Criteri di scelta per una terapia anticoagulante - FCSA AGENO.pdf · Criteri di scelta per una...
20
Criteri di scelta per una terapia anticoagulante Walter Ageno Degenza Breve Internistica e Centro Trombosi Dipartimento di Medicina Clinica e Sperimentale Università dell’Insubria Varese
-
Upload
nguyentruc -
Category
Documents
-
view
219 -
download
0
Transcript of Criteri di scelta per una terapia anticoagulante - FCSA AGENO.pdf · Criteri di scelta per una...

Criteri di scelta per una terapia anticoagulante
Walter Ageno Degenza Breve Internistica e Centro Trombosi
Dipartimento di Medicina Clinica e Sperimentale Università dell’Insubria
Varese

Conflitti di interesse
• Supporto alla ricerca: Bayer Healthcare, Boehringer Ingelheim
• Advisory Boards: Bayer Healthcare, Boehringer Ingelheim, Daiichi Sankyo, BMS-Pfizer, Italfarmaco, ONO
• Fees per letture a congressi: Bayer Healthcare, Boehringer Ingelheim, Daiichi Sankyo, BMS-Pfizer, Stago
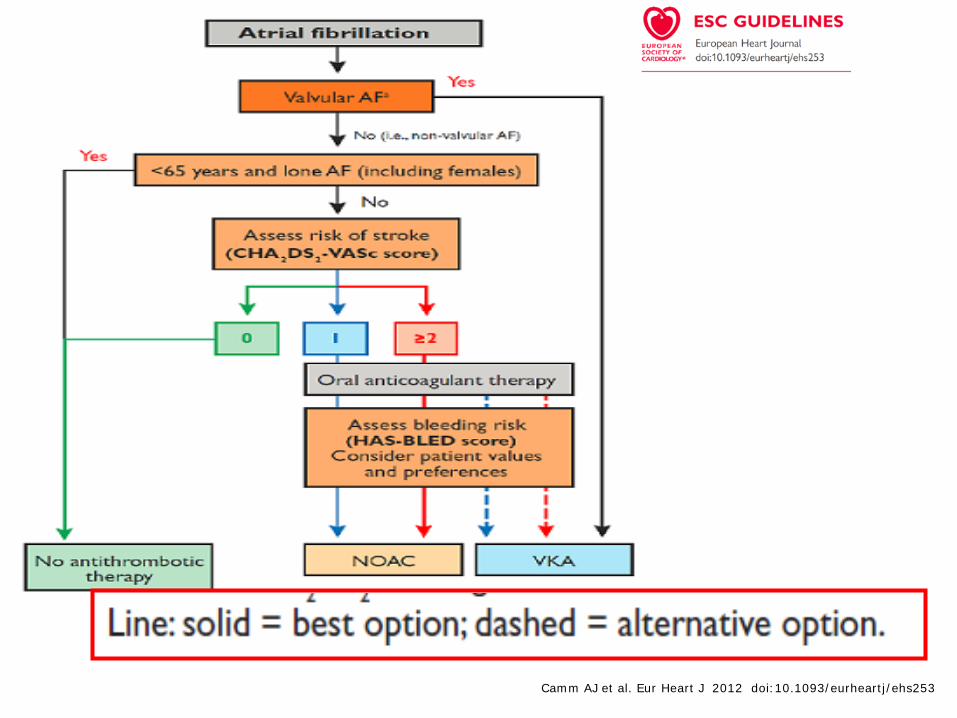
Camm AJ et al. Eur Heart J 2012 doi:10.1093/eurheartj/ehs253

Event rates in patients with a CHA2DS2-VASc score of 1
Risk of stroke or stroke/TIA/SE
CHA2DS2-VASc score 1 (all) 1 (men) 1 (women)
Events rate per 100 person-yrs 0.5 – 0.9 0.5 – 0.7 0.1 – 0.2
1. 140,420 untreated patients from the Swedish National Patient Register (2005–2010). Friberg L, et al. J Am Coll Cardiol 2015;65:225-32.
The low annual event rates call into question the need for or use of oral anticoagulation therapy in low-risk patients

ESC recommendations based on CHA2DS2-VASc score
RISK GOUPS And Guideline Recommendations
CHA2DS2-VASc score
Men Women
Do not anticoagulate (ESC) 0 1
Consider anticoagulation (ESC 2012) 1 -
Consider anticoagulation (ESC 2016) 1 2
Consider / not recommend anticoagulation (ESC 2016) - 2
Recommend anticoagulation (ESC 2012) ≥2 ≥2
Recommend anticoagulation (ESC 2016) ≥2 ≥3

Direct Oral Anticoagulants Compared to Warfarin: Stroke or Systemic Embolism
0.5 1
HR 0.65 (95% CI, 0.52 to 0.81)
HR 0.90 (95% CI, 0.74 to 1.10)
HR 0.88 (95% CI, 0.74 to 1.03)
HR 0.79 (95% CI, 0.66 to 0.95)
Hazard Ratio
Study Drug Better Warfarin Better
1. Connolly SJ et al. N Engl J Med. 2010;363:1875-1876. 2. Patel MR et al. N Engl J Med. 2011;365:883-891. 3. Granger CB et al. N Engl J Med. 2011;365:981-992. 4. Giugliano RP et al, for the ENGAGE-AF TIMI 48 Investigators; NEJM; 2013, doi: 10.1056/NEJMoa1310907
Dabigatran 150 mg BID1
Dabigatran 110 mg BID1
Rivaroxaban 20 mg QD2
Apixaban 5 mg BID3
Edoxaban 60 mg QD4
Edoxaban 30 mg QD4
1.5
HR 1.13 (95% CI, 0.96 to 1.34)
HR 0.87 (95% CI, 0.73 to 1.04)

Meta-analysis: ARISTOTLE, ENGAGE-AF, RE-LY and ROCKET AF
VKAs versus novel OACs: organ-specific patterns of bleeding
Relative risk difference (%) (95% CI)
Intracranial bleeding
Other major bleeding
Gastrointestinal bleeding
Vanassche et al, 2014
Favours novel OAC Favours warfarin –100 –50 0 50 100
84,540 patients and 4781 bleeding events
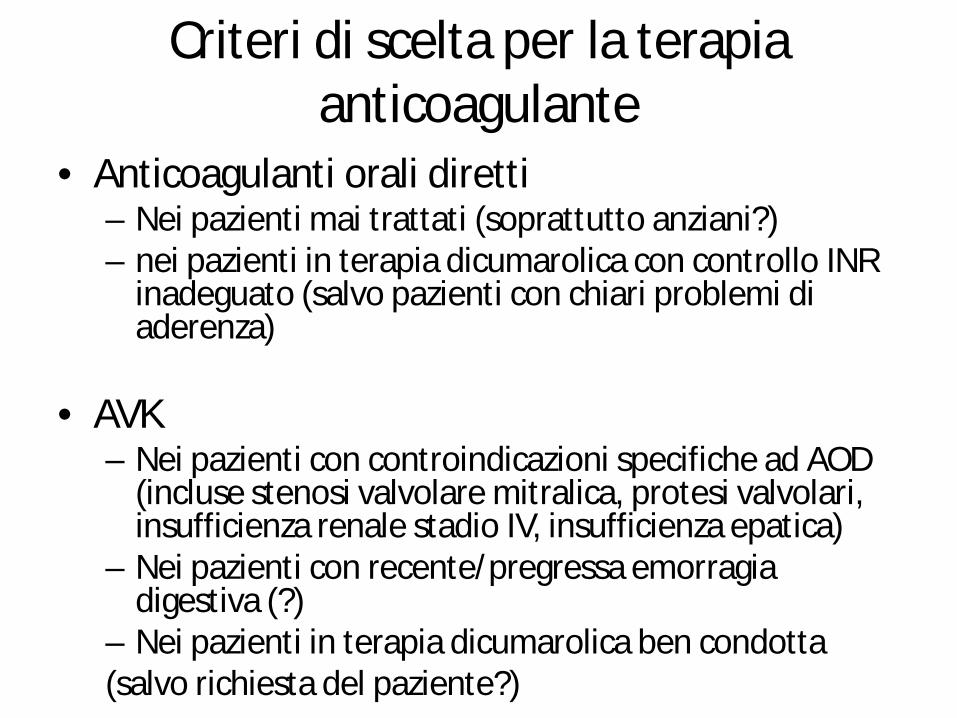
Criteri di scelta per la terapia anticoagulante
• Anticoagulanti orali diretti – Nei pazienti mai trattati (soprattutto anziani?) – nei pazienti in terapia dicumarolica con controllo INR
inadeguato (salvo pazienti con chiari problemi di aderenza)
• AVK
– Nei pazienti con controindicazioni specifiche ad AOD (incluse stenosi valvolare mitralica, protesi valvolari, insufficienza renale stadio IV, insufficienza epatica)
– Nei pazienti con recente/pregressa emorragia digestiva (?)
– Nei pazienti in terapia dicumarolica ben condotta (salvo richiesta del paziente?)

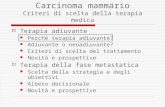
Evolution in baseline treatment for patients enrolled in sequential cohorts of GARFIELD-AF
4,2 13,8 26,3 37,2 43,1
0
20
40
60
80
100
Cohort 1 Cohort 2 Cohort 3 Cohort 4 Cohort 5
Prop
ortio
n of
pat
ient
s on
trea
tmen
t, %
VKA±AP FXA/DTI±AP AP None
57.4% 71.8%
2010–2011 2011–2013 2013–2014 2014–2015 2015–2016
Cohorts 1–5, N=51,270

How are low and high risk AF patients managed in practice?
• Contrary to international guideline recommendations, – 28% high-risk patients (CHA2DS2-VASc ≥2) are not anticoagulated
0 1 ≥2 CHA2DS2-VASc
0
10
20
30
40
50
60
70
80
90
100
(n=352) (n=1336) (n=9027)
Prop
ortio
n of
pat
ient
s, %
– 51% of very low-risk patients (CHA2DS2-VASc 0) are anticoagulated
VKA ± AP
NOAC ± AP
Camm AJ et al. Heart 2016 (in press)
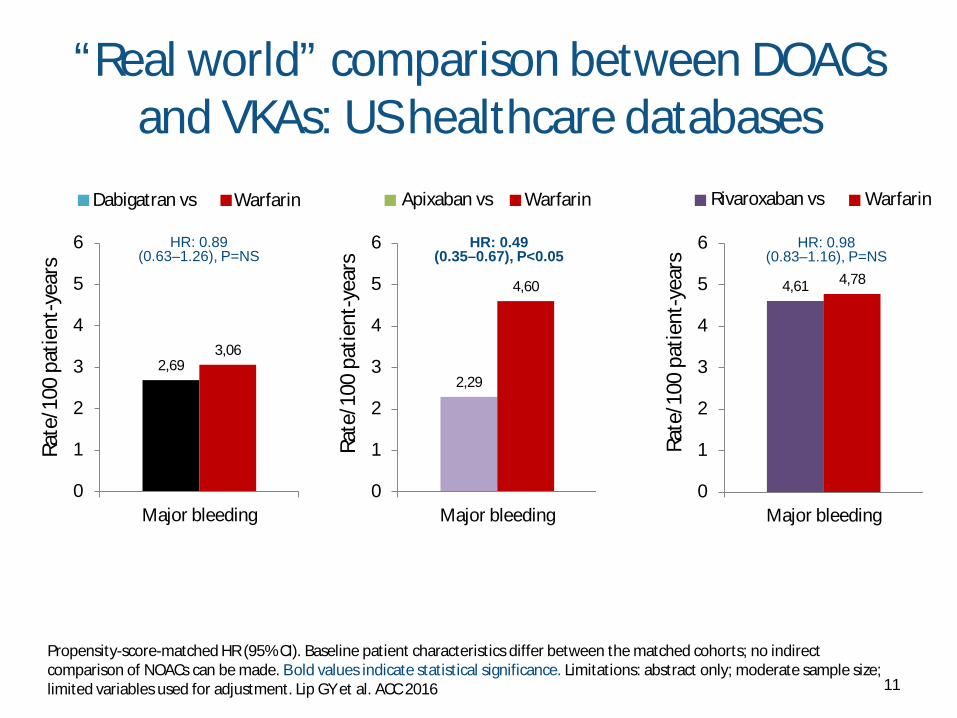
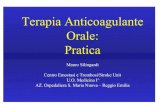
“Real world” comparison between DOACs and VKAs: US healthcare databases
11
2,69 3,06
0
1
2
3
4
5
6
Major bleeding
Rate
/100
pat
ient
-yea
rs
2,29
4,60
0
1
2
3
4
5
6
Major bleeding
Rate
/100
pat
ient
-yea
rs
4,61 4,78
0
1
2
3
4
5
6
Major bleeding
Rate
/100
pat
ient
-yea
rs HR: 0.89
(0.63–1.26), P=NS HR: 0.49
(0.35–0.67), P<0.05 HR: 0.98
(0.83–1.16), P=NS
Propensity-score-matched HR (95% CI). Baseline patient characteristics differ between the matched cohorts; no indirect comparison of NOACs can be made. Bold values indicate statistical significance. Limitations: abstract only; moderate sample size; limited variables used for adjustment. Lip GY et al. ACC 2016
Dabigatran vs Warfarin Apixaban vs Warfarin Rivaroxaban vs Warfarin

Efficacy: propensity-matched medication comparison
Event Rate per 100 person-years
Xiaoxi Yao et al. J Am Heart Assoc. 2016;5:e003725 - doi: 10.1161/JAHA.116.003725
Hazard Ratio (95% CI) p value
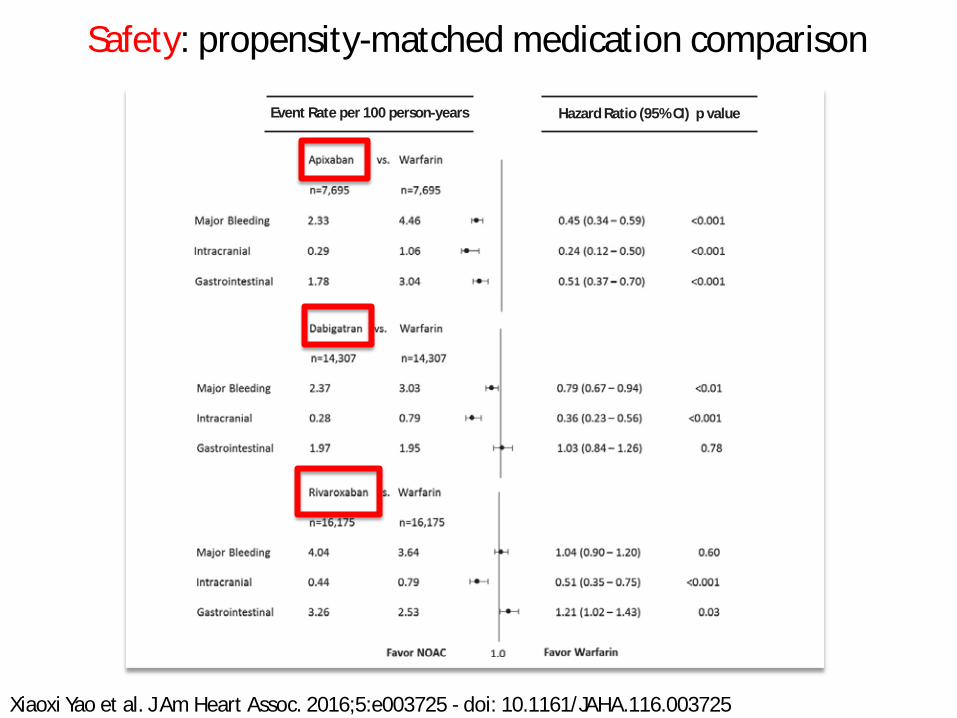
Safety: propensity-matched medication comparison
Xiaoxi Yao et al. J Am Heart Assoc. 2016;5:e003725 - doi: 10.1161/JAHA.116.003725
Event Rate per 100 person-years
Hazard Ratio (95% CI) p value

Real-World Evidence
• Real-world evidence is a broad term for many different study designs, including, in order of strength of evidence: – Retrospective clinical studies (including case/case
series studies) – Claims database analyses – Prospective registries – Phase IV non-interventional studies
Low
High
Strength of evidence

Design of GLORIA-AF
When baseline characteristics of patients receiving dabigatran and VKA are comparable
Before approval of dabigatran, the first
available NOAC After approval of dabigatran
Patients on dabigatran
Baseline Visit
Phase I Cross-sectional analysis
All patients
Phase II Cross-sectional and dabigatran follow-up
Phase III Cross-sectional and comparative analyses
Baseline Visit Baseline Visit
3M 6M 1YR 2YR 6M 1YR 2YR 3YR
Status: Currently ongoing (Europe, Asia, North America, Latin America, Africa/Middle East)
Status: Ended January 2013
Status: Currently ongoing (Europe, Asia, North America, Latin America)
Huisman MV, et al. Am Heart J. 2014;167:329–334 NOAC, non-Vitamin K antagonist oral anticoagulant; VKA, vitamin K antagonist
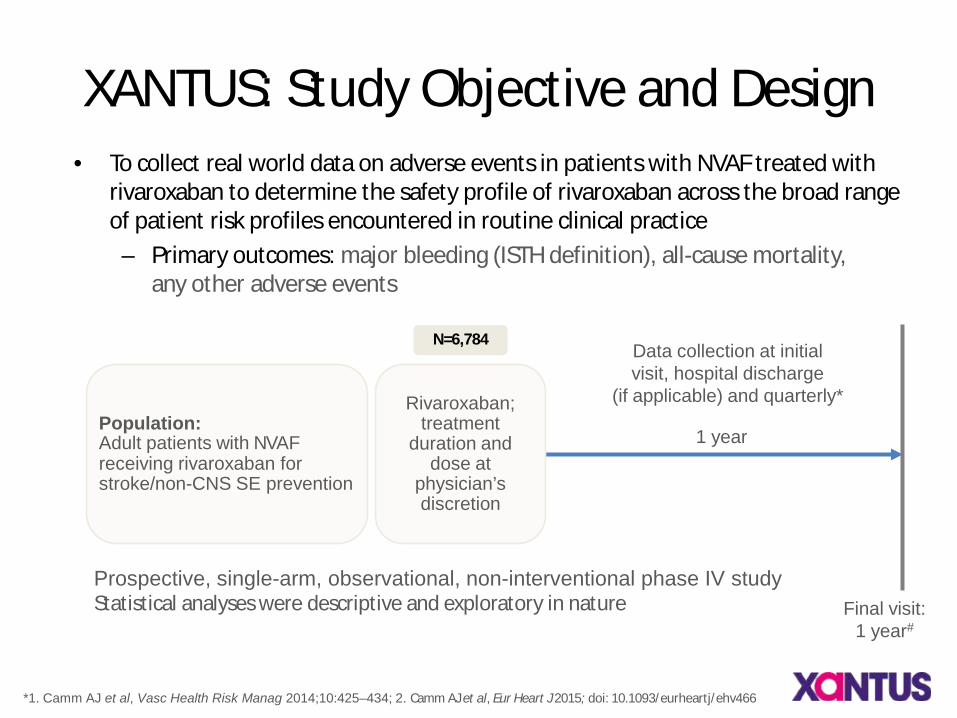
XANTUS: Study Objective and Design • To collect real world data on adverse events in patients with NVAF treated with
rivaroxaban to determine the safety profile of rivaroxaban across the broad range of patient risk profiles encountered in routine clinical practice – Primary outcomes: major bleeding (ISTH definition), all-cause mortality,
any other adverse events
Final visit: 1 year#
Data collection at initial visit, hospital discharge
(if applicable) and quarterly*
Population: Adult patients with NVAF receiving rivaroxaban for stroke/non-CNS SE prevention
Rivaroxaban; treatment
duration and dose at
physician’s discretion
*1. Camm AJ et al, Vasc Health Risk Manag 2014;10:425–434; 2. Camm AJ et al, Eur Heart J 2015; doi: 10.1093/eurheartj/ehv466
Prospective, single-arm, observational, non-interventional phase IV study Statistical analyses were descriptive and exploratory in nature
1 year
N=6,784

RCP: dosi raccomandate per età e funzionalità renale
1. Apixaban SmPC 2014 2. Dabigatran SmPC 2013 3. Rivaroxaban SmPC 2013
2. 4. Edoxaban SmPc, 2016
Caratteristiche Apixaban1 Dabigatran2 Rivaroxaban3 Edoxaban4
Insufficienza renale lieve (CrCl 50–80 mL/min) 5 mg BID 150 mg BID 20 mg OD 60 mg OD
Insufficienza renale moderata (CrCl: 30–50 mL/min)
5 mg BID
Pazienti con insufficienza renale moderata: la dose di dabigatran (300 mg o 220 mg) dovrebbe essere selezionata sulla base del rischio tromboembolico ed emorragico
Ridurre a 15 mg OD
Ridurre a 30 mg OD
Insufficienza renale severa (CrCl: 15–29 mL/min)
Ridurre la dose a 2,5 mg BID
Controindicato
Ridurre a 15 mg OD
Ridurre a 30 mg OD
Insufficienza renale con CrCl: <15 mL/min
Non raccomandato
Controindicato Non raccomandato Non raccomandato
Età 75–80 anni 5 mg BID
Pazienti 75–80 anni: la dose giornaliera di dabigatran (300 mg o 220 mg) dovrebbe essere selezionata sulla base del rischio tromboembolico ed emorragico
20 mg OD 60 mg OD
Età >80 anni 5 mg BID
Ridurre a 110 mg BID per l’aumentato rischio di sanguinamento in questa popolazione
20 mg OD 60 mg OD

Dabigatran 110 mg BID is used more widely in clinical practice
18 1. Connolly et al. N Engl J Med 2009; 2. BI, Data on file: DBG 15–04; 3. IMS Information Solutions UK Ltd. Patient data, June 2015
40%
58% 2%
RE-LY®1 Prescription data2,3
(All indications; IMS data June 2014–June 2015)
50% (n=6076)
50% (n=6015)
150 mg BID
110 mg BID
75 mg BID*
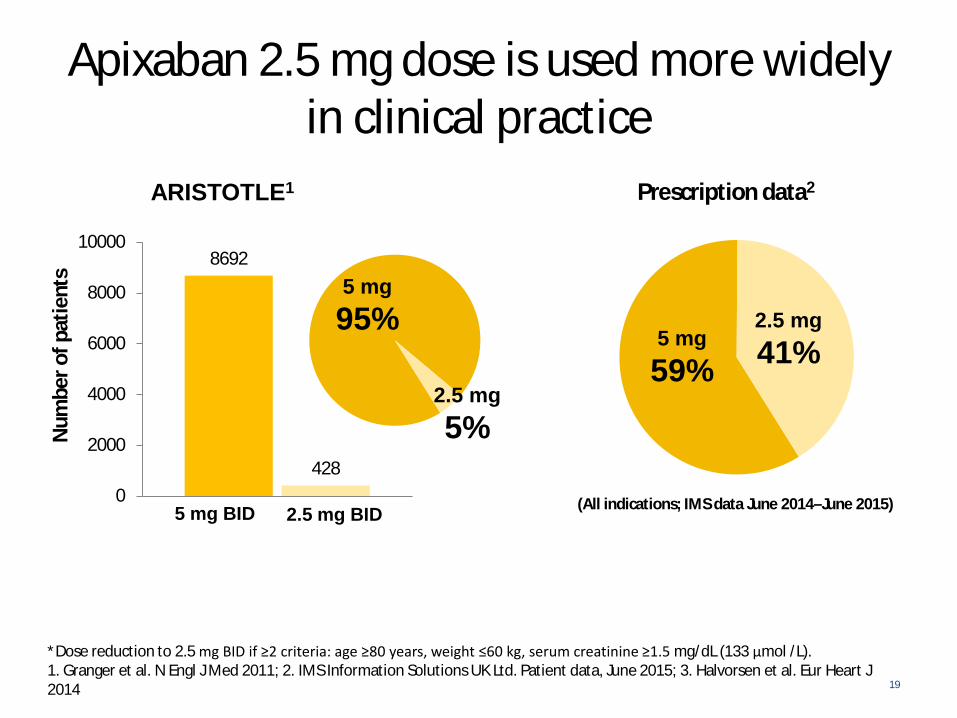
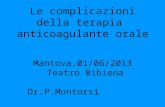
Apixaban 2.5 mg dose is used more widely in clinical practice
19
*Dose reduction to 2.5 mg BID if ≥2 criteria: age ≥80 years, weight ≤60 kg, serum creatinine ≥1.5 mg/dL (133 μmol /L). 1. Granger et al. N Engl J Med 2011; 2. IMS Information Solutions UK Ltd. Patient data, June 2015; 3. Halvorsen et al. Eur Heart J 2014
ARISTOTLE1 Prescription data2
(All indications; IMS data June 2014–June 2015)
8692
428 0
2000
4000
6000
8000
10000
Num
ber o
f pat
ient
s 95%
5 mg BID 2.5 mg BID
5 mg 95%
2.5 mg 5%
5 mg 59%
2.5 mg 41%

Conclusioni
• La prima scelta riguarda l’opportunità di anticoagulare
• La seconda scelta riguarda il farmaco, ricordando che non dovrebbe esserci più posto per l’ASA
• Gli anticoagulanti orali diretti offrono vantaggi per i pazienti che iniziano la terapia
• Esiste probabilmente il farmaco (e il dosaggio) giusto per il singolo paziente, ma dobbiamo imparare di più