Corso nazionale SIE di aggiornamento in ematologia clinica ... · Corso nazionale SIE di...
45
Corso nazionale SIE di aggiornamento in ematologia clinica Il trapianto allogenico nella LLC Bolzano, 18-19 giugno 2009 Francesco Zaja - Clinica Ematologica, Udine
Transcript of Corso nazionale SIE di aggiornamento in ematologia clinica ... · Corso nazionale SIE di...

Corso nazionale SIE diaggiornamento in ematologia clinica
Il trapianto allogenico nella LLC
Bolzano, 18-19 giugno 2009
Francesco Zaja - Clinica Ematologica, Udine
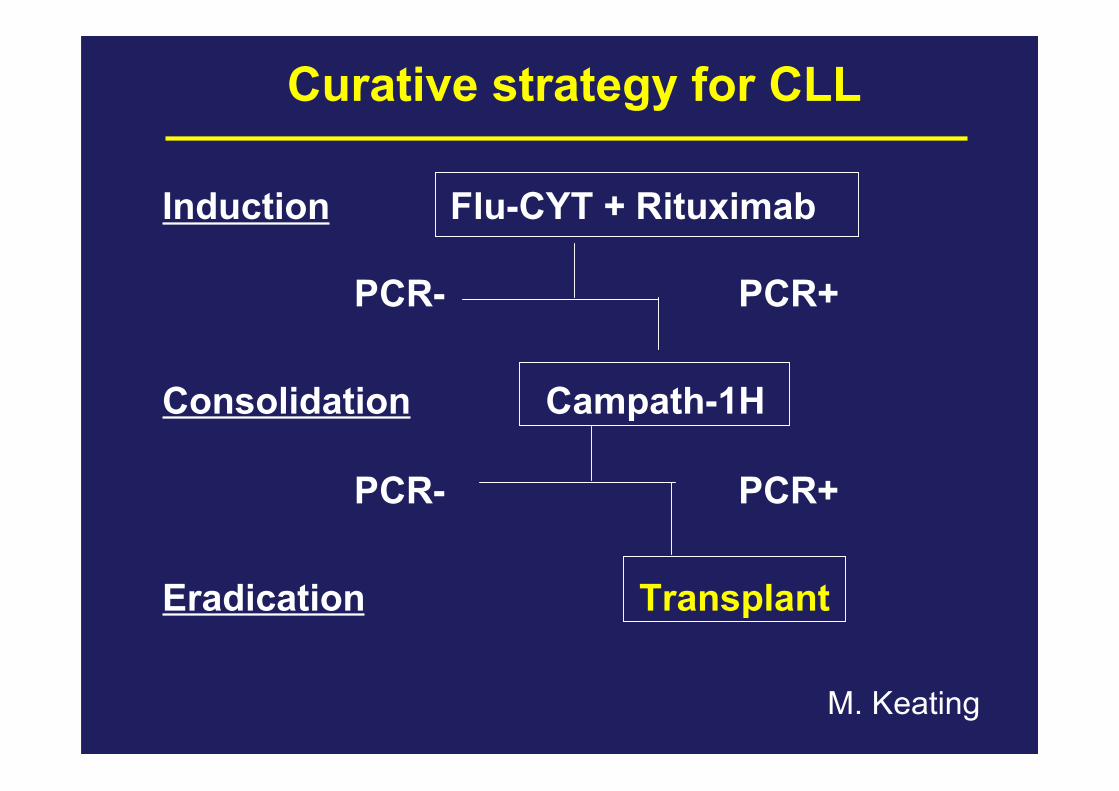
Curative strategy for CLL
Induction Flu-CYT + Rituximab
PCR- PCR+
Consolidation Campath-1H
PCR- PCR+
Eradication Transplant
M. Keating
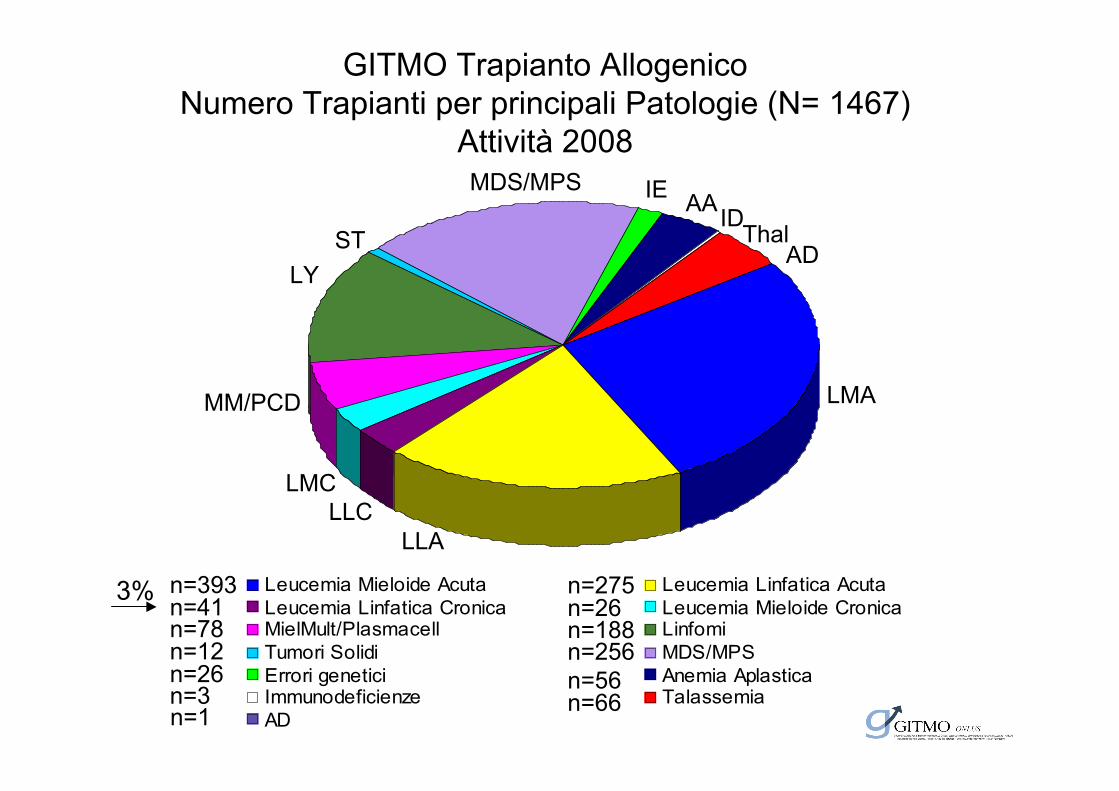
Leucemia Mieloide Acuta Leucemia Linfatica Acuta
Leucemia Linfatica Cronica Leucemia Mieloide CronicaMielMult/Plasmacell Linfomi
Tumori Solidi MDS/MPS
Errori genetici Anemia AplasticaImmunodeficienze Talassemia
AD
n=26 n=56
AAThal
AD
LMA
LLALLC
LMC
MM/PCD
LYST
MDS/MPS
n=12
n=66n=1
n=41n=78
n=393 n=275n=26n=188n=256
n=3
ID
GITMO Trapianto AllogenicoNumero Trapianti per principali Patologie (N= 1467)
Attività 2008IE
3%

• La più frequente forma leucemica dell’adulto (25% delle leucemie)
• Incidenza pari a 2-6 x 100.000 abitanti anno (paesi occidentali), ma13 x 100.000 abitanti anno a 65 anni e circa 30 x 100.000 abitantianno dopo i 70 anni
• Età mediana di insorgenza 65 anni
• M/F: 2/1
• 30% dei pazienti ha un’età < 60 anni
• 10-15% dei pazienti ha un’età < 50 anni
Epidemiologia CLL
Rationale of SCT in CLL
CLL in relapsed/advanced stage or with high risk features:- poor prognosis- conventional therapies not curative
Potentially curative in CLL:- Stem cell source free of tumour contamination- Graft vs leukemia effect

Who are poor risk patients?
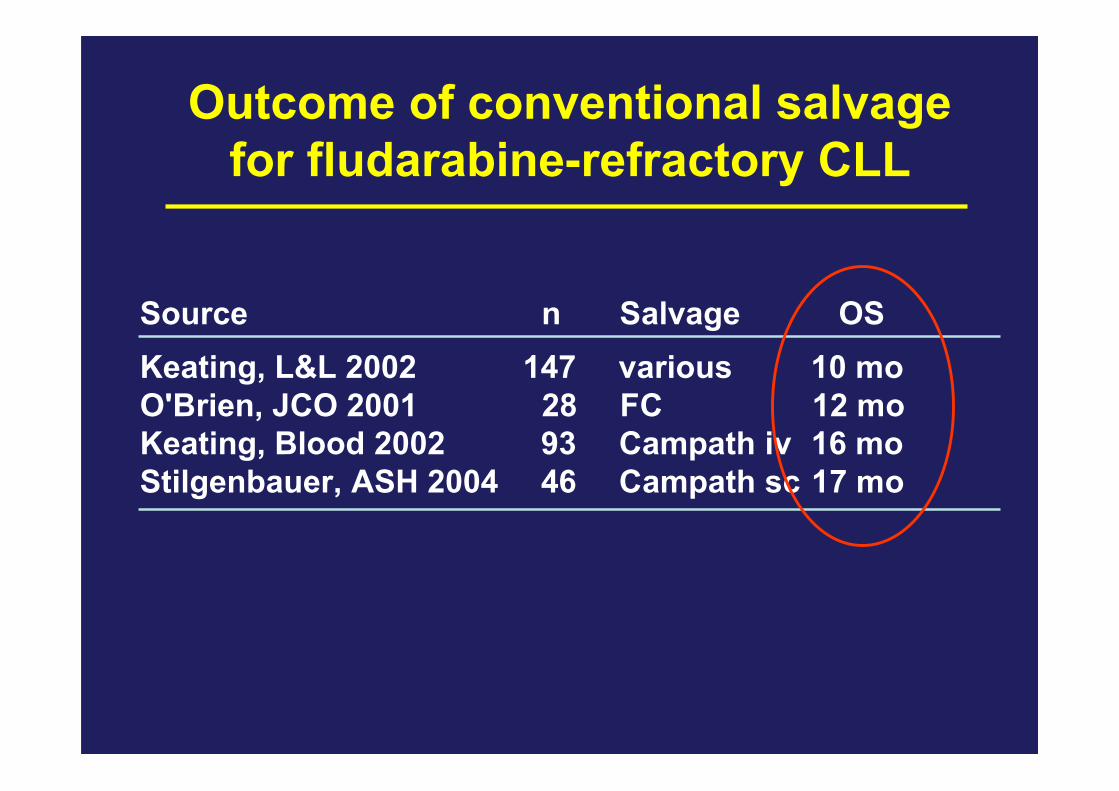
Outcome of conventional salvagefor fludarabine-refractory CLL
Source n Salvage OSKeating, L&L 2002 147 various 10 moO'Brien, JCO 2001 28 FC 12 moKeating, Blood 2002 93 Campath iv 16 moStilgenbauer, ASH 2004 46 Campath sc 17 mo

Survival from Time of Diagnosis (n=325)
13q- single
Survival in Months
11q-
+12
17p-
36 72 108 144 180
20
40
60
80
100
00
Overall survival ofCLL patients by FISHkaryotype
Döhner, NEJM 2000
Prognostic impact ofFISH karyotype in CLL

SopravvivenzamedianadeipzconLLCinrapportoallostatomutazionaleIgVHedespressioneZAP-70
Hamblin et al Blood 1999 Crespo et al, 2003

Definition of poor risk patients fortherapeutic purpose
• NR or early relapse (within 12 months) after purine analogue containing therapy• Relapse within 24 months from ASCT• p53 deletion/mutation requiring therapy
Dreger et al Leukemia 2007 (EBMT consensus)

Years
0 2 61 3 4 5
Probability of survival after Probability of survival after autologousautologous and andHLA-identical sibling SCT for CLL, 1998HLA-identical sibling SCT for CLL, 1998––20062006
Autotransplant (N=394)
CONV (N=382) RIC (N=529)
P<.0001.
0
20
40
60
80
100
10
30
50
70
90
0
20
40
60
80
100
10
30
50
70
90
Probab
ility
of Surv
ival
, %
CIBMTR

PFS after auto-SCT in CLL:retrospective studies
Years
Probability 0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Auto
Allo
24% (±7)
42% (±9)
Esteve 2001
n = 124
Gribben 2005
n = 137
TCDTCDn = 25

Allo-SCT in CLL: key issues
Dreger et al Leukemia 2007 (EBMT consensus)
1. Does GVL activity in CLL exist?
2. What is the success rate of SCT (disease controlvs. toxicity)?
3. Is it effective in high-risk disease?
4. Indications for allo-SCT in CLL?

1. Does GVL activity in CLL exist?

Evidence for GVL in CLL: relapse rate• Few late relapses after allo-SCT in contrast to auto-SCT (Esteve ’01)
•• MRD kinetics correlate to immune intervention MRD kinetics correlate to immune intervention ((RitgenRitgen ’’04)04)
Years
Probability
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Auto
Allo
24% (±7)
42% (±9)
Esteve 2001
n = 124 n = 137
auto
allo
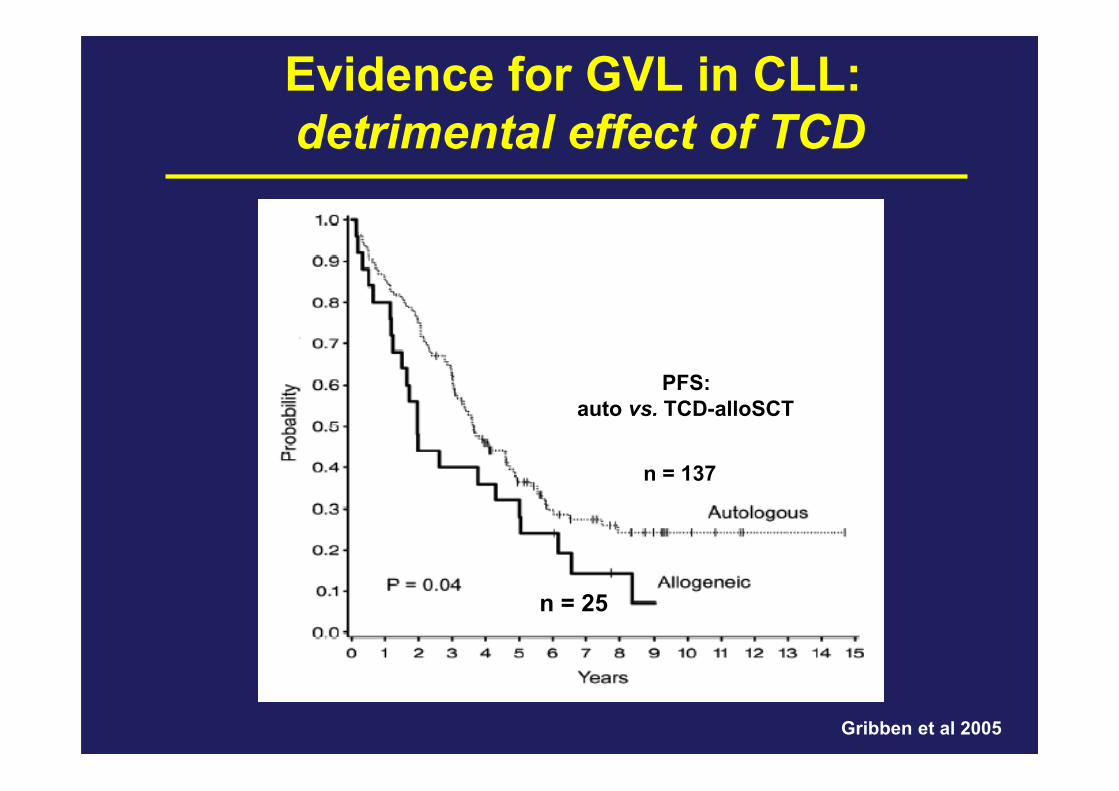
Evidence for GVL in CLL: detrimental effect of TCD
PFS:auto vs. TCD-alloSCT
n = 137
Gribben et al 2005
n = 25

Evidence for GVL in CLL:beneficial effect of DLI
• 1 x 107 CD4+ cells/kg or 3 x 107 CD4+ cells/kg • 6/7patients responded to DLI
Gribben et al 2005

Dreger, Leukemia ’03; Ritgen, Leukemia ’08; Schetelig, JCO ’08; Corradini, Haematologica ’09
Evidence for GVL in CLL:favorable effect of cGVHD
0 12 24 36 48
0
25
50
75
100
after cGVHD onset
cGVHD always absent
Months from SCT
Percent with relapse or
progression
Dreger et al. Leukemia 2003

Higher incidence of PCR negativity in patients with
cGvHD (75% vs 46%)
2. in PCR neg pts with a delayed clearance of MRD, the onset
of GvHD preceded the achievement of molecular remission;
3. overall GvHD was more frequent in patients who did not
relapse (p=0.04): the crude incidence of grade 2-4 acute
and chronic GvHD was 22% in relapsed and and 70% in
not relapsed patients.
Evidence for GVL in CLL:favorable effect of cGVHD
Corradini, Haematologica 2009

CLL3x: m (sib) p# 05001
-180 180 360 540SCT
10 -5
10 -4
10 -3
10 -2
10 -1
10 0
0
25
50
75
100
CSA
start of cGVHD
BLOOD 2004;104:2600
Chimerism

Does GVL activity in CLL exist?
Yes

2. What is the success rate of SCT
(disease control vs. toxicity)?

Survival After SCT
Years
Pro
bab
ility 0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Auto
Allo
63% (±7)
56% (±7)
Auto=124 (28 dead)
Allo=46 (20 dead)
Esteve et al, ASH 2001
100 days CONV allo-TRM: 31%

CONV Allo-SCT with in CLL
Dreger et al. Leukemia ’07

EBMT survey on RIC allografting for CLL:Treatment-related mortality (n=77)
0 12 24 36 480
25
50
75
100
18% (9;27)
Months from SCT
Percent TRM
Dreger et al Leukemia 2003
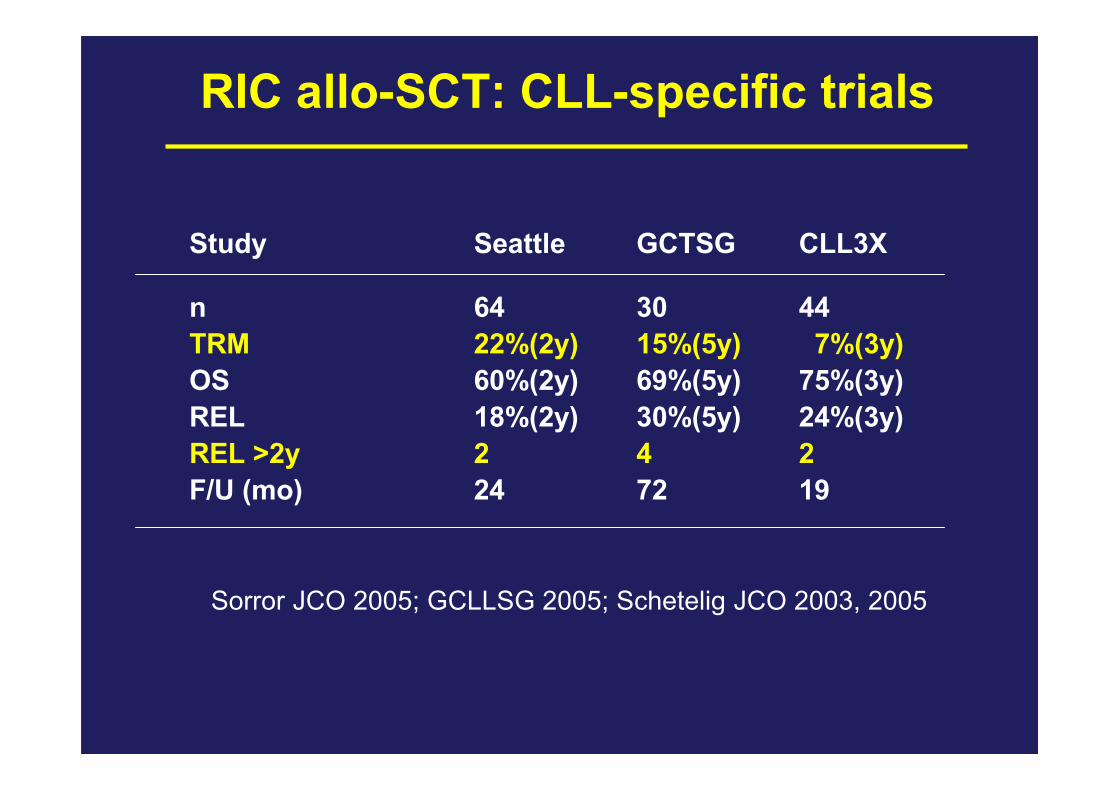
RIC allo-SCT: CLL-specific trials
Study Seattle GCTSG CLL3X
n 64 30 44
TRM 22%(2y) 15%(5y) 7%(3y)
OS 60%(2y) 69%(5y) 75%(3y)
REL 18%(2y) 30%(5y) 24%(3y)
REL >2y 2 4 2
F/U (mo) 24 72 19
Sorror JCO 2005; GCLLSG 2005; Schetelig JCO 2003, 2005

Allo-SCT in CLL (EBMT):
Population-matched analysis
- 73 RIC cases (survey), 82 MC cases (registry)
- matched for age, donor, remission status, sex
- by serial Cox modeling
- RIC reduces TRM (HR 0.4; p 0.025)
- RIC increases relapse (HR 2.7; p 0.054) (?)
- no influence on EFS and OS
Prospective controlled studies are needed!
Dreger et al Leukemia 2005

RIC allo-SCT on CLL:MRD vs. MUD
Study Seattle CLL3X
MRD MUD MRD MUD
n 44 20 25 25
TRM (2y) 22% 20% 0% 14%
OS (2y) 56% 74% 87% 77%
REL (2y) 34% 5% 13% 23%
GCLLSG 2005; Sorror JCO 2005

CLL3X: PFS according to MRDnegativity (n=26)
0 12 24 36 48 60 720
25
50
75
100
HR 0.06; p 0.0002
not MRD neg at 12 mo
MRD neg at 12 mo
Months post SCT
% progression-free
CLL3X: TRM
0 12 24 36 48 60 720
25
50
75
100
11% (0, 23%)
Months from allo-SCT
Perc
ent T
RM
RIC allo-SCT in CLL: results from theGCLLSG CLL3X trial
• Molecular response ≥ 50% of the pts with high-risk CLL• Prognostic impact of MRD negativity at +12 month
Ritgen et al Leukemia 2008
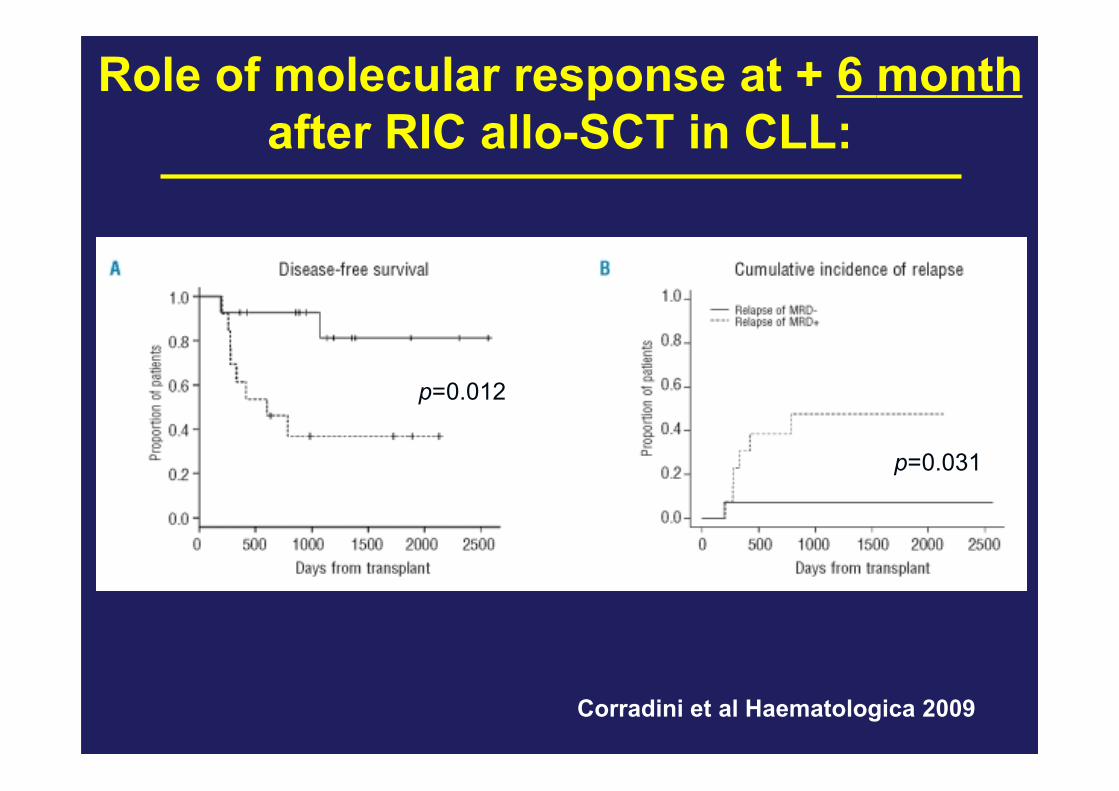
Corradini et al Haematologica 2009
p=0.012
p=0.031
Role of molecular response at + 6 monthafter RIC allo-SCT in CLL:

What is the success rate of SCT
(disease control vs. toxicity)?
• Allo SCT active
• Molecular remission
• RIC associated with reduced TRM

3. Is it effective in high-risk disease?
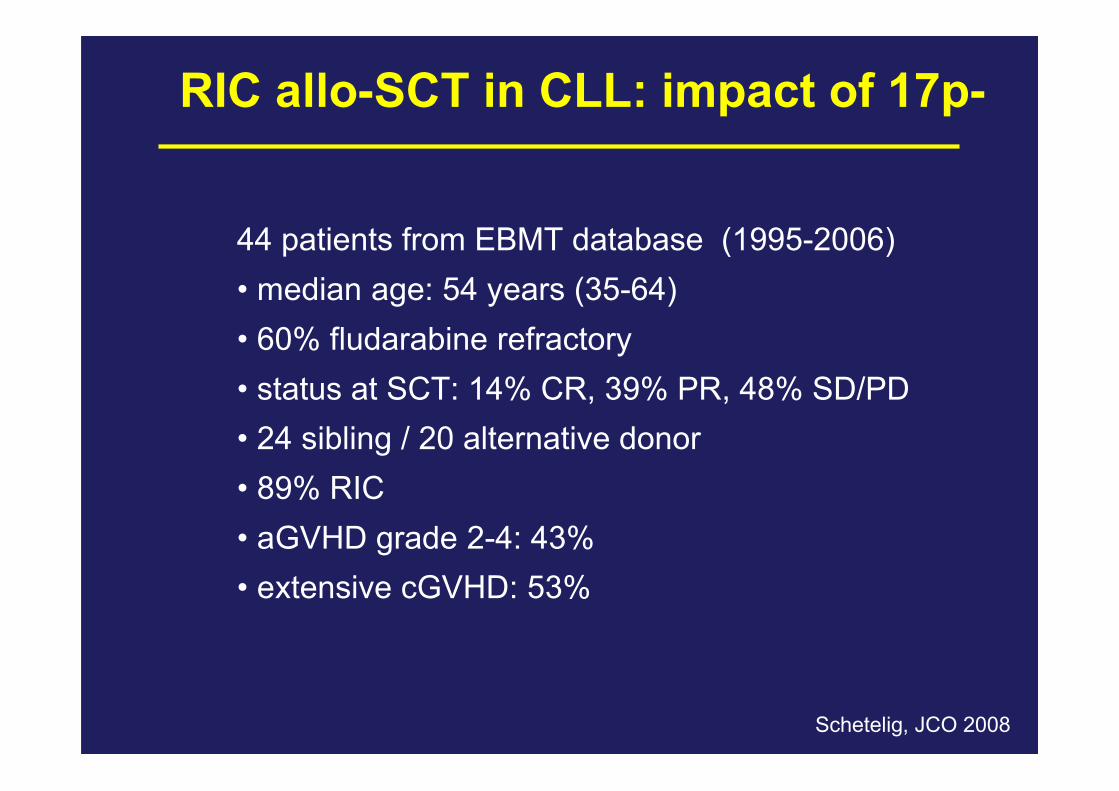
RIC allo-SCT in CLL: impact of 17p-
44 patients from EBMT database (1995-2006)• median age: 54 years (35-64)• 60% fludarabine refractory• status at SCT: 14% CR, 39% PR, 48% SD/PD• 24 sibling / 20 alternative donor• 89% RIC• aGVHD grade 2-4: 43%• extensive cGVHD: 53%
Schetelig, JCO 2008

RIC allo-SCT in CLL: impact of 17p-
3-year OS 44% 3-year PFS 37%
3-year relapse 30%3-year TRM 32%
Schetelig et al JCO 2008

Dreger 2005
CLL3X: Relapse incidence byFISH karyotype (n=42)
0 12 24 36 48 60 720
25
50
75
100
other
del 11q- / del 17p-
Months post SCT
% relapsed

RIC allo-SCT in CLL:Impact of poor-risk factors
Other adverse prognostic factors like VH genemutational status or ZAP-70 espression seem to
have no major influence on the outcome afterallogeneic SCT.
Ritgen, Blood 2004; Moreno, JCO 2005 (VH gene); Caballero, Clin Cancer Res 2005;Khouri, BJH 2007 (ZAP-70)
Is it effective in high-risk disease?
• Yes.
• Allo SCT has the potential toinduce long-term DFS in patientswith 17p-CLL.
• Detrimental effect of TCD.

4. Indications for allo-SCT in CLL?

EBMT guidelines for SCT in CLL
Dreger et al. Leukemia ’07 (EBMT consensus panel)
Allo-SCT in poor-risk CLL including:• Fludarabine resistence – non response or early relapse (<12 months) after purine analogue-based tx• Relapse <24 months after purine analogue combinations or auto-SCT (+ high risk genetics)• p53 mutation with treatment indication
Auto-SCT indicated in clinical trial only.

Criteri di eleggibilità per ricerca MUD.Standard IBMDR maggio ’09
Linfomiaggressivi in
francaprogressione
Frontline
Ricaduto/resistenteall’autologo e/o
polichemioterapiadi età ≤ 65 anni
LNH/LLC
Categoria Csenza
indicazione
Categoria Bsperimentale
Categoria Acomprovata
Patologia
Pazienti 66-70 anni:• Nell’ambito di protocolli clinici• Specifica richiesto al registro

Allo SCT in CLL
RIC
CONV
PRO vs CONS
++
--

Proposal for alloSCT in poor risk CLL
• Good disease control• Older• Comorbidities
RIC
• Refractory• Younger (???)• No comorbidities
CONV

• 3.986 patients with CLL/SLL (1975-2005, MDACC)• 204 patients (5.1%): possible RS• 148 patients (3.7%): biopsy proven RS• 20 patients underwent alloSCT
Richter’s syndrome
AM Tsimberidou et al. JCO 2006

Patients who received alloSCT as postremission therapyhad longer survival than patients who achieved remissionand received no additional therapy or patients who underwent allo or autoSCT as salvage therapy (P = .019).
AM Tsimberidou et al. JCO 2006