Giornate Mediche Fiorentine - ASIAM - congressi … Paolo Pieragnoli Università degli Studi di...
87
Dr Paolo Pieragnoli Università degli Studi di Firenze Giornate Mediche Fiorentine Firenze 16 Novembre 2012
-
Upload
truongliem -
Category
Documents
-
view
217 -
download
0
Transcript of Giornate Mediche Fiorentine - ASIAM - congressi … Paolo Pieragnoli Università degli Studi di...

Dr Paolo Pieragnoli Università degli Studi di Firenze
Giornate Mediche Fiorentine
Firenze 16 Novembre 2012

• Incidenza e prevalenza della fibrillazione atriale (FA) aumentano con l’aumentare dell’età
Epidemiologia
Inc
ide
nza
(n
• 1
03/2
an
ni)
Benjamin EJ, et al. JAMA 1994
Uomini
Donne
Età (anni)
0
20
40
80
60
55-64 75-84 65-74 85-94
Framingham study

Prevalenza di fibrillazione atriale per età e sesso nello Studio ATRIA
0,10,4
1
1,7
3,4
5
7,2
9,1
0,2
0,9
1,7
3
5
11,1
10,3
7,3
<55 55-64 60-64 70-74 65-69 80-84 75-79 >85
Gruppi di età (anni)
Pre
vale
nza (
%)
0
2
4
6
8
10
12
Uomini
Donne
Go AS et al, JAMA 2001
17,974 soggetti con FA (0.95%) in
una popolazione USA (California)
di 1.89 milioni di persone
Rif. 1.7.1996-31.12.1997

Sti
ma d
ei so
gg
ett
i co
n F
A
(N, m
ilio
ni)
0
4
8
12
16
2000 2010 2020 2030
Anno
2040
Stima conservativa – Nessun
ulteriore aumento di incidenza
Miyasaka Y. Circulation, 2006
2050
Stima NON conservativa –
Continuo aumento di incidenza


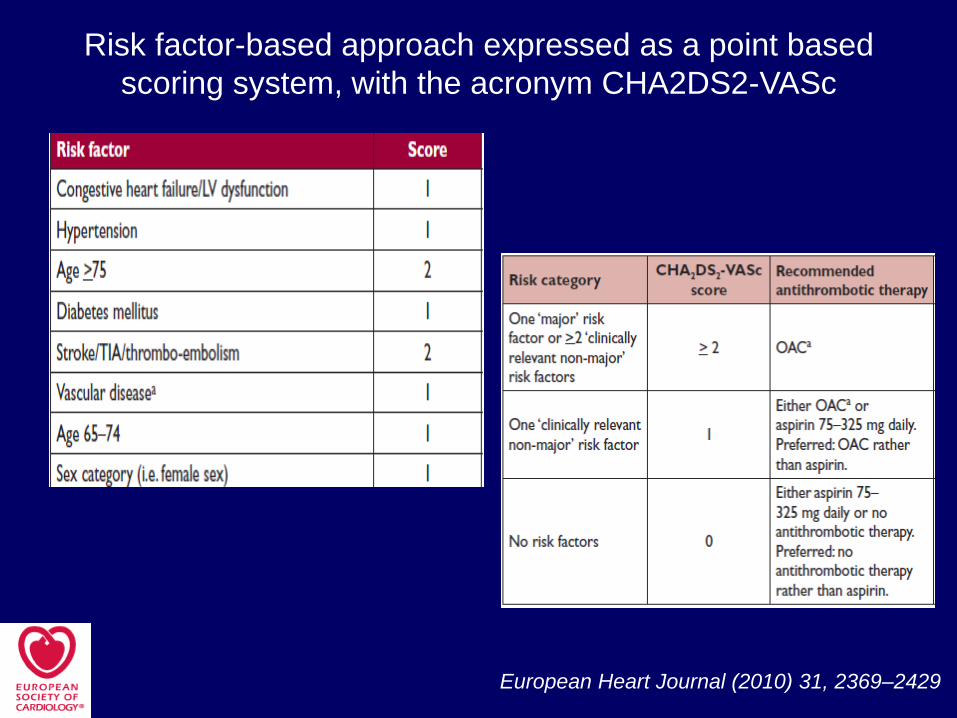
Risk factor-based approach expressed as a point based
scoring system, with the acronym CHA2DS2-VASc
European Heart Journal (2010) 31, 2369–2429

25 % Cardioembolic
Atherothrombotic
5-20 % Lacunar
5-10 % Infrequent
20 % Cryptogenic
25-30 %
20 %
15-20%
5-10 %
25-30 %
Artery
occlusion Vessel
rupture
15% 85%
Etiology of Stroke

Detection of Atrial Fibrillation After Stroke
and the Risk of Recurrent Stroke
Kamel et al. Journal of Stroke and Cerebrovascular Diseases, 2011

Atrial Fibrillation and Risk of Dementia:
A Prospective Cohort Study
Dublin et al. J Am Geriatric Soc 59:1369-1375, 2011
Risk of Incident Dementia and Alzheimer’s Disease (AD) Associated with Atrial Fibrillation
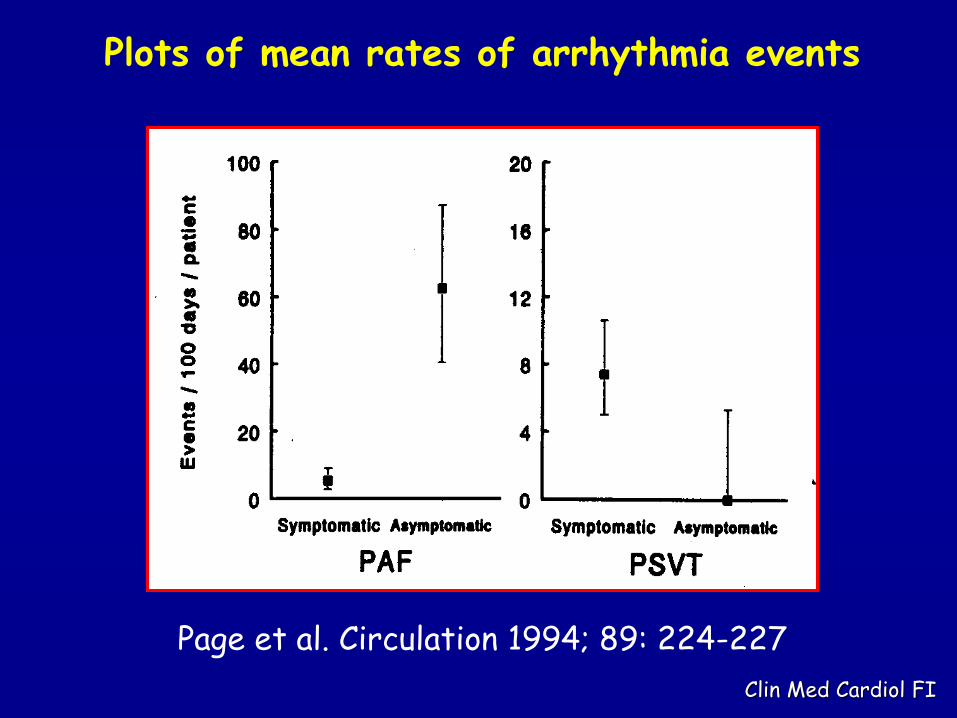
Clin Med Cardiol FI
Page et al. Circulation 1994; 89: 224-227
Plots of mean rates of arrhythmia events

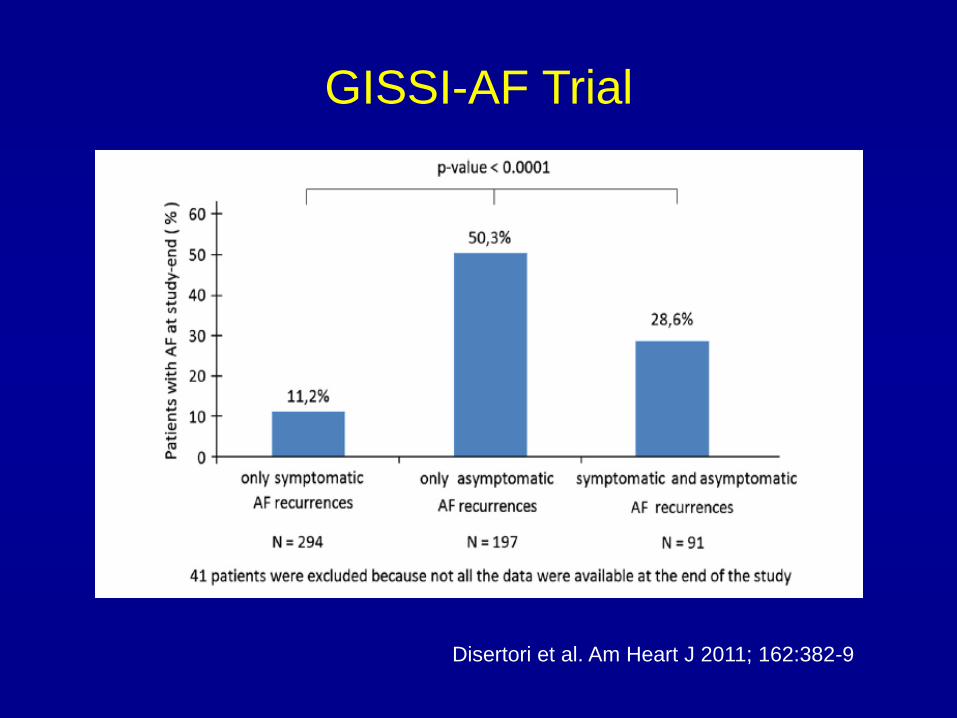
Disertori et al. Am Heart J 2011; 162:382-9
GISSI-AF Trial
Disertori et al. Am Heart J 2011; 162:382-9
GISSI-AF Trial

Disertori et al. Am Heart J 2011; 162:382-9
GISSI-AF Trial
CHADS2 Score > 2
OAC
Asymptomatic 77%
Symptomatic 50%
CHADS2 Score = 0
OAC
Asymptomatic 73,3%
Symptomatic 44,8%
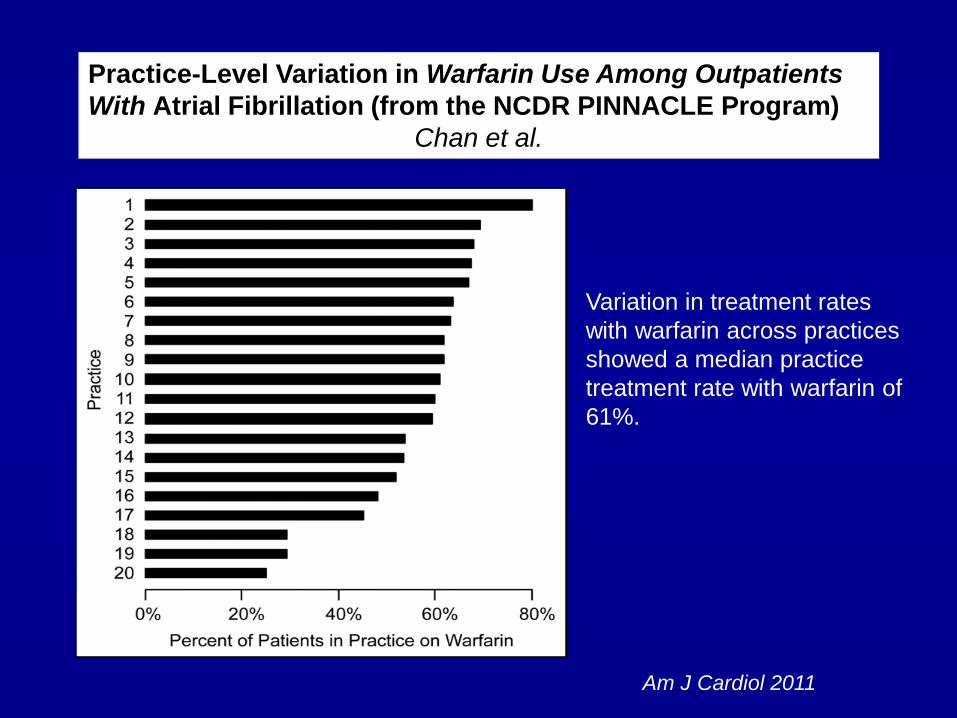
Practice-Level Variation in Warfarin Use Among Outpatients
With Atrial Fibrillation (from the NCDR PINNACLE Program)
Chan et al.
Variation in treatment rates
with warfarin across practices
showed a median practice
treatment rate with warfarin of
61%.
Am J Cardiol 2011

Kirchhof et al. Thromb Haemost 2011; 105: 1010–1023
Impact of the type of centre on management of AF patients:
Surprising evidence for differences in antithrombotic therapy decisions
Use of oral anticoagulation in the AFNET registry
split by type of enrolling centre.
A) Percentage of adequately anticoagulated patients according
to the 2001 ESC/AHA/ACC guidelines.
B) Percentage of adequately anticoagulated patients according
to the CHADS2 score .
C) Percentage of adequately anticoagulated patients according
to the CHA2DS2-VASc score .
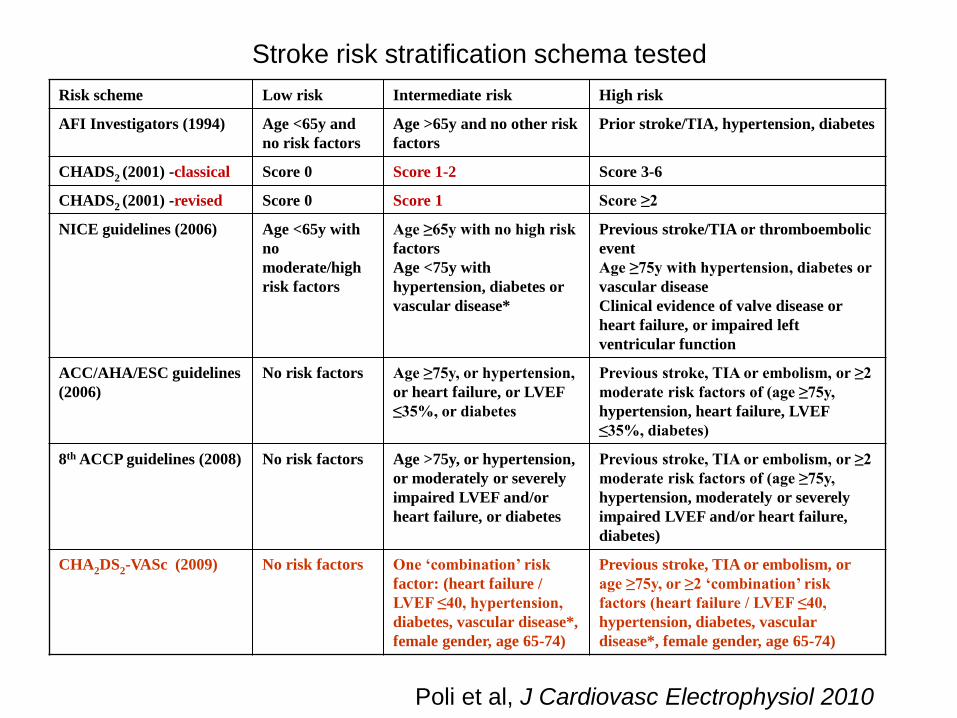
Stroke risk stratification schema tested
Risk scheme Low risk Intermediate risk High risk
AFI Investigators (1994) Age <65y and
no risk factors
Age >65y and no other risk
factors
Prior stroke/TIA, hypertension, diabetes
CHADS2 (2001) -classical Score 0 Score 1-2 Score 3-6
CHADS2 (2001) -revised Score 0 Score 1 Score ≥2
NICE guidelines (2006) Age <65y with
no
moderate/high
risk factors
Age ≥65y with no high risk
factors
Age <75y with
hypertension, diabetes or
vascular disease*
Previous stroke/TIA or thromboembolic
event
Age ≥75y with hypertension, diabetes or
vascular disease
Clinical evidence of valve disease or
heart failure, or impaired left
ventricular function
ACC/AHA/ESC guidelines
(2006)
No risk factors Age ≥75y, or hypertension,
or heart failure, or LVEF
≤35%, or diabetes
Previous stroke, TIA or embolism, or ≥2
moderate risk factors of (age ≥75y,
hypertension, heart failure, LVEF
≤35%, diabetes)
8th ACCP guidelines (2008) No risk factors Age >75y, or hypertension,
or moderately or severely
impaired LVEF and/or
heart failure, or diabetes
Previous stroke, TIA or embolism, or ≥2
moderate risk factors of (age ≥75y,
hypertension, moderately or severely
impaired LVEF and/or heart failure,
diabetes)
CHA2DS2-VASc (2009) No risk factors One ‘combination’ risk
factor: (heart failure /
LVEF ≤40, hypertension,
diabetes, vascular disease*,
female gender, age 65-74)
Previous stroke, TIA or embolism, or
age ≥75y, or ≥2 ‘combination’ risk
factors (heart failure / LVEF ≤40,
hypertension, diabetes, vascular
disease*, female gender, age 65-74)
Poli et al, J Cardiovasc Electrophysiol 2010
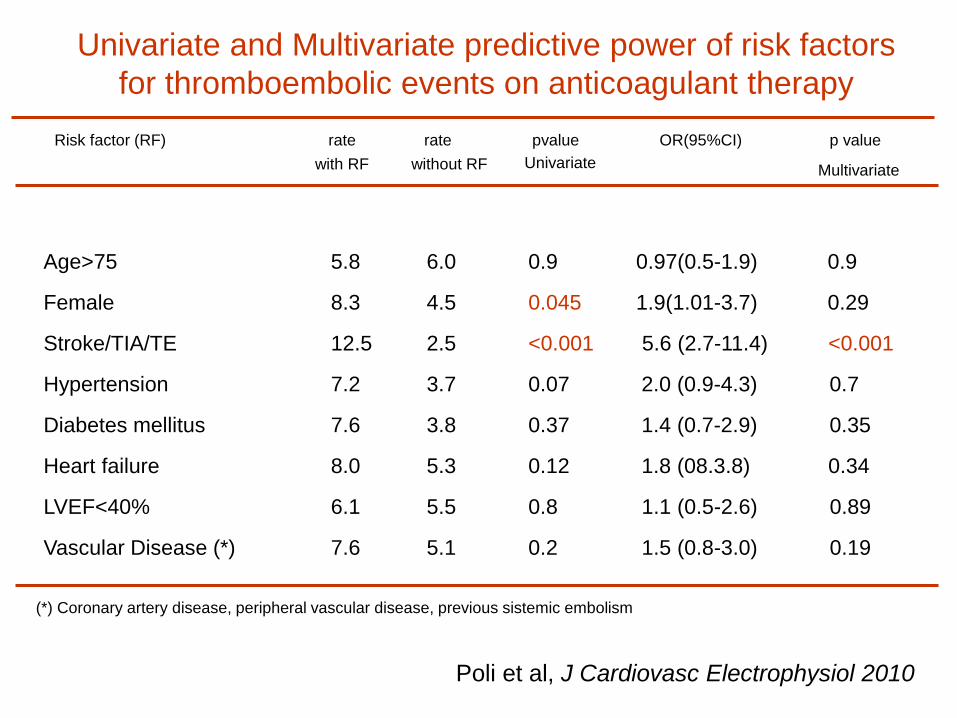
Univariate and Multivariate predictive power of risk factors
for thromboembolic events on anticoagulant therapy
Poli et al, J Cardiovasc Electrophysiol 2010
Risk factor (RF) rate rate pvalue OR(95%CI) p value
Age>75 5.8 6.0 0.9 0.97(0.5-1.9) 0.9
Female 8.3 4.5 0.045 1.9(1.01-3.7) 0.29
Stroke/TIA/TE 12.5 2.5 <0.001 5.6 (2.7-11.4) <0.001
Hypertension 7.2 3.7 0.07 2.0 (0.9-4.3) 0.7
Diabetes mellitus 7.6 3.8 0.37 1.4 (0.7-2.9) 0.35
Heart failure 8.0 5.3 0.12 1.8 (08.3.8) 0.34
LVEF<40% 6.1 5.5 0.8 1.1 (0.5-2.6) 0.89
Vascular Disease (*) 7.6 5.1 0.2 1.5 (0.8-3.0) 0.19
(*) Coronary artery disease, peripheral vascular disease, previous sistemic embolism
with RF without RF Univariate Multivariate
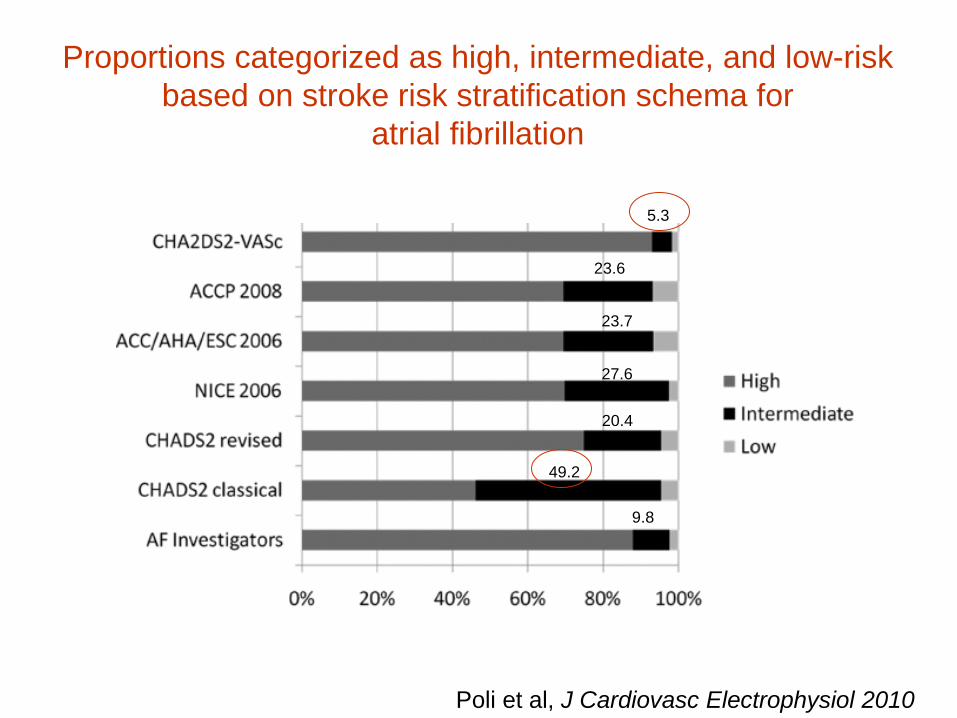
Proportions categorized as high, intermediate, and low-risk
based on stroke risk stratification schema for
atrial fibrillation
Poli et al, J Cardiovasc Electrophysiol 2010
5.3
49.2
23.6
27.6
20.4
23.7
9.8
The proportion of patients assigned to
individual risk categories varied widely across
the schema, with those categorised as
‘moderate-risk’ ranging from 5.3% (CHA2DS2-
VASc) to 49.2% (CHADS2-classical). Patients
classified as ‘low-risk’ by all risk schemas were
truly low risk, with no TE events recorded.

In this cohort of consecutive elderly AF patients
attending an anticoagulation clinic, current
published risk schemas have modest predictive
ability, with c-statistics ranging from 0.54 (AFI) to
0.72 (CHA2DS2-VASc).
CHADS2 and CHA2DS2-VASc schemas show the
best predictive value for thromboembolism.

CHADS2 Score, PAF Duration and Stroke Risk
• 568 pts. with MDT AT500 continuously monitored for 1 year
No AF at FU (AT/AF < 5 min in 1 day)
5 min < AT/AF Episodes < 24 h
AT/AF Episodes > 24 h
CHADS2 score 0 1 2 3
58 Pts 4 Pts 24 Pts
54 Pts 7 Pts 76 Pts 42 Pts
59 Pts 113 Pts 6 Pts 45 Pts
(3 out of 351 Pts) 0.8 % vs 5 % (11 out of 217 Pts)
P = 0.035 Botto, Padeletti et al. J Cardiovasc El 2009
Risk Stratification
80 Pts
Patients with a dual-chamber pacemaker (Medtronic AT-500) and history of
paroxysmal atrial tachyarrhythmias were included into this study.
A day by day trend of AF burden (= time spent in AF during each day) was
available for each patient during 1-year follow-up.
Patients were divided into 3 groups: (i) maximum AF burden <5min per day [AF-
free]; (ii) maximum AF burden >5min but <24h per day [AF-5min]; and (iii) AF
burden of 24h or higher (episodes longer than 24h) [AF-24h].
Stroke 2011, 42(6):1768-70

Results 1:
Sensitivity & Specificity of CHADS2 score
0
20
40
60
80
100
Sensitivity Specificity
Case 1:Treating all Pts with score ≥ 1
CHADS2 score:
0 1 2 ≥3
0
20
40
60
80
100
Sensitivity Specificity
Case 2: Treating all Pts with score ≥ 2
CHADS2 score:
0 1 2 ≥3
Stroke 2011, 42(6):1768-70
86
30 43
78
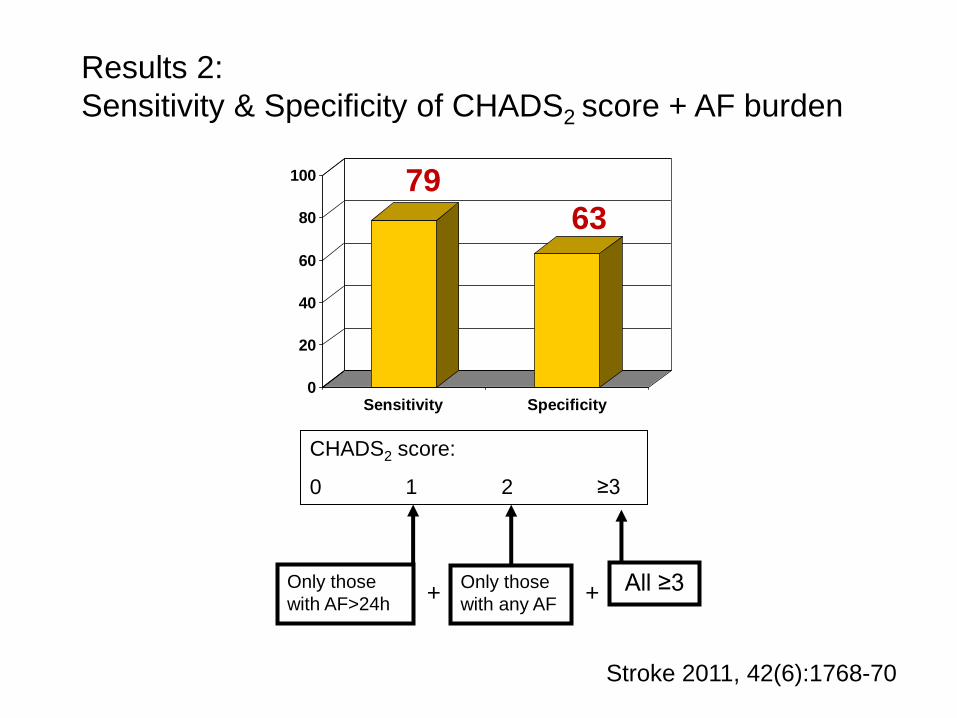
Results 2:
Sensitivity & Specificity of CHADS2 score + AF burden
0
20
40
60
80
100
Sensitivity Specificity
Only those
with AF>24h
Only those
with any AF All ≥3
CHADS2 score:
0 1 2 ≥3
+ +
Stroke 2011, 42(6):1768-70
79
63
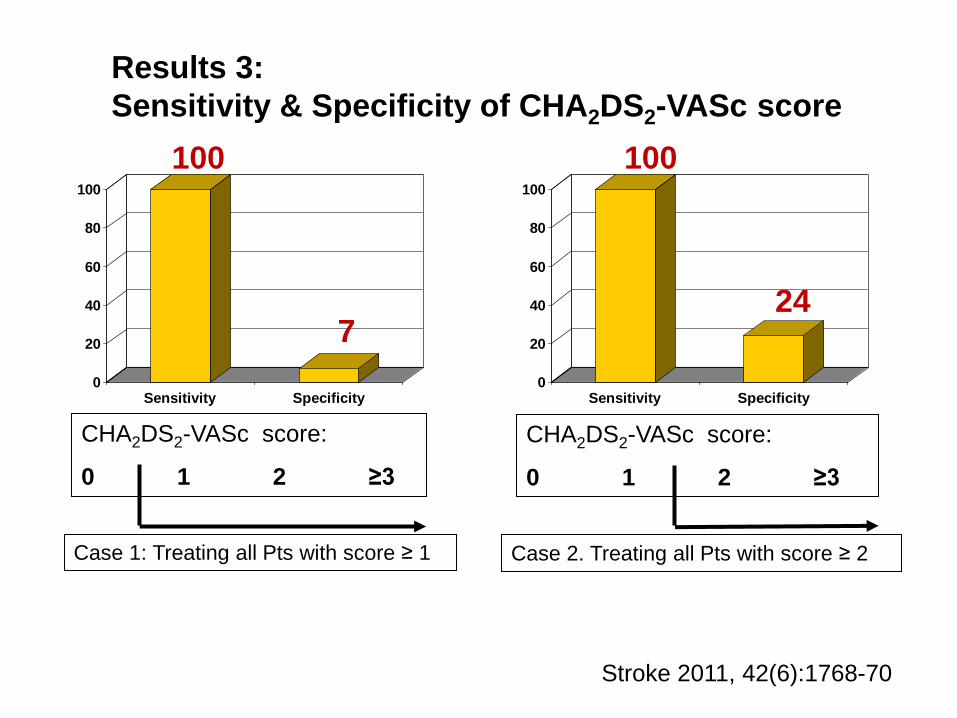
Results 3:
Sensitivity & Specificity of CHA2DS2-VASc score
Case 1: Treating all Pts with score ≥ 1
CHA2DS2-VASc score:
0 1 2 ≥3
Case 2. Treating all Pts with score ≥ 2
CHA2DS2-VASc score:
0 1 2 ≥3
0
20
40
60
80
100
Sensitivity Specificity0
20
40
60
80
100
Sensitivity Specificity
Stroke 2011, 42(6):1768-70
100
7
100
24
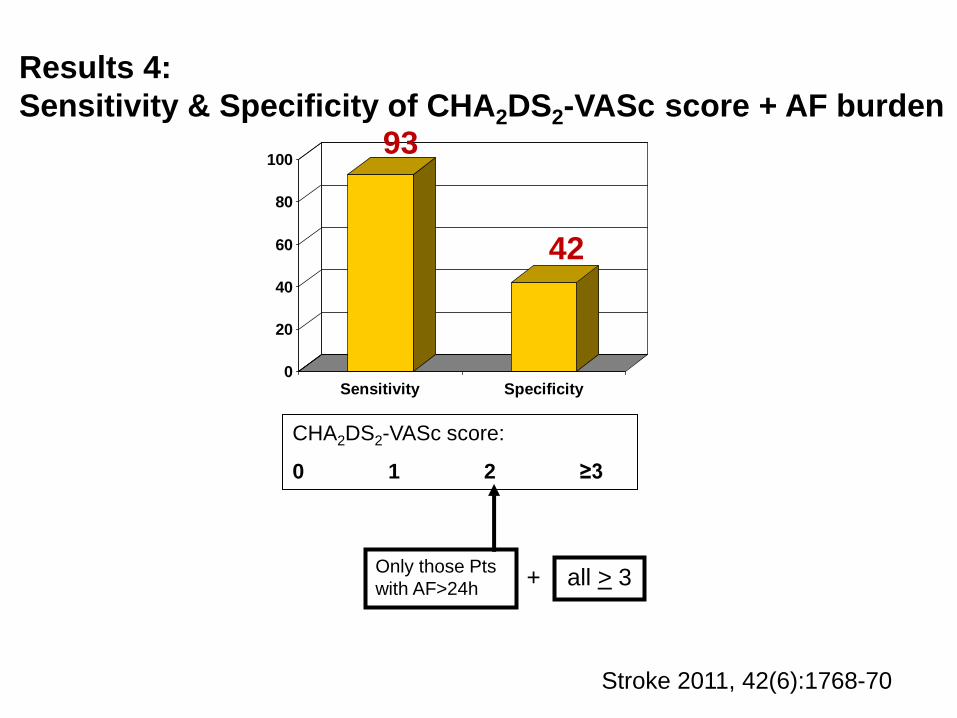
Results 4:
Sensitivity & Specificity of CHA2DS2-VASc score + AF burden
0
20
40
60
80
100
Sensitivity Specificity
CHA2DS2-VASc score:
0 1 2 ≥3
Only those Pts
with AF>24h all > 3 +
Stroke 2011, 42(6):1768-70
93
42

• Risk stratification for stroke can be improved by combining either CHADS2 or CHA2DS2-VASc score with AF parameters.
• CHA2DS2-VASc scheme has the highest sensitivity to predict TE: its integration with continuous AF burden improves specificity and the discriminating ability for TE.
• Thus, data on AF burden may refine risk stratification for stroke and this is evident even when OAC is more commonly prescribed, as expected, in patients with the highest AF burden.
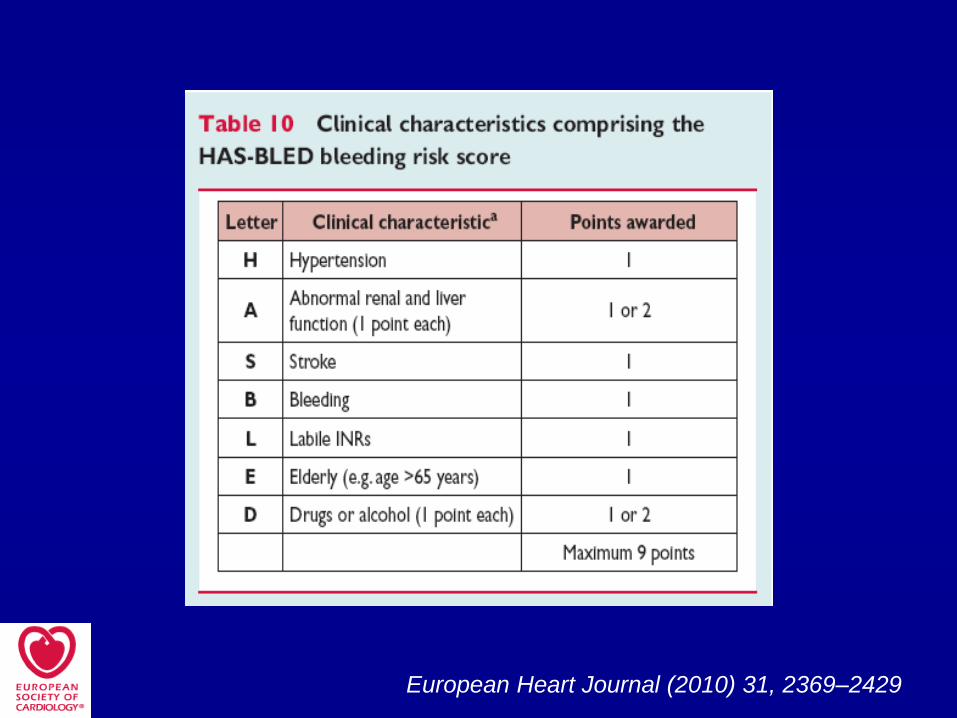
European Heart Journal (2010) 31, 2369–2429

Thromb Haemost 2011
Risks of Thromboembolism and Bleeding
with Thromboprophylaxis in patients with Atrial Fibrillation:
A net clinical benefit analysis using a ‘real world’ nationwide cohort study Olesen et al.
What does this paper add?
● Regardless of HAS-BLED score, there is negative net clinical
benefit of oral anticoagulation if patients are ‘truly low risk’
(i.e. CHA2DS2-VASc score = 0) and, a neutral or positive net
clinical benefit of oral anticoagulation for patients with
CHADS2 score ≥ 0 or CHA2DS2-VASc score ≥ 1.
● Acetylsalicylic acid should not be used for
thromboprophylaxis in any patient with atrial fibrillation.





Eur Heart J 2010
European Heart Journal (2010) 31, 2369–2429
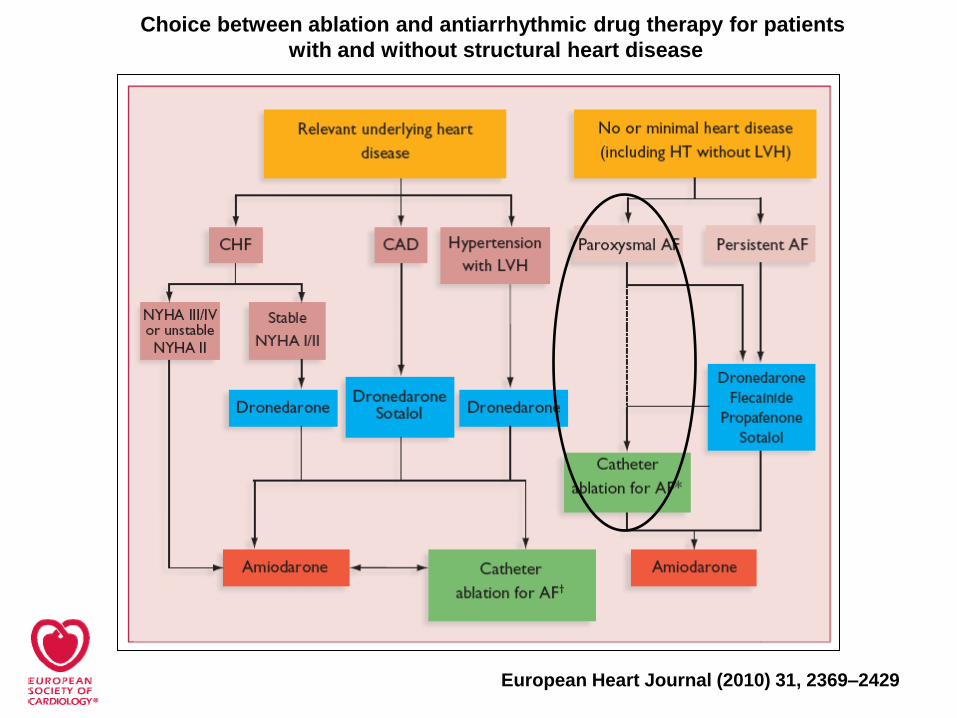
Choice between ablation and antiarrhythmic drug therapy for patients
with and without structural heart disease
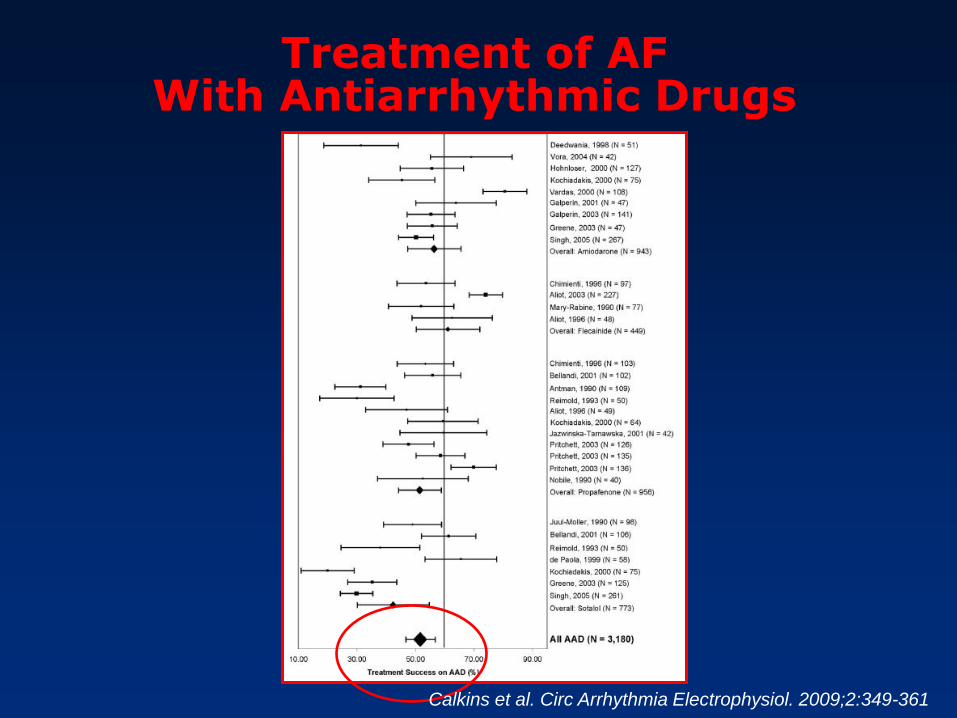
Treatment of AF With Antiarrhythmic Drugs
Calkins et al. Circ Arrhythmia Electrophysiol. 2009;2:349-361
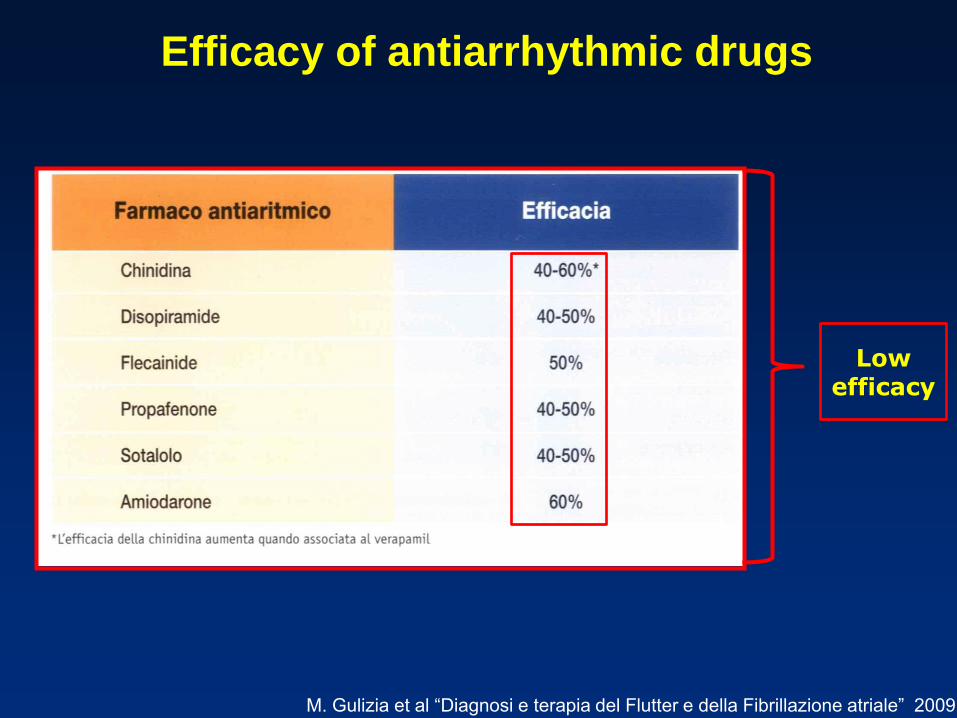
Efficacy of antiarrhythmic drugs
M. Gulizia et al “Diagnosi e terapia del Flutter e della Fibrillazione atriale” 2009
Low efficacy





Registry on Cardiac Rhythm Disorders Assessing
the Control of Atrial Fibrillation (RecordAF)
Rhythm control
Atrial fibrillation and
Structural Heart Disease.
Atrial fibrillation and Congestive
Heart Failure.
Lone Atrial Fibrillation
Kowey PR et al. Clin. Cardiol. 33, 3, 172–178 (2010)
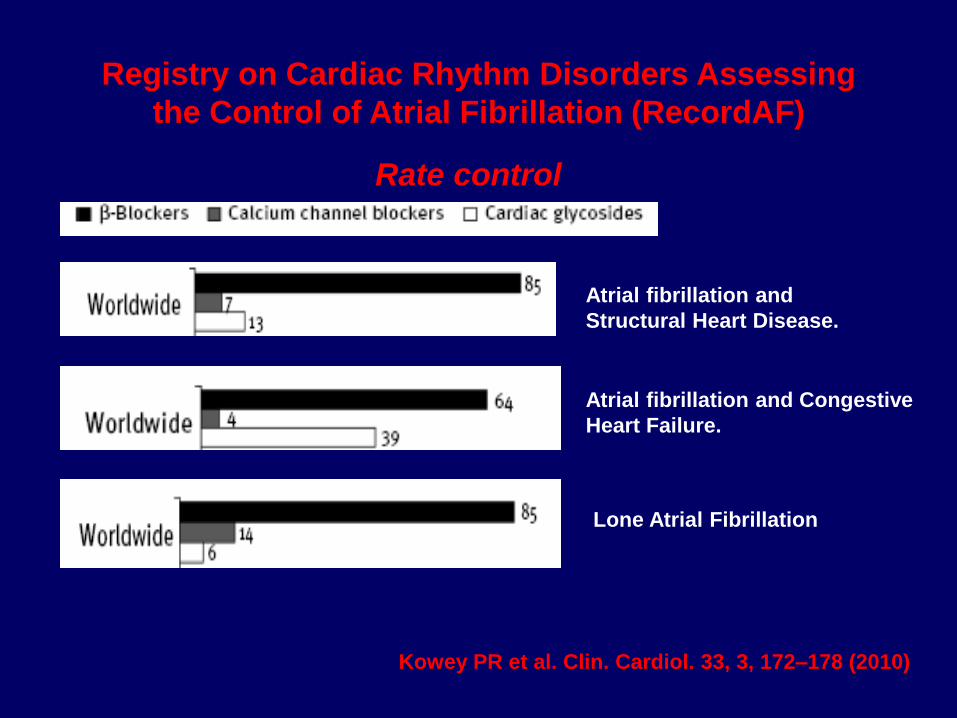
Registry on Cardiac Rhythm Disorders Assessing
the Control of Atrial Fibrillation (RecordAF)
Rate control
Atrial fibrillation and
Structural Heart Disease.
Atrial fibrillation and Congestive
Heart Failure.
Lone Atrial Fibrillation
Kowey PR et al. Clin. Cardiol. 33, 3, 172–178 (2010)

UK General Practice Research Database
(GPRD) Rhythm control agents and Adverse Events
Relative risk of adverse effects of Amiodarone, Flecainide or Sotalol in
cases compared with controls.
Taylor et al. Int J Clin Pract 2010
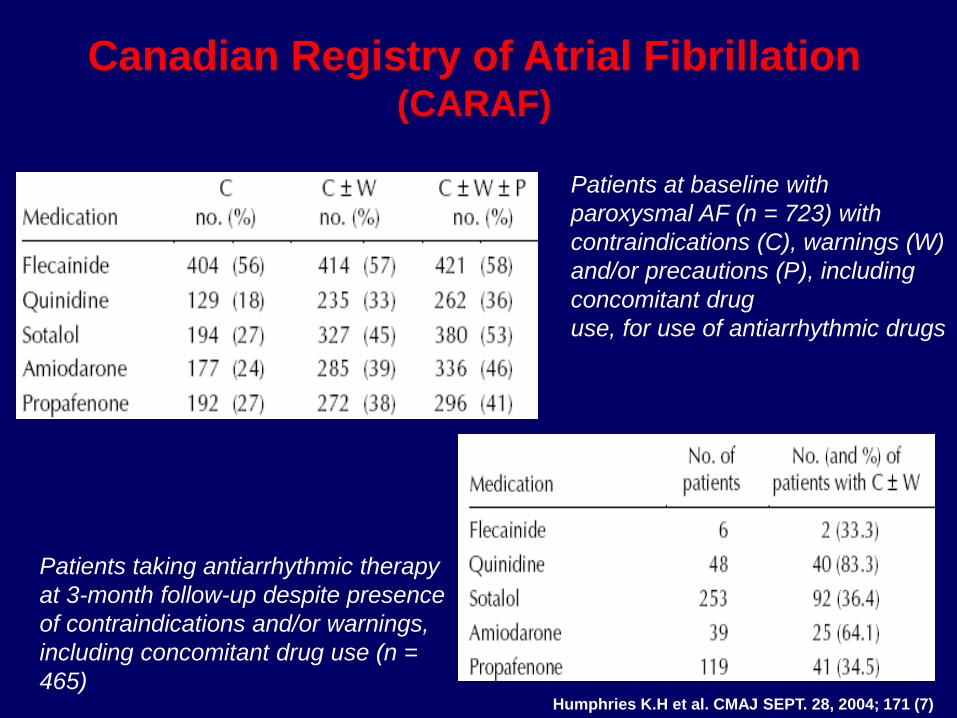
Canadian Registry of Atrial Fibrillation (CARAF)
Humphries K.H et al. CMAJ SEPT. 28, 2004; 171 (7)
Patients at baseline with
paroxysmal AF (n = 723) with
contraindications (C), warnings (W)
and/or precautions (P), including
concomitant drug
use, for use of antiarrhythmic drugs
Patients taking antiarrhythmic therapy
at 3-month follow-up despite presence
of contraindications and/or warnings,
including concomitant drug use (n =
465)

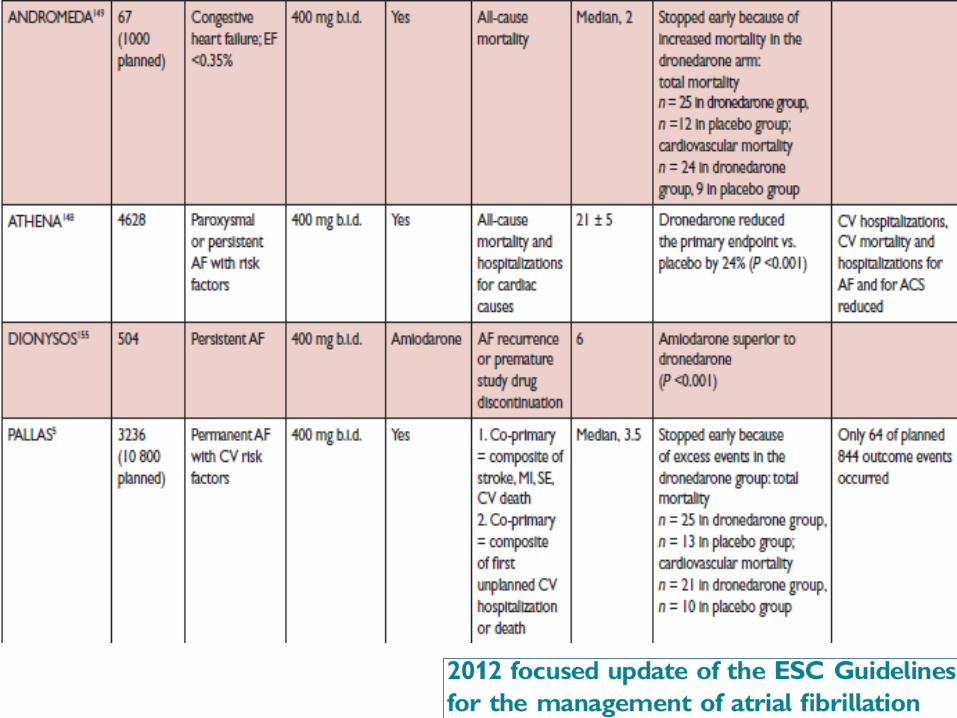
Tung R et al. J Am Coll Cardiol 2008;52:1111–21
Amiodarone and Dronedarone:
not innocent drugs!
Dronedarone in patients
with congestive heart
failure: insights from
ATHENA
Stefan H. Hohnloser et al.
Conclusion …. Dronedarone
should be controindicated in
patients with NYHA class IV or
unstable classes II and III CHF.
European Heart Journal April 30, 2010

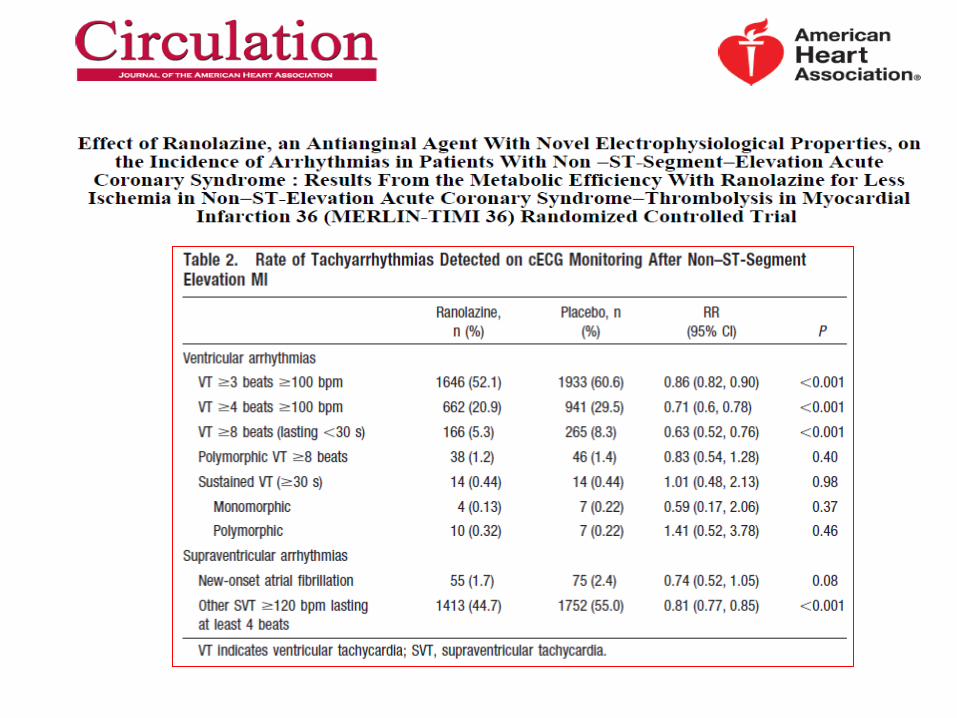


Conclusion: High
dose oral ranolazine
shows utility as a
possible safe agent to
convert new or
paroxysmal AF
(13 on 18)

Am J Cardiol 2011;108:673-676
The present study compared amiodarone versus ranolazine for the prevention of AF after CABG
The patients received either amiodarone (400 mg preoperative followed by 200 mg twice daily for 10 to 14 days)
or ranolazine (1500 mg preoperative followed by 1000 mg twice daily for 10 to 14 days)
Number of Patients: 393
Amiodarone (n=211 [53.7%]) Ranolazine (n=182 [46.3%])





Catheter ablation: pulmonary veins isolation

Catheter ablation: pulmonary veins isolation
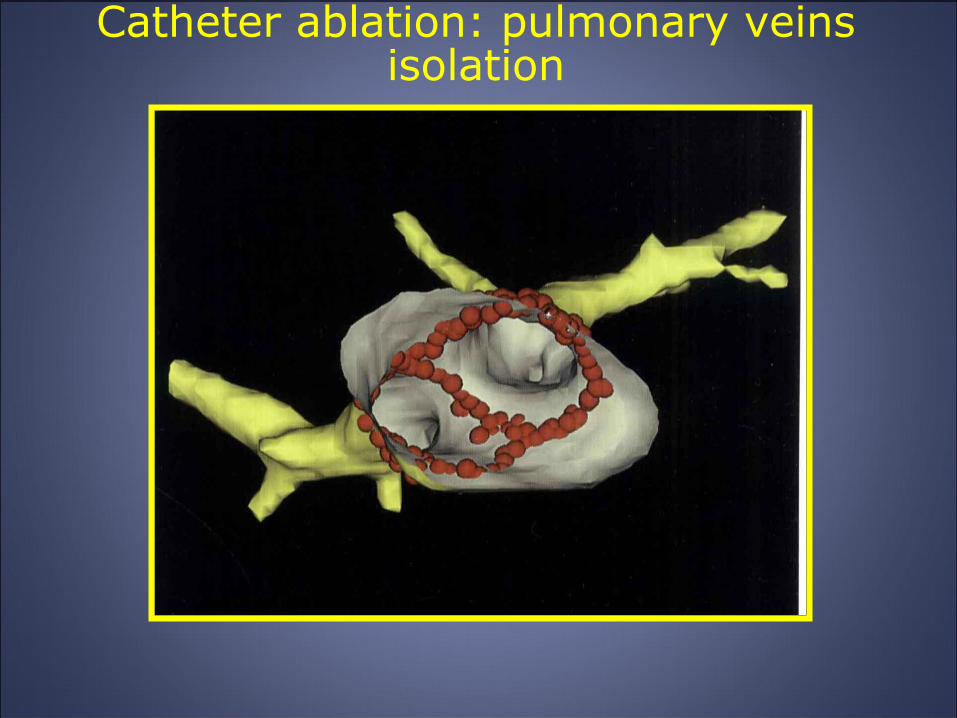
Catheter ablation: pulmonary veins isolation
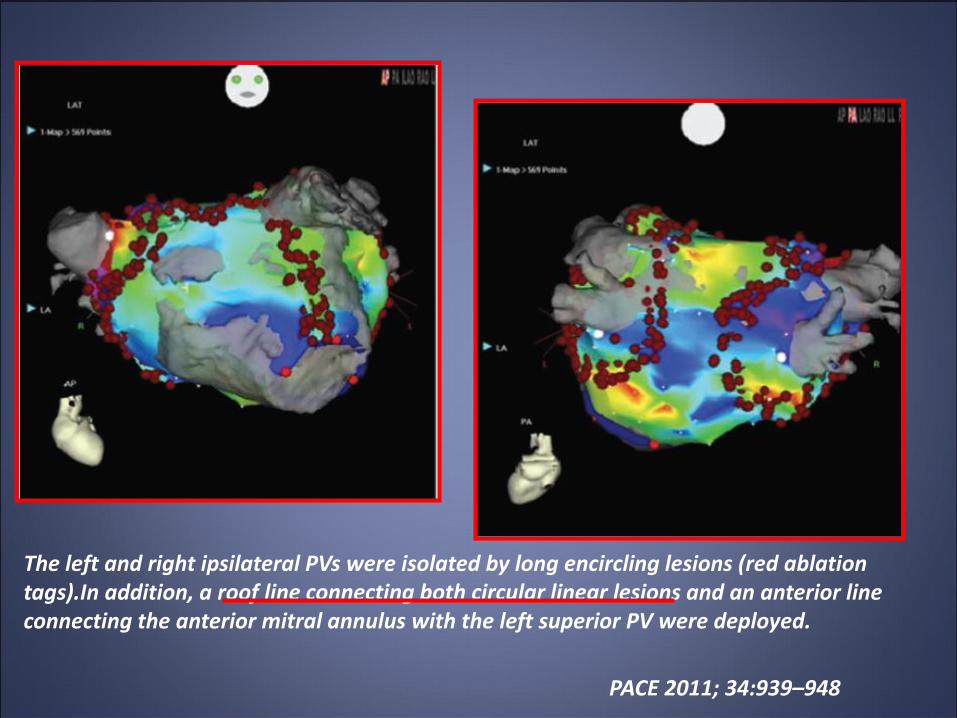
The left and right ipsilateral PVs were isolated by long encircling lesions (red ablation tags).In addition, a roof line connecting both circular linear lesions and an anterior line connecting the anterior mitral annulus with the left superior PV were deployed.
PACE 2011; 34:939–948
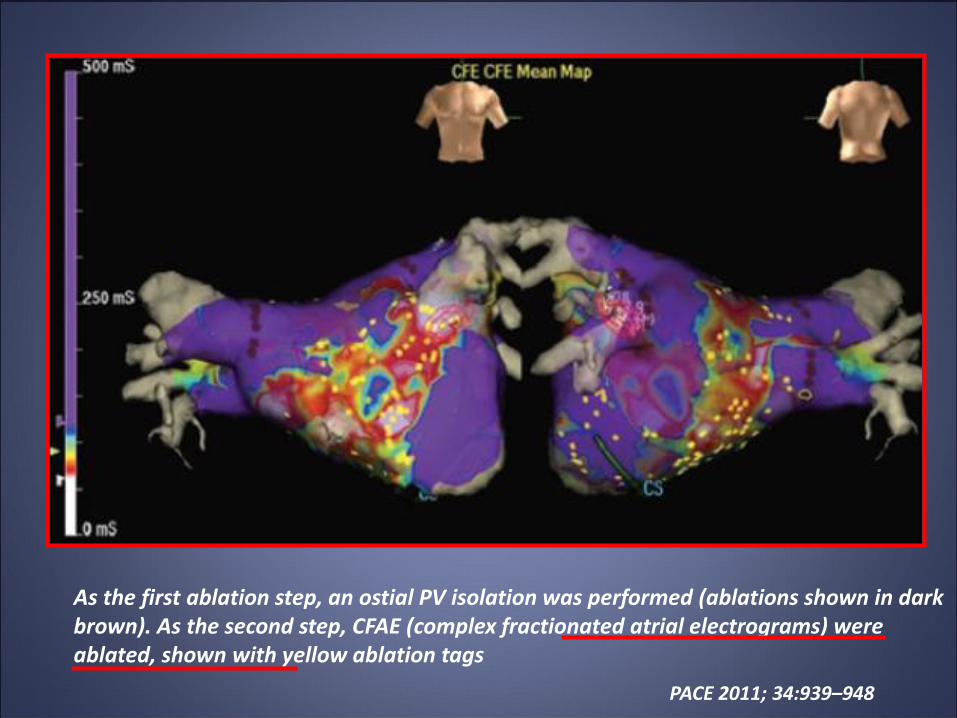
As the first ablation step, an ostial PV isolation was performed (ablations shown in dark brown). As the second step, CFAE (complex fractionated atrial electrograms) were ablated, shown with yellow ablation tags
PACE 2011; 34:939–948

Fluoroscopic anteroposterior view of the circular mapping catheter positioned at the ostium of the LAA and the ablation catheter during isolation of the LAA. 3-dimensional CT reconstruction registered into the CARTO mapping system showing the ablation sites required to complete the LAA isolation.

Angioplasty in Acute MI
We were overzealous with the angiojet. Let
us fly her to Boston for
a body transplant
Have we done enough work
on the left atrium to prevent
atrial fibrillation?
AF Ablation
85





Long-term outcome after catheter ablation
for atrial fibrillation: safety, efficacy and
impact on prognosis
Long-term freedom from AF or
other atrial tachyarrhythmias for
paroxysmal AF and persistent
AF.
The studies shown have the
longest follow-up reported to
date (2.5 e 4.7 years).
Hunter RJ et al. Heart 2010;96:1259e1263

Catheter Ablation Is Established as a Treatment Option for Atrial Fibrillation
Takahashi A. Circ J 2010; 74: 1972 – 1977
Freedom from atrial fibrillation in Randomized Clinical Trials comparing the outcomes of
catheter ablation and antiarrhythmic drugs


Percentiles (70%, 80% and 90%) of the burden of atrial fibrillation in the two groups
at baseline and during follow-up are shown. The same poercentiles are also shown
for the cumulative burden of atrial fibrillation

Cost Comparison of Ablation Versus Antiarrhythmic Drugs as First-Line Therapy for Atrial Fibrillation:
An Economic Evaluation of the RAAFT Pilot Study
Khaykin Y et al. J Cardiovasc Electrophysiol, Vol. 20, pp. 7-12, January 2009

…there are substantial data that clearly show
ablation to be a reasonable alternative to
antiarrhythmic drugs at least in patients with no
or minimal heart disease who have paroxysmal
AF, assuming that the electrophysiologist
performing the study has substantial experience
in ablation…
J Cardiovasc Electrophysiol, Vol. 21, pp. 946-958, August 2010
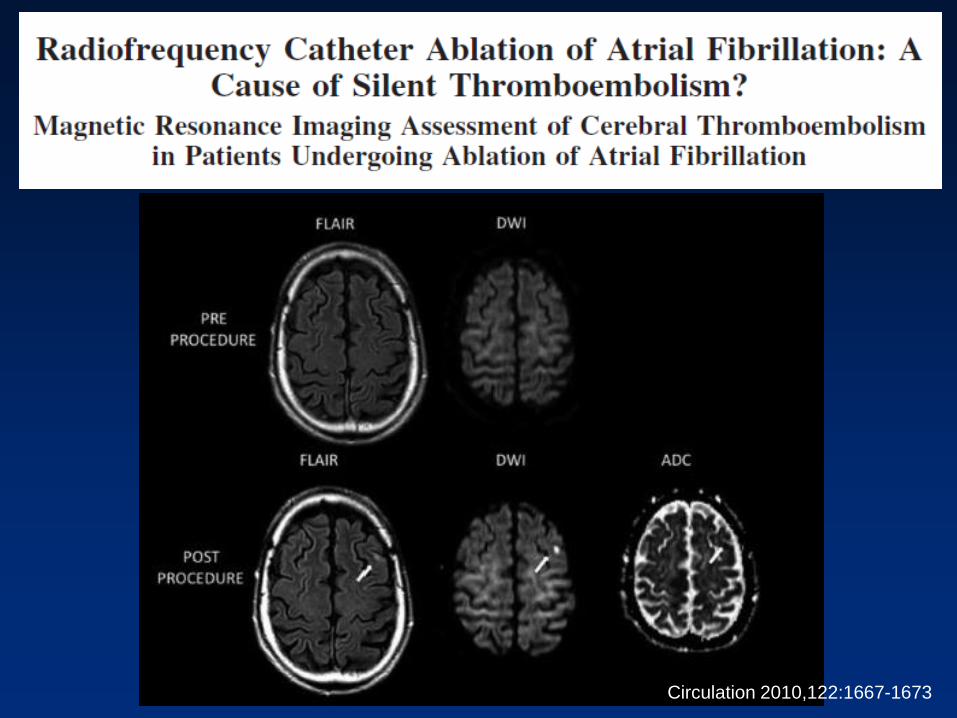
Circulation 2010,122:1667-1673

Circulation 2010,122:1667-1673

Circulation 2010,122:1667-1673
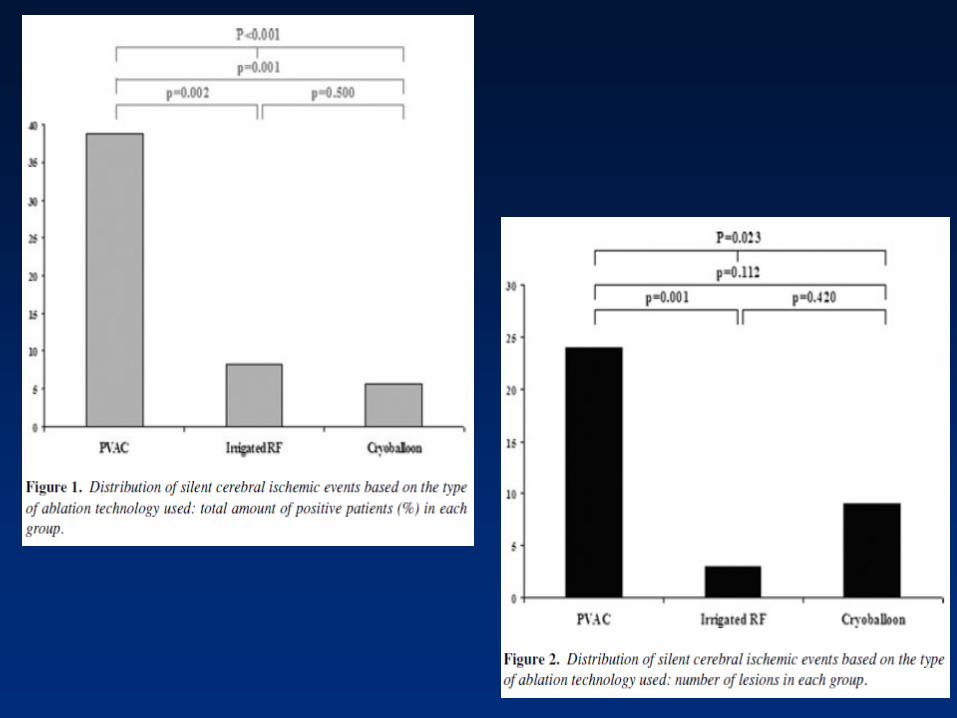
• LA transcatheter ablation for AF is associated with silent cerebral
thromboembolism.
• Periprocedural symptomatic cerebral thromboembolism (transient ischemic
attack) represents only a minimal part of the thromboembolic risk (0.4%
symptomatic versus 14% asymptomatic; odds ratio40.53).
• The thromboembolic risk is independent from clinical parameters such as age,
hypertension, and diabetes mellitus and from the type of AF, occurrence of previous
cerebral thromboembolic events, preprocedural antithrombotic treatment, and the
ablation strategy used.
•In univariate and multivariable analyses, the most important factor that correlated
with cerebral embolism was electric or pharmacological conversion to sinus rhythm
during the procedure,with a significantly increased odds ratio of 2.75.
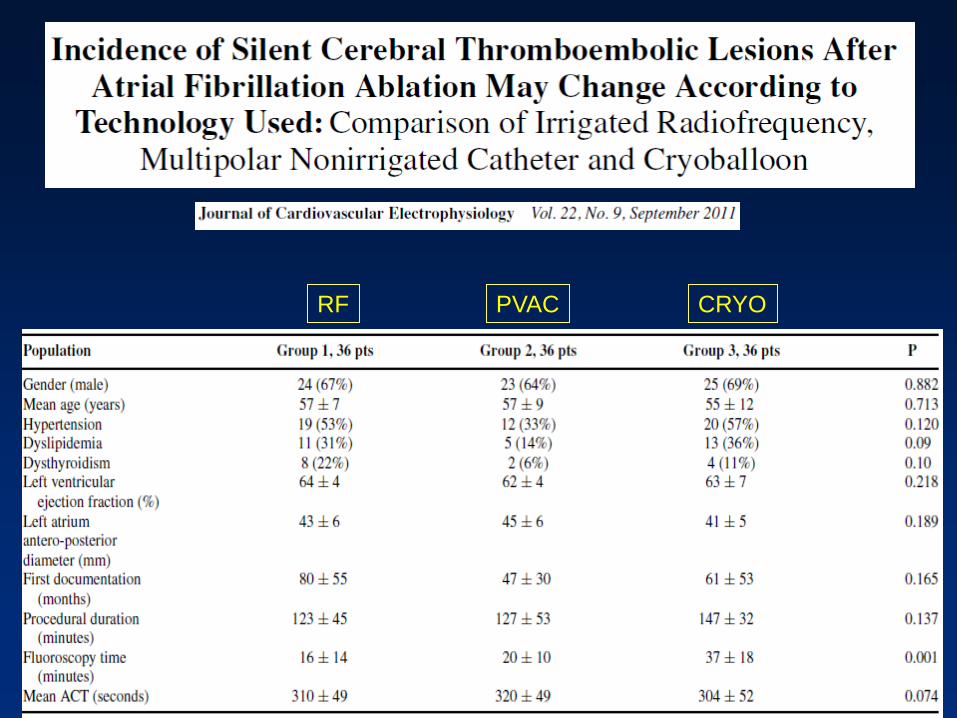
RF PVAC CRYO

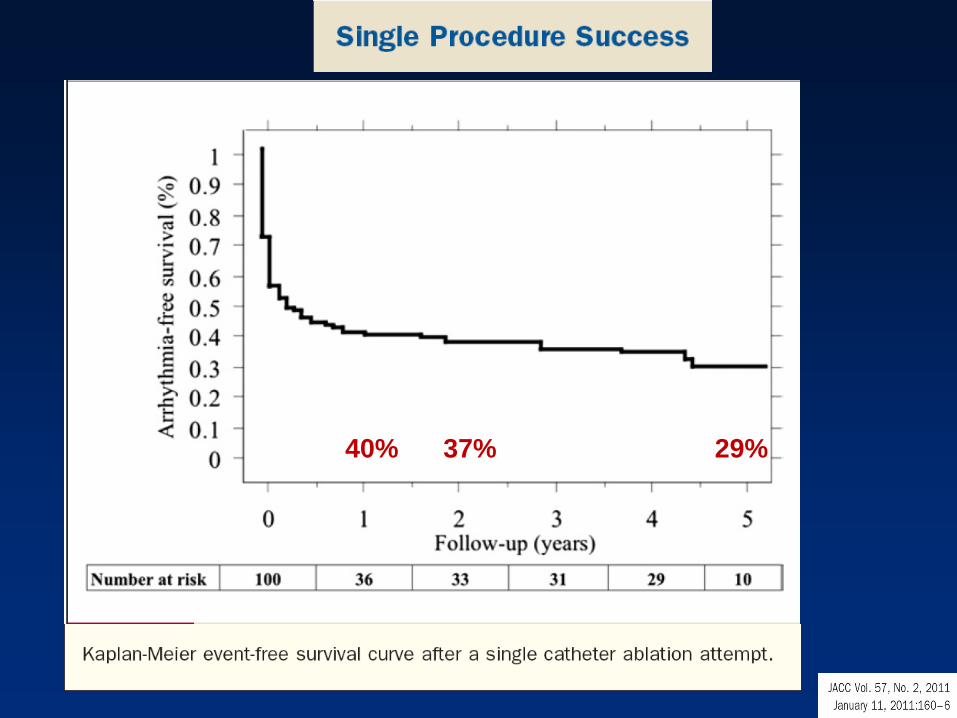
40% 37% 29%
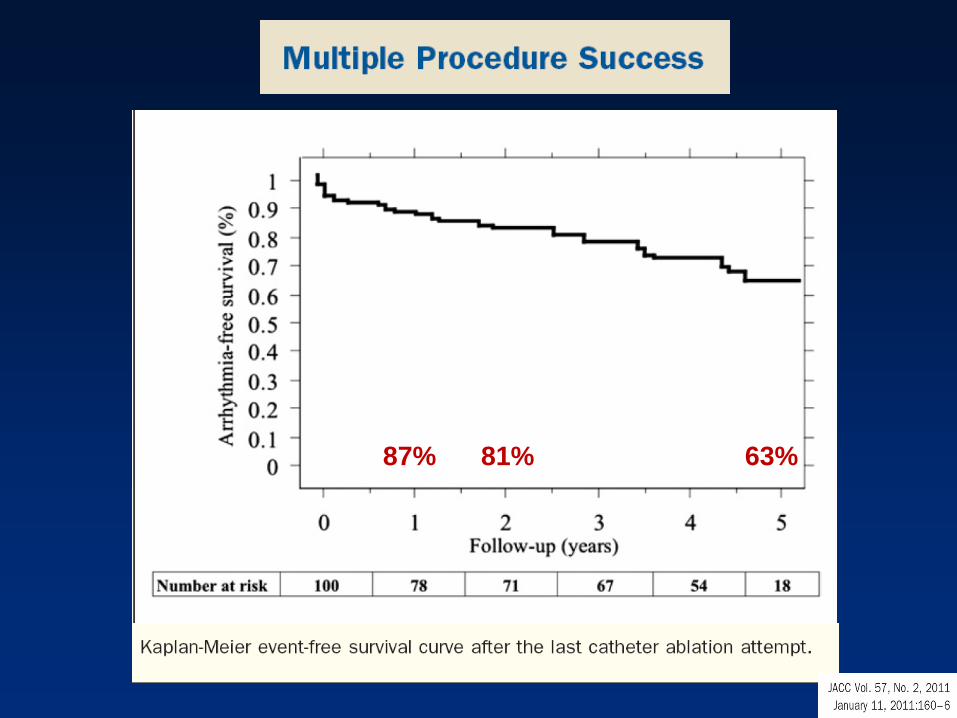
87% 81% 63%

Statua romana di Atlante (sec II
d.) Museo Archeologico
Nazionale di Napoli

Dear Professor Einthoven,
… At present we are working at
Fibrillation of the Auricles, but it is a
very tough nut to crack.
With kindest regards, Very sincerely,
yours,
Thomas Lewis.
Sept. 2 1919