Riabilitazione cardiorespiratoria nell anziano - fimeg.org · 05/11/2016 4 ISWT = Incremental...
9
05/11/2016 1 Università degli Studi di Salerno Amelia Filippelli Dipartimento di Medicina e Chirurgia, Università degli Studi di Salerno Servizio Farmacologia Clinica - AOU S. Giovanni di Dio e Ruggi d'Aragona [email protected] - [email protected] Riabilitazione cardiorespiratoria nell’anziano Cardiopulmonary rehabilitation in elderly http://www.who.int/mediacentre/factsheets/fs310/en/index1.html CARDIOVASCULAR AND RESPIRATORY DISEASES ARE THE LEADING CAUSES OF DEATH ASSOCIATIONS BETWEEN CARDIOVASCULAR DISEASE AND RESPIRATORY DISEASE : common risk factors and common symptoms/signs Early-life risk factors for chronic non respiratory diseases. Chacko A, Carpenter DO, Callaway L, Sly PD. Eur Respir J. 2015 Jan;45(1):244-59. dyspnea fatigue exercise tollerance cognitive and daily activities impairment SYMTOMS/SIGNS RISK FACTORS Obstructive Diseases* Restrictive Diseases Interstitial Chest Wall Neuromuscular Other Diseases (lung cancer, pulmonary, before and after thoracic and abdominal surgery, obesity-related respiratory disease…) *COPD, persistent asthma, cystic fibrosis, bronchiolitis obliterans Recent myocardial infarction Coronary bypass Valvular heart disease Heart failure Valve surgery Percutaneous coronary Intervention Cardiac transplantation Stable angina INTERNATIONAL GUIDELINES: INDICATIONS FOR REHABILITATION GOLD Guidelines AHA/ACC Guidelines
Transcript of Riabilitazione cardiorespiratoria nell anziano - fimeg.org · 05/11/2016 4 ISWT = Incremental...

05/11/2016
1
Università degli Studi di Salerno
Amelia Filippelli Dipartimento di Medicina e Chirurgia, Università degli Studi di Salerno
Servizio Farmacologia Clinica - AOU S. Giovanni di Dio e Ruggi d'Aragona [email protected] - [email protected]
Riabilitazione cardiorespiratoria nell’anziano
Cardiopulmonary rehabilitation in elderly
http://www.who.int/mediacentre/factsheets/fs310/en/index1.html
CARDIOVASCULAR AND RESPIRATORY DISEASES ARE
THE LEADING CAUSES OF DEATH
ASSOCIATIONS BETWEEN CARDIOVASCULAR DISEASE AND
RESPIRATORY DISEASE :
common risk factors and common symptoms/signs
Early-life risk factors for chronic non respiratory diseases.
Chacko A, Carpenter DO, Callaway L, Sly PD.
Eur Respir J. 2015 Jan;45(1):244-59.
dyspnea
fatigue
exercise tollerance
cognitive and daily
activities impairment
SYMTOMS/SIGNS
RISK FACTORS Obstructive Diseases*
Restrictive Diseases
Interstitial
Chest Wall
Neuromuscular
Other Diseases (lung cancer,
pulmonary, before and after
thoracic and abdominal surgery,
obesity-related respiratory
disease…)
*COPD, persistent asthma, cystic fibrosis,
bronchiolitis obliterans
Recent myocardial infarction
Coronary bypass
Valvular heart disease
Heart failure
Valve surgery
Percutaneous coronary
Intervention
Cardiac transplantation
Stable angina
INTERNATIONAL GUIDELINES: INDICATIONS FOR
REHABILITATION GOLD Guidelines AHA/ACC Guidelines
05/11/2016
2
http://www.burke.org/rehab/inpatient/cardiopulmonary
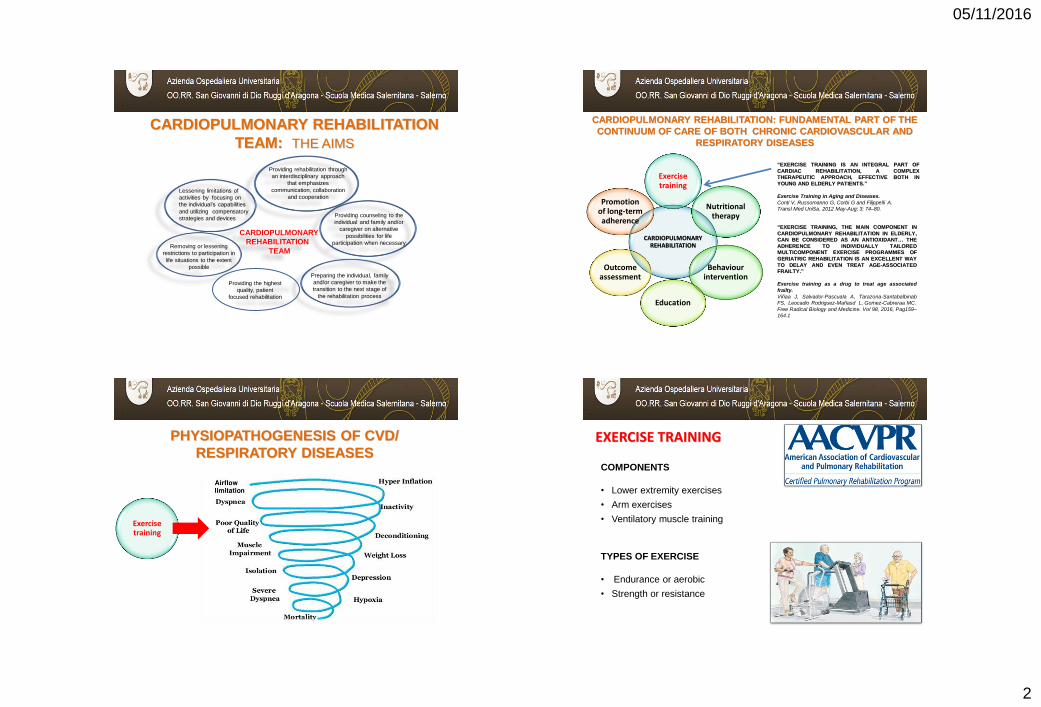
CARDIOPULMONARY REHABILITATION
TEAM: THE AIMS
CARDIOPULMONARY
REHABILITATION
TEAM
Lessening limitations of
activities by focusing on
the individual’s capabilities
and utilizing compensatory
strategies and devices
Removing or lessening
restrictions to participation in
life situations to the extent
possible
Providing counseling to the
individual and family and/or
caregiver on alternative
possibilities for life
participation when necessary
Preparing the individual, family
and/or caregiver to make the
transition to the next stage of
the rehabilitation process
Providing rehabilitation through
an interdisciplinary approach
that emphasizes
communication, collaboration
and cooperation
Providing the highest
quality, patient
focused rehabilitation
CARDIOPULMONARY REHABILITATION: FUNDAMENTAL PART OF THE
CONTINUUM OF CARE OF BOTH CHRONIC CARDIOVASCULAR AND
RESPIRATORY DISEASES
“EXERCISE TRAINING IS AN INTEGRAL PART OF
CARDIAC REHABILITATION, A COMPLEX
THERAPEUTIC APPROACH, EFFECTIVE BOTH IN
YOUNG AND ELDERLY PATIENTS.”
Exercise Training in Aging and Diseases.
Conti V, Russomanno G, Corbi G and Filippelli A.
Transl Med UniSa. 2012 May-Aug; 3: 74–80.
“EXERCISE TRAINING, THE MAIN COMPONENT IN
CARDIOPULMONARY REHABILITATION IN ELDERLY,
CAN BE CONSIDERED AS AN ANTIOXIDANT… THE
ADHERENCE TO INDIVIDUALLY TAILORED
MULTICOMPONENT EXERCISE PROGRAMMES OF
GERIATRIC REHABILITATION IS AN EXCELLENT WAY
TO DELAY AND EVEN TREAT AGE-ASSOCIATED
FRAILTY.”
Exercise training as a drug to treat age associated
frailty.
Viñaa J, Salvador-Pascuala A, Tarazona-Santabalbinab
FS, Leocadio Rodriguez-Mañasd L, Gomez-Cabreraa MC.
Free Radical Biology and Medicine. Vol 98, 2016, Pag159–
164.1
CARDIOPULMONARY REHABILITATION
Exercise training
Nutritional therapy
Behaviour intervention
Education
Outcome assessment
Promotion of long-term adherence
PHYSIOPATHOGENESIS OF CVD/
RESPIRATORY DISEASES
Exercise training
COMPONENTS
• Lower extremity exercises
• Arm exercises
• Ventilatory muscle training
TYPES OF EXERCISE
• Endurance or aerobic
• Strength or resistance
EXERCISE TRAINING

05/11/2016
3
INTERNATIONAL GUIDELINES:
CONTRAINDICATIONS FOR REHABILITATION
GOLD Guidelines AHA/ACC Guidelines
Patients with severe orthopedic
or neurological disorders limiting
their mobility
Severe pulmonary arterial
hypertension
Exercise induced syncope
Unstable angina or recent MI
Refractory fatigue
Inability to learn, psychiatric
instability and disruptive behavior
Unstable angina
Uncompensated heart failure
Uncontrolled arrhythmias
Severe ischemia, LV disfunction
during exercise testing
Poorly controlled hypertension
Acute thrombophlebitis
Pulmonary or sistemic embolism
Myocarditis
Severe psychological disorders
Severe mobility limitations
• Improved exercise capacity
• Reduced the perceived intensity of
breathlessness
• Improved health-related quality of life
• Reduced the number of hospitalizations and
days in the hospital
• Reduced anxiety and depression associated with
COPD
• Strength and endurance training of the upper
limbs improves arm function
• Benefits extend well beyond the immediate period
of training
• Improved survival
• Respiratory muscle training can be beneficial,
especially when combined with general exercise
training
• Improved recovery after hospitalization for an
exacerbation
• Enhanced the effect of long-acting bronchodilators
• Decreased mortality at up to 5 years post
participation
• Decreased cardiovascular events
• Reduced symptoms (angina, dyspnea,
fatigue)
• Improved Modifiable Risk Factors
• Improved function and exercise capacity
• Improved health-related quality of life
• Improved health factors like lipids and blood
pressure
• Enhanced ability to perform activities of
daily living
• Improved psychosocial symptoms
• Reduced hospitalizations and use of
medical resources
• Increased ability to return to work or engage
in leisure activities
INTERNATIONAL GUIDELINES: OUTCOMES
GOLD (Global Initiative for Chronic Obstructive Lung
Disease) Guidelines
AHA/ACC (American Heart Association/American College
of Cardiology) Guidelines
COPD and CHF coexistence
The risk ratio of developing HF in COPD pts is 4.5
The rate-adjusted hospital prevalence of CHF is 3 times greater among pts. discharged with a diagnosis of COPD compared with patients discharged without mentioned of COPD
• Up to 1/3 of elderly pts. with CHF have COPD
• Up to 1/5 of elderly pts. with COPD have CHF
14 million
Americans
have
COPD
And
5 million
have
CHF
Pier Luigi Temporelli. Monaldi Archives for Chest Disease Cardiac Series 2015:
«Cardiopulmonary rehabilitation in patient with heart failure and chronic pulmonary
disease»
05/11/2016
4
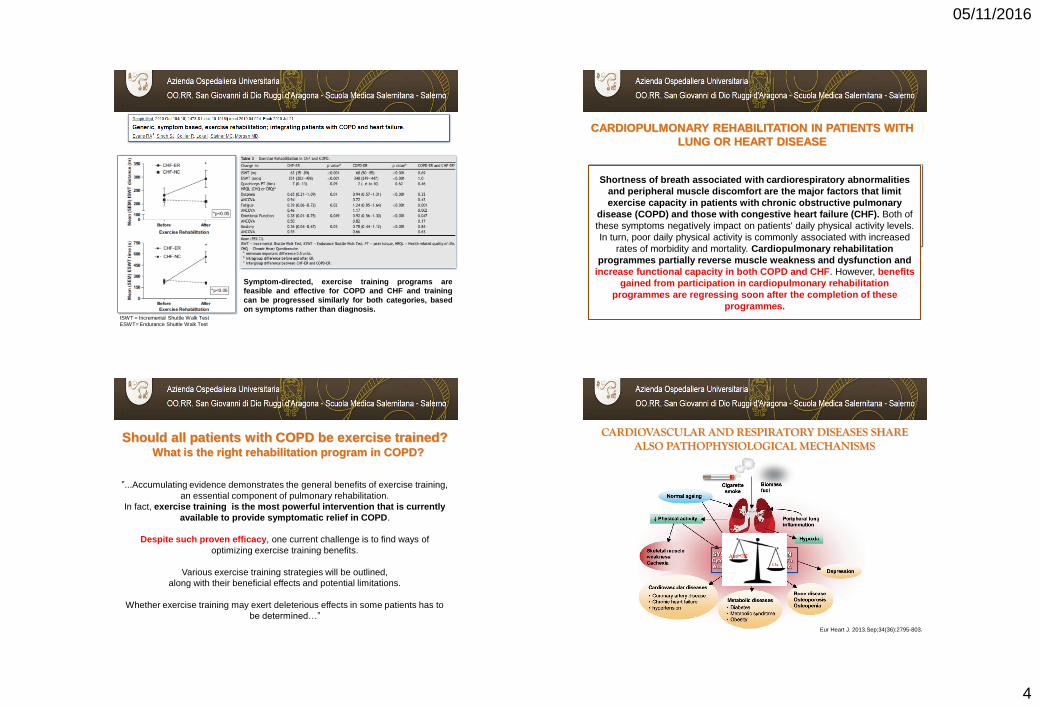
ISWT = Incremental Shuttle Walk Test
ESWT= Endurance Shuttle Walk Test
Symptom-directed, exercise training programs are
feasible and effective for COPD and CHF and training
can be progressed similarly for both categories, based
on symptoms rather than diagnosis.
Shortness of breath associated with cardiorespiratory abnormalities
and peripheral muscle discomfort are the major factors that limit
exercise capacity in patients with chronic obstructive pulmonary
disease (COPD) and those with congestive heart failure (CHF). Both of
these symptoms negatively impact on patients' daily physical activity levels.
In turn, poor daily physical activity is commonly associated with increased
rates of morbidity and mortality. Cardiopulmonary rehabilitation
programmes partially reverse muscle weakness and dysfunction and
increase functional capacity in both COPD and CHF. However, benefits
gained from participation in cardiopulmonary rehabilitation
programmes are regressing soon after the completion of these
programmes.
CARDIOPULMONARY REHABILITATION IN PATIENTS WITH
LUNG OR HEART DISEASE
Should all patients with COPD be exercise trained? What is the right rehabilitation program in COPD?
”...Accumulating evidence demonstrates the general benefits of exercise training,
an essential component of pulmonary rehabilitation.
In fact, exercise training is the most powerful intervention that is currently
available to provide symptomatic relief in COPD.
Despite such proven efficacy, one current challenge is to find ways of
optimizing exercise training benefits.
Various exercise training strategies will be outlined,
along with their beneficial effects and potential limitations.
Whether exercise training may exert deleterious effects in some patients has to
be determined…”
CARDIOVASCULAR AND RESPIRATORY DISEASES SHARE ALSO PATHOPHYSIOLOGICAL MECHANISMS
Eur Heart J. 2013.Sep;34(36):2795-803.

05/11/2016
5
CARDIOVASCULAR AND RESPIRATORY DISEASES ARE
age-related diseases
Inflammaging Free radicals hypothesis
Genetic hypothesis Telomeres Why do we age?
AGING
Proteins Lipids
Membrane damage
Enzymatic activity loss
Inert complex formation
Transcriptional and traslocation defects
Nucleic acids
Ox Anti-Ox
OXIDATIVE STRESS IN AGING

05/11/2016
6
Guarente L. Franklin H. Epstein Lecture: Sirtuins, aging, and medicine.
N Engl J Med. 2011;364(23):2235-44.
Sirtuins, aging and aging-associated diseases
Corbi et al. Int J Mol Sci. 2013 Jun
17;14(6):12696-713..
+
CHF COPD
SIRT1 LEVELS ARE DECREASED IN BOTH CARDIOVASCULAR AND
RESPIRATORY DISEASES EXERCISE BENEFITS…OUR RESULTS

05/11/2016
7
Cardiac rehabilitation in CHF patients:
Study design
30-minute sessions of aerobic exercise + respiratory exercises
5 days /week for 4 weeks
cardiopulmonary
stress test
ECG and
echocardiographic
examinations Comorbility and risk factors
Clinical and demographic features
blood chemistry tests
cardiopulmonary
stress test
blood chemistry tests
Subjects with post-ischemic
HF in clinically stable
conditions
In vivo and in
vitro experiments
Antioxidative and antisenescent
effects of cardiac rehabilitation:
Role for Sirt1
Unpublished data
Antioxidative and antisenescent effects of cardiac
rehabilitation: Role for Sirt1
Unpublished data
Sirt 1 and catalase as indicator of rehabilitation program
efficacy: role in exercise tolerance
Unpublished data

05/11/2016
8
SIRT1 AND «THE AGING THEORY OF COPD»
Conti et al. Anal Cell Pathol (Amst). 2015;2015:897327.
.Conti et al. .Anal Cell Pathol (Amst). 2015;2015:897327.
Ito K et al. COPD as a disease of accelerated lung aging.
Chest. 2009 Jan;135(1):173-80.
Sirtuins
AGING HYPOTHESIS FOR COPD
• Total oxidative status (TOS) • Trolox equivalent antioxidant capacity
(TEAC) • Oxidative stress index (OSI) • IL-6 expression
LYMPHOCYTES • Sirt1 expression • Sirt1 activity
FICOLL
GEL
ERYTHROCIYTES AND NEUTROPHYLS
PLASMA
Sirt 1 as predictive and prognostic marker for COPD: study disegn
HS, Healthy smokers HnS ,Healthy non smokers COPD, patients
ng
/ml
Sirt1 expression
P=0,04
Sirt1 activity
P<0,001
AU
Sirt 1 activity as predictive and prognostic marker for
COPD: preliminary data
=
05/11/2016
9
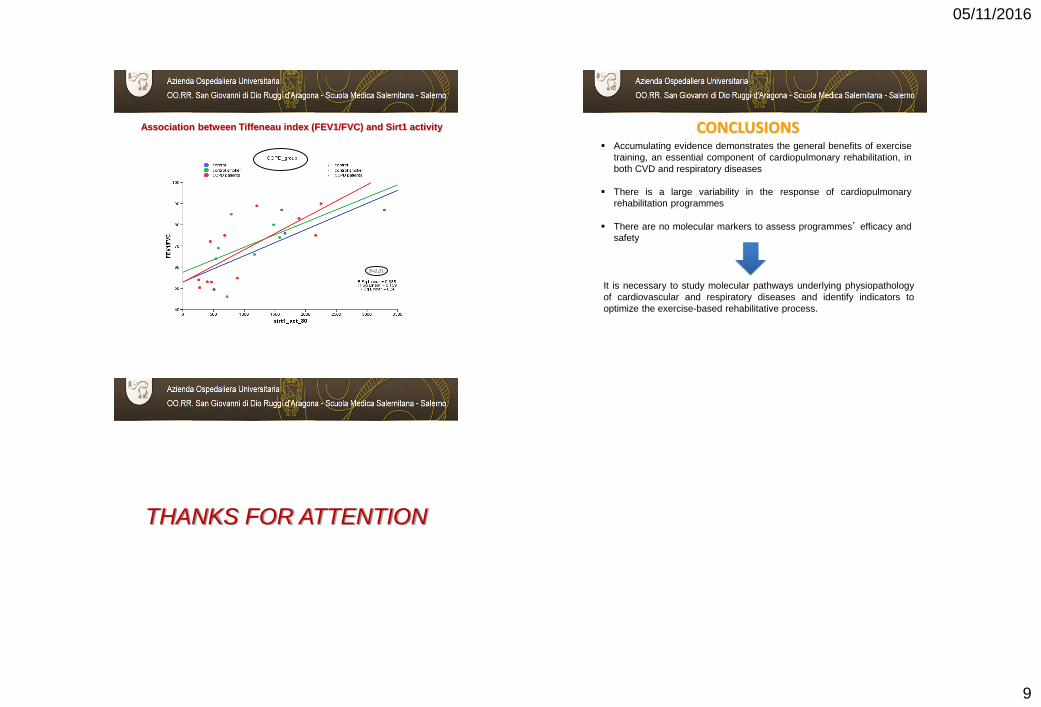
Association between Tiffeneau index (FEV1/FVC) and Sirt1 activity
P<0,01
CONCLUSIONS Accumulating evidence demonstrates the general benefits of exercise
training, an essential component of cardiopulmonary rehabilitation, in
both CVD and respiratory diseases
There is a large variability in the response of cardiopulmonary
rehabilitation programmes
There are no molecular markers to assess programmes’ efficacy and
safety
It is necessary to study molecular pathways underlying physiopathology
of cardiovascular and respiratory diseases and identify indicators to
optimize the exercise-based rehabilitative process.
THANKS FOR ATTENTION