
La nutrizione enterale e la nutrizione...
50
La nutrizione enterale e la nutrizione parenterale Riccardo Caccialanza Servizio di Dietetica e Nutrizione Clinica Fondazione IRCCS Policlinico San Matteo [email protected]
Transcript of La nutrizione enterale e la nutrizione...

La nutrizione enterale e la nutrizione parenterale
Riccardo Caccialanza
Servizio di Dietetica e Nutrizione Clinica Fondazione IRCCS Policlinico San Matteo
PREMESSE GENERALI

LA NUTRIZIONE ARTIFICIALE
Metodica terapeutica con la quale attraverso vie non naturali vengono
introdotti tutti i nutrienti, in forma più o meno semplice
• NUTRIZIONE ENTERALE (tratto gastroenterico funzionante e accessibile ad una sonda)
• NUTRIZIONE PARENTERALE (accesso vascolare adeguato alle necessità)
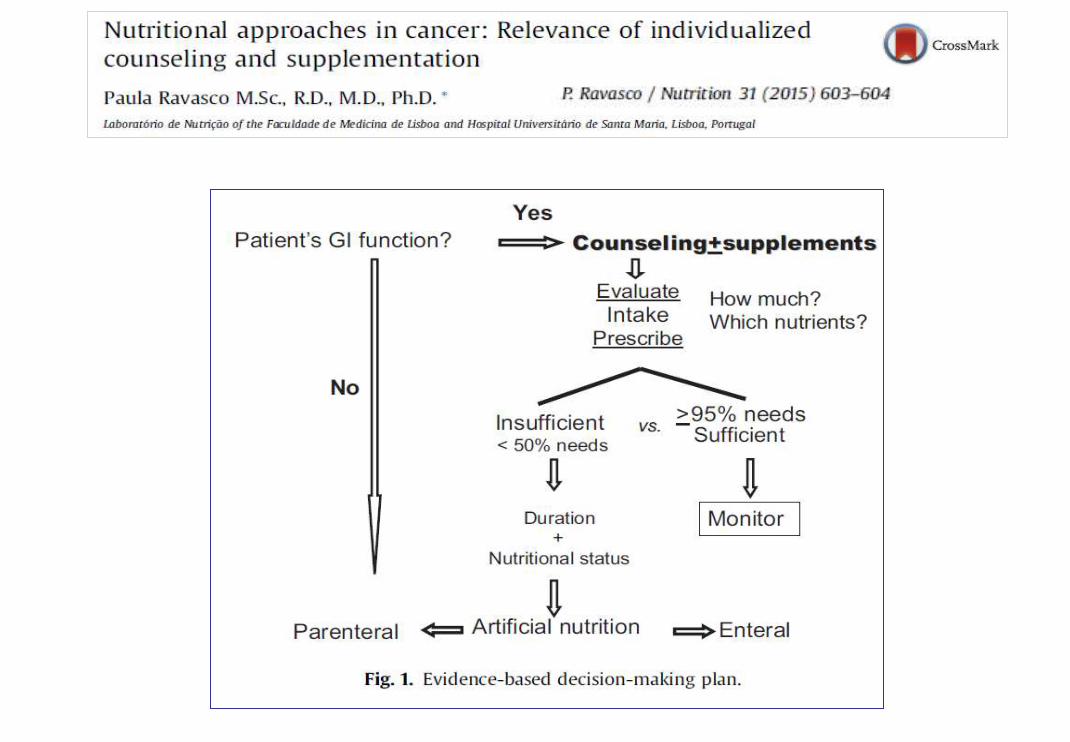

CRITERI DI SCELTA TRA NUTRIZIONE ENTERALE E
PARENTERALE
L’INTESTINO È FUNZIONANTE?
SI N0
ENTERALE PARENTERALE
< 30 gg > 30 gg < 15 gg > 15 gg
SONDINO:
NASOGASTRICO
NASODIGIUNALE
GASTROSTOMIA
DIGIUNOSTOMIA
PERIFERICA CENTRALE
OBIETTIVI
NUTRIZIONALI
RAGGIUNTI?
SI
N0
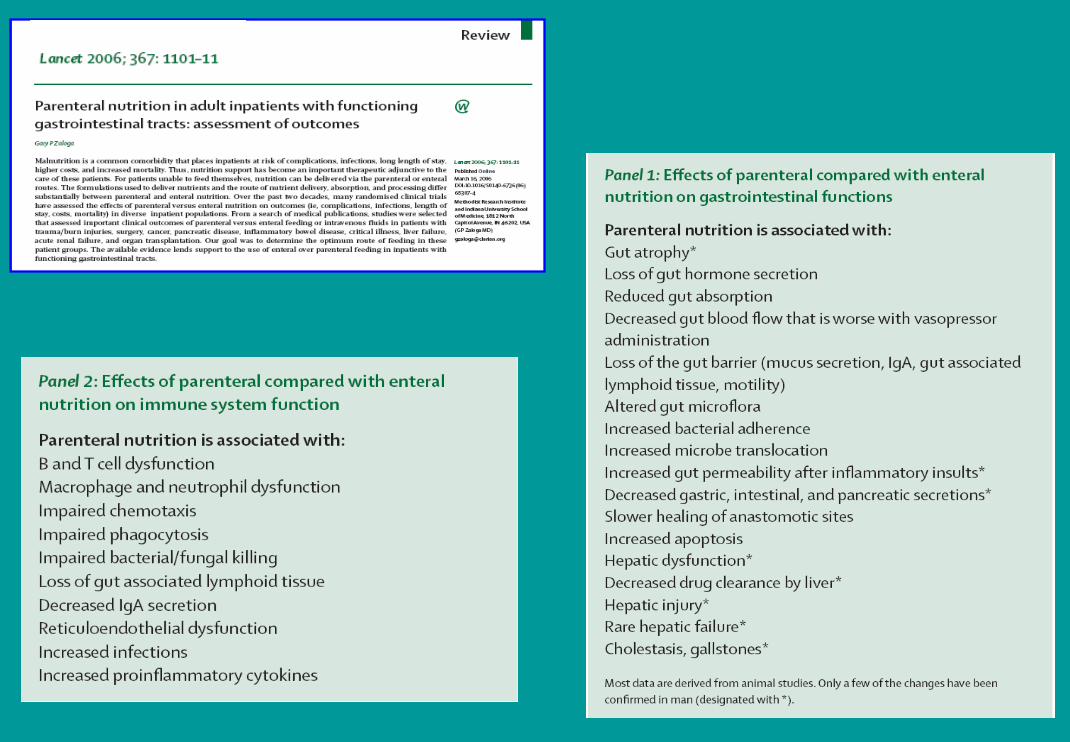
Zaloga GP. Lancet 2006, 1, 367 (9516): 1101-11

OUTCOME DEL SUPPORTO NUTRIZIONALE
Mortalità Qualità della vita
Complicanze – Ricoveri
Praticabilità delle terapie
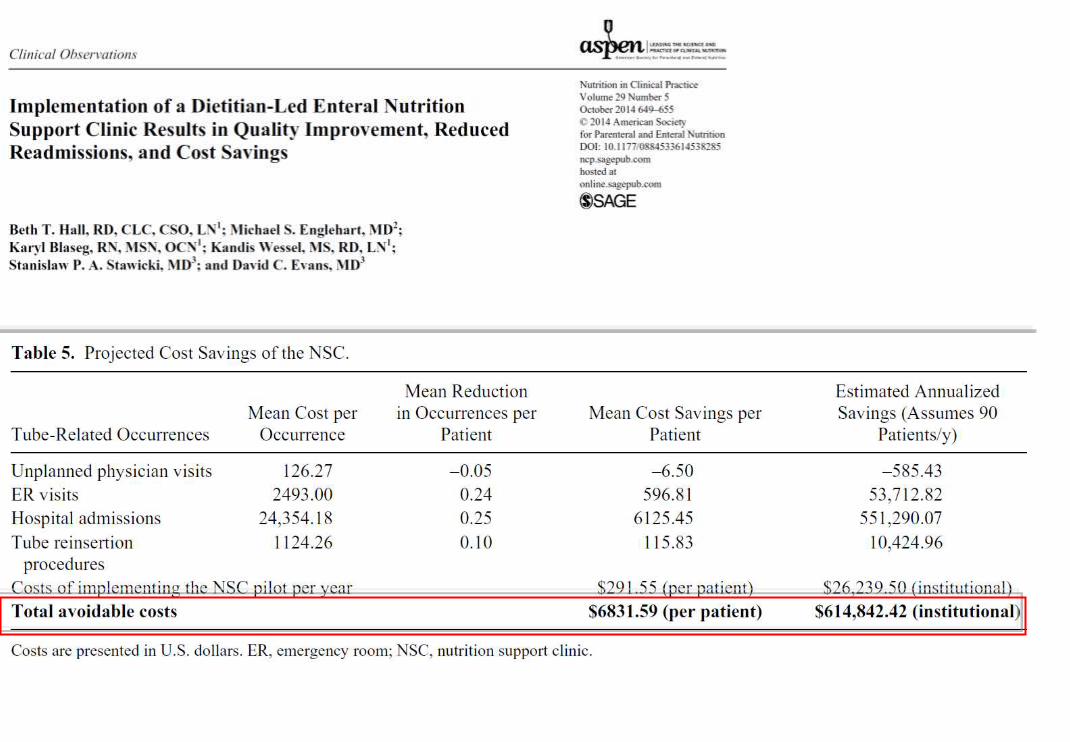
Costi
Parametri antropometrici
Parametri biochimici
Composizione corporea Test funzionali
Secondari
Primari

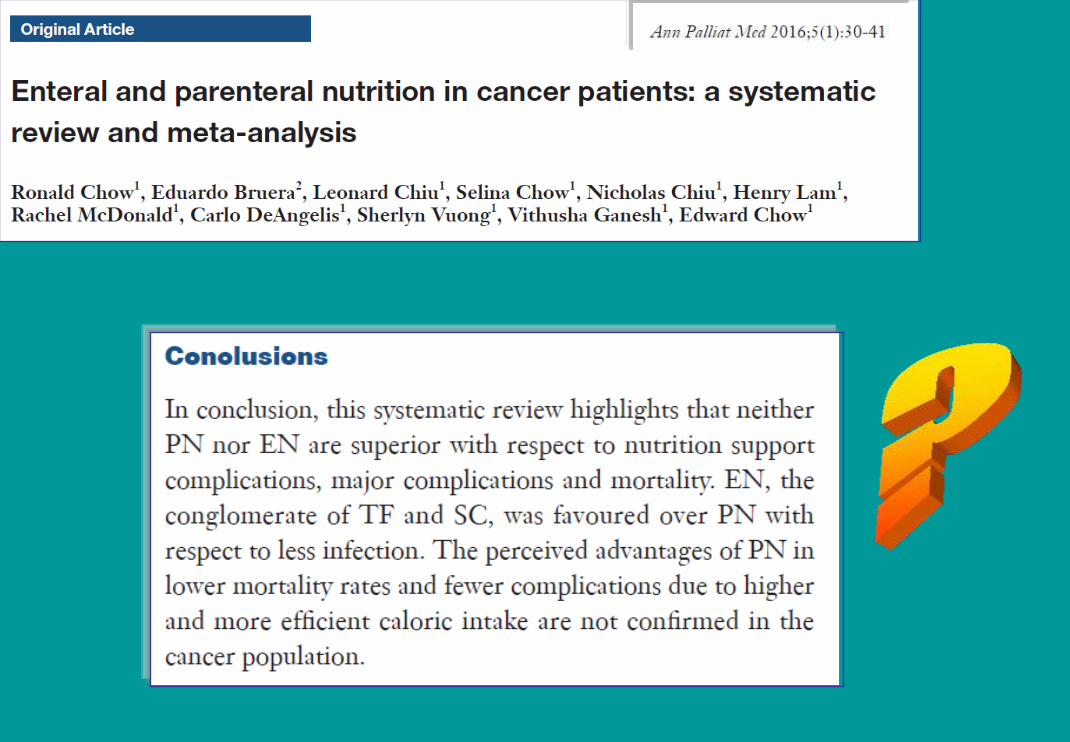
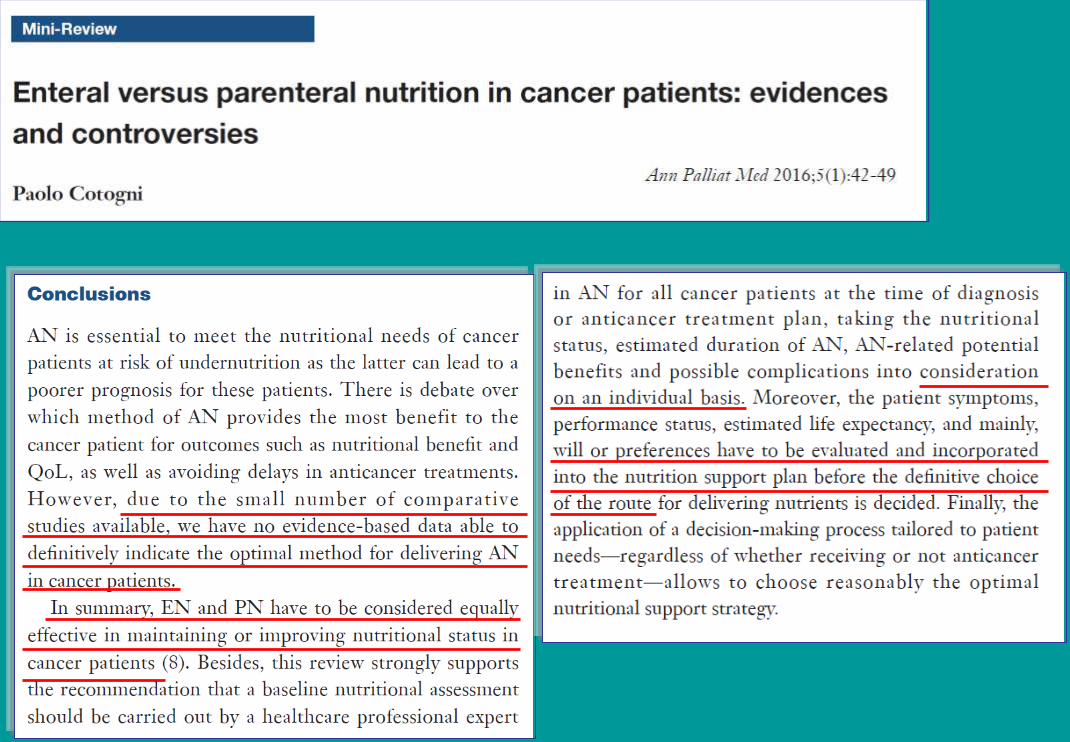
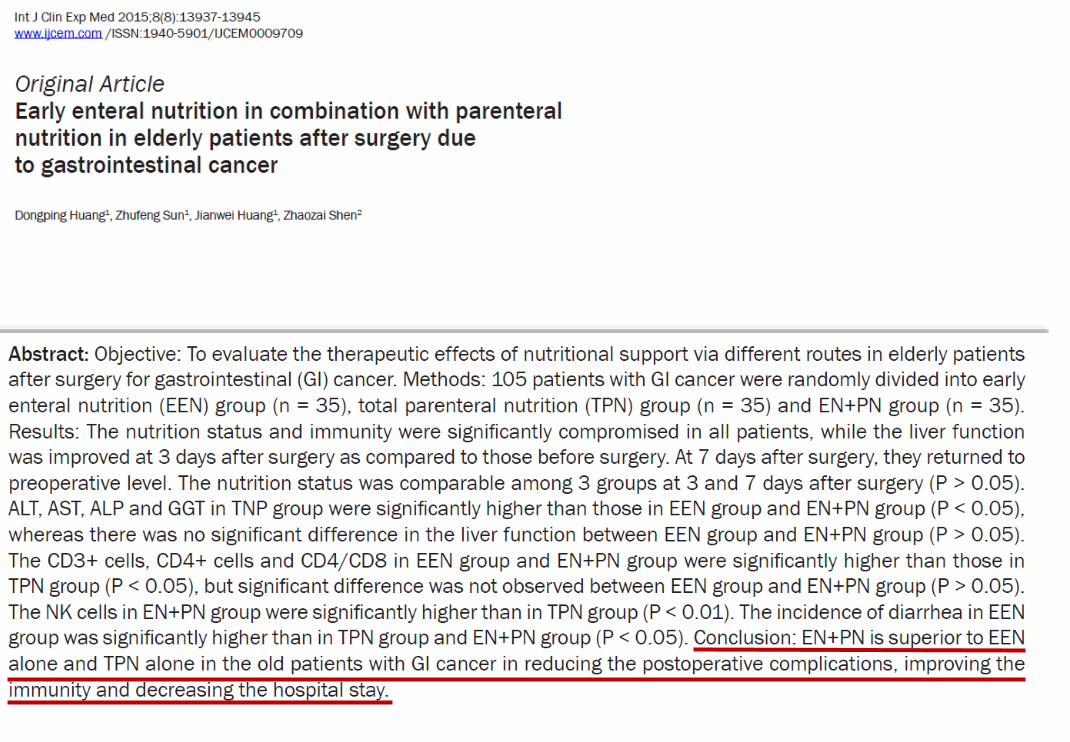
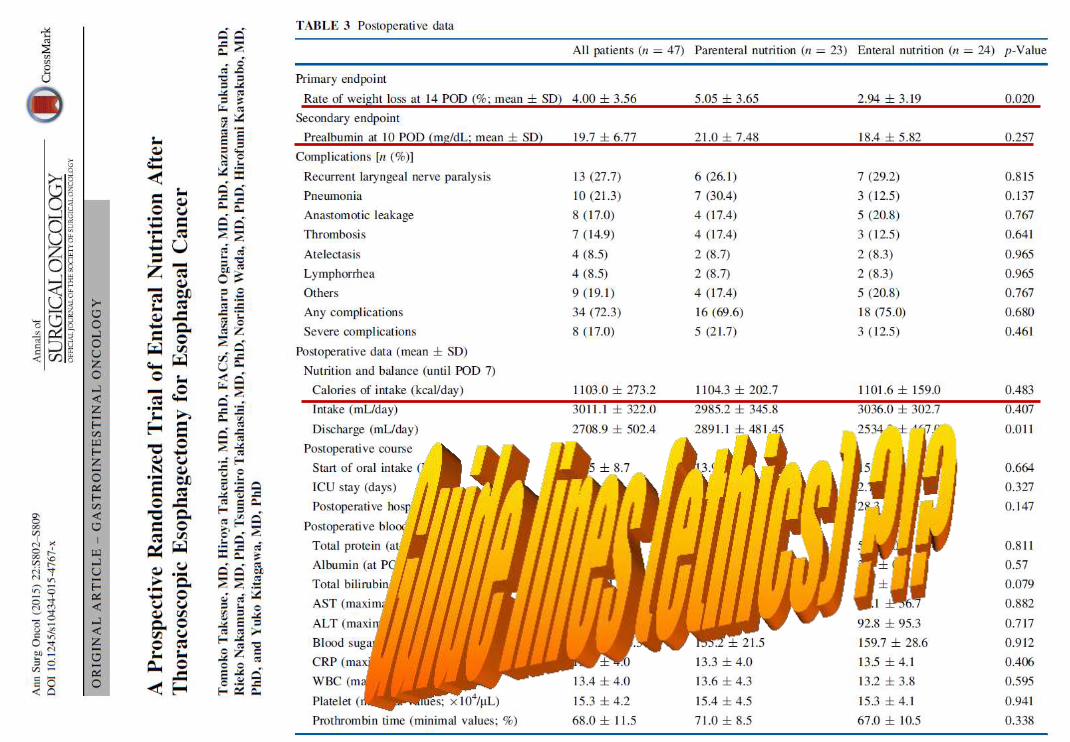
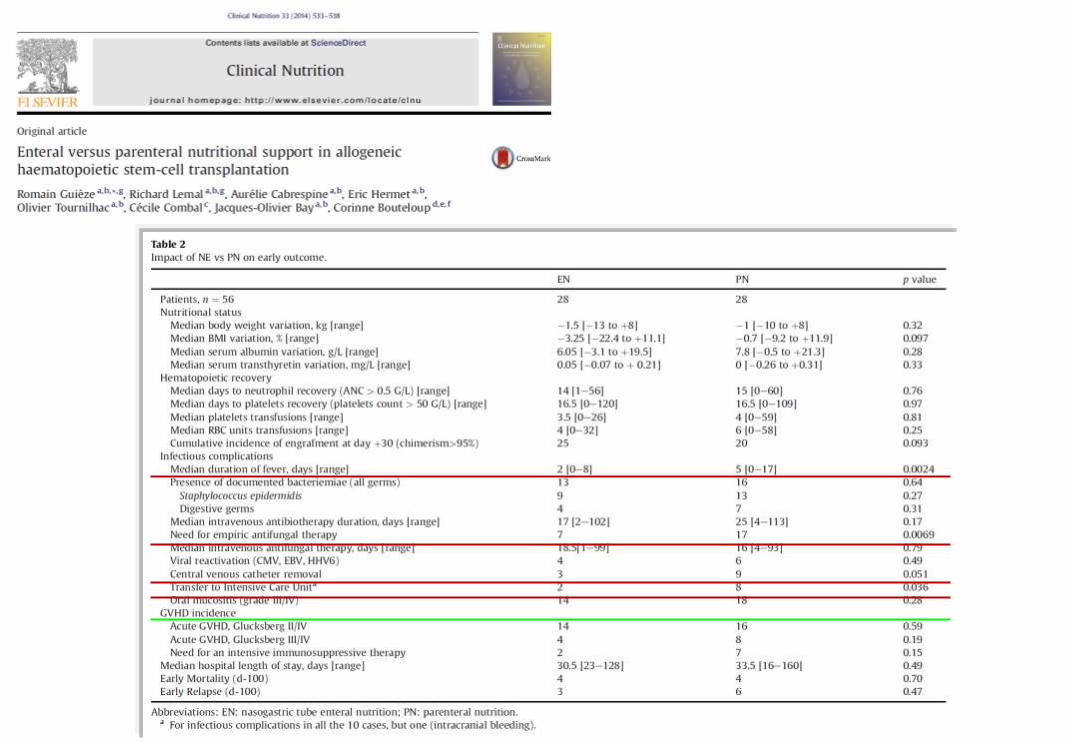
NE versus NP ?
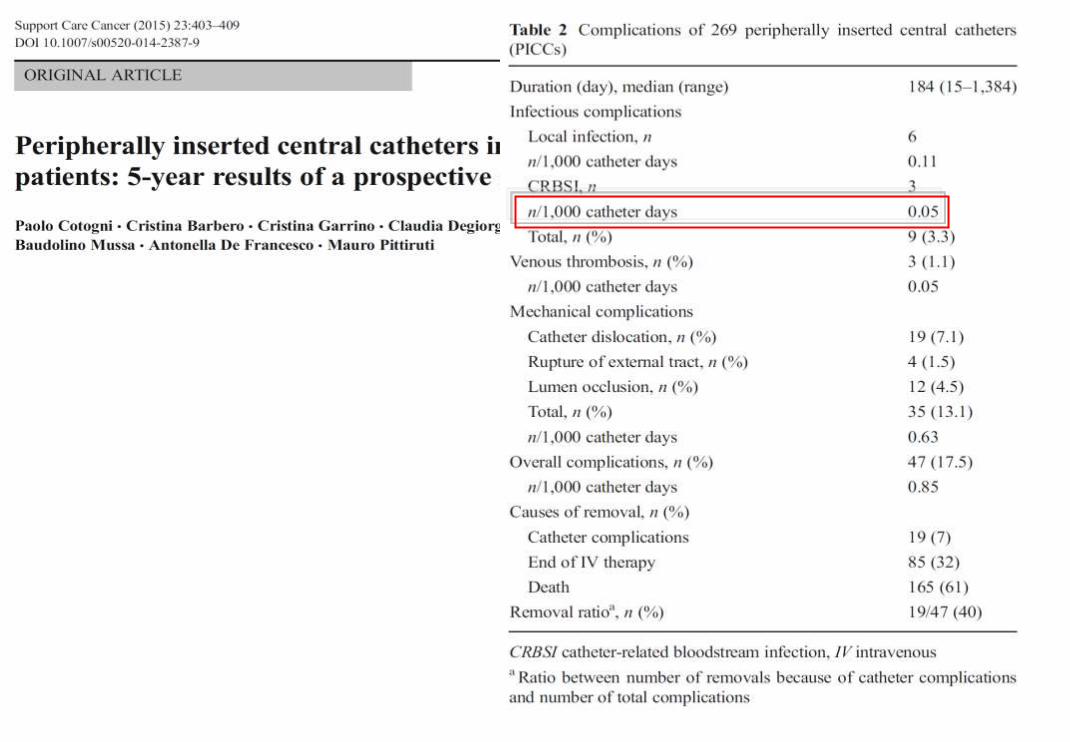
Vantaggi della NE rispetto alla NP:
• minore incidenza di complicanze infettive
• più semplice gestione
• minore invasività (?)
• minori costi (1:6 - 1:10)
La NE non è in antitesi con la NP

Highlights
• Parenteral nutrition may be considered when oral
intake and/or enteral nutrition are not sufficient to
maintain nutritional status and the patient is likely to die
sooner from starvation than from the cancer disease.
• A detailed assessment should be made before the
decision about whether parenteral nutrition should be
started.
• A follow-up plan should be documented with objective
and patient-centered treatment goals as well as specific
time points for evaluation.
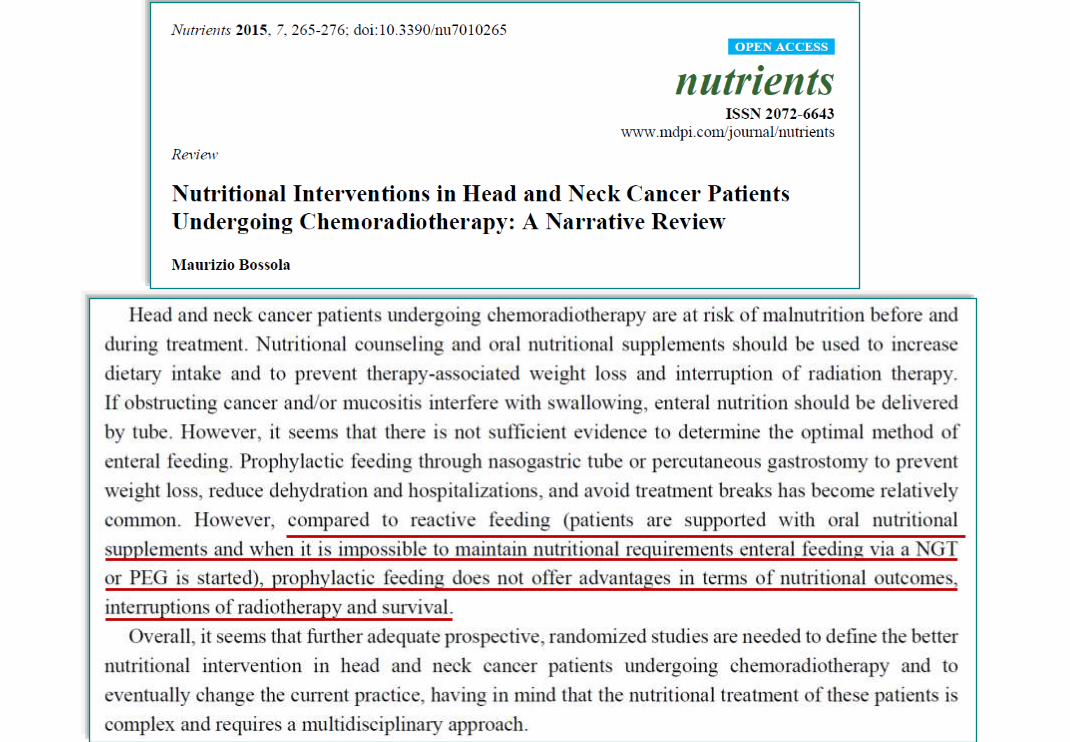
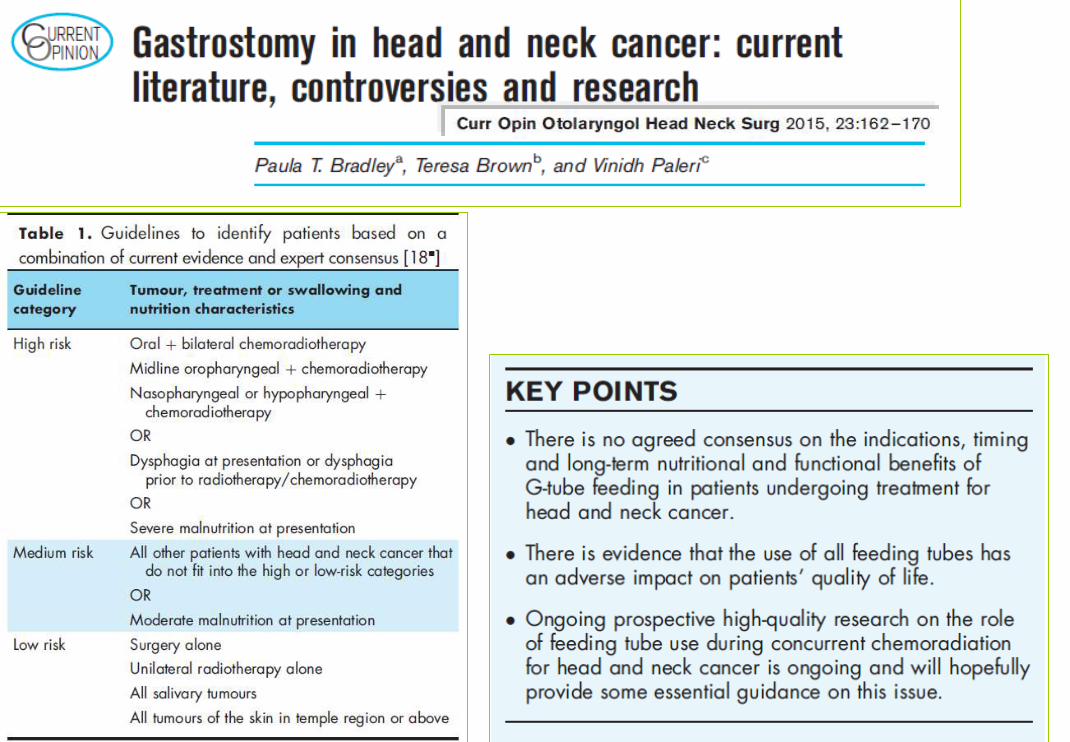
Highlights
• Feeding through a nasogastric or a gastrostomy
tube is recommended for patients with established
(or impending) malnutrition that compromises a
proper plan of therapy and oral nutrition is
inadequate or impossible.
• Percutaneous endoscopic gastrostomy is
preferred to nasogastric tube feeding when the
duration of enteral support is expected to exceed
1 month.
• There are no clear differences between the two
procedures regarding their long-term outcomes.

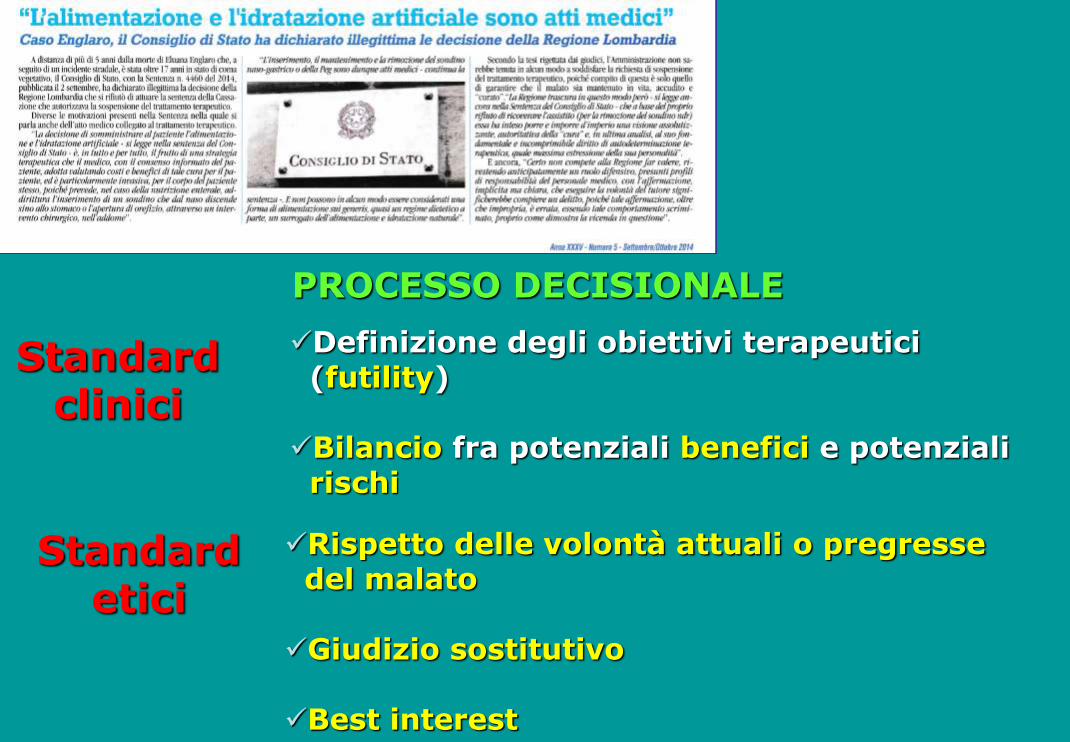
PROCESSO DECISIONALE
Definizione degli obiettivi terapeutici (futility)
Bilancio fra potenziali benefici e potenziali rischi
Rispetto delle volontà attuali o pregresse del malato
Giudizio sostitutivo
Best interest
Standard etici
Standard clinici


Daily energy and substrate guidelines for adult PN
PN calories - 20-30 kcal/kg/die
- Glucose/lipids ratio (%) = 70:30 or 60:40
- Glucose < 5 g/kg/die
- Lipids (LCT or LCT + MCT) 0.5-1 g/kg/die
Aminoacids - 0.13-0.35 g Nitrogen/kg/die = 0.8 – 2 g di AA/kg/die
Electrolytes
Vitamins Adequate and complete supplementation
Microelements
www.espen.org www.nutritioncare.org



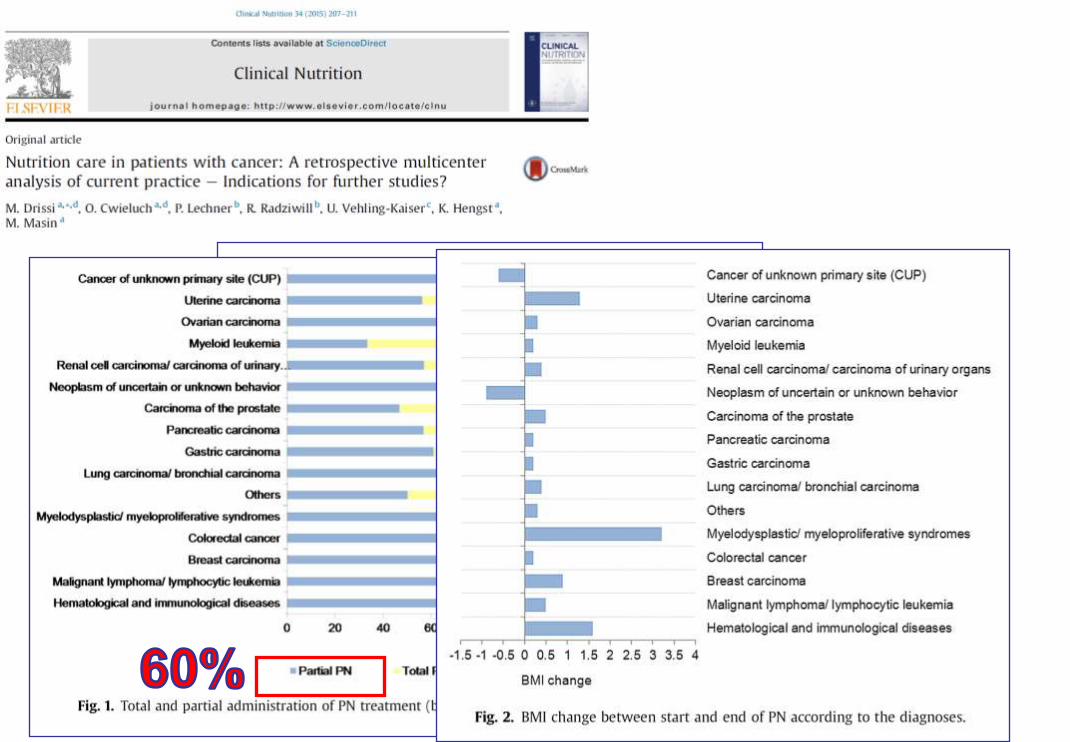
57%
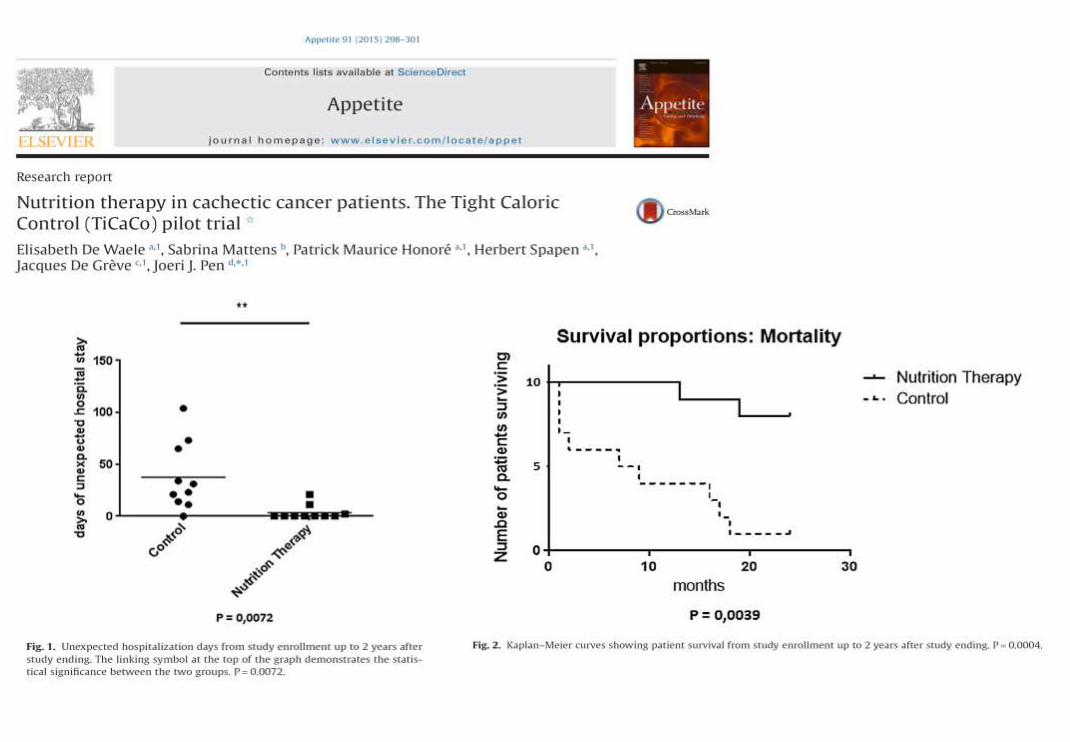
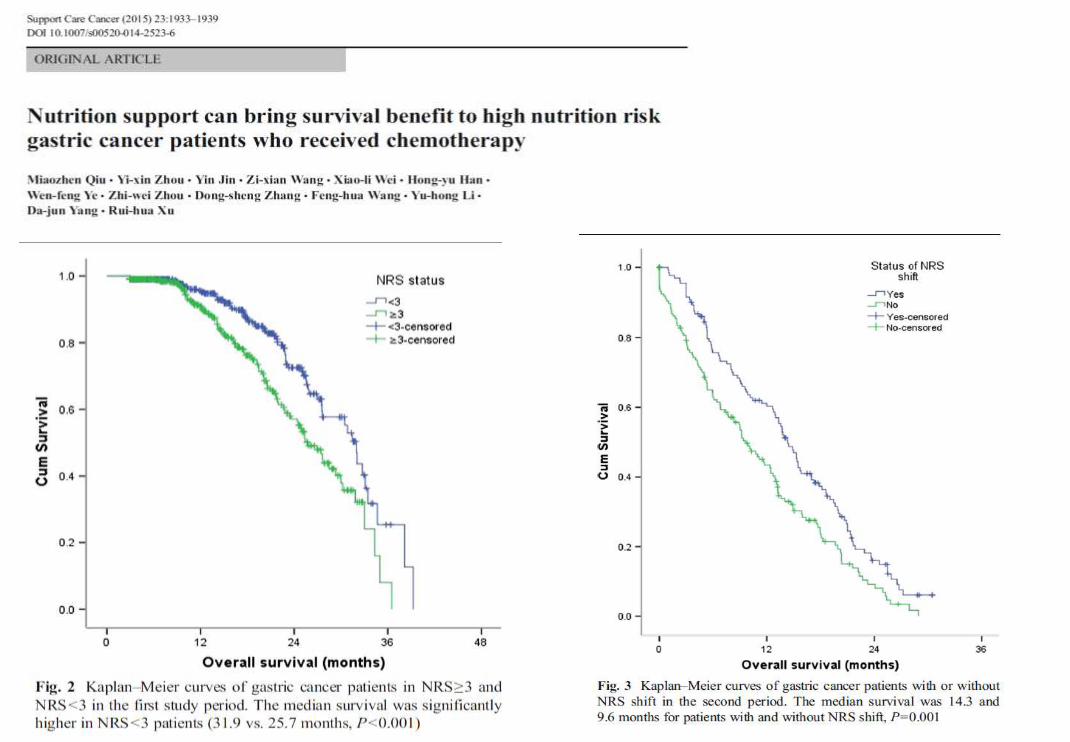
EVIDENZE DI EFFICACIA









Anti-cancer treatments & Nutrition
Palliative
care
Surgery
±
adjuvant
CT
CT and/or
RT
neo-
adjuvant
Nutrition
support
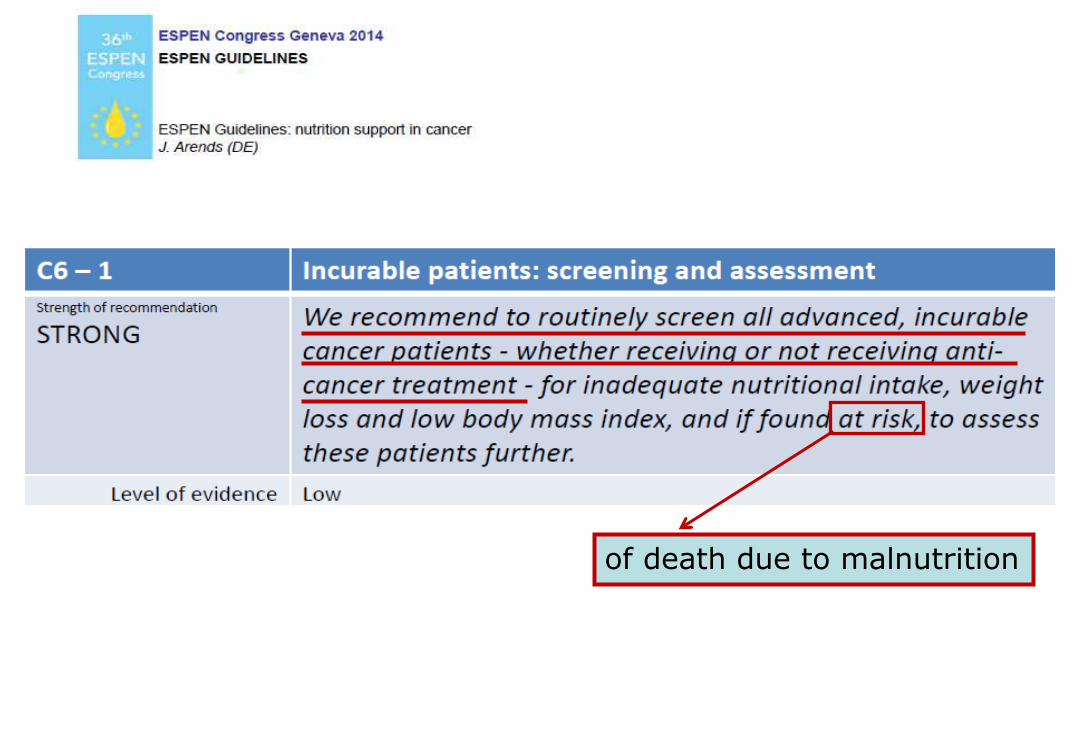
of death due to malnutrition
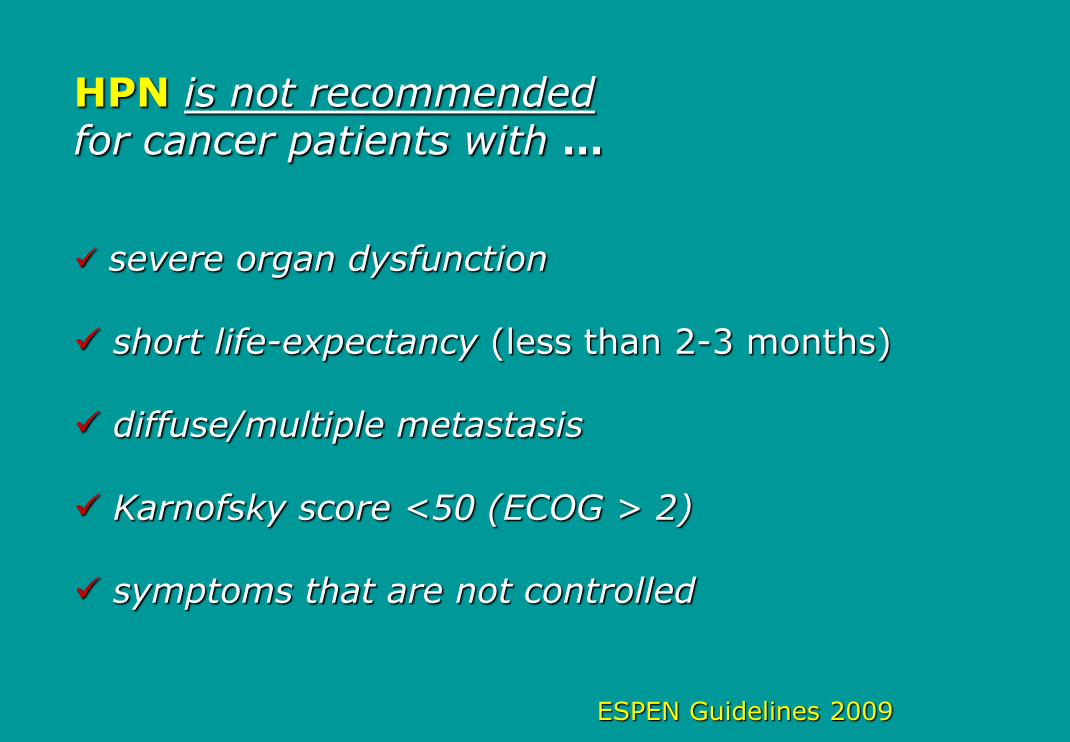
HPN is not recommended for cancer patients with …
severe organ dysfunction
short life-expectancy (less than 2-3 months)
diffuse/multiple metastasis
Karnofsky score <50 (ECOG > 2)
symptoms that are not controlled
ESPEN Guidelines 2009

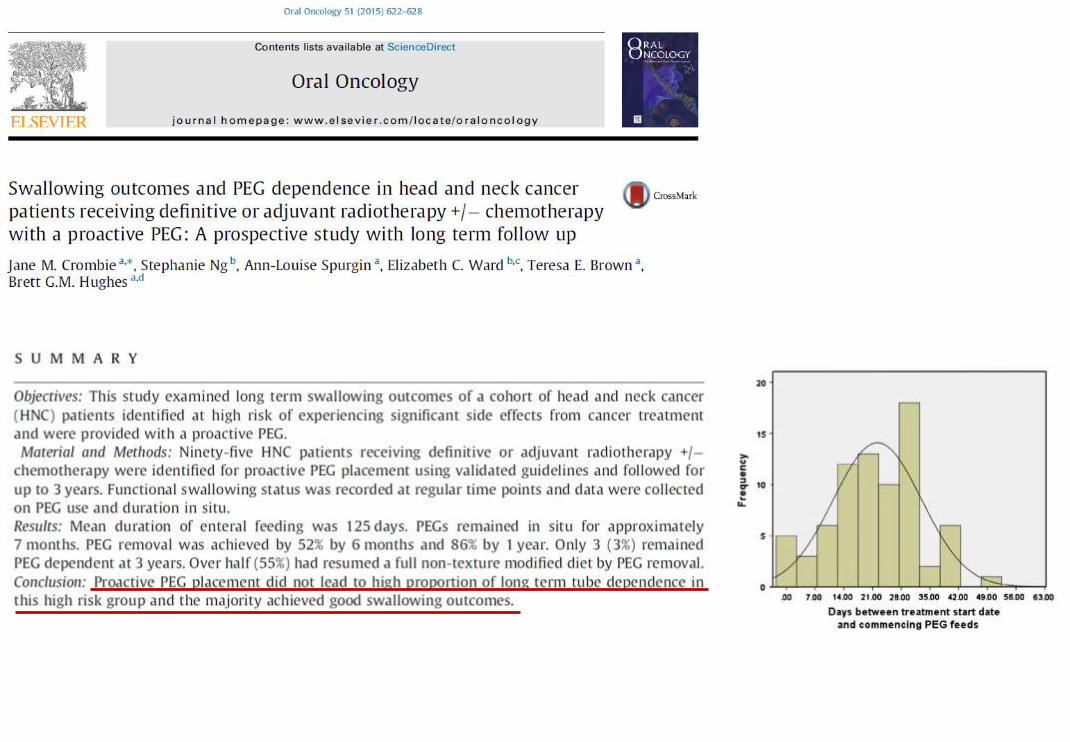
Median survival was 140 days
(20-783)

Messages to take home
NO alla NA solo quando il/la paziente ha:
calo ponderale > 10%
afagia/anoressia grave
malnutrizione causa di sospensione dei
trattamenti
sospensione dei trattamenti attivi

Messages to take home
NO alla NA quando il/la paziente ha:
aspettativa di vita < 2 mesi
sintomi non controllabili
insufficienza d’organo
performance status <50 (KPS) o ECOG 3

Messages to take home
SÌ alla NA già quando il/la paziente:
è a rischio di malnutrizione
ed il ‘counselling’ (± ONS)
non raggiungono l’obiettivo
della copertura dei fabbisogni
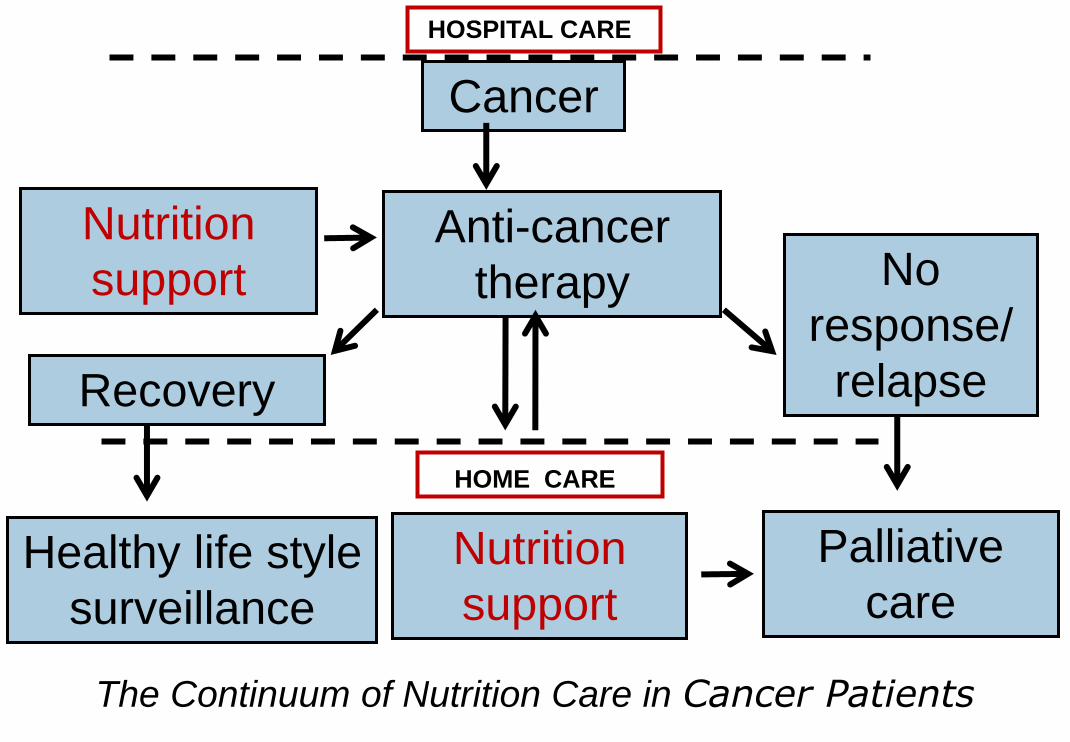
Cancer
Anti-cancer
therapy
Nutrition
support
Recovery
No
response/
relapse
Palliative
care Nutrition
support
HOME CARE
HOSPITAL CARE
Healthy life style
surveillance
The Continuum of Nutrition Care in Cancer Patients


















