Emesis decreased in 6/8 patients (75%)
pH monitoring parameterspH monitoring parameters
N of refluxesN of refluxes 193 vs. 124 193 vs. 124 (39%)(39%) P 0.01P 0.01
RIRI 17 vs. 1117 vs. 11 (40%)(40%) P 0.21P 0.21
N of long acid refluxesN of long acid refluxes 11 vs. 411 vs. 4 (56%)(56%) P 0.02P 0.02
T of longest acid refluxT of longest acid reflux 41’ vs. 27’41’ vs. 27’ (37%)(37%) P 0.13P 0.13
In conclusions: 1 week baclofen therapy…had significant effects In conclusions: 1 week baclofen therapy…had significant effects on GERD in NI childrenon GERD in NI children
J Pediatr Gastroenterol Nutr. 2004 Mar; 38(3):317J Pediatr Gastroenterol Nutr. 2004 Mar; 38(3):317
Ondansetron: a review of its use as an antiemetic in Ondansetron: a review of its use as an antiemetic in childrenchildren
Ondansetron is a selective serotonin 5Ondansetron is a selective serotonin 5--HT3 receptor HT3 receptor antagonist.antagonist.
In dose ranging and large placeboIn dose ranging and large placebo--controlled trials, controlled trials, intravenous (0.075 to 0.15 mg/Kg) orintravenous (0.075 to 0.15 mg/Kg) or oral (0.1oral (0.1 mg/kg)mg/kg)ondansetron was significantly more effective than ondansetron was significantly more effective than placebo in preventing emesis in children undergoing placebo in preventing emesis in children undergoing surgery associated with a high risk of postop. nausea surgery associated with a high risk of postop. nausea and vomitingand vomiting
Paediatr Drugs 2001; 3(6): 441Paediatr Drugs 2001; 3(6): 441
DA PEDGIDA PEDGI
For this very difficult population, I have noticed For this very difficult population, I have noticed that often Baclofen or Tranzene or some other that often Baclofen or Tranzene or some other med prescribed by neurologist work better for med prescribed by neurologist work better for vomiting or reflux than “our” medicines do (H2 vomiting or reflux than “our” medicines do (H2 blockers and PPIs)blockers and PPIs)
I use ondansetron 4 mg od I use ondansetron 4 mg od –– bidbid
Adrian Jones, Adrian Jones, Professor of PediatricsProfessor of Pediatrics
Edmonton, Alberta Edmonton, Alberta
CanadaCanada

Trattamenti “operativi“Trattamenti “operativi“NO medicina, NO chirurgiaNO medicina, NO chirurgia
sondino ng sondino ng
sondino transpiloricosondino transpilorico

Trattamenti “operativi“Trattamenti “operativi“NO medicina, NO chirurgiaNO medicina, NO chirurgia
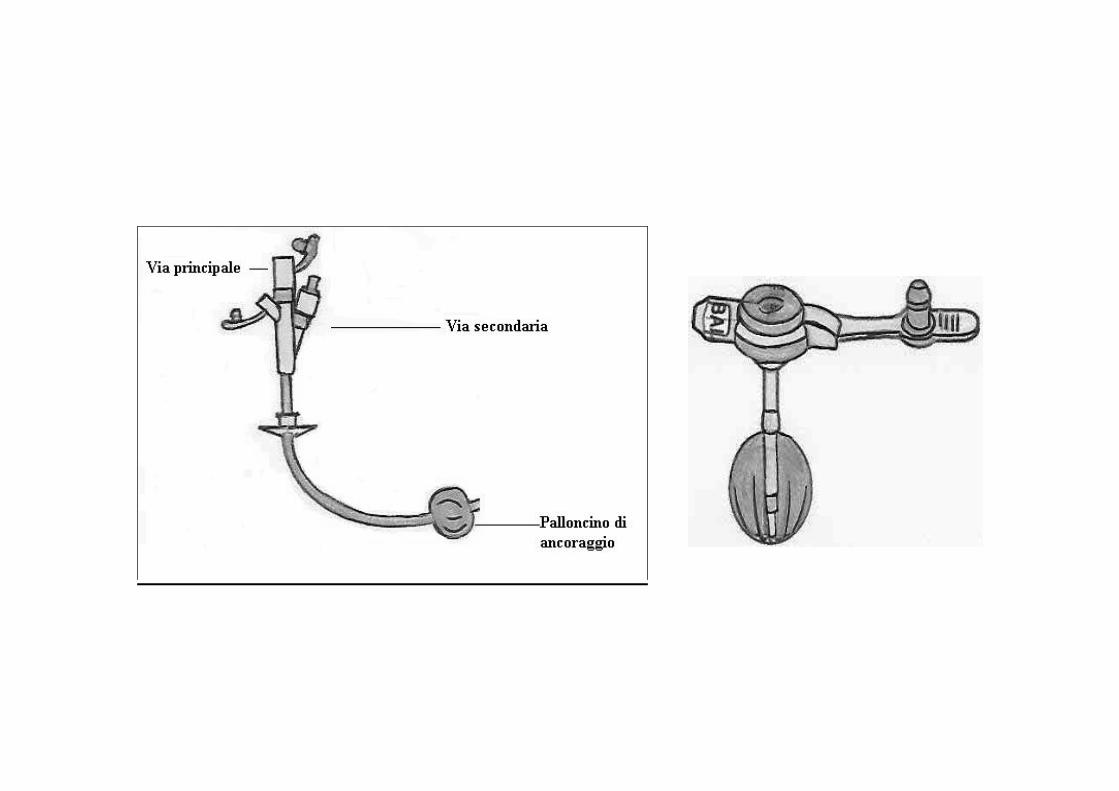
Gastrostomia (chirurgica, percutanea Gastrostomia (chirurgica, percutanea endoscopica, laparoscopica)endoscopica, laparoscopica)
Digiunostomia (chirurgica, percutanea Digiunostomia (chirurgica, percutanea endoscopica, laparoscopica)endoscopica, laparoscopica)
GastrostomiaGastrostomia
ObiettiviObiettivi
••migliorare lo stato nutrizionalemigliorare lo stato nutrizionale
••evitare un riempimento eccessivo dello evitare un riempimento eccessivo dello stomacostomaco

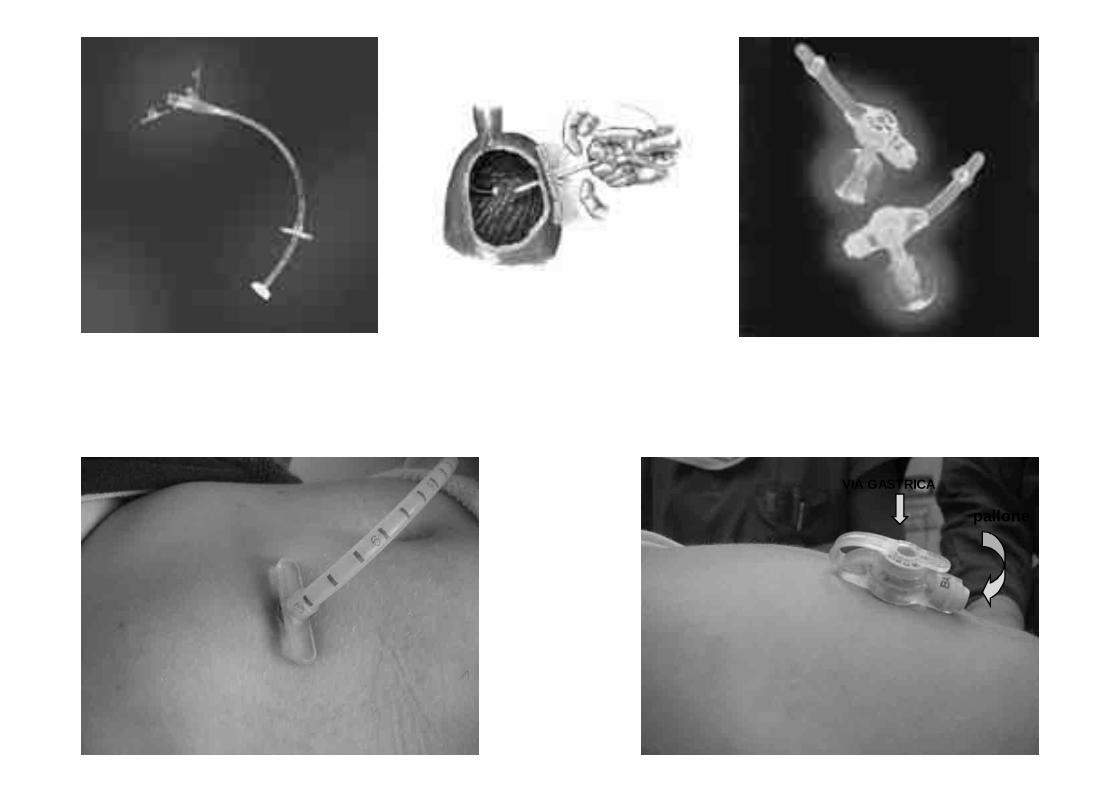
VIA GASTRICA
pallone
VANTAGGI DELLA GASTROSTOMIAVANTAGGI DELLA GASTROSTOMIA
Miglioramento dello stato nutrizionaleMiglioramento dello stato nutrizionale
Somministrazione sicura di farmaci e di altri Somministrazione sicura di farmaci e di altri trattamenti (stipsi)trattamenti (stipsi)
Impact of nutritional rehabilitation on Impact of nutritional rehabilitation on GER in neurological impaired childrenGER in neurological impaired children
10 malnourished NI children10 malnourished NI children (triceps skin fold thickness (triceps skin fold thickness [TSF] below the 5th percentile) treated with aggressive [TSF] below the 5th percentile) treated with aggressive nutritional rehabilitationnutritional rehabilitation,, fed through a PEG.fed through a PEG.
When TSF was > or = 50th percentile the 24When TSF was > or = 50th percentile the 24--hour pH probe hour pH probe study showed marked improvement in 6/10 patientsstudy showed marked improvement in 6/10 patients
J Pediatr Surg 1994 Feb; 29(2):167J Pediatr Surg 1994 Feb; 29(2):167
VANTAGGI DELLA GASTROSTOMIAVANTAGGI DELLA GASTROSTOMIA
Miglioramento dello stato nutrizionaleMiglioramento dello stato nutrizionale
Somministrazione sicura di farmaci e di altri Somministrazione sicura di farmaci e di altri trattamenti (stipsi)trattamenti (stipsi)
Miglioramento della qualità di vita (paziente e Miglioramento della qualità di vita (paziente e care givers)care givers)

This study has quantified for the This study has quantified for the first time a significant, measurable first time a significant, measurable improvement in the quality of life improvement in the quality of life
of carers (mothers predominately) of carers (mothers predominately) after overcoming the feeding after overcoming the feeding
problems of children with CP by problems of children with CP by insertion of gastrostomy tubeinsertion of gastrostomy tube
Dev. Med. And Child Neurol. 2004Dev. Med. And Child Neurol. 2004

GastrostomiaGastrostomia
ProblemaProblema
RGERGE
DigiunostomiaDigiunostomia
ObiettivoObiettivo
“Saltare” lo stomaco“Saltare” lo stomaco
Venting dello stomacoVenting dello stomaco


VIA GASTRICA
pallone
via digiunale

Istituti Clinici di PerfezionamentoOspedale di rilievo nazionale e di alta specializzazione convenzionato con l’Università degli
Studi di MilanoOspedale dei Bambini “V. Buzzi”
U.O di Chirurgia Pediatrica
ambulatorio per la riabilitazione dei bambini ambulatorio per la riabilitazione dei bambini incontinenti e stomizzatiincontinenti e stomizzati
AMBULATORIO DI GASTROENTEROLOGIA CHIRURGICAAMBULATORIO DI GASTROENTEROLOGIA CHIRURGICA
LA STOMIA NUTRIZIONALELA STOMIA NUTRIZIONALEGUIDA PER I GENITORIGUIDA PER I GENITORI

Terapia chirurgicaTerapia chirurgica
Risultati assai deludenti: circa 20% di recidiveRisultati assai deludenti: circa 20% di recidive(5% nei bambini senza danno neurologico)(5% nei bambini senza danno neurologico)
Alta incidenza di complicanzeAlta incidenza di complicanze
Complicanze più frequentiComplicanze più frequenti
“retching”“retching”
impossibiltà di vomitare (gas bloat syndrome)impossibiltà di vomitare (gas bloat syndrome)
occlusione intestinaleocclusione intestinale

The failure rate of surgery for gastroesophageal refluxThe failure rate of surgery for gastroesophageal reflux
The main presentingThe main presenting symptomssymptoms at the time of the diagnosis of at the time of the diagnosis of failure wasfailure was severe retching, recurrent vomiting and aspiration severe retching, recurrent vomiting and aspiration and gas bloat syndrome.and gas bloat syndrome.
The predominant cause of The predominant cause of fundoplication failure is herniationfundoplication failure is herniationinto the posterior mediastinuminto the posterior mediastinum, which occured most frequently , which occured most frequently in children with in children with hypertonic cerebral palsy.hypertonic cerebral palsy.
J J Pediatr Surg. 1998 Jan; 33(1):64Pediatr Surg. 1998 Jan; 33(1):64
GOSGOS

National trends in the use of antireflux procedures for children
…retrospective cohort study of children undergoing antireflux surgery in US from 1996 to 2003…
During the study period, 48665 antireflux procedures were performed…
Pediatrics, 2006

National trends in the use of antireflux procedures for children
There was a significant decrease in the percentages of children undergoing antireflux procedures who were neurologically impaired between 1996 and 2003
Pediatrics, 2006

SCOMPARSA O MIGLIORAMENTO SIGNIFICATIVO DEI SINTOMI(giudizio solo clinico)
94% =>84.6% (NON NEUROLOGICI/ NEUROLOGICI)
COMPLICANZE
4.2% =>12.8% (NON NEUROLOGICI/NEUROLOGICI)
REINTERVENTI (REDO FUNDO O OCCLUSIONE)
3.6% =>11.8% (NON NEUROLOGICI/NEUROLOGICI)
Surgical treatment of gastroesophageal reflux in children: a combinedhospital study of 7467 patients
Pediatrics, 1998

INDICAZIONI ALLA CHIRURGIAINDICAZIONI ALLA CHIRURGIA
=>mancato controllo dei sintomi dopo PEG/PEGJ
=>gravi alterazioni anatomiche della regione esofago-gastrica
Razionale dell’intervento chirurgico
Tutte le tecniche chirurgiche adottate sipropongono lo scopo di:
=>ottenere un segmento di esofagoaddominale sufficentemente lungo
=>Fissare meccanicamente lo SEI al disotto del diaframma=>Ricostruire un angolo di His di 0°

Razionale dell’intervento chirurgico
Tutte le tecniche chirurgiche adottate sipropongono lo scopo di:
=>ottenere un segmento di esofagoaddominale sufficentemente lungo
=>Fissare meccanicamente lo SEI al disotto del diaframma=>Ricostruire un angolo di His di 0°
Scelta della tecnica
=>Opzione di Scuola

Risultati della chirurgia
The results of pediatric series of
laparoscopic fundoplication suggest that
the results and complications rates aresimilar to those of the openprocedure, but hospitalization isshortened
NASPGHAN

Indications must remain identical for open and laparoscopic procedures
Journal of Pediatric Surgery Lecture
Juan A. Tovar
Journal of Pediatric Surgery 42, 277, 2007

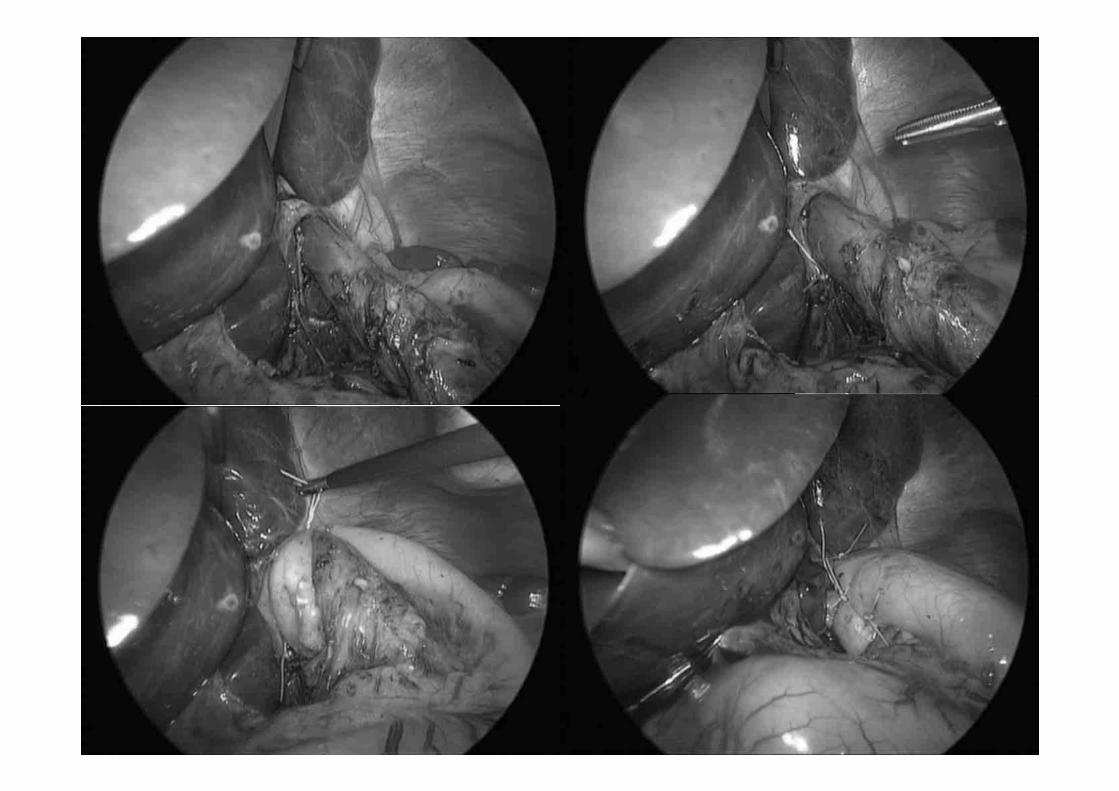
The laparoscopic Nissen and LAPEG are realizable also in
neurologically impaired children using personalized solutions
adapted to the patient’s deformities and spasticity. The choice to perform an initially PEG, indicated in cases of
severe malnutrition or moderate GER, doesn’t represent a formal indication against the laparoscopic fundoplicatio;
SIGENP, 2007

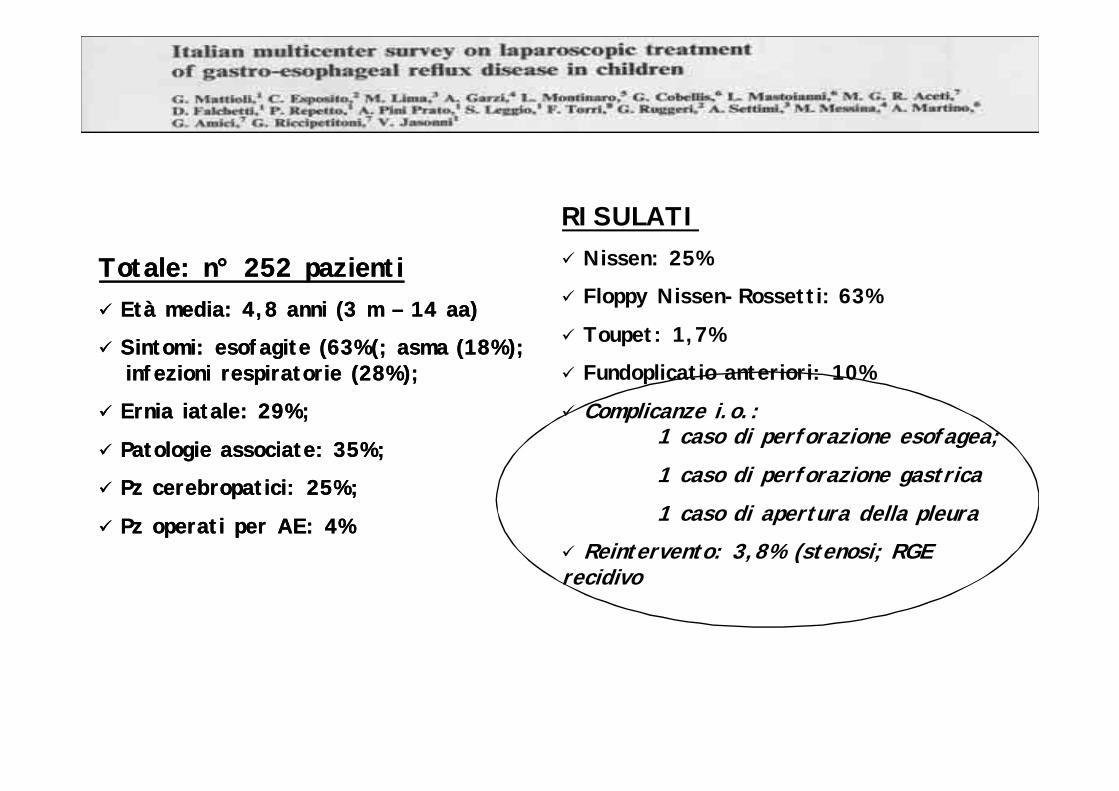
RISULATINissen: 25%
Floppy Nissen-Rossetti: 63%
Toupet: 1,7%
Fundoplicatio anteriori: 10%
Complicanze i.o.: 1 caso di perforazione esofagea;1 caso di perforazione gastrica1 caso di apertura della pleura
Reintervento: 3,8% (stenosi; RGE recidivo
Totale: nTotale: n°° 252 pazienti252 pazientiEtà media: 4,8 anni (3 m Età media: 4,8 anni (3 m –– 14 aa)14 aa)
Sintomi: esofagite (63%(; asma (18%); Sintomi: esofagite (63%(; asma (18%); infezioni respiratorie (28%); infezioni respiratorie (28%);
Ernia iatale: 29%; Ernia iatale: 29%;
Patologie associate: 35%;Patologie associate: 35%;
Pz cerebropatici: 25%;Pz cerebropatici: 25%;
Pz operati per AE: 4%Pz operati per AE: 4%
PROPOSTAPROPOSTA
Trattamento medico “gastroenterologico”Trattamento medico “gastroenterologico”
Trattamento medico “non gastroenterologico”Trattamento medico “non gastroenterologico”
PEGPEG
PEJPEJ
LapLap--fundo+lapegfundo+lapeg














![Esophageal motility abnormalities in …...ineffective esophageal acid and bolus clearance, delayed gastric emptying and impaired mucosal defensive fac-tors[9,10]. The recent advent](https://static.fdocumenti.com/doc/165x107/5f02136b7e708231d40273b5/esophageal-motility-abnormalities-in-ineffective-esophageal-acid-and-bolus-clearance.jpg)