UPDATE SULLA TERAPIA DELLA CORIORETINOPATIA SIEROSA … parte 1.pdf · 2017-06-03 · UPDATE SULLA...
16
UPDATE SULLA TERAPIA DELLA CORIORETINOPATIA SIEROSA CENTRALE Giacomo Savini Studio Oculistico d’Azeglio - Bologna Fondazione G.B. Bietti - Roma APERITIVO AL D’AZEGLIO
Transcript of UPDATE SULLA TERAPIA DELLA CORIORETINOPATIA SIEROSA … parte 1.pdf · 2017-06-03 · UPDATE SULLA...

UPDATE SULLA TERAPIA DELLA CORIORETINOPATIA SIEROSA CENTRALE
Giacomo Savini
Studio Oculistico d’Azeglio - BolognaFondazione G.B. Bietti - Roma
Caro CollegaSiamo lieti di invitarti ad una serie di incontri che si terranno mensilmente presso lo Studio Oculistico d’Azeglio con la finalità di aggiornarci in maniera continuativa su diversi campi di interesse oculistico.L’obiettivo è quello di utilizzare il singolo caso clinico come metodo di approfondimento degli argomenti di comune riscontro nella pratica clinica quotidiana. Gli incontri saranno focalizzati su tre aree d’interesse: chirurgia refrattiva e della cataratta, retina medica e chirurgica, glaucoma e neuro-oftalmologia.Saranno incontri informali dove lasceremo ampio spazio alla discussione finale e alla presentazione di casi cinici anche da parte dei partecipanti.Siete tutti invitati ad esporre la vostra esperienza e i vostri casi.
Piero Barboni Giacomo SaviniMichele Carbonelli
Via d’Azeglio 5 - 40123 Bologna - Tel. 051-6493203 Fax [email protected] www.studiodazeglio.itISCRIZIONI PER EMAIL O TELEFONO
APERITIVO AL D’AZEGLIO
STUDIO OCULISTICO D’AZEGLIO
15 FebbraioRetina medica
Update sulla terapia della corioretinopatia sierosa centrale
21 MarzoChirurgia refrattiva
FemtoLASIK: storia di un successo annunciato
11 AprileNeuro-oftalmologia
Edema e pseudoedema del disco ottico
20 GiugnoRetina medica e chirurgica
Iniezioni intravitreali: discussione di casi clinici
17 OttobreRetina chirurgica
Chirurgia vitreoretinica mini-invasiva: discussione di casi clinici
5 DicembreGlaucoma
Diagnosi precoce del glaucoma. Anche la chirurgia deve essere precoce?
CALENDARIO INCONTRI

Terapia farmacologica
Valutazione sistemica
Valutazione psichiatrica
Terapia laser
Novità

Terapia farmacologica
BevacizumabFinasterideRifampicinaMifepristoneKetoconazoloAspirina
Novità

Terapia laser
PDTPDT a metà fluenzaPDT a metà dose
Laser micropulsato sottosoglia
Novità

BEVACIZUMAB (AVASTIN)
La coroide è ispessita nella corio-retinopatia sierosa centrale
Jirattanasopa - Ophthalmol 2012

RazionaleSe l’Avastin attraversa l’EPR, potrebbe indurre vasocostrizione della coroide
BEVACIZUMAB (AVASTIN)
Dopo 1 iniezione di Avastin:Ridotta permeabilità della coroide (ICGA) (Lim et al. Retina 2010)

DubbiNon esiste la prova di un aumento del VGEF nella CRSCSolo 2 studi con gruppo di controllo (e con risultati dubbi...)
BEVACIZUMAB (AVASTIN)

Risultati - CRSC recidivanteScomparsa liquido in 4/5 pz con sintomi >3 mesi e storia di CRSC recidivante, senza precedente terapia laserMiglioramento AV in 5/6 pzRecidiva entro 6 mesi in 4/6 pz
BEVACIZUMAB (AVASTIN)
Lim et al - Retina 2010

Risultati - CRSC recidivanteRisultati peggiori vs Laser a diodi micropulsato sottosogliaOutcome migliore rispetto a controllo
BEVACIZUMAB (AVASTIN)
Subthreshold diodelaser micropulsephotocoagulationversus intravitrealinjections ofbevacizumab inthe treatment ofcentral serouschorioretinopathy
MJ Koss, I Beger and FH Koch
Abstract
Purpose To evaluate the treatment of central
serous chorioretinopathy (CSC) with either
subthreshold diode laser MicroPulse (SDM)
or intravitreal bevacizumab (BCZ).
Methods This comparative, controlled,
prospective study conducted over a period of
10 months examined 52 eyes of 52 patientswith (a) treatment with SDM at the active
leakage site guided by fluorescein
angiography (FA) (n! 16 eyes), (b) intravitreal
injection of 1.25 mg BCZ (n! 10 eyes), or
(c) observation (n! 26 eyes). Outcome
measures included changes in retinal pigment
epithelium (RPE) leakage at FA, central macular
thickness (CMT), best-corrected visual acuity(BCVA), and 101 macular perimetry.
Results At the end of the study, there was
12.5% persistent leakage in the SDM,
compared with 60% in the BCZ and 92% in the
control group. Mean CMT decreased by 94 lm
in the SDM, 38 lm in the BCZ, and did not
change in the control group. Mean BCVA
improved more than 6 early treatment ofdiabetic retinopathy study letters in the SDM,
decreased by one letter in the BCZ, and by two
letters in the control group. In the SDM group,
mean perimetric deficit improved by 1.5
decibels and corrected lost variance by 2.6. In
the BCZ, it improved by 0.6, and in the control
group by 0.5. Retreatment was required in 7/16
eyes of the SDM group (43.75%), and in 5/10eyes of the BCZ group (50%).
Conclusion SDM photocoagulation was
superior to intravitreal injections of 1.25 mg
BCZ in the treatment of CSC, which resultedin enhanced visual acuity and macular
perimetry.
Eye (2012) 26, 307–314; doi:10.1038/eye.2011.282;published online 11 November 2011
Keywords: central serous chorioretinopathy;micropulse laser, subthresholdphotocoagulation; bevacizumab
Introduction
Central serous chorioretinopathy (CSC) is anidiopathic disorder characterized by neuro-epithelial serous detachment, with or withoutconcomitant pigment epithelium detachment(PED) and decompensated retinal pigmentepithelium (RPE) associated with one or morefocal active leakage sites (ALS) at the level of theRPE (‘smoke-stack’ on fluorescein angiography(FA)). The underlying pathogenesis of CSC isnot thoroughly understood.1 Abnormalitiesof choroidal circulation (most likelychoriocapillaris) at indocyanine greenangiography (ICGA) precede disintegrationof the RPE.2 CSC may be associated withextraocular conditions, including type Apersonality, organ transplantation, use ofsteroids, systemic lupus erythematous,Cushing’s disease, and other systemic factors.3–6
Blurred vision is perceived typically by patientsas a dark spot in the center of the visual fieldwith associated hyperopic shift, micropsia, andmetamorphopsia, caused by anterior
Received: 5 September2011Accepted in revised form:16 September 2011Published online: 11November 2011
Unit of Vitreo-RetinalSurgery, Department ofOphthalmology, GoetheUniversity, Frankfurtam Main, Germany
Correspondence: MJ Koss,Unit of Vitreo-RetinalSurgery, Department ofOphthalmology, Klinikumder Johann WolfgangGoethe-UniversitatFrankfurt/Main, TheodorStern Kai 7 (Haus 7c), 60590Frankfurt am Main,GermanyTel: "49 69 6301 5649;Fax: " 49 69 6301 5621.E-mail: [email protected]
Eye (2012) 26, 307–314& 2012 Macmillan Publishers Limited All rights reserved 0950-222X/12
www.nature.com/eye
CL
INIC
AL
ST
UD
Y

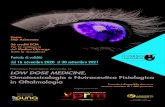
Risultati - CRSC acutaPiù rapida scomparsa del liquido (13 occhi / 22 pz) rispetto a gruppo di controllo (9 occhi)Le differenze sono statisticamente significati-ve, ma clinicamente...
BEVACIZUMAB (AVASTIN)
Avastin (2 mg) Control
Mean BCVA at baseline 0.39 +/-0.16 0.25 +/-0.17
Mean BCVA 6-month 0.73 +/-0.17 0.67 +/-0.13OCT baseline 414 +/-103 510 +/-81OCT 3-month 256 +/-85 336 +/-128OCT 6-month 198 +/-30 206 +/-20
Aydin - J Ocul Pharmacol Ther 2012

Pillola del giorno dopo
RazionaleAntagonista dei glucocorticoidi
MIFEPRISTONE (RU486)

Un solo studio...
MIFEPRISTONE (RU486)
ORAL MIFEPRISTONE FOR CHRONICCENTRAL SEROUSCHORIORETINOPATHY
JARED S. NIELSEN, MD,*† LEE M. JAMPOL, MD*
Background: Chronic central serous chorioretinopathy (CCSC) can result in permanentloss of vision. Unfortunately, many cases of CCSC are not eligible or do not respond totreatment with thermal laser or photodynamic therapy. Glucocorticoids have beenimplicated in the pathogenesis of central serous chorioretinopathy. Mifepristone, an oralglucocorticoid receptor antagonist, may be helpful in cases of CCSC.
Methods: Mifepristone 200 mg was administered orally to 16 CCSC subjects in2 separate protocols for up to 12 weeks. Visual acuity, examination, angiography, opticalcoherence tomography, and liver function were monitored during the treatment period.
Results: Favorable response to oral mifepristone was seen in CCSC patients with sevensubjects gaining five or more letters of vision and seven subjects having improved opticalcoherence tomography findings. Treatment was well tolerated without serious adverseeffects.
Conclusion: Systemic glucocorticoid receptor antagonism with daily oral mifepristonedoes have a beneficial effect in treating some cases of CCSC. Further study is warranted.
RETINA 31:1928–1936, 2011
Central serous chorioretinopathy (CSC) is typicallya self-limited condition with favorable clinical
outcomes. A minority of cases progress to chroniccentral serous chorioretinopathy (CCSC) an oftenrecurrent, progressive, and persistent variant that canaffect both eyes and results in permanent vision lossfrom retinal thinning with retinal pigment epithelium(RPE) atrophy.1 Classic CSC is manifest as focal RPEleakage, often with a pigment epithelial detachmentand accumulation of subretinal fluid. Chronic casesusually demonstrate diffuse leakage, intraretinal cysticchanges, with extensive RPE and retinal atrophy, andmay show no or very little subretinal fluid. Choroidalhyperpermeablity on indocyanine green (ICG) angi-ography2 and thickened choroid best seen on enhanceddepth imaging spectral domain optical coherencetomography (EDI-sdOCT)3 are typical CSC findings.The precise mechanism underlying the development
of CSC remains unknown. Primary dysfunction in
CSC may reside in the choroid. Hyperpermeablechoriocapillaris drives leakage through compromisedRPE, leading to secondary retinal changes over time.Glucocorticoids (GCs) have been implicated in thepathogenesis of CSC,4–6 and it is reasonable to surmisethat anti-GC therapy may be helpful in its treatment.4
Mifepristone (Mifeprex; Danco Laboratories, NewYork, NY), more popularly known as RU-486, is anorally bioavailable, high-affinity, GC receptor antag-onist.7,8 It is also a potent antiprogesterone agent and isFood and Drug Administration approved for use as anabortifacient when coadministered with a prostaglan-din agent. Mifepristone binds cytosolic GC receptors,preventing coactivator recruitment rendering thereceptor complex inactive, thus preventing genetranscription.7 Long-term oral mifepristone hasbeen investigated for several disorders includingmeningioma, depression, Cushing disease, uterineleiomyomata, endometriosis, diabetes, and obesity.7,8
Long-term treatment with mifepristone is generallywell tolerated and has a typically benign side effectprofile including skin rash, nausea, dizziness, fatigue,reversible liver transaminase elevation, and endome-trial hyperplasia.7,8 Presently, the cornerstone oftreatment for recurrent or persistent CSC is verteporfin(Visudyne; QLT Inc., Vancouver, British Columbia,Canada) photodynamic therapy (PDT). Laser activa-tion of verteporfin after infusion generates local
From the *Department of Ophthalmology, Feinberg School ofMedicine, Northwestern University, Chicago, Illinois; and †WolfeEye Clinic, West Des Moines, Iowa.
Supported in part by grants from The Macula Foundation, NewYork, NY, and Research to Prevent Blindness Inc., New York, NY.
The authors report no conflicts of interest.Reprint requests: Jared S. Nielsen, MD, Wolfe Eye Clinic, 6200
Westown Parkway, West Des Moines, IA 50266; e-mail: [email protected]
1928

DubbiUn solo studioFarmaco impossibile da ottenere (disponibile solo in ospedale con ricovero per aborto farmacologico)
MIFEPRISTONE (RU486)

Inibitore del diidrotestosterone usato nella terapia dell’ipertrofia prostatica, tumori prostata, alopecia androgenica e irsutismo
RazionaleInibisce la sintesi del diidrotesto-sterone (anche gli androgeni sono implicati nella patogenesi della CRSC) [Ahad et al. Eye 2006, Grieshaber et al. BJO 2007]
FINASTERIDE (PROSCAR)

FINASTERIDE (PROSCAR)
FINASTERIDE FOR CHRONIC CENTRALSEROUS CHORIORETINOPATHY
FARZIN FOROOGHIAN, MD, ANNAL D. MELETH, MD, MS, CATHERINE CUKRAS, MD, PHD,EMILY Y. CHEW, MD, WAI T. WONG, MD, PHD, CATHERINE B. MEYERLE, MD
Purpose: To evaluate the safety and efficacy of finasteride, an inhibitor ofdihydrotestosterone synthesis, in the treatment of chronic central serous chorioretinopathy.
Methods: Five patients with chronic central serous chorioretinopathy were pro-spectively enrolled in this pilot study. Patients were administered finasteride (5 mg) dailyfor 3 months, after which study medication was withheld and patients were observed for3 months. Main outcome measures included best-corrected visual acuity, centralsubfield macular thickness, and subretinal fluid volume as assessed by optical coherencetomography. Serum dihydrotestosterone, serum testosterone, and urinary cortisol werealso measured.
Results: There was no change in mean best-corrected visual acuity. Mean center-subfield macular thickness and subretinal fluid volume reached a nadir at 3 months androse to levels that were below baseline by 6months. The changes in both optical coherencetomography parameters paralleled those in serum dihydrotestosterone level. In fourpatients, center-subfield macular thickness and/or subretinal fluid volume increased afterdiscontinuation of finasteride. In the remaining patient, both optical coherence tomographyparameters normalized with finasteride and remained stable when the study medicationwas discontinued.
Conclusion: Finasteride may represent a novel medical treatment for chronic centralserous chorioretinopathy. Larger controlled clinical trials are needed to further assess theefficacy of finasteride for the treatment of central serous chorioretinopathy.
RETINA 31:766–771, 2011
Central serous chorioretinopathy (CSC) is anacquired chorioretinal disease characterized by
the presence of exudative detachment of the neurso-sensory retina and/or retinal pigment epithelium(RPE). The pathophysiology is poorly understood,but alterations in choroidal circulation and RPEfunction have been hypothesized to play a role.Indocyanine green angiography and enhanced depthimaging spectral-domain optical coherence tomogra-phy (OCT) have provided evidence suggesting hyper-permeability and increased hydrostatic pressure withinthe choroidal circulation.1–4 Fundus autofluorescence
imaging has shown decreased autofluorescence incases of chronic CSC, suggesting reduced metabolicactivity of the RPE.5 While acute CSC can sometimesbe recurrent, it generally resolves spontaneously withminimal sequelae. However, chronic CSC can resultin significant visual loss.6 Diffuse retinal pigmentepitheliopathy, which is characterized by widespreadRPE damage and destruction, may develop in somepatients.7 Chronic CSC can be challenging to treat;however, recent studies8,9 have demonstrated safetyand efficacy using photodynamic therapy at reducedfluence or reduced dosage. Despite the improvedsafety of reduced-fluence photodynamic therapy,complications such as tears of the RPE have beendescribed,10 and concerns over the potential for RPEatrophy with repeated treatments persist.Based on the proposed role of glucocorticoids in the
pathogenesis of CSC, inhibition of cortisol has beenproposed as a medical treatment option.11 In one smallstudy12 of chronic CSC, ketoconazole (a glucocorti-coid antagonist) reduced urinary cortisol levels andresulted in a decrease in lesion height as measured by
From the Division of Epidemiology and Clinical Applications,National Eye Institute, National Institutes of Health, Bethesda,Maryland.
Supported by the National Eye Institute Intramural ResearchProgram.
The authors have no conflicts of interest to disclose.Reprint requests: Catherine B. Meyerle, MD, Division of
Epidemiology and Clinical Research, National Eye Institute,National Institutes of Health, Building 10, Magnuson Room10s235, 10 Center Drive, Bethesda, MD 20892; e-mail: [email protected]
766

Dosaggio5 mg/die per almeno tre mesi
Effetti collateraliTeratogenesi, calo libido
Esami da richiedere primaNessuno
FINASTERIDE (PROSCAR)