Presentazione di PowerPoint - Section of Psychiatry
49
QT lungo Flavio Ribichini Cardiologia Università di Verona 01/10/2010 1
Transcript of Presentazione di PowerPoint - Section of Psychiatry

QT lungo
Flavio RibichiniCardiologiaUniversitagrave di Verona
01102010
1
01102010
2
Referto ECG ritmo sinusale QT lungo
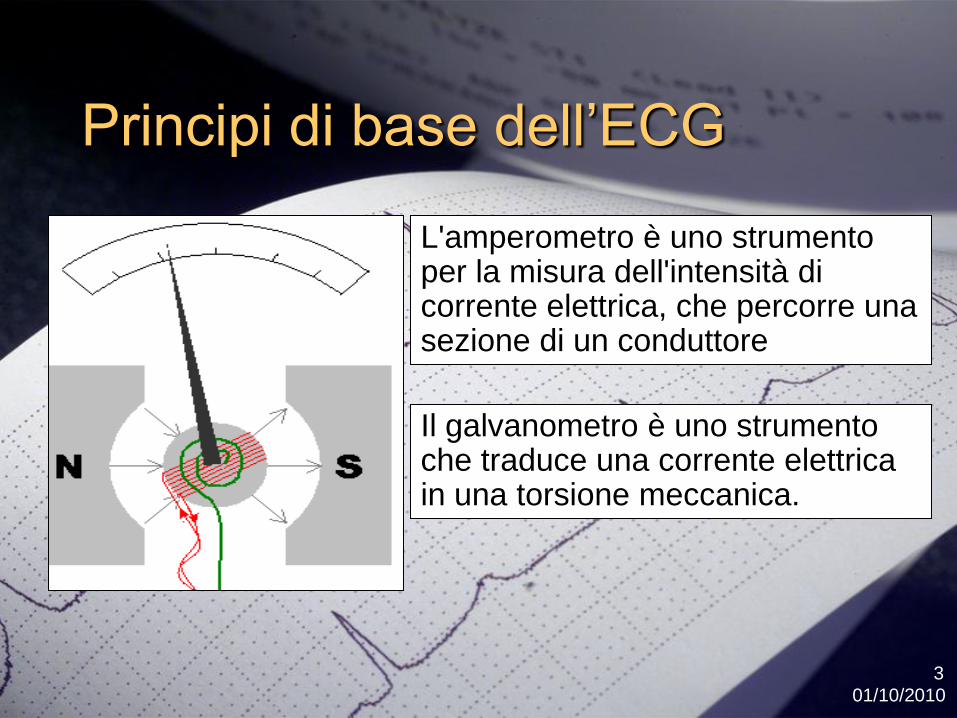
Principi di base dellrsquoECG
01102010
3
Lamperometro egrave uno strumento per la misura dellintensitagrave di corrente elettrica che percorre una sezione di un conduttore
Il galvanometro egrave uno strumento che traduce una corrente elettrica in una torsione meccanica
ECG
01102010
4
Lelettrocardiogramma (ECG) egrave la registrazione dellattivitagrave elettrica del cuore che si verifica nel ciclo cardiaco
rsquo
ECG
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
2
Referto ECG ritmo sinusale QT lungo
Principi di base dellrsquoECG
01102010
3
Lamperometro egrave uno strumento per la misura dellintensitagrave di corrente elettrica che percorre una sezione di un conduttore
Il galvanometro egrave uno strumento che traduce una corrente elettrica in una torsione meccanica
ECG
01102010
4
Lelettrocardiogramma (ECG) egrave la registrazione dellattivitagrave elettrica del cuore che si verifica nel ciclo cardiaco
rsquo
ECG
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
Principi di base dellrsquoECG
01102010
3
Lamperometro egrave uno strumento per la misura dellintensitagrave di corrente elettrica che percorre una sezione di un conduttore
Il galvanometro egrave uno strumento che traduce una corrente elettrica in una torsione meccanica
ECG
01102010
4
Lelettrocardiogramma (ECG) egrave la registrazione dellattivitagrave elettrica del cuore che si verifica nel ciclo cardiaco
rsquo
ECG
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

ECG
01102010
4
Lelettrocardiogramma (ECG) egrave la registrazione dellattivitagrave elettrica del cuore che si verifica nel ciclo cardiaco
rsquo
ECG
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

rsquo
ECG
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
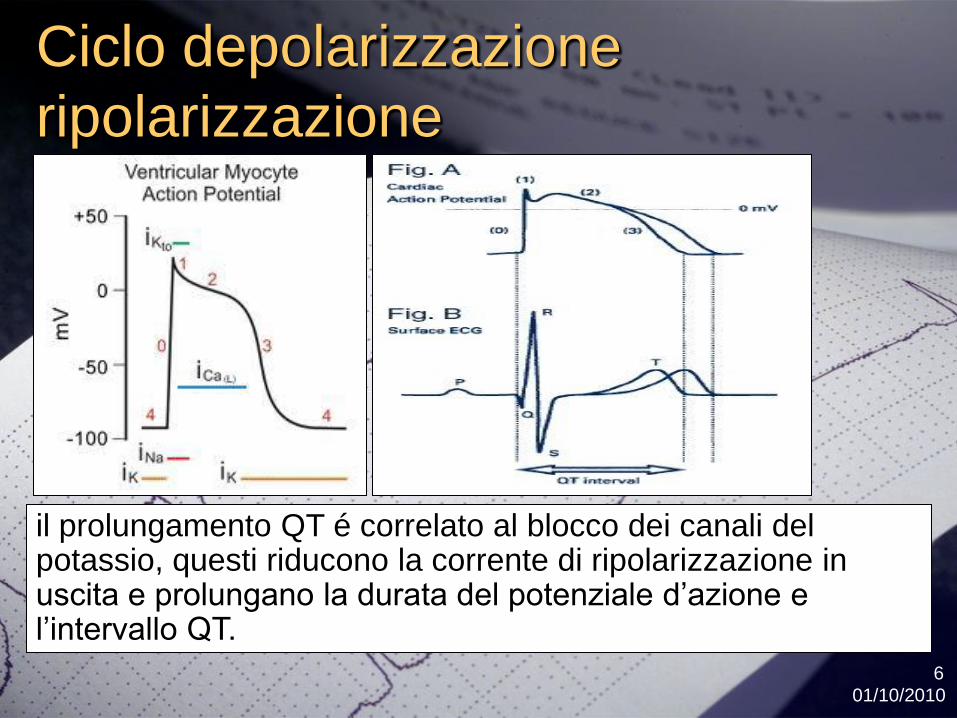
Ciclo depolarizzazione
ripolarizzazione
01102010
6
il prolungamento QT eacute correlato al blocco dei canali del potassio questi riducono la corrente di ripolarizzazione in uscita e prolungano la durata del potenziale drsquoazione e lrsquointervallo QT
E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

E il QT lungo
01102010
7
INTERVALLO QT egrave la distanza tra la prima deflessione del QRS e la fine dellrsquoonda T
IL QTc misura la durata (tempo) diviso la radice dellrsquointervallo RR in sec
Nota il QT viene misurato in msec
Lrsquointervallo RR in sec
quindi il QTc egrave una standardizzazione della durata del QT per la FC (idealmente a 60bpm)
Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Valori di normalitagrave del QT
01102010
8
Un intervallo QT non corretto oltre 500 msec egrave usualmente considerato patologico
ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

ECG normale esercizio 1
01102010
9
1quadratino piccolo 40 msec
1 quadrato grande 200 msec
1 quadrato grande e 3 piccoli
200+120=320 msec
Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Esercizio 2
01102010
10
3 quadrati grandi da 200 msec
+ 1quadratino piccolo 40 msec
Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Esercizio 3
01102010
11
3 quadrati grandi = 600 msec
Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Numerosi sono i meccanismi con cui gli antipsicotici alteranola conduzione cardiaca quasi sempre gli antipsicoticiantagonizzano la componente rapida del canale delpotassio Ikr
Il canale del potassio IKr egrave codificato dal gene umano HERG(human Ether-agrave-go-go Related Gene) e studi di tranfezione dicellule del gene HERG mostrano un antagonismo diretto dialcune sostanze tra cui aloperidolo (Suessbrich 1997)sertindolo (Rampe D1998) clozapina (Tie H 2000)tioridazina e clorpromazina (Tie H 2001) Questo egrave ilmeccanismo maggiormente implicato nellrsquoallungamento delQT (William J 2006)
Il blocco del recettore IKr risulta dose dipendente (Drolet1999 Tie H 2000)
Alcuni antipsicotici sembrano interferire anche con i canali delsodio e del calcio (Shader 1999)
Lrsquoinizio del problemahellip
01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
13
Lrsquoinizio del problemahellip
httpwwwagenziafarmacoitsitesdefaultfilesbif0703120pdf
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
01102010
14
Non egrave chiaro lrsquoeffetto sul QTc a bassi dosaggi (5 mg die) o a dosaggi moderati (5-20 mg die) (Fulop 1987 Czekalla 1961)
Segnalato allungamento del QTc e torsioni di punta per alti dosaggi per os (gt20 mg die) (Kriwisky 1990 Metzger 1993) o in caso di sovradosaggio (Henderson 1991)
Alti dosaggi (gt50 mg die) per via endovenosa si associano ad un allungamento del QTc con casi descrtitti di torsioni di punta (Lawrence 1997 OrsquoBrien 1999)
Per dosaggi endovenosi da 5-25 mg sono segnalati aumenti del QTc a valori superiori a 500 ms (Hatta 2000)
Per somministrazione intramuscolare di una dose di 75 mg seguita da dose di 10 mg egrave segnalato un aumento medio del QTc di 15 ms(Miceli JL 2002)
01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
15
Concetti praticihellip
1 La dose e la via di somministrazione ha unrsquoimportanza nella possibile tossicitagrave
2 Ersquo da preferireevitare una via parenterale ad una via orale
3 Lrsquoeffetto degli antipsicotici sul QT egrave sinergico
4 Lo egrave anche con i farmaci antiaritmici
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
01102010
16
Concetti praticihellip
1 La dose e la via di somministrazione hanno unrsquoimportanza nella possibile tossicitagrave
SI la dose e le somministrazioni parenterali aumentano la biodisponibilitagrave di questi farmaci e quindi possono causare un maggior blocco dei canali del K e maggior allungamento del QT
Lrsquoeffetto egrave comunque molto modesto
01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
17
Abstract
STUDY OBJECTIVE To characterize the effect of oral ziprasidone and haloperidol on the corrected QT (QTc) interval under steady-state conditions Design Prospective randomized open-label parallel-group study
SETTING Inpatient clinical research facility Patients Fifty-nine adults (age range 25-59 yrs) with schizophrenia or schizoaffective disorder who had no clinically significant abnormality on electrocardiogram (ECG) at screening Intervention During period 1 (days -10 to -4) antipsychotic and anticholinergic drugs were tapered On the first day (day -3) of period 2 the drugs were discontinued and placebo was given for the next 3 days (days -2 to 0) On the last day (day 0) of period 2 serial baseline ECGs were collected During period 3 (days 1-16) patients received escalating oral doses of ziprasidone and haloperidol to reach steady state Period 4 (days 17-19) allowed for study drug washout and initiation of outpatient antipsychotic therapy safety assessments were also performed during this period
MEASUREMENTS AND RESULTS At each steady-state dose level three ECGs and a serum or plasma sample were collected at the predicted time of peak exposure to the administered drug Point estimates and 95 confidence intervals (CIs) were determined for the mean QTc interval at baseline and for the mean change from baseline in QTc at each steady-state dose level Mean changes from baseline in the QTc interval (msec) for ziprasidone were 45 (95 CI 19-71) 195 (95 CI 155-234) and 225 (95 CI 157-294) for steady-state doses of 40 160 and 320 mgday respectively for haloperidol -12 (95 CI -41-17) 66 (95 CI 16-117) and 72 (95 CI 14-131) for steady-state doses of 25 15 and 30 mgday Although no patient in either treatment group experienced a QTc interval of 450 msec or greater the QTc interval increased 30 msec or more in 11 and 17 ziprasidone-treated patients at 160 and 320 mgday respectively and in 3 and 5 haloperidol-treated patients at 15 and 30 mgday respectively Most treatment-emergent adverse drug reactions were mild in intensity and none were severe
CONCLUSION The QTc interval in ziprasidone- and haloperidol-treated patients increased with dose Treatment with high doses of ziprasidone or haloperidol did not result in any patient experiencing a QTc interval of 450 msec or greater
Pharmacotherapy 2010 Feb30(2)127-35 Effects of Oral Ziprasidone and Oral Haloperidol on QTc interval in patients with Schizophrenia or Schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano R OGorman C Harrigan RH
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)
CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
18
Concetti praticihellip
Ersquo da preferireevitare una via IM ad una via IV
Una minor biodisponibilitagrave del farmaco riduce il rischio di tossicitagrave nelle somministrazioni estemporanee in PS
Rischio che permane comunque modesto
01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
19
Expert Opin Drug Saf 2003 Nov2(6)543-7
Torsade de pointes associated with the administration of intravenous haloperidola review of the literature and practical guidelines for use
Hassaballa HA Balk RA
Division of Pulmonary and Critical Care Medicine Rush-Presbyterian St Lukes Medical Center 1653 West Congress Parkway Chicago IL 60612 USA
Abstract
Haloperidol is the most commonly used medication for the treatment of delirium and psychosis in the critically ill patient Whilst generally considered to be safe haloperidol has been associated with a number of important cardiovascular side effects The major toxicities include hypotension cardiac arrhythmias and prolongation of the corrected QT (QTc) interval In particular torsade de pointes a polymorphic ventricular tachyarrhythmia has been associated with both intravenous and oral haloperidol administration The management of torsade de pointes consists of discontinuation of the possible offending agent(s) correction of electrolyte abnormalities administration of magnesium sulfate and if necessary overdrive pacing Although clinicians should be aware of this potentially lethal complication of intravenous haloperidol therapy it should not deter clinicians from using intravenous haloperidol to treat acute agitation in the critically ill patient with a normal QTc
J Hosp Med 2010 Apr5(4)E8-16
The FDA extended warning for intravenous haloperidol and torsades de pointes how should institutions respond
Meyer-Massetti C Cheng CM Sharpe BA Meier CR Guglielmo BJ
Department of Clinical Pharmacy School of Pharmacy University of California San Francisco Medication Outcomes Center San Francisco California USA carlameyerunibasch
Abstract
BACKGROUND In September 2007 the Food and Drug Administration (FDA) strengthened label warnings for intravenous (IV) haloperidol regarding QT prolongation (QTP) and torsades de pointes (TdP) in response to adverse event reports Considering the widespread use of IV haloperidol in the management of acute delirium the specific FDA recommendation of continuous electrocardiogram (ECG) monitoring in this setting has been associated with some controversy We reviewed the evidence for the FDA warning and provide a potential medical center response to this warning
METHODS Cases of intravenous haloperidol-related QTPTdP were identified by searching PubMed EMBASE and Scopus databases (January 1823 to April 2009) and all FDA MedWatch reports of haloperidol-associated adverse events (November 1997 to April 2008)
RESULTS A total of 70 of IV haloperidol-associated QTP andor TdP were identified There were 54 reports of TdP 42 of these events were reportedly preceded by QTP When post-event QTc data were reported QTc was prolonged gt450 msec in 96 of cases Three patients experienced sudden cardiac arrest Sixty-eight patients (97) had additional risk factors for TdPprolonged QT most commonly receipt of concomitant proarrhythmic agents Patients experiencing TdP received a cumulative dose of 5 mg to 645 mg patients with QTP alone received a cumulative dose of 2 mg to 1540 mg
CONCLUSIONS While administration of IV haloperidol can be associated with QTPTdP this complication most often took place in the setting of concomitant risk factors Importantly the available data suggest that a total cumulative dose of IV haloperidol of lt2 mg can safely be administered without ongoing electrocardiographic monitoring in patients without concomitant risk factors
01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
20
Concetti praticihellip
Lrsquoeffetto della politerapia con antipsicotici sul QT egrave sinergico
SI sono potenzialmente sinergici sullrsquoallungamento del QT e quindi questi pazienti meritano piugrave attenzione
Ann Gen Psychiatry 2005 Jan 254(1)1
QT interval prolongation related to psychoactive drug treatment a comparison of monotherapy versus polytherapy
Sala M Vicentini A Brambilla P Montomoli C Jogia JR Caverzasi E Bonzano A Piccinelli M Barale F De Ferrari GM
Department of Health Sciences-Section of Psychiatry IRCCS Policlinico S Matteo University of Pavia School of Medicine Pavia Italy michelasalacapyahooit
Abstract
BACKGROUND Several antipsychotic agents are known to prolong the QT interval in a dose dependent manner Corrected QT interval (QTc) exceeding a threshold value of 450 ms may be associated with an increased risk of life threatening arrhythmias Antipsychotic agents are often given in combination with other psychotropic drugs such as antidepressants thatmay also contribute to QT prolongation This observational study compares the effects observed on QT interval between antipsychotic monotherapy and psychoactive polytherapy which included an additional antidepressant or lithium treatment
METHOD We examined two groups of hospitalized women with Schizophrenia Bipolar Disorder and Schizoaffective Disorder in a naturalistic setting Group 1 was composed of nineteen hospitalized women treated with antipsychotic monotherapy (either haloperidol olanzapine risperidone or clozapine) and Group 2 was composed of nineteen hospitalizedwomen treated with an antipsychotic (either haloperidol olanzapine risperidone or quetiapine) with an additional antidepressant (citalopram escitalopram sertraline paroxetine fluvoxamine mirtazapine venlafaxine or clomipramine) or lithium An Electrocardiogram (ECG) was carried out before the beginning of the treatment for both groups and at a second time after four days of therapy at full dosage when blood was also drawn for determination of serum levels of the antipsychoticStatistical analysis included repeated measures ANOVA Fisher Exact Test and Indipendent T Test
RESULTS Mean QTc intervals significantly increased in Group 2 (24 +- 21 ms) however this was not the case in Group 1 (-1 +- 30 ms) (Repeated measures ANOVA p lt 001) Furthermore we found a significant difference in the number of patients who exceeded the threshold of borderline QTc interval value (450 ms) between the two groups with seven patients in Group 2 (38) compared to one patient in Group 1 (7) (Fisher Exact Text p lt 005)
CONCLUSIONS No significant prolongation of the QT interval was found following monotherapy with an antipsychotic agent while combination of these drugs with antidepressants caused a significant QT prolongation Careful monitoring of the QT interval is suggested in patients taking a combined treatment of antipsychotic and antidepressant agents
01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
21
Concetti praticihellip1 Lo egrave anche con i farmaci antiaritmici
2 Assolutamente SI i farmaci antiaritmici di classe terza allungano il QT per loro stesso meccanismo drsquoazione
01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
22
Definizione della Sindrome del QT lungo
La sindrome da QT lungo (LQTS) egrave un eterogeneo gruppo di disturbi congeniti o acquisiti dei canali ionici coinvolti nella ripolarizzazione
Ersquo caratterizzata da un prolungamento dellrsquointervallo QT allrsquoECG di superficie e dalla conseguente predisposizione a svilupparesincope e morte cardiaca improvvisa (SCD) per causa aritmica
Nella maggior parte dei casi lrsquoexitus egrave provocato da tachicardie ventricolari polimorfe maligne chiamate ldquotorsades de pointesrdquo (TdP)
W Hurst Il cuore capitolo 31 1068-1070 11 edizione
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
01102010
23
Fattori di rischio per il QT lungo
Legati al paziente
bull Sindrome congenita del QT lungo
bull Sesso femminile
bull Bradicardia significativa storia di aritmie sintomatiche o altre malattie cardiache
bull Bilancio elettrolitico alterato
bull Alterate funzioni renale o epatica
bull Ipotirodismo
01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
24
Classificazione
Esistono diverse forme di LQTS
congenite canalopatie (poche) interesse cardiologico
acquisite iatrogene (molte) interesse cardiologico e psichiatrico
Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Egrave con il QT lungo cosa succede
01102010
25
Lrsquoallungamento dellrsquointervallo QT
puograve esacerbare una Triggered
activity ossia la comparsa di
ldquopost-potenziali tipicamente
precoci
Questi sono anormale oscillazioni
del potenziale di membrana che
seguono un potenziale drsquoazione A
differenza dellrsquoautomaticitagrave i post-
potenziali dipendono dal
precedente potenziale drsquoazione (il
trigger) e lrsquoaritmia che ne risulta
mantiene una relazione con esso
Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Torsione di punta e adesso
01102010
26
O termina o innesca un rientro che
determina un fibrillazione ventricolare con
exitus del paziente se non defibrillata
Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Quanto egrave grande il problema
01102010
27
Un QT marcatamente prolungato spesso accompagnato da torsioni di punta puograve accadere nellrsquo1-10 dei pazienti che ricevono farmaci antiaritmici noti per prolungare il QT ma egrave molto piugrave raro nei pazienti che ricevono farmaci ldquonon cardiovascolari ldquo che potenzialmente prolungano il QT
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il problema egrave principalmente correlato a farmaci cardiologici che prolungano il QT per loro stesso meccanismo drsquoazione questi farmaci andrebbero iniziati in ambiente ospedaliero con monitoraggio ECG
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
Problema limitato in psichiatria
01102010
28
Abstract
BACKGROUND Psychotropic drugs have the potential for QT interval prolongation the frequency is not known The aim of this study was to monitor the occurrence of QT interval prolongation in a non-selected population of patients treated with psychotropic drugs with proarrhythmic potential
METHODS In consecutive patients hospitalized at psychotic wards at the Department of Psychiatry treated with antipsychotic and antidepressant drugs with known or unexplored proarrhythmic potential a 12-lead ECG was recorded (50 mms 20 mmmV) on therapy the QT interval was measured manually corrected according to Bazett and Fridericia QTc intervals of 470 ms (females) and 450 ms (males) were considered borderline longer QTc intervals were considered pathologic
RESULTS ECGs were recorded in 452 patients (187 females 265 males aged 43+-16 years) Using Bazetts correction abnormal QTc values were observed only in 2 of the whole group and in 18 of the patients treated with drugs associated with QT prolongation (the greatest QTc value is 490 ms in female and 480 ms in male) With Fridericias correction there was only 1 case of borderline QTc in the whole group (the greatest QTc value is 450 ms in both sex groups)
CONCLUSIONS Our 2-year real-life experience shows that occurrence of QTc prolongation in present psychiatric patients is low Values associated with high risk of arrhythmias (QTcgt500 ms) were not observed This might be related to the recent changes of spectrum of antipsychotic therapy used the general trend to use lower doses and increasing awareness about the drug-induced long QT syndrome
Int J Cardiol 2007 May 2117(3)329-32 Epub 2006 Jul 24 Monitoring of QT interval in patients treated with psychotropic drugs Novotny T Florianova A Ceskova E Weislamplova M Palensky V Tomanova J Sisakova M Toman O Spinar J
Abstract
Although intravenous haloperidol (HAL) is an effective medication that is often prescribed to treat agitation several instances of torsade de pointes or prolonged QT interval have been reported To investigate the association between intravenous HAL and QT prolongation and between intravenous HAL and ventricular tachyarrhythmia a cross-sectional cohort study was performed that included measuring corrected QT intervals (QTc) on an emergency basis before intravenous HAL and continuously monitoring electrocardiographic (ECG) findings after intravenous HAL During a 2-month period 47 patients received intravenous injections to control psychotic disruptive behavior According to clinical practice patients were divided as follows The FZ-alone group was treated with intravenous flunitrazepam (FZ) and the FZ-plus-HAL group received intravenous FZ followed by intravenous HAL Although the difference in the mean QTc immediately after intravenous FZ between the two groups was not significant the mean QTc after 8 hours in the FZ-plus-HAL group was longer than that in the FZ-alone group (p lt 0001) Four patients in the FZ-plus-HAL group had a QTc of more than 500 msec after 8 hours The change in QTc during 8 hours significantly differed between the two groups (t = 264 p gt 005) Furthermore the change in QTc was moderately correlated with the dose of intravenous HAL as evidenced by a coefficient of correlation of 048 (p lt 0001) However ventricular tachyarrhythmia was not detected among 307 patients within a 1-year period although the ECG was continuously monitored for at least 8 hours after intravenous HAL The modest nature of QTc prolongation and the apparent absence of ventricular tachyarrhythmia under continuous ECG monitoring indicate that QTc prolongation associated with intravenous HAL is not necessarily dangerous However in an emergency situation clinicians cannot exclude patients predisposed to torsade de pointes such as those with inherited ion channel disorders Therefore clinicians should be aware of the association between intravenous HAL and QT prolongation
J Clin Psychopharmacol 2001 Jun21(3)257-61The association between intravenous haloperidol and prolonged QT interval Hatta K Takahashi T Nakamura H Yamashiro H Asukai N Matsuzaki I Yonezawa Y Department of Psychiatry Tokyo Metropolitan Bokuto General Hospital Japan hattak8scdmbnorjp
Abstract BACKGROUND Antipsychotic agents have been associated with a prolonged QT interval Data on the effects of ziprasidone and haloperidol on the QTc interval are lacking OBJECTIVE This study aimed to characterize the effects of 2 high-dose intramuscular injections of ziprasidone and haloperidol on the QTc interval at T(max) METHODS This randomized single-blind study enrolled patients with schizophrenia or schizoaffective disorder in whom long-term antipsychotic therapy was indicated Patients were randomized to receive 2 high-dose intramuscular injections of ziprasidone (20 and 30 mg) or haloperidol (75 and 10 mg) separated by 4 hours The primary outcome measure was the mean change from baseline in QTc at the T(max) of each injection Each dose administration was followed by serial ECG and blood sampling for pharmacokinetic determinations Twelve-lead ECG data were obtained immediately before and at predetermined times after injections ECG tracings were read by a blinded central reader Blood samples were obtained immediately before and after injections Point estimates and 95 CIs for mean QTc and changes from baseline in QTc were estimated No between-group hypothesis tests were conducted For the assessments of tolerability and safety profile patients underwent physical examination including measurement of vital signs clinical laboratory evaluation and monitoring for adverse events (AEs) using spontaneous reporting RESULTS A total of 59 patients were assigned to treatment and 58 received study medication (ziprasidone 31 patients haloperidol 27 age range 21-72 years 79 male) After the first injection mean (95 CI) changes from baseline were 46 msec (04-89) with ziprasidone (n = 25) and 60 msec (14-105) with haloperidol (n = 24) After the second injection these values were 128 msec (67-188) and 147 msec (102-192) respectively Mild and transient changes in heart rate and blood pressure were observed with both treatments None of the patients had a QTc interval gt480 msec Two patients in the ziprasidone group experienced QTc prolongation gt450 msec (457 and 454 msec) and QTc changes that exceeded 60 msec (62 and 76 msec) relative to the time-matched baseline values With haloperidol QTc interval values were lt450 msec with no changes gt60 msec Treatment-emergent AEs were reported in 29 of 31 patients (935) in the ziprasidone group and 25 of 27 patients (926) in the haloperidol group most events were of mild or moderate severity Frequently reported AEs were somnolence (903 and 815 respectively) dizziness (226 and 74) anxiety (161 and 74) extrapyramidal symptoms (65 and 333) agitation (65 and 185) and insomnia (0 and 148)CONCLUSIONS In this study of the effects of high-dose ziprasidone and haloperidol in patients with schizophrenic disorder none of the patients had a QTc interval gt480 msec and changes from baseline QTc interval were clinically modest with both drugs Both drugs were generally well tolerated
Clin Ther 2010 Mar32(3)472-91 Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration a randomized single-blind parallel-group study in patients with schizophrenia or schizoaffective disorder Miceli JJ Tensfeldt TG Shiovitz T Anziano RJ OGorman C Harrigan RH
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
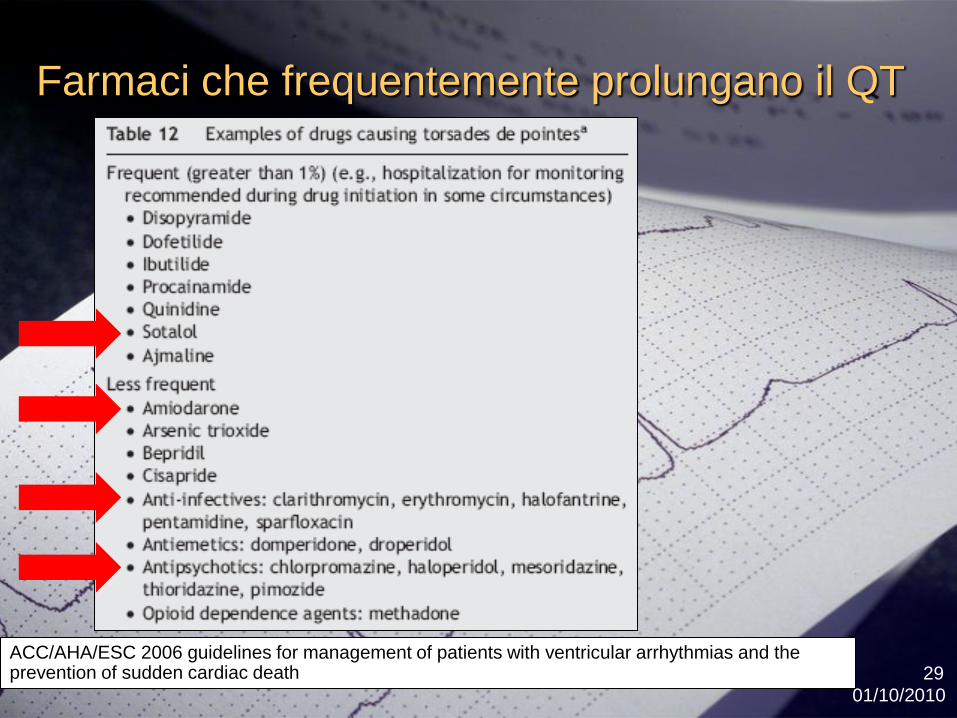
Farmaci che frequentemente prolungano il QT
01102010
29ACCAHAESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death
ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

ALOPERIDOLO
01102010
30
antagonista dopaminergico non selettivo
+
antagonista a-adrenergico
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
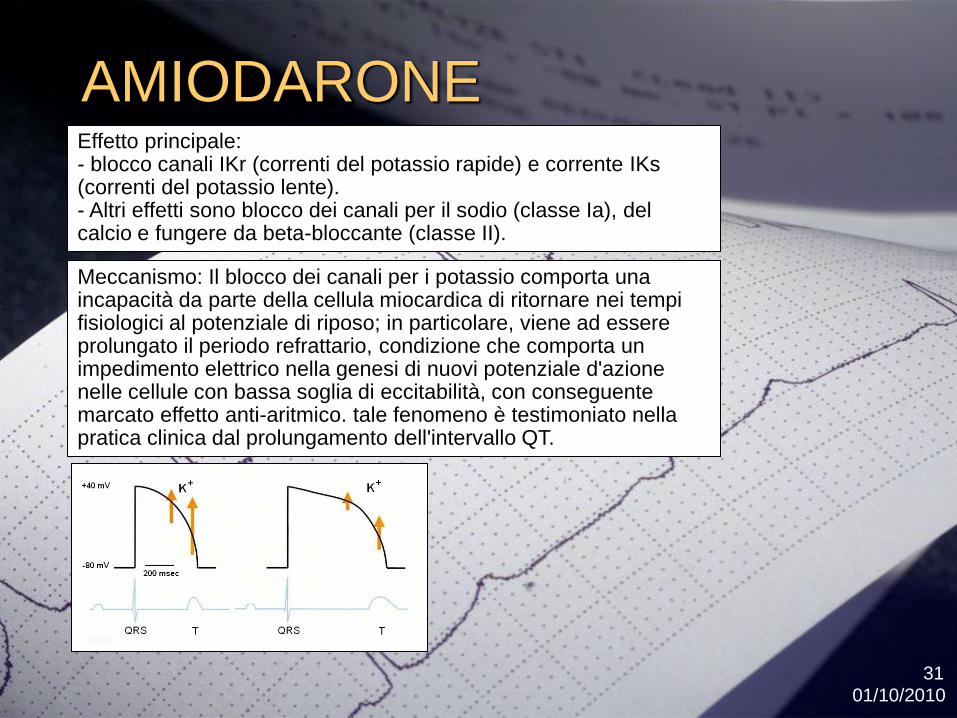
AMIODARONE
01102010
31
Effetto principale - blocco canali IKr (correnti del potassio rapide) e corrente IKs (correnti del potassio lente)- Altri effetti sono blocco dei canali per il sodio (classe Ia) del calcio e fungere da beta-bloccante (classe II)
Meccanismo Il blocco dei canali per i potassio comporta una incapacitagrave da parte della cellula miocardica di ritornare nei tempi fisiologici al potenziale di riposo in particolare viene ad essere prolungato il periodo refrattario condizione che comporta un impedimento elettrico nella genesi di nuovi potenziale dazione nelle cellule con bassa soglia di eccitabilitagrave con conseguente marcato effetto anti-aritmico tale fenomeno egrave testimoniato nella pratica clinica dal prolungamento dellintervallo QT
SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

SOTALOLO
01102010
32
Beta bloccante non selettivo
+
Bloccante canali del potassio
01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
33
Farmaci con rischio di TDP
wwwtorsadesorg
Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Un paziente ldquoverordquo della cardiologia UCIC
rianimazione o medicina generalehellip
Anziano con infezione respiratoria in FA cronica con
agitazione psicomotoria (notturna)
Ersquo sotto cordarone (FA) ha iniziato la claritromicina
da tre giorni e nella notte diamo il Serenase ivhellip
Nella pratica clinica
Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Nuovi farmaci confronti
01102010
35
Curr Drug Saf 2010 Jan5(1)97-104 QT alterations in psychopharmacology proven candidates and suspects Alvarez PA Pahissa J Department of Internal Medicine CEMIC Buenos Aires Argentina palvarezcemiceduar
Abstract
Psychotropics are among the most common causes of drug induced acquired long QT syndrome Blockage of Human ether-a-go-go-related gene (HERG) potassium channel by psychoactive drugs appears to be related to this adverse effect Antipsychotics such as haloperidol thioridazine sertindole pimozide risperidone ziprasidone quetiapine olanzapine and antidepressants such as amitriptyline imipramine doxepin trazadone fluoxetine depress the delayed rectifier potassium current (IKr) in a dose dependent manner in experimental models The frequency of QTc prolongation (more than 456 ms) in psychiatric patients is estimated to be 8 Age over 65 years tricyclic antidepressants (TCA) thioridazine droperidol olanzapine and higher antipsychotic doses were predictors of significant QTc prolongation In large epidemiological controlled studies a dose dependent increased risk of sudden death has been identified in current users of antipsychotics (conventional and atypical) and of TCA Thioridazine and haloperidol shared a similar relative risk of SCD Lower doses of risperidone had a higher relative risk than haloperidol for cardiac arrest and ventricular arrhythmia No increased risk was identified in current users of selective serotonin reuptake inhibitors (SSRI) Cases of TdP have been reported with thioridazine haloperidol ziprazidone olanzapine and TCA Evidence of QTc prolongation with sertindole is significant and this drug has not been approved by the Food and Drugs Administration (FDA) A large trial is ongoing to evaluate the cardiac risk profile of ziprazidone and olanzapine Selective serotonin reuptake inhibitors have been associated with QTc prolongation but no cases of TdP have been reported with the use of these agents There are no reported cases of lithium induced TdP Risk factors for drug induced LQT syndrome and TdP include female gender concomitant cardiovascular disease substance abuse drug interactions bradychardia electrolyte disorders anorexia nervosa and congenital Long QT syndrome Careful selection of the psychotropic and identification of patients risk factors for QTc prolongation is applicable in current clinical practice
Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Raccomandazioni specifiche del AIFA
Sullrsquoutilizzo di
Serenase
Droperidolo
Primozide
Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Raccomandazioni
01102010
37
ACCAHAESC 2006 guidelines for management of patients with
ventricular arrhythmias and the prevention of sudden cardiac death
Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Il mio paziente ha il QT lungo
cosa faccio
01102010
38
1- sospensione dei farmaci implicati nellrsquoallungamento del tratto QT
2- il mantenimento di livelli di concentrazione di K+ plasmatici tra 4 ndash 45 mmolL
3- la somministrazione di 1 ndash 2 g di solfato magnesio EV con possibilitagrave di aumentare la dose e la velocitagrave drsquoinfusione in base alla gravitagrave del quadro clinico
4- in caso di refrattarietagrave al trattamento e di concomitante bradicardia puograve essere drsquoaiuto il ldquopacing cardiaco temporaneordquo o lrsquoisoproterenolo
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
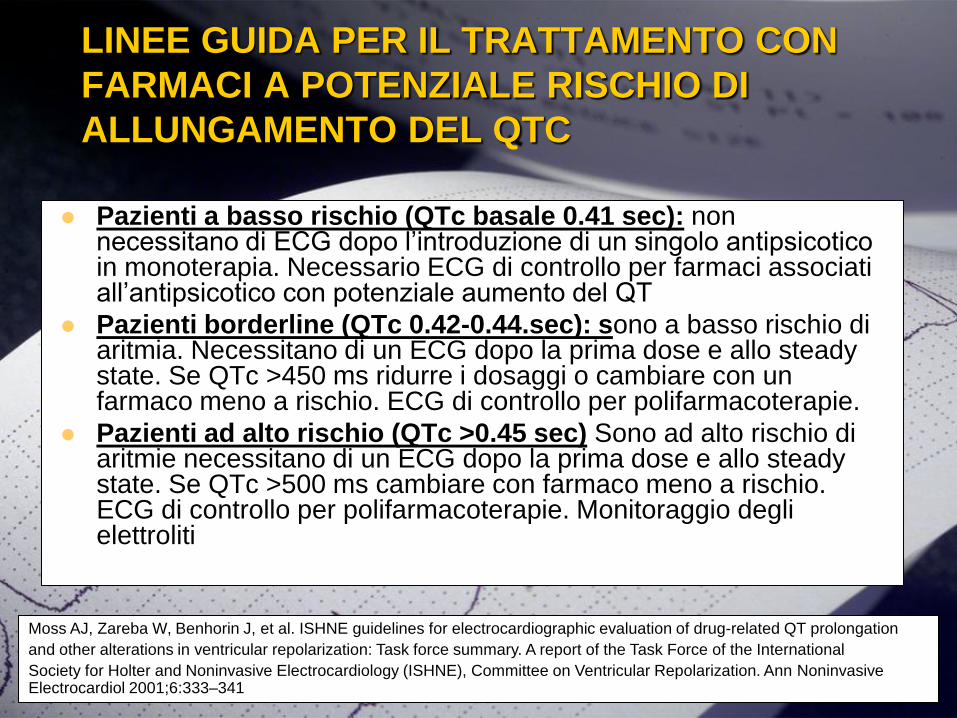
LINEE GUIDA PER IL TRATTAMENTO CON
FARMACI A POTENZIALE RISCHIO DI
ALLUNGAMENTO DEL QTC
Pazienti a basso rischio (QTc basale 041 sec) non necessitano di ECG dopo lrsquointroduzione di un singolo antipsicotico in monoterapia Necessario ECG di controllo per farmaci associati allrsquoantipsicotico con potenziale aumento del QT
Pazienti borderline (QTc 042-044sec) sono a basso rischio di aritmia Necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt450 ms ridurre i dosaggi o cambiare con un farmaco meno a rischio ECG di controllo per polifarmacoterapie
Pazienti ad alto rischio (QTc gt045 sec) Sono ad alto rischio di aritmie necessitano di un ECG dopo la prima dose e allo steady state Se QTc gt500 ms cambiare con farmaco meno a rischio ECG di controllo per polifarmacoterapie Monitoraggio degli elettroliti
Moss AJ Zareba W Benhorin J et al ISHNE guidelines for electrocardiographic evaluation of drug-related QT prolongation
and other alterations in ventricular repolarization Task force summary A report of the Task Force of the International
Society for Holter and Noninvasive Electrocardiology (ISHNE) Committee on Ventricular Repolarization Ann Noninvasive Electrocardiol 20016333ndash341
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
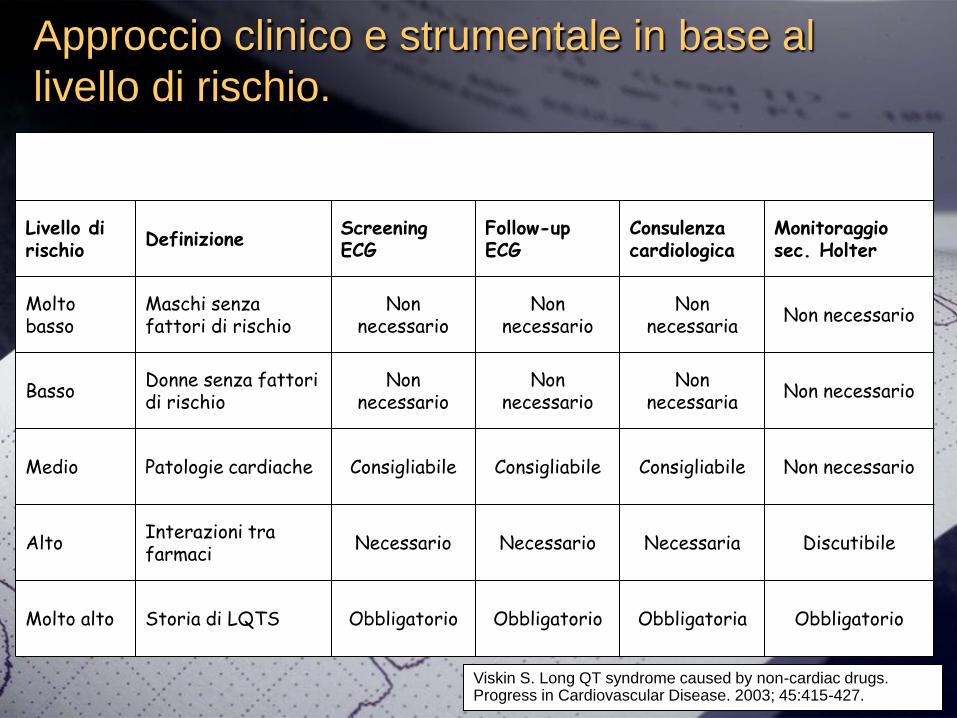
Livello di rischio
DefinizioneScreening ECG
Follow-up ECG
Consulenza cardiologica
Monitoraggio sec Holter
Molto basso
Maschi senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
BassoDonne senza fattori di rischio
Non necessario
Non necessario
Non necessaria
Non necessario
Medio Patologie cardiache Consigliabile Consigliabile Consigliabile Non necessario
AltoInterazioni tra farmaci
Necessario Necessario Necessaria Discutibile
Molto alto Storia di LQTS Obbligatorio Obbligatorio Obbligatoria Obbligatorio
Approccio clinico e strumentale in base al
livello di rischio
Viskin S Long QT syndrome caused by non-cardiac drugs Progress in Cardiovascular Disease 2003 45415-427
01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
41
Il farmaco che sto dando
prolunga il QT
wwwqtdrugsorg
wwwtorsadesorg
Su questi siti si trova una lista sempre aggiornata dei farmaci che possono prolungare il QT
E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

E il QT corto
01102010
42
La sindrome del QT breve egrave una patologia ereditaria a carattere autosomico dominante
Si caratterizza per la presenza sullrsquoecg di
base di un intervallo QT spiccatamente
breve ed una propensione a sviluppare
aritmie ipercinetiche a livello atriale eo
ventricolare in assenza di anomalie
strutturali cardiache
01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
43
ECG QT corto
bull Intervallo QT breve genericamente le 300 ms che non cambia in maniera significativa con il ritmo cardiaco
bull Si possono notare in oltre onde T alte ed appuntite
bull Alcuni individui possono anche presentare fibrillazione atriale sottostante
01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

01102010
44
Basi genetiche
Basi genetiche della Short QT SyndromeWilde AAM e Coll Heart 2005911352-1358
Le mutazioni nei geni KCNH2 KCNJ2 e KCNQ1 Questi geni codificano le proteine-canale di membrana del K
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49
01102010
45
Trattamento
Al momento lrsquounica azione terapeutica efficace per i soggetti affetti da sindrome del QT breve egrave lrsquoimpianto di un defibrillatore automatico
Trattamento mediante AICD
bull Lrsquounica ldquocoperturardquo sicuramente efficace nei pazienti considerati ad alto rischio in rapporto anche alla difficile valutazione della efficacia farmacologica
bull Sono stati segnalati diversi casi di ldquoShock inappropriato da doppio conteggio includente una onda T di elevato voltaggio
Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Trattamento
Un suggerimento da cardiologo
Provate a dare lrsquoaloperidolohellip magari si allunga il QT e risparmiamo un defihellip
Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Commenti conclusivi
Il QT lungo esiste nella misura in cui lo si misura Lrsquoocchio del cardiologo quasi non vede un QT lt500msec mentre lrsquoelettrocardiografo misura variazioni anche ldquoimpercettibilirdquo che spesso corrispondono allrsquoallungamento massimo che questi farmaci possono causare (40msc) sono sempre poi un quadratino da 1 mmhellip
Gli effetti cardiotossici avvengono quasi sempre in pazienti cardiopatici con farmaci antiaritmici in politerapia o con disturbi elettrolitici
Quando vi arriva un referto ECG con diagnosi di QT lungo spesso egrave giagrave soppesato dal cardiologo Il significato egrave = sospendi il farmaco
Non sottovalutare il QT lungo ma valutalo insieme al cardiologo
Le dimostrazioni del nesso tra lrsquoallungamento del QT e la morte cardiaca sono note ma lrsquoincidenza (NNT - NNH) egrave poco conosciuta poicheacute molto bassa Infatti le torsioni di punta da antipsicotico sono molto molto rare
0110201047
La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

La riflessione di un cardiologo
Il possibile rischio cardiologico conferito da questi farmaci egrave comunque MINORE del sicuro effetto dei fattori di rischio convenzionali tra i quali il fumo sedentarietagrave il sovrappeso e lrsquoipertensione o della sindrome metabolica spesso presenti nei pazienti psichiatrici
01102010
Grazie dellrsquoattenzione
01102010
49

Grazie dellrsquoattenzione
01102010
49