ottimizzazione della terapia nel paziente complesso€¦ · ottimizzazione della terapia nel...
45
Transcript of ottimizzazione della terapia nel paziente complesso€¦ · ottimizzazione della terapia nel...

category HbA1c target statin
1. healthy < 7.5 yes
2. complex / intermediate healthy < 8.0 yes
3. very complex / poor health < 8.5 consider

0.4
75 80 85 90 95
0.6
0.8
1.0
1.2
1.4
0.4
75 80 85 90 95
0.6
0.8
1.0
1.2
1.4
0.4
75 80 85 90 95
0.6
0.8
1.0
1.2
1.4
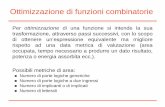
Statins for primary prevention in old adults
0.4
75 80 85 90 95
0.6
0.8
1.0
1.2
1.4
no diabetes type 2 diabetes
age age
Ramos R. et al.: BMJ 362:k3359, 2018 doi: 10.1136/bmj.k3359.
all
cause m
ort
ality
Hazard
Ratio
CV d
isease
Hazard
Ratio

ADA/EASD

Step 1: assess cardiovascular diseasePresence of cardiovascular disease is compelling indication
ASCVD PREDOMINATES HEART FAILURE (HF) PREDOMINATES
GLP-1 RAwith provenCVD benefit1
SGLT2-iwith proven
CVD benefit1-2
if eGFR adequate
orGLP-1 RAwith provenCVD benefit1
SGLT2-iwith proven
CVD benefit2-3
if eGFR adequate
or
if further intensification is required or patient is unable to tolerate GLP-1 RA and/or SGLT2-i, choose agents demonstrating CV safety:• consider adding the other class with proven CVD benefit• DPP4i if not on GLP-1 RA• basal insulin4
• TZD5
• SU6
• Avoid TZD
• consider adding the other class with proven CVD benefit1
• DPP4i (not saxagliptin) if not on GLP-1 RA• basal insulin4
• SU6
Choose agents demonstrating CV safety:
1. SGLT2-i = empagliflozin preferred, GLP-1 RA = liraglutide preferred. Proven CVD benefit means it has label indication of reducing CVD events. 2. Be aware that SGLT2-i vary by region and individual agent with regard to indicated level of eGFR for initiation and continued use. 3. Both empagliflozin and canagliflozin have shown reduction in HF in CVOT trial. 4. Degludec or U100 glargine have demonstrated CVD safety. 5. Low dose may be better though less well studied for CVD effect. 6. Choose later generation SU with lower risk of hypoglycaemia.
if HbA1c above target if HbA1c above target

ADA/EASD

Terapia farmacologica nell’anziano:Principali fattori da considerare:
• rischio di ipoglicemia
• insufficienza renale
• pregresso ictus/IMA
• storia di scompenso cardiaco
• profilo glicemico
• riserva funzionale beta cellula
• stato nutrizionale
• facilità di somministrazione

SIGG-SID per la terapia del diabete

obiettivi e terapia del diabete
obiettivodi glicata
farmaco peril diabete

obiettivi e terapia del diabete
farmaco peril diabete
obiettivodi glicata
a rischiodi ipoglicemia
NON a rischiodi ipoglicemia
• SUs• repaglinide• insulina
• metformina• SGLT-2i• DPP-4i• GLP-1 RA• pioglitazone• acarbosio
HbA1c < 7% HbA1c 7.0 – 7.5 %
HbA1c 7.5 – 8.0 %
2a scelta1a scelta
se fragile

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina
SU e glinidi
pioglitazone
Gliptine
GLP-1 RA
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi
pioglitazone
Gliptine
GLP-1 RA
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone
Gliptine
GLP-1 RA
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007

events
%
0
5
10
25
30
0 12 18 366
pioglitazoneplacebo
months
PROACTIVE: primary outcome
24
20
15
HR 95% CI p value
pioglitazone vs placebo
0.904 0.802, 1.018 0.0951
Dormandy JA et al.: Lancet 366:1279, 2005

events
%
0
5
15
0 12 18 366
pioglitazone
months
PROACTIVE: MACEMI, stroke and CV mortality
24
10
pio vs. placeboHR 0.82
(0.70-0.97)p=0.02
Wilcox R. et al AHJ 155:712, 2008
placebo

PROACTIVE: Heart failure risk
Erdmann E et al.: Diabetes Care 30:2773, 2007
events
%
0
2
4
6
0 12 18 30 366
pioglitazone
placebo
months
24

Heart Failure CV diseaseAll cause mortality
No treat. 1.00 1.00 1.00
Metformin0.68 *
(0.65 to 0.71)
0.76 *
(0.74 to 0.79
0.64 *
(0.63 to 0.66
SUs1.00
(0.94 to 1.07)
1.00
(0.95 to 1.05)
1.24 †
(1.20 to 1.28)
Insulin1.26 †
(1.10 to 1.44)
1.22 †
(1.08 to 1.37)
1.64 †
(1.55 to 1.74)
Glitazones0.50 *
(0.26 to 0.97)
0.79
(0.53 to 1.18)
0.89
(0.67 to 1.18)
Gliptins0.87
(0.58 to 1.31)
1.14
(0.85 to 1.54)
1.20
(1.00 to 1.44)
Hippisley-Cox J et al.: BMJ 354:i3477, 2016
diabetes treatments and CV riska cohort (469,688) study in primary care in UK

months
IRIS primary endpoint(stroke or MI, fatal or non-fatal)
Insulin Resistance Intervention after Stroke
Kernan WN et al. NEJM 374:1321, 2016
years 50 1 2 3 4
0
3
6
9
12
15
18
pioglitazone
placebo
patients
with e
vents
(%)
pio vs. placeboHR 0.76
(0.62-0.93)p=0.007
insulin-resistant, non-diabetic subjects

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone NO no<15 SI SI digiuno si
Gliptine
GLP-1 RA
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007

gliptin vs. glipizideadd-on to metformin
%
6.0
7.5
8.0
7.0
6.5
weeks
glipizide + met
6 5230 380 12 18 24 46
Nauck MA Diab Ob Metab 9:194, 2007
sitagliptin 100 mg + met
0
10
20
30
40
n episodes
hypos
titrated glipizide + met

gliptins: efficacy according to basal HbA1cthe higher is HbA1c, the higher is efficacy
Reductions are placebo-subtractedNauck MA Diab Ob Metab 9:194, 2007
-2.0
-1.5
-1.0
-0.5
0
<8 8-9 >9
Δ%
HbA1c
sitagliptin 100 mg + met

TECOS: Primary CV Outcome PP Analysis for Non-inferiority
events
%
0
5
10
15
0 2 3 41
sitagliptinplacebo
years
Green JB et al. NEJM 2015* CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina

SAVOR: Hospitalization for HF
0%
1%
2%
3%
4%
5%
0 180 360 540 720 900Ho
sp
ita
liza
tio
n f
or
HF
Days
Saxagliptin Placebo
Scirica BM, et al. November 2013. HR: hazard ratio

TECOS: First hospitalization for HF
TECOS, McGuire DK et al.: JAMA Cardiol 1:126, 2016years
410 2 3
patients
with e
vents
(%)
5
4
3
2
1
0
placebo
sitagliptin

CARMELINA hHF
Linagliptin event rate 2.77/100 PY Placebo event rate 3.04/100 PY Treated set, Kaplan-Meier estimate. Hazard ratio and 95% CI based on Cox regression model with terms for treatment group (p=0.2635), region (p=0.0012), history of heart failure (p≤0.0001); *Two-sidedhHF, hospitalization for heart failureRosenstock J et al. JAMA 2018; doi: 10.1001/jama.2018.18269
HR 0.90
(95% CI 0.74, 1.08)
Years
Pa
tie
nts
wit
h e
ve
nt
(%)
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.50
5
10
15
Placebo
Linagliptin

gliptins: time to insulin initiation
0%
10%
20%
30%
40%
0 1 2 3 4 5 6 7
patients
requirin
g insulin
initia
tion
years
N=7,728 sulphonylureas
sitagliptin
Valensi P et al. for The Odyssee Observational Study: Diabetes Metab 41:231, 2015

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone NO no<15 SI SI digiuno si
Gliptine NO SI NO dig/pra SI si
GLP-1 RA
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007
farmacidiversi

short and long-acting GLP-1R agonistsShort-acting GLP-1
RALong-acting GLP-1 RA
FPG reduction + +++
PPG reduction +++ ++
HbA1c reduction ++ +++
Body weight reduction ++ ++
Gastric empting rate +++ +
fasting glucagon secr. +/Neutral ++
GI effects ++ +
Compliance + ++

LEADER: primary composite CV outcome
MACE 3: CV death, non-fatal MI or stroke
years
50 1 2 3 4
0
3
6
9
12
15
18
liraglutide
placebo
Marso SP et al.: NEJM 375:311, 2016
HR: 0.8795% CI: 0.78.097p<0.001 for non-inferiorityp=0.01 for superiority
patients
with e
vents
(%)

months2460
placebo
semaglutide
12 18patients
with e
vent
(%)
SUSTAIN6: MACE (primary outcome)CV Death, Nonfatal Myocardial Infarction or Nonfatal Stroke
Marso SP et al.: NEJM 375:1834, 2016
Hazard ratio, 0.74 (95% CI, 0.58–0.95) P<0.001 for noninferiorityP=0.02 for superiority
10
8
6
4
1
0

HARMONY OUTCOMESMACE CV death
MI stroke
Hernandez AF et al.: Lancet. 2018 Oct 1. doi: 10.1016/S0140-6736(18)32261-X

REWIND press release

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone NO no<15 SI SI digiuno si
Gliptine NO SI NO dig/pra SI si
GLP-1 RA NO NO NO vario SI
Gliflozine
Insulina bas
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007
farmacidiversi
farmacidiversi
farmacidiversi

CANVAS & EMPAREGMACE 3: CV death, non-fatal MI or stroke
EMPAREG, Zinman B et al.: NEJM 373:2117, 2015CANVAS, Neal B et al.: NEJM Jun 12, 2017
years
5 610 2 3 4
patients
with e
vents
(%)
20
16
12
8
4
0
EMPAREG:99 % with previous CV event
CANVAS:65 % with previous CV event
placebo
canagliflozin
empaglifllozin

Zinman B et al.: NEJM 373:2117, 2015
9
8
7
6
5
4
3
2
1
0
empagliflozin
placebo
1 2 3 40
HR 0.62(95% CI 0.49, 0.77)
p<0.0001risk reduced by 38%
patients
with e
vent
(%)
years
EMPAREG: CV mortality

FINALLY!happy doctors

DECLARE has the broadest representation of the T2D patients with CV risk among the of the SGLT2i CV outcomes studies
CV, cardiovascular; SGLT2, sodium glucose co-transporter 2; T2D, type 2 diabetes; eCVD, established CV disease.
1. Zinman B, et al. N Engl J Med 2015;373:2117–2128;; 2. Neal B, et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1611925;3. SattarDiabetologia (2013) 56:686–695 4. Raz I, et al. Diabetes Obes Metab 2018. http://dx.doi.org/10.1111/dom.13217
.
34%of patients did not have eCVD
~60%of patientsdid not have eCVD
1%of patients
did not have eCVD
The proportion of patients with and without established CV disease varied across the three SGLT2 CV outcome studies
EMPAREG(N=7,020)
CANVAS(N=10,142)
DECLARE(N=17,160)

In this low CV risk population, dapagliflozin patients had a significant reduction of hHF/CV death and fewer MACE events compared to placebo
N at risk is the number of subjects at risk at the beginning of the period. 2-sided p-value is displayed; HR, CI, and p-value are from cox proportional hazard model.
CV, cardiovascular; Dapa, dapagliflozin; hHF, hospitalization for heart failure; MACE, major adverse cardiac event
Wiviott SD et al. Online ahead of print. N Engl J Med. 2018
hHF/CVD
HR 95% CI P value
0.83 (0.73, 0.95) 0.005Patients
with e
vent
(%)
6
0 1 2 3 4 5
4
2
0
Placebo (496 Events)
DAPA 10 mg (417 Events)
yearsPatients
with e
vent
(%)
10.0
0 1 2 3 4 5
7.5
5.0
2.5
0.0
Placebo (803 Events)
DAPA 10 mg (756 Events)
MACE
HR 95% CI P value
0.93 (0.84, 1.03) 0.172
years

hHF per CV history
Dapagliflozin prevents hHF consistently across a broad range of T2D patients regardless of history of eCVD or HF
Overall population
CV, cardiovascular; eCVD, established CV disease; HF, heart failure; hHF, hospitalized heart failure; SGLT-2i, SGLT co-transporter 2 inhibitor; T2D, type 2 diabetes
Wiviott SD et al. Online ahead of print. N Engl J Med. 2018
0.78 (0.63, 0.97)
Hazard ratio (95% CI)
Favors Dapagliflozin
Favors Placebo
0.64 (0.46, 0.88)
0 0,5 1 1,5
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
CV history
0.73 (0.61, 0.88) Overall population
0 0,5 1 1,5
0.73 (0.55, 0.96)
Hazard ratio (95% CI)
Favors Dapagliflozin
Favors Placebo
Prior HF*
0.73 (0.58, 0.92)No prior HF
*10% of patients in DECLARE had prior HF
hHF per HF history
0.73 (0.61, 0.88)
HF history

The renal protective effects of dapagliflozin were similar across baseline CV risk subgroup
CV, cardiovascular; eCVD, established CV disease; HF, heart failure; hHF, hospitalized heart failure; SGLT-2i, SGLT co-transporter 2 inhibitor; T2D, type 2 diabetes
Wiviott SD et al. Online ahead of print. N Engl J Med. 2018
0.79 (0.66, 0.94)
Hazard ratio (95% CI)
Favors Dapagliflozin
Favors Placebo
0.74 (0.60, 0.91)
0 0,5 1 1,5 0 0,5 1 1,5
0.55 (0.41, 0.75)
Hazard ratio (95% CI)
Favors Dapagliflozin
Favors Placebo
0.51 (0.37, 0.69)
composite Renal & CV death composite Renal
Overall population
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
CV history
0.76 (0.67, 0.87) 0.53 (0.43, 0.66)Overall population
Established CV Disease (eCVD)
Multiple Risk Factors (No eCVD)
CV history
composite Renal: composite of ≥40% decrease in eGFRa to <60 mL/min/1.73 m2, ESRD, or renal death

add on tomonotherapy
efficacy of gliflozins in various settingscompared vs. placebo at 24 weeks
-0,23-0,3
-0,04-0,13
-0,42-0,3
-0,89 -0,84
-0,45
-0,82
-0,97-0,9
-1,2
-1
-0,8
-0,6
-0,4
-0,2
0
1Ferrannini E, et al. Diabetes Care 2010;33:2217-24. 2Bailey CJ, et al. Lancet 2010;375:2223-33. 3Jabbour et al., Diabetes Care, pub online 15Jan2014 ; 4Strojek K, et al. Diabetes Obes Metab 2011;13:928-38. 5Rosenstock J, et al. 71st ADA Scientific Sessions, San Diego, 24-28 June, 2011 Abstract 0986-P. 6Wilding J, et al. Diabetes. 2010;59 (Suppl 1):A21-A22. Abstract 0078-OR.
HbA1c (
%)
met gliptin SU pio insulin

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone NO no<15 SI SI digiuno si
Gliptine NO SI NO dig/pra SI si
GLP-1 RA NO NO NO vario SI
Gliflozine NO NO SIpreviene
!dig/pra si
Insulina bas
farmacidiversi
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007
farmacidiversi
farmacidiversi

Terapia farmacologica nell’anziano
rischio di IPO
uso in IRC
prevCVD
scompcard
fenotipo
glicriserva β-cell
stato nutr.
facilitàsomm. fragile
Metformina NO no<30 SI NO digiuno XR
SU e glinidi SIsolo
gliclaziderischio neutro vari SI no
pioglitazone NO no<15 SI SI digiuno si
Gliptine NO SI NO dig/pra SI si
GLP-1 RA NO NO NO vario SI
Gliflozine NO NO SIpreviene
!dig/pra si
Insulina bas SI SI NO NO dig prandiale no obbligato?
farmacidiversi
Management of Diabetes in Older AdultsSesti G. et al.: NMCD 28:206, 2018 doi: 10.1016/j.numecd.2017.11.007
farmacidiversi
farmacidiversi

Migliorare qualità della VITA
Evitare ipoglicemieEvitare i sintomi della iperglicemia
Evitare reazioni avverse
Prevenire rischio cardiovascolare
Prevenire il calo ponderale eccessivo
Prevenire complicanze vascolari
Valutazione comprensiva BIOLOGICA-PSICOLOGICA-SOCIALE
Scelta del miglior rapporto rischio beneficiopossibile
conoscere il PAZIENTE conoscere i FARMACI
obiettivi della personalizzazione della terapia nell’ anziano diabetico
take home messages

team diabete
Gian Pio
Francesca
Flavia
Ilaria Teresa Simona
RacheleChiara
Serena