Corso teorico di Ecografia generalista Villasimius 1 … acute e croniche - Dr... ·...
79
Piero Zaninetti Scuola di Ecografia Generalista SIEMG5 FIMMG Le pancreatiti acute e croniche Corso teorico di Ecografia generalista Villasimius 1-5 ottobre 2012 martedì 16 ottobre 12
Transcript of Corso teorico di Ecografia generalista Villasimius 1 … acute e croniche - Dr... ·...
Piero&Zaninetti&Scuola'di'Ecografia'Generalista
SIEMG5'FIMMG
Le pancreatiti acute e croniche
Corso teorico di Ecografia generalista Villasimius 1-5 ottobre 2012
martedì 16 ottobre 12
Pancreatite acuta
martedì 16 ottobre 12
Fattori eziologici
• Calcolosi biliare
• Abuso alcoolico
• Infezioni
• ipertrigliceridemia
• Ipercalcemia
• Tumori pancreatici e ampollari
• Cause jatrogene(chirurgia addominale e ERCP)
70-80 %
martedì 16 ottobre 12

Pancreatite acuta
• Classificazione di Atlanta ( 1992)
• Pancreatite lieve(80%): edema eventualmente associato a piccoli focolai di necrosi parenchimale
• Pancreatite severa(20 %): necrosi parenchimale,necrosi del tessuto adiposo peripancreatico,focolai emorragici intra e peri ghiandolari,essudazione intraperitoneale
martedì 16 ottobre 12
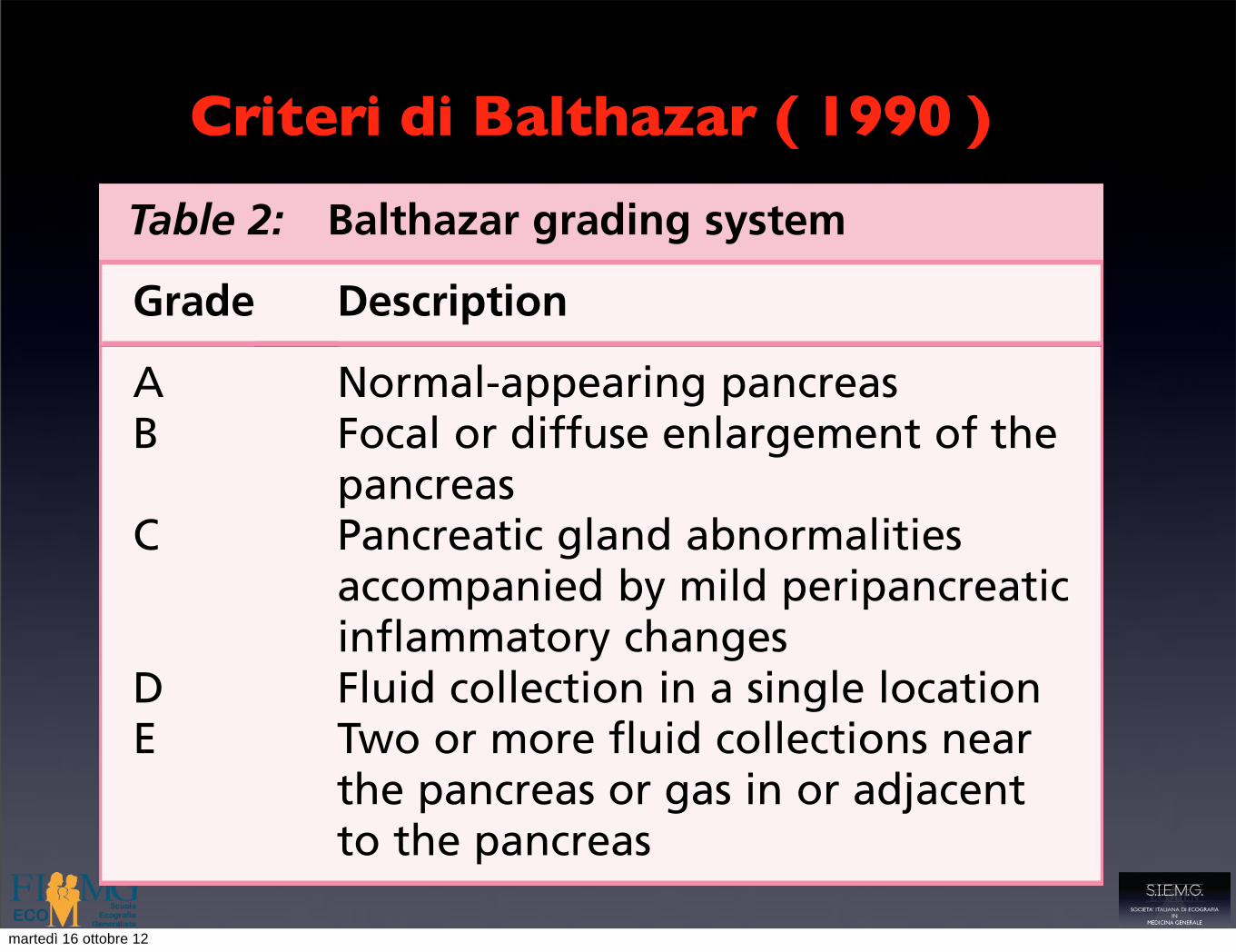
Criteri di Balthazar ( 1990 )
because of its anatomic contiguity with the pan-creas. Erosion of arteries can result in free hemor-rhage from the erosion site or in the formation ofa pseudoaneurysm (Fig. 9). The latter has the po-tential to rupture into the lesser sac, into the perito-neal cavity, or into an adjacent hollow organ. Onimaging, a pseudoaneurysm can be seen as a com-pletely or partially vascular cystic mass. In patientswho have a history of acute pancreatitis, one shouldsuspect a pseudoaneurysm when a cystic pancreaticmass demonstrates transient vascular enhance-ment. CT angiography and 3D reconstructions candemonstrate precisely the specific vessel involved.In addition to arterial complications, venousthrombosis in the portal-mesenteric circulation
can occur. In order of frequency, the splenic veinis involved most commonly, followed by the portaland the superior mesenteric veins (Fig. 10). Whenthe splenic vein is involved, left-sided portal hyper-tension can occur with the development of gastricand mesenteric varices.
Extrapancreatic findingsIn addition to peripancreatic fluid collections andvascular complications, abnormalities in othersolid organs (eg, liver and spleen) occasionallymay be seen at imaging. Because of the close prox-imity of the pancreatic tail and spleen, inflamma-tory processes may extend along splenic vesselsinto the splenic hilum. Splenic involvement in pan-creatitis includes intrasplenic pseudocyst, abscess,hemorrhage, and infarction (Fig. 11). Intrasplenichemorrhage occurs because of the erosion of smallintrasplenic vessels. Blood may collect beneath thesplenic capsule resulting in subcapsular hematoma.When hemorrhage is large, splenic laceration andrupture can occur and may be catastrophic. Splenic
Fig. 6. Pancreatic abscess following necrotizing pan-creatitis. A well-defined fluid collection with a thickenhancing rim, containing debris and air, is seen inthe pancreatic tail (arrows). This abscess was drainedsuccessfully by percutaneous catheter placement. Sur-gery is an alternative treatment depending on thestatus of the patient and condition of the remainderof the pancreas.
Fig. 7. Pancreatic necrosis in a 38-year-old man. Notea fluid attenuation collection in the pancreatic bed(white arrows) with islands of preserved fatty tissuesuggestive of fat necrosis (arrowheads). Glandular en-hancement is only seen in the head (black arrow).
Fig. 8. Pancreatic necrosis in a 38-year-old man. Afterinitial conservative management, the patient inFig. 7. developed fever, and a subsequent CECT exam-ination demonstrated gas within the collection rais-ing concern for infection/abscess (arrows).
Table 2: Balthazar grading system
Grade Description
A Normal-appearing pancreasB Focal or diffuse enlargement of the
pancreasC Pancreatic gland abnormalities
accompanied by mild peripancreaticinflammatory changes
D Fluid collection in a single locationE Two or more fluid collections near
the pancreas or gas in or adjacentto the pancreas
Cross-Sectional Imaging in Acute Pancreatitis 453
martedì 16 ottobre 12

Criteri di Ranson e Apache II
Imaging, most commonly with contrast-enhancedcomputed tomography (CE-CT), plays a significant role inthe identification of local and systemic complications and inplanning further management. Image-guided interven-tional procedures tend to be less invasive than surgery,often reducing the need for surgical intervention, andthereby improving outcome.
Natural course of acute pancreatitis
The clinical definition of acute pancreatitis, whether inthe presence or absence of underlying chronic pancreatitis,requires two of the following three features8:
1) Abdominal pain strongly suggestive of acutepancreatitis.
2) Serum amylase and/or lipase activity !3 times theupper limit of normal.
3) Characteristic imaging findings of acute pancreatitis.
Mild acute pancreatitis is characterised by minimal or noorgan dysfunction without parenchymal necrosis and bya prompt, uncomplicated recovery. The presence of organfailure (at least one of: respiratory, cardiovascular, or renal)for more than 48 h is defined as severe acute pancreatitis(SAP) which has two phases with a bimodal distribution formortality.
Severe acute pancreatitis-early phase (during the1st week)
The early phase of SAP occurs within the first weekand is associated with increasing pancreatic and peri-pancreatic inflammation with ischaemia. These changescan either resolve or progress to irreversible necrosisand liquefaction, which may be associated with thedevelopment of fluid collections in and around thepancreas.
Clinical course and outcome are determined by thedevelopment of organ failure.9 Patients with organ failurethat resolves within 48 h of onset have been shown to havezero mortality rate.10 However, development of thesystemic inflammatory response syndrome (SIRS), anexaggerated inflammatory response, and subsequent multi-organ failure are responsible for approximately 50% of allSAP-associated deaths.11e13
Severe acute pancreatitis-late phase
The late phase starts in the second and subsequentweeks and can either resolve (oedematous pancreaswithout necrosis), stabilise (but not normalise) or prog-ress. Pancreatic necrosis itself is not usually the cause ofdeath in these patients, however, the necrotic tissueserves as a focus for infection in 40e70% of cases14 andmortality is related to infection.8 Disease progression ismarked by increasing necrosis, infection, persisting SIRSand multi-organ failure causing a significant increase inmortality.15
Clinical severity scoring
There are several clinical and biochemical scoringsystems that can be employed to assess the severity of acutepancreatitis. Organ failure can be quantified using theMarshall,16 SOFA (based on 6 organ systems),17 APACHE II18
or Ranson (only applies 48 h after onset)19 scoring systems(Table 1).
Radiological scoring systems
In 1985, Balthazar et al introduced a scoring systembased on radiological findings by grading the severity ofpancreatitis into 5 different groups on unenhanced CT20
(Table 2; Fig. 1). The main drawback of this scoring systemwas the inability to reliably depict pancreatic necrosis. Thesystem was updated to incorporate CE-CT findings of thedegree of necrosis in the CT severity index (CTSI) in anattempt to improve the early prognostic value of radiolog-ical staging21 (Table 2). An overall CTSI score can be corre-lated with morbidity and mortality (Table 3).21
Since Balthazar’s original system,20 numerous othermorphological scoring systems have been proposed, eachwith their own flaws.22 In 2004, Mortel!e et al modified theCTSI, combining pancreatic inflammation, necrosis andextra-pancreatic complications in a 10-point scale (Table 4)which showed a stronger correlation between outcome andseverity than the original.23
Contrast-enhanced computed tomography (CE-CT)
CE-CT is considered to be the gold standard imagingmodality in the evaluation of patients with acute pancrea-titis.9 MRI and ultrasound (US) are used in specific clinicalsituations and can be useful in determining aetiology.24,25
CE-CT should be performed 48e72 h after the onset of anacute attack. With this delay, the scan yields a higheraccuracy in the depiction of necrotising pancreatitis.26
Table 1Ranson and APACHE II criteria.
Ranson Criteria APACHE II
Age >55 years Age >55 yearsWBC >16,000/mL WBC <3,000 or >14,900/mLGlucose >200 mg/dL Rectal temperature <36 C or> 38.4 CLDH >350 IU/mL MAP <70 or >109 mmHgAST >250 IU/L HR <70 or >109 bpmHct decrease >10 RR <12 or >24BUN increase >5 mg/dL pH <7.33 or >7.49Calcium <8 mg/dL Na" <130 or >149 mMolPO2< 60 mm Hg K" <3.5 or <5.4 mMolBase deficit >4 mEq/L PO2< 70 or >200 mmHgFluid sequestration >6 L Creatinine <0.6 or >1.4 mg/100 mL
Hct <30% or >45.9%GCSChronic health points
Abbreviations: WBC: white blood cell count; LDH: lactate dehydrogenase;AST: aspartate transaminase; Hct: haematocrit; BUN: blood urea nitrogen;PO2: arterial partial pressure of oxygen; MAP: mean arterial pressure; HR:heart rate; bpm: beats per minute; Na": sodium; K": potassium; GCS:Glasgow Coma Score; RR: respiratory rate.
N. Bharwani et al. / Clinical Radiology 66 (2011) 164e175 165
martedì 16 ottobre 12
5/2/2011
10
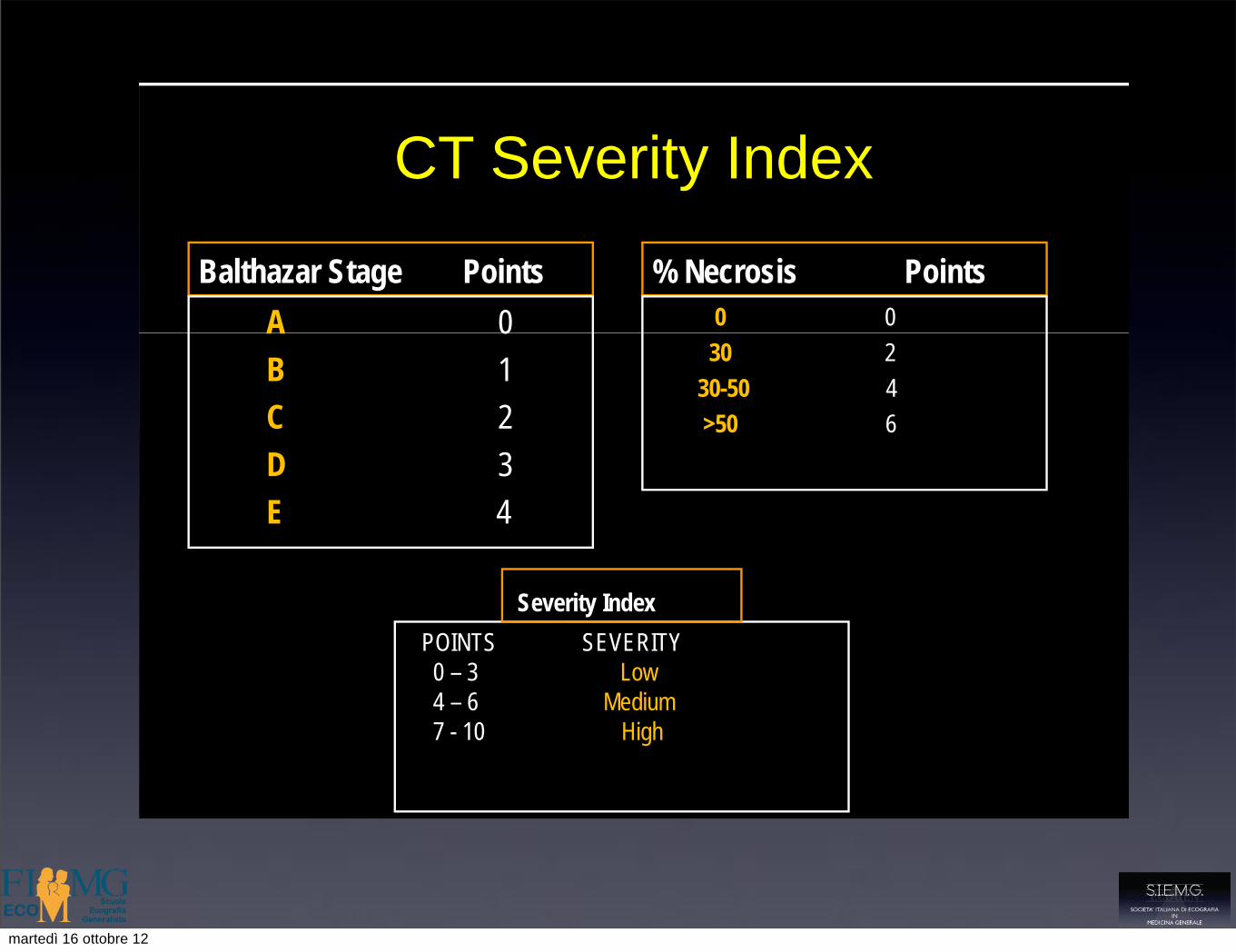
CT Severity Index
Balthazar Stage PointsA 0
% Necrosis Points0 0A 0
B 1C 2D 3E 4
30 230-50 4>50 6
POINTS SEVERITY0 – 3 Low4 – 6 Medium7 - 10 High
Severity Index
Severity Index:Morbidity and Mortality
GRADE MORBIDITY MORTALITY(Points)
Low 0- 3 8 % 3 %
Medium 4-6 35 % 6 %
High 7-10 92 % 17 %g
Balthazar E et al, Radiology 1990; 174: 331-336.
martedì 16 ottobre 12
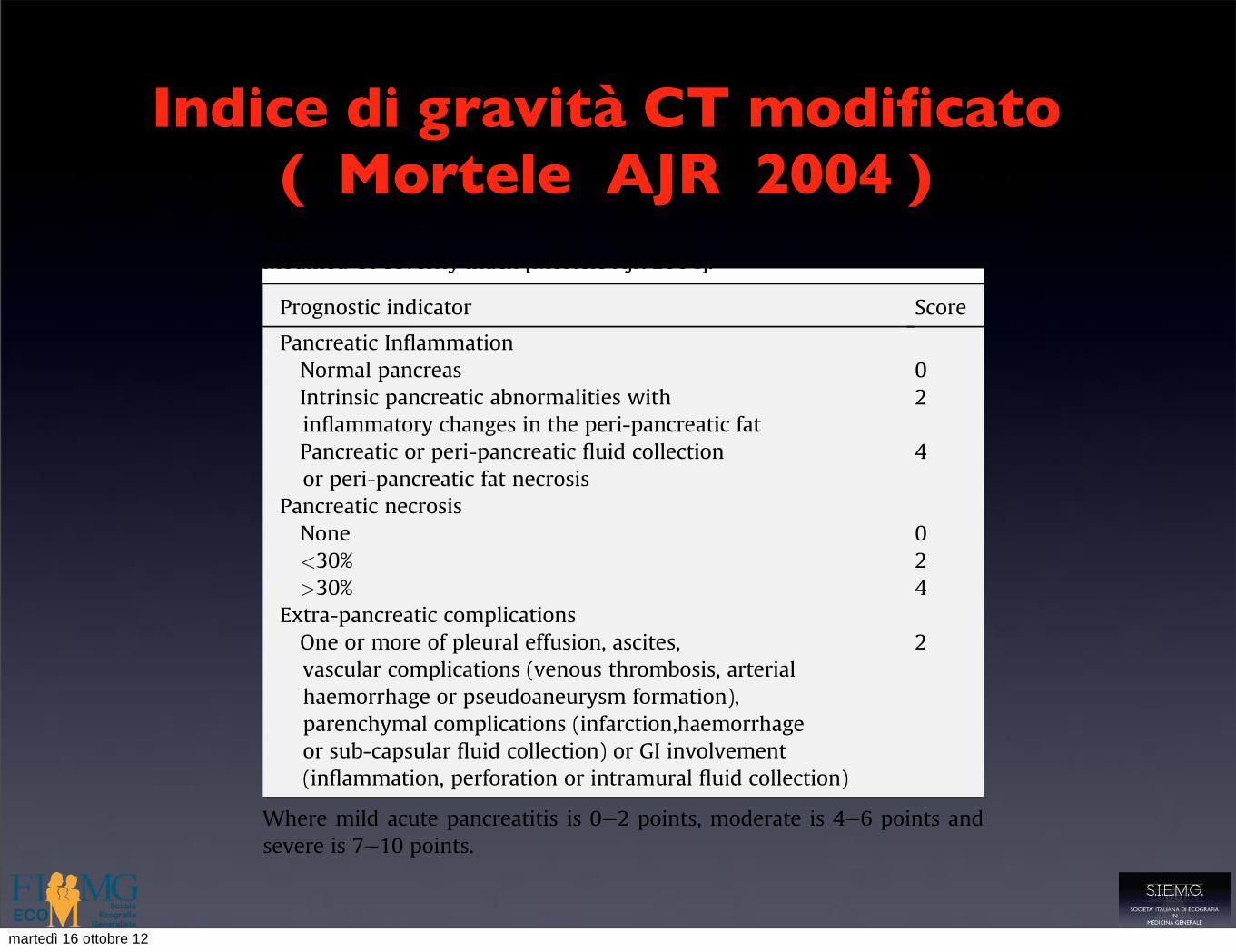
Indice di gravità CT modificato ( Mortele AJR 2004 )
Morphological stages of acute pancreatitis
Interstitial oedematous pancreatitis (IOP)
IOP is characterised by enlargement of the pancreas(which can be localised or diffuse) and homogeneousenhancement of pancreatic parenchyma following IVcontrast administration (Fig. 2). Peak enhancementof normalpancreatic parenchyma is to 80e150 Hounsfield Units(HU).21,27 Adjacent peri-pancreatic and retroperitonealtissues can appear entirely normal or may demonstratehaziness and stranding with varying amounts of associatedperi-pancreatic fluid.
Necrotising pancreatitis
Pancreatic necrosis is seen as diffuse or focal areas of non-viable pancreatic tissue, indicated by the lack of parenchymalenhancement following IV contrast administration(enhancement less than 30 HU correlates well withnecrosis28,29) (Figs. 3 and 4). TheAtlanta Classificationdefinesnecrotising pancreatitis as being associated with more than30% parenchymal necrosis.7 Necrosis develops early in thecourse of SAP (withinhours of onset) and is due to thrombosisof the pancreatic microcirculation. It is usually well estab-lished by 96 h after onset of clinical symptoms, but generallynot before 48 h.26 The relative amounts of solid and liquidcomponents in a region of necrosis are dependent on the time
that has elapsed since the onset of pancreatic necrosis. Theprocess starts initially as solid necrosis and progresses toliquefaction. Complete resolution of necrosis can occur witheventual reabsorption of this fluid component. Patients withsterile necrosis do not generally require intervention unlessthey remain persistently unwell (usually secondary to masseffect) for more than 4 weeks after onset.
Pancreatic Necrosis is sub-divided into three types22,30
1. Organised pancreatic necrosis (OPN)An evolving collection characterised by encapsulation andinhomogeneous contents of liquefied, necrotic fatty tissueand solid necrotic pancreatic and extra-pancreatic debris.31
Table 3Correlation of CT Severity Index with patient morbidity and mortality[Balthazar Radiology 1990].
CT severity index* Morbidity (%) Mortality (%)
0e3 8 34e6 35 67e10 92 17
* CT Severity Index! CT Grade score" CT Necrosis score (see Table 2).
Table 4Modified CT severity index [Mortele AJR 2004].
Prognostic indicator Score
Pancreatic InflammationNormal pancreas 0Intrinsic pancreatic abnormalities withinflammatory changes in the peri-pancreatic fat
2
Pancreatic or peri-pancreatic fluid collectionor peri-pancreatic fat necrosis
4
Pancreatic necrosisNone 0<30% 2>30% 4
Extra-pancreatic complicationsOne or more of pleural effusion, ascites,vascular complications (venous thrombosis, arterialhaemorrhage or pseudoaneurysm formation),parenchymal complications (infarction,haemorrhageor sub-capsular fluid collection) or GI involvement(inflammation, perforation or intramural fluid collection)
2
Where mild acute pancreatitis is 0e2 points, moderate is 4e6 points andsevere is 7e10 points.
Figure 2 Interstitial Oedematous Pancreatitis (IOP). Axial contrast-enhanced CT performed 72 h after admission. Image demonstratesdiffuse enlargement of the pancreas with homogeneous enhance-ment following IV contrast administration. Associated peri-pancreaticfat stranding results in CT grade C by the Balthazar scoring system.
Figure 3 Pancreatic Necrosis. Axial contrast-enhanced CT sectiondemonstrating an area of non-enhancing parenchyma in thepancreatic head (white arrow) 10 days after admission with acuteabdominal pain. A region of interest drawn over this area shows anattenuation of 17HU compared to normally enhancing pancreaticparenchyma in the taile attenuation 60HU. Necrotising pancreatitis isdefined as #30% parenchymal necrosis.
N. Bharwani et al. / Clinical Radiology 66 (2011) 164e175 167
martedì 16 ottobre 12
Diagnosi
• Dolore addominale
• Esami laboratoristici ( elevazione amilasi e lipasi > 3 volte il limite sup della norma)
• Ecografia
• Tomografia computerizzata
martedì 16 ottobre 12
Ecografia
• Alterazioni a carico del pancreas
• Patologia litiasica biliare
• Valutazione parenchima epatico ( etilista)
• Diagnosi e monitoraggio complicanze
martedì 16 ottobre 12

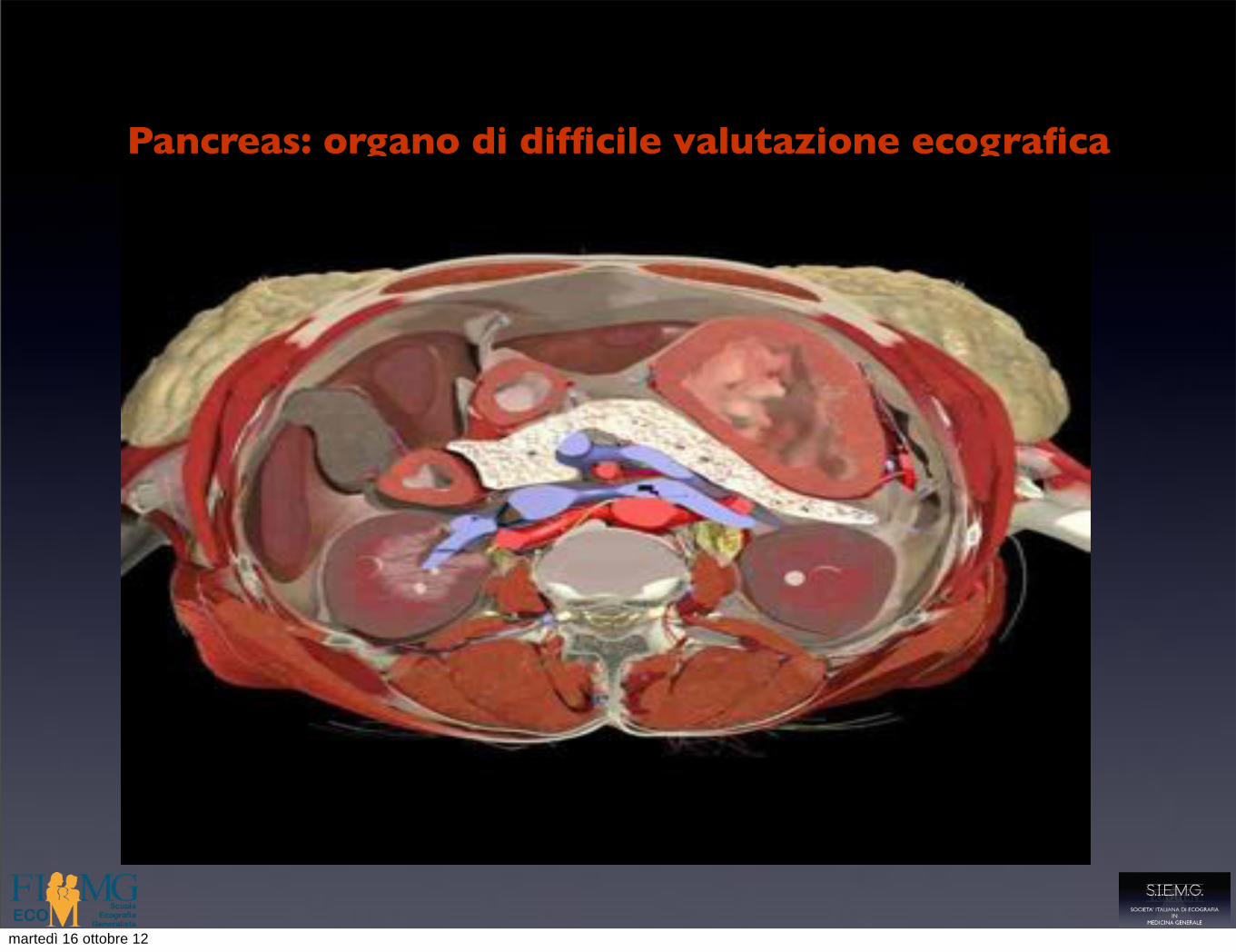
Pancreas: organo di difficile valutazione ecografica
• Visibilità globale difficile nel 15-20 % dei casi
• La difficoltà di visualizzazione aumenta nella sequenza testa-corpo-coda
• La regione periampollare è di solito la più facile da visualizzare
• Esame operatore dipendente
martedì 16 ottobre 12
Pancreas: organo di difficile valutazione ecografica
• Visibilità globale difficile nel 15-20 % dei casi
• La difficoltà di visualizzazione aumenta nella sequenza testa-corpo-coda
• La regione periampollare è di solito la più facile da visualizzare
• Esame operatore dipendente
martedì 16 ottobre 12

Limiti dell’esame ecografico
• Difficoltosa visualizzazione del pancreas( meteorismo ,obesità )
• Nel 40 % delle forme lievi l’esame ecografico è normale
• Difficoltosa differenziazione delle aree edematose da quelle necrotiche
martedì 16 ottobre 12
Pancreatite lieve
martedì 16 ottobre 12

Alterazioni ecografiche
• Variazioni di volume ( aumento diffuso o focale, a volte riduzione )
martedì 16 ottobre 12

Alterazioni ecografiche
• Variazioni di volume ( aumento diffuso o focale, a volte riduzione )
martedì 16 ottobre 12
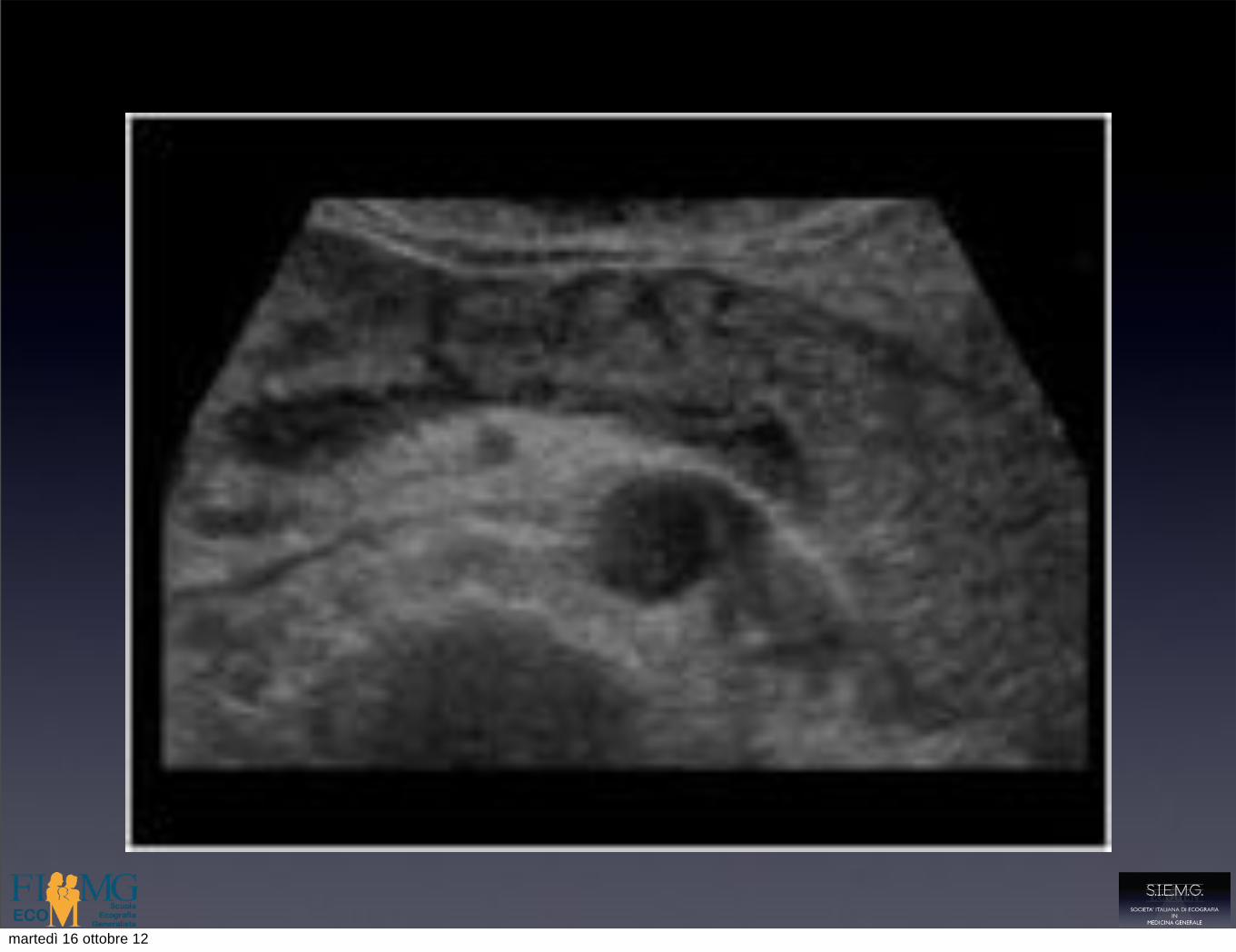
Alterazioni ecografiche
• Alterazioni della ecogenicità
• ipoecogenicità diffusa
• ipoecogenicità segmentaria
• disomogeneità
martedì 16 ottobre 12
Alterazioni ecografiche
• Alterazioni della ecogenicità
• ipoecogenicità diffusa
• ipoecogenicità segmentaria
• disomogeneità
martedì 16 ottobre 12
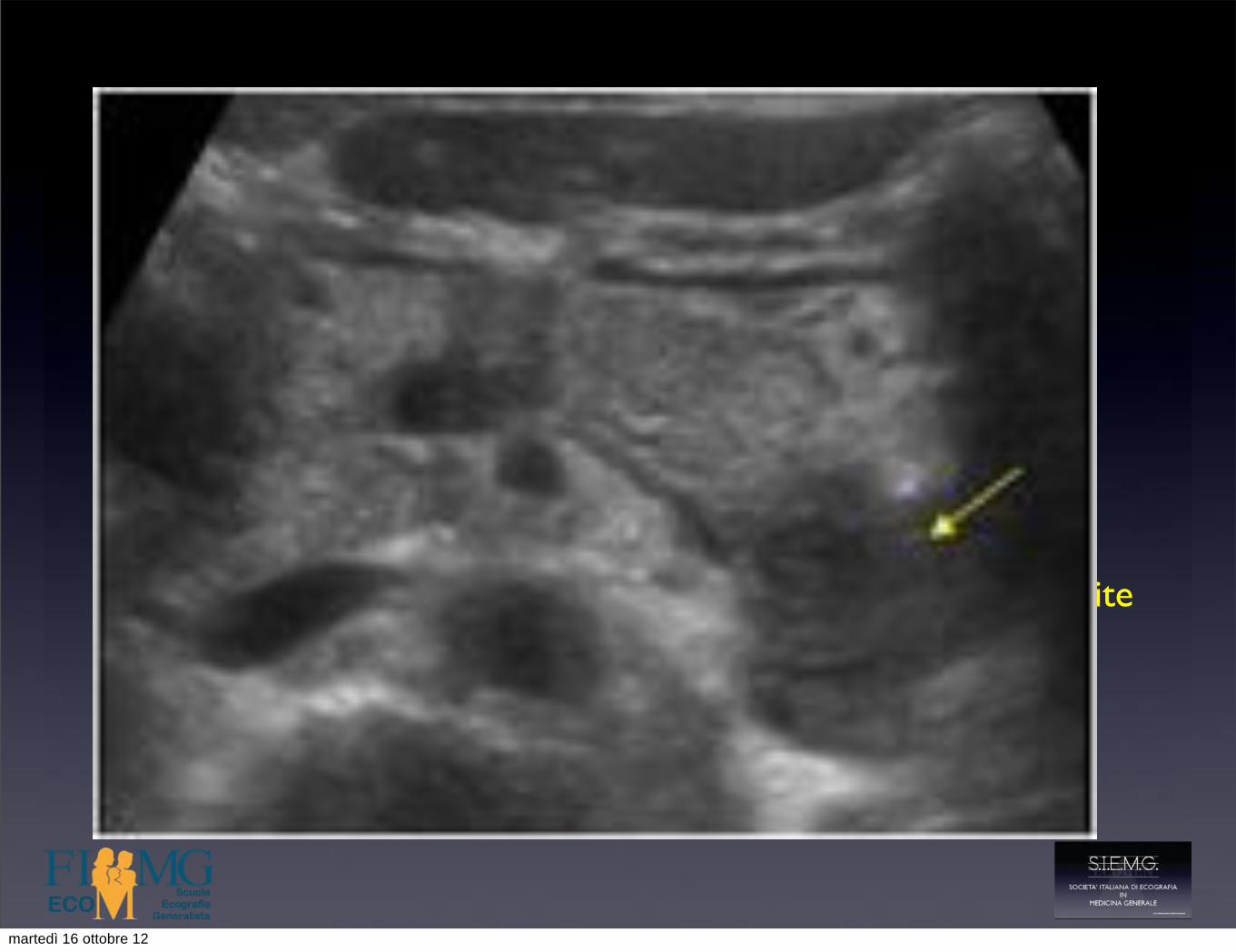
!Pancreatite focale !
"• Area ipoecogena disomogenea""• Può deformare il profilo ghiandolare""• Può comprimere le strutture circostanti ( Vie biliari ) ""• Carcinoma di solito ipovascolarizzato e ipoperfuso, pancreatite
focale più vascolarizzata per l’infiltrato flogistico""• Spesso necessario esame bioptico "
martedì 16 ottobre 12
!Pancreatite focale !
"• Area ipoecogena disomogenea""• Può deformare il profilo ghiandolare""• Può comprimere le strutture circostanti ( Vie biliari ) ""• Carcinoma di solito ipovascolarizzato e ipoperfuso, pancreatite
focale più vascolarizzata per l’infiltrato flogistico""• Spesso necessario esame bioptico "
martedì 16 ottobre 12

Adenocarcinoma duttale!
martedì 16 ottobre 12
Pancreatite severa
martedì 16 ottobre 12
Alterazioni ecografiche
• Aree di necrosi: zone ipoecogene che si alternano ad aree di ecostruttura normale
• Aree ecoprive a contenuto fluido per colliquazione necrotica
• Contorni ghiandolari irregolari e maldelineati
martedì 16 ottobre 12

Alterazioni ecografiche
• Aree di necrosi: zone ipoecogene che si alternano ad aree di ecostruttura normale
• Aree ecoprive a contenuto fluido per colliquazione necrotica
• Contorni ghiandolari irregolari e maldelineati
martedì 16 ottobre 12
Complicanze della pancreatite acuta
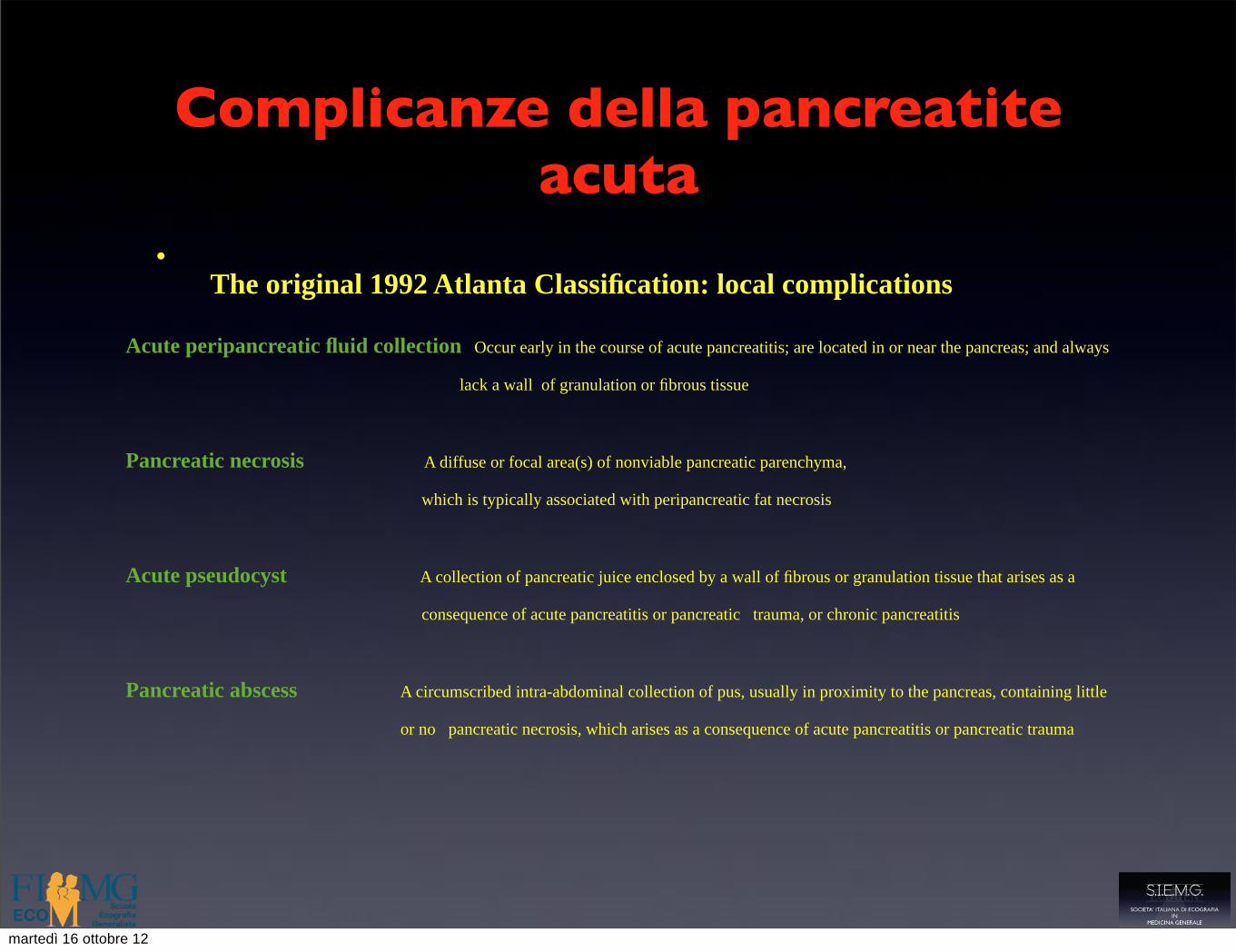
•The original 1992 Atlanta Classification: local complications
Acute peripancreatic fluid collection Occur early in the course of acute pancreatitis; are located in or near the pancreas; and always
lack a wall of granulation or fibrous tissue
Pancreatic necrosis A diffuse or focal area(s) of nonviable pancreatic parenchyma,
which is typically associated with peripancreatic fat necrosis
Acute pseudocyst A collection of pancreatic juice enclosed by a wall of fibrous or granulation tissue that arises as a
consequence of acute pancreatitis or pancreatic trauma, or chronic pancreatitis
Pancreatic abscess A circumscribed intra-abdominal collection of pus, usually in proximity to the pancreas, containing little
or no pancreatic necrosis, which arises as a consequence of acute pancreatitis or pancreatic trauma
martedì 16 ottobre 12
termed acute necrotic collections. Acute necroticcollections represent a combination of paren-chymal and/or peripancreatic fat necrosis togetherwith pancreatic secretions. It is believed that thenecrotic component of acute necrotic collectionsoccurs following the liberation of activated pancre-atic enzymes in the pancreatic and peripancreaticarea, leading to (peri)pancreatic fat saponificationand necrosis. Thus, the contents of acute necroticcollections are a spectrum ranging from predomi-nantly necrotic (nonliquid) to both fluid andnecrotic material (with varying degrees of eachcomponent), and generally also contain areas ofloculations or septa.
OnCECT, acute necrotic collections are depictedas homogeneous (fluid density) or heterogeneous(combination of fluid and nonliquid densities) in thepancreatic and/or peripancreatic area (Fig. 16). Anacute necrotic collection has no capsule or is onlypartially encapsulated. It remains uncertain as towhat proportion of peripancreatic fluid collectionscontains necrotic debris because CECT, the most
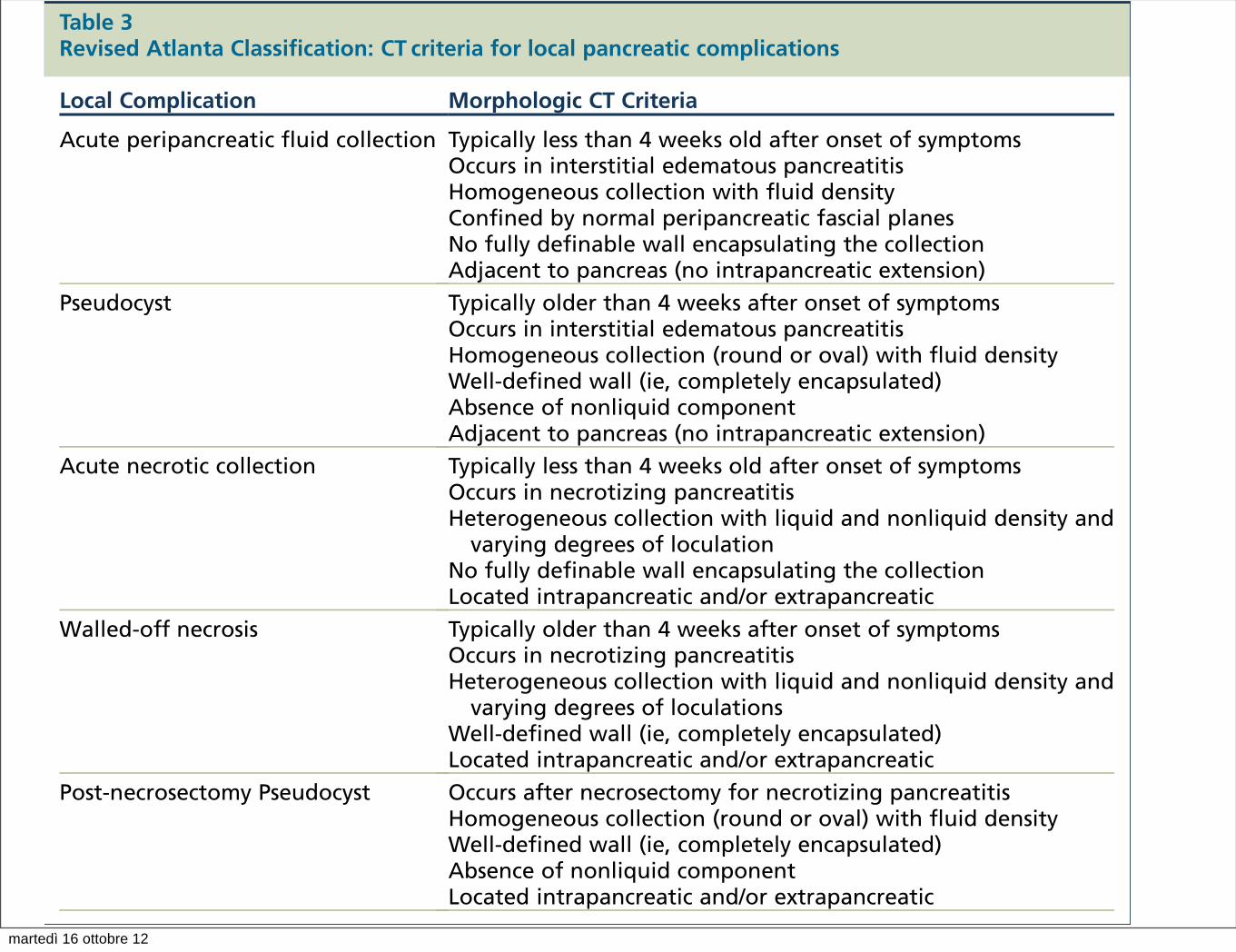
Table 3Revised Atlanta Classification: CT criteria for local pancreatic complications
Local Complication Morphologic CT Criteria
Acute peripancreatic fluid collection Typically less than 4 weeks old after onset of symptomsOccurs in interstitial edematous pancreatitisHomogeneous collection with fluid densityConfined by normal peripancreatic fascial planesNo fully definable wall encapsulating the collectionAdjacent to pancreas (no intrapancreatic extension)
Pseudocyst Typically older than 4 weeks after onset of symptomsOccurs in interstitial edematous pancreatitisHomogeneous collection (round or oval) with fluid densityWell-defined wall (ie, completely encapsulated)Absence of nonliquid componentAdjacent to pancreas (no intrapancreatic extension)
Acute necrotic collection Typically less than 4 weeks old after onset of symptomsOccurs in necrotizing pancreatitisHeterogeneous collection with liquid and nonliquid density and
varying degrees of loculationNo fully definable wall encapsulating the collectionLocated intrapancreatic and/or extrapancreatic
Walled-off necrosis Typically older than 4 weeks after onset of symptomsOccurs in necrotizing pancreatitisHeterogeneous collection with liquid and nonliquid density and
varying degrees of loculationsWell-defined wall (ie, completely encapsulated)Located intrapancreatic and/or extrapancreatic
Post-necrosectomy Pseudocyst Occurs after necrosectomy for necrotizing pancreatitisHomogeneous collection (round or oval) with fluid densityWell-defined wall (ie, completely encapsulated)Absence of nonliquid componentLocated intrapancreatic and/or extrapancreatic
Fig. 15. Acute peripancreatic fluidcollection(<4 weeks).CT shows normal enhancement of the pancreas witha fluid collection extending into the left anterior parare-nal compartment (arrows). The fluid collection lacksa well-defined wall and conforms to the anatomic spacein which it arises. The acute peripancreatic fluid collec-tion resolved spontaneously.
Imaging of Acute Pancreatitis 439
martedì 16 ottobre 12
Raccolta acuta fluida pancreatica/peripancreatica a insorgenza precoce
• Area transonica ,con contorni non delineati ,che si adatta alla cavità che la contiene
• Non presenta componenti solide al suo interno ed è costituita da succo pancreatico ricco di enzimi
martedì 16 ottobre 12

Raccolta fluida pancreatica /peripancreatica post necrotica
• Si sviluppa come sequela della necrosi pancreatica
• Contenuto disomogeneo ,con detriti di tessuto adiposo e di parenchima pancreatico in sospensione
• Spesso conseguente a necrosi coinvolgente il Wirsung e perciò in comunicazione con esso
martedì 16 ottobre 12

Localizzazione
• Intrapancreatica
• Retrocavità degli epiploon
• Spazio pararenale anteriore
• Mediastinica ( attraverso il forame diaframmatico)
• Nei foglietti mesocolici e mesenterici
• Docce parieto coliche
martedì 16 ottobre 12
Retrocavità degli epiploon
martedì 16 ottobre 12
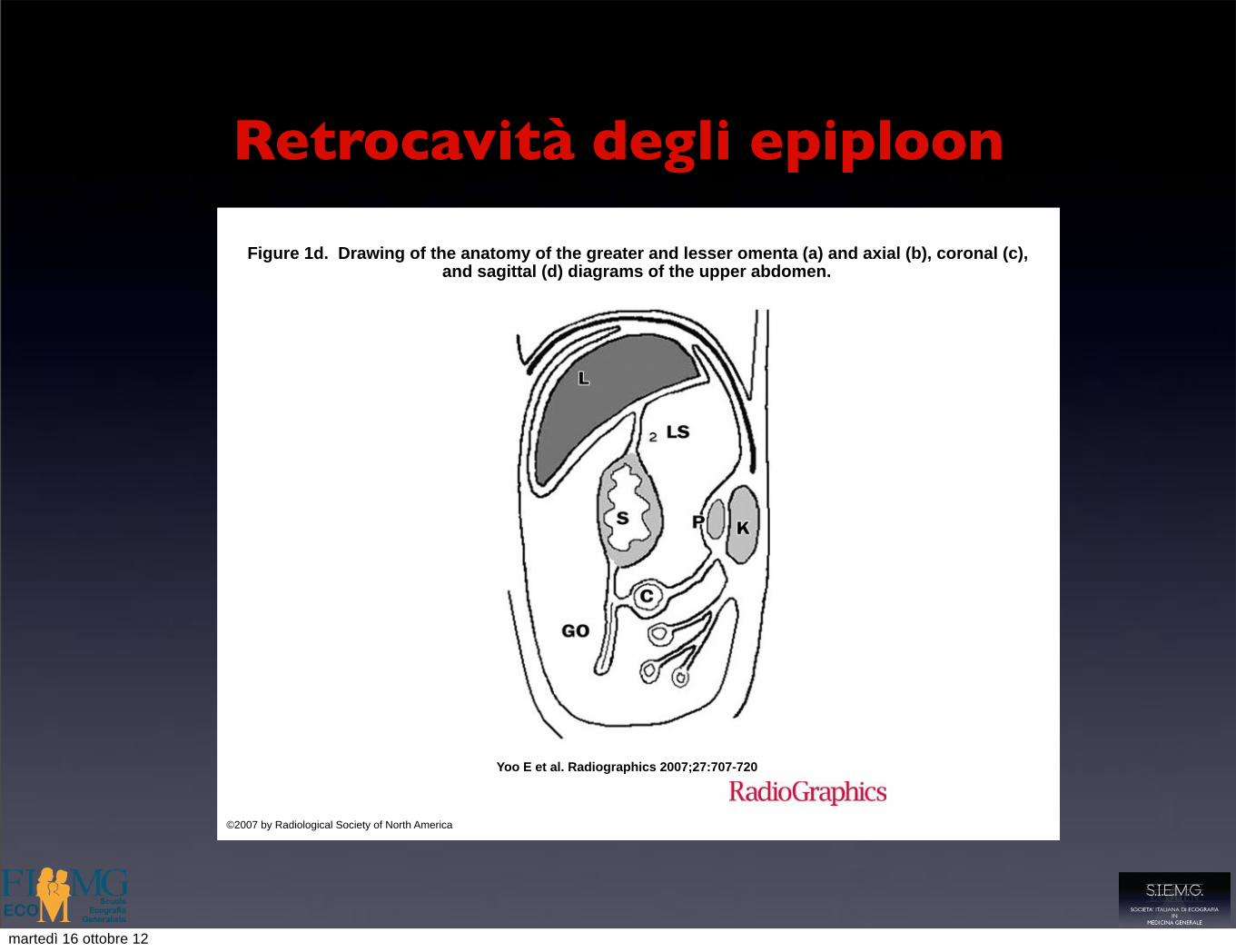
Retrocavità degli epiploon
Figure 1d. Drawing of the anatomy of the greater and lesser omenta (a) and axial (b), coronal (c), and sagittal (d) diagrams of the upper abdomen.
Yoo E et al. Radiographics 2007;27:707-720
©2007 by Radiological Society of North America
martedì 16 ottobre 12
Retrocavità degli epiploon
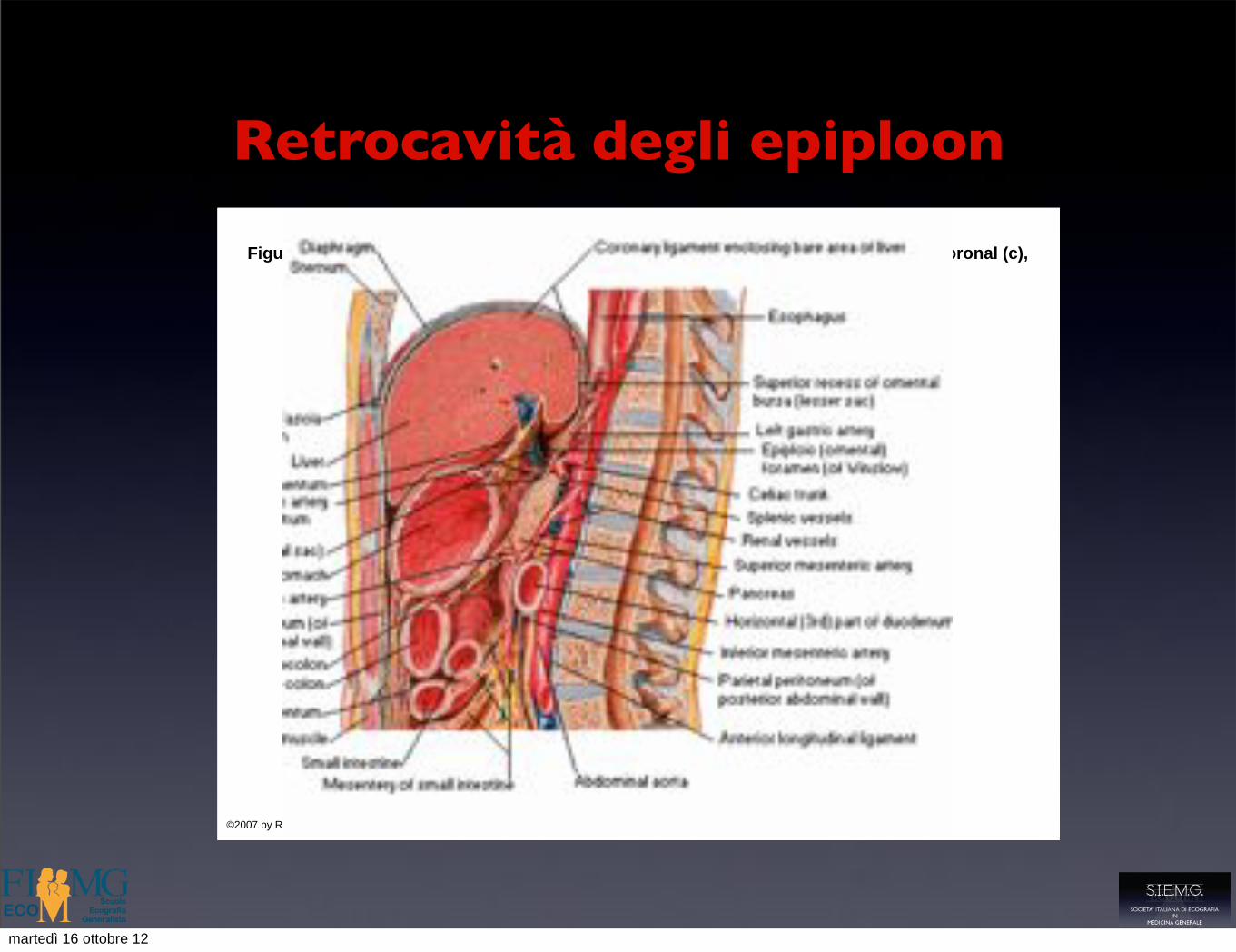
Figure 1d. Drawing of the anatomy of the greater and lesser omenta (a) and axial (b), coronal (c), and sagittal (d) diagrams of the upper abdomen.
Yoo E et al. Radiographics 2007;27:707-720
©2007 by Radiological Society of North America
martedì 16 ottobre 12
Retrocavità degli epiploon
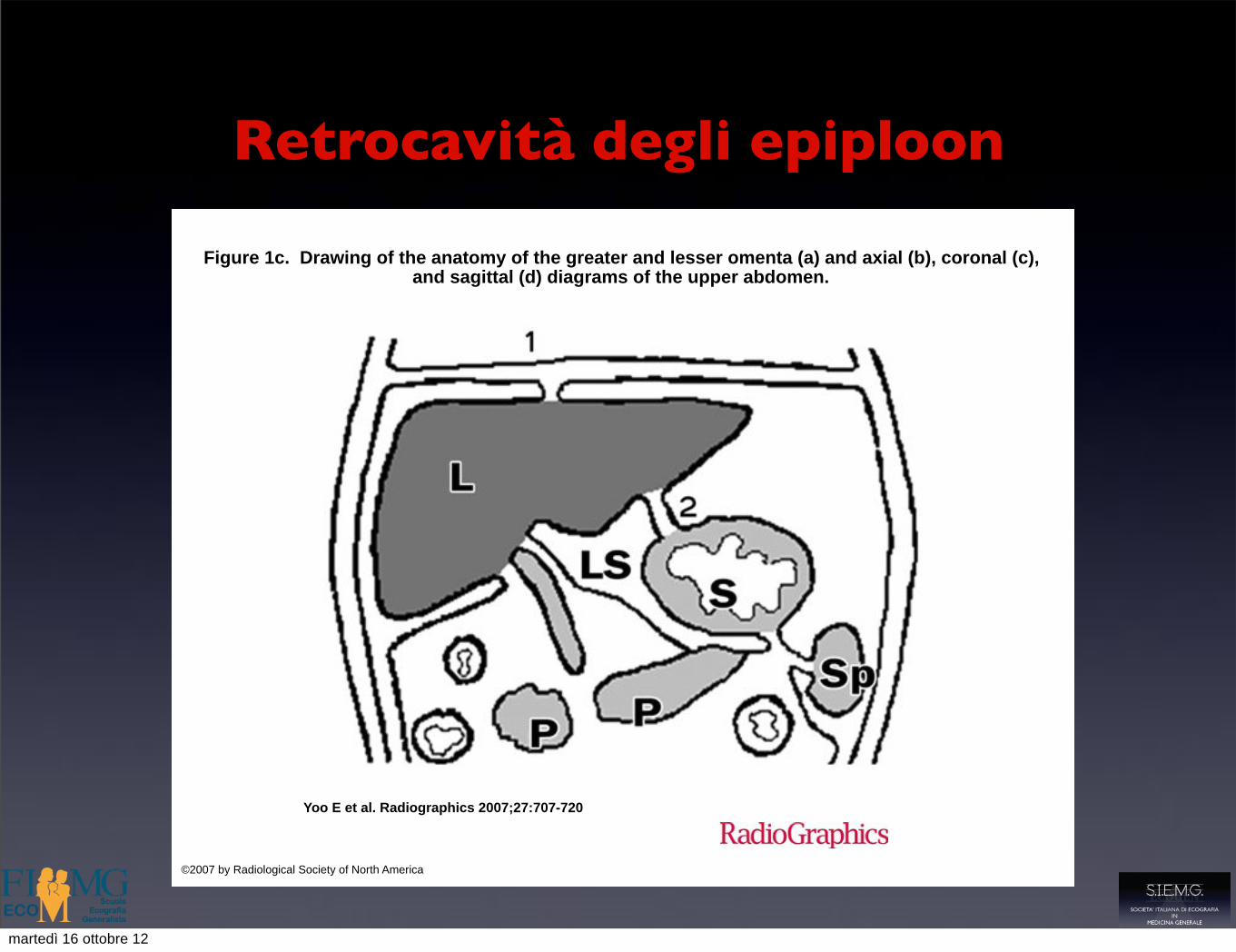
Figure 1c. Drawing of the anatomy of the greater and lesser omenta (a) and axial (b), coronal (c), and sagittal (d) diagrams of the upper abdomen.
Yoo E et al. Radiographics 2007;27:707-720
©2007 by Radiological Society of North America
martedì 16 ottobre 12

Retrocavità degli epiploon
Figure 1c. Drawing of the anatomy of the greater and lesser omenta (a) and axial (b), coronal (c), and sagittal (d) diagrams of the upper abdomen.
Yoo E et al. Radiographics 2007;27:707-720
©2007 by Radiological Society of North America
martedì 16 ottobre 12
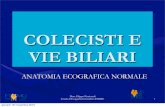
Rapporti del pancreas con TM e SBM
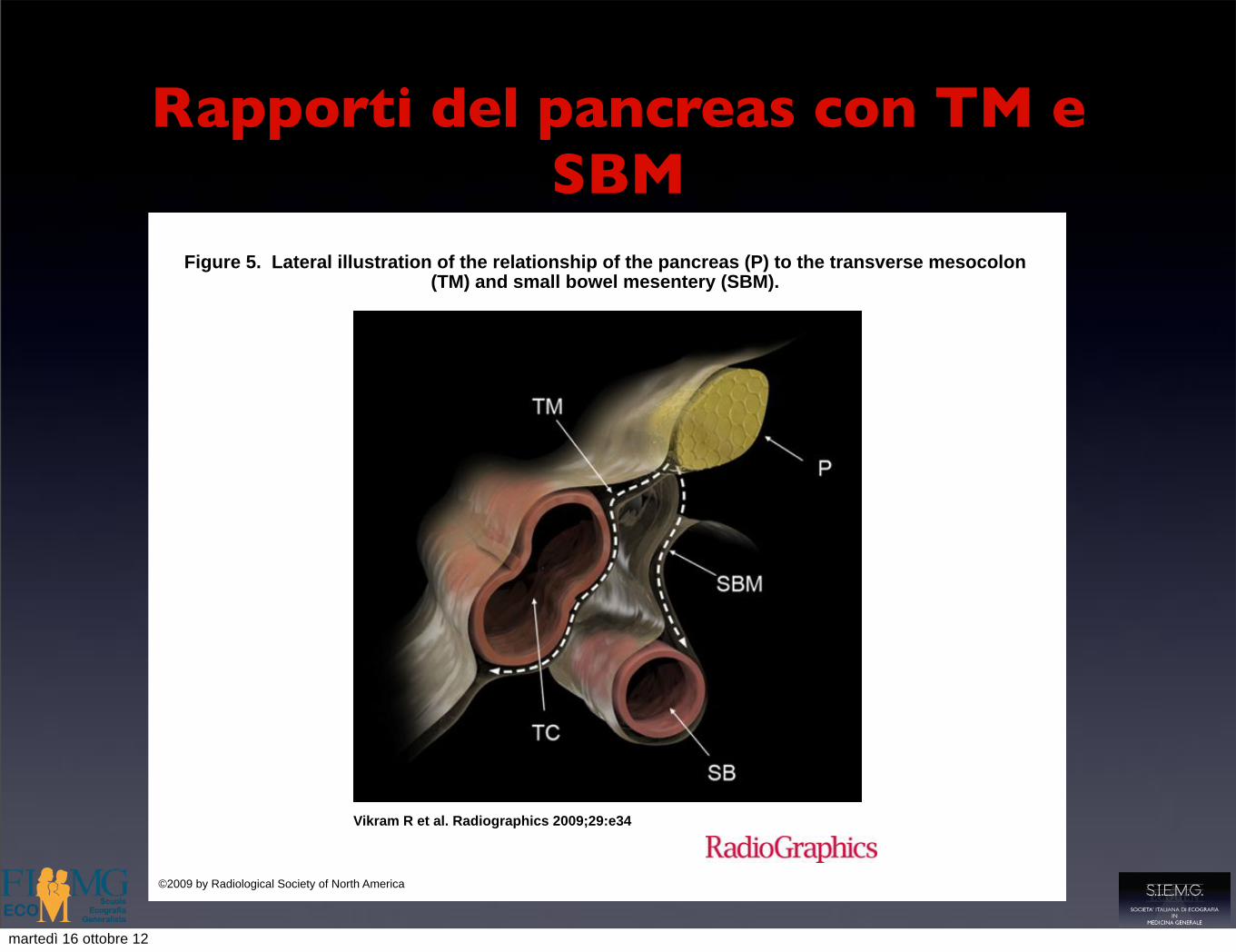
Figure 5. Lateral illustration of the relationship of the pancreas (P) to the transverse mesocolon (TM) and small bowel mesentery (SBM).
Vikram R et al. Radiographics 2009;29:e34
©2009 by Radiological Society of North America
martedì 16 ottobre 12

Raccolta fluida peripancreatica
martedì 16 ottobre 12

Raccolta nella retrocavità epiploon
martedì 16 ottobre 12

Pseudocisti pancreatica
• Formazione a contenuto fluido ,anecogena che persiste > di 4 settimane
• Presenza di parete propria infiammatoria
• Contorni definiti e arrotondati
• Residui necrotici, sepimentazioni, calcificazioni
• Effetto massa correlato alle dimensioni
martedì 16 ottobre 12

Pseudocisti pancreatica
• regressione spontanea (50 % dei casi)
• complicazione (30 % dei casi )
• stabilità ( 20 % dei casi )
martedì 16 ottobre 12

Pseudocisti pancreatica: complicanze
• Estensione agli organi adiacenti
• Emorragia
• Peritonite
• Ostruzione del duodeno
• Ostruzione biliare
• Infezione
martedì 16 ottobre 12
Emorragia
• Area ecogena disomogenea più e meno estesa ,generalmente in sede peripancreatica ,che tende a colliquarsi diventando ecopriva
• Necessaria la conferma con TC che rileva la densità tipica del sangue
martedì 16 ottobre 12

Ascesso o necrosi infetta
• Evoluzione di una raccolta fluida
• Comparsa di echi interni fluttuanti o declivi
• Spots iperecogeni espressione della presenza di aria
• Quadro clinico ( febbre,dolore,leucocitosi)
martedì 16 ottobre 12
Complicanze vascolari
• Trombosi venosa
• Pseudoaneurisma
martedì 16 ottobre 12

Trombosi venosa
• Danno infiammatorio intimale o compressione estrinseca
• Vena splenica (è la più frequente 10-40% dei casi )
• Vena mesenterica superiore
• Vena porta
martedì 16 ottobre 12

Pseudoaneurismi
• erosione delle pareti di un vaso
• formazione anecogena pulsante
• Conferma diagnostica con ecocolor Doppler
martedì 16 ottobre 12

Pancreatite acuta : 6 settimane dopo l’esordio
martedì 16 ottobre 12
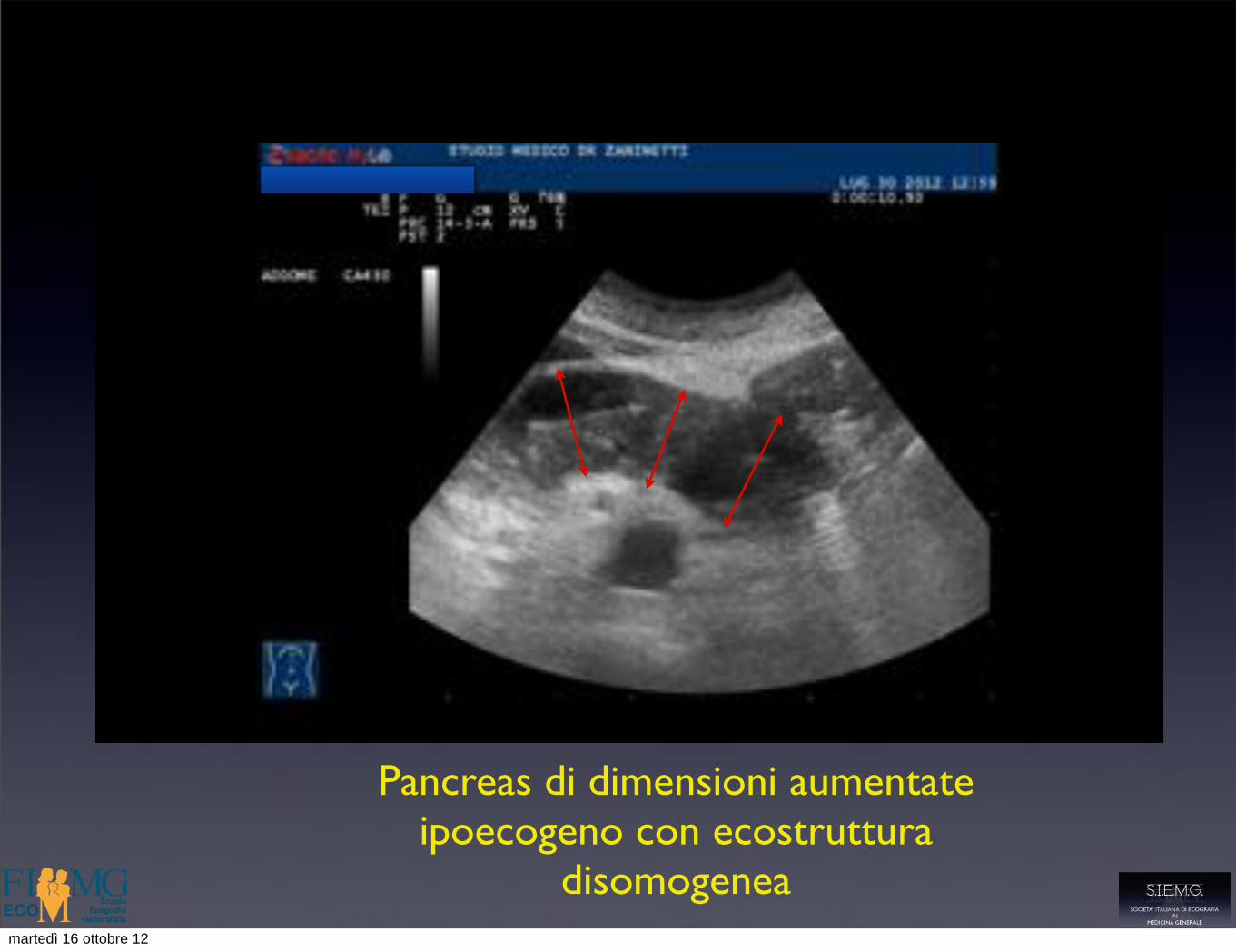
Pancreas di dimensioni aumentate ipoecogeno con ecostruttura
disomogeneamartedì 16 ottobre 12

Margini irregolari
martedì 16 ottobre 12

area ipo-anecogena nella parte anteriore della testa
martedì 16 ottobre 12
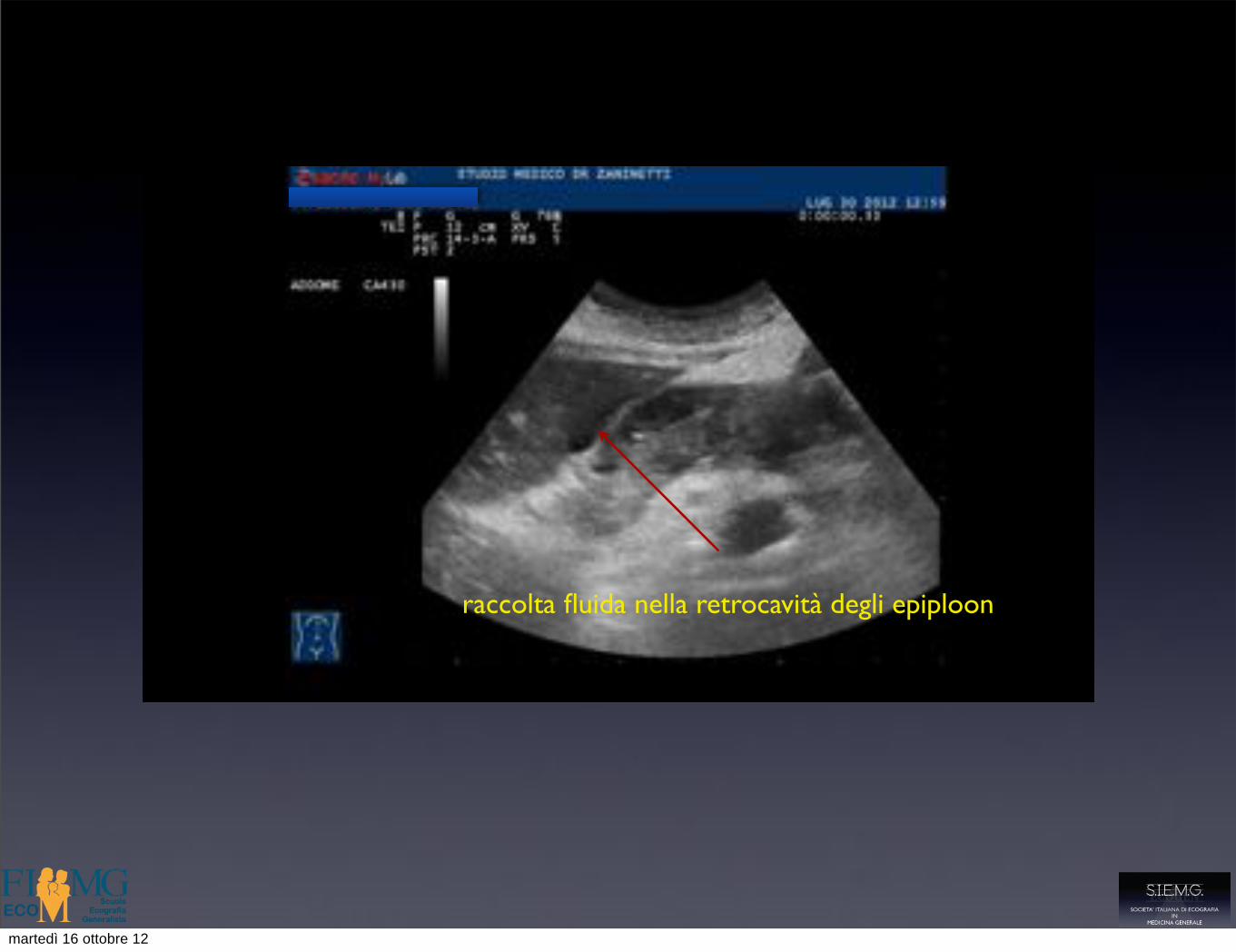
raccolta fluida nella retrocavità degli epiploon
martedì 16 ottobre 12

area rotondeggiante anecogena con spots ecogeni , priva di parete propria
martedì 16 ottobre 12

area disomogenea ipo anecogena della coda
martedì 16 ottobre 12

raccolta fluida posteriore al pancreas
vena splenica compressa
martedì 16 ottobre 12
Pancreatite cronica
• Alcool
• Iperlipidemia
• Ipertiroidismo
• Fibrosi cistica
• Cause ereditarie e idiopatiche
martedì 16 ottobre 12

Imaging ecografico
• Alterazioni delle dimensioni ghiandolari
• Alterazioni della ecogenicità
• Alterazioni della ecostruttura
• Calcificazioni parenchimali
• Alterazioni di calibro del dotto di Wirsung
• Calcolosi intraduttale
• Variazioni del calibro della SMV
martedì 16 ottobre 12
Alterazioni delle dimensioni ghiandolari
• Presenti nel 50% dei casi, soprattutto negli stadi avanzati di malattia
• Atrofia diffusa
• Alterazioni focali
martedì 16 ottobre 12
Alterazioni della ecogenicità
• Solitamente aumentata per fibrosi e infiltrazione adiposa
• Reperto non specifico( presente in anziani e obesi )
martedì 16 ottobre 12
Alterazioni della ecostruttura
• Nel 40% dei casi ( precoci ) è normale
• Nel 60 % dei casi è disomogenea ( coesistenza di foci di fibrosi iperecogeni e foci di flogosi ipoecogeni )
martedì 16 ottobre 12

Calcificazioni parenchimali
• Costituiscono il criterio diagnostico più importante
• Depositi di calcio carbonato su una matrice proteica ( plugs) o in aree di necrosi interstiziale
• Spots iperecogeni con o senza cono d’ombra posteriore
martedì 16 ottobre 12

Calcificazioni parenchimali
• Costituiscono il criterio diagnostico più importante
• Depositi di calcio carbonato su una matrice proteica ( plugs) o in aree di necrosi interstiziale
• Spots iperecogeni con o senza cono d’ombra posteriore
martedì 16 ottobre 12

Calcificazioni parenchimali
• Costituiscono il criterio diagnostico più importante
• Depositi di calcio carbonato su una matrice proteica ( plugs) o in aree di necrosi interstiziale
• Spots iperecogeni con o senza cono d’ombra posteriore
martedì 16 ottobre 12
Alterazioni di calibro del dotto di Wirsung
• Calibro normale < 3 mm
• Irregolarità del profilo con alternanza di tratti ectasici
• Nelle neoplasie spesso dilatazione uniforme con profili regolari
• Segno specifico ,ma non sensibile
martedì 16 ottobre 12

Alterazioni di calibro del dotto di Wirsung
• Ultrasonography of the Pancreas Giulia A. Zamboni, MD*, Maria Chiara Ambrosetti, MD, Mirko D’Onofrio,
MD, Roberto Pozzi Mucelli, MD
Radiol Clin N Am 50 (2012) 395–406
• “la dilatazione ( > 3 mm) è presente nel 52,3% dei pazienti affetti da pancreatite cronica “
• da Bolondi L, Priori P, Gullo L, et al.Relationship between morphological changes detected by ultra- sonography and pancreatic exocrine function in chronic pancreatitis.Pancreas 1987;2(2):222–9.
martedì 16 ottobre 12

Calcolosi intraduttale
• Aggregati proteici con depositi di calcio carbonato
• Mobilità condizionata dalle dimensioni
• Patognomonici di pancreatite cronica
martedì 16 ottobre 12
Calcolosi intraduttale
• Ultrasonography of the Pancreas Giulia A. Zamboni, MD*, Maria Chiara Ambrosetti, MD, Mirko D’Onofrio,
MD, Roberto Pozzi Mucelli, MD
Radiol Clin N Am 50 (2012) 395–406 “the presence of calcifications is the most important and pathognomonic diagnostic
criterion for chronic pancreatitis”
Homma T, Harada H, Koizumi M. Diagnostic criteria for chronic pancreatitis by the Japan Pancreas Society. Pancreas 1997;15(1):14–5.
martedì 16 ottobre 12
Pancreatite cronica: un nuovo segno ecografico
• Impairment of Changes in the Diameter of the Pancreatic Portion of the Superior Mesenteric Vein
An Ultrasonographic Sign of Chronic Pancreatitis or Fibrosis
Hiroshi Kitamura, MD, Kazuhiko Nomura, MD, Masayuki Arai, MD, Masakazu Kobayashi, MD, Hideharu Miyabayashi, MD, Kiyoshi Furuta, MD, Shoichiro Koike, MD, Kan Nakagawa, MD
• J Ultrasound Med 2009; 28:1229–1234 • 0278-4297/09
martedì 16 ottobre 12

Pancreatite cronica: un nuovo segno ecografico
• La pressione nella porta e nei suoi rami è influenzata dalla pressione intra addominale e intratoracica: tali pressioni aumentano durante la inspirazione profonda
• Il diametro della SMV ,misurato in scansione sagittale aumenta significativamente durante la inspirazione profonda
• Una minore elasticità del parenchima pancreatico per pancreatite cronica o fibrosi ,riduce in modo significativo la variazione di calibro del tratto pancreatico della SMV
martedì 16 ottobre 12

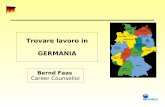
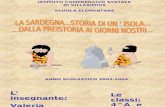
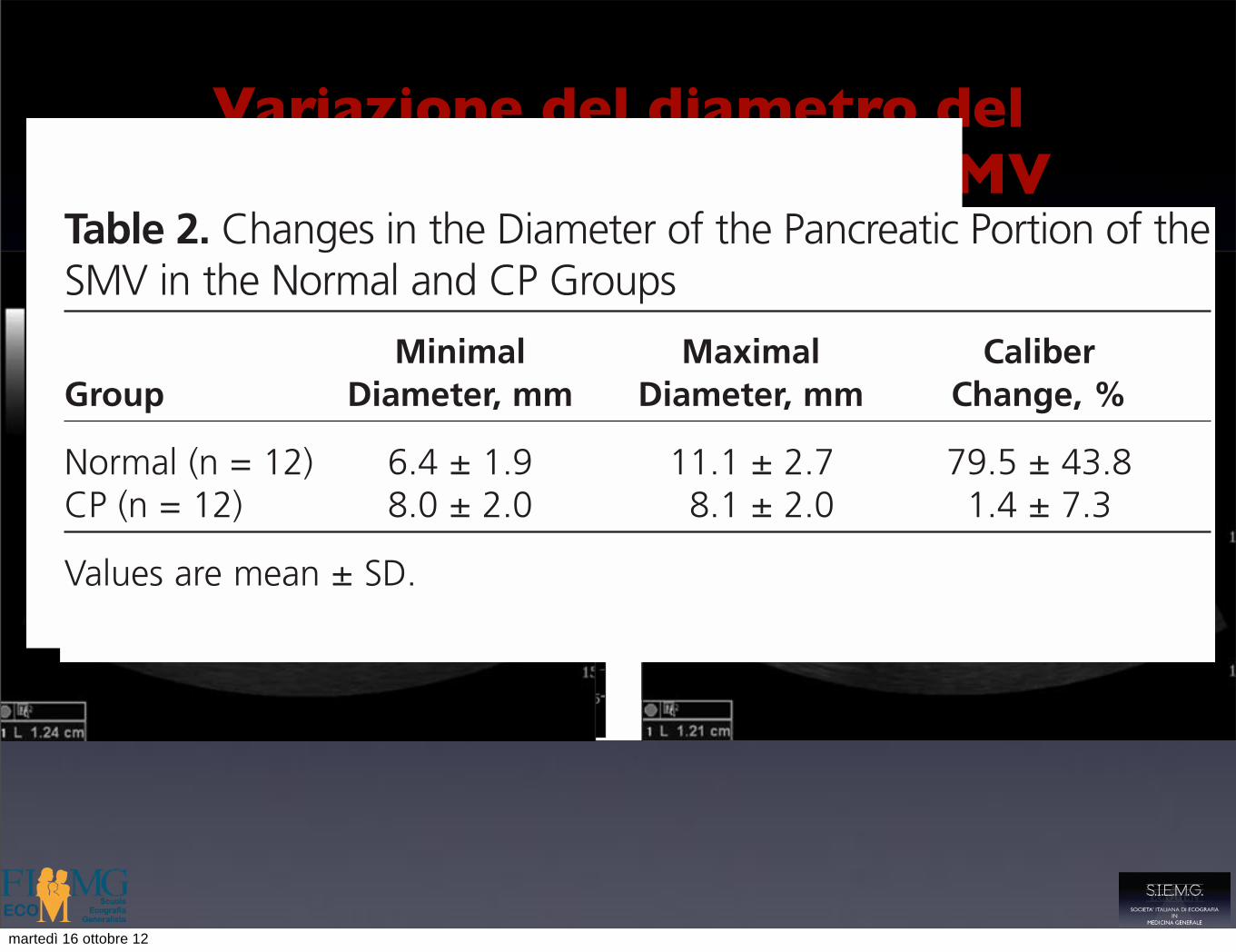
Variazione del diametro del tratto pancreatico della SMV
istence of hyperechoic and hypoechoic foci andfoci of fibrosis and inflammation, respective-ly.12,15 These findings have been described in 50%to 70% of cases.10,11 Apparent normality of theglandular echo structure in CP has been reportedin up to 40% of cases, and this is expected, espe-cially in the early stages of the disease.10,16–18
According to the Japan Pancreas Society,8 the
most important diagnostic criterion for CP is thepresence of pancreatic calcifications, the identifi-cation of which is pathognomonic. Pancreaticcalcifications are calcium carbonate deposits,usually on a protein matrix or in areas of intersti-tial necrosis. On ultrasonography, these appearas hyperechoic foci with posterior shading; how-ever, they may be hardly detectable if the calcifi-
1232 J Ultrasound Med 2009; 28:1229–1234
Superior Mesenteric Vein Diameter in Chronic Pancreatitis
Figure 2. Images from a patient with a normal pancreas. A longitudinal image of the pancreatic portion of the SMV in the expiration phase duringnormal breathing (A) shows its minimal diameter. The diameter of the SMV lumen is markedly enlarged on deep inspiration (B). The number 1 thatlabels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
A B
A B
Figure 3. Images from a patient with CP. There is no change in the diameter of the SMV lumen between the expiratory (A) and deep inspiratory (B)phases. The number 1 that labels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1232
martedì 16 ottobre 12

Variazione del diametro del tratto pancreatico della SMV
istence of hyperechoic and hypoechoic foci andfoci of fibrosis and inflammation, respective-ly.12,15 These findings have been described in 50%to 70% of cases.10,11 Apparent normality of theglandular echo structure in CP has been reportedin up to 40% of cases, and this is expected, espe-cially in the early stages of the disease.10,16–18
According to the Japan Pancreas Society,8 the
most important diagnostic criterion for CP is thepresence of pancreatic calcifications, the identifi-cation of which is pathognomonic. Pancreaticcalcifications are calcium carbonate deposits,usually on a protein matrix or in areas of intersti-tial necrosis. On ultrasonography, these appearas hyperechoic foci with posterior shading; how-ever, they may be hardly detectable if the calcifi-
1232 J Ultrasound Med 2009; 28:1229–1234
Superior Mesenteric Vein Diameter in Chronic Pancreatitis
Figure 2. Images from a patient with a normal pancreas. A longitudinal image of the pancreatic portion of the SMV in the expiration phase duringnormal breathing (A) shows its minimal diameter. The diameter of the SMV lumen is markedly enlarged on deep inspiration (B). The number 1 thatlabels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
A B
A B
Figure 3. Images from a patient with CP. There is no change in the diameter of the SMV lumen between the expiratory (A) and deep inspiratory (B)phases. The number 1 that labels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1232
istence of hyperechoic and hypoechoic foci andfoci of fibrosis and inflammation, respective-ly.12,15 These findings have been described in 50%to 70% of cases.10,11 Apparent normality of theglandular echo structure in CP has been reportedin up to 40% of cases, and this is expected, espe-cially in the early stages of the disease.10,16–18
According to the Japan Pancreas Society,8 the
most important diagnostic criterion for CP is thepresence of pancreatic calcifications, the identifi-cation of which is pathognomonic. Pancreaticcalcifications are calcium carbonate deposits,usually on a protein matrix or in areas of intersti-tial necrosis. On ultrasonography, these appearas hyperechoic foci with posterior shading; how-ever, they may be hardly detectable if the calcifi-
1232 J Ultrasound Med 2009; 28:1229–1234
Superior Mesenteric Vein Diameter in Chronic Pancreatitis
Figure 2. Images from a patient with a normal pancreas. A longitudinal image of the pancreatic portion of the SMV in the expiration phase duringnormal breathing (A) shows its minimal diameter. The diameter of the SMV lumen is markedly enlarged on deep inspiration (B). The number 1 thatlabels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
A B
A B
Figure 3. Images from a patient with CP. There is no change in the diameter of the SMV lumen between the expiratory (A) and deep inspiratory (B)phases. The number 1 that labels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1232
martedì 16 ottobre 12
Variazione del diametro del tratto pancreatico della SMV
istence of hyperechoic and hypoechoic foci andfoci of fibrosis and inflammation, respective-ly.12,15 These findings have been described in 50%to 70% of cases.10,11 Apparent normality of theglandular echo structure in CP has been reportedin up to 40% of cases, and this is expected, espe-cially in the early stages of the disease.10,16–18
According to the Japan Pancreas Society,8 the
most important diagnostic criterion for CP is thepresence of pancreatic calcifications, the identifi-cation of which is pathognomonic. Pancreaticcalcifications are calcium carbonate deposits,usually on a protein matrix or in areas of intersti-tial necrosis. On ultrasonography, these appearas hyperechoic foci with posterior shading; how-ever, they may be hardly detectable if the calcifi-
1232 J Ultrasound Med 2009; 28:1229–1234
Superior Mesenteric Vein Diameter in Chronic Pancreatitis
Figure 2. Images from a patient with a normal pancreas. A longitudinal image of the pancreatic portion of the SMV in the expiration phase duringnormal breathing (A) shows its minimal diameter. The diameter of the SMV lumen is markedly enlarged on deep inspiration (B). The number 1 thatlabels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
A B
A B
Figure 3. Images from a patient with CP. There is no change in the diameter of the SMV lumen between the expiratory (A) and deep inspiratory (B)phases. The number 1 that labels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1232
istence of hyperechoic and hypoechoic foci andfoci of fibrosis and inflammation, respective-ly.12,15 These findings have been described in 50%to 70% of cases.10,11 Apparent normality of theglandular echo structure in CP has been reportedin up to 40% of cases, and this is expected, espe-cially in the early stages of the disease.10,16–18
According to the Japan Pancreas Society,8 the
most important diagnostic criterion for CP is thepresence of pancreatic calcifications, the identifi-cation of which is pathognomonic. Pancreaticcalcifications are calcium carbonate deposits,usually on a protein matrix or in areas of intersti-tial necrosis. On ultrasonography, these appearas hyperechoic foci with posterior shading; how-ever, they may be hardly detectable if the calcifi-
1232 J Ultrasound Med 2009; 28:1229–1234
Superior Mesenteric Vein Diameter in Chronic Pancreatitis
Figure 2. Images from a patient with a normal pancreas. A longitudinal image of the pancreatic portion of the SMV in the expiration phase duringnormal breathing (A) shows its minimal diameter. The diameter of the SMV lumen is markedly enlarged on deep inspiration (B). The number 1 thatlabels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
A B
A B
Figure 3. Images from a patient with CP. There is no change in the diameter of the SMV lumen between the expiratory (A) and deep inspiratory (B)phases. The number 1 that labels the cursor is automatically numbered for numeric order of measurements by a preinstalled application.
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1232
Ultrasonographic examinations were performedas routine checkups for CP and as abdominalexaminations for various reasons in patients with-out aforementioned symptoms and findings sug-gestive of CP with written informed consent. Theapproval of the local Institutional Review Boardwas obtained.
Twelve patients with clinically and radio-graphically diagnosed CP and the same num-ber of patients with a normal pancreas werematched for age and sex. The mean age ± SDand male to female sex ratio were 56 ± 8 years(range, 47–77 years) and 8:4, respectively. Theetiology of CP was alcoholic in 10 cases andidiopathic in 2. Patients with liver cirrhosis wereexcluded because existing portal hypertensionmay have affected the results.5,7
The clinical stage of CP was determinedaccording to diagnostic criteria of the JapanPancreas Society (Table 1).8 In the pancreatitisgroup, 10 of 12 patients were classified as havingprobable CP, whereas the remaining 2 were clas-sified as having definite CP. The examiner (H.K.)was blinded to the details of the patients’ dis-eases except for the ultrasonographic findings.
All results are expressed as mean ± SD. Statisticalanalysis of the change in diameter was performedby an unpaired t test. In addition, an F test wasused to compare variance. Differences at P < .05were considered statistically significant.
The conventional ultrasonographic criteriafor CP, such as microcalcifications, an irregularcontour, and main duct dilatation, were alsorecorded.
Results
There were no technical difficulties in visualiz-ing the region of interest in any of these cases(Table 2). The patients classified as having prob-able CP showed no intrapancreatic coarsehyper-reflectivity, irregular dilatation of thepancreatic duct, or pancreatic deformity with anirregular contour. In contrast, images showingmicrocalcifications and an irregular contourwere obtained in both cases classified as definiteCP. However, the main pancreatic duct was notirregularly dilated, and no pseudocysts weredetected in either of these cases.
In the normal group, the minimal diameter ofthe anteroposterior axis of the pancreatic por-tion of the SMV was 6.4 ± 1.9 mm, and this waschanged by 79.5% ± 43.8% during deep inspira-tion (Figure 2). In the CP group, the minimaldiameter was 8.0 ± 2.0 mm, and this waschanged by 1.4% ± 7.3% during deep inspiration(Figure 3). The difference between the twogroups was statistically significant (P < .0001).
Discussion
The overall sensitivity of ultrasonography indiagnosis of CP is variable, with an averagerange in most series of 60% to 70%. Alterationsin the size, shape, and surface irregularities ofthe pancreas may be seen in less than half of allpatients affected by CP.9–11 This percentage dropsmarkedly in the early stages of the disease. Theechogenicity of the pancreas is usually increasedin CP because of adipose infiltration and fibro-sis.12–15 Hyperechogenicity is not a specific find-ing, however, because it is also seen in elderlyand obese patients. Alteration of the parenchy-mal echo structure, on the other hand, is a morespecific sign of CP. The pancreatic echo texture isinhomogeneous and coarse because of the coex-
J Ultrasound Med 2009; 28:1229–1234
Kitamura et al
Table 1. Diagnostic Criteria for the CP GroupAccording to the Japan Pancreas Society
Criterion Patients (n)
Definite CP on ultrasonographya 2Probable CP
CTb 2ERCPc 8
aPancreatic stones evidenced by intrapancreatic hyper-reflective echoes with acoustic shadows behind.bPancreatic deformity with an irregular contour.cIrregular dilatation of the main pancreatic duct aloneand intraductal filling defects suggestive of noncalcifiedpancreatic stones or protein plugs.
Table 2. Changes in the Diameter of the Pancreatic Portion of theSMV in the Normal and CP Groups
Minimal Maximal CaliberGroup Diameter, mm Diameter, mm Change, %
Normal (n = 12) 6.4 ± 1.9 11.1 ± 2.7 79.5 ± 43.8CP (n = 12) 8.0 ± 2.0 8.1 ± 2.0 1.4 ± 7.3
Values are mean ± SD.
1231
289_online.qxp:Layout 1 8/13/09 1:40 PM Page 1231
martedì 16 ottobre 12

Pancreatite cronica
martedì 16 ottobre 12
Pancreatite cronica focale o “mass forming “
• 20 % dei casi
• Massa ipoecogena a volte contenente calcificazioni
• Coinvolge tipicamente la testa pancreatica
• Di difficile distinzione ecografica rispetto al carcinoma
• CEUS e biopsia
martedì 16 ottobre 12

CEUS
• Nelle fasi precoci impregnazione simile al parenchima circostante
• Wash-out simile a quello della ghiandola pancreatica
• Impregnazione correlata alla intensità del processo infiammatorio
martedì 16 ottobre 12

Pancreatite cronica autoimmune
• Meccanismo patogenetico autoimmune
• In associazione a colangite sclerosante e colite ulcerosa
• Infiltrato linfocitario periduttale
• Evoluzione in fibrosi
martedì 16 ottobre 12
Pancreatite cronica autoimmune
• Pancreas diffusamente aumentato di volume
• Aspetto a salsiccia
• Dotto di Wirsung compresso o filiforme
• Assenza di flogosi peripancreatica
• Assenza di calcificazioni
• Ecogenicità marcatamente ridotta
martedì 16 ottobre 12
Conclusioni
martedì 16 ottobre 12
Ecografia nella pancreatite acuta
• Per confermare la diagnosi clinica
• Per una diagnosi di eziologia
• Per la dimostrazione di complicanze
• Per il follow up
• Consente una valutazione morfologica di massima , non essendo in grado di identificare direttamente la necrosi parenchimale
martedì 16 ottobre 12
Ecografia nella pancreatite cronica
• Metodica di prima istanza, economica, rapida,non invasiva
• Tecnica di scelta per il follow up
• Forti limiti nella DD fra pancreatite cronica focale e carcinoma
martedì 16 ottobre 12

grazie per la attenzione
martedì 16 ottobre 12