DAL CASO CLINICO ALLA DECISIONE Bologna, 15 16 … · infezioni necrotizzanti di cute +/- tessuti...
37
Quello che le linee guida non dicono Le infezioni dei tessuti molli a rapida evoluzione Francesco Cristini – Malattie Infettive Bologna DAL CASO CLINICO ALLA DECISIONE Bologna, 15‐16 novembre 2013
-
Upload
nguyenlien -
Category
Documents
-
view
214 -
download
0
Transcript of DAL CASO CLINICO ALLA DECISIONE Bologna, 15 16 … · infezioni necrotizzanti di cute +/- tessuti...

Quello che le linee guida non dicono
Le infezioni dei tessuti molli a rapida evoluzione
Francesco Cristini – Malattie Infettive Bologna
DAL CASO CLINICO ALLADECISIONE
Bologna, 15‐16 novembre 2013
INFEZIONI CUTANEE SUPERFICIALI
INFEZIONI CUTANEE PROFONDE NON NECROTIZZANTI
NECROTIZZANTI
INFEZIONI NECROTIZZANTI ESTESE AI TESSUTI MOLLI
FASCITI NECROTIZZANTI
GANGRENA GASSOSA
GANGRENA di FOURNIER
INFEZIONI NECROTIZZANTI DI CUTE +/- TESSUTI MOLLI
Caratteristiche comuni
• SEGNI e SINTOMI SISTEMICI
da FEBBRE a SEPSI, SEPSI SEVERA, SHOCK SETTICO • SEGNI e SINTOMI LOCALI
dolore importante, spesso non proporzionato all’entità della lesionelesioni cutanee poco circoscritteedema esteso anche oltre la sede di lesionepresenza di flittenecrepitio cutaneo correlato a presenza di gas in sottocuterapida evoluzione locale e sistemica
• NECESSITA’ DI APPROCCIO MEDICO-CHIRUGICO PRECOCE
• RUOLO DECISIVO DELLA CORRETTA TERAPIA ANTIMICROBICA
• MORTALITA’ ANCORA SIGNIFICATIVAMENTE ELEVATA

2009 20122000 20062003
PUBMED: “necrotizing fasciitis”
1990
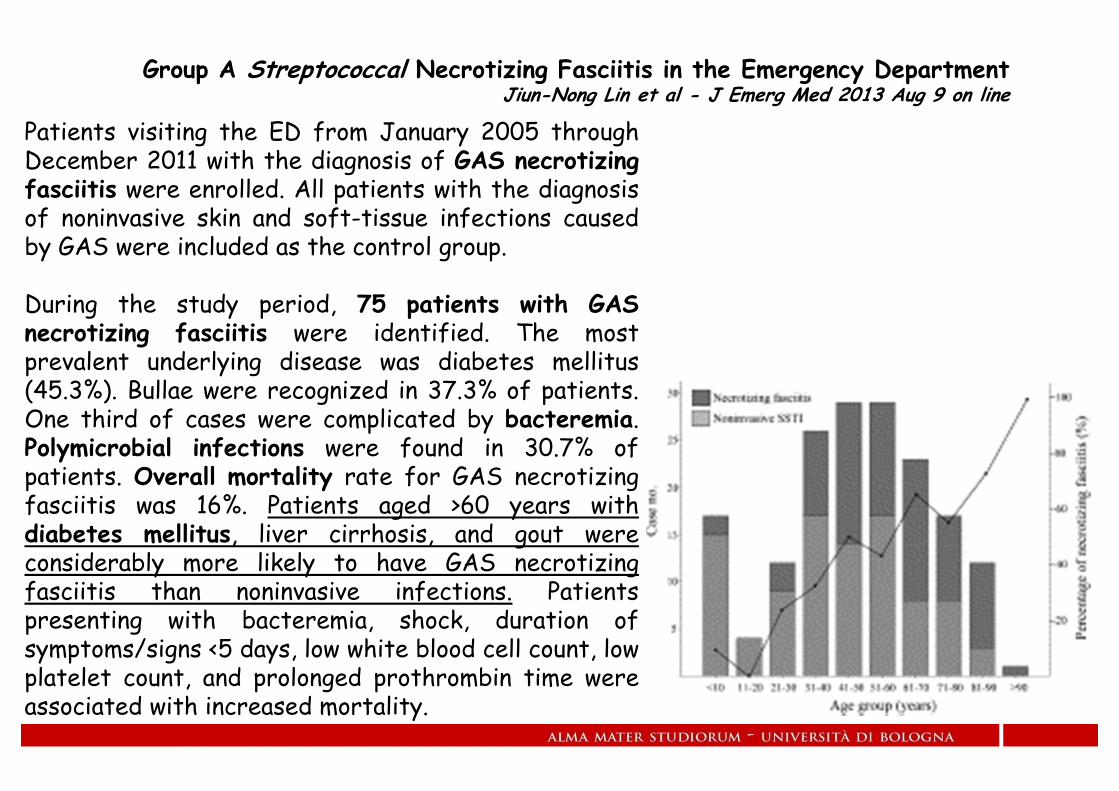
Group A Streptococcal Necrotizing Fasciitis in the Emergency DepartmentJiun-Nong Lin et al - J Emerg Med 2013 Aug 9 on line
Patients visiting the ED from January 2005 throughDecember 2011 with the diagnosis of GAS necrotizingfasciitis were enrolled. All patients with the diagnosisof noninvasive skin and soft-tissue infections causedby GAS were included as the control group.
During the study period, 75 patients with GASnecrotizing fasciitis were identified. The mostprevalent underlying disease was diabetes mellitus(45.3%). Bullae were recognized in 37.3% of patients.One third of cases were complicated by bacteremia.Polymicrobial infections were found in 30.7% ofpatients. Overall mortality rate for GAS necrotizingfasciitis was 16%. Patients aged >60 years withdiabetes mellitus, liver cirrhosis, and gout wereconsiderably more likely to have GAS necrotizingfasciitis than noninvasive infections. Patientspresenting with bacteremia, shock, duration ofsymptoms/signs <5 days, low white blood cell count, lowplatelet count, and prolonged prothrombin time wereassociated with increased mortality.

Quello che le linee guida non dicono
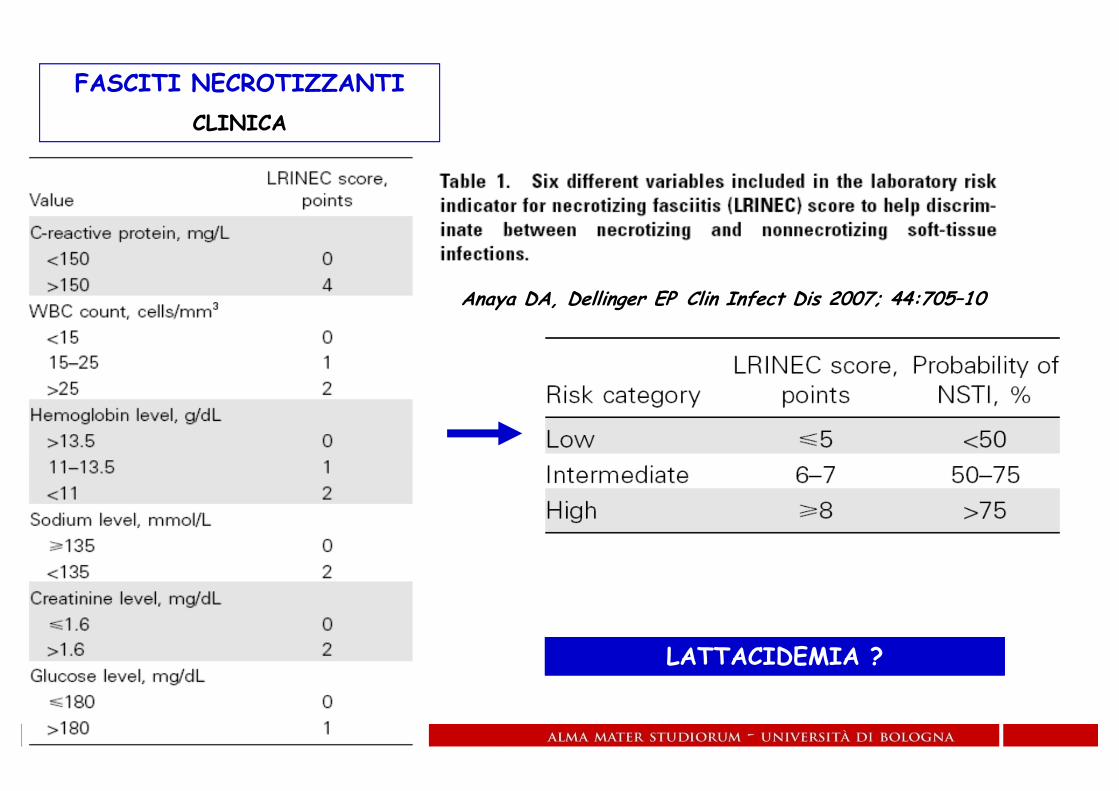
Anaya DA, Dellinger EP Clin Infect Dis 2007; 44:705–10
FASCITI NECROTIZZANTICLINICA
LATTACIDEMIA ? LATTACIDEMIA ?
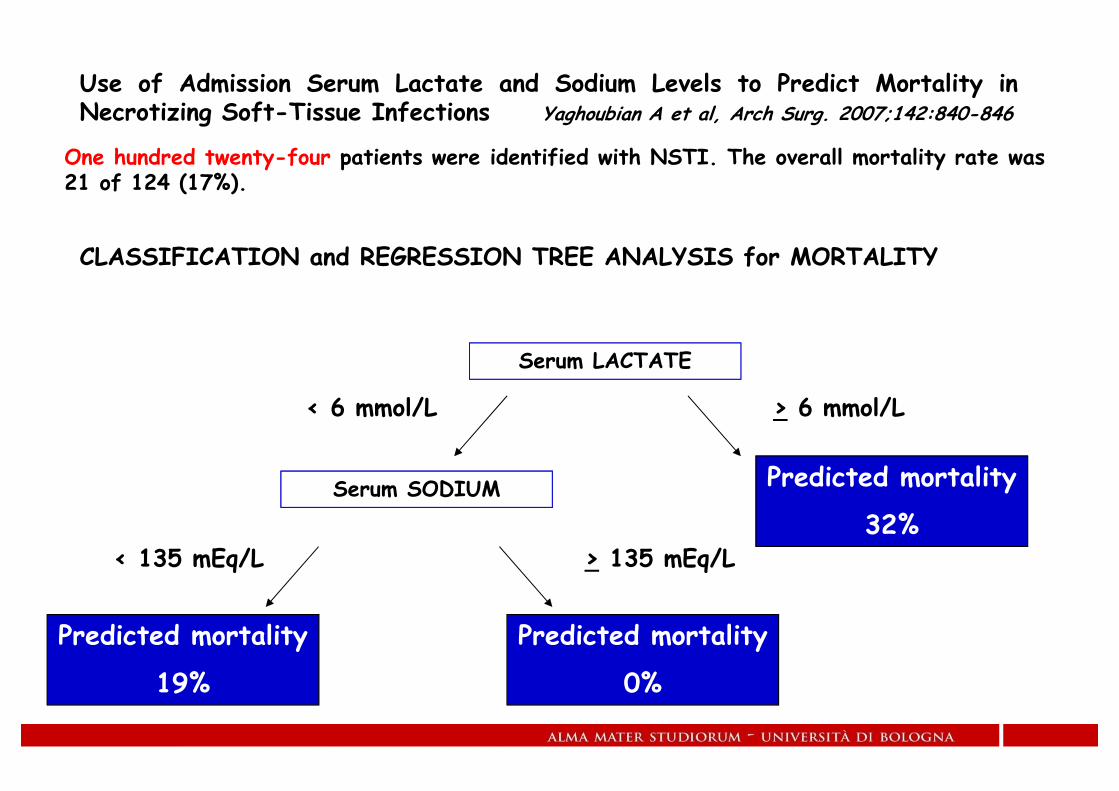
Use of Admission Serum Lactate and Sodium Levels to Predict Mortality inNecrotizing Soft-Tissue Infections Yaghoubian A et al, Arch Surg. 2007;142:840-846
CLASSIFICATION and REGRESSION TREE ANALYSIS for MORTALITY
Serum LACTATE
> 6 mmol/L
Predicted mortality
32%
< 6 mmol/L
Serum SODIUM
> 135 mEq/L< 135 mEq/L
Predicted mortality
0%
Predicted mortality
19%
One hundred twenty-four patients were identified with NSTI. The overall mortality rate was 21 of 124 (17%).
Clinical assessment of the severity of infection is crucial…
Patients with soft-tissue infection and SEPSIS (e.g., fever or
hypothermia, tachycardia, tachypnea), or with SEVERE SEPSIS
(e.g, hypotension) HOSPITALIZATION
Search for definitive etiologic diagnosis
Prompt surgical evaluation for suspected necrotizing infections
Prompt antimicrobial therapy

Other clues to potentially severe deep soft-tissue infection include the following:
- pain disproportionate to the physical findings,- violaceous bullae,- cutaneous hemorrhage,- skin sloughing,- skin anesthesia,- gas in the tissue,- rapid progression
Unfortunately, these signs and symptoms often appear later in the course ofnecrotizing infections. In these cases, emergent surgical evaluation is of paramountimportance for both diagnostic and therapeutic reasons.… dozens of microbes may cause soft-tissue infections, and although specificbacteria may cause a particular type of infection, considerable overlaps in clinicalpresentations exist.

Quello che le linee guida non dicono
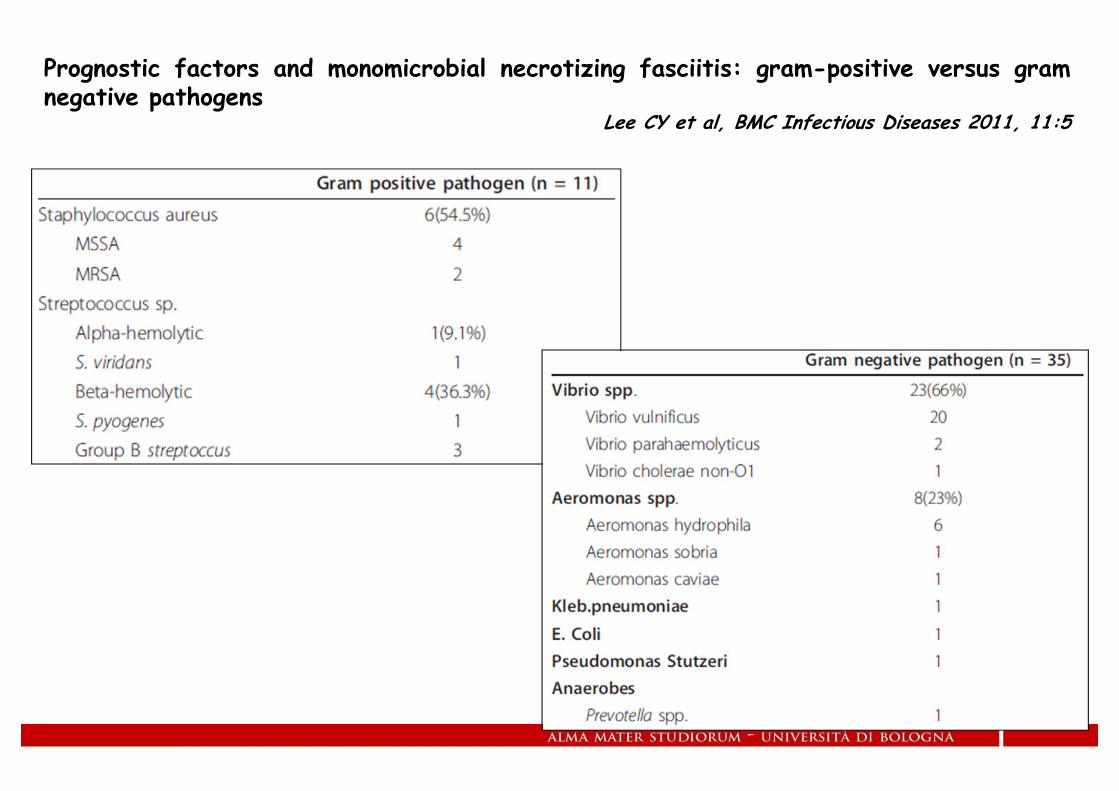
Prognostic factors and monomicrobial necrotizing fasciitis: gram-positive versus gramnegative pathogens
Lee CY et al, BMC Infectious Diseases 2011, 11:5
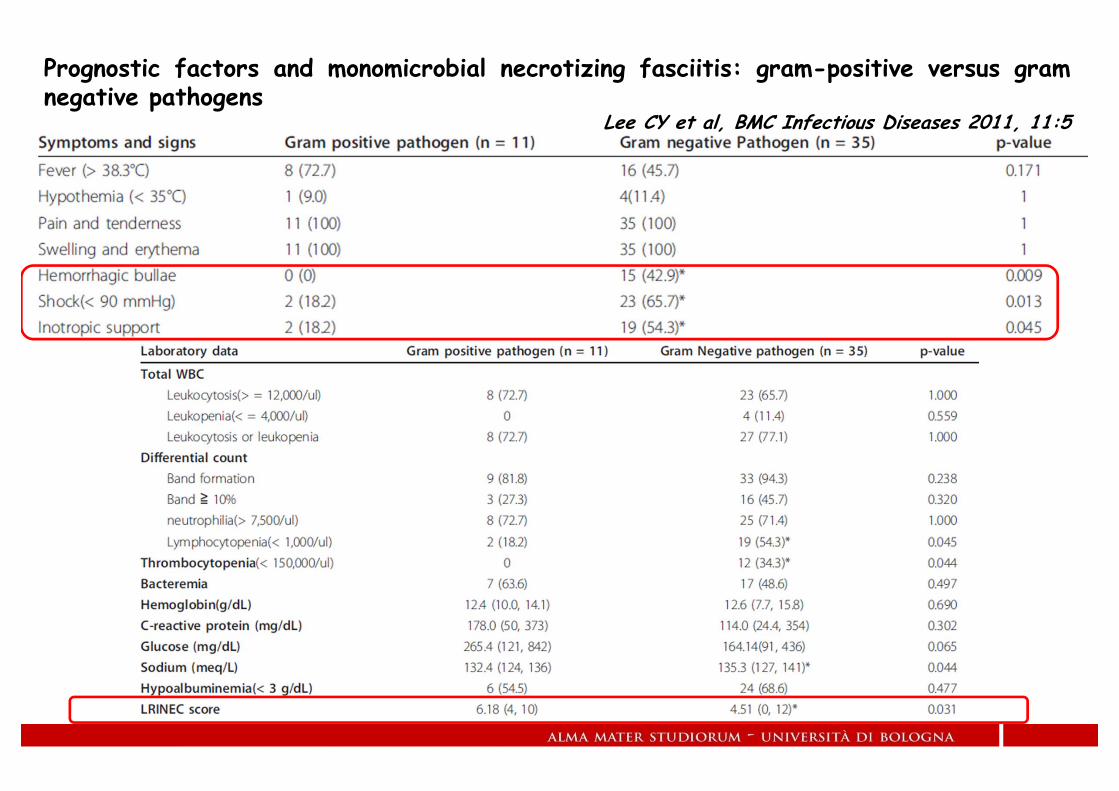
Prognostic factors and monomicrobial necrotizing fasciitis: gram-positive versus gramnegative pathogens
Lee CY et al, BMC Infectious Diseases 2011, 11:5

FONDAMENTI TERAPEUTICI DELLE FASCITI NECROTIZZANTI
Precocità diagnostica
Precocità ed aggressività chirurgica
Approccio intensivistico
Terapia antibiotica precoce- spettro ampio comprendente anche patogeni emergenti
CA-MRSAS. pyogens MLS-RP. aeruginosa in soggetti immunodepressiEnterobacteriaceae ESBL + in G. di Fournier e diabetici
- attività battericida massimale- azione correlata ad inibizione della sintesi proteica

Practice Guidelines for the Diagnosis and Management of Skin and Soft-TissueInfections
Dennis L. Stevens et al - Clinical Infectious Diseases 2005; 41:1373–406

Quello che le linee guida non dicono
“… Current treatment guidelines for the management of cSSTIsand cIAIs do not reflect the availability of new antibiotics, or thelatest trends in bacterial resistance…”
Review of the guidelines for complicated skin and soft tissue infections andintra-abdominal infections—are they applicable today?
Caìnzos M Clin Microbiol Infect 2008; 14 (Suppl. 6): 9–18

Acute bacterial skin infections: developments since the 2005 Infectious diseasessociety of america (idsa) guidelines
Gregory J. Moran et al - J Emerg Med. 2013 Jun;44(6):e397-412
When the Infectious Diseases Society of America (IDSA) prepared their 2005guidelines on the management of skin and soft tissue infections, the role of CA-MRSAwas not yet recognized, and therefore, empiric treatment of this organism was notrecommended.

Antimicrobial resistance surveillance in Europe 2010

Antimicrobial resistance surveillance in Europe 2010
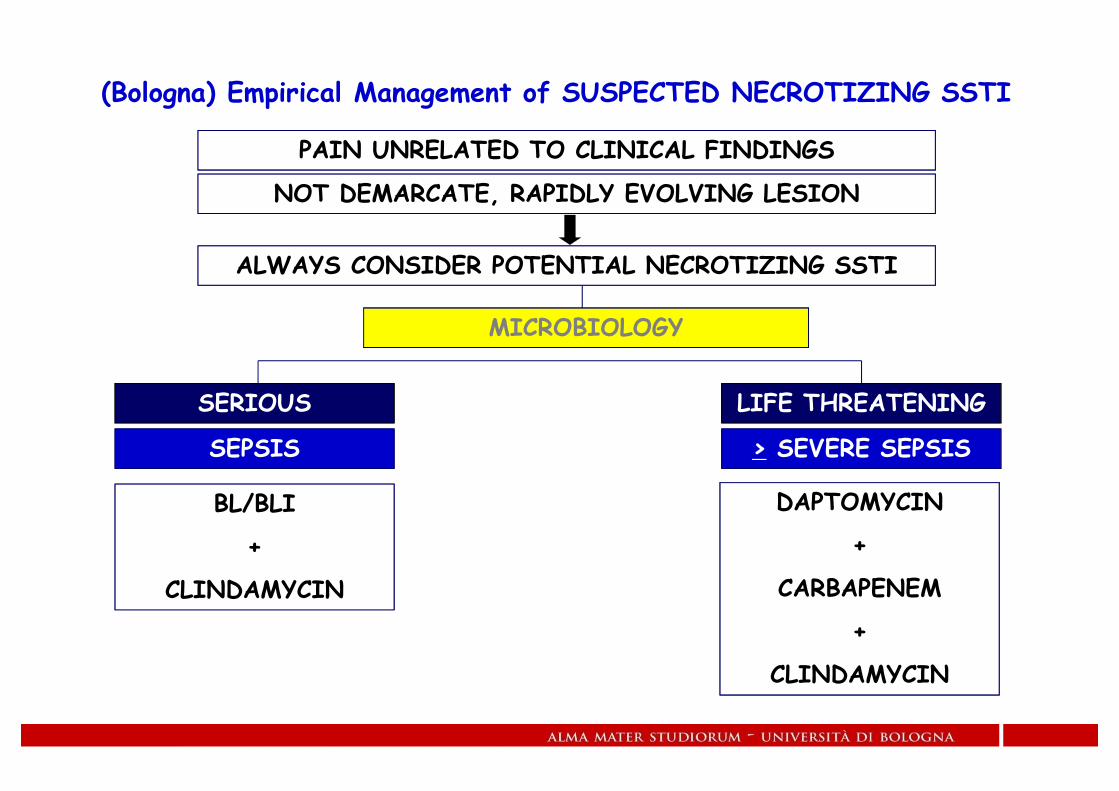
(Bologna) Empirical Management of SUSPECTED NECROTIZING SSTI
PAIN UNRELATED TO CLINICAL FINDINGS
NOT DEMARCATE, RAPIDLY EVOLVING LESION
MICROBIOLOGY
SERIOUS LIFE THREATENING
SEPSIS > SEVERE SEPSIS
BL/BLI
+
CLINDAMYCIN
DAPTOMYCIN
+
CARBAPENEM
+
CLINDAMYCIN
ALWAYS CONSIDER POTENTIAL NECROTIZING SSTI

SINDROME DELLO SHOCK TOSSICO
DEFINIZIONE di CASOWorking Group on Severe Streptococcal Infection, JAMA 1993
I. Isolamento di S. pyogenes
A. da sito normalmente sterile (sangue / ferita chirurgica)
B. da sito non sterile (cavo orale/ vagina / lesione cutanea)
II. Segni Clinici
A. Ipotensione (sistolica < 90 mmHg)
B. Due o più dei seguenti segni
1. Creatinina > 2 mg/dl
2. Piastrine < 100.000 / mmc o quadro di CID
3. AST o ALT o Bilirubina > 2 volte limite superiore di norma
4. ARDS
5. Esantema micro-papulare disseminato
6. Fascite necrotizzante e/o mionecrosi o gangrenaDIAGNOSI di CERTEZZA
IA + II (A + B)DIAGNOSI di PROBABILITA’
IB + II (A + B)

TERAPIA TSS
IMMUNOGLOBULINE ad alto dosaggiostrumento di prevenzione e trattamento della TSS azione correlata ad antagonismo verso i super-antigeni di GASriduzione della mortalità in studi retrospettiviriduzione mortalità a 28 giorni (10% vs 36%) in piccolo studio prospettico
Darenberg J et al, Clin Infect Dis 2003; 37:333-340
dati clinici non decisiviassenza di consenso sulla posologia (0.5 g/kg per 2 giorni)
Darenberg J et al, Clin Infect Dis 2003; 37:333-340

Toxic Shock Syndrome: Major Advances in Pathogenesis, But Not TreatmentDonald E. Low - Crit Care Clin 2013 Jul;29(3):651-75
Toxic shock syndrome (TSS) is primarily the result of a superantigen-mediated cytokine storm and M protein-mediated neutrophil activation, resulting in the release of mediators leading to respiratory failure, vascularleakage, and shock. Mortality for streptococcal TSS still hovers at 50%. There is evidence to support a role forintravenous immunoglobulin (IVIG) in the treatment of streptococcal TSS. An observational study suggests that aninitial conservative surgical approach combined with the use of immune modulators, such as IVIG, may reduce themorbidity associated with extensive surgical exploration in hemodynamically unstable patients without increasingmortality.
(GAS)
Staphylococcal TSS is secondary to a localized infection, whereas STSS is the result of an invasive infection.

trappole e forme subdole

Despite two intravenous doses ofamoxi/clav acid, her pain worsened andthe erythema continued to extend. Overthe next 8 h, pain prevented her frombreastfeeding; she was hypotensive andhad rigors and persisting pyrexia (38.0 C).Blood tests showed leucocytosis (125 10⁹/L) and high CRP (183 mg/L) andcreatine kinase (150 IU/L).
Ten days after an uncomplicated vaginaldelivery at home, a 35-year-old womanpresented to the ED with a 16 h historyof severe, burning right breast pain, and2 h of diarrhoea and vomiting. Onexamination, her temperature was37.9 C, she was tachycardic (120/min),and her blood pressure was 100/70 mmHg. Her chest was clear, with oxygensaturation 96% on air. Blood testsshowed leucocytosis of 11 3 10⁹/L anda high C-reactive protein (CRP) of 61mg/L. The initial diagnosis was mastitis.
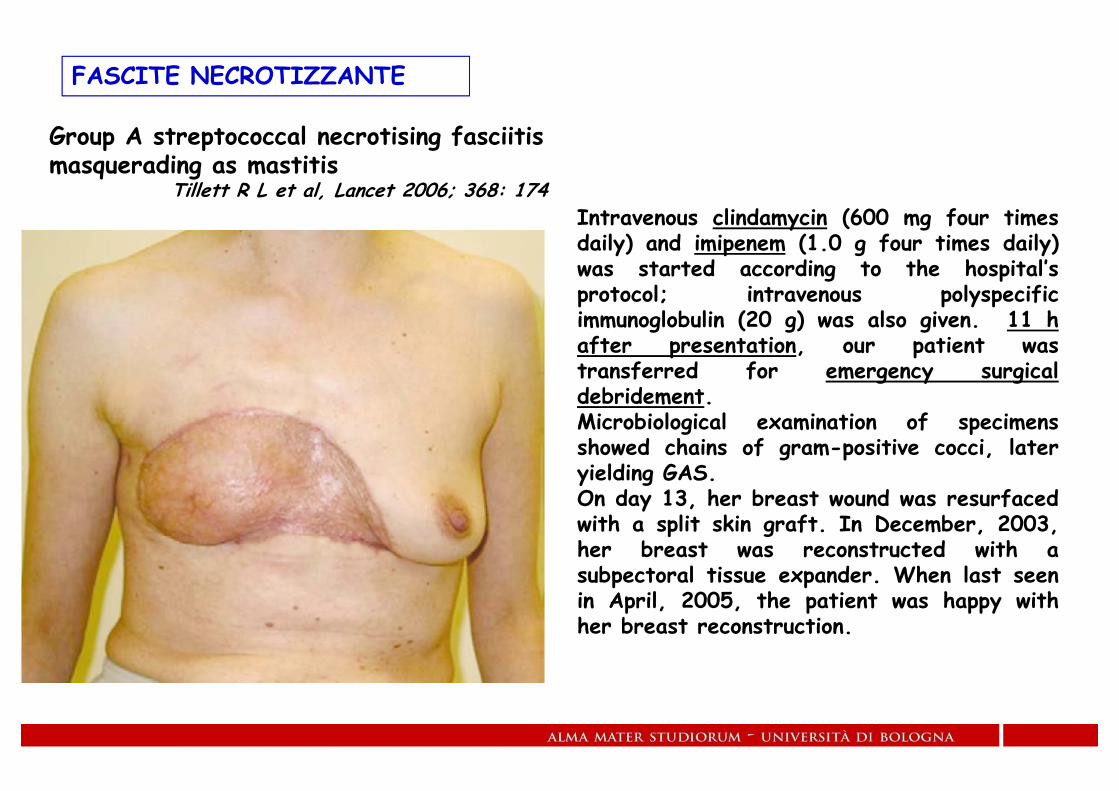
Intravenous clindamycin (600 mg four timesdaily) and imipenem (1.0 g four times daily)was started according to the hospital’sprotocol; intravenous polyspecificimmunoglobulin (20 g) was also given. 11 hafter presentation, our patient wastransferred for emergency surgicaldebridement.Microbiological examination of specimensshowed chains of gram-positive cocci, lateryielding GAS.On day 13, her breast wound was resurfacedwith a split skin graft. In December, 2003,her breast was reconstructed with asubpectoral tissue expander. When last seenin April, 2005, the patient was happy withher breast reconstruction.
Group A streptococcal necrotising fasciitis masquerading as mastitis
Tillett R L et al, Lancet 2006; 368: 174
FASCITE NECROTIZZANTE

Immunocompromised Status in Patients With Necrotizing Soft-Tissue InfectionEmily Z. Keung et al - JAMA Surg. 2013;148(5):419-426
Corticosteroid use, active malignancy, receipt of chemotherapy or radiation therapy, diagnosis of HIV or AIDS, orprior solid organ or bone marrow transplantation with receipt of chronic immunosuppression.
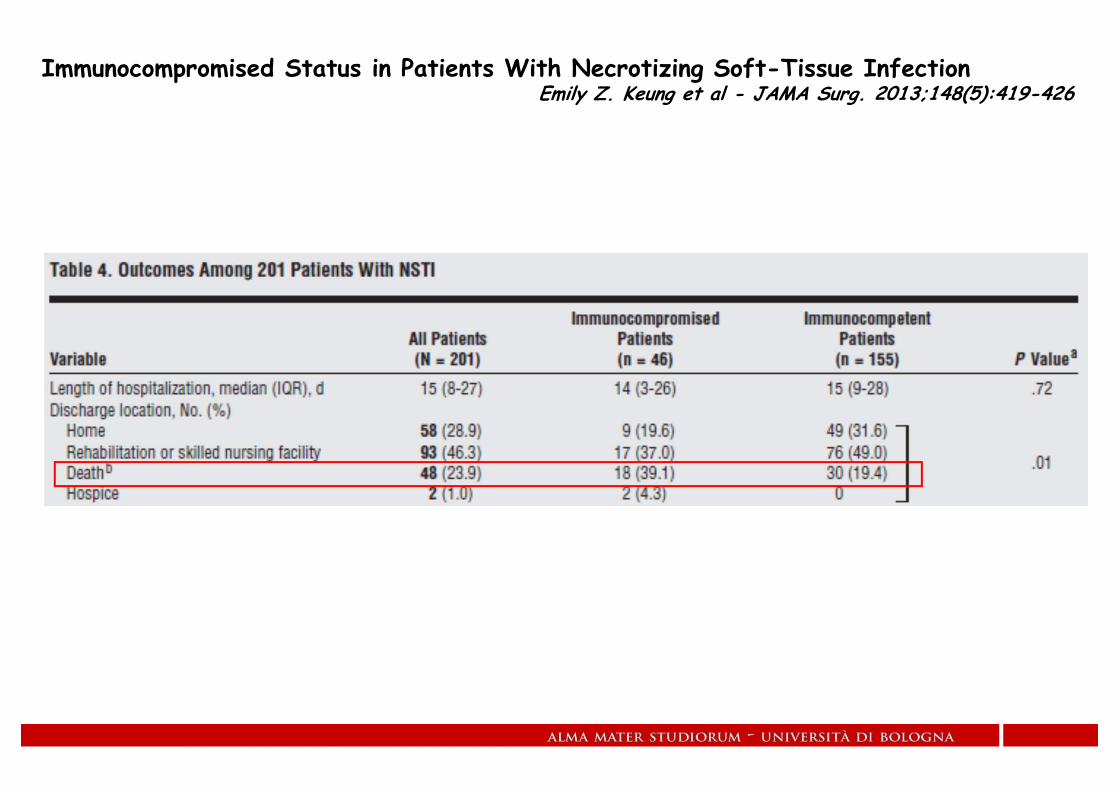
Immunocompromised Status in Patients With Necrotizing Soft-Tissue InfectionEmily Z. Keung et al - JAMA Surg. 2013;148(5):419-426

ECTIMA GANGRENOSO
Infezione cutanea su base ematogena,conseguente ad invasione batterica dei vasi delderma con vasculite necrotizzante.
Si manifesta con la formazione di aree nodulariindolenti, necrotiche con componenteemorragica che si espandono progressivamentema restano sempre ben delimitata dalla cutesana.
Ad esso si associano segni e sintomi di SIRS
Occorre in paziente immunocompromessi (speciein soggetti con emopatie maligne, HIV, terapieimmunodeprimenti, diabete) o critici (ustionati)
L’agente etiologico preminente è P. aeruginosa
Pz, di anni 72 affetta da LLC afferita con quadro di sepsi grave, evoluta in shock settico nel volgere di poche ore.
Caso clinicoCaso clinico
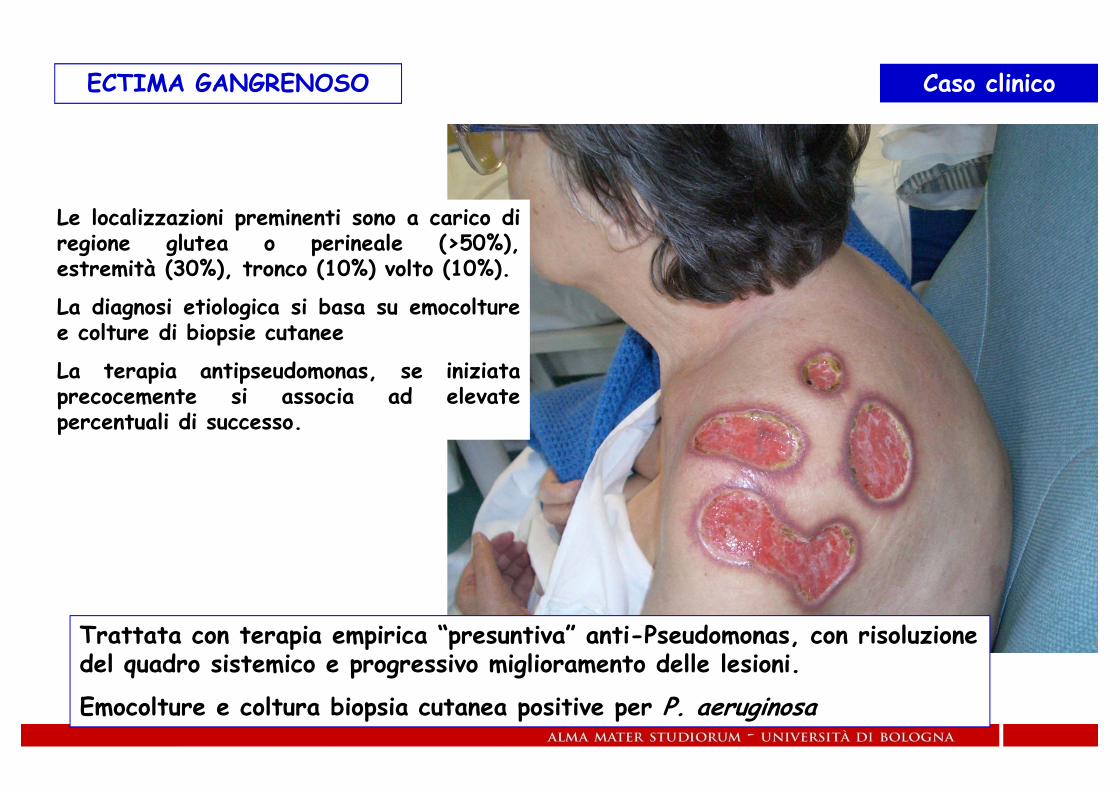
ECTIMA GANGRENOSO
Le localizzazioni preminenti sono a carico diregione glutea o perineale (>50%),estremità (30%), tronco (10%) volto (10%).
La diagnosi etiologica si basa su emocolturee colture di biopsie cutanee
La terapia antipseudomonas, se iniziataprecocemente si associa ad elevatepercentuali di successo.
Trattata con terapia empirica “presuntiva” anti-Pseudomonas, con risoluzione del quadro sistemico e progressivo miglioramento delle lesioni.
Emocolture e coltura biopsia cutanea positive per P. aeruginosa
Caso clinicoCaso clinico

Ectima gangrenoso in soggetto maschio affetto da NHL
Emocolture positive per P. aeruginosa
ECTIMA GANGRENOSO Caso clinicoCaso clinico

Associata VAC-therapy
ECTIMA GANGRENOSO Caso clinicoCaso clinico

Evoluzione locale dopo 2 settimane di VAC therapy
Successiva guarigione con lembo
ECTIMA GANGRENOSO Caso clinicoCaso clinico

Paziente cirrotico, diabetico scompensato, IRC, ipopituitarismo in terapia steroidea cronica.
Mucormicosi da Rhizopus spp
Caso clinicoCaso clinico

INFEZIONI cute e tessuti molli DEL PAZIENTE IMMUNODEPRESSO