Concetti chiave sulle “cosiddette” reazioni allergiche Antonino Romano [email protected].
La prevenzione primaria delle
malattie allergiche del bambino
Roberto BernardiniDirettore Unità Operativa Complessa di Pediatria
Nuovo Ospedale San Giuseppe, Empoli
Presidente della Società Italiana di Allergologia e ImmunologiaPediatrica
International Study of Allergy and Asthma in Childood(ISAAC)
Per quanto concerne i dati italiani, la prevalenza, nello studio ISAAC, di:
1) rinocongiuntivite allergica, presente negli ultimi 12 mesi, è del 6,6% nei bambini di 6-7 anni di età e del 17,4% nei bambini di 13-14 anni di età;
1) asma, presente negli ultimi 12 mesi, è dell’8,4% nei bambini di 6-7 anni di età e del 9,5% negli adolescenti di 13-14 anni di età.
Sestini P et al. La prevalenza di asma e allergie nei bambini e adolescenti italiani: i risultati del progetto SIDRIA-2. Epidemiol Prev 2005;29(2)Suppl:1-96.
Kostadinova AI, Willemsen LEM, Knippels LMJ, Garssen J. Immunotherapy – risk/benefit in food allergy. PediatrAllergy Immunol 2013;24:633-44.
Approx. 6% of children, vs. 3–4% of adults, suffer from allergy to food proteins.
The majority of food allergies (about 90%) are causedby milk, egg, peanut, tree nuts, wheat, soybeans, and seafood.
Cow’s milk and egg allergies are the most common foodallergies, but they are also more likely to be spontaneously outgrown with time (approx. 85%), while <20% of peanut and tree nut allergiesspontaneously resolve, but, on the contrary, are associated with persistency and the majority of life-threatening and fatal anaphylaxis.
Bambino a rischio di malattia allergica:bambino con almeno un consanguineo di 1° grado (genitori, fratelli)
affetto da patologia atopica.
COORDINATORIGiuseppe di MauroPresidente Società Italiana di Pediatria Preventiva e Sociale (SIPPS) Segretario Nazionale FIMP alle Attività Scientifiche ed Etiche Pediatra di Famiglia ASL Caserta- Regione Campania
Roberto BernardiniDirettore UOC Pediatria, Nuovo Ospedale San Giuseppe, EmpoliPresidente della Società Italiana di Allergologia e Immunologia Pediatrica
Salvatore BarberiClinica Pediatrica, Ospedale San Paolo, Università degli Studi di Milano
Annalisa Capuano Dipartimento di Medicina Sperimentale, Sezione di Farmacologia “L. Donatelli”, Seconda Università degli Studi di Napoli (SUN)
Elena Chiappini Dipartimento di Scienze della Salute, Università di Firenze, Ospedale Pediatrico Anna Meyer, Firenze
Antonio CorreraDirettore della UOC di Pediatria Generale e Neonatologia dell'Ospedale S.S. Annunziata di Napoli (AORN) Santobono-Pausilipon)
Gian Luigi de’ AngelisDirettore Dipartimento Materno Infantile dell’Azienda Ospedaliero-Universitaria di ParmaDirettore Gastroenterologia ed Endoscopia Digestiva e della Clinica Pediatrica
Iride Dello Iacono Responsabile UOS Pediatria e Allergologia - Ospedale Fatebenefratelli, Benevento
Maurizio De Martino Dipartimento di Scienze della Salute, Uni-versità di Firenze, Ospedale Pediatrico Anna Meyer, Firenze
Daniele GhiglioniDirigente Medico, Azienda Ospedaliera Fatebenefratelli e Oftalmico, Milano
Dora Di MauroSpecializzanda in Pediatria, Dipartimento Materno Infantile dell’Azienda Ospedaliero-Universitaria di Parma
Marcello GiovanniniProfessore emerito di Pediatria, Clinica Pediatrica, Ospedale San Paolo, Università degli Studi di Milano
Massimo LandiPediatra di Famiglia Asl TO1 - TorinoGian Luigi MarsegliaDirettore Clinica Pediatrica - Fondazione IRCCS Policlinico San Matteo Università degli Studi di Pavia
Alberto Martelli Responsabile U.O.C. Pediatria, Presidio Garbagnate Milanese – Bollate. Azienda Ospedaliera G. Salvini
Vito Leonardo Miniello Azienda Ospedaliero-UniversitariaConsorziale Policlinico di Bari - Ospedale Giovanni XXIII
Diego Peroni Professore, Clinica Pediatrica, Università di VeronaLucilla RicottiniPediatra, Roma
Maria Giuseppa Sullo Dipartimento di Medicina Sperimentale, Sezione di Farmacologia “L. Donatelli”, Seconda Università degli Studi di Napoli (SUN)
Luigi TerraccianoDirigente Medico, Azienda Ospedaliera Fatebenefratelli e Oftalmico, MilanoCristina Vascone Dipartimento di Medicina Sperimentale, Sezione di Farmacologia “L. Donatelli”, Seconda Università degli Studi di Napoli (SUN)
Elvira Verduci Ricercatore Universitario Clinica Pediatrica Ospedale San Paolo Dipartimento Scienze della Salute Università degli Studi di Milano
Maria Carmen VergaPediatra di famiglia, ASL Salerno Vietri sul Mare
SOCIETÀ SCIENTIFICHE, FEDERAZIONI E ASSOCIAZIONI RAPPRESENTATE Società Italiana di Pediatria, Società Italiana di Pediatria Preventiva e Sociale, Società Italiana di Allergologia e Immunologia Pediatrica
NOTA PER GLI UTILIZZATORIIl presente documento costituisce una versione integrale della Consensus che può essere scaricato nella sua interezza dal sito web della Società Italiana di Pediatria Preventiva e Sociale www.sipps.it sezione RIPPS
Nessun componente del panel ha dichiarato alcun conflitto di interesse relativamente all’argomento trattato
Iniziativa realizzata grazie al contributo incondizionato di



..the recent study, entitled “Randomized Trial of Peanut Consumption in Infants at Risk for
Peanut Allergy (Learning Early about PeanutAllergy —LEAP Trial)”, demonstrated a
successful 11–25% absolute reduction in the risk of developing peanut allergy in high-risk
infants if peanut was introduced between 4 and 11 months of age..
DuToit G et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015;372:803–813.Allergy 70 (2015) 1193–1195.
DuToit G et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015;372:803–813.Allergy 70 (2015) 1193–1195.
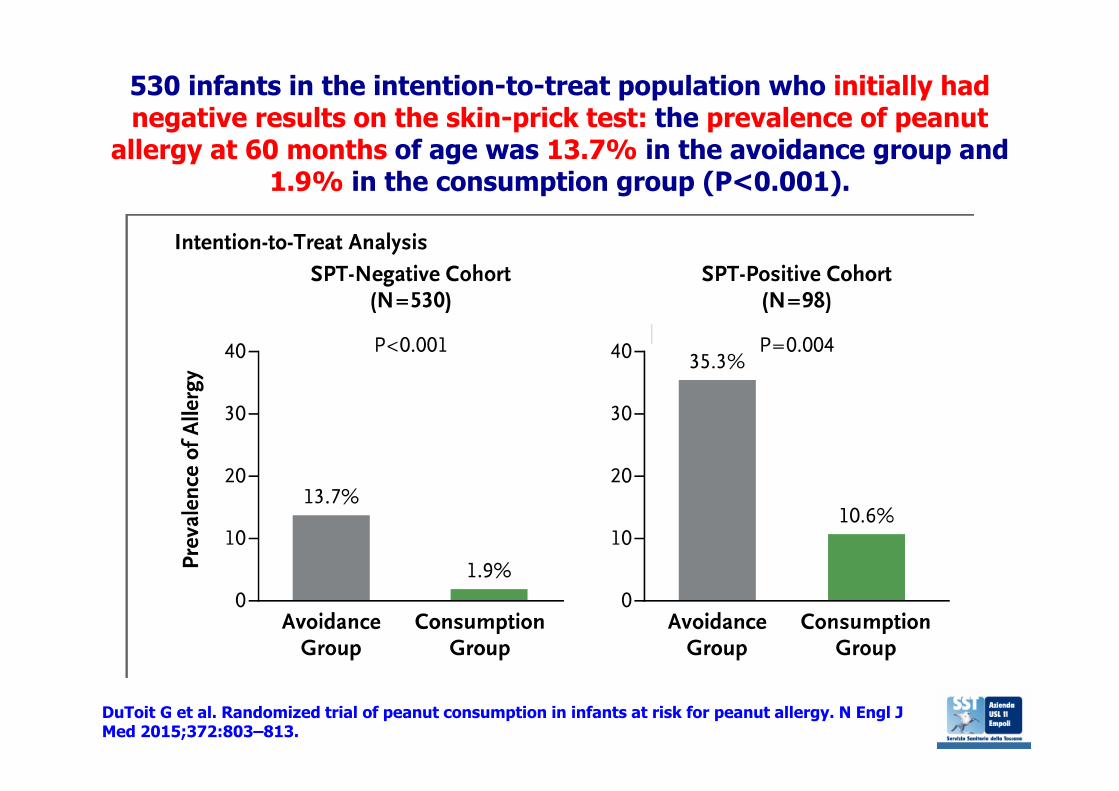
530 infants in the intention-to-treat population who initially hadnegative results on the skin-prick test: the prevalence of peanut
allergy at 60 months of age was 13.7% in the avoidance group and 1.9% in the consumption group (P<0.001).
DuToit G et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl JMed 2015;372:803–813.
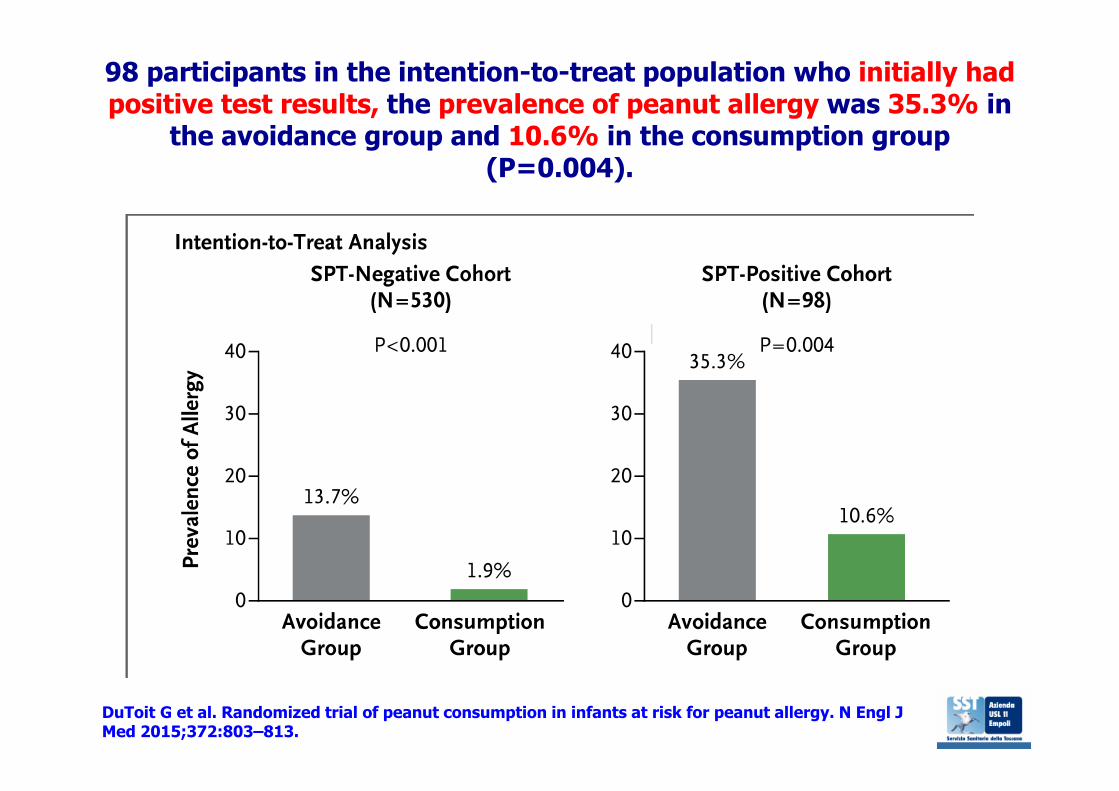
98 participants in the intention-to-treat population who initially hadpositive test results, the prevalence of peanut allergy was 35.3% in
the avoidance group and 10.6% in the consumption group(P=0.004).
DuToit G et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl JMed 2015;372:803–813.
Allergy 70 (2015) 1193–1195
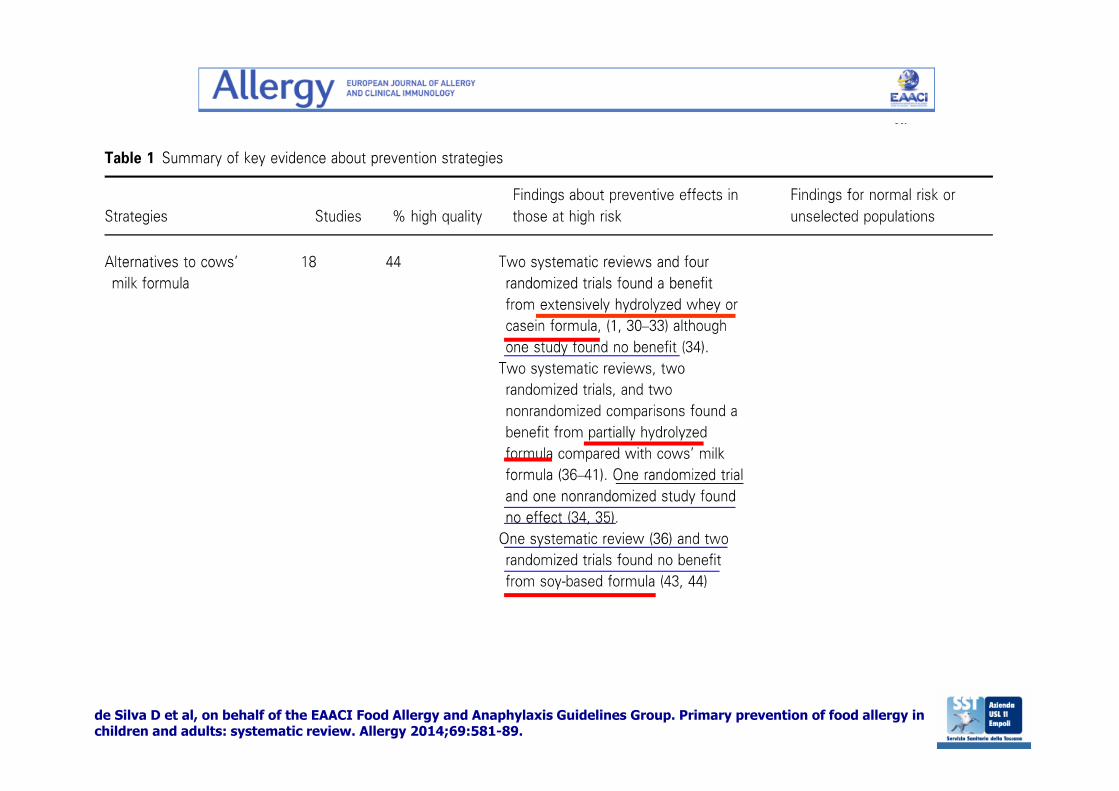
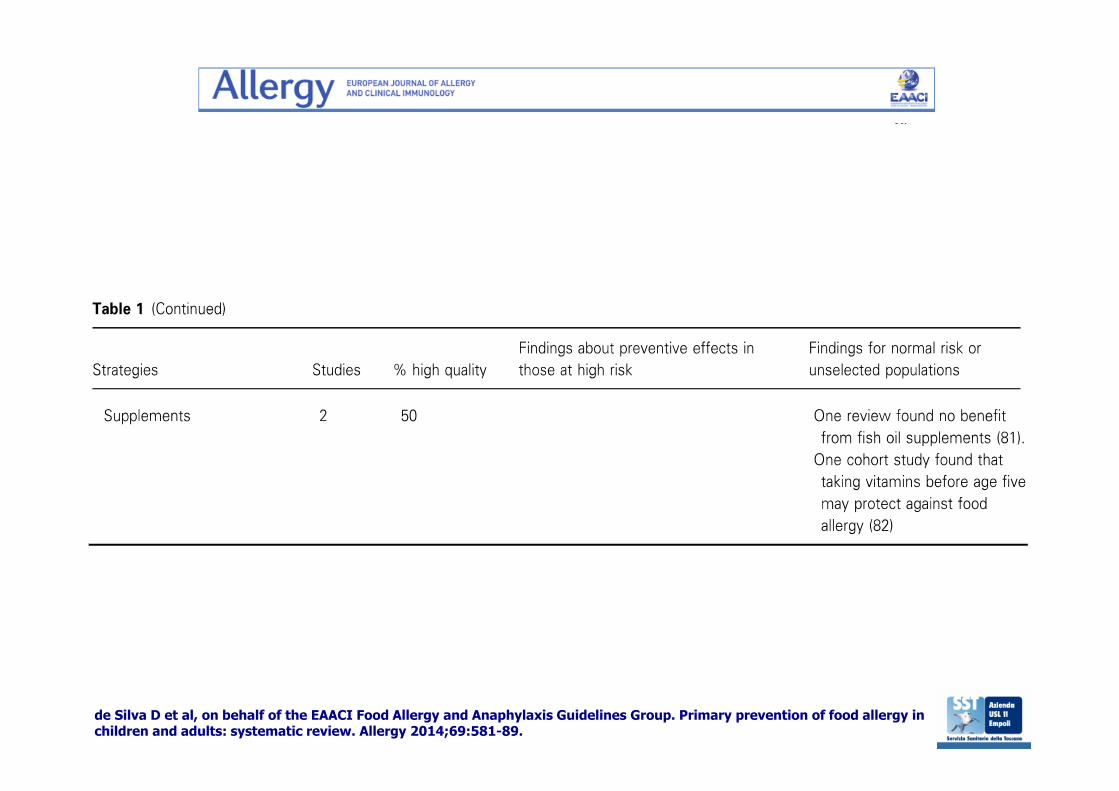
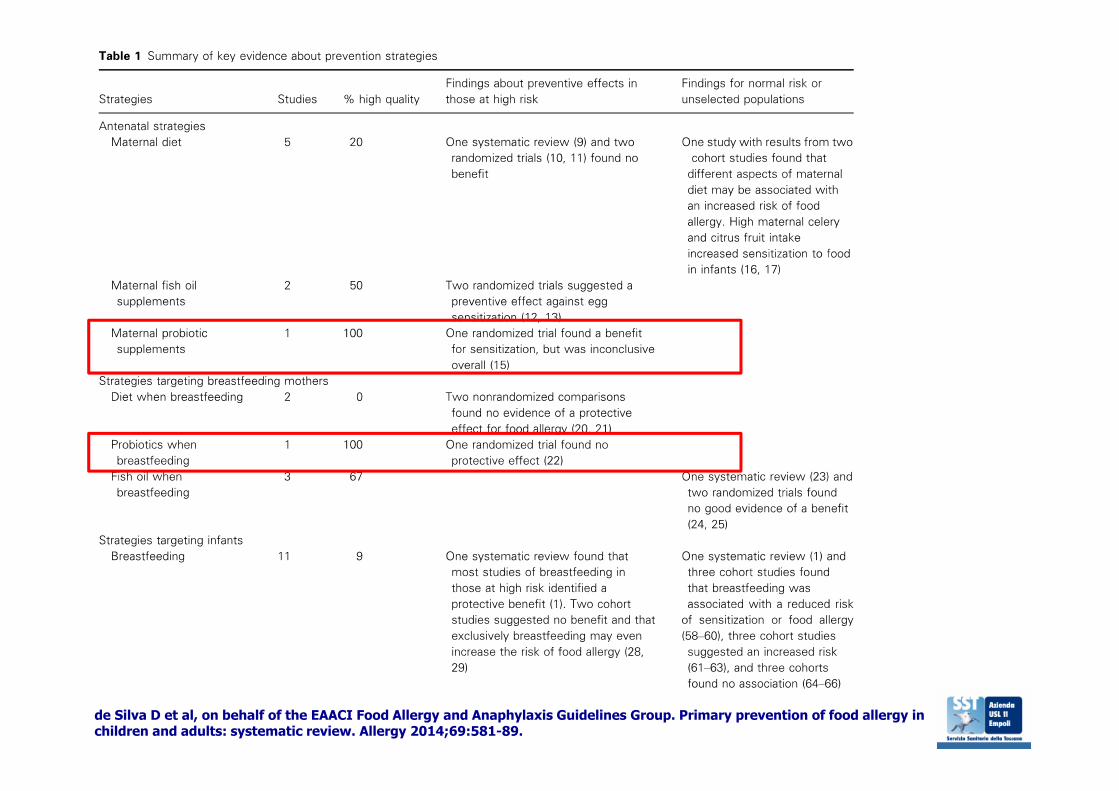
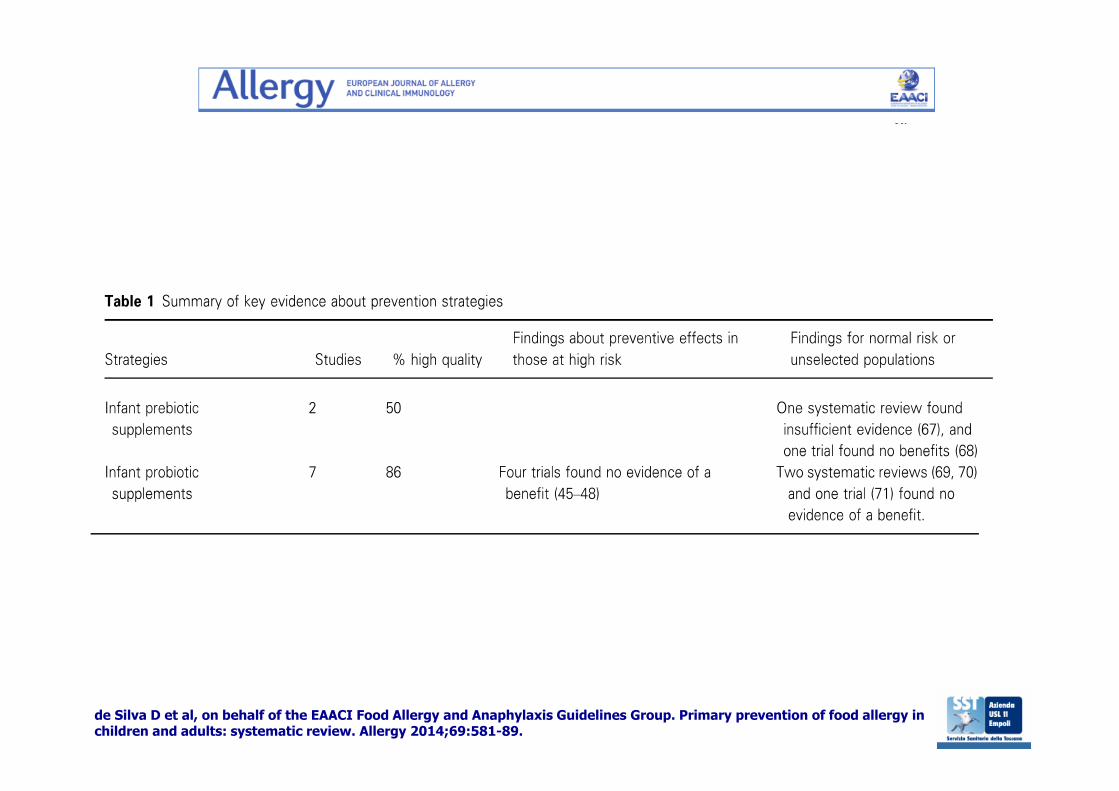
de Silva D et al, on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Primary prevention of food allergy in children and adults: systematic review. Allergy 2014;69:581-89.
de Silva D et al, on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Primary prevention of food allergy in children and adults: systematic review. Allergy 2014;69:581-89.
de Silva D et al, on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Primary prevention of food allergy in children and adults: systematic review. Allergy 2014;69:581-89.
de Silva D et al, on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Primary prevention of food allergy in children and adults: systematic review. Allergy 2014;69:581-89.
What others are saying
The European Academy of Allergy and Clinical Immunology (EAACI) Food Allergy and Anaphylaxis Guidelines state that “there is no evidence to recommend that women modify their diet duringpregnancy or take any supplements such as probiotics in order to prevent food allergy in their children”.
Guidelines from the US National Institute of Allergy and InfectiousDiseases, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPHGAN), the World GastroenterologyOrganisation Global Guidelines on Probiotics and Prebiotics, and the Food & Agriculture Organization (FAO)/ World Health Organization (WHO) Guidelines on Probiotics make no specific recommendationsabout the use of probiotics in pregnant women
Fiocchi A et al. World Allergy Organization Journal (2015) 8:4
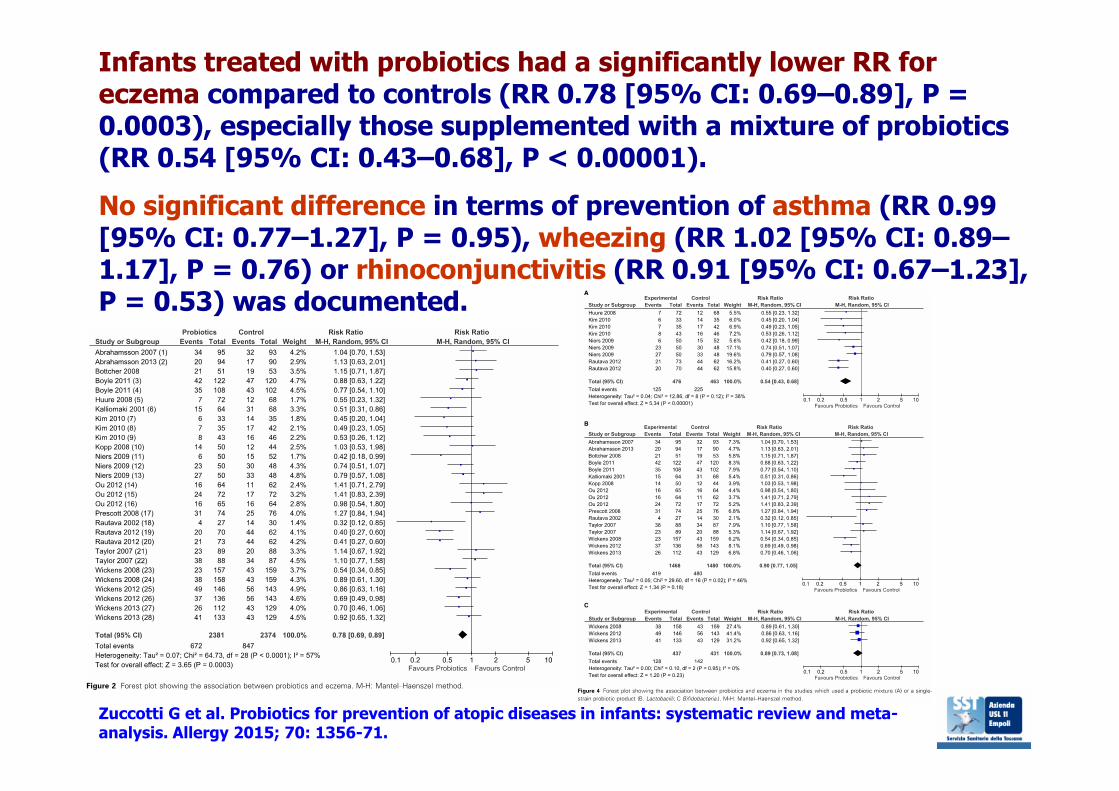
Zuccotti G et al. Probiotics for prevention of atopic diseases in infants: systematic review and meta-analysis. Allergy 2015; 70: 1356-71.
Infants treated with probiotics had a significantly lower RR for eczema compared to controls (RR 0.78 [95% CI: 0.69–0.89], P = 0.0003), especially those supplemented with a mixture of probiotics(RR 0.54 [95% CI: 0.43–0.68], P < 0.00001).No significant difference in terms of prevention of asthma (RR 0.99 [95% CI: 0.77–1.27], P = 0.95), wheezing (RR 1.02 [95% CI: 0.89–1.17], P = 0.76) or rhinoconjunctivitis (RR 0.91 [95% CI: 0.67–1.23], P = 0.53) was documented.
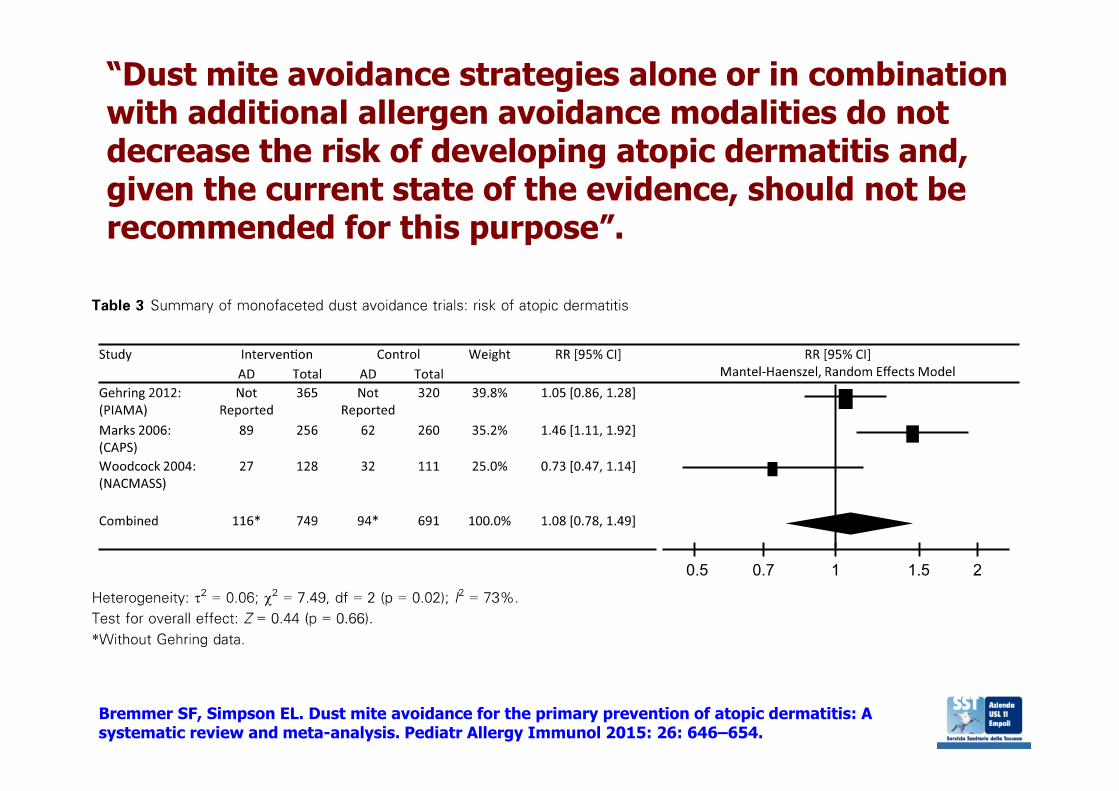
Bremmer SF, Simpson EL. Dust mite avoidance for the primary prevention of atopic dermatitis: A systematic review and meta-analysis. Pediatr Allergy Immunol 2015: 26: 646–654.
“Dust mite avoidance strategies alone or in combinationwith additional allergen avoidance modalities do notdecrease the risk of developing atopic dermatitis and, given the current state of the evidence, should not be recommended for this purpose”.
“There is strong evidence that the origins of allergic disease risk liein in utero development: allergy-associated genetic variants, alongwith the uterine environment – influenced by maternal exposuresand experiences – produce phenotypic differences already visible atbirth between those who go on to develop allergic disease and those who do not.
Our current best predictors of childhood asthma retain a degree of inaccuracy, suggesting we have not yet captured the full range of variations, exposures and interaction effects that explain allergyrisk.
Yet despite this, the greater ability to set disease trajectories in early development points to interventions very early in life, perhapseven in utero, as offering the greatest opportunity for primaryprevention of allergic disease.”
Lockett GA, Huoman J, Holloway JW. Does allergy begin in utero? Pediatr Allergy Immunol 2015: 26: 394–402.
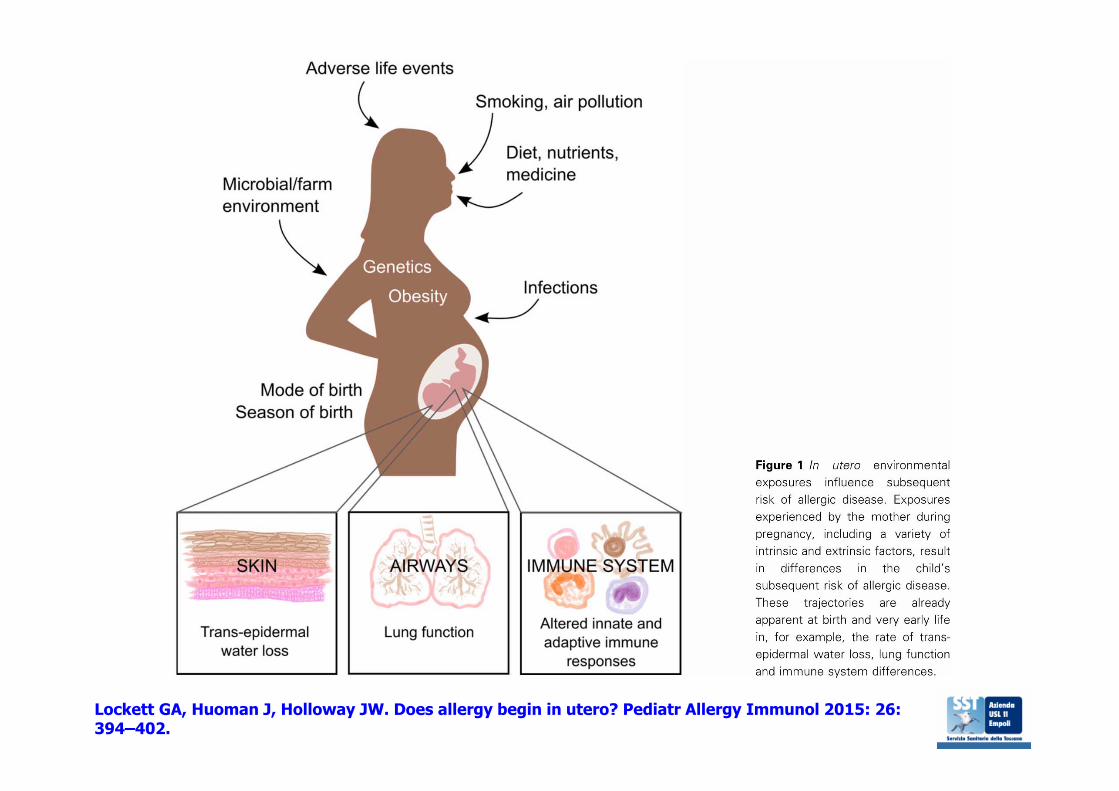
Lockett GA, Huoman J, Holloway JW. Does allergy begin in utero? Pediatr Allergy Immunol 2015: 26: 394–402.








![LE (MALATTIE) NEOPLASIE MIELOPROLIFERATIVE … · Policitemia vera Trombocitemia essenziale Mielofibrosi [Primaria] LEUCEMIA ACUTA MIELOIDE. Prof AM Vannucchi-AA2010-11 7 Myeloproliferative](https://static.fdocumenti.com/doc/165x107/5ba2b3ac09d3f295388c807f/le-malattie-neoplasie-mieloproliferative-policitemia-vera-trombocitemia-essenziale.jpg)