Nursing Network News - Breast Cancer Now · 2016-04-12 · 4 Nursing Network News A view from…...
32
ISSUE 20 • MARCH 2016 IN THIS ISSUE 10 19 22 Nursing Network Awards Nursing Network News San Antonio Breast Cancer Symposium Lymphoedema Q&A
Transcript of Nursing Network News - Breast Cancer Now · 2016-04-12 · 4 Nursing Network News A view from…...

ISSUE 20 • MARCH 2016
IN THIS ISSUE
10
19
22
Nursing Network Awards
Nursing Network News
San Antonio Breast Cancer Symposium
Lymphoedema Q&A

2 Nursing Network News
Section
References1. Paik S et al. N Engl J Med 2004; 351: 2817-2826; 2. Dowsett M et al. J Clin Oncol 2010; 28: 1829-1834; 3. Paik S et al. J Clin Oncol 2006; 24: 3726-3734; 4. Albain KS et al. Lancet Oncol 2010;11: 55-65.
The ONLY multi-gene assay that helps to identify patients at risk of distant recurrence1,2 and patients who are likely, or unlikely, to bene� t from chemotherapy3,4
Intended for newly diagnosed patients with early-stage, ER-positive, HER2-negative invasive breast cancer that is node negative or with 1-3 positive nodes1,2
This piece is intended to educate physicians on the clinical utility of the Oncotype DX® Breast Cancer Assay and should not be provided to patients. Genomic Health and Oncotype DX are registered trademarks of Genomic Health, Inc. © 2015 Genomic Health, Inc. All rights reserved.
Visit us at www.oncotypeDX.com
DECIDE WITH CONFIDENCETMINFORMING LIFE DECISIONS
GHI10448_0215_EN_INT
An individual question...
...An individual answer
D O I N E E D C H E M O T H E R A P Y ?
150209_GHI10448_0215_EN_INT_advert_195x130.indd 1 06.03.2015 10:25:05
Contact uswww.breastcancercare.org.ukFree Helpline 0808 800 6000(Text Relay 18001)
Calls may be monitored for training purposes. Confidentiality is maintained between callers and Breast Cancer Care
Nursing Network and professional developmentTelephone 0345 092 0802Email [email protected]
Scotland and Northern IrelandTelephone 0345 077 1892Email [email protected]
Wales, South West and Central EnglandTelephone 0345 077 1894Email [email protected]
East Midlands and the North of EnglandTelephone 0345 077 1893Email [email protected]
London and the South East of EnglandTelephone 0345 077 1895Email [email protected]

www.breastcancercare.org.uk 3
References1. Paik S et al. N Engl J Med 2004; 351: 2817-2826; 2. Dowsett M et al. J Clin Oncol 2010; 28: 1829-1834; 3. Paik S et al. J Clin Oncol 2006; 24: 3726-3734; 4. Albain KS et al. Lancet Oncol 2010;11: 55-65.
The ONLY multi-gene assay that helps to identify patients at risk of distant recurrence1,2 and patients who are likely, or unlikely, to bene� t from chemotherapy3,4
Intended for newly diagnosed patients with early-stage, ER-positive, HER2-negative invasive breast cancer that is node negative or with 1-3 positive nodes1,2
This piece is intended to educate physicians on the clinical utility of the Oncotype DX® Breast Cancer Assay and should not be provided to patients. Genomic Health and Oncotype DX are registered trademarks of Genomic Health, Inc. © 2015 Genomic Health, Inc. All rights reserved.
Visit us at www.oncotypeDX.com
DECIDE WITH CONFIDENCETMINFORMING LIFE DECISIONS
GHI10448_0215_EN_INT
An individual question...
...An individual answer
D O I N E E D C H E M O T H E R A P Y ?
150209_GHI10448_0215_EN_INT_advert_195x130.indd 1 06.03.2015 10:25:05
Contents News
4 A view from…
Denise Flett, young women’s breast nurse at the Royal Marsden Hospital
5 Our work for 2016 on secondary breast cancer
Breast Cancer Care’s policy aims for people with secondary breast cancer
8 Policy news in brief
9 Healthcare professional annual conference
A summary of our annual conference held in November last year
10 Nursing Network Awards
Read about the 2015 awards and last year’s winners
Sharing practice
14 Choosing not to reconstruct post mastectomy
A study on younger breast cancer patients who have opted not to have reconstruction following a mastectomy
16 Younger Women with Secondaries Together (YWST)
An evaluation of the free two-day event run by Breast Cancer Care
19 San Antonio Breast Cancer Symposium
Dr Emma Pennery, CBE, discusses presentations from the conference
Learning Together
22 Lymphoedema Q&A
Experts answer questions about lymphoedema after breast cancer
26 Sequencing of chemotherapy and radiotherapy for women following surgery for early breast cancer
A summary of the Cochrane Review
28 What is metastatic spinal cord compression?
Read about symptoms, diagnosis and management of MSCC
30 Breast Cancer Care’s spinal cord compression card
Breast Cancer Care has worked with a specialist to develop an alert card
About Breast Cancer CareBreast Cancer Care is the only UK-wide charity providing specialist support and tailored information for anyone affected by breast cancer.
Editorial boardDr Emma Pennery CBE, Clinical Director; Katie Parsons, Editor.
FeedbackThis is our 20th issue of Nursing Network News and we’d love to know what you think. Please email [email protected]
Your viewsWe’re always looking for contributions for future issues. If you have an idea you’d like to share with network members, please get in touch at [email protected]
Contents

4 Nursing Network News
A view from…
Denise Flett, young women’s breast nurse, Royal Marsden Hospital. Denise talks about attending a Breast Cancer Care Younger Women Together event.My role at the Royal Marsden as young women’s breast nurse is a new post that works in alliance with the breast clinical nurse specialist team, to deliver the best treatment whilst supporting complex, emotional and challenging needs of this patient group. Lack of connectivity and isolation are often key themes of distress described by these patients.
This position commenced in March 2015, and in April 2015 I was privileged to attend a Breast Cancer Care Younger Women Together event in London. These events are aimed at women aged 20–45 who have been diagnosed with primary breast cancer in the last three years. They’re held at various locations around the UK including London, Bristol, Liverpool, Leeds, Cambridge, Cardiff and Edinburgh.
The two-day symposium includes an overnight stay and an evening group dinner to offer the attendees some social time and an opportunity to connect and share experiences with other participants. All this incredible hospitality is organised and funded by the charity. Prior to the event attendees can connect on Breast Cancer Care’s online forum, allowing an opportunity to meet with a familiar person on the day.
The two-day programme is excellent, with key topics related to clinical management of breast cancer, wellbeing and side effects of breast cancer treatment such as menopausal symptoms, fertility and sexuality.
The delivery combined lectures and informal breakout groups, all led by
notable experts including consultant oncoplastic breast surgeon Jennifer Rusby, specialist oncology dietician Suzy Coughlan, oncologist Dr Judy King, gynaecology clinical nurse specialist Andreia Fernandes and of course Breast Cancer Care’s clinical nurse specialist for younger women, Grete Brauten-Smith.
But is wasn’t all sitting and talking. Therapeutic laughter practitioner Robin Graham had us all laughing and bonding, followed later with independent cancer exercise specialist Lizzy Davis facilitating a group workout, which was enthusiastically received by all.
Many of the young women I spoke to felt the fertility information was particularly relevant and important. I think this validates the important work that Breast Cancer Care and its Younger Women’s Champion Group have achieved in the development of Breast Cancer Care’s Fertility Toolkit, a tool to aid in streamlining fertility preservation referrals: www.breastcancercare.org.uk/fertility-toolkit
Younger Women Together is an excellent face-to-face opportunity for women under 45 who have been treated for early breast cancer to connect and learn more about breast cancer treatment and management of the many consequences.
It is a great resource to offer patients, in addition to the other Breast Cancer Care networking services such as the online Forum and Someone Like Me service (see www.breastcancercare.org.uk).
A view from...

www.breastcancercare.org.uk 5
Our work for 2016 on secondary breast cancer
Danni Manzi, Head of Policy and Campaigns, talks about Breast Cancer Care’s policy aims in 2016.As some of you may recall, in 2015 Breast Cancer Care launched its bucket list campaign for secondary breast cancer, with the aim of outlining the key things that need to change for those diagnosed and living with the disease.
We know many people living with secondary breast cancer experience poor levels of care and support (especially when compared to early stage disease) so we created our own bucket list of changes we want to see:
•No one living in unnecessary pain.•Everyone having access to the
treatments they need.•All patients having a clinical nurse
specialist as part of their care.•Hospitals being able to plan services
to meet patients’ needs.•Everyone’s care being co-ordinated
and joined up.
Through the bucket list campaign, Breast Cancer Care was able to raise awareness of the needs of those living with and affected by secondary breast cancer at some of the highest levels, culminating in an exchange between the Prime Minister and Jeremy Corbyn, Leader of the Labour Party, at Prime Minister’s Questions.
In 2016, we’re building on our achievements with three exciting new pieces of work.
Campaign on secondary breast cancer dataWe’ll be launching a campaign on secondary breast cancer data. Despite it being mandatory in England for hospitals to collect data, we know this is not happening consistently. It is impossible to know from existing statistics the number of people diagnosed with secondary breast cancer in any given year, which in turn makes it almost impossible to understand patient needs, or plan services effectively. We have called on the government for some time to ensure that data is properly collected and although such data has been planned for publication, no such information has been forthcoming.
With this in mind, we are working with our vibrant and committed campaigns community and supporters. Individuals will write to their local hospital trusts to find out which trusts are collecting data and what the picture is for diagnosis rates of secondary breast cancer locally. We want to use this information to gather a national picture, and to go back to Government and NHS England about increasing the pace of change and making this a priority. The learning from this campaign in England will also support our work in Scotland and Wales.
News
continued overleaf »

6 Nursing Network News
Understanding patient experience and needs for those with secondary breast cancerBreast Cancer Care’s secondary breast cancer taskforce undertook its work in 2006-2008. Since then, the landscape for health has changed immeasurably, with the co-ordination and integration of care becoming more difficult, and budgets and resource coming under increased pressure.
We will undertake a piece of work that identifies what the issues and challenges are for people living with secondary breast cancer in England, Scotland and Wales today. An online and postal survey will be made available to patients and the results will give us an up-to-date picture about experiences of care and treatment, as well as the impact of living with the disease, from diagnosis onwards. We will analyse (and continue to influence) what needs to change to put secondary breast cancer on a par with early stage disease.
Understanding the value and impact of dedicated secondary breast cancer nursesOur third piece of work is a new piece of research.
We know through Cancer Patient Experience Surveys that access to a clinical nurse specialist (CNS) has been shown to be the number one indicator of a positive patient experience. A CNS can provide invaluable support and help guide patients through the health system. However, we also know that a secondary breast cancer patient is far less likely to have access to a dedicated CNS than a primary breast cancer patient.
Breast Cancer Care believes that everyone should have a CNS involved in their care. However, we’re also aware that there’s a range of different models and roles in existence for secondary breast cancer and that little research has been done on the value and impact they bring to patients. The research we have commissioned will therefore seek to evidence the value and impact of different models of nursing provision for secondary breast cancer patients.
News
Who’s counting?

www.breastcancercare.org.uk 7
It will take place in two key phases. Firstly, the researchers will map out the different models of nursing provision in place for secondary breast cancer patients in England. We will also seek to undertake a similar mapping exercise in Scotland and Wales.
The researchers will then work at up to 10 hospital sites to look in depth at different models of nursing available for secondary breast cancer patients. These models could range from a key worker role, to a dedicated CNS for secondary breast care, to a CNS that supports patients with any type of breast cancer – primary, recurrent or secondary disease. The research will
gather both quantitative and qualitative data and will identify similarities, differences, and trends against key outcomes and experience measures.
This research will give Breast Cancer Care significant opportunity to progress current thinking and understanding in this area, as well as the opportunity and argument we need to affect real change in the field of secondary breast cancer nursing. We feel certain that this research will be welcomed by key stakeholders, within and beyond the NHS, and will influence government thinking.
News
Tofindoutmoreaboutanyaspectsofourworkonsecondarybreastcancer, ortoregisteryourinterestinourresearch,pleasedropusalineat [email protected] or call 0345 092 0800.
Catherine Priestley, Clinical Nurse Specialist – Secondary Breast Cancer, Breast Cancer Care

8 Nursing Network News
Policy news in brief
A summary of policy aims and developments from Breast Cancer Care.
Cancer Drugs Fund update Over the last few months, NICE and NHS England have been consulting on proposed changes to the way the Cancer Drugs Fund (CDF) works in England.
The CDF in its current form is due to end on 31 March 2016. The consultation put forward suggested changes to the CDF, to come into effect from 1 April 2016. The main change is that the CDF becomes a ‘managed access’ fund, through which drugs are tested out before going back to NICE for a final appraisal.
We responded to the consultation, and included within our response a range of feedback from people affected by breast cancer. You can view our response on our website at www.breastcancercare.org.uk/get-involved/campaign-us/what-we-think
If the planned changes go ahead, drugs which are currently on the CDF will be reassessed during the course of 2016/17. For secondary breast cancer, these are:
•eribulin (Halaven)•pertuzumab (Perjeta)•everolimus (Afinitor)• trastuzumab emtansine (Kadcyla or
TDM-1).
Once a final decision has been made, if a drug is removed, no new patients will have access to the drug. However, patients currently receiving drugs on the CDF during this phase will continue to have access to them for as long as it is clinically appropriate.
For more information about the changes, see our guide on our website, or email [email protected]
Wigs and prostheses for black,Asianandminorityethnic(BAME)womenWe’re working with NHS England to look at access to wigs and prostheses for BAME women. We’ve heard from patients that it can be difficult to find an appropriate wig or a prosthesis to match their skin tone. NHS England is looking into whether they should develop guidance for Clinical Commissioning Groups on this topic. We’d be really interested to hear from you about any examples of good practice, or any issues you’re facing accessing appropriate wigs or prostheses for BAME women.
Get in touch with [email protected] to share your experience or to find out more information about the project.
Supporting people to create change We’re developing the way we support people affected by breast cancer to get involved with our policy and campaigning work. If you, or your patients, would like to find out more about our influencing work and how to get involved go to www.breastcancercare.org.uk/campaign to sign up to our regular newsletter full of information, support, and things you can do to help.
8 Nursing Network News
News

News
www.breastcancercare.org.uk 9
Healthcare professional annual conference: Friday 6 November 2015, Hotel Russell, London
Our annual conference for healthcare professionals took place on Friday 6 November, at the Hotel Russell in London.
We were delighted to welcome 200 breast care nurse specialists from across the UK to network with peers and hear presentations from a wide range of speakers. We’ve recorded the day and all the presentations will be available online.
On behalf of our team, I would like to thank you for an excellent annual conference. Everything was very well organised from the booking to the final goodbye at the end of the day. Each one of us was able to bring something back to our large team... as well as enhance our personal learning. Excellent informative speakers, great exhibition stands and not least a wonderful venue and food and drink.Kay,UniversityofLeicester
‘ ‘
OurNursingNetworkAwardwinnersfor2015werealsoannouncedontheday. Further information on the winners and their entries can be found overleaf.

10 Nursing Network News
Nursing Network Awards 2015
The Nursing Network Awards Winners were announced at our Healthcare Annual Conference on Friday 6 November 2015.
These Awards champion best practice in specialist breast care nursing and go to individuals or teams who have taken innovative ideas into practice, making a positive difference to patient care. Entries were judged by a panel of specialists from across the UK.
10 Nursing Network News
News
Thankyoutoeveryonewhoentered,andcongratulationstoourwinnersandhighly commended!
Gill Donovan Breast Oncology Nurse Specialist, Velindre Cancer Centre, Cardiff
Dr Julie Wray Senior Lecturer Multi-Professional Post-Graduate Studies, School of Nursing, Midwifery, Social work and Social science, University of Salford (patient representative)
DrEmmaPenneryCBE Clinical Director and Head of the Nursing Network, Breast Cancer Care
AmandaShewbridge Nurse Consultant in Breast Cancer, Guys and St Thomas’ NHS Foundation Trust
The judges

www.breastcancercare.org.uk 11
Nursing Network Award winners: Patient Support or Involvement
JOINTWINNER
ClaireLiu,NightingaleCentre,WythenshaweHospitalAwardedfor:Development of an educational resource employing a tablet device to display images of a variety of breast surgical procedures
The team wanted an efficient way of having huge numbers of photos at their disposal that could also be updated quickly. Patient needs were at the very core of the proposal and the judges were very impressed with their honesty, reporting on what went wrong, and their tenacity to overcome these issues as their route was not an easy one.
Judges thought the project was very sustainable with such good plans for evaluation.
JOINTWINNER
JaneWattsandRuthJohnson,FrimleyParkHospitalandRoyalSurreyCounty HospitalAwardedfor:Collaborative working to support metastatic breast cancer patients
An innovative project with two breast care nurses from different hospitals joining together to start a patient-led metastatic breast cancer support group. The judges were extremely impressed with their proposal that had patients at the core; a true collaboration with the linkage of two hospitals not usually joined or working together in this way.
News

Nursing Network Award winners: Team Initiative
WINNER
ClaireHerlihyandAmyBarrow,NorthDevonDistrictHospitalAwardedfor:Joint nursing initiative with the lymphoedema team
The judges were impressed at how the breast care nurses worked with patients to identify the gaps in their understanding of lymphoedema and the ongoing risk.
It was a great collaboration with the lymphoedema team as they obtained new equipment together and breast clinic slots were set aside where the lymphoedema team attended alongside the breast care nurses.
HIGHLYCOMMENDED
LindaHammel,StJohn’sHospital,LivingstonAwardedfor:High risk family history clinic
This team wanted to introduce designated pathways in relation to the revised NICE family history guidance, specifically:
•MRI imaging for high risk patients.•Chemo-prevention.
The judges were impressed that they redesigned their breast care nursing team and the responsibilities within the team to free up time to set up these clinical pathways. As far as we’re aware, this is the only unit in Scotland that has a structured pathway in chemo-prevention for high risk patients.
12 Nursing Network News
News
ThiswasthefirstyearwereceivedanyentriesfromScotland, and we had a total of three!

www.breastcancercare.org.uk 13
Celebrating the success of you and your team
Breast Cancer Care’s Nursing Network is our initiative for healthcare professionals working with breast cancer patients.It was created six years ago to give specialist breast care nurses the opportunity to come together to share best practice, develop skills and knowledge, and work more closely with us to ensure our services and campaigns are responsive to patient needs.
The Nursing Network Awards champion best practice in specialist breast care nursing, and recognise individuals or teams who have demonstrated innovative and successful nurse-led initiatives that have had a positive difference on patient care.
The awards are open to all Nursing Network members and are run bi-annually, so look out for details on how to enter the 2017 awards later this year.
News
Our healthcare professional training programme and the Nursing Network are generously supported byReferences
1. Paik S et al. N Engl J Med 2004; 351: 2817-2826; 2. Dowsett M et al. J Clin Oncol 2010; 28: 1829-1834; 3. Paik S et al. J Clin Oncol 2006; 24: 3726-3734; 4. Albain KS et al. Lancet Oncol 2010;11: 55-65.
The ONLY multi-gene assay that helps to identify patients at risk of distant recurrence1,2 and patients who are likely, or unlikely, to bene� t from chemotherapy3,4
Intended for newly diagnosed patients with early-stage, ER-positive, HER2-negative invasive breast cancer that is node negative or with 1-3 positive nodes1,2
This piece is intended to educate physicians on the clinical utility of the Oncotype DX® Breast Cancer Assay and should not be provided to patients. Genomic Health and Oncotype DX are registered trademarks of Genomic Health, Inc. © 2015 Genomic Health, Inc. All rights reserved.
Visit us at www.oncotypeDX.com
DECIDE WITH CONFIDENCETMINFORMING LIFE DECISIONS
GHI10448_0215_EN_INT
An individual question...
...An individual answer
D O I N E E D C H E M O T H E R A P Y ?
150209_GHI10448_0215_EN_INT_advert_195x130.indd 1 06.03.2015 10:25:05

Choosing not to reconstruct post mastectomy: Exploring younger women’s experiences
A team of researchers visited Breast Cancer Care recently to discuss their study on younger breast cancer patients who had chosen not to reconstruct post-mastectomy. Dr Fiona Holland from the University of Derby’s psychology department summarises the project and its implications.Of the 54,000 women diagnosed with invasive breast cancer in the UK per year, 20% are under the age of 501. 90% of these younger women have breast conserving surgery or mastectomy as part of their treatment2. Immediate or delayed breast reconstruction (IBR/DBR) are routinely conducted3,4 and often considered to be beneficial for psychological adjustment, especially in younger women5,6. Although data from the USA indicates that younger women are more likely to select reconstruction7, less than 50% of women worldwide reconstruct post-mastectomy.
Little is known about younger women’s experiences around this decision-making process. Our study aimed to explore the younger breast cancer patient’s perspective when reconstruction was not chosen. We focused on a sample of women recruited via the Breast Cancer Care web forum. The women had been diagnosed with primary breast cancer under the age of 50; all had undergone unilateral mastectomy at least five years previously. None had undergone IBR, although all were eligible for DBR. All lived and were treated in England. The age of the women at diagnosis ranged
from 31-46 years. The women were asked about decision-making when facing the loss of a breast, perception of self and body before and after their surgery, and support received around their decision to not pursue reconstruction.
FindingsDuring the initial consultation with their medical teams, both treatment and DBR were discussed. Several of the women reported this led to feeling a sense of pressure to make a decision to reconstruct while still experiencing the ‘angst’ that accompanied the news of their diagnosis. As it became apparent that IBR was not an option, the additional time between mastectomy and DBR provided an opportunity for them to think, gather more information, and evaluate their individual circumstances.
In some cases, there was a lack of information provided about life post-mastectomy without breast reconstruction; it was apparent that the majority of resources available, both formal and informal, tended to focus on reconstruction.
The messages reportedly received from some healthcare teams, particularly from surgeons, promoted reconstruction. Some of the women said their surgeons assumed they would want DBR even if this was not what they wanted.
The women described their interactions with breast care nurses as having more of a counselling role. Despite feeling supported in these conversations, some felt that nurses and support group facilitators were generally more
14 Nursing Network News
Sharing practice

www.breastcancercare.org.uk 15
pro-reconstruction. Some of the women described having to defend their decision not to reconstruct multiple times to their medical team who continued to question this. It was only through persistence and tenacity that these women felt their decision was finally accepted. This experience left the women with a sense of going against the perceived norm of reconstruction.
Implications for practiceFor this group of women DBR was not their preferred choice for a variety of reasons including avoiding additional healing and hassle, unwillingness to have an unnecessary cosmetic procedure, wishing to self-examine without any obstruction and not seeing reconstruction as a positive choice. Although they acknowledged that reconstruction was a valid option for some, they believed it should not be assumed that all women, even younger women, would want it.
Recommendations from this study include increasing the resources available that educate and support non-reconstruction as a permanent and acknowledged option even for younger women. The women in this study would have benefitted from seeing and being able to talk with women of a
similar age to them who had had both reconstruction and non-reconstruction. This would have positively informed their decision-making process and decreased their sense of being ‘odd’ and going against the perceived ‘norm’ of reconstruction. The women acknowledged the need for positive messages regarding non-reconstruction from their medical teams, and also from the media.
Some of the women highlighted the need for additional and independent counselling during their decision-making process. Practical information around prostheses, navigating relationships and accepting their new normal were discussed as necessary to promote a more positive experience. Support for partners was also suggested.
Moving forward, it’s recommended that medical teams and breast cancer support services review current practice and beliefs about the reconstruction process for women of all ages. Additionally, more information about the pros and cons of IBR and DBR could be presented. Having clear statistics on reconstruction rates for women, and being careful not to assume that younger women will automatically choose reconstruction would be positive changes for medical teams to make.
Sharing practice
References: 1 Cancer Research UK (2013). Breast Cancer Incidence Statistics. www.cancerresearchuk.org/cancer- info/cancerstats/types/breast/incidence/uk-breast-cancer-incidence-statistics (accessed 23/02/2016). 2 Lawrence G et al (2011) The Second All Breast Cancer Report. National Cancer Intelligence Network: London. 3 Morrow M et al (2009) Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA, 302(14): 1551-1556. 4 National Institute for Health and Clinical Excellence (NICE) (2009). Early and Locally Advanced Breast Cancer: Diagnosis and Treatment. National Collaborating Centre for Cancer: Cardiff, Wales. 5 Roje Z et al (2010). Breast Reconstruction after Mastectomy. Coll. Antropol, S1: 113-123. 6 Wilkin EG et al (2000) Prospective Analysis of Psychosocial Outcomes in Breast Reconstruction: One Year Postoperative Results from the Michigan Breast Reconstruction Outcome Study. Plastic and Reconstructive Surgery, 106(5): 1014-1025. 7 Jagsi R et al, (2014) Trends and Variation in Use of Breast Reconstruction in Patients With Breast Cancer Undergoing Mastectomy in the United States. Journal of Clinical Oncology, 32(9): 919-926. A full summary of the project and findings can be downloaded from the Breast Cancer Care website or by contacting [email protected]

Younger Women with Secondary breast cancer Together (YWST)
Last October Breast Cancer Care ran a free, two-day Younger Women with Secondary breast cancer Together (YWST) event in Manchester. This was following the successful pilot event in London in 2014.YWST was open to anyone aged 45 and under with a diagnosis of secondary breast cancer and 35 women attended, from across the UK. Some women had been given details about the event from their specialist nurse, but most had found out about it from Breast Cancer Care.
We often hear from this age group that they feel very isolated and would like to meet others in a similar situation and support and learn from each other. Furthermore when someone young is diagnosed with secondary breast cancer, specialist breast care nurses often contact us for a safe place to direct their patients to for additional support.
Throughout the event we wanted to create an environment where thoughts and fears could be openly discussed, especially as some concerns can be hard to share with family and friends. We certainly had a mixture of tears and laughter across the two days, with the women expressing their relief at sharing concerns and working out coping strategies.
The two-day programme was a balance of plenary sessions that allowed all the women to come together as a group, and breakout sessions that participants could choose based on their needs. A number of expert speakers including medical oncologists, clinical nurse specialists, counsellors and child bereavement specialists delivered these sessions. There was also plenty of time throughout the event for the women to get to know each other, share experiences and support each other, as well as plenty of rest time. Staff from our services team and two clinical nurse specialists from Breast Cancer Care specialising in secondary breast cancer and younger women were also on hand.
The plenary sessions covered the management of secondary breast cancer in younger women and current research. These sessions were extremely valued by the women. One described it as ‘cutting edge specific information’. The women also felt ‘hopeful’ and ‘reassured’ by the information provided about treatment options. One woman said this gave her ‘a greater understanding of my journey ahead’.
The Palliative Care session was also well received. The group explored common misconceptions, such as fearing that palliative care means imminent end
16 Nursing Network News
Sharing practice
One of my patients… gained valuable experience from the event… It has enabled them to have greater confidence in themselves and to come to terms with their diagnosis, which was this patient’s biggest hurdle.Rebecca, breast care nurse
‘ ‘

www.breastcancercare.org.uk 17
of life and no further treatment. It addressed the benefits of palliative care such as symptom control, quality of life and support for families. Several of the women felt able to seek palliative care support after the event as it no longer frightened them.
In order to best tailor the sessions about talking to children, we ran two groups, one for women with younger children and one for those with teenagers. These sessions were highly emotional.
One woman said ‘I really benefitted from speaking with the young children group.’ She added that it was a ‘safe space to talk.’ One discussion focused how much or how little information the women chose to give their children. Others talked about the guilt behind the decision not to make strong bonds with their new born children (18 months and younger) in order not to let them down in the future.
From the evaluations it was apparent that the opportunity to talk freely in a safe environment with other younger women was greatly valued. Several women discussed their experience of isolation as a younger woman with life-limiting illness. One said it was ‘good to meet other young women and realise
although our situations are different we share the same hopes and fears.’
Overall, these events have been a great success. Evaluations have shown that the women were hugely appreciative of the opportunity to connect, learn and share with others. All the women said they would recommend this service to other younger women with secondary breast cancer, and hoped that others like themselves could be given the opportunity to gain so much from future events. We hope to run this event yearly and are now planning the next one for April 2016 in London – so please keep this in mind when you see a younger woman with secondary breast cancer and help us continue to provide valuable support to others.
Sharing practice
Choosing the breakout groups beforehand meant the two days were tailored to my needs. The sessions were informative and educational. I left the event with a sense of optimism and I am pleased I attended.Fiona,attendee
‘ ‘Plenary
•Medical Update•Current Research
Breakout
•Adjusting / adapting to a life-limiting illness
•Palliative Care•Talking to Children•Relationships and
Communications•Sexuality and Intimacy•Laughter Workshop•Mindfulness•Exercise
Session topics

Come to a Younger Women Together event and meet other women under 45 who’ve been diagnosed with primary breast cancer.Whether you have questions about pain management, treatments and side effects, or just want to talk openly to others who have had a secondary diagnosis, these sessions can provide you with helpful information and support in a relaxed environment.
10June2016Younger Women Together London
4November2016Younger Women Together Bristol
23September2016Younger Women Together Leeds
3February2017Younger Women Together Liverpool
Visitourwebsitetofindoutmore:www.breastcancercare.org.uk/ywt
Younger women together events
18 Nursing Network News
Upcoming events
Come along to one of our Living with Secondary Breast Cancer meet-ups.These events have been designed to give you the chance to meet and share experiences with other people living with a secondary diagnosis, and get the information and support you need. Sessions take place on a monthly basis, at the following locations:
Bristol • Cardiff • Cornwall • Coventry (from May 2016) • Derby • Dorset Edinburgh • Forth Valley • Glasgow • Halifax/Huddersfield • Lanarkshire Leeds • Liverpool • Maidstone and Tunbridge Wells • Manchester Milton Keynes (from May 2016) • North London/Hertfordshire • Oxford Romford • Salisbury (from May 2016) • Sheffield • Sutton (South London) West Midlands • York/Harrogate
Visitourwebsitetofindoutmore:www.breastcancercare.org.uk/lwsbc
Living with secondary breast cancer events

www.breastcancercare.org.uk 19
Conference report: San Antonio Breast Cancer Symposium (SABCS) 2015
More than 8,000 delegates gathered for the 38th annual meeting of the SABCS in December last year. Dr Emma Pennery, CBE, describes some notable presentations from the conference.Smith,Betal.Complicationandeconomic burden of local therapy options for early breast cancer. AbstractS3‑07
This retrospective review compared complications (including infection, seroma, fat necrosis, and implant removal) and costs of local treatment options for breast cancer up to two years post diagnosis. It included patients having wide local excision +/- radiotherapy or mastectomy +/- reconstruction +/- radiotherapy.
Nearly 100,000 patients were selected from two US databases with a median age of 53 in one and 75 in the other, allowing comparisons between younger and older women.
The analysis revealed mastectomy plus reconstruction (without radiotherapy) had the highest complication rate in younger and older women – nearly twice that for breast conserving surgery plus radiotherapy. It was also the most expensive treatment in terms of complication-related costs.
Complication rates for all types of local therapy were higher in older women. Sixty five percent of older women had complications with mastectomy plus reconstruction compared to fifty four percent of younger women; and thirty seven percent of older women had
complications with breast conserving surgery plus whole breast radiotherapy, compared to twenty nice percent of younger women. Even in patients treated with mastectomy alone (no local adjuvant therapy) thirty seven percent of older women had complications compared to twenty five percent of younger women.
Gnant,Metal.TheImpactof adjuvant denosumab on disease‑freesurvival:Resultsfrom3,425postmenopausalpatientsoftheABSCG‑18trial.AbstractS2‑02
This study reported on patients enrolled in the ABSCG-18 trial, which randomised postmenopausal women with early breast cancer to adjuvant denosumab or placebo (in addition to an aromatase inhibitor).
Sharing practice
Key Points
•Older women have higher rates of shorter-term complications regardless of the type of local therapy.
• In older women, complications rates were equivalent for breast conserving surgery plus whole breast radiotherapy (38%) and mastectomy without reconstruction (37%).
•The review findings could help specialist nurses support patients to make informed treatment choices about type of local therapy.
continued overleaf »

Previous results had demonstrated the benefits of denosumab over placebo for bone health and reduced fracture risk but this analysis looked at disease-free survival.
The results showed women having denosumab had improved disease-free survival (borderline significant). The absolute benefit was 2.1% at 5 years.
Wildiers,Hetal.Trastuzumabemtansine improves overall survival versustreatmentofphysician’schoice in patients with previously treatedHER2‑positivemetastaticbreastcancer:Finaloverallsurvivalresultsfromthephase3TH3RESAstudy.AbstractS5‑05
The TH3RESA study compared trastuzumab emtansine (T-DM1) with treatment of physician’s choice in patients with HER2-positive, metastatic breast cancer, previously treated with a taxane (any setting), and both trastuzumab and lapatinib (advanced setting).
Earlier interim results from the TH3RESA study had shown the addition of T-DM1 almost doubled progression-free survival. But these final results found it also increases overall survival for pretreated patients with HER2-positive, metastatic breast cancer. Those having T-DM1 lived a median of 22.7 months versus 15.8 months in the other group;
and T-DM1 resulted in fewer severe side effects than other treatments.
The survival benefits were seen regardless of age, extent and location of metastatic disease and hormone receptor status.
Chandarlapaty,Setal.cfDNAanalysisfromBOLERO‑2plasmasamplesidentifiesahighrateofESR1mutations:Exploratoryanalysis for prognostic and predictive correlation of mutations revealsdifferentefficacyoutcomesof endocrine therapy–based regimens.AbstractS2‑07
There’s increasing interest in so-called liquid biopsies, which involve taking a blood sample to analyze trace amounts of tumour DNA.
This study looked at blood plasma in 541 patients with metastatic breast cancer already enrolled in the BOLERO-2 trial (comparing everolimus and exemestane versus exemestane and placebo).
The analysis found nearly 30% of patients had one or both of two specific mutations. The presence of these mutations increased the risk of relapse and reduced overall survival. Patients with neither mutation had a median overall survival of 32.1 months compared to 26 or 20 months in patients with one of either mutation and 15.2 months in patients with both.
But interestingly, the two mutations had quite different effects on response to treatment with everolimus. For patients with neither mutation, the overall effect of adding everolimus was to double progression-free survival from 3.9 months to 8.5 months. Similar effects were seen in patients with one specific or both mutations (improvements of around 2.5 to 5.5 months).
However, in patients with the other specific mutation, everolimus offered no benefit. Progression free survival was 4.1
20 Nursing Network News
Learning together
Key Points
•Adjuvant aromatase inhibitors may compromise bone health.
•Adjuvant denosumab improves disease free survival in postmenopausal patients with ER+ early breast cancer (data is still awaited on overall survival).
•The benefits of adjuvant denosumab are comparable with adjuvant bisphosphonates.

www.breastcancercare.org.uk 21
months with the drug and 4.2 months without. More research is needed to verify this finding but the implication is different mutations can have quite different effects on drug sensitivity.
Mutations found in liquid biopsies also predicted treatment success in another presentation (Baselga, J et al. Abstract S6-01). The researchers analysed blood samples from patients in the BELLE-2 trial, which is testing the safety and effectiveness of adding a drug called buparlisib to fulvestrant to treat women with ER+ breast cancer grown resistant to aromatase inhibitors. Patients with a mutated PIK3CA gene (around a third) had improved progression-free survival on buparlisib while those without the mutation derived no advantage from the drug.
Nielsen,Tetal.HighriskpremenopausalluminalAbreastcancerpatientsderivenobenefitfromadjuvanttherapy:resultsfromDBCG77Brandomisedtrial.AbstractS1‑08
Several studies have shown distinct breast cancer subtypes. The luminal A subtype has a favourable prognosis in comparison to luminal B, HER2 and basal-like subtypes.
This study involved a retrospective molecular analysis of premenopausal patients with axillary node positive or large primary breast cancer entered
into a trial conducted during the 1970s and 1980s. Nowadays a placebo arm in this setting would be considered unethical, but this older trial included randomisation to no chemotherapy.
The researchers found no difference in 10-year disease-free survival rates between women with luminal A disease who did and did not receive chemotherapy, suggesting they do not benefit from chemotherapy.
The authors cautioned the study did not mirror current standards of care (none of the women received adjuvant hormone therapy) but suggested there’s evidence withholding chemotherapy may be safe for young women with luminal A breast cancer.
Of course, genomic testing now plays an important part in helping to identify women with early breast cancer who may safely avoid chemotherapy. Specifically, two poster presentations on Oncotype DX provided additional evidence of the test’s ability to accurately predict patient outcomes. Each reported patients with low Recurrence Scores have less than 1% chance of distant recurrence at five years [Shak et al, Abstract P5-15-01, and Sparano et al, Abstract P2-08-01].
Learning together
Key Points
•Mutations can be found using a simple blood test (cheaper and less invasive than tissue biopsies).
•Different mutations have different implications for prognosis and specific treatment response, potentially guiding future treatment recommendations.

Lymphoedema: Q&A
A question and answer session on Lymphoedema with Professor Dominic Furniss and Mr Alex Ramsden, Consultant Plastic Surgeons at Oxford Lymphoedema Practice.
What are the chances of developing lymphoedema after breast cancer?DF: This is a very interesting question, and there is no perfect answer! The chances of developing lymphoedema depend on the treatment that has been given. If a woman has just had local treatment of the breast, then the chances of developing lymphoedema are low. However, many women with breast cancer require treatment of the lymph glands in the armpit, and this increases the risk of developing lymphoedema. If a woman requires an axillary node clearance, or has radiotherapy to the axilla, then the risk becomes high.
However, every woman is an individual. Some patients have minimal treatment and develop lymphoedema, whereas others have very invasive treatment, and don’t get lymphoedema. We don’t currently have the technology to predict who will be affected, which is why screening for lymphoedema and early treatment is so important.
Why does removing or treating the lymph nodes have such a devastating effectonpatients?AR: When blood goes into the arm, some of the fluid from the blood leaks out into the tissues to keep the body cells alive. This fluid has to find its way back into the blood stream – this is
where the lymphatic system comes in. It is a series of interconnected tubes that deliver the tissue fluid back to the bloodstream in the neck. Removing the lymph nodes in the armpit, or treating them with radiotherapy or chemotherapy, blocks this return causing fluid to build up in the arm. This fluid causes swelling that is often progressive, and can predispose to cellulitis. Patients’ quality of life can be severely reduced, with many people reporting that the swollen arm is a constant reminder of their cancer and its treatment. It can be devastating for women to be told that as a result of their treatment they have developed a condition that is chronic, progressive and incurable.
What are the early symptoms and risk factors for lymphoedema?DF: The early symptoms of lymphoedema are a dull aching feeling in the arm, often accompanied by a feeling of tightness or heaviness. Women commonly say that their arm “just doesn’t feel normal”. These feelings can affect a localized part of the arm, such as near the elbow. The feeling of tightness and heaviness happens before any measurable swelling occurs. It is really interesting when we undertake ICG lymphography in women with these symptoms, as patches of lymphoedema seen on the scan often precisely match the symptomatic areas.
The risk factors for developing lymphoedema are related to treatment of the breast cancer. In particular, surgery and radiotherapy to the armpit increases the risk of developing lymphoedema.
22 Nursing Network News
Learning together

www.breastcancercare.org.uk 23
Can you explain the screening programme? How successful is it and how often should you get screened?AR: The Oxford Lymphoedema Practice screening programme is the first of its kind in the UK. We use the latest ICG lymphography technology to image the function of the lymphatics in real time in the clinic. This can reveal the earliest signs of lymphoedema, even before the swelling can be seen. This allows us to intervene early in the course of the disease, potentially curing lymphoedema, stopping the patient needing other treatments. This is a real paradigm shift in the management of lymphoedema.
We recommend the first screening appointment at 3 months after breast cancer treatment is completed. If the scan is normal, we repeat screening every six months for three years, as this is the time when lymphoedema is most likely to develop.
Howdifferentisitthesedays treating someone with lymphoedemathanitwas10years ago? DF: Traditionally, a patient who developed swelling in their arm following breast cancer would be told that they have lymphoedema, it slowly will get worse and there is no cure. The only treatment available was a lifetime of compression garments and massage.
Today patients can be screened for early and accurate diagnosis. With that knowledge the patient is now empowered to choose between reliable and safe supermicrosurgical reconstruction that treats the underlying disease, or ICG guided massage. Supermicrosurgical techniques can prevent the development of the devastating symptoms of lymphoedema.
Learning together
Mr Alex Ramsden and Professor Dominic Furniss, Oxford Lymphoedema Practice
continued overleaf »

24 Nursing Network News
What is the success rate for lymphoedema surgery?AR: At the Oxford Lymphoedema Practice, we undertake a supermicrosurgical procedure called lymphaticovenular anastomosis (LVA). LVA is performed under local anaesthetic as a day case operation, and has the advantage of having low risks in combination with high success rates. Our figures show that 83% of all our patients have a measurable volume improvement with an average reduction in the excess limb volume of over 50%. The psychological aspects of lymphoedema are often underestimated but we have shown the overall quality of life in our patients increased by 30% after surgery. The outcomes vary depending on how severely affected the limb is initially but in patients who present early for surgery, we have successfully returned their arm to normal without the need for restrictive compression sleeves in the long term.
Where do you see the treatment for lymphoedema infiveyearstime?DF: The diagnosis and treatment of lymphoedema is a rapidly advancing and exciting area. New technology such as ICG and MRI lymphography are transforming our understanding of the disease and allowing rapid and accurate diagnosis. Advances in surgical microscopes and instruments will permit surgery to the lymphatic system to become routine, with very low risks and improved outcomes. Patients will be treated earlier, even before swelling appears, and potentially avoid the disabling symptoms of lymphoedema altogether. ICG lymphography will also guide and improve conservative treatments such as manual lymphatic drainage. These techniques are also used to treat lower limb lymphoedema following treatment of pelvic lymph nodes.
Learning together
By using ICG lymphography, the location of functioning lymphatics can be drawn on the skin, enabling LVA to be performed through small incisions under local anaesthetic

www.breastcancercare.org.uk 25
Dates for your diary
April201614April Teleconference: New developments in lymphoedema management, Professor Dominic Furniss, Associate Professor, Oxford University and Mr Alex Ramsden, Consultant Plastic and Microsurgeon, Oxford University Hospitals NHS Trust
November2016Nursing Network News Issue 22
June201621June Teleconference: Update on bone metastases, Dr Mark Harries, Consultant Medical Oncologist, Guys & St Thomas’ Hospitals NHS Foundation Trust
January2017January teleconference (details TBC)
July2016Nursing Network News Issue 21
February20174 February World Cancer Day
September201626September Teleconference: Fertility Preservation and breast cancer, Mr Stuart Lavery, Consultant Gynaecologist, Hammersmith Hospital
March2017Nursing Network News Issue 23
October2016Breast Cancer Awareness Month
Dates for your diary
Callfree08088006000www.breastcancercare.org.ukContact the Nursing Network team on 0345 092 0802 or at [email protected]

26 Nursing Network News
Sequencing of chemotherapy and radiotherapy for women following surgery for early breast cancer
This is a summary of a Cochrane Review.
BackgroundThe clinical outcome of sequencing chemotherapy (CT) and radiation therapy (RT) after surgical treatment in early breast cancer remains unclear. Several studies have suggested that adjuvant radiotherapy could be safely delayed until adjuvant CT was completed. Other studies report a delay with RT to give CT first results in an increased rate of local recurrence. Concomitant administration of the two treatments is also an option. This systematic review aimed to determine the effects of different sequencing of adjuvant CT and RT for women with early breast cancer.
Nurses play a key role in supporting the breast cancer patient at every stage of the disease process. Having clear treatment guidelines based on the best available evidence helps nurses in providing support to patients and families. Clarifying the uncertainty of outcome in the timing of interventions (RT, CT and concomitant CT and RT) will help both patients and clinicians make treatment decisions.
Objective/sTo determine the effects of different sequencing of adjuvant CT and RT for women with early breast cancer.
Intervention/MethodsThe intervention in this review includes current practices for the timing of RT and CT following breast-conserving surgery in early breast cancer. CT regimens included those administered at standard doses only. For one
sequencing method (RT followed by CT vs CT followed RT), anthracyclines but not taxanes were used. RT had to be delivered to the breast or chest wall, either including or excluding the supraclavicular fossa and axilla.
Randomised controlled trials (RCT) evaluating the three identified sequencing methods (administering CT before RT, administering CT and RT concurrently, or ‘sandwiching’ RT in the middle of the CT course) were eligible. The primary outcome includes local recurrence in the ipsilateral breast. Secondary outcomes such as overall survival, relapse-free survival and other treatment-related effects, quality of life, adherence and costs were also considered.
ResultsThe comparisons in this review are concurrent versus sequential treatment. Based on the three trials included, no significant differences were shown between the various methods of sequencing adjuvant therapy for local recurrence-free survival, overall survival, relapse-free survival and metastasis-free survival based on 1166 randomised women in three trials. Concurrent chemoradiation increased anaemia (1 study involving 710 participants), telangiectasia (1 study involving 214 participants) and pigmentation (1 study involving 211 participants). Treated women did not report worse cosmesis with concurrent chemoradiation but physician-reported assessments did. Other measures of toxicity did not differ between the two types of sequencing.
Learning together

www.breastcancercare.org.uk 27
On the basis of one trial (244 women), RT before CT was associated with an increased risk of neutropenic sepsis compared with CT before RT, but other measures of toxicity did not differ.
ConclusionsThis review included data from three well-conducted randomised trials. Findings imply that different methods of sequencing CT and RT do not appear to have a major effect on recurrence or survival for women with breast cancer if RT is commenced within seven months after surgery. The trials provided limited or no information regarding adverse events, side effects or quality of life associated with the different sequences of treatment. The limited evidence available does suggest that the frequency and severity of side effects of chemotherapy and radiotherapy are similar regardless of which sequence is used. However, it should be noted that the women in these trials were treated, on average, in the early 2000s. Therefore, the trials do not assess the modern types of radiotherapy, and newer regimens of chemotherapy. The review authors indicated that future updates of this review will include relevant trials with these more recent treatments available.
ImplicationsforPracticeThe review results showed that there were no significant differences between the three identified methods of adjuvant therapy in terms of local recurrence. While it may be safe to adopt or advocate any of the sequencing methods included in this review, the secondary outcomes should also be examined. For example, based on one study, anaemia increased with concurrent CT/RT while nausea/vomiting and grade III/IV skin, infection or oesophagitis did not. In RT followed by CT, neutropenic sepsis was worse but other measures of toxicity (pneumonia, skin and haematological toxicities) did not differ. Patients should be made aware of the degree of benefit of treatment, including timing of treatment.
The limitations of the review should also be taken into consideration. For example, there was no available data regarding the differences to the quality of life, costs and patient preferences. From a nursing perspective, further research should be done with a focus on how nurses can positively impact these outcomes.
Author: RhodaRedulla,DNP,RN‑BC MemorialHospitalofSalemCounty Salem,NJ,DrexelUniversity,Philadelphia,PA
Learning together
References: Hickey BE, Francis, DP, Lehman, Margot. (2013) Sequencing of chemotherapy and radiotherapy for early breast cancer. The Cochrane Collaboration: John Wiley & Sons, Ltd

28 Nursing Network News
What is metastatic spinal cord compression?
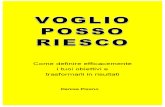
Kate Baker and Kathryn Elias discuss the symptoms and management of metastatic spinal cord compression.Metastatic spinal cord compression (MSCC) is defined as ‘spinal cord or cauda equina compression by direct pressure and/or induction of vertebral collapse or instability by metastatic spread or direct extension of malignancy that threatens or causes neurological disability’1.
In 2008 the National Institute of Health and Care Excellence (NICE) published MSCC guidelines to help healthcare professionals provide evidence-based care for the condition. As cancer survival rates continue to improve with advancing oncological treatments, the incidence of MSCC is increasing.
IncidenceAs cancer survival rates continue to improve with advancing oncological treatments, the incidence of MSCC is increasing. It’s a complex, debilitating complication of cancer affecting 5-14% of all patients and is deemed an oncological emergency1. Breast cancer patients are among the most common to develop MSCC.
Research has shown that approximately 23% of all MSCC’s are cancer of the unknown primary2. MSCC affects individuals physically, psychologically and socially. It can have a significant impact on quality of life and the ability of carrying out normal activities of daily living.
Signs and symptoms•Back pain in 83–95% of MSCC cases3.•Reduced muscle power in upper or
lower limbs.•Sensory changes including numbness
and pins and needles.•Bladder and bowel dysfunction
including urinary retention, and constipation or loss of bowel control.
Patients who have cancer that has spread to their bones, or who are at risk of this, should be given information, preferably in the form of an alert card and leaflet that explains what to do and who to contact if they develop symptoms of MSCC.
Learning together
References: 1 National Institute for Health and Clinical Excellence. Metastatic Spinal Cord Compression: diagnosis and management of patients at risk or with metastatic spinal cord compression. Clinical guidelines 75. 2008. 2 Levack P, Graham J et al. Don’t wait for a sensory level – listen to the symptoms: a prospective audit of the delays in diagnosis of malignant cord compression. Clinical Oncology. 2002. 14:472-80. 3 Sciubba DM, Gokaslan ZL. Diagnosis and management of metastatic spine disease, Surgical Oncology. 2006. 15:141-51. 4 Baur A, Stabler A et al. Acute osteoporotic and neoplastic vertebral compression fractures: fluid sign at MR imaging. Radiology. 2002. 225:730-5.

www.breastcancercare.org.uk 29
Investigations and diagnosisPrompt diagnosis is imperative to prevent irreversible neurological damage. Patients presenting with symptoms of MSCC should be referred for an urgent whole spine MRI scan within 24 hours of the onset of symptoms.
Management• If MSCC is suspected, patients should
be nursed flat.•Baseline neurological examination. •Dexamethazone 16mg stat dose then
8mg bd1.•Whole spine MRI (optimal imaging
modality for assessing spinal disease)4.
•Appropriate analgesia.•Formulate a treatment plan within
24 hours of diagnosis1, with consideration of a) surgical opinion and b) radiotherapy treatment.
RehabilitationAppropriate rehabilitation services, aids and adaptations, to maximise functional independence and quality of life.
Author: KateBaker&KathrynElias MetastaticSpinalCordCompression Service Improvement LeadsforSouthWales
Learning together
Breast Cancer Care has worked with Kate Baker to produce a Spinal Cord Compression alertcard.Readaboutitonthenextpage.
Spinal cord compression
Tumour
Vertebrae

30 Nursing Network News
Breast Cancer Care’s spinal cord compression card
As an oncological emergency, the key to treating or preventing spinal cord compression, avoiding permanent damage and retaining quality of life is early intervention. Patient education is critical to prompt reporting of symptoms, accurate diagnosis, intervention and rehabilitation. With this in mind, patients with known bone metastases and those with high risk tumour types should be educated on the importance of reporting symptoms early.
Nurses in inpatient and outpatient settings play an important role in early recognition of symptoms, patient and family education and co-ordination of appropriate care pathways. Knowing who is at high risk, providing information and educating these patients of the importance of reporting what may seem like minor symptoms is major step in early intervention. Time is crucial to positive outcomes and nurses can often help expedite these.
NICE (2008) guidelines state that patients should be informed if they are at risk of spinal cord compression, and provided with information on what symptoms to look out for and the need to alert the appropriate healthcare professional. In addition they affirm the importance of prompt recognition of symptoms by the primary care team and fast access to diagnosis and treatment.
NICE suggested that written information for patients is provided in the form
of an alert card or leaflet, along with who to contact to report symptoms immediately.
To help specialist teams facilitate patient education, Breast Cancer Care has worked with Kate Baker to produce a Spinal Cord Compression alert card.
The cards seek to remind patients they should seek medical attention from their specialist team or out of hours services straight away, rather than wait to see if the symptom improves or until their next hospital appointment.
Packed in 15’s these credit card sized cards can be given to patients who are at risk of MSCC, reminding them of the symptoms to report immediately.
On the reverse, information for healthcare professionals who may come into contact with patients reporting symptoms highlights the need for urgent investigation and possible treatment. A single copy of the card is also included in our new secondary breast cancer resource pack.
Learning together
Download or order our secondary breast cancer resource pack and other publications from our website www.breastcancercare.org.uk/publications
Resource pack
Living with secondary
breast cancer
Lorem ipsum dolore estes
Secondary breast
cancer in the boneThis booklet is for anyone
who has been diagnosed with
secondary breast cancer in
the bone. It describes what
secondary breast cancer in the
bone is, what the symptoms are
and the treatments that may
be used.
Secondary breast cancer
BCC30_Secondary in the bone_2015_final.indd 1
20/04/2015 15:11
Secondary breast cancerresource pack
Resource pack
For patients
You’ve been given this card because you have secondary breast cancer in the bone and are at risk of spinal cord compression.If you develop any of the following symptoms, contact your local Accident and Emergency Department or a doctor or nurse from your specialist team straight away.• Severe back pain, especially if it’s
different from any other pain you experience and/or affects the top part of your spine or neck.
• Pain in the back that changes when you lie down, stand up or lift something, or prevents you from sleeping.
• Pain which starts in the back and goes around the front to the chest and towards the belly.
• Pain or numbness extending down a leg or arm.
• Difficultly walking or feeling clumsy or weak – especially in the arms and legs.
• Difficulties going to the toilet, problems passing urine or opening the bowels.
For healthcare professionals
This patient has secondary breast cancer in the bone and is at risk of spinal cord compression. They may need an urgent MRI scan.They should be made comfortable and placed in a flat position to protect the spine.If spinal cord compression is confirmed they will need urgent treatment to prevent further damage to the spine.Further copies of this card can be obtained from www.breastcancercare.org.ukBCC231Registered charity in England and Wales 1017658 Registered charity in Scotland SC038104
front back


FINDAWALKNEARYOUBlenheimPalace,Oxfordshire14MayPolesdenLacey,Surrey21May
Chatsworth,Derbyshire4JuneStourhead,Wiltshire11June GlasgowatNight25JuneLondonatNight9July
Registered charity: England and Wales 1017658, Scotland SC038104. BCC351
Take on a 5, 10 or 20 mile Pink Ribbonwalk 2016 and help us be there for thousands of women affected by breast cancer.
SIGN UP TODAYbreastcancercare.org.uk/Ribbonwalk