Scompenso cardiaco Acuto > Scompenso cardiaco Acuto ESC 2005

Una testimonianza
5° CONVEGNO NAZIONALE ANNUALE AISC – 30 SETTEMBRE 2019 – ASCEA MARINA (SA)
FONDAZIONE ALARIO- SALA AUDITORIUM PARMENIDE
www.associazioneaisc.org [email protected]
COMBATTERE OGNI GIORNO CON LO SCOMPENSO CARDIACO
( e non solo….)
GIUSEPPE LEONARDI
U.O.s.d. «Scompenso Cardiaco Grave»Az. Ospedaliero Universitaria «Policlinico – V. Emanuele»
Catania

Abiti da Lavoro

Scompenso Cardiaco
• Lo scompenso non può essere considerato come una patologia omogenea, ma è piuttosto una sindrome, che riconosce diverse tipologie di malati con caratteristiche differenti anche all’interno della stessa classe funzionale.
• Diversi fattori possono modificare il percorso gestionale e l’aderenza ai programmi di cura al di fuori dell’ospedale
Ital Heart J Suppl 2006; 7 (6): 381-432

Popolazione generale 0,5-1,5%
Età > 70 anni 5-10%
Prevalenza di scompenso cardiaco nella popolazione generale
2008 17.260 ricoveri2009 31% riospedalizzazioni
9% riospedalizzazioni precoci
Età 65-84 anni (popolazione Lazio) 6-7%
50% sopravvivenza a cinque anni
Studio Predictor 2008-2010 (Regione Lazio)
Mosterd A., Hoes AW, Clinical epidemiology of heart failure Heart 2007

• Circa 14 milioni di europei sono affetti da insufficienza cardiaca, l’equivalente della popolazione del Belgio, con
un’incidenza di 3.6 milioni di nuovi casi annui e una stima di oltre
30 milioni di pazienti previsti per il 2020. Nei paesi occidentali, la percentuale di malati varia dall’1% al 2% della
popolazione, valore che cresce in modo esponenziale con l’aumentare dell’età. La mortalità per questa patologia è comunque
elevata, nonostante si osservi una riduzione del rischio di morte laddove siano stati intrapresi idonei programmi di prevenzione 3-6.
• P. Fontalive et. Al. G Ital Cardiol 2015;16(1):21-30

L’aumento dell’incidenza si ritiene sia dovuto :
• 1) all’aumento progressivo dell’età media
della popolazione
• 2) al maggior numero di diagnosi effettuate a
seguito di una maggiore sensibilizzazione al
riconoscimento di questa patologia
• 3) Aumento dei pazienti trattati in modo
adeguato

G. Di Salvo- II Cattedra Cardiologia-Osp. Monaldi-Napoli


14
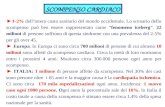
Chronic decline
Mortality
Acute episodes
Disease progression
Function& quality
of life (QoL)
▪ With each acute event, myocardial injury may contribute to progressive LV dysfunction
▪ Increasing frequency of acute events with disease progression leads to high rates of hospitalization and increased risk of mortality
Ahmed et al. Am Heart J 2006;151:444–50; Gheorghiade et al. Am J Cardiol 2005;96:11G–17G
Gheorghiade & Pang. J Am Coll Cardiol 2009;53:557–73; Holland et al. J Card Fail 2010;16:150–6Muntwyler et al. Eur Heart J 2002;23:1861–6
Adapted from Gheorghiade et al. 2005
HF is a chronic condition interspersed with acute episodes
▪ Increasing frequency of acute events with disease progression leads to high rates of hospitalization and increased risk of mortality1–5
1. Ahmed et al. Am Heart J 2006;151:444–50; 2. Gheorghiade et al. Am J Cardiol 2005;96:11G–17G 3. Gheorghiade, Pang. J Am Coll Cardiol 2009;53:557–73; 4. Holland et al. J Card Fail 2010;16:150–6
5. Muntwyler et al. Eur Heart J 2002;23:1861–6

HEART FAILURE IS A HIGH MORTALITY SYNDROME, DESPITE SIMPTOMS
SYMPTOMS AND REALITY
1 2017 Metra_JCardiovascMed_20172 Butler_et_al-2016-European_Journal_of_Heart_Failure

NYHA I NYHA II NYHA III NYHA IV
ACTUAL DISEASE PROGRESSION

Costi ricovero Scompenso
• Degenza ospedaliera che mediamente supera i dieci giorni
• il Servizio sanitario nazionale spende complessivamente 550 milioni di euro l’anno (equivalenti a 11.800 euro per ciascun paziente) di cui l’85% è rappresentato dai costi di ospedalizzazione.
• Il costo delle riospedalizzazioni quasi il doppio rispetto a quello del primo ricovero: oltre 7 mila euro contro i circa 4.500 per il primo ricovero.
Maggioni AP et al: The real word evidence CHF:
Findings from 41413 patients of the ARNO database 2015

Acute Heart Failure: Hospitalizations
• Worsening chronic heart failure (HF):80% of all admissions
• Acute de novo heart failure (diagnosed for the first time): 15%
• Advanced/end-stage/refractory HF: 5%
Gheorghiade M, Circulation 2005

Insufficienza cardiaca ( DRG 127)
• 52% dei ricoveri avviene per ‘’Scompenso a basso rischio’’
• 40% delle riospedalizzazioni per scarsa compliance del paziente
Piccinino-68° Congresso Nazionale SIC 2007





Ital Heart J Suppl 2006; 7 (6): 381-432

Paziente
Medico di FamigliaCardiologo ExO
Home CareService
Esiti
Organo di Controllo (ASL)
Ospedale di Rete -spokecon USC/Ambulatorio SC
Struttura di III livello - hubCentro Trapianti
Malato
oligo-asintomatico
Malato severo
NYHA III-IV
Candidato TCO
Malato con
disfunzione
asintomatica
Malato anziano
+ comorbilita’
Paziente
Medico di FamigliaCardiologo ExO
Home CareService
Esiti
Organo di Controllo (ASL)
Ospedale di Rete -spokecon USC/Ambulatorio SC
Struttura di III livello - hubCentro Trapianti
Malato
oligo-asintomatico
Malato severo
NYHA III-IV
Candidato TCO
Malato con
disfunzione
asintomatica
Malato anziano
+ comorbilita’
Malato severo
NYHA III-IV
Candidato TCO
Malato
Scompenso
Terminale
Malato
HFA nuova
diagnosi
Instabilizzato
Ital Heart J Suppl 2006; 7 (6): 381-432

I modelli di gestione del paziente scompensato
cronico utilizzati fino ad oggi sono
essenzialmente di quattro tipi:
• 1. modello gestionale infermieristico: imperniato sulla figura
dell’infermiere specializzato, con supervisione di un medico;
• 2. modello gestionale basato su contatti telefonici e visite di
controllo programmate;
• 3. modelli a multicompetenza: infermiere specializzato,
dietista, assistente sociale, cardiologo, assistenza
domiciliare, contatti telefonici;
• 4. unità scompenso: ricoveri in unità specialistiche
cardiologiche con impostazione di una terapia farmacologica
intensiva, infermiere specializzato, dietista, assistenza
sociale, fisioterapia con follow-up gestito dal cardiologo,
dall’infermiere dell’unità, in solido con il medico di medicina
generale.


ACC/AHA Practice Guidelines
Pyramid Approach to HF Stages
High Risk for Developing HFHypertension
CAD
Diabetes mellitus
Family history of cardiomyopathy
Asymptomatic HFPrevious MI
LV systolic dysfunctionAsymptomatic valvular disease
Symptomatic HFKnown structural heart diseaseShortness of breath and fatigue
Reduced exercise tolerance
Refractory End-Stage HF
Marked symptoms at restdespite maximal medical therapy
A
B
C
D
Hunt SA et al. Circulation. 2005 Sep 20;112(12):e154-235 .
Cardiol.
MMG

PREVENIRE
-
COSA SI PUO’ FARE?
DIAGNOSTICARE
FOLLOW-UP
CURARE

TABLE 24Recommended components of care and following programmes
( Class of recommendacion I, level of evidence C
Use of multisciplinary team approach
Vigilant follow-up, first FU within 10 days of discarge
Discharge planning
Increased access to health care
Optimizing medical therapy whit guidelines
Early attemtion to sign and symptoms
• Flexible diuretic regimen
• Intense education and counseling
• Inpatient and outpatient• ( Home-based)
• Attention to behavioural strategies
• Address barriers to compliance
ESC GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF CHF UPDATE 2005

Luigi Tavazzi et al. Circ Heart Fail. 2013;6:473-481 IN-HF OUTCOME

Comorbidity Burden & Prognosis:Impact of non-cardiac comorbidities on mortality and HF
hospitalization
Deursen VM, EJHF 2014

1. Il BENESSERE DEL PAZIENTE;
2. LA RIDUZIONE DEI RICOVERI:
3. LA RIDUZIONE DELLA MORTALITA’.
LA GESTIONE SUL TERRITORIO
QUALI GLI OBIETTIVI

Kaplan–Meier curves for admission to hospital for HF
Luigi Tavazzi et al. Circ Heart Fail. 2013;6:473-481
Copyright © American Heart Association, Inc. All rights reserved.IN-HF Outcome Tavazzi L, Circ HF 2013

Rehospitalization is particularly high in the early phase after hospitalization
Alkshay D, Circ HF 2012



All-cause death or HF hospitalization Tavazzi L, Circ HF 2013
IN-HF Outcome

“Vulnerable Phase”: week to 1-3 months post-discharge
Marti NC, Circ HF 2013

Value of follow-up visit after discharge


Circulation 2010




Chronic HF survival rates have improved over time with the advent of new therapies
Population-based cohort study analyzing data from the Rochester Epidemiology Project, Minnesota, USA. 4,537 patients with a diagnosis of HF between 1979 and 2000 were included. Framingham criteria and clinical criteria were used to validate the diagnosis.
Temporal trends in 5-year mortality after the diagnosis of HF by gender show
improvements in survival …
Su
rviv
al (%
)
100
80
60
40
20
0
Men Women
0 1 2 3 4 5 6 7 8 9 10
YearsS
urv
iva
l (%
)
100
80
60
40
20
0
1996–2000
1991–1995
1985–1990
1979–1984
... nevertheless, the 5-year mortality rate remains high
Roger et al. JAMA 2004;292:344–50
0 1 2 3 4 5 6 7 8 9 10
Years

LCZ696 is the first agent to demonstrate a significant clinical benefit with NP system enhancement in chronic HF with reduced ejection fraction
1981Discovery of ANP1
1980s
1988NEP identified as the
primary enzyme responsible for degrading ANP2
1990sNEPi
NEP inhibition alone fails to demonstrate efficacy in patients with chronic HF, mainly due to
the ‘promiscuity’ of NEP towards other substrates such as Ang II3
2009
LCZ696 (ARNI)Phase III PARADIGM-HF
(HFrEF) initiated5,6
2002 Omapatrilat (NEPi+ACEI)Combined NEP and ACE
inhibition with omapatrilat indicates trends towards efficacy in chronic HF, but
raises significant safety concerns3,4
2014LCZ696 (ARNI)
PARADIGM-HF studyLCZ696 was superior to
enalapril in reducing the risks of death and HF
hospitalization in patients with HFrEF6
1990s 2000s 2010s
1. de Bold et al. Life Sci 1981;28:89–94; 2. Sonnenberg et al. Peptides 1988;9:173–80; 3. Von Lueder et al. Pharmacol Ther 2014;144:41–9; 4. Packer et al. Circulation 2002;106:920–6; 5. McMurray et al. Eur J Heart Fail 2013;15:1062–73; 6. McMurray et al. N Engl J Med 2014;371:993–1004
ACE: angiotensin-converting enzyme; ACEI: angiotensin-converting-enzyme inhibitor; Ang: angiotensin; ANP: atrial natriuretic peptide; ARNI: angiotensin receptor neprilysin inhibitor; AT1R:angiotensin II type 1 receptor; HF: heart failure; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; NEP: neprilysin; NEPi: neprilysin inhibition; NP: natriuretic peptide; NT-proBNP: N-terminal pro-B-type natriuretic peptide; PARADIGM-HF: Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure

NYHA I NYHA II NYHA III NYHA IV
EXPECTED DISEASE PROGRESSION BY ARNI

50
▪ HF mortality remains high, with ~50% of patients with HF dying within 5 years of diagnosis1,2
Outcomes for patients with HF are poor in clinical practice
IN-CHF Registry
1-year follow-up (n=1,315 patients)
12.4
23.8
Ho
sp
ita
liza
tio
n
du
e to
HF
25
20
15
10
5
0
Pa
tie
nts
(%
)
12.8
38.1
Chronic HF3 Acute HF4
*From hospital discharge; IN-CHF=Italian Network on Congestive Heart Failure
1. Roger et al. JAMA 2004;292:344–50; 2. Levy et al. N Engl J Med 2002;347:1397–402
3. Senni et al. J Cardiac Fail 2005;11:270–8; 4. Tavazzi et al. Eur Heart J 2006;27:1207–15
All-cause
mortality
All-cause
hospitalization
50
40
30
20
10
0
Pa
tie
nts
(%
)
All-cause
mortality
All-cause
hospitalization

Morte improvvisa e per peggioramento di scompenso: incidenza relativa
Willenheimer R. Eur. Heart J.Supplements 2006 (8) (Supplement C), C43-C50

• Aumenta l’incidenza relativa della morte per peggioramento di scompenso
Vanoli et Al, Eur Heart Journal Suppl (2006) 8
Con il progredire della malattia

• Causes of death and rehospitalization in patients hospitalized with worsening heart failure and reduced left
ventricular ejection fraction: Results from efficacy of vasopressin antagonism in heart failure outcome studywith tolvaptan (EVEREST) program.
O’Connor C.M. et al Am. Heart J. 2010; 159:841-849.e1
Elevata incidenza di morte e ri-ospedalizzazioni post-dimissione nonostante le terapie ricevute in ospedale

• Resuscitated sudden deaths* occurred in 16 patients receiving LCZ696 versus 28 patients receiving enalapril (HR 0.57, 95% CI: 0.31–1.04, p=0.07). Further, LCZ696 significantly reduced the risk of combined resuscitated and non-resuscitated sudden deaths by 22% when compared with enalapril (HR 0.78, 95% CI: 0.66–0.92, p=0.002)
LCZ696 significantly reduced the number of sudden cardiac deaths compared with enalapril
Desai et al. Eur Heart J 2015
Hazard ratio = 0.80 (95% CI: 0.68–0.94) p=0.008
Enalapril
LCZ696
0 180 360 540 720 900 1,080 1,260
0
0.02
0.04
0.06
0.08
0.10
Days since randomizationNo. at riskLCZ696 4,187 3,891 2,478 1,005Enalapril 4,212 3,860 2,410 994
Cu
mu
lati
ve p
rob
abili
ty o
f ev
ent
*Resuscitated sudden deaths were defined as successful resuscitation following cardiac arrest
CI=confidence interval; HR=hazard ratio

Death due to worsening of heart failure was significantly reduced by LCZ696 treatment compared with enalapril
Desai et al. Eur Heart J 2015;
Enalapril
LCZ696
Hazard ratio = 0.79 (95% CI: 0.64–0.98)p=0.034
0 180 360 540 720 900 1,080 1,2600
0.02
0.04
0.06
0.08
0.10
Cu
mu
lati
ve p
rob
abili
ty o
f ev
ent
Days since randomizationNo. at riskLCZ696 4,187 3,891 2,478 1,005Enalapril 4,212 3,860 2,410 994
CI=confidence interval

• Compared with enalapril, sacubitril/valsartan treatment significantly decreased the rates of
readmission for any cause at 30 days (p=0.031) and readmission for HF at 30 days (p=0.006)
• Rates of both all-cause (p-0.045) and HF readmission (p=0.01) at 60 days were also
significantly reduced with sacubitril/valsartan versus enalapril
ESC GL objective: Prevent hospital admissionLCZ696 significantly reduced the rates of all-cause and HF readmissions
21
13,4
30,5
20,3
17,8
9,7
27,8
17,1
0
5
10
15
20
25
30
35
0,2 0,4 0,6 0,8 1 1,2 1,4 1,6 1,8
All-cause readmissionSac/val: 192/1076
Enalapril: 275/1307
HF readmissionSac/val: 104/1074Enalapril: 175/1302
All-cause readmissionSac/val: 294/1059
Enalapril: 391/1283
HF readmissionSac/val: 180/1055Enalapril: 259/1275
30-d
ay
read
mis
sio
n60
-day
re
adm
issi
on
0.74 (0.56-0.97)
0.62 (0.45-0.87)
0.77 (0.60-0.99)
0.68 (0.50-0.92)
Odds Ratio(95% CI)
Favors Sacubitril/valsartan Favors enalapril
% o
f re
adm
issi
on
s af
ter
inve
stig
ato
r re
po
rted
HF
ho
spit
aliz
atio
n
Sacubitril/valsartan
Enalapril
30-day all-cause readmission
30-day HF readmission
60-day all-cause readmission
60-day HF readmission
Effect of sacubitril/valsartan treatment on readmission rates after investigator reported HF hospitalization
HF, heart failure
Desai et al., J Am Coll Cardiol. 2016;68(3):241-8


• Autorizzazione del Servizio Farmaceutico
• Scheda del MMG
• Piano terapeutico
• Ritiro in Farmacia ASP
• Controlli clinici ed ematochimici
SEMBRA FACILE….

Conclusioni I°
La gestione dello scompenso cardiaco è un atto chedeve prevedere la partecipazione sul territorio didiverse figure professionali (mediche e non-mediche).
Una attenta valutazione prognostica è la condizioneindispensabile per una corretta gestione delfollow-up del paziente con insufficienza cardiaca.
La differenzazione e l’individuazione di soggetti abasso ed alto rischio ci aiuterà nell’ottimizzazionedella terapia e nel ricorso oculato al ricoveroospedaliero responsabile principale dei costieconomici della IC.

Conclusioni II°
LA COMPETENZA dovrebbe essere ascoltata dagli
amministratori per ottimizzare risorse e percorsi
assistenziali.
Dovrebbero essere ascoltati gli operatori di prima linea,
che hanno un chiaro quadro di cio’ che accade sul
territorio e negli ospedali, per adattare le risorse alla
realta’ locale.
Si dovrebbe finalmente strutturare una rete per lo
scompenso cardiaco, in quanto non meno pericoloso
dell’IMA…

“………Avrò in sorte di essere il più curatodei malati. Ma nessuno può superare ilimiti prescritti dalla natura; le gambe gonfie non mi sostengono più nelle lunghe cerimonie di Roma;mi sento soffocare; ed ho sessant’anni”.
da “Memorie di Adriano”, M. Yourcenar

GRAZIE
DELLA
ATTENZIONE