candida in DM
4
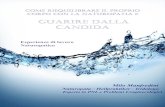
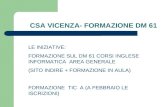
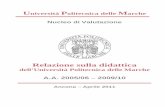
© JAP I VOL. 53 • JULY 2005 w w w.ja p i.or g 599 Original A rticle Prevalence of Candida in the Oral Cavity of Diabetic Subjects BV Kumar*, NS Padshetty**, KY Bai***, MS Rao+ Abstract Objective: Estimat ion of preva lence of Candida in the oral cavity of diabetic and non-diabetic subjec ts. Material and Method s: One hund red and three subjects of diabetes melli tus (49 Type 1 diabetes mellitus and 54 Type 2 diabetes melli tus) and one hu ndr ed non -diabetic subjec ts (control) were stud ied. Results: 41(83.67%) out of 49 Type 1 diabetes mellitus, 37(68.52%) out of 54 Type 2 diabetes mellitus and 27( 27%) out of 100 in non -diabet ic subjec ts w ere foun d to car ry Candida in their oral cavity. Colony Forming Unit (CFU) of Candida in the oral cavity ranking in group s was Type 1 diabetes mellitus > Type 2 diabetes mellitus > non-diabetic subjects. Conclusion: Colonization and carriage of Candida in the oral cavity was found to be higher in diabetic subjects than in non-diabetic subj ects. How ever anti-diabetic therapy and glyc aemic control in diabetes were found to bear n o relation with carriage of Candida in the or al cavity. © INTRODUCTION T he frequent occurrence of Candida infections in patients with d iabetes mell itus has been r ecogni zed for many years and oral candidiasis in particular is thought to be more prevalent among these individuals. 1 The carriage of Candida in the oral cavity of diabetic subjec ts is claimed to be higher. 2-4 The cand idal density has also been reported h igher in diabetes melli tus than in non-diabetic subjects, 2-3 not confirmed by other investigators. 5-7 The disparity in results may of course, be du e to difference in samp ling technique. 8 Hence the present study w as und ertaken to estimate the prevalenc e of c and idal carriage and their colonization in oral cavity of diabetic subjects and make an attempt to find the relationsh ip of oral carriage of Candida in diabetics with their degr ee of diabetic control and with an ti-diabeti c treatment. MATERIAL AND METHODS One hundred and three diabetic subjects and one hundred age and sex matched non-diabetic subjects participated in the present study with prior informed consent. Non-diabetic subj ects had fasting an d 2 hr. post- *Former Research Scholar, Gulbarga University and Lecturer, Dept. of Microbiology, MR M edical College; ** Professor, Dep t. of Microbiology, Gulbarga University; ***Former Reader and Incharge H.O.D. of Pedodontia, H.K.E.S. S.N.Institute of Dental Sciences and Research; +Professor, Dept. of Medicine, M. R. Medical College, Gulbarga. Received : 15.4.2002; Revised : 24.3.2005; Accepted : 31.5.2005 prandial blood sugar estimation. Out of 103 diabetic subjects 49 were Type 1 and 54 were Type 2. After a detailed history especiall y of symp toms su ggestive of any chronic complicati ons of diabetes like neuropa thy, cardiovascular complications or nephropathy and associ ated h ypertension, each su bj ect was su bj ected to a systematic physical examination particularly for the presence of severe anaemia, oedema, jaundice, lymphadenopathy, abdominal masses, cardiovascular, neurological and respiratory systems. Routine investigations l ike urine analysis, complete haemog ram , chest x-ray, ECG (in relevant cases) apart from fasting, 2 hr. post-pran dial blood sugar, glycos ylated haem oglobi n and in a few cases lipid profile were d one. B esides, where it was felt necessary abdominal ultrasound and blood testing for HIV were also done. The glyc aemic control was considered to be good if gl ycosyl ated h aemoglobin was less than 8%, values between 8-10 % were regar ded as fair control, and greater than 10% were seen as poor glycaemic control. 9 Individuals were excl ud ed from the stud y in ei ther grou ps if they had r ecei ved any an tibioti c / steroid therapy or had been using antiseptic mou thwash es or dentu re wearers. The diabetic subjec ts who had received both oral anti-diabetic therapy and insulin are also exc luded from the stud y. Each individual was supplied with a universal container containing 10ml. of sterile phosph ate bu ffer saline solution (PBS 0.1M pH 7.2), and was asked to rinse mou th in the p resence of clinic ian. After rinsing the mou th 60 seconds thorough ly, expell ed the m outh rinse in to a sterile container. Saliva samples were
-
Upload
drjamal1983 -
Category
Documents
-
view
219 -
download
0
Transcript of candida in DM

8/7/2019 candida in DM
http://slidepdf.com/reader/full/candida-in-dm 1/4

8/7/2019 candida in DM
http://slidepdf.com/reader/full/candida-in-dm 2/4

8/7/2019 candida in DM
http://slidepdf.com/reader/full/candida-in-dm 3/4

8/7/2019 candida in DM
http://slidepdf.com/reader/full/candida-in-dm 4/4