Lo screening dell'ipertrofia ventricolare sinistra (IVS) nell ...
Upload
centro-diagnostico-nardiCategory
view
32download
2
“ “ Arrythmogenic Right Arrythmogenic Right Ventricular Cardiomyopathy ”Ventricular Cardiomyopathy ”
An Electrophysiologic OverviewStefano Nardi, MD
AZIENDA OSPEDALIERA SANTA MARIA TERNIAZIENDA OSPEDALIERA SANTA MARIA TERNI DIVISIONE DI CARDIOLOGIA DIVISIONE DI CARDIOLOGIA
UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA LABORATORIO DI ELETTROFISIOLOGIA ED ELETTROSTIMOLAZIONE LABORATORIO DI ELETTROFISIOLOGIA ED ELETTROSTIMOLAZIONE
Arrhythmogenic Right Ventricular Cardiomyopathy
Sudden Cardiac Death in Children
• Primary electrical diseases– Congenital Long QT Syndrome– WPW with rapid antegrade conduction
• Cardiomyopathies– Hypertrophic– Dilated (idiopathic, post-chemo, etc.)– Arrhythmogenic right ventricular
cardiomyopathy• Structural abnormalities
– Anomalous coronary arteries– Severe aortic stenosis

Arrhythmogenic Right Ventricular Cardiomyopathy
Background
•“ARVC” proposed in 1977 by Fontaine
•Occurs in teenagers and young adults (>80% diagnosed by age 40)
–Rarely in early childhood •Italian study – ARVC = 20% of postmortem sudden deaths in patients < 35 years old
•Incidence 1:~5,000
Arrhythmogenic Right Ventricular Cardiomyopathy
Genetics
• Familial pattern in ~50%; Autosomal Dominant
• Variable penetrance• Multiple loci on chromosomes 14, 1, 10
• Requires thorough investigation of family history, suspicious symptoms, other unexplained sudden deaths
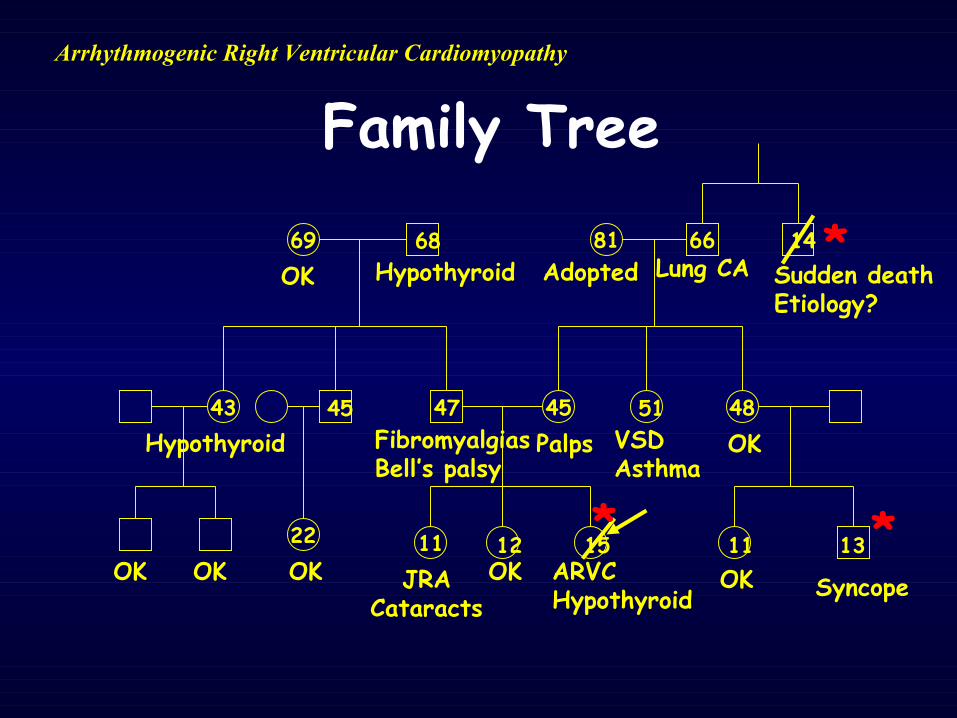
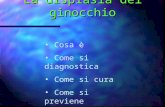
Arrhythmogenic Right Ventricular Cardiomyopathy
Family Tree
43
66
47
22
81
45 48
69
11 12 15JRA
CataractsSyncope
1311
Adopted Lung CA Sudden deathEtiology?
VSDAsthma
Hypothyroid FibromyalgiasBell’s palsy
Hypothyroid
45 51
1468
ARVCHypothyroid
OK OK OK OK
OK
Palps OK
OK
* *
*
Arrhythmogenic Right Ventricular Cardiomyopathy
Etiology?• Degeneration
– Myocyte death due to inherited metabolic or ultrastructural defect
– “Myocardial dystrophy”• Inflammatory/infectious/myocarditis
– Coxsackie-like RNA found in some cases• Apoptosis
– Programmed cell death• Transdifferentiation
– From myocardial cells to adipose tissue
Arrhythmogenic Right Ventricular Cardiomyopathy
Presentation
• Variable and non-specific symptoms– Palpitations– Shortness of breath; CHF-like symptoms
– Syncope• Many present with sudden death primarily
Arrhythmogenic Right Ventricular Cardiomyopathy
Natural history• “Concealed” phase - subtle RV changes;
+/- minor ventricular arrhythmias; rarely SD during competitive athletics
• “Overt electrical disorder” – overt RV structural/functional changes; symptomatic RV arrhythmias
• “Right heart failure” – global RV dysfunction w/ preserved LV function
• “Biventricular pump failure” – signif LV dysfunction
Arrhythmogenic Right Ventricular Cardiomyopathy
Physical Exam
• May be normal• Extra-systoles• Gallop rhythm, AV valve insufficiency (systolic murmur)
Arrhythmogenic Right Ventricular Cardiomyopathy
ECG
• Abnormal in 90%, though non-specific • T waves flattened, inverted (esp in V1-V3)
• Right precordial QRS prolongation • Epsilon waves (small amplitude potentials at start of ST segment – “intraventricular myocardial defect”)
• Signal averaging (SAECG)
Arrhythmogenic Right Ventricular Cardiomyopathy
Ventricular Arrhythmias• May be associated with palps, presyncope,
and syncope• Isolated PVC’s, sustained ventricular
tachycardia, or ventricular fibrillation leading to sudden cardiac arrest
• Usually LBBB (suggesting right sided ectopy), sometimes of multiple morphology
• Not specific for ARVC – rule out congenital heart disease – repaired TOF,
Ebstein anomaly, etc.– Idiopathic RVOT VT
Arrhythmogenic Right Ventricular Cardiomyopathy
Ventricular Arrhythmias
• Ventricular fibrillation in ARVC– Incidence unclear – Many cases discovered post-mortem– Most likely mechanism of sudden death
Arrhythmogenic Right Ventricular Cardiomyopathy
Echocardiography
• Hypokinetic, dilated right ventricle– Especially in RV outflow tract
• LV dilation if LV also involved
Arrhythmogenic Right Ventricular Cardiomyopathy
MRI
• The definitive test?• Requires experienced cardiac imaging specialist
• Can distinguish fat from muscle• Cine MRI helps qualitate free wall function
Arrhythmogenic Right Ventricular Cardiomyopathy
Cardiac Catheterization
• Right ventricular angiography– Dilated, poorly contractile RV free wall and RV outflow tract
• RV endomyocardial biopsy– Excessive fatty infiltration– Sporadic, typically involves epicardium first (ie. False negative sampling)
Arrhythmogenic Right Ventricular Cardiomyopathy
Treatment• Main objective is to prevent sudden
death• Primary vs. secondary prevention• Risk stratification
– Young age– Competitive sports– Malignant FHx– Signif RV disease or LV involvement– Syncope, – VT/VF
Arrhythmogenic Right Ventricular Cardiomyopathy
Treatment
• Restricted activities• Medic Alert bracelet/necklace• Medications
– Amiodarone, sotalol, beta-blockers• Catheter ablation• Implantable cardioverter-defibrillator (ICD)
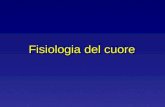
Arrhythmogenic Right Ventricular Cardiomyopathy
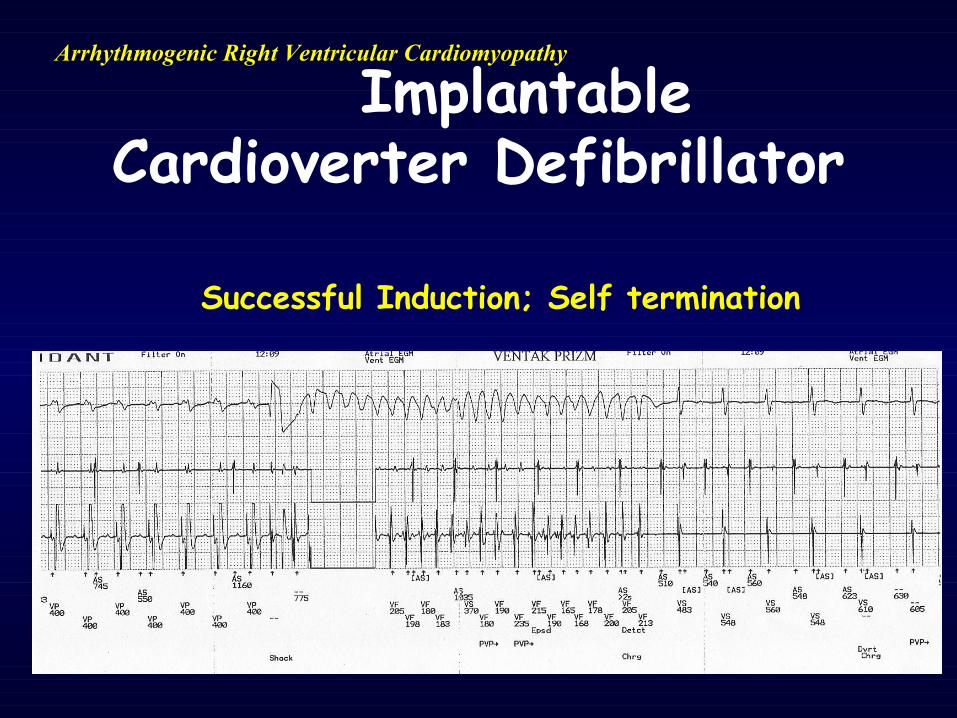
Implantable Cardioverter Defibrillator
Successful Induction; Self termination
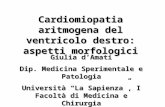
Arrhythmogenic Right Ventricular Cardiomyopathy
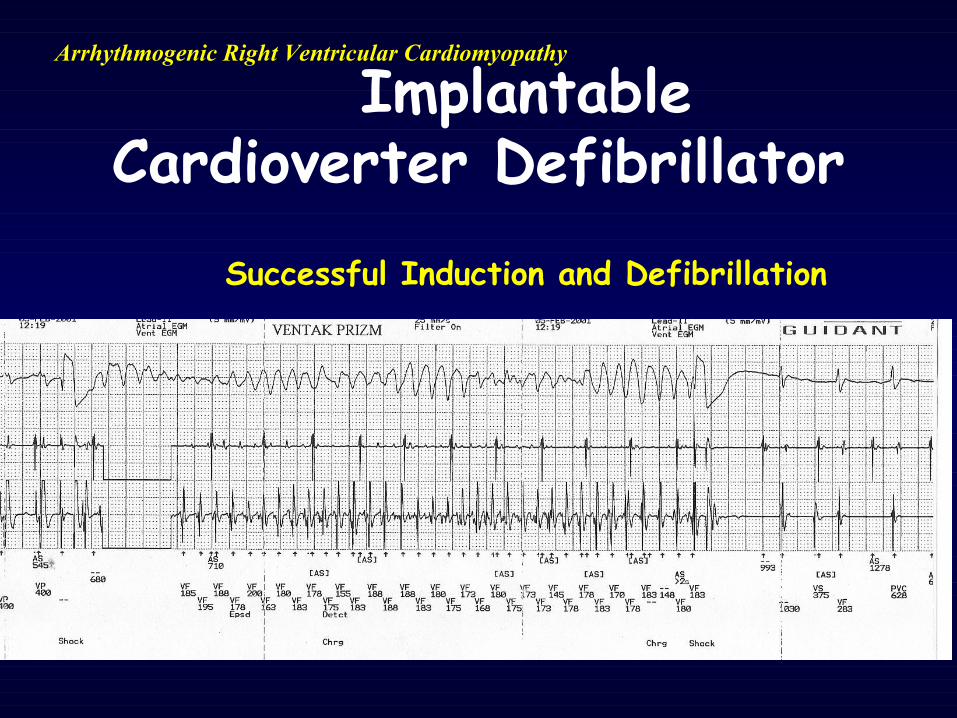
Implantable Cardioverter Defibrillator
Successful Induction and Defibrillation
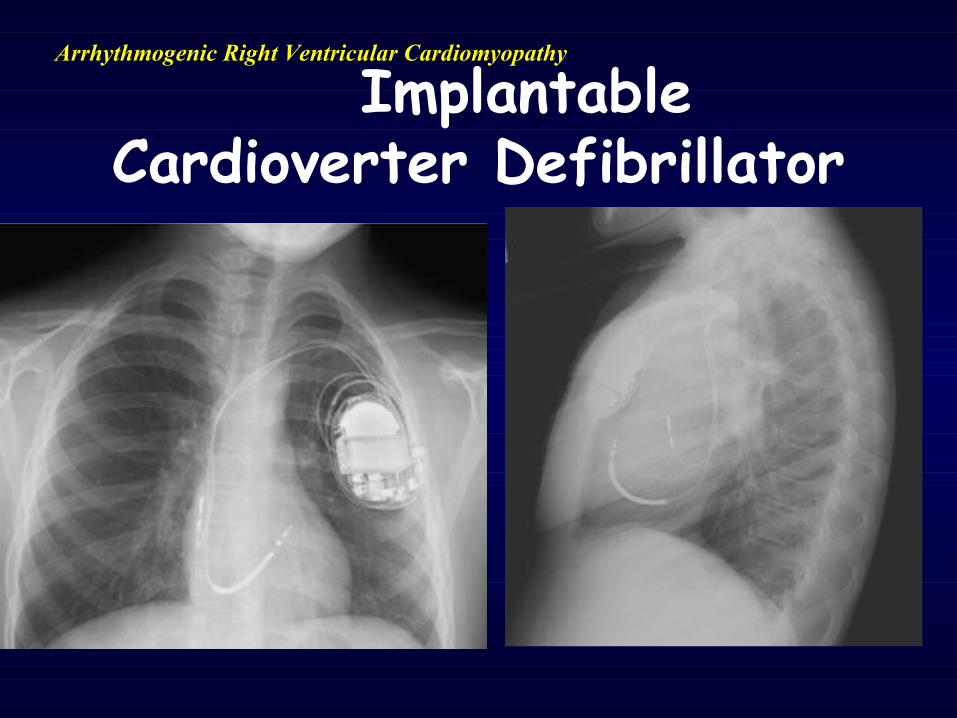
Arrhythmogenic Right Ventricular Cardiomyopathy
Implantable Cardioverter Defibrillator
Arrhythmogenic Right Ventricular Cardiomyopathy
Take Home Points
• Rare disorder, but increasing recognized as cause of malignant ventricular arrhythmias
• Sudden death can be initial presentation• Consider in young pts with arrhythmias
or unexplained cardiomyopathy• Management via suppression of
arrhythmias, AICD placement• Families need support!!