I Fenotipi del Wheezing in Età Prescolare - siaip.it · L’asma non è un’unica malattia, ma un...
36
1 1 I Fenotipi del Wheezing in Età Prescolare Enrico Lombardi SODs Broncopneumologia Azienda Ospedaliero-Universitaria “Anna Meyer” Ospedale Pediatrico Firenze
Transcript of I Fenotipi del Wheezing in Età Prescolare - siaip.it · L’asma non è un’unica malattia, ma un...

1
1
I Fenotipi del Wheezing in Età Prescolare
Enrico Lombardi SODs Broncopneumologia
Azienda Ospedaliero-Universitaria
“Anna Meyer” Ospedale Pediatrico
Firenze

2
I Fenotipi di Wheezing In Pediatria
L’asma non è un’unica malattia, ma
un insieme di malattie eterogenee
con sintomi in comune
Una delle maggiori sfide nel
trattamento dell’asma è la
comprensione dei diversi fenotipi
e dei meccanismi biologici sottostanti
L’identificazione di questi meccanismi ha
l’obiettivo finale di migliorare l’efficacia
dei trattamenti e delle strategie
Belgrave DCM et al. Expert Rev Clin Immunol 2013;9:921-936
3
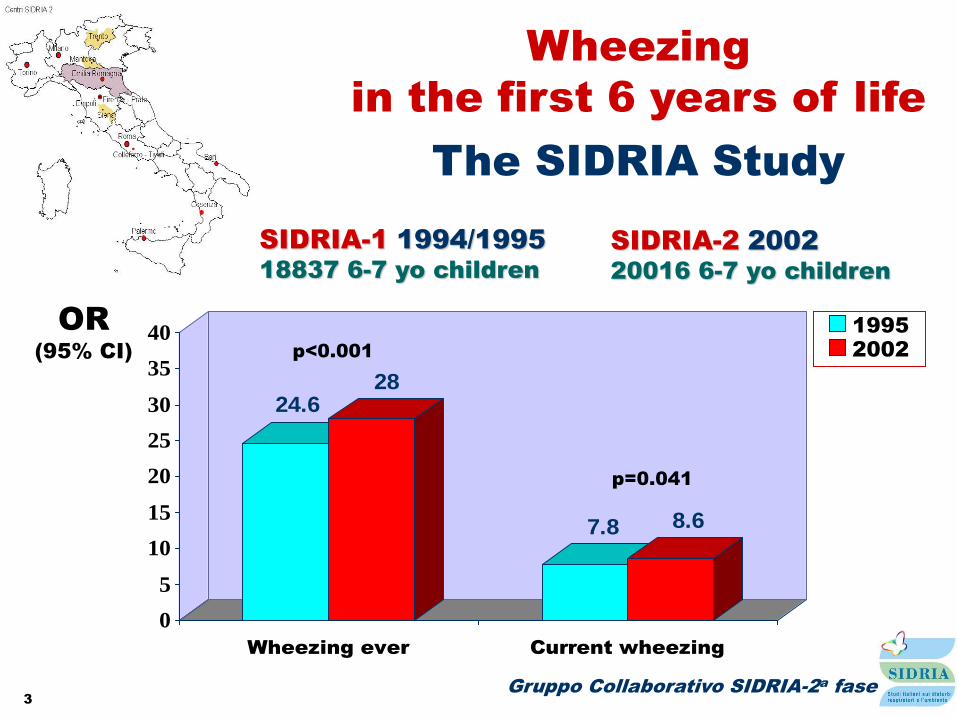
Wheezing
in the first 6 years of life
The SIDRIA Study
Gruppo Collaborativo SIDRIA-2a fase
24.628
7.8 8.6
0
5
10
15
20
25
30
35
40
Wheezing ever Current wheezing
2002
1995
p<0.001
OR
(95% CI)
p=0.041
SIDRIA-1 1994/1995
18837 6-7 yo children
SIDRIA-2 2002
20016 6-7 yo children

4
Non tutto è
asma quel che
fischia

5
Cause di Respiro Sibilante
in Lattanti e Bambini Piccoli
COMUNI MENO COMUNI RARE
Wheezing
transitorio
Asma
Aspirazione (RGE o
disfunz. deglutizione)
Infezioni (pertosse,
micoplasma, clamidia,
tubercolosi)
BPD
Corpo estraneo
Anafilassi
Fibrosi cistica
Anomalie vascolari
Anomalie tracheo-
bronchiali
Masse mediastiniche
Bronchiolite
obliterante
Immunodeficienza
Discinesia ciliare
Insuff. cardiaca
Avila PC. Lippincott’s Prim Care Pract 1998;2:559-77

6 Belgrave DCM et al. Expert Rev Clin Immunol 2013;9:921-936
7

8
Fenotipi di Sibilo
nei primi 6 anni di vita
Stein RT et al. Thorax 1997;52:946-952
Martinez FD et al. N Engl J Med 1995;332:133-138
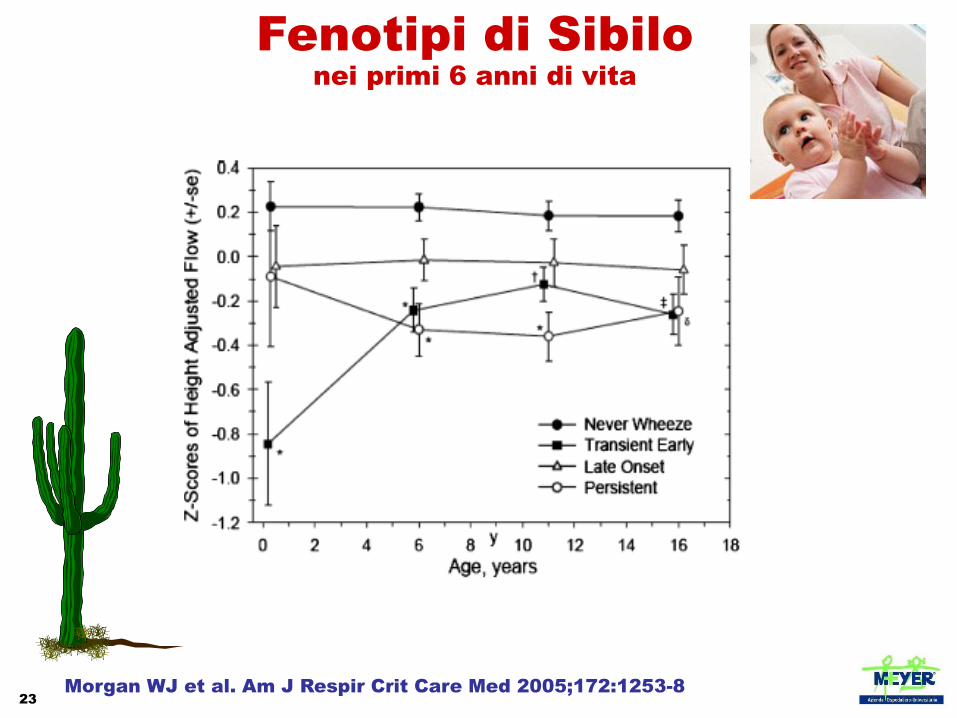
Never wheezers mai sibilo
Transient early wheezers sibilo nei primi 3 anni, no a 6
Late wheezers no sibilo nei primi 3 anni, sì a 6
Persistent wheezers sibilo 0-6 anni
51.5 %
19.8 %
15.0 %
13.7 %

9 Belgrave DCM et al. Expert Rev Clin Immunol 2013;9:921-936
Wheezing Phenotypes
10
Wheezing Ricorrente
Prognosi
40% a 10 anni – Isle of Whight Study
37% a 13 anni – German Multicenter Allergy Study (MAS)
30% a 16 anni – Tucson Children’s Respiratory Study (CRS)

11
1. Sibilo transitorio
Sibilo soltanto durante
i primi 2-3 anni di vita
2. Sibilo non atopico
Principalmente scatenato da
infezioni virali e tende a sparire
3. Asma persistente
Sibilo associato a:
Manifestazioni cliniche di atopia,
eosinofilia e/o IgE totali elevate
Sensibilizzazione IgE-mediata ad alimenti nei primi anni di vita
e, successivamente, ai comuni inalanti
Sensibilizzazione ad inalanti prima dei 3 anni di età
Genitore/i con asma
Fenotipi di Sibilo
in età pediatrica
PRACTALL consensus report. Allergy 2008;63:5-34
4. Sibilo grave intermittente
Episodi di sibilo acuti ma non frequenti associati a:
Morbidità minima al di fuori dei periodi di infezione respiratoria
Caratteristiche di atopia
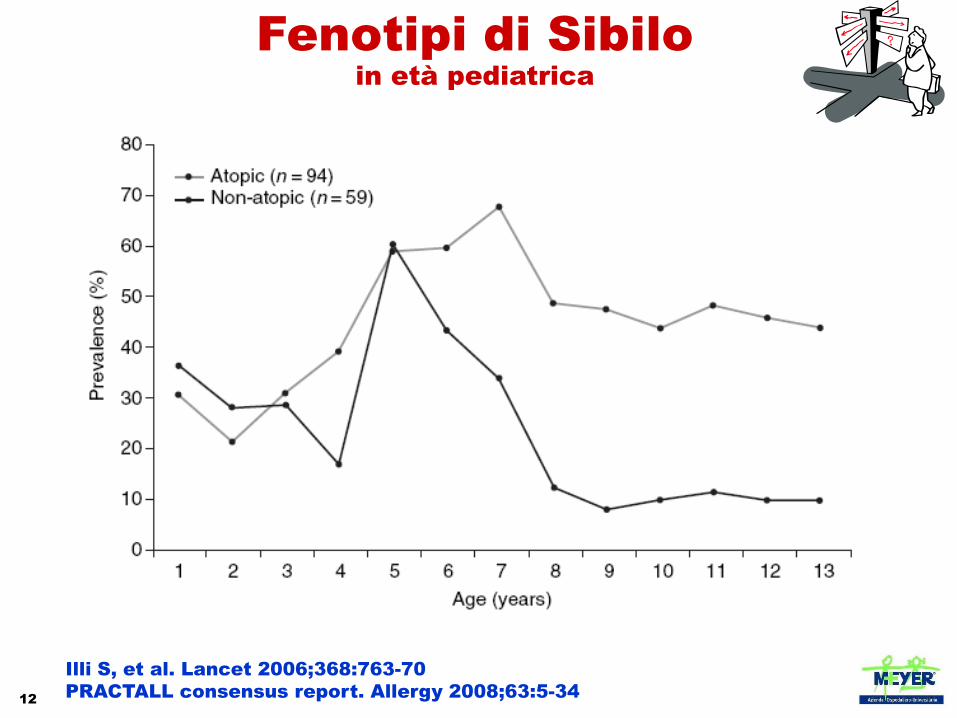
12
Fenotipi di Sibilo
in età pediatrica
Illi S, et al. Lancet 2006;368:763-70
PRACTALL consensus report. Allergy 2008;63:5-34

13
Castro-Rodríguez JA, et al. Am J Respir Crit Care Med 2000;162:1403-6
Guilbert TW, et al. JACI 2004;114:1282-7
Asthma Prediction Index
Asma diagnosticato da un
medico in uno o entrambi i
genitori
Dermatite atopica diagnosticata
da un medico nei primi 3 anni di
vita
Sensibilizzazione verso >1
allergene inalante
CRITERI MAGGIORI
Sensibilizzazione a latte, uovo o
arachidi
Sibilo non associato ad episodi
infettivi
Eosinofilia (> 4%)
CRITERI MINORI
Asma attivo a 6-13 anni
1 criterio maggiore
o
2 criteri minori
59 %
77 %
Sibilo nei primi 3 anni
> 1 episodio
> 3 episodi
14
Asthma Prediction Index
The PIAMA study suggests 8 clinical parameters for the risk
score
male sex
post-term delivery
parental education
Inhaled medicatiom
Wheezing frequency
Wheeze/dyspnea apart from colds
Respiratory infections
Eczema
Caudri D, et al. JACI 2009;124:903-10
API has been proposed has the best, most practical strategy
for predicting children who will develop persistent wheezing
Matricardi PM, et al. ERJ 2010;35:701-3
Belgrave DCM, et al. Expert Rev Clin Immunol 2013;9:921-6

15
There is increasing evidence that obesity affects
childhood asthma and its severity
Papoutsakis C, et al. J Acad Nutr Diet 2013;113:77-105
The nature of the association between obesity
and asthma remains obscure in children and appears to be stronger for
non-atopic asthma.
Longitudinal studies suggest that high body weight precedes asthma
symptoms
However, it is not clear how body mass may influence primary acquisition of
persistent wheeze
It is also of interest that body mass can exert cross generational epigenetic
effects so it is possible that parental obesity may affect their offspring.
Obesity
Walker ML, et al. Front Immunol 2014;5:447

16
Age 22 Age 16 Age 11
PEF
BMI
SPTs
Questionnaires
BMI
SPTs
Questionnaires
BMI
SPTs
Questionnaires
Age 26
BMI
SPTs
Questionnaires
Tucson Children’s Respiratory Study 2
02
53
0
BM
I (K
g/m
2)
10.9 16.6 22.1 26.5Age (years)
Normal PFvar at Yr11
High PFvar at Yr11
p = 0.268
p = 0.013
p < 0.001
p < 0.001
20
25
30
BM
I (K
g/m
2)
10.9 16.6 22.1 26.5Age (years)
Normal PFvar at Yr11
High PFvar at Yr11
Females Males

17
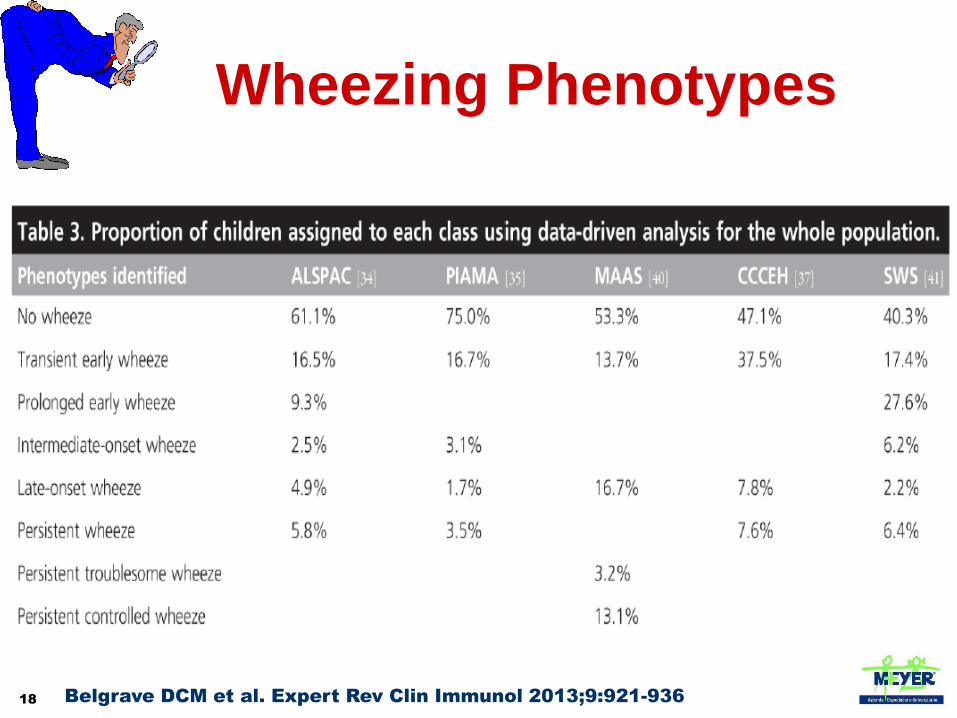
6265 children in a
longitudinal birth
cohort (the ALSPAC
study) were analysed
Measures of atopy,
airway function and
bronchial
responsiveness were
made at 7–9 years of
age
The wheezing
phenotypes most
strongly associated
with atopy and airway
responsiveness were
characterised by
onset after age 18
months
18
Wheezing Phenotypes
Belgrave DCM et al. Expert Rev Clin Immunol 2013;9:921-936
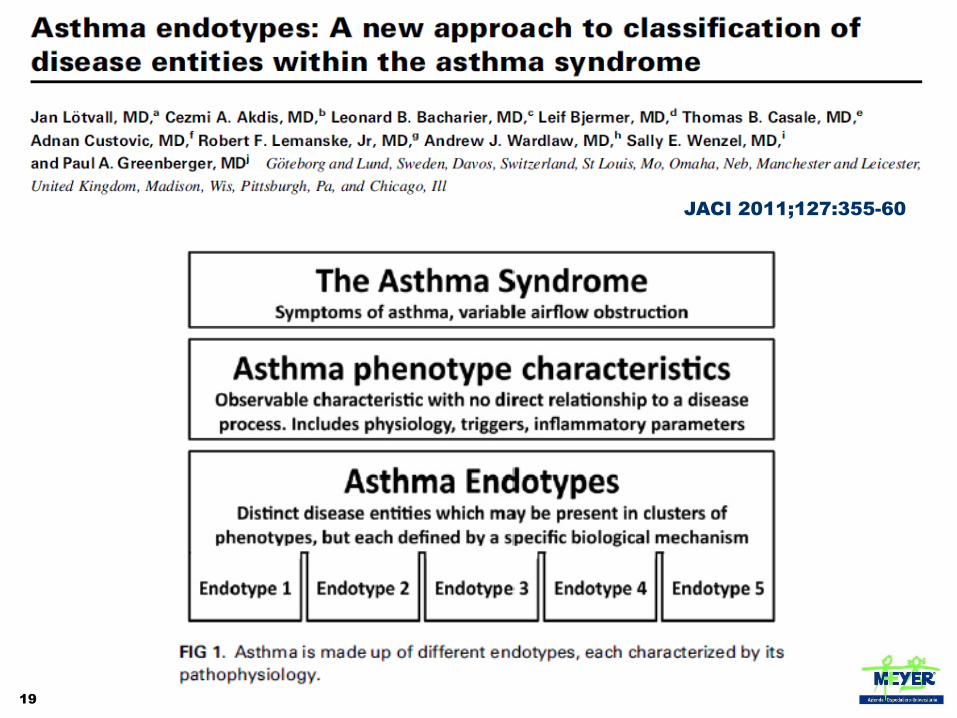
19
JACI 2011;127:355-60
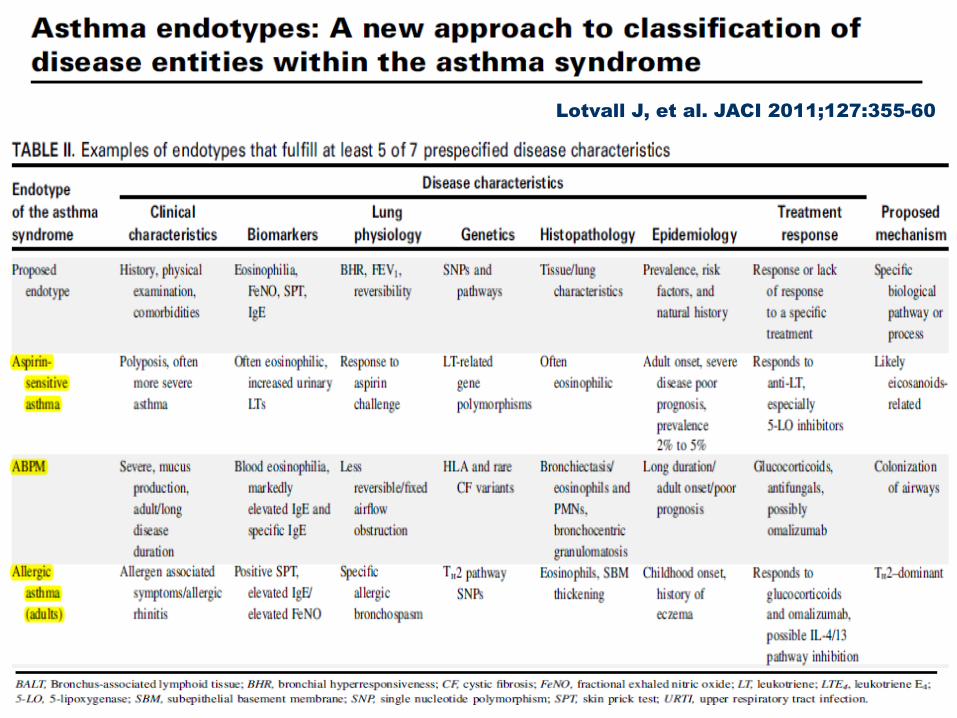
20
Lotvall J, et al. JACI 2011;127:355-60
21

22
L’Evoluzione a Lungo Termine
del Wheezing in Età Prescolare
23
Fenotipi di Sibilo
nei primi 6 anni di vita
Morgan WJ et al. Am J Respir Crit Care Med 2005;172:1253-8

24

25
Children with severe asthma are at
increased risk of developing adult
COPD
Children with intermittent asthma
are not at increased risk of
developing adult COPD
Tai A, et al. Thorax 2014;69:805-10

26
Outcomes of childhood asthma and wheezy
bronchitis - a 50-year cohort study
A cohort of children recruited in 1964 at age 10-15years, followed-up in
1989, 1995, and 2001 was followed-up in 2014 at age 60-65 years
330 subjects, mean age 61 years, were followed-up, 38 with childhood
asthma, 53 with childhood wheezy bronchitis, and 239 controls
In adjusted multivariate analyses childhood asthma was associated with
an increased risk of COPD odds ratio (95% confidence interval) 6.37
(3.73-10.94), as was childhood wheezy bronchitis 1.81 (1.12-2.91)
The COPD risk increased with childhood asthma and wheezy bronchitis
was associated with reduced FEV1 evident by the fifth decade and not
accelerated rate of FEV1 decline
Tagiyeva N, et al. Am J Respir Crit Care Med, 2015 Sep 9.
27
Associations of some early childhood factors with adult obstructive
airways disease, such as low birth weight and early childhood
infections, have been recognised for a considerable time
The challenge is to understand the mechanisms by which exposures
in early life, including pregnancy, influence lung growth and
development and to develop interventions to rectify the effects of
adverse influences during these critical years.

28
La Terapia a Lungo Termine
del Wheezing in Età Prescolare

29

30 Castro-Rodriguez JA et al. Pediatrics 2009;123:e519-e525
This effect was higher in those with a diagnosis of asthma than
wheeze
31
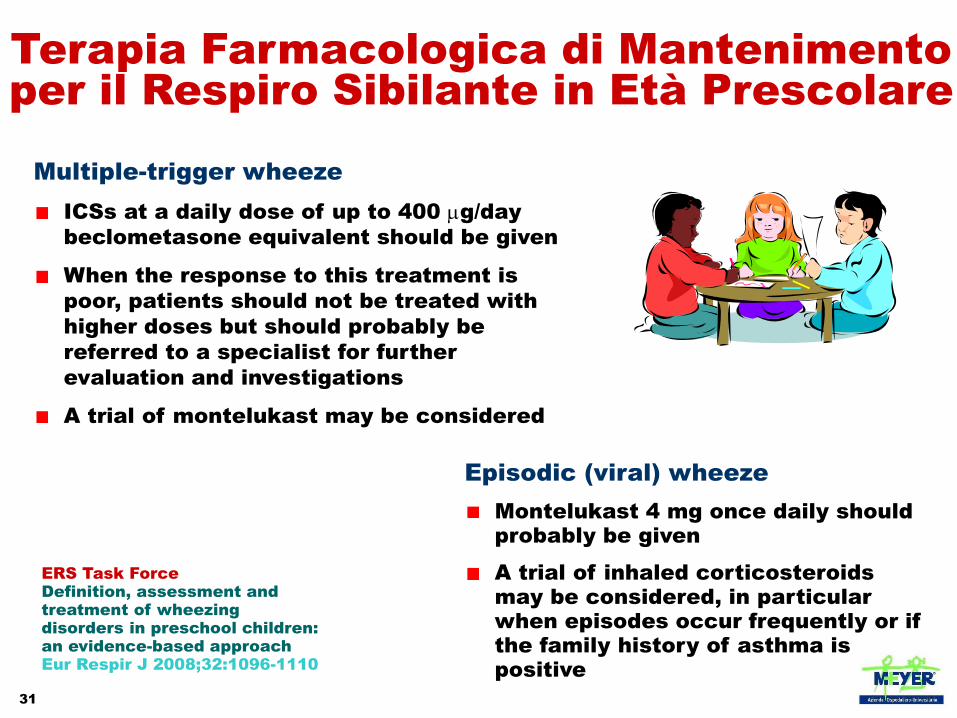
ERS Task Force
Definition, assessment and
treatment of wheezing
disorders in preschool children:
an evidence-based approach
Eur Respir J 2008;32:1096-1110
Terapia Farmacologica di Mantenimento
per il Respiro Sibilante in Età Prescolare
Multiple-trigger wheeze
ICSs at a daily dose of up to 400 mg/day
beclometasone equivalent should be given
When the response to this treatment is
poor, patients should not be treated with
higher doses but should probably be
referred to a specialist for further
evaluation and investigations
A trial of montelukast may be considered
Episodic (viral) wheeze
Montelukast 4 mg once daily should
probably be given
A trial of inhaled corticosteroids
may be considered, in particular
when episodes occur frequently or if
the family history of asthma is
positive
32 Acta Paediatrica 2010;99:56-60
33

34
Wheeze patterns in young children vary over time and with treatment, rendering
the distinction between episodic viral wheeze and multiple-trigger wheeze
unclear in many patients
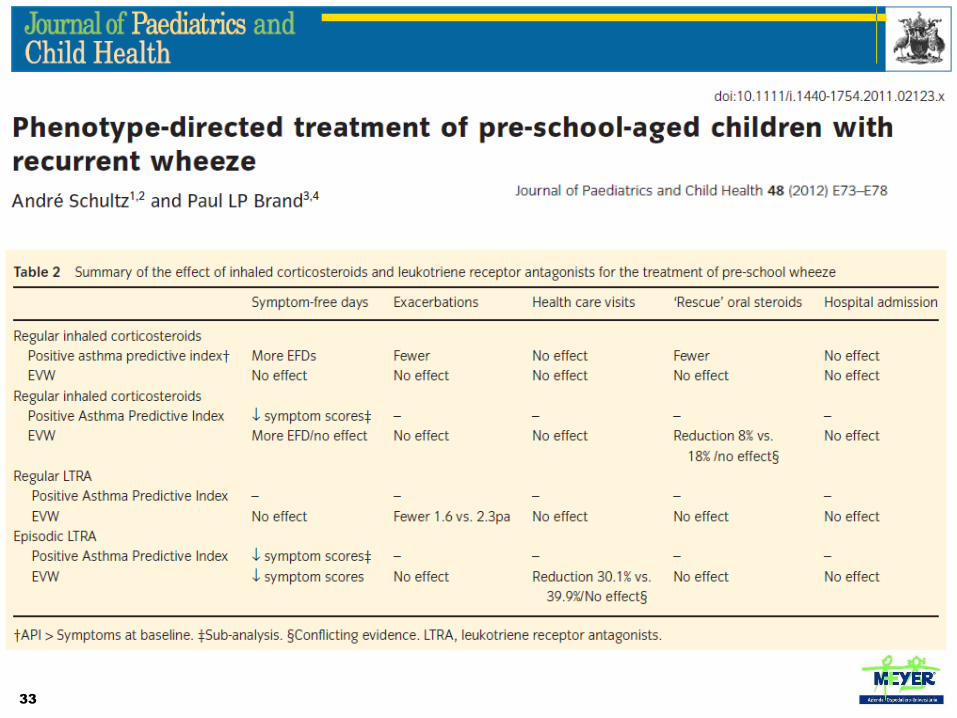
Inhaled corticosteroids remain first-line treatment for multiple-trigger wheeze,
but may also be considered in patients with episodic viral wheeze with frequent
or severe episodes, or when the clinician suspects that interval symptoms are
being under reported
Any controller therapy should be viewed as a treatment trial, with scheduled
close followup to monitor treatment effect
The group recommends discontinuing treatment if there is no benefit and taking
favourable natural history into account when making decisions about long-term
therapy

35
Conclusioni
I Fenotipi di Wheezing in Pediatria
L’asma non è un’unica malattia, ma
un insieme di malattie eterogenee
con sintomi in comune
Una delle maggiori sfide nel
trattamento dell’asma è la
comprensione dei diversi fenotipi
e dei meccanismi biologici sottostanti
L’identificazione di questi meccanismi ha
l’obiettivo finale di migliorare l’efficacia
dei trattamenti e delle strategie
Belgrave DCM et al. Expert Rev Clin Immunol 2013;9:921-936

36