



Le lingue
Pagine
Legale

8/10/2019 Semiologia y Dg 2
1/21
Review Article
Diagnostic Terms for Pulpal Health and Disease States 109J! " #olume $%& 'um(er 1)& Decem(er )009
A
*dentif+ and Define All Diagnostic Terms for PulpalHealth and Disease States
,inda -. ,evin& DDS& PhD&/ Alan S. ,aw&DDS& PhD&
-.R. Holland& Sc& DS& PhD& 2ert !ndo&
2RS!&3
Paul #. A((ott& DSc& 4DS& 5RA2DS6!ndo7&8
and Ro(ert S. Roda& DDS& 4S
A(stract
*ntroduction: 2onsensus 2onference Su(committee )
was charged with the identification and definition of
all diagnostic terms for pulpal health and disease states
(+ using a s+stematic review of the literature. 4ethods:
!ight data(ases were searched& and numerous
widel+ recogni;ed endodontic te tions that can (e
identified in the dental pulp& diagnostic terms that can
(est represent pulpal health and disease& and metrics
used to arrive at such designations. Results and
2onclusions: n the (asis of the findings of this
in=uir+& specific diagnostic terms forpulpal health and
disease are suggested. *n addition& numerous areas
for further stud+ were identified. 6J !ndod
)009?$%:1@%B
1@%C7
e+ EordsDental pulp& diagnosis& metrics
5rom the /School of Dentistr+& Fniversit+ of'orth 2arolinaat 2hapel Hill& 2hapel Hill& 'orth 2arolina?
Private
Practice& ,aGe !lmo& 4innestoa?3School of Dentistr+&
Fniversit+ of 4ich> igan& Ann Ar(or& 4ichigan?8School of
Dentistr+& Fniversit+ of Eestern Australia& Perth& EA&Australia? and
a+lor2ollege of Dentistr+& Dallas& Tevid& Pu(4ed& Ee( of nowledge& 2ochrane ral Health -roup& !4AS!&S2PFS& -oogle Scholar& and 4edstor+. 'onB!nglish language citations andnonhuman studies were e!lsevier& St ,ouis& 4& )00@? Principles and Practice of !ndodontics&th ed& Tora(inead 4& Ealton R!& Saunders& Philadelphia& PA& )00M? !nc+clopediaof Pain& Schmidt R5& Eillis ED& Springer& erlin& -erman+& )00@? !ssential!ndodontol> og+: Prevention and Treatment of Apical Periodontitis& NrstaviG D&Pitt 5ord TR& lacGwell Pu(lishing&
8/10/2019 Semiologia y Dg 2
2/21
Review Article
110 ,evin et al. J!" #olume $%& 'um(er 1)& Decem(er )009
pain& moderate pain& and severe pain. The patientchooses the word that (est descri(es their
pain& and a num(er is assigned to this& depending onits ranGing in terms of intensit+.
'umeric rating scales are a list of num(ers& fore sponds to their pain intensit+.
8/10/2019 Semiologia y Dg 2
3/21
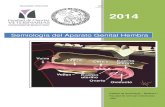
TA,! 1. Fse of Dolorimetr+ Techni=ue in (servations of Pulpal Pain
#er(al rating 'umeric rating #isual analog 2olor analog 2ali(rated 5inger Span 2ortical evoGedscales scales scales scales =uestionnaires Scale potentials
1@ $ 1@ ) ) $ %
#isual analog scales consist of a line with ) end points of no painLLand worst pain ever.LL The patient marGs a point on the line that relatesto the intensit+ of their pain. The distance of that point from nopainLListhe measure of pain intensit+.
2olor analog scales are used with children. A series of graded inintensit+ colors are anchored at each end (+ the terms no painLLandworstpain.LL
2ali(rated =uestionnaires should reall+(e cali(rated =uestion>naire (ecause there is onl+ one that has gained widespread acceptance&the 4c-ill Pain uestionnaire. This consists of )0 groups of descriptorsselected from the medical literature that descri(e the sensor+ =ualitiesof the pain& the affective =ualities of the pain& or are evaluativedescri(ingthe overall intensit+ of the e mined on the ranG values of the words. The 4c-ill Painuestionnairehas (een translated into at least 1@ languages and is ver+ widel+ used. *tsadvantage is that it allows measurement of the different components ofthe pain edimensional measure ofthe edimen>sional.
5inger span scaling has largel+ (een used in children (ecause itovercomes the comple sent a tin+LL hurt& and a somewhat wider distance ismediumLLhurt. Ehen the forefinger and thum( are moved as farapart aspossi(le&this is mostpossi(le hurt.LLThe span in each instance is measured.
2ortical evoGed potentials are components of an electroencepha>logram taGen while appl+ing a no
8/10/2019 Semiologia y Dg 2
4/21
ined the efficac+ of the various scales in descri(ing pulpal pain. Thisrepresents a significant deficit of Gnowledge in the area of pulpal
pain assessment. The most prevalent approach endodontists use toassess pulpal pain is an informal ver(al descriptor scale& withterms such as severe& intermittent& or spontaneous (eing widel+used. The visual analog scale has achieved wide acceptance in thee sion to num(ers. The scale is clinicall+ useful&
particularl+ with long> term pain& and serves as a valua(le tool for themonitoring and assess> ment of clinical interventions. 2ali(rated
=uestionnaires 6essentiall+ the 4c-ill Pain uestionnaire7 have ver+(road acceptance in man+ areas&(ut the+ would (e less appropriateand more time>consuming in the setting of the dental office thaneither ver(al descriptor or visual analog scales. The use of fingerspan and color analog scales is generall+ confined to ver+ +oungsu(ects and would (e of limited application in the dental office.Although electroencephalograph+ would (e an e
8/10/2019 Semiologia y Dg 2
5/21
8/10/2019 Semiologia y Dg 2
6/21
s+mptoms or pain. *rreversi(le inflammation of the pulp is produced (+carious e
8/10/2019 Semiologia y Dg 2
7/21
enhanced (lood suppl+ created (+ the open apices allows the immaturepulp to(etter resist (acterial invasion than a more mature pulp 6M1&M$7& and the opening through the carious lesion into the oralcavit+esta(lishes a pathwa+ for drainage of pulpal inflammator+ efloatingcells of the oral mucosa are seededLL onto the proliferating granuloma>tous tissue& resulting in a stratified s=uamous epithelium 6C7& andthe resultant lesion is rarel+ painful epathic in that the trigger for the metaplastic transformation ofnormal pulp cells into clastic ones is unGnown. Several h+potheseshave(eenproposed 6M& M%7& and it is possi(le that it might (e acom(ination of these that starts the resorptive process. The resorptionsometimes moves swiftl+ and then might (e followed (+ a time ofslower or no growth in the si;e of the lesion 6C7. *nternalresorption is generall+ painless and is usuall+ found clinicall+ throughroutine radiographic screening& when it appears generall+ as anovoid enlargement of the pulp space 6M@7 in which the original
(orders of the pulp space (ecome distorted or disappear altogether6M& M%& MC7. The lesion sta+s associ> ated with the root canal on
angled radiographs 6M& M%7. The tooth might respond to pulpsensi(ilit+ tests& (ut occasionall+ the tests might(e negative if there ispartial necrosis with the advancing resorptive lesion within theliving portion of the pulp tissue su(acent to the necrotic tissue6@%& M& M%7. *f perforation of the tooth structure has occurred andthe tissue in the pulp space is e lowingthe color of the underl+ing granulomatous tissue to (e visi(le?however& this might also (e due to undermining& su(epithelial e f+ing 6MM& M97. -enerall+& pulp fi(rosis or atroph+ isa histologic change that is not clinicall+ discerni(le unless the pulpspace is entered during the initial phases of root canal therap+& so itsvalue as a diagnostic term is =uestiona(le. Pulp calcification& however&is usuall+ clinicall+ detect> a(le (efore treatment and can directl+ affectthe prognosis of treatment& in that severel+ calcified teeth arepredisposed to tooth perforation during the search for canals 6907.This entit+ is also sometimes referred to as pulp canal o(literation 6@%7or calcific metamorphosis 691& 9)7& (ut (oth terms appear to (einaccurate (ecause the canal is rarel+ completel+ o(literated 69$7&and there is actuall+ no metamorphosisLL of the tooth& ust a
progressive deposition of dentin 6secondar+ or tertiar+7 resultingin radiographicall+ apparent shrinGage of thepulp
8/10/2019 Semiologia y Dg 2
8/21
canal space 6@7. 2alcification& per se& does not necessaril+ impl+that progressive inflammation of the pulp or pulp necrosis willoccur. *n fact& pulp necrosis is found in less than C of traumaticall+induced calcified pulps 697. ,astl+& the mineral content of thetertiar+ dentin represents more than ust calcium hence the term pulpcanal mineral> i;ation would (e a more accurate term.
Previousl+ *nitiated Treatment
ccasionall+& a tooth that has had endodontic therap+ previousl+started (ut not completed will present for diagnosis 6@7. These teeth
would have undergone previous pulpotom+ or pulpectom+& andthe histor+ and clinical e
8/10/2019 Semiologia y Dg 2
9/21
TA,! ). 2omprehensive 2linical Diagnostic S+stem
2linicall+ normal pulp: (ased on clinical eitis is defined in dictionaries as indicating inflammation of the tissuewhose name it is attached to& ie& the pulp 610C& 10M7.
Some teeth with pulpitis can (e clinicall+ managed via conservativemeans 6such as a simple restoration or a sedative dressing followed
(+ a restoration7& whereas others re=uire more radical treatment&which
implies removal of the pulp either as part of endodontic treatment orvia eversi(le pulpitis& although some dispute e ni;ed that in the disease continuum& partial necrosis cane
8/10/2019 Semiologia y Dg 2
10/21
most important aspect of this assessment is to determine whetherthe root canal s+stem is infected (ecause an infected canal willcause apical
8/10/2019 Semiologia y Dg 2
11/21
Review
Ar
ti
cl
e
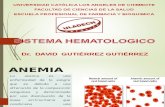
1@%0TA,! $. 2omparative Terminolog+ and 2lassifications of Pulp Diseases Fsed (+ #arious Authors and rgani;ations 6)B17
Eorld Healthrgani;ation
)Eeine
$*ngle
Selt;er and ender
%2ohen and
urns@
TronstadC
6'ote: 'ormalpulp not 6'ote: 'ormal pulp not Health+pulp 6'ote: 'ormalpulp not Eithin normal limits& Health+pulpmentioned7 mentioned7 mentioned7 normal pulp& calcific
metamorphosisPulpitis: initial Pulpitis: h+peralgesia Pulpitis: h+per>reactive Pulpitis: incipient form Pulpitis: reversi(le& Pulpitis: as+mptomatic
6h+peremia7& acute& 6reversi(lepulpitis7& pulpalgia& of chronicpulpitis& irreversi(le& pulpitis& s+mptomaticsuppurative 6pulpal h+persensitive h+persensitivit+& acute pulpitis& as+mptomatic& pulpitisa(scess7& chronic& dentin& h+peremia& h+peremia& acute chronicpartial irreversi(lepulpitis&chronic ulcerative& painful pulpitis& pulpalgia& incipient& pulpitis with partial h+perplastic pulpitis&chronic h+perplastic acute pulpalgia moderate& advanced& necrosis& chronic internal resorption&6pulpal pol+p7& other 6acute pulpitis7& chronicpulpalgia& totalpulpitis with canal calcification&unspecified pulpitis& chronicpulpalgia h+perplasticpulposis partial li=uefaction s+mptomaticpulpitis unspecified 6su(acute pulpitis7& necrosis& chronic irreversi(lepulpitis
nonpainful pulpitis& partialpulpitischronic ulcerative 6h+perplastic form7
pulpitis& chronicpulpitis 6no caries7&chronic h+perplasticpulpitis 6pulp pol+p7
'ecrosis of thepulp Pulp necrosis Pulp necrosis& Pulp necrosis 'ecrosis: partial& 'ecroticpulpli=uefaction& sicca complete
Pulp degenerations& Pulp degeneration& Pulp degeneration& Pulp degeneration&denticles&pulpal atroph+& d+strophic atrophic pulposis& atrophic pulp&calcification& pulpal calcification calcific pulposis d+strophicstones minerali;ation
A(normal hard tissue *nternal resorption *nternal resorptionformation inpulp&secondar+ orirregular dentin
American Association of!ndodontists-lossar+
MHart+
9Ealton and
Tora(inead10
-rossman11
2astellucci1)
StocG1$
ergenholt;1
'ormalpulp 'ormalpulp 6'ote: 'ormalpulp not 6'ote: 'ormalpulp not Health+pulp 'ormalpulp Pulpa sanamentioned7 mentioned7
Pulpitis: reversi(le Pulpitis: reversi(le Pulpitis: reversi(le H+peremia&pulpitides& Pulpitis: H+peremia& 2oncussedpulp& Pulpitispulpitis& irreversi(le pulpitis& irreversi(le pulpitis& irreversi(le acute pulpitis& pulpitis irreversi(le reversi(lepulpitis&pulpitis pulpitis pulpitis& h+perplastic chronic ulcerative irreversi(le pulpitis
pulpitis pulpitis& chronich+perplastic pulpitis
Pulp necrosis 'ecrosis Pulpal necrosis 'ecrosis 'ecrosis Pulpal necrosis 'ecrosis pulpaePulp calcification& internal Pulp degeneration& *nternal resorption
6intracanal7 resorption calcific& fi(rous&atrophic& internal
resorption
5rom A((ott P #& Uu 2. A clinical classification of the status of the pulp and the root canal s+stem. Aust Dent J )00C?%):61 Suppl7:S1CBS$1. Reproduced with permission from the Australian Dental Journal.
8/10/2019 Semiologia y Dg 2
12/21
Review Article
Diagnostic Terms for Pulpal Health and Disease States 11%J! " #olume $%& 'um(er 1)& Decem(er )009
periodontitis. *t is also important to assess the technical standard ofthe root canal filling (ecause this might determine whether furthertreat> ment is re=uired andIor feasi(le. Such determination is usuall+(ased on the radiographic appearance of the root canal filling.
*f there are no signs or s+mptoms to suggest that a root>filled toothis infected& then the management of such a tooth might (e simpl+ one ofo(servation and reassessment. *n other cases& the root filling might(e
udged as(eing technicall+ unsatisfactor+ and re=uiring replacement(efore further restoration of the tooth. Hence& specific diagnostic termsare re=uired for these situations. ecause the tooth is not infected& itwould (e appropriate to sa+ it is a root>filled tooth with no signsof infectionLL 6@%7. The phrase no signs of infection does notnecessaril+ impl+ that the root canal s+stem is not infected& (ut merel+that there isno clinical or radiographic evidence of it (eing infected at the time ofefilled toothLL6@%7.
Teethwith *ncomplete !ndodontic TreatmentPatients might present to dentists andIor endodontists with a
tooth that has had endodontic treatment commenced at some time inthepast& (ut the treatment was not completed. There are a widevariet+ ofpossi(le reasons wh+ the treatment might not have (eencompleted 6eg& patient did not return for treatment& patient wasreferred to a specialist for further treatment7? these might or mightnot (e relevant to the diagnosis in all cases. *t is important todistinguish these cases from other conditions outlined a(ove and
(elow (ecause their clinical management might (e different.*f a tooth has had endodontic treatment commenced (ut
not completed and it has no signs of the root canal s+stem (eing
infected&then the tooth could (e classified as having incompleteendodontictreatment with no signs of infectionLL6@%7. The phrase no signs ofinfection does not necessaril+impl+ that the root canal s+stem is notinfected& (ut merel+ that there is no clinical or radiographic evidenceof it (eing infected at the time of etion& untreated canal7 should (e listed as part of the diagnosis 6@%7.
Teethwith Degenerative andIor Ph+siologic 2hanges tothe Pulp
Dental pulps undergo ph+siologic changes ust liGe allother tissues in the (od+. Such changes are not pathologic innature& and the+ might (e difficult to diagnose clinicall+. ,iGewise&some pulps might undergo degenerative changes over time. *f there areclinical or radio> graphic manifestations of the degeneration& it isimportant to consider these conditions as part of the diagnostic
process and therefore to include them in a classification of theStatus of the Pulp and the Root 2anal S+stem.LL
T+pical conditions are pulp canal calcification& either part of thenormal aging process or it can (e an indication of long>standing
irrita>tion to the pulp. 2alcification is defined as a(normaldeposition of
calcium salts within tissueLL 61107. H+perplasia is defined as ana(normal increase in cells in a tissue or organ& e
8/10/2019 Semiologia y Dg 2
13/21
Review Article
11@ ,evin et al. J!" #olume $%& 'um(er 1)& Decem(er )009
tion& where(+ the (ulG of the tissue or organ is increasedLL 61117.This term can (e used when there has (een an overgrowth ofgranulation tissue originating from the pulp& and it might result in thedevelopment of a pulp pol+p. *t has (een suggested that theinflammation might (e limited to the pulp cham(er and that theapical pulp tissues might (e normal& e tion. ecause this condition isassociated with inflammation& the term should (e h+perplasticpulpitis.
Teethwith *nternal ResorptionThree forms of internal root resorption have (een reported&
although var+ing terminolog+ has(een used to descri(e them. Thedifferent forms of internal resorption re=uire different clinical manage>ment& and therefore it is essential that the+ (e differentiall+ diagnosedfrom one another. The proposed terminolog+ is internal surface resorp>tion& when ust minor areas of the root canal wall have(een resor(ed611)7. This resorption might(e self>limiting and might repair if thepulp is relativel+ health+ and if the irritating stimulus has (een removedfrom the tooth.
*nternal inflammator+ resorption occurs when an inflammator+response within the pulp 6ie& pulpitis7 leads to activation of dentinoclas>tic cells& which resor( the dentin walls of the root canal and then prog>ress through the dentin toward the cementum 611$7. This resorption is
(elieved to (e a result of the presence of microorganisms withinthecoronal part of the root canal that cause pulpitis in the pulp apical tothe resorptive area 611$7. Hence& a tooth with active internal inflamma>tor+ resorption will have some necrotic and infected pulp tissue as wellas some pulp tissue with irreversi(le pulpitis. *f the condition is definedas such& then there is no need to mention each of these conditions in thediagnosis. The dentinoclasts present in internal inflammator+resorp>tion will onl+ remain alive and active as long as there is a via(le(loodsuppl+ to the apical part of the pulp. *f this (lood suppl+ is lost& then theapical part of the pulp will necrose& and the dentinoclasts will alsodie. Thus& the internal inflammator+ resorption will no longer (e
active.T+picall+& the necrotic apical pulp tissue is then digested and removed(+ the microorganisms& and the entire canal will (ecome pulpless 6asdescri(ed a(ove7& resulting in apical periodontitis. nce apicalperio>dontitis is evident& it is highl+ liGel+ that the resorption is no longeractive& which will maGe clinical management somewhat easier andless involved. Hence& it is important to distinguish (etween active andnonactive states of internal inflammator+ resorption.
*nternal replacement resorption is a metaplastic t+pe of change tothe dental pulp in which the pulp first is replaced (+ (one& andthensu(se=uentl+ the dentin is replaced (+ (one 611$7. This conditionmust (e distinguished from the other ) t+pes of internal resorptionmentioned a(ove (ecause its clinical management is =uite different&ie& the tooth can (e e
8/10/2019 Semiologia y Dg 2
14/21
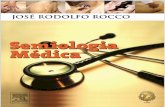
TA,! . Accurac+ of 2old Testing
Reference -old standard Sensitivit+ Specificit+ Positive predictive value 'egative predictive value
Selt;er et al 61)M7 Histolog+ 0.CM 0.M1 0.C 0.9Dummer et al 61$)7 Histolog+ 0.@M 0.C0 0.$$ 0.91Petersson et al 61$$7 2linical
a
0.M$ 0.9$ 0.M9 0.90!vans et al 61)17 2linical
(0.9) 0.M9 " "
-opiGrishna et al 61)07 2linicalc
0.M1 0.9) 0.9) 0.M1
a*n Petersson et al 619997& gold standard was determined (+ directpulp inspec tion.LL
(*n !vans et al 619997& pulpal status was confirmed(+ pulpectom+. LLc*n -opiGrishn a et al 6)00C7& pulpal status was evaluated (+ direct visual inspection.
agreed on definition for pulpal disease& which might or might not(e impractical or desira(le to use within clinical practice& is termedthe gold standard test or reference test. The results from such a goldstan> dard test for pulp diagnosis is used to compare with thediagnostic test (eing evaluated for the determination of testing accurac+.Studies as> sessing diagnostic accurac+ for pulpal disease testinghave used ) differentgold standard tests: a clinicall+ derived measure6eg& presence of necrotic tissue on accessing a tooth would indicatethat the tooth was nonvital7 and a histologicall+derived measure 6eg&on e ular changes& metrics used toesta(lish a perirad icular diagnosis might aid in the determination of a
pulpal diagnosis. 5or e
8/10/2019 Semiologia y Dg 2
15/21
TA,! @. Accurac+ of !lectric Pulp Testing
Reference -old standard Sensitivit+ Specificit+ Positive predictive value 'egative predictive value
Selt;er et al 61)M7 Histolog+ 0.9M " " "Petersson et al 61$$7 2linical
a
0.C) 0.9$ 0.MM 0.M!vans et al 61)17 2linical
(0.MC 0.9@
-opiGrishna et al 61)07 2linicalc
0.C1 0.9) 0.91 0.C
a*n Petersson et al 619997& gold standard was determined (+ directpulp inspection.LL
(*n !vans et al 619997& pulpal status was confirmed(+ pulpectom+. LL
c*n -opiGrishn a et al 6)00C7& pulpal status was evaluated (+ direct visual inspection.
!vans et al 61)17 reported that the presence of esion& and histor+ of pain were all found to have a high specificit+60.9C or (etter7 (ut low sensitivit+ 60.9 or lower7 for nonvitalit+.However& the authors failed to disclose the clinical criteria that wereused for assessment of these characteristics& maGing it impossi(le tovalidate their findings. A clinical finding of carious pulp e
8/10/2019 Semiologia y Dg 2
16/21
a*n -opiGrishn a et al 6)00C7& pulpal status was evaluated (+ direct visual inspection.
8/10/2019 Semiologia y Dg 2
17/21
TA,! M. Accurac+ of ,aser Doppler 5lowmetr+
Reference -old standard Sensitivit+ Specificit+ Positive predictive value 'egative predictive value
!vans et al 61)17 2linicala 1.0 1.0 " "
a*n !vans et al 619997& pulpal status was confirmed(+ pulpect om+.LL
determine when the pulpal inflammation is irreversi(le. The a(ilit+ to
determine when inflammation of the pulp has(ecome irreversi(lewould& therefore& guide the pract itioner and patient in treatmentchoices 6ie& nonsurgical root canal treatment vs e =uent necrosis & infection& and apicalperiodontitis.
DiscussionSu(=uestion O%: Ehat -aps in nowledge Remain forDeveloping and #alidating 4etrics and the ResultingPulpal Diagnoses
*n the area of clinical =uantification of pulpal pain& it was o(servedthat the maorit+ of studies were performed in e ical setting. #er(al rating scales& numeric rating scales& visualanalog scales& color analog scales& cali(rated =uestionnaires& andfinger span scaling were reviewed in the conte
nolog+& clinical classifications are the most appropriate. The clinicall+normal pulp is that pulp that is free from s+mptoms and vital. *nflam>mation of the pulp orpulpitis is a(road categor+ that can (e furtherdivided into reversi(le or irreversi(le& depending on the degree andcharacter of presenting s+mptoms. The demarcation is significant
(ecause endodontic intervention is recommended for the latter. These) categories can (e further divided on the (asis of s+mptoms or thelacG thereof. As+mptomatic irreversi(le pulpitis and s+mptomaticirrevers> i(le pulpitis have different presentations (ut the sametherapeuticoutcome. Presuma(l+ ever+ tooth with deca+& minor trauma& or peri>odontal disease has as+mptomatic reversi(le pulpitis. 4inor s+mptomsof sweet or thermal sensitivit+ represent s+mptomatic reversi(le
pulpitis.
Pulp necrosis is characteri;ed (+ necrosis of thepulp tissue. Totalnecrosis is the most easil+ diagnosed entit+& whereas partial necrosiscan (e the most difficult. H+perplastic pulpitis is a rare condition usuall+descri(ed in immature teeth with gross pulpal etor+ mediators to resor( dentin. Although painless& it can threatentoothretention if left unchecGed. Pulp calcification is the result of degenera>tive changes in the dentalpulp& with efilled tooth without signs of infection Root>filled tooth with signs of infection
*ncomplete endodontic treatment without signs of infection *ncomplete endodontic treatment with signs of infection Pulp canal minerali;ation
H+perplastic pulpitis
*nternal inflammator+ resorption 6active or inactive7 *nternal surface resorption
The su(committee recogni;es that there are other =ualifierssuch as the perceived presence or a(sence of infection 6ie& necrotic
pulp with infection7. This is not alwa+s easil+ determined clinicall+. *tis recom> mended as a point of discussion in terms of adopting it as
part of termi> nolog+. *t should (e emphasi;ed that levels of evidence inthe literature supporting the use of specific clinical diagnosticterminolog+ are gener> all+ ver+ low& in that the classification schemesappear to (e mainl+ the opinions of the various authors who providelogical arguments for their choices in developing nomenclature on the
(asis of studies with levels of evidence rarel+ eopment of sensitivit+& specificit+& positive predictive values& and negative
predictive values (+ esta(lishing a gold standard. The identification of(iologic marGers for reversi(le and irreversi(le pulpal inflammationwill (e of immense value in determining the need for endodonticinter>vention and the prevention of apical periodontitis.
TA,! 9. A(normal Response to 2old Testing and *rreversi(le Pulpitis
Reference -old standardLL Sensitivit+ Specificit+ Positive predictive value 'egative predictive value
8/10/2019 Semiologia y Dg 2
18/21
Selt;er et al 61)M7 Histolog+ 0.1 0.C@ 0.$ 0.M1Dummer et al 61$)7 Histolog+ 0.@$ 0.M0 0.M 0.MM-arfunGle et al 61197 Histolog+ 0.%C " " "
5rom H+man JJ& 2ohen 4. The predictive value of endodontic diagnostic tests. ral Surg ral 4ed ral Pathol 19M?%M:$$B@.
8/10/2019 Semiologia y Dg 2
19/21
TA,! 10. 4etrics for pulpal diagnosis 6and specificall+ reversi(le versusirreversi(le pulpitis7 on the (asis of histor+ of the presenting s+mptoms
Reversi(le pulpitis *rreversi(le pulpitis
Sensitivit+ to mild discomfort Pain might(e a(sent orpresent
1C. de Pa; #illanueva ,!2. 5uso(acterium nucleatum in endodontic flare>ups. ralSurg ral 4ed ral Pathol ral Radiol !ndod )00)?9$:1C9BM$.
1M. DoroschaG A4& owles ER& Hargreaves 4. !valuation of the com(ination offlur> (iprofen and tramadol for management of endodontic pain. J !ndod1999?)%:@@0B$.
19. !hrmann !H& 4esser HH& 2larG R4. 5lare>ups in endodontics and their relation>Short duration or shooting
sensation
Histor+ of pain is usuall+given
ship to various medicaments. Aus !ndod J )00C?$$:119B$0.
)0. Hsiao>Eu -E& Susarla S4& Ehite RR. Fse of the cold test as a measure ofpulpal
'ot severe Pain is often moderate tosevere
anesthesia during endodontic therap+: a randomi;ed& (linded&place(o> controlled
clinical trial. J !ndod )00C?$$:0@B10.*nfre=uent episodes of
discomfort
Seldom hurts to (ite unless
tooth also fractured orrestoration is loose andocclusion is affected
2ould result in irreversi(lepulpitis if source notremoved
S+mptoms usuall+ su(side
immediatel+ after removal
if cause
Pain is often spontaneous
Pain is increasing infre=uenc+& often to thepoint of (eing continuous
Pain usuall+ lingers& especiall+with increasing episodes
Patient often re=uires some
t+pe of analgesic
4ight(e a(le to identif+specific or multiple stimuli
Pain radiates or is diffuse or
might(e locali;ed
)1. emppainen P& Ealtimo A& Ealtimo T& ononen 4& Pertovaara A. Differentialeffects of notar+ hospital. J Dent )00@?$:@$%B0.
@. 2oda & TanaGa A& Jaco(son R2& Donaldson -& 2hapman 2R. H+dromorphoneanalgesia after intravenous (olus administration. Pain 199C?C1:1BM.
C. 2oda A& Hill H5& Schaffer R,& ,uger TJ& Jaco(son R2& 2hapman 2R. !nhance>ment of morphine analgesia (+ fenfluramine in su(ects receiving tailored opioidinfusions. Pain 199$?%):M%B91.
M. 5alace DA& Reid & Ra+ens 4. The influence of deep 6odontogenic7pain inten>sit+& =ualit+& and duration on the incidence and characteristics of referred oro>facial pain. J rofac Pain 199@?10:)$)B9.
9. 5ran;en -& Ahl=uist 4,. The intensive aspect of information processing in theintradental A>delta s+stem in man: aps+choph+siological anal+sis of sharp dentalpain. ehav rain Res 19M9?$$:1B11.
10. -angarosaSr ,P& 2iarlone A!& 'eaverth !J& Johnston 2A& Snowden JD&
Thompson E. Fse of ver(al descriptors& thermal scores and electrical pulptesting aspredictors of tooth pain (efore and after application of (en;ocainegels into cavities of teeth with pulpitis. Anesth Prog 19M9?$@:)C)B%.
11. lages F& Fluso+ & ianifard S& Eehr(ein H. Dental trait antip intraosseous inection in patients with irreversi(le pulpitis. J!ndod )00$?)9:C)BM.
1%. wat; 2& han AA& Schindler E-& Schwart; SA& eiser & Hargreaves 4. Theincidence of mechanical allod+nia in patients with irreversi(le pulpitis. J !ndod)00C?$$:%%)B@.
1@. lement E& 4edert HA& Arndt J. 'al(uphine does not act analgeticall+ in electricalpainful tooth pulp stimulation in man. Pain 199)?M:)@9BC.
the effectiveness of incisiveImental nerve(locG: a randomi; ed& controlled& dou(le>(lind stud+ in adult volunteers. J !ndod )00C?$$:119B%.
)M. ;tas '& Flusu T& odur H& Dogan 2. The wand inpulp therap+: an alternative toinferior alveolar nerve (locG. uint *nt )00%?$@:%%9B@.
)9. 'aidu S& ,oughlin P& 2oldwell S!& 'o onan 2J& 4 ilgrom P. A randomi;ed controlledtrial comparing mandi(ular local anesthesia techni=ues in children receivingnitrous oogenc+ department. Pediatrics )00)?110:e$$.
$$. Ahl=uist 4& 5ran;en & 2offe+ J& Pashle+ D . Dental pain evoGed (+ h+drostaticpres>
sures applied to enociceptiveneurons in trigeminal su(nucleus cauda lis 6medullar+ dorsal horn7 and itsimplications for referred pain. Pain 19M@?)C:)19B$%.
$@. 4ellor A2& Dorman 4,& -irdler '4. The use of an intra>oral inection of Getorolacin the treatment of irreversi(le pulpitis. *ntl !ndod J )00%?$M:CM9B9).
$C. Ahl=uist 4,& 5ran;en -. !ncoding of the su(ective intensit+ of sharp dental pain.!ndod Dent Trauma 199?10:1%$B@@.
$M. 'ewto n JT& ucG DJ. A n
8/10/2019 Semiologia y Dg 2
20/21
M. Selt;er S& ender *. The dental pulp: (iologic considerations in dentalproce> dures. $rd ed. Philadelphia: ,ippincott? 19M.
9. erman ,H& Hartwell -R. Diagnosis. *n: 2ohen S& Hargreaves 4& eds. Pathwa+s ofthe pulp. 9th ed. St ,ouis: 4os(+>!lsevier? )00@:)B$9.
%0. -licGman -'& 4icGel A& ,evin ,-& 5ouad A5& Johnson ET. -lossar+ of endodonticterms. Cth ed. 2hicago: American Association of !ndodontists? )00$.
%1. 4orse DR& Selt;er S& Sinai *& iron -. !ndodontic classification. J Am Dent Assoc19CC?9:@M%B9.
%). Tora(inead 4. Pulp and periradicular pathosis. *n: Ealton R!& Tora(inead 4&eds. Principles and practice of endodontics. $rd ed. Philadelphia: E Saunders?
)00):$BC.%$. Sigurdsson A. 2linical manifestations and diagnosis. *n: NrstaviG D& Pitt>5ord TR&
eds. !ssential endodontolog+. )nd ed.
i(le pulpitis: treatment and prognosis. J !ndod )00C?$$:10%BC.@M. Trow(ridge H. Histolog+ of pulpal inflammation. *n: Hargreaves 4& -oodis H!&
eds. Selt;er and enderLs dental pulp. 2hicago: uintessence? )00):))CB%.@9. Reeves R& Stanle+ HR. The relationship of(acterial penetrat ion and p ulpal pathosis
in carious teeth. ral Surg ral 4ed ral Pathol 19@@?)):%9B@%.C0. 4ichaelson P,& Holland -R. *spulpitis painful *nt !ndod J )00)?$%:M)9B$).C1. -oodis H!& owles ER& Hargreaves 4. Prostaglandin !) enhances (rad+>
Ginin>evoGed i2-RP release in (ovine dental pulp. J Dent Res )000?C9:1@0BC.
C). owles ER& Eithrow J2& ,epinsGi A4& Hargreaves 4. Tissue levels of immunore>active su(stance P are increased inpatients with irreversi( le pulpitis. J !ndod)00$?)9:)@%BC.
C$. Hargreaves 4. Pain mechanisms of the pulpodentin completomatolog+ of acute dental pain. ral Surg ral 4ed ral Pathol 19M%?%9:)9CB$01.
CM. 4esser HH. Permanent restorations and the dental pulp. *n: Hargreaves 4&-oodis H!& eds. Selt;er and enderLs dental pulp. 2hicago: uintessence ooGs?)00):$%B@9.
C9. Di!lsevier? )00@:@10B9.
M@. Andreasen J& Andreasen 54. Telence of reactive and ph+siologic sclerotic dentin& reparative dentin and dead tracts(eneath various t+pes of dental lesions according to tooth surface and age. J ralPathol 19M$?1):)%CBM9.
M9. Pashle+ DH& ,iewehr 5R. Structure and functions of the dentin>pulp comple!lsev>ier? )00@:@0B%1$.
90. 'ewton 2E& 2oil J4. -eriatric endodontics. *n: 2ohen S& Hargreaves 4& eds. Path>wa+s of the pulp. 9th ed. St ,ouis: 4os(+>!lsevier? )00@:MM$B91C.
91. Schindler E-& -ullicGson D2. Rationale for the management of calcific metamor>
phosis secondar+ to traumatic inuries. J !ndod 19MM?1:0MB1).9). Smith JE. 2alcific metamorphosis: a treatment dilemma. ral Surg ral 4ed ral
Pathol 19M)?%:1B.9$. u+G J& Ealton R!. 2omparison of the radiographic appearance of root canal si;e
to its actual diameter. J !ndod 1990?1@:%)MB$$.9. Holcom( J& -regor+ E Jr.. 2alcific metamorphosis of the pulp: its incidence and
treatment. ral Surg ral 4ed ral Pathol 19@C?):M)%B$0.9%. 2veG 4. Treatment of non>vital permanent incisors with calcium h+droEe(sterLs medical dictionar+. 4erriam>Ee(ster& *nc. Availa(le at: http: IId ict ionar + .ref erence .c o mI(rowseInecro s is. Ac>cessed: 4a+ 0& )00M.
110. 2alcification. Dictionar+.com. The American Heritage StedmanLs medical dictio>nar+. Houghton 4ifflin 2ompan+. Availa(le at: http:IId ictiona r+.reference.comI
(rowseIcalc ification. Accessed 4a+ 0& )00M.
http://dictionary.reference.com/browse/itishttp://dictionary.reference.com/browse/itishttp://dictionary.reference.com/browse/pulpitishttp://dictionary.reference.com/browse/pulpitishttp://dictionary.reference.com/browse/pulpitishttp://dictionary.reference.com/browse/necrosishttp://dictionary.reference.com/browse/necrosishttp://dictionary.reference.com/browse/calcificationhttp://dictionary.reference.com/browse/calcificationhttp://dictionary.reference.com/browse/calcificationhttp://dictionary.reference.com/browse/calcificationhttp://dictionary.reference.com/browse/itishttp://dictionary.reference.com/browse/pulpitishttp://dictionary.reference.com/browse/necrosishttp://dictionary.reference.com/browse/calcificationhttp://dictionary.reference.com/browse/calcification8/10/2019 Semiologia y Dg 2
21/21
111. H+perplasia. Dictionar+.com. The American Heritage StedmanLs medical dictio>nar+. Houghton 4ifflin 2ompan+. Availa(le at: http :IId ictionar +.referen ce.c omI(rowseIh+perpla s ia. Accessed 4a+ 0& )00M.
11). Andreasen 54& Andreasen J& 2veG 4. Root fractures. *n: Andreasen J&Andreasen 54& Andersson ,& eds. Te