
Facoltà di medicina e Chirurgia - fisiobrain.com · L’EMG di superfiie misura l’attività...
31
Università degli Studi di Genova Facoltà di medicina e Chirurgia Master in Riabilitazione dei Disturbi Muscoloscheletrici A.A. 2009-2010 Campus Universitario di Savona In collaborazione con Master of Science in Manual Therapy Vrije Universiteit Brussel Affidabilità dell’utilizzo di sistemi sEMG: studio della fatigue dei muscoli del cingolo scapolare e le conseguenti modificazioni nel controllo motorio dell’arto superiore. Candidato: Paolo Borean Relatore: Manolo Migliorini
Transcript of Facoltà di medicina e Chirurgia - fisiobrain.com · L’EMG di superfiie misura l’attività...

Università degli Studi di Genova Facoltà di medicina e Chirurgia
Master in Riabilitazione dei Disturbi Muscoloscheletrici A.A. 2009-2010
Campus Universitario di Savona In collaborazione con Master of Science in Manual Therapy
Vrije Universiteit Brussel
Affidabilità dell’utilizzo di sistemi sEMG: studio della fatigue
dei muscoli del cingolo scapolare e le conseguenti
modificazioni nel controllo motorio dell’arto superiore.
Candidato:
Paolo Borean
Relatore:
Manolo Migliorini
1
Indice
Abstract 2
1. Introduzione 4
2. Materiali e metodi 7
3. Risultati 8
3.1 diagramma di flusso 9
3.2 tabelle sinottiche 10
4. Discussione 17
4.1 sEMG 17
4.2 controllo motorio 19
5. Conclusioni 25
6. Bibliografia 27
2
Abstract
Obiettivi: l’obiettivo del nostro lavoro è quello di valutare l’affidabilità della sEMG in
relazione all’analisi della fatica muscolare e alle conseguenze legate al controllo motorio
dell’arto superiore.
Materiali e metodi: La ricerca è stata effettuata sul data base MEDLINE, in un
lasso di tempo che va dal 01/01/2001 al 01/01/2011, utilizzando le parole chiave “ EMG”,
“fatigue”, “shoulder”, “upper trapezius”, “kinematics”, “scapula”, “healthy subjects”
combinandole tra loro attraverso l’utilizzo degli operatori booleani. Sono stati inseriti i
limiti rispetto alla lingua di pubblicazione (inglese) e al campionamento dei soggetti (sani).
Risultati: la ricerca ha portato alla selezione di 20 articoli di cui 4 reviews.
Discussione: La registrazione del segnale EMG è, come è noto, influenzata da un
numero elevato di fattori; a fronte di tanta variabilità il numero di lavori rintracciabili in
letteratura che offrano risultati e conclusioni supportate da un corretto uso degli strumenti
statistici è decisamente ridotto. Non sembra inoltre esserci accordo sul concetto di
ripetibilità e sui protocolli da effettuare per verificarne la consistenza, né sulla tipologia di
elettrodi da utilizzare.
Da tutti gli studi presi in esame, tranne uno, si rivela una correlazione tra fatica muscolare e
alterazioni della dinamica del movimento dell’arto superiore, soprattutto del controllo
cinematico della scapola e dell’omero.
Conclusioni: Non sono numerose le evidenze che mettono in relazione uno specifico task
motorio con determinate alterazioni del segnale EMG o che evidenziano il rapporto tra
fatica e deficit nel controllo motorio.
Nonostante ciò i dati riportati da tali studi sembrano comunque confermare l’importanza di
un corretto approccio all’utilizzo della sEMG nella valutazione della fatica, sia nella
metodica ( set up, tipo di elettrodo, task motorio richiesto, ecc..) sia nella interpretazione
delle variabili prese in esame nell’analisi EMG (meglio mioelettriche?)

3
Alcuni autori sembrano concordi che la fatica muscolare influenza la mobilità scapolo
toracica e scapolo omerale, e quindi l’accuratezza la precisione la stabilità dell’intero arto
superiore, ma i meccanismi su come questo avvenga sono tuttora sconosciuti.
4
1. Introduzione
Il fenomeno di fatica è un esperienza comune nella pratica clinica quotidiana,
particolarmente complesso perché varia al variare dell’esercizio effettuato e decisamente
controverso a causa delle diverse interpretazioni e definizioni che si trovano in letteratura.
Il termine fatica muscolare è usato per indicare una diminuzione transitoria nella capacità di
compiere azioni fisiche. I seguenti estratti caratterizzano la varietà di effetti attribuiti alla
fatica muscolare (1):
Un’intensa attività muscolare causa un declino nella performance,
conosciuto come fatica (2)
Eseguire un compito motorio per lunghi periodi induce fatica muscolare, che
è generalmente definita come un declino nella capacità della persona di generare
forza (1)
La fatica si ritiene riflessa nel segnale EMG come un aumento della sua
ampiezza e una diminuzione delle sue caratteristiche frequenze spettrali (9)
La fatica muscolare, come risulta, può riferirsi ad un deficit motorio, può descrivere la
graduale diminuzione nella capacità di generare forza del muscolo o la fine di un’attività
sostenuta, e può essere misurata come una riduzione della forza muscolare, un
cambiamento nella attività EMG o come un esaurimento della funzione contrattile.
Questo ampio uso del termine è problematico perché la fatica in questo contesto può
comprendere alcuni fenomeni che sono anche conseguenza di differenti meccanismi
fisiologici. Per superare questo limite, alcuni autori hanno cercato di spiegare in maniera più
precisa tale fenomeno, definendo la fatica muscolare come “riduzione esercizio-indotta
nella capacità del muscolo di generare forza e potenza sia che il compito affaticante possa
essere sostenuto come no (1”).
Classicamente, considerato che il complesso sistemico interessato è piuttosto ampio e
comprende la singola fibra muscolare, la giunzione neuromuscolare e le singole unità
motorie, centri superiori quali corteccia, cervelletto, nuclei della base,ecc.. ma anche
circuiti a feedback dei riflessi spinali, si tende a suddividere il fenomeno in fatica periferica e
5
fatica centrale attribuendo alla prima cause prevalentemente metaboliche ed alla seconda
invece motivazioni essenzialmente di tipo neurale (32).
La fatica centrale è caratterizzata da una graduale diminuzione nella drive volontaria dal
sistema nervoso centrale dovuta a molteplici fattori che includono un output sovra spinale
sub ottimale, riflessi inibitori all’interno del muscolo, inibizione ricorrente, povero input
sensoriale.
La fatica periferica, invece,è ricondotta ad altri fattori quali: alterata trasmissione del
potenziale d’azione attraverso la giunzione neuromuscolare, variazioni metaboliche a livello
di membrane (inibizione della glicolisi), problematiche legate alle caratteristiche di
interazione tra miosina ed actina o per alterato rilascio di calcio a livello
sarcoplasmatico,ecc., ossia tutti quei fenomeni che agiscono a livello
periferico/microscopico (4).
Nonostante questa suddivisione, il quadro generale non è sempre cosi perfettamente
distinguibile, ed i vari fattori scatenanti spesso si sovrappongono rendendo la situazione
difficile da interpretare.
Uno degli strumenti che negli ultimi anni sta compiendo notevoli progressi nella analisi
della fatica muscolare è l’elettromiografia di superficie.
Il suo impiego sta avendo una notevole diffusione sia per le caratteristiche di non invasività,
sia per le potenzialità offerte dalle moderne tecniche di analisi numerica del segnale
elettromiografico che possono fornire utili informazioni quantitative sulle condizioni di
attività del distretto muscolare esaminato.
L’EMG di superficie misura l’attività elettrica muscolare, tramite elettrodi posti sulla cute,
dandoci informazioni circa le modalità con cui i muscoli lavorano durante un compito
motorio specifico (37,38)
Durante una contrazione (sia volontaria che indotta elettricamente) da un punto di vista
elettrico si registrano alterazioni di ampiezza, forma e velocità di propagazione del
potenziale d’azione, che sono alla base delle variazioni nel tempo di alcuni parametri di
ampiezza e frequenza del segnale mioelettrico. A tali variazioni si fa comunemente
riferimento con il termine di manifestazioni mioelettriche di fatica muscolare localizzata.
Variabili di ampiezza di uso corrente sono il valore rettificato medio (ARV) e il valore
efficace (RMS), mentre variabili di frequenza sono la frequenza media (MNF) e la frequenza
6
mediana (MDF); un’altra variabile di notevole interesse è la velocità di conduzione (CV)
delle fibre muscolari (37,40)
La velocità di conduzione è la più importante tra le grandezze fisiche che determinano sia le
variabili spettrali sia le variabili di ampiezza : con il sopraggiungere della fatica essa
diminuisce, ciò implica una diminuzione della MDF e della MNF e un aumento di ARV e
RMS. Tuttavia numerosi altri fattori, oltre alla CV, influenzano le variabili di ampiezza e
frequenza. Tra questi la forma del potenziale d’azione, la dispersione statistica di CV, la
disperzione delle giunzioni neuromuscolari nella zona di innervazione, la profondità delle
fibre sotto la cute, ecc (37,38,39).
Pertanto l’obiettivo della tesi è stato quello di selezionare gli articoli scientifici nei quali
l’utilizzo dell’EMG è considerato come un utile strumento di valutazione della fatica
muscolare a livello del cingolo scapolare cercando di individuare quali possano essere
considerate le modalità di applicazione (1 o più elettrodi, tipo di elettrodo, posizionamento,
ecc..) più affidabili. Nel dettaglio abbiamo cercato di capire quali siano i task motori che
sviluppano fatica (misurabile con sEMG) nei muscoli scapolari e in particolare quanto
questo possa influenzare il controllo del movimento del complesso arto superiore.
7
2. Materiali e metodi
Criteri di selezione degli articoli
Per questo lavoro è stata effettuata una revisione della letteratura attraverso il data base
MEDLINE, ricercando gli articoli pubblicati tra il 01/01/2001 e il 01/01/2011 in lingua
inglese su soggetti sani adulti (di età >18 ann).
Sono stati revisionati esclusivamente gli articoli disponibili tramite la Biblioteca Informatica
e sono state utilizzate le seguenti stringhe di ricerca:
1) “EMG” AND “fatigue”
2) “EMG” and “Fatigue” AND “Shoulder” AND “Healthy Subjects”
3) “EMG” AND “Fatigue” AND “Upper Trapezius”
4) “EMG” AND “Fatigue” AND “Kinematics”
5) “EMG” AND “Scapula” AND “Fatigue”
La prima selezione degli articoli è stata eseguita sulla base della lettura del titolo e
dell’abstract. In seguito è stata effettuata una valutazione più approfondita attraverso la
lettura del testo integrale.
Sono stati esclusi dalla ricerca articoli di cui non fosse reperibile il full text (biblioteca
universitaria) e quelli non pertinenti con l’obiettivo della ricerca.
8
3. Risultati
1) Essendo la prima stringa comprensiva di articoli non riguardanti solamente il cingolo
scapolare, sono stati ottenuti 1416 articoli. Di questi abbiamo selezionato esclusivamente le
Review (50), tra queste solamente 4 rispondevano ai nostri criteri di ricerca.
2) Attraverso questa ricerca sono emersi 25 articoli dei quali 4 rispondevano ai nostri criteri
di ricerca. Review 0
3)attraverso la terza stringa abbiamo trovato 46 articoli, ne abbiamo selezionati selezionati
6. Una sola review è stata trovata ma non risponde ai criteri utilizzati.
4) mettendo come parole chiave “EMG” AND “Fatigue” AND “Kinematics sono stati trovati
54 articoli, selezionati 3. Review 1 selezionata 0
5) l’ultima ricerca ha evidenziato 10 articoli di cui sono stati selezionati 3. Review 1 ma non
selezionata
Pertanto gli articoli effettivamente utilizzati per la revisione sono in totale 20.
9
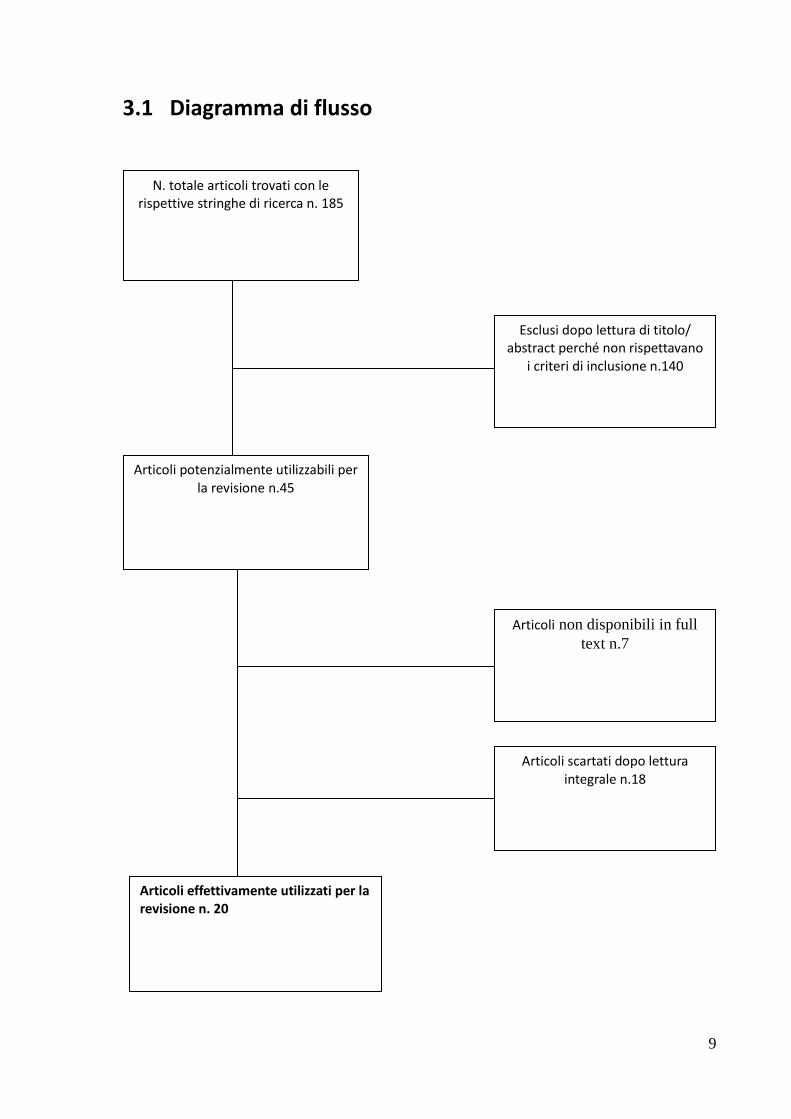
3.1 Diagramma di flusso
N. totale articoli trovati con le rispettive stringhe di ricerca n. 185
Esclusi dopo lettura di titolo/ abstract perché non rispettavano
i criteri di inclusione n.140
Articoli potenzialmente utilizzabili per la revisione n.45
Articoli non disponibili in full
text n.7
Articoli scartati dopo lettura integrale n.18
Articoli effettivamente utilizzati per la revisione n. 20
3.2 Tabelle sinottiche
Titolo, autore
e anno Campione Fatiguing task EMG analysis EMG results Motor control
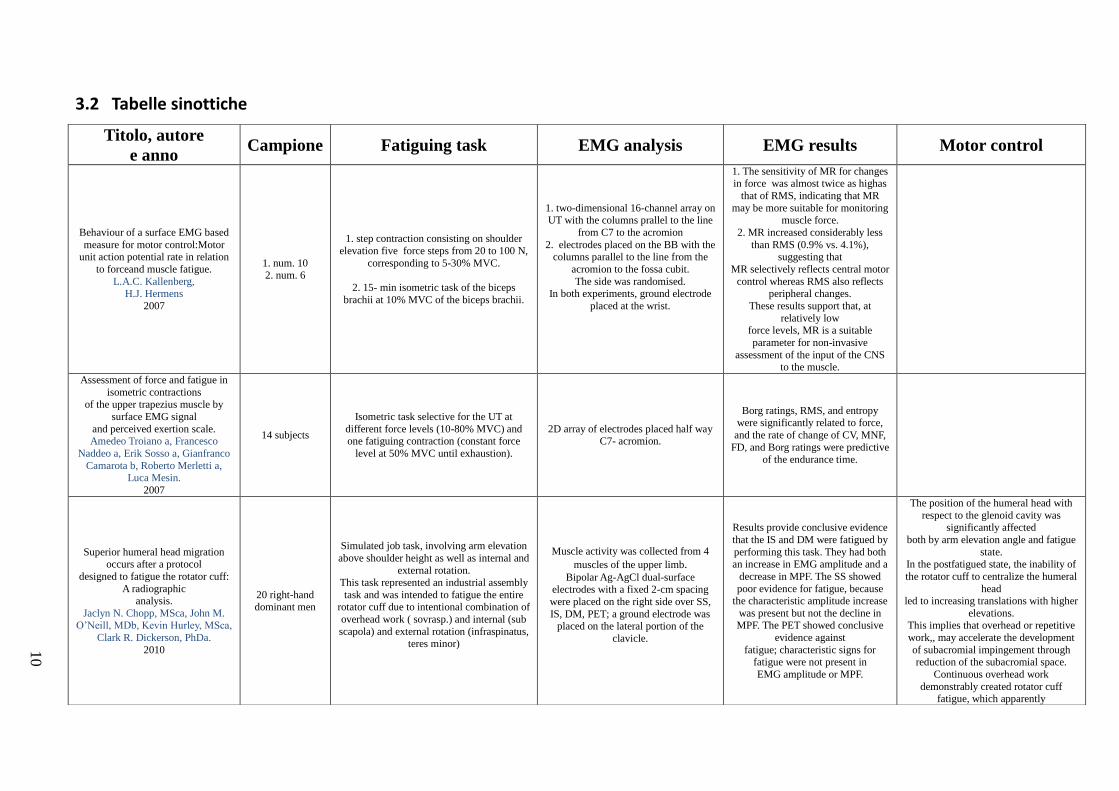
Behaviour of a surface EMG based
measure for motor control:Motor unit action potential rate in relation
to forceand muscle fatigue.
L.A.C. Kallenberg, H.J. Hermens
2007
1. num. 10 2. num. 6
1. step contraction consisting on shoulder
elevation five force steps from 20 to 100 N,
corresponding to 5-30% MVC.
2. 15- min isometric task of the biceps
brachii at 10% MVC of the biceps brachii.
1. two-dimensional 16-channel array on UT with the columns prallel to the line
from C7 to the acromion
2. electrodes placed on the BB with the columns parallel to the line from the
acromion to the fossa cubit.
The side was randomised. In both experiments, ground electrode
placed at the wrist.
1. The sensitivity of MR for changes in force was almost twice as highas
that of RMS, indicating that MR
may be more suitable for monitoring muscle force.
2. MR increased considerably less
than RMS (0.9% vs. 4.1%), suggesting that
MR selectively reflects central motor
control whereas RMS also reflects peripheral changes.
These results support that, at
relatively low force levels, MR is a suitable
parameter for non-invasive
assessment of the input of the CNS to the muscle.
Assessment of force and fatigue in
isometric contractions
of the upper trapezius muscle by
surface EMG signal
and perceived exertion scale. Amedeo Troiano a, Francesco
Naddeo a, Erik Sosso a, Gianfranco
Camarota b, Roberto Merletti a, Luca Mesin.
2007
14 subjects
Isometric task selective for the UT at
different force levels (10-80% MVC) and one fatiguing contraction (constant force
level at 50% MVC until exhaustion).
2D array of electrodes placed half way C7- acromion.
Borg ratings, RMS, and entropy were significantly related to force,
and the rate of change of CV, MNF,
FD, and Borg ratings were predictive of the endurance time.
Superior humeral head migration
occurs after a protocol
designed to fatigue the rotator cuff:
A radiographic analysis.
Jaclyn N. Chopp, MSca, John M. O’Neill, MDb, Kevin Hurley, MSca,
Clark R. Dickerson, PhDa.
2010
20 right-hand dominant men
Simulated job task, involving arm elevation
above shoulder height as well as internal and
external rotation. This task represented an industrial assembly
task and was intended to fatigue the entire rotator cuff due to intentional combination of
overhead work ( sovrasp.) and internal (sub
scapola) and external rotation (infraspinatus, teres minor)
Muscle activity was collected from 4
muscles of the upper limb. Bipolar Ag-AgCl dual-surface
electrodes with a fixed 2-cm spacing
were placed on the right side over SS,
IS, DM, PET; a ground electrode was placed on the lateral portion of the
clavicle.
Results provide conclusive evidence
that the IS and DM were fatigued by
performing this task. They had both
an increase in EMG amplitude and a
decrease in MPF. The SS showed
poor evidence for fatigue, because the characteristic amplitude increase
was present but not the decline in MPF. The PET showed conclusive
evidence against
fatigue; characteristic signs for fatigue were not present in
EMG amplitude or MPF.
The position of the humeral head with
respect to the glenoid cavity was significantly affected
both by arm elevation angle and fatigue
state.
In the postfatigued state, the inability of
the rotator cuff to centralize the humeral
head led to increasing translations with higher
elevations. This implies that overhead or repetitive
work,, may accelerate the development
of subacromial impingement through reduction of the subacromial space.
Continuous overhead work
demonstrably created rotator cuff fatigue, which apparently
10
inhibited the ability of the shoulder musculature to resist upward humeral
translation.
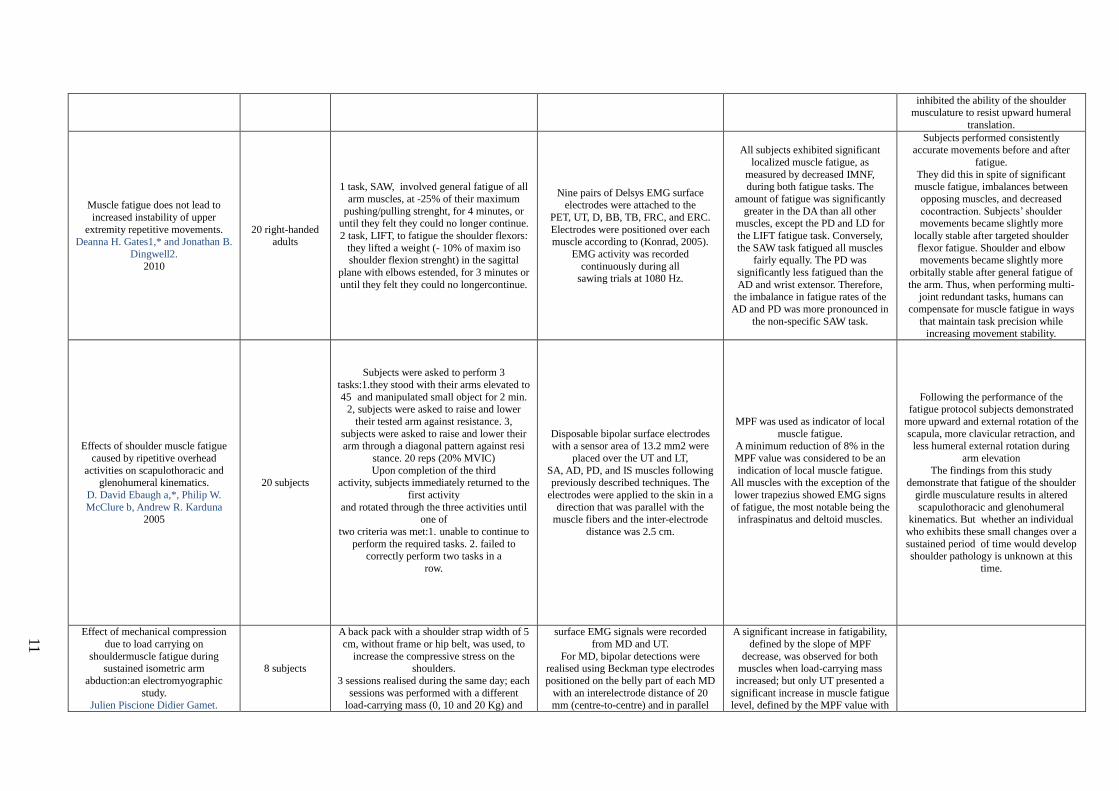
Muscle fatigue does not lead to
increased instability of upper
extremity repetitive movements.
Deanna H. Gates1,* and Jonathan B.
Dingwell2.
2010
20 right-handed
adults
1 task, SAW, involved general fatigue of all
arm muscles, at -25% of their maximum
pushing/pulling strenght, for 4 minutes, or until they felt they could no longer continue.
2 task, LIFT, to fatigue the shoulder flexors:
they lifted a weight (- 10% of maxim iso shoulder flexion strenght) in the sagittal
plane with elbows estended, for 3 minutes or
until they felt they could no longercontinue.
Nine pairs of Delsys EMG surface electrodes were attached to the
PET, UT, D, BB, TB, FRC, and ERC.
Electrodes were positioned over each
muscle according to (Konrad, 2005).
EMG activity was recorded
continuously during all sawing trials at 1080 Hz.
All subjects exhibited significant
localized muscle fatigue, as
measured by decreased IMNF, during both fatigue tasks. The
amount of fatigue was significantly
greater in the DA than all other muscles, except the PD and LD for
the LIFT fatigue task. Conversely,
the SAW task fatigued all muscles fairly equally. The PD was
significantly less fatigued than the
AD and wrist extensor. Therefore, the imbalance in fatigue rates of the
AD and PD was more pronounced in
the non-specific SAW task.
Subjects performed consistently accurate movements before and after
fatigue.
They did this in spite of significant muscle fatigue, imbalances between
opposing muscles, and decreased
cocontraction. Subjects’ shoulder movements became slightly more
locally stable after targeted shoulder
flexor fatigue. Shoulder and elbow movements became slightly more
orbitally stable after general fatigue of
the arm. Thus, when performing multi-joint redundant tasks, humans can
compensate for muscle fatigue in ways
that maintain task precision while increasing movement stability.
Effects of shoulder muscle fatigue
caused by ripetitive overhead
activities on scapulothoracic and glenohumeral kinematics.
D. David Ebaugh a,*, Philip W.
McClure b, Andrew R. Karduna 2005
20 subjects
Subjects were asked to perform 3
tasks:1.they stood with their arms elevated to
45 and manipulated small object for 2 min. 2, subjects were asked to raise and lower
their tested arm against resistance. 3,
subjects were asked to raise and lower their arm through a diagonal pattern against resi
stance. 20 reps (20% MVIC)
Upon completion of the third activity, subjects immediately returned to the
first activity
and rotated through the three activities until one of
two criteria was met:1. unable to continue to
perform the required tasks. 2. failed to
correctly perform two tasks in a
row.
Disposable bipolar surface electrodes with a sensor area of 13.2 mm2 were
placed over the UT and LT,
SA, AD, PD, and IS muscles following previously described techniques. The
electrodes were applied to the skin in a
direction that was parallel with the muscle fibers and the inter-electrode
distance was 2.5 cm.
MPF was used as indicator of local
muscle fatigue. A minimum reduction of 8% in the
MPF value was considered to be an
indication of local muscle fatigue. All muscles with the exception of the
lower trapezius showed EMG signs
of fatigue, the most notable being the infraspinatus and deltoid muscles.
Following the performance of the fatigue protocol subjects demonstrated
more upward and external rotation of the
scapula, more clavicular retraction, and less humeral external rotation during
arm elevation
The findings from this study demonstrate that fatigue of the shoulder
girdle musculature results in altered
scapulothoracic and glenohumeral kinematics. But whether an individual
who exhibits these small changes over a
sustained period of time would develop
shoulder pathology is unknown at this
time.
Effect of mechanical compression
due to load carrying on
shouldermuscle fatigue during sustained isometric arm
abduction:an electromyographic
study. Julien Piscione Didier Gamet.
8 subjects
A back pack with a shoulder strap width of 5
cm, without frame or hip belt, was used, to
increase the compressive stress on the shoulders.
3 sessions realised during the same day; each
sessions was performed with a different load-carrying mass (0, 10 and 20 Kg) and
surface EMG signals were recorded
from MD and UT.
For MD, bipolar detections were realised using Beckman type electrodes
positioned on the belly part of each MD
with an interelectrode distance of 20 mm (centre-to-centre) and in parallel
A significant increase in fatigability,
defined by the slope of MPF
decrease, was observed for both muscles when load-carrying mass
increased; but only UT presented a
significant increase in muscle fatigue level, defined by the MPF value with
11
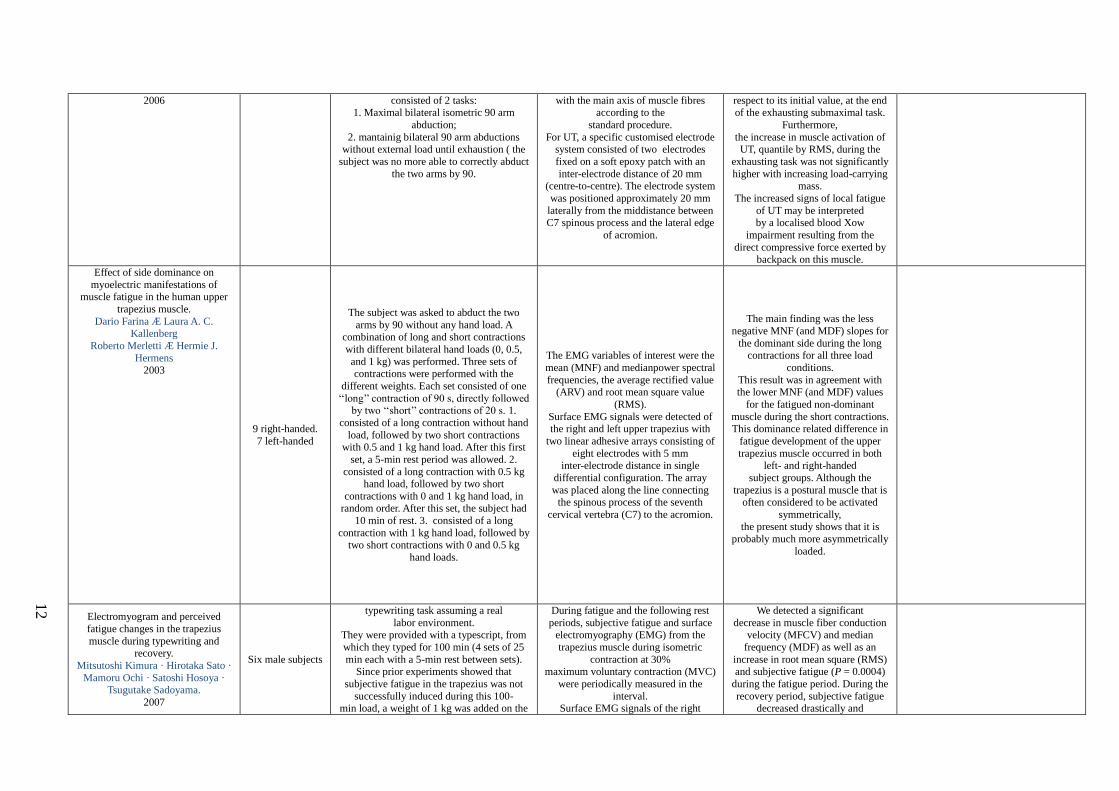
2006 consisted of 2 tasks: 1. Maximal bilateral isometric 90 arm
abduction;
2. mantainig bilateral 90 arm abductions without external load until exhaustion ( the
subject was no more able to correctly abduct
the two arms by 90.
with the main axis of muscle fibres according to the
standard procedure.
For UT, a specific customised electrode system consisted of two electrodes
fixed on a soft epoxy patch with an
inter-electrode distance of 20 mm (centre-to-centre). The electrode system
was positioned approximately 20 mm
laterally from the middistance between C7 spinous process and the lateral edge
of acromion.
respect to its initial value, at the end of the exhausting submaximal task.
Furthermore,
the increase in muscle activation of UT, quantile by RMS, during the
exhausting task was not significantly
higher with increasing load-carrying mass.
The increased signs of local fatigue
of UT may be interpreted by a localised blood Xow
impairment resulting from the
direct compressive force exerted by backpack on this muscle.
Effect of side dominance on
myoelectric manifestations of muscle fatigue in the human upper
trapezius muscle.
Dario Farina Æ Laura A. C. Kallenberg
Roberto Merletti Æ Hermie J.
Hermens 2003
9 right-handed.
7 left-handed
The subject was asked to abduct the two
arms by 90 without any hand load. A combination of long and short contractions
with different bilateral hand loads (0, 0.5,
and 1 kg) was performed. Three sets of contractions were performed with the
different weights. Each set consisted of one
‘‘long’’ contraction of 90 s, directly followed by two ‘‘short’’ contractions of 20 s. 1.
consisted of a long contraction without hand
load, followed by two short contractions with 0.5 and 1 kg hand load. After this first
set, a 5-min rest period was allowed. 2.
consisted of a long contraction with 0.5 kg hand load, followed by two short
contractions with 0 and 1 kg hand load, in random order. After this set, the subject had
10 min of rest. 3. consisted of a long
contraction with 1 kg hand load, followed by two short contractions with 0 and 0.5 kg
hand loads.
The EMG variables of interest were the
mean (MNF) and medianpower spectral
frequencies, the average rectified value (ARV) and root mean square value
(RMS).
Surface EMG signals were detected of the right and left upper trapezius with
two linear adhesive arrays consisting of
eight electrodes with 5 mm inter-electrode distance in single
differential configuration. The array
was placed along the line connecting the spinous process of the seventh
cervical vertebra (C7) to the acromion.
The main finding was the less
negative MNF (and MDF) slopes for
the dominant side during the long contractions for all three load
conditions.
This result was in agreement with the lower MNF (and MDF) values
for the fatigued non-dominant
muscle during the short contractions. This dominance related difference in
fatigue development of the upper
trapezius muscle occurred in both left- and right-handed
subject groups. Although the
trapezius is a postural muscle that is often considered to be activated
symmetrically, the present study shows that it is
probably much more asymmetrically
loaded.
Electromyogram and perceived
fatigue changes in the trapezius
muscle during typewriting and recovery.
Mitsutoshi Kimura · Hirotaka Sato ·
Mamoru Ochi · Satoshi Hosoya · Tsugutake Sadoyama.
2007
Six male subjects
typewriting task assuming a real
labor environment. They were provided with a typescript, from
which they typed for 100 min (4 sets of 25
min each with a 5-min rest between sets). Since prior experiments showed that
subjective fatigue in the trapezius was not
successfully induced during this 100- min load, a weight of 1 kg was added on the
During fatigue and the following rest
periods, subjective fatigue and surface electromyography (EMG) from the
trapezius muscle during isometric
contraction at 30% maximum voluntary contraction (MVC)
were periodically measured in the
interval. Surface EMG signals of the right
We detected a significant
decrease in muscle fiber conduction velocity (MFCV) and median
frequency (MDF) as well as an
increase in root mean square (RMS) and subjective fatigue (P = 0.0004)
during the fatigue period. During the
recovery period, subjective fatigue decreased drastically and
12

wrist. The seat height was adjusted for each subject
before the experiment to maintain the upper
arm in an upright position and the lower arm horizontal.
Measurements during the task were
performed at 0 (before task), 30, 60, 90 and 120 min (immediately after the end of the
last 25-min set).The measurements consisted
of subjective evaluation of muscle fatigue, EMG (MFCV, MDF and RMS), surface and
core tissue temperatures, and muscle
hardness of the trapezius.
trapezius were detected with a multiple active electrode composed of four
parallel silver wires .
The electrode was placed slightly inside the midpoint
between the 7th cervical vertebrae (C7)
and the acromion, avoiding the innervation zone.
A ground electrode, a disk of 12 mm in
diameter, was placed on C7.
significantly, however, the EMG parameters did not recover
completely. Thus, physiological
muscle fatigue in the trapezius developed in accordance with
subjective muscle fatigue during
typewriting. On the other hand, differences between the
physiological and subjective
parameters were found during recovery.
Electromyographical manifestations
of muscle fatigue during different levels of simulated light manual
assembly work.
T. Bosch a,b,c,*, M.P. de Looze a,b,c, I. Kingma b, B. Visser b,c,
J.H. van Diee¨n b,c
2008
Ten healthy
subjects
The subjects had to perform a 3-h simulated
assembly work task at two intensity levels. The task was based on a realistic assembly
task.
The task consisted of constructing and taking apart a small tower of eight blocks.
Subjects constructed and broke down a
tower in front of them with a cycle time of 30 s.
Both hands were used in alternating order
and one block was picked-up at a time. After completing a tower, subjects put it in a box
in front of them.
In the first condition (low condition), the table height was individually adjusted so the
elbow was flexed slightly more than 90_ and
the palms of the hands were just above the table. In the second condition (high
condition) table height was increased by 10
cm, the box height of the parts was increased by 15 cm and the front boxes were placed 35
cm further away. In both conditions, subjects
were not allowed to lean on the table during the tasks.
EMG was recorded using four pairs of bipolar electrodes over the left and right
trapezius muscles during the task itself
and during isometric test contractions. EMG signals were recorded from the
descending part of the upper trapezius
muscle by using bipolar Ag/AgCl surface electrodes. Four pairs of bipolar
electrodes were placed on both the right
and left upper trapezius muscle. The reference electrode was placed over
the C7 spinous process.
Both recordings (during task and
test) showed a significant decrease in the mean power frequency (MPF), at
both intensity levels while the
amplitude remained constant. A regression analysis showed
significantly different temporal
patterns for the MPF decrease for the two intensities. No differences in
manifestations of muscle fatigue
development were found between different
parts of the muscle. These results
indicate that in a highly repetitive low-intensity task,
electromyographical manifestations
of muscle fatigue can be observed from signals recorded in the task
itself. Furthermore, the rate of
development of fatigue manifestations was different
between the two assembly tasks.
This fatigue development appeared to be homogenous across the muscle.
EMG amplitude distribution changes over the upper trapezius
muscle are similar in sustained and
ramp Contractions.
A. Holtermann and K. Roeleveld.
2005
Fourteen subjects
The procedure involved the generation of
two separate contractions. In the first contraction, the subject generated three
smooth isometric ramp contractions from
0% to 90% of MVC. The first properly performer contraction was used for further
analyses. The subjects were instructed to
smoothly increase the force with 9% MVC per second. Each contraction lasted 10 s with
10-s recovery period. After a 3-min recovery
period, the subjects performed a sustained isometric contraction at 25% of MVC lasting
A multi-channel system with a 130-
channel grid was used to acquire multi-channel surface electromyographical
(MCSEMG) data. The multi-electrode
array consisted of 13 · 10 gold covered pin electrodes placed in a holder of
7 · 5 cm. The electrode diameters were
1.5 mm with an inter-electrode distance of 5 mm.
The centre of the MCSEMG grid was
placed on the right trapezius muscle in the middle of the line between the
The main findings were: (1) the
EMG amplitude was spatially non-uniform distributed over the skin
above the upper trapezius muscle at
all investigated time periods, (2) the correlation coefficient between EMG
amplitude distributions at different
time periods varied with time and force level, showing that the non-
uniform amplitude distribution
changed both with contraction level and time and (3) the amplitude
these results indicate that (i) the
activation of the upper trapezius muscle is inhomogeneously distributed in both
sustained and ramp isometric
contractions, (ii) this inhomogeneous activation changes both with contraction
level and time, mainly because of motor
unit recruitment and (iii) global motor unit recruitment to compensate for
muscle fatigue during a sustained
contraction and to regulate force increase during a ramp contraction is
13
3 min. processus spinosus of the seventh cervical (C7) vertebra and the lateral
edge of the acromion.
distribution of the muscle late in the sustained contraction was more
similar to the amplitude distribution
observed at higher force levels.
controlled in similar manners.
EMG analysis of shoulder muscle
fatigue during resisted isometric shoulder elevation.
Stephen Minning *, Colin A. Eliot,
Tim L. Uhl, Terry R. Malone. 2006
Sixteen
asymptomatic subjects
The subjects held a weight equivalent to
60% of his/her Maximum Voluntary
Isometric Contraction (MVIC) while elevating in the scapular plane.
Shoulder muscle fatigue was measured by
having the subject perform an isometric contraction at 60% of their maximal
voluntary isometric contraction force
(MVIC). Sixty percent was chosen as research has
shown that above this level of force output
there is a greater recruitment of Type II muscle fibers as compared to lower levels of
force
Output. The subject was considered fatigued and the
trial over when the subject was no longer
able to maintain his or her arm at the predetermined test position or
if 30 s had elapsed with the subject
maintaining the position. At the completion of the first trial, the subject was allowed a 5-
min rest, after which a second trial was
performed in the same manner. The trial was terminated at 30 s to provide more consistent
data for the statistical analysis.
Surface electrodes were applied to
collect electromyographic activity from
the UT, MD, SA, and LT muscles while the arm was held at 90_ elevation. Data
collection ceased when the subject was
no longer able to maintain 90_ of elevation. The subject then rested and a
second trial performed. One week later,
the two-trial procedure was repente. Electrode placement locations were
selected based on previous published
studies involving EMG data collection from the muscles of interest.
Bipolar silver–silver chloride surface
electrodes were used with a constant interelectrode distance of 2.0 cm.
Electrodes for the UT were placed 2 cm
lateral to the midpoint between the spinous process of the seventh cervical
vertebra and the posterior tip of the
acromion process along the line of the trapezius. The MD
electrodes were placed midway
between the deltoid tuberosità and the acromion process. The SA electrodes
were placed at the apex of the lateral
side of the thorax3 cm caudal to the inferior spine of the scapula, obliquely
upward and posterior. The electrodes
for the LT were placed obliquely upward and laterally along a
line between the intersection of the
spine of the scapula and with the vertebral border of the scapula and the
seventh thoracic spinous process. A ground
electrode was placed on the left
acromion process.
A significant interaction of trial · day
· muscle was found for the rate of
fatigue. Post hoc analysis revealed
that the rate of fatigue of the middle
deltoid was significantly greater than
the other muscles tested. The intraday reliability was good for all
muscles but interday
reliability was poor except for the middle deltoid.
The average median power
frequency shifts were most apparent in the middle deltoid and upper
trapezius muscles, with the serratus
anterior and lower trapezius exhibiting slightly lower changes.
All of the muscles
showed a decrease in median power frequency output indicating fatigue
with this task.
The results also revealed good intrasession reliability for all of the
muscles of interest and poor
intersession reliability for 3 of the 4 muscles tested, excluding the middle
deltoid. demonstrates intrasession
and intersession reliability for the muscles studied.
Shoulder muscle fatigue has been
associated with alterations in joint mechanics and possibly contributes to
shoulder dysfunction.
This study suggests that the middle deltoid appears to fatigue faster than the
other shoulder muscles tested at the
selected level of shoulder elevation. This should be considered in designing a
rehabilitation program to develop a
sequence that does not overly fatigue the middle deltoid.
Spatial distribution of active muscle fibre characteristics in the upper
trapezius muscle and its dependency
on contractionlevel and duration. Andreas Holtermann a,*, Christer
Gro¨nlund b,c, J. Stefan Karlsson
b,c, Karin Roeleveld. 2006
five male subjects
Subjects performing isometric shoulder elevation at different force levels. The five
subjects performed shoulder elevation using
a dynamometer.
Two-dimensional (2-D) multi-channel surface electromyography recordings
were used, with 13 · 10 electrodes
covering 6 · 4.5 cm of the skin’s surface. A previously developed method
was applied to detect individual
propagating motor unit action potentials and to estimate their corresponding
The main results were: (1) the general relationship between MFCV
and force generation was non-
systematic, with a positive relationship at the inferior part of the
muscle, (2) the spatial distribution of
MFCV at different force levels and fatigue was
14
muscle fibre conduction velocity (MFCV) and muscle fibre orientation
(MFO).
inhomogeneous and (3) the MFO (muscle fiber orientation) was
slightly different (6°) of the muscle
fibres with origin superior compared to inferior to the C7
vertebra.
Scapular muscle activation and co-activation following a fatigue task.
Kimberly Szucs Æ Anand
Navalgund Æ John D. Borstad.
2009
28 asyntomatic
subjects
Subjects performed a task to fatigue the serratus anterior.
each subject performed five repetitions of
maximum scapular plane elevation in standing at an estimated velocity of 90_ per
s.
Subjects then performed a task intended to fatigue the serratus anterior by placing their
feet on a 23-cm step and holding a pushup
plus position. The pushup plus position involves assuming the starting position for a
pushup and then adding maximum scapular
protraction bilaterally. Subjects held this position until they
voluntarily stopped due to fatigue.
Immediately following the task, subjects returned to standing and repeated the five
repetitions of scapular plane elevation. EMG
data were collected during both series of arm
elevation and during the fatigue task.
A Delsys Bagnoli 8-channel EMG
system collected raw surface EMG data from the SA, UT and LT muscles.
Surface electrodes were bipolar Ag–
AgCl parallel bar electrodes. The SA
electrode was placed on the lateral
midline of the thorax at approximately
the sixth rib, anterior to the latissimus dorsi. The UT electrode was placed
halfway along a line between the
acromioclavicular joint and the seventh cervical spinous process. The LT
electrode was placed just
medial and superior to an oblique line between the root of the spine of the
scapula and eighth thoracic spinous
process. All electrodes were aligned in parallel with the
muscle fibers and a disposable
reference electrode was positioned on the subject’s contralateral acromio
n.
All muscles demonstrated meaningful declines in the median
frequency of the electromyographic
signal during the task. Following the task, only the upper
trapezius had higher mean activation
levels (mean difference 10.79% MVIC), while the serratus
anterior/lower trapezius activation
ratio was altered (mean difference -0.3).
A task intended to fatigue the serratus
anterior resulted primarily in upper trapezius activation increases at the
shoulder. These increases may be fatigue
related, but could suggest that the upper trapezius is less susceptible to fatigue
and may attempt to compensate for
fatigue of other shoulder muscles. Supporting this possibility is the fact
that the upper trapezius activation
increases are at 60_, 90_ and 120_ of arm elevation, angles where the
gravitational force effects on the arm are
greatest and larger muscle force requirements are thus required. Serratus
anterior endurance training may be
beneficial for the prevention of shoulder pathology for those with increased
exposure to forceful overhead
contractions.
Scapula kinematic alterations
following a modified push-up plus task.
John D. Borstad *, Kimberly Szucs,
Anand Navalgund.
2009
Twenty-eight participants.
The experimental task consisted of five
repetitions of scapular plane arm elevation
at an estimated velocity of 90°/s and the fatigue consisted of an isometric hold of a
modified push-up plus position.
Delsys Bagnoli 8-EMG. One bipolar Ag–AgCl parallel bar
surface electrode with contact material
composed of 99.9% Ag and a detection area of 10 mm2 was used on each
muscle. A disposable reference
electrode was placed over the
participants contralateral acromion. The
serratus anterior electrode was placed
approximately 1 cm above the level of the inferior angle of the scapula,
anterior to latissimus dorsi on the lateral
thorax at the level of the fifth or sixth rib. The upper trapezius electrode was
placed at the midpoint of the line
between the acromioclavicular joint and the seventh cervical spinous process.
The lower trapezius electrode was
placed just medial and superior to a line between the root of the spine of the
The fatigue task resulted in decreased median power frequency
in all four muscles and significantly
increased Borg scores. An a priori decline of 8% was selected to signify
local muscle fatigue.
Three muscles, serratus anterior
(27.2%), infraspinatus (26.7%), and
lower trapezius (29.0%)
demonstrated mean percent declines greater than 20%, while the upper
trapezius declined 14.6%.
Infraspinatus percent MPF decline is greatest in males,
while lower trapezius shows the
largest decline in females and the smallest decline in males, while
lower trapezius shows the largest
decline in females and the smallest decline in males. Also
Scapula kinematics during arm elevation and lowering were altered following the
fatigue task. This scapular alterations
were more pronounced at higher elevations angles, where increased
serratus EMG activity is noted.
Scapula posterior tilting and internal
rotation were most impacted by muscle
fatigue, with decreased posterior tilting
and increased internal rotation after the task.
Other muscles demonstrated fatigue:
kinematics changes cannot be attribuited to serratus anterior fatigue alone.
Shoulder muscle fatigue contributes to
scapular kinematic alterations and is a plausible risk factor for subacromial
impingement syndrome.
Fig. 4 NB. Fatigue contribute to scapulothoracic
15

scapula and eighth thoracic spinous process. The infraspinatus electrode
was placed medial to the posterior
deltoid approximately 1 cm below the spine of the scapula.
notable are the considerably lower MPF declines for upper trapezius
and infraspinatus in women, with
upper trapezius failing to meet the 8% decline threshold for fatigue.
kinematic alterations that are similar to the alterations noted in participants with
subacromial impingement. Although
serratus anterior fatigue may preferentially influence scapular
posterior tilting because of its favorable
moment arm, fatigue of the UT, LT, IS be contributing to alterations in this
rotation. LT fatigue appears to influence
scapular internal rotation in the transverse plane during arm motion.
Periodic increases in force during sustained contraction reduce fatigue
and facilitate spatial redistribution of
trapezius muscle activity. Deborah Falla Æ Dario Farina
2007
9 volunteers.
This study compared fatigue and the spatial
distribution of upper trapezius electromyographic (EMG) amplitude during
a 6-min constant force shoulder elevation
task at 20% of the maximal voluntary contraction force
(MVC) (constant force) and during the same
task interrupted by brief (2 s) periodic increases in force to 25%
MVC every 30 s (variable force).
Surface EMG signals were detected
from the right upper trapezius with a semi-disposable adhesive grid of 64
electrodes.
The grid consists of 13 rows and 5 columns of electrodes (1 mm diameter,
8 mm interelectrode distance in both
directions) with one missing electrode at the upper right corner.
Before placement of the grid, the main
innervation zone location of the upper trapezius along the seventh cervical
vertebra (C7)-acromion line was
identified with an array of eight electrodes (silver bars, 5 mm long, 1
mm diameter,
5 mm interelectrode distance). The centroid (center of activity) of the
EMG root mean square map
was computed to assess changes over time in the spatial distribution of EMG
amplitude.
MVC force decreased by 9.0 ± 3.9% after the constant force task but was
unchanged following the variable
force contraction. The centroid of EMG
amplitude shifted in the cranial
direction across the duration of the variable forcecontraction but not
during the constant force
contraction. This study demonstrates that force
variations enhance the
change in the spatial distribution of upper trapezius EMG amplitude over
time and that this is associated with
less fatigue with respect to a constant force contraction. Differences in the
change in EMG amplitude
distribution may reflect different mechanisms involved in fatigue
development between the two tasks.
Myoelectric manifestations of
fatigue at low contraction levels in subjects with and without chronic
pain.
Laura A.C. Kallenberg a,*, Elke Schulte b, Catherine Disselhorst-
Klug b,
Hermie J. Hermens a,c 2006
10 healthy and 10
with cronic pain subjects.
1. 2 step contractions consisted of five force levels with a duration of 10 second each.
2. isometric sustained contraction of 15 min
at a force level of 40 N The step contractions were performed before
and after the sustained contraction to
examine possible changes in motor control.
EMG of the dominant upper trapezius
was recorded using a two-dimensional
16-channel electrode array. The array
consisted of four rows of gold-coated
pin electrodes with a diameter of 1.5
mm. The electrode array was placed with the
rows parallel to the line from C7 to the
acromion with the centre of the electrode array 2 cm distally from the
midpoint, in accordance with the
SENIAM Recommendations.
During the sustained contraction,
cases showed less increase in RMSG
than controls. FMEDG and CV
decreased in controls and stayed
constant (FMEDG) or slightly
increased in cases. Overall, cases showed a less pronounced
myoelectric response to the fatiguing
task than controls, which may be related to additional recruitment
of higher-threshold MUs. A possible
explanation might be that cases were already fatigued before the
experiment started.
16
17
4. Discussione
4.1 sEMG
Dall’analisi fatta attraverso le review e gli articoli selezionati emerge una certa confusione e
non omogeneità di interpretazione dei dati EMG, tanto che diversi autori concludono
importanti review affermando che “I dati EMG devono essere presi con cautela (37,43,1,2)”.
La registrazione del segnale EMG è, come è noto, influenzata da un numero elevato di
fattori: la forma e il tipo di elettrodi utilizzati, il loro posizionamento rispetto alla direzione
delle fibre, alla zona di innervazione e all’inserzione tendinea, l’impedenza di uscita della
sorgente e di ingresso dell’amplificatore, la temperatura del muscolo (37,38,39).
A fronte di tanta variabilità il numero di lavori rintracciabili in letteratura che offrano
risultati e conclusioni supportate da un corretto uso degli strumenti statistici è decisamente
ridotto.
Non sembra inoltre esserci accordo sul concetto di ripetibilità e sui protocolli da effettuare
per verificarne la consistenza.
Dall’analisi dei dati provenienti dagli articoli presi in esame risulta difficile una loro
comparazione in quanto sono differenti i metodi di valutazione della fatica muscolare.
In particolare la comparazione dei dati elettromiografici di superficie non è possibile in
quanto per ogni articolo, gli elettrodi, sono stati posizionati in punti differenti sulla pelle del
paziente; anche la frequenza di campionamento del segnale varia da articolo ad articolo; in
alcuni articoli la posizione degli elettrodi di superficie non viene descritta (14,15).
Considerando anche la difficoltà stessa di interpretazione del dato sEMG, è facile
comprendere come la comparazione di dati provenienti da diversi metodi di studio sia poco
attendibile.
Inoltre, le analisi sEMG avvengono quasi sempre per condizioni di lavoro muscolare
isometrico (8,10,15,16,18,25,35), con l’obiettivo di limitare il più possibile le interferenze possibili
col “vero” segnale elettromiografico, dato ad esempio dallo scorrimento della cute, o dello
scorrimento relativo del muscolo rispetto alla cute, inevitabile in una contrazione dinamica.
Questo è quindi un grosso limite della sEMG, che risulta non essere pienamente efficace ed
attendibile, per analizzare l’attività elettrica muscolare in condizione dinamica, come ad
18
esempio durante una contrazione eccentrica o concentrica, o durante un gesto lavorativo
(5,7,12,14,19).
Le grandezze fisiche utilizzate per caratterizzare il segnale mioelettrico legato alla fatica
sono spesso classificate come “nel dominio del tempo”, perché richiedono, per il loro
calcolo, solo il tracciato temporale del segnale e forniscono informazioni sulle sue
caratteristiche, e “nel dominio della frequenza” perché richiedono l’analisi spettrale e
caratterizzano lo spettro del segnale(37) Sebbene studiate a lungo, le ragioni alla base dei
cambiamenti di queste variabili sono ancora poco chiare (42).
Tra i vari parametri che generalmente vengono ricavati dalle registrazioni di segnali
elettromiografici di superficie (MNF, MDF, ARV, RMS,CV), la stima della velocità di
conduzione sembra essere il miglior candidato per il ruolo di valore normativo, almeno sui
muscoli con fibre parallele. Su questi muscoli l’errore percentuale inter-soggetto nella stima
del suo valore è infatti estremamente basso (2%-5%) e praticamente uniforme sia in
contrazioni stimolate elettricamente sia in contrazioni volontarie (37).
Numerosi articoli hanno messo in evidenza il fatto che la posizione degli elettrodi sia un
problema molto critico per la stima delle variabili del segnale e che le variazioni che se ne
ricavano possono variare moltissimo posizionando gli elettrodi in maniera diversa. L’utilizzo
delle schiere lineari di elettrodi sembra possa far superare i limiti dati dai metodi classici
usati per la stima dei valori globali CV e MNF, come il rilevamento bipolare, e in generale
può provvedere ad una più completa visione dell’attività muscolare per cui nn solo
l’informazione temporale ma anche quella spaziale diventa disponibile, soprattutto per
livelli di forza da bassi a moderati (9); essi infatti permettono di ricavare un valore mediato
sull’intero volume di prelievo, nascondendo le differenze tra i singoli contributi generati da
UM molto diverse. I valori globali possono rimanere inalterati anche se i singoli contributi
cambiano. Poiché, infatti, con l’utilizzo delle schiere lineari di elettrodi è più semplice
riconoscere i singoli potenziali d’azione (40), la stima delle variabili di interesse passa dal
valore globale (medio) alla stima del valore per ciascun contributo.
Le schiere offrono molti campi di applicazione interessanti. La possibilità di seguire il
potenziale nella sua propagazione permette ad esempio di valutare la qualità del prelievo e
l’influenza della posizione degli elettrodi sulle stime dei parametri di fatica o sulla stima del
grado di attività di un muscolo (38,39).
19
Andando ad analizzare nello specifico i 16 articoli selezionati si evidenzia che in 7 articoli gli
autori hanno utilizzato per l’analisi sEMG rilevamenti bipolari, mentre in 9 articoli sono stati
applicati sistemi di acquisizione a schiera per l’analisi elettromiografia. Anche in questo caso
esiste comunque una variabilità nell’acquisizione dei dati legata al numero di elettrodi (es:
griglie da 5 x 13 o 10 x 13) alla distanza inter-elettrodo (es: 1.5mm – 8mm) e alla superficie
cutanea coperta dalla griglia (es: 7 x 5 cm; 6 x 4.5 cm).
Nonostante la non omogeneità delle metodiche utilizzate, negli ultimi anni alcuni studi
hanno seguito le raccomandazioni SENIAM (Surface ElectroMyoGraphy for the Non-Invasive
Assessment of Muscles) nate da un programma di ricerca Europeo dall’obiettivo di
sviluppare protocolli condivisi al fine di favorire lo scambio di dati e di esperienze cliniche e
di stabilire linee di condotta Europee nella ricerca di base e applicata.
Per quanto l’analisi fatta circa la valutazione dell’attività muscolare è emerso che il trapezio
superiore è sicuramente il target della maggior parte degli studi ergonomici presenti in
letteratura, proprio per il ruolo chiave nei disordini muscolo-scheletrici nella regione
cervico-brachiale Tra gli altri distretti muscolari, risultano maggiormente analizzati il
Trapezio Inferiore, il Deltoide nelle sue 3 componenti, il Dentato Anteriore e il Bicipite
Brachiale in relazione della sua funzione a livello della spalla.
Risultano tuttavia più affidabili il TS, TI e il Deltoide, siti presenti nelle raccomandazioni
SENIAM.
4.2 controllo motorio
Le evidenze riguardanti il rapporto tra fatica muscolare a livello del cingolo scapolare e
alterazione del controllo motorio (ovvero legato ad un gesto finalizzato), sono ancora
scarse. Inoltre, a causa della complessità sia anatomica che funzionale, gli studi condotti a
livello del cingolo scapolare e dell’arto superiore in soggetti sani sono ancora tropo pochi.
La precisione del movimento è comunque da considerare critica per la salute di tutta la
regione della spalla anche se è ancora poco conosciuto il meccanismo per cui la fatica o lo
squilibrio tra muscoli/gruppi muscolari possa influenzare il controllo della stabilità del
movimento (5,36).
20
In primo luogo perché la dinamica nell’uso del braccio comporta la sincronizzazione e
l’attivazione di molteplici muscoli che permette molti gradi di libertà di movimento.
Non è sorprendente dunque, data la complessità della spalla, che ci siano numerose
patologie muscolo scheletriche che possano interessare l’intero arto superiore e che
svariati meccanismi vengano proposti alla base di queste problematiche. Tra questi si
notano alterazioni biomeccaniche (cinematiche), variazioni anatomiche, infortuni acuti o
cronici, patologie o debolezza muscolari, difetti posturali (36).
Con il termine alterazioni biomeccaniche si intendono movimenti o forze che deviano dalla
normalità di un gesto, e possono derivare da patterns di movimento ripetuti o da
alterazioni dell’attivazione neuromuscolare secondarie ad uno stimolo come la fatica o il
dolore (25, 34)
Le alterazioni neuromuscolari sono particolarmente problematiche perché possono
interferire con il normale timing di attivazione, fondamentale nel nostro caso, per il
movimento del cingolo scapolare e della spalla (36).
Dall’analisi della letteratura abbiamo individuato alcuni articoli che hanno messo in
relazione la fatica muscolare a livello del cingolo scapolare, con alterazioni cinematiche e di
stabilità dell’arto superiore (5,7,12,16,35,36) ed in particolare della scapola.
Quali siano i task motori da utilizzare, quali muscoli è possibile affaticare maggiormente con
un determinato task e che interpretazione dare ai vari risultati EMG e cinematici è tuttora
di difficile analisi.
Mc Quade (41) nel suo studio, 25 partecipanti, ha riscontrato alcuni cambiamenti nel ritmo
scapolo-omerale, soprattutto nell’upward rotation scapolare in diversi angoli di elevazione.
Utilizzando ripetute elevazioni contro resistenza del braccio a 150° ha riportato alterazioni
cinematiche scapolo-omerali dopo le varie ripetizioni.
I partecipanti allo studio si affaticavano dopo circa 90-120 secondi in media e dimostravano
una diminuzione di circa il 20% dell’MPF per il trapezio superiore, dentato anteriore,
deltoide medio, mentre una percentuale di diminuzione più bassa si evidenziava al trapezio
inferiore. Questi dati differiscono da quelli riscontrati nello studio di Borstad (35) dove
nessun cambiamento nella upward rotation è stato riscontrato. Una possibile spiegazione
sta probabilmente nella differente richiesta che viene fatta al paziente, dinamica nello
studio di Mc Quade con possibili strategie di movimento compensatorie che differiscono da
quelle create da un compito isometrico dello studio di Bortsad.
21
Ebaugh et al. (12) hanno analizzato gli effetti della fatica muscolare del cingolo scapolare
sulla cinematica tridimensionale scapolo toracica e gleno-omerale. I muscoli analizzati sono
stati il trapezio superiore, il dentato anteriore, il deltoide ant. e post. e l’ infraspinato. I 20
partecipanti hanno eseguito un protocollo dinamico composto da tre task motori, e i
risultati che emergono da questo studio dimostrano che la fatica della muscolatura
scapolare porta ad alterazioni biomeccaniche: in particolare si riscontrò un aumento della
upward ed external rotation ad angoli di elevazione più alti, e un diminuito downward
rotation ad angoli di elevazione più bassi.
L’autore riporta un declino della MPF maggiore dell’8% di tutti i muscoli, tranne che per il
trapezio inferiore. Contrariamente allo studio di Ebaugh, i partecipanti a quello di Borstad
dimostrano un aumento nella rotazione interna scapolare, e una diminuzione maggiore del
29% nell’analisi elettromiografia del trapezio inferiore. Questo suggerisce un ruolo chiave
del trapezio inferiore nel mantenimento della stabilità della scapola nel piano trasversale
durante l’elevazione del braccio.
Le alterazioni cinematiche riscontrate nel lavoro di Borstad divergono quindi sia dai risultati
di Mc Quade che da quelli di Ebaugh.
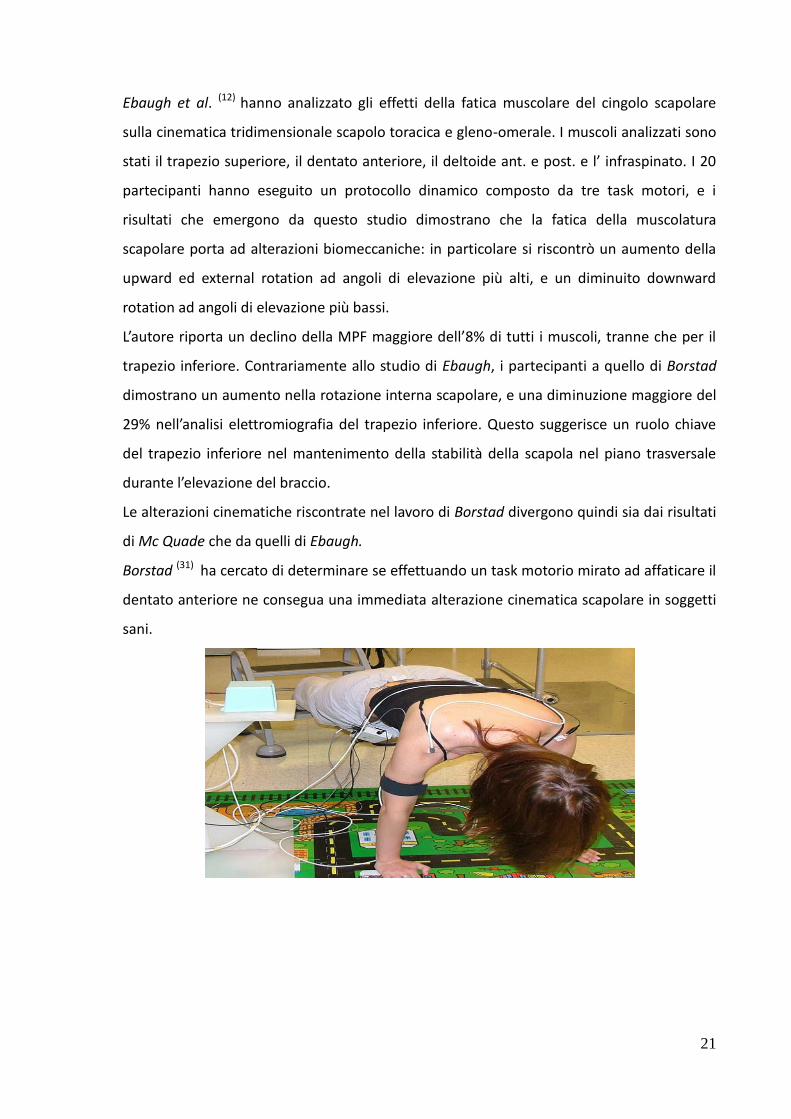
Borstad (31) ha cercato di determinare se effettuando un task motorio mirato ad affaticare il
dentato anteriore ne consegua una immediata alterazione cinematica scapolare in soggetti
sani.
22
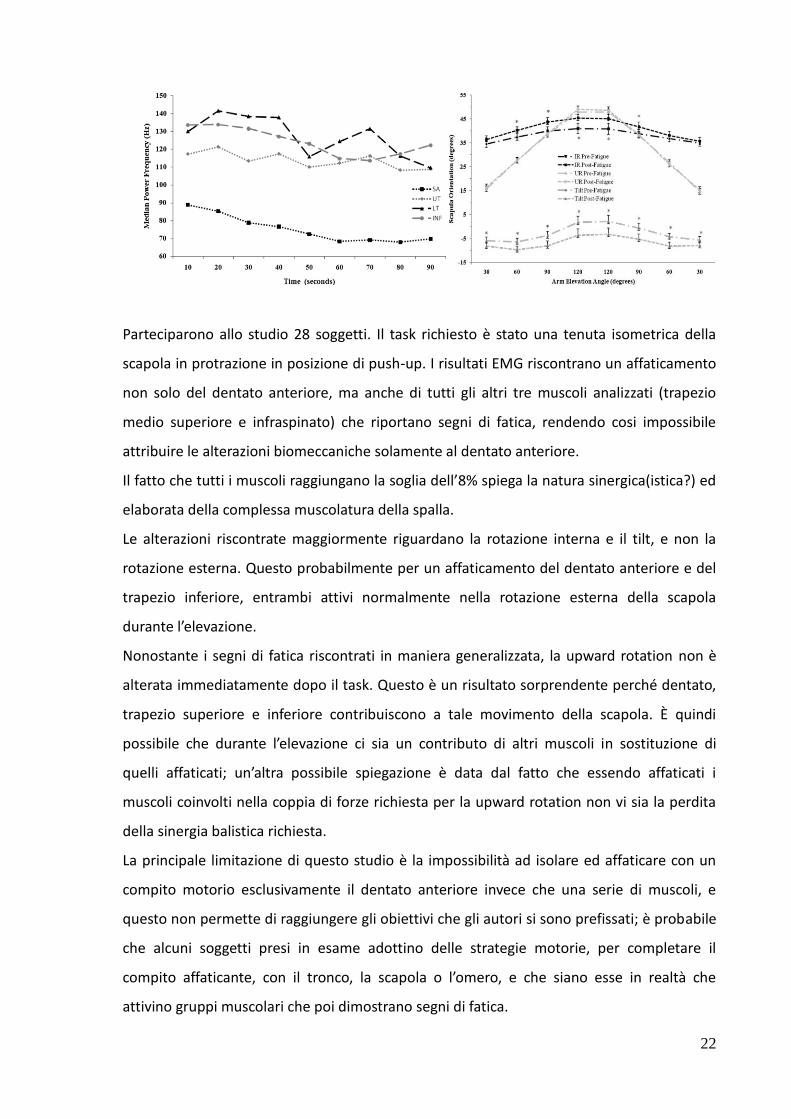
Parteciparono allo studio 28 soggetti. Il task richiesto è stato una tenuta isometrica della
scapola in protrazione in posizione di push-up. I risultati EMG riscontrano un affaticamento
non solo del dentato anteriore, ma anche di tutti gli altri tre muscoli analizzati (trapezio
medio superiore e infraspinato) che riportano segni di fatica, rendendo cosi impossibile
attribuire le alterazioni biomeccaniche solamente al dentato anteriore.
Il fatto che tutti i muscoli raggiungano la soglia dell’8% spiega la natura sinergica(istica?) ed
elaborata della complessa muscolatura della spalla.
Le alterazioni riscontrate maggiormente riguardano la rotazione interna e il tilt, e non la
rotazione esterna. Questo probabilmente per un affaticamento del dentato anteriore e del
trapezio inferiore, entrambi attivi normalmente nella rotazione esterna della scapola
durante l’elevazione.
Nonostante i segni di fatica riscontrati in maniera generalizzata, la upward rotation non è
alterata immediatamente dopo il task. Questo è un risultato sorprendente perché dentato,
trapezio superiore e inferiore contribuiscono a tale movimento della scapola. È quindi
possibile che durante l’elevazione ci sia un contributo di altri muscoli in sostituzione di
quelli affaticati; un’altra possibile spiegazione è data dal fatto che essendo affaticati i
muscoli coinvolti nella coppia di forze richiesta per la upward rotation non vi sia la perdita
della sinergia balistica richiesta.
La principale limitazione di questo studio è la impossibilità ad isolare ed affaticare con un
compito motorio esclusivamente il dentato anteriore invece che una serie di muscoli, e
questo non permette di raggiungere gli obiettivi che gli autori si sono prefissati; è probabile
che alcuni soggetti presi in esame adottino delle strategie motorie, per completare il
compito affaticante, con il tronco, la scapola o l’omero, e che siano esse in realtà che
attivino gruppi muscolari che poi dimostrano segni di fatica.
23
Una scoperta di particolare interesse in questo studio è la differenza sui dati della fatica
riscontrati tra maschi e femmine, con i primi che dimostravano maggior diminuzione della
MPF in tutti e 4 i muscoli, nonostante la maggior resistenza nell’esecuzione del compito
richiesto rispetto alle donne.
Dai dati proveniente dalla letteratura sembra l’intensità del fatiguing task (% MVC) la
variabile più importante ed un recente studio di (42) ha riportato come in esercizi di minore
intensità le donne dimostrano segni di fatica minori rispetto agli uomini.
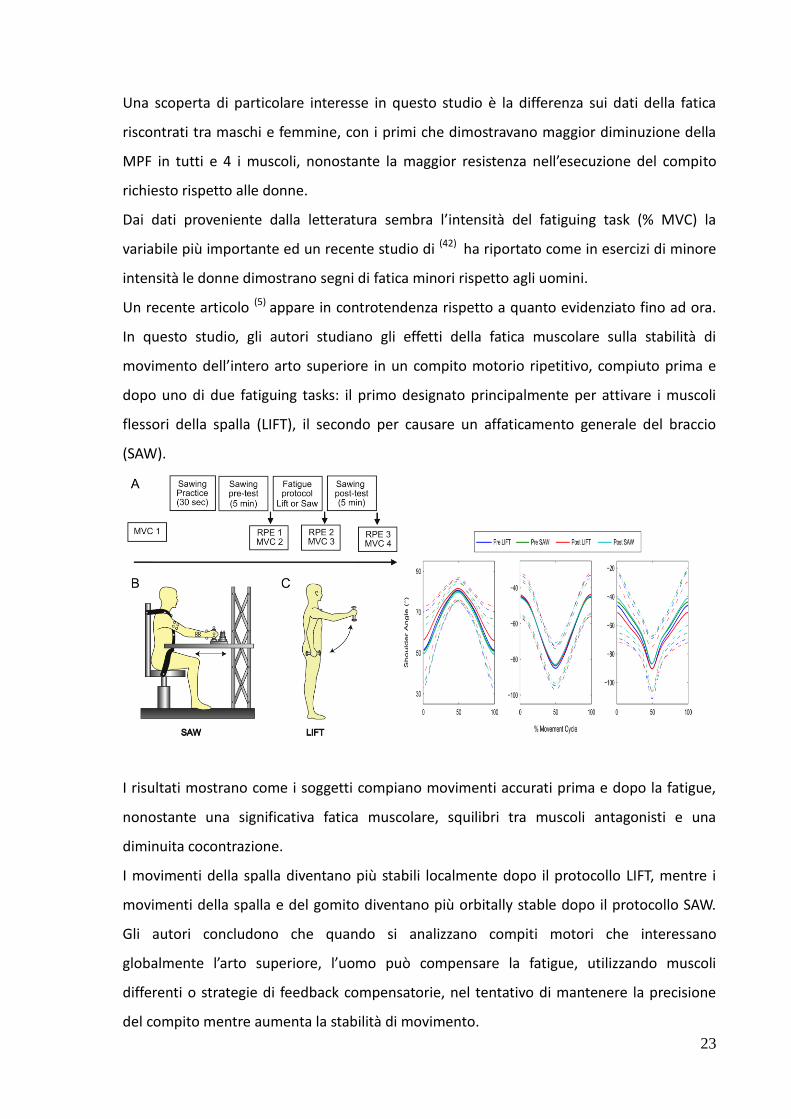
Un recente articolo (5) appare in controtendenza rispetto a quanto evidenziato fino ad ora.
In questo studio, gli autori studiano gli effetti della fatica muscolare sulla stabilità di
movimento dell’intero arto superiore in un compito motorio ripetitivo, compiuto prima e
dopo uno di due fatiguing tasks: il primo designato principalmente per attivare i muscoli
flessori della spalla (LIFT), il secondo per causare un affaticamento generale del braccio
(SAW).
I risultati mostrano come i soggetti compiano movimenti accurati prima e dopo la fatigue,
nonostante una significativa fatica muscolare, squilibri tra muscoli antagonisti e una
diminuita cocontrazione.
I movimenti della spalla diventano più stabili localmente dopo il protocollo LIFT, mentre i
movimenti della spalla e del gomito diventano più orbitally stable dopo il protocollo SAW.
Gli autori concludono che quando si analizzano compiti motori che interessano
globalmente l’arto superiore, l’uomo può compensare la fatigue, utilizzando muscoli
differenti o strategie di feedback compensatorie, nel tentativo di mantenere la precisione
del compito mentre aumenta la stabilità di movimento.

24
Sebbene i risultati della maggior parte di questi studi indichino che la fatica muscolare
influenza la mobilità scapolo toracica e scapolo omerale, e quindi l’accuratezza la precisione
la stabilità dell’intero arto superiore, i meccanismi su come questo avvenga sono tuttora
sconosciuti. Alcuni autori ritengono possa essere il risultato di una ridotta propriocezione,
altri il risultato di un cambiamento nell’attività/sensibilità del sistema dei fusi
neuromuscolari che porta ad un alterato feedback al sistema nervoso centrale. Queste
dinamiche potrebbero portare ad una scorretta coordinazione muscolare con conseguenti
alterazioni nella cinematica scapolare (2).

25
5. Conclusioni
Dall’analisi della letteratura presa in considerazione per rispondere al quesito che ci siamo
posti nello svolgimento di questa tesi emerge che:
Il sistema sEMG non sembra essere uno strumento utile alla valutazione della fatica nel
cingolo scapolare.
Gli studi che utilizzano l’sEMG per la valutazione della fatica nel cingolo
scapolare sono limitati.
I protocolli utilizzati risultano ancora non omogenei e poco standardizzati
(set up, tipo di elettrodo e parametri di acquisizione)
I siti e il numero dei muscoli presi in considerazione presentano un alta
variabilità tra i diversi studi.
Quali siano i task motori da utilizzare (isometrici o dinamici, differente %MVC
presa in esame, tempistica di recupero,ecc..), quali muscoli è possibile
affaticare maggiormente con un determinato task e che interpretazione dare
ai vari risultati EMG è tuttora di difficile analisi.
Le evidenze riguardanti il rapporto tra fatica muscolare e il controllo motorio a livello
dell’arto superiore sono ancora scarse.
L’analisi dei parametri cinematici specifici non viene presa in considerazione
nella maggior parte degli studi.
Le limitate evidenze ottenute sulla relazione tra fatica e controllo motorio
indicano che la fatica stessa influenza la mobilità scapolo toracica e scapolo
omerale, e quindi l’accuratezza la precisione e la stabilità dell’intero arto
superiore. Tuttavia i meccanismi su come questo avvenga sono tuttora
sconosciuti.
La complessa anatomia e la dinamica stessa dell’uso del braccio ne rende
assai complessa un’analisi che tenga conto della globalità del movimento.

26
La popolazione presa in considerazione nei diversi studi presenta caratteristiche tali da
creare un bias statistico (età, sesso, attività lavorativa/sportiva, ecc.) pertanto rappresenta
un ulteriore limite alla possibilità di confrontare i dati raccolti in letteratura.
Sebbene numerosi limiti siano evidenziati nella nostra ricerca, appare indispensabile
adottare negli studi futuri condotte metodologiche uniformi e standardizzate come
proposto dalle raccomandazioni SENIAM.
27
6. Bibliografia
1. Roger M. Enoka and Jacques Duchateau. Muscle fatigue: what, why and how it influences
muscle function. J Physiol 586.1 (2008) pp 11–23
2. François Hug Can muscle coordination be precisely studied by surface electromyography?
Journal of Electromyography and Kinesiology 21 (2011) 1–12
3. Andrew W. Davidson And Charles L. Rice, Effect of shoulder angle on the activation pattern
of the elbow extensors during a submaximal isometric fatiguing contraction Muscle Nerve
42: 514–521, 2010
4. Didier Maqueta, Jean-Louis Croisier, Catherine Duponta, Michel Moutschen, Marc
Ansseauc, Bernard Zeevaerta, Jean-Michel Crielaarda Fibromyalgia and related conditions:
Electromyogram profile during isometric muscle contraction Joint Bone Spine 77 (2010)
264–267
5. Deanna H. Gates and Jonathan B. Dingwell Muscle fatigue does not lead to increased
instability of upper extremity repetitive movements J Biomech. 2010 March 22; 43(5): 913–
919
6. P. Madeleine On functional motor adaptations: from the quantification of motor strategies
to the prevention of musculoskeletal disorders in the neck–shoulder region Acta Physiol
2010, 199 (Suppl. 679), 1–46
7. Jaclyn N. Chop, John M. O’Neill, Kevin Hurley, Clark R. Dickerson, PhD Superior humeral
head migration occurs after a protocol designed to fatigue the rotator cuff: A radiographic
analysis J Shoulder Elbow Surg (2010) 19, 1137-1144
8. Amedeo Troiano, Francesco Naddeo, Erik Sosso, Gianfranco Camarota, Roberto Merletti,
Luca Mesin Assessment of force and fatigue in isometric contractions of the upper trapezius
muscle by surface EMG signal and perceived exertion scale Gait & Posture 28 (2008) 179–
186
9. Kallenberg, H.J. Hermens Behaviour of a surface EMG based measure for motor control:
Motor unit action potential rate in relation to force and muscle fatigue Journal of
Electromyography and Kinesiology 18 (2008) 780–788
10. Julien Piscione Didier Gamet Effect of mechanical compression due to load carrying on
shoulder muscle fatigue during sustained isometric arm abduction: an electromyographic
study Eur J Appl Physiol (2006) 97: 573–581
28
11. Dario Farina, Laura A. C. Kallenberg, Roberto Merletti, Hermie J. Hermens Effect of side
dominance on myoelectric manifestations of muscle fatigue in the human upper trapezius
muscle Eur J Appl Physiol (2003) 90: 480–488
12. D. David Ebaugh, Philip W. McClure, Andrew R. Karduna Effects of shoulder muscle fatigue
caused by repetitive overhead activities on scapulothoracic and glenohumeral kinematics
Journal of Electromyography and Kinesiology 16 (2006) 224–235
13. Mitsutoshi Kimura, Hirotaka Sato, Mamoru Ochi, Satoshi Hosoya, Tsugutake Sadoyama
Electromyogram and perceived fatigue changes in the trapezius muscle during typewriting
and recovery Eur J Appl Physiol (2007) 100:89–96
14. T. Bosch, M.P. de Looze, Kingma B. Visser J.H. van Diee¨n Electromyographical
manifestations of muscle fatigue during different levels of simulated light manual assembly
work Journal of Electromyography and Kinesiology 19 (2009) 246–256
15. A. Holtermann and K. Roeleveld EMG amplitude distribution changes over the upper
trapezius muscle are similar in sustained and ramp contractions Acta Physiol 2006, 186,
159–168
16. Stephen Minning, Colin A. Eliot, Tim L. Uhl, Terry R. Malone EMG analysis of shoulder
muscle fatigue during resisted isometric shoulder elevation Journal of Electromyography
and Kinesiology 17 (2007) 153–159
17. Grace P. Y. Szeto, Leon M. Straker Peter B. O’Sullivan Examining the low, high and range
measures of muscle activity amplitudes in symptomatic and asymptomatic computer
usersperforming typing and mousing tasks Eur J Appl Physiol (2009) 106:243–251
18. Laura A.C. Kallenberg, Elke Schulte b, Catherine Disselhorst-Klug b,Hermie J. Hermens
Myoelectric manifestations of fatigue at low contraction levels in subjects with and without
chronic pain Journal of Electromyography and Kinesiology 17 (2007) 264–274
19. Deborah Falla, Dario Farina Periodic increases in force during sustained contraction reduce
fatigue and facilitate spatial redistribution of trapezius muscle activity Exp Brain Res (2007)
182:99–107
20. Danuta Roman-Liu, Tomasz Tokarski, Karina Wo´ Quantitative assessment of upper limb
muscle fatigue depending on the conditions of repetitive task load Journal of
Electromyography and Kinesiology 14 (2004) 671–682
21. A. Hummel, T. La¨ ubli, M. Pozzo, P. Schenk S. Spillmann, A. Klipstein Relationship between
perceived exertion and mean power frequency of the EMG signal from the upper trapezius
muscle during isometric shoulder elevation Eur J Appl Physiol (2005) 95: 321–326
29
22. Macdonald J. H., D. Farina, And S. M. Marcora Response of Electromyographic Variables
during Incremental and Fatiguing Cycling. Med. Sci. Sports Exerc., Vol. 40, No. 2, pp. 335–
344, 2008
23. Kimberly Szucs, Anand Navalgund, John D. Borstad Scapular muscle activation and co-
activation following a fatigue task Med Biol Eng Comput (2009) 47:487–495
24. Dario Farina, Daniel Zennaro, Marco Pozzo Roberto Merletti, Thomas La¨ ubli Single motor
unit and spectral surface EMG analysis during low-force, sustained contractions of the
upper trapezius muscle Eur J Appl Physiol (2006) 96: 157–164
25. Andreas Holtermann, Christer Gro¨nlund, J. Stefan Karlsson, Karin Roeleveld Spatial
distribution of active muscle fibre characteristics in the upper trapezius muscle and its
dependency on contraction level and duration Journal of Electromyography and Kinesiology
18 (2008) 372–381
26. Han-Ming Chen, Chun-Tong Leung The effect on forearm and shoulder muscle activity in
using different slanted computer mice Clinical Biomechanics 22 (2007) 518–523
27. Pascal Madeleine, Dario Farina Time to task failure in shoulder elevation is associated to
increase in amplitude and to spatial heterogeneity of upper trapezius mechanomyographic
signals Eur J Appl Physiol (2008) 102:325–333
28. E. Schulte, O. Miltner, E. Junker, G. Rau C. Disselhorst-Klug Upper trapezius muscle
conduction velocity during fatigue in subjects with and without work-related muscular
disorders: a non-invasive high spatial resolution approach Eur J Appl Physiol (2006) 96: 194–
202
29. Pascal Madeleine, Dario Farina, Roberto Merletti Lars Arendt-Nielsen Upper trapezius
muscle mechanomyographic and electromyographic activity in humans during low force
fatiguing and non-fatiguing contractions Eur JAppl Physiol (2002) 87: 327–336
30. N. Goudy, L. McLean Using myoelectric signal parameters to distinguish between computer
workers with and without trapezius myalgia Eur J Appl Physiol (2006) 97: 196–209
31. Olivier Missenard, Denis Mottet, Stephane Perrey The role of cocontraction in the
impairment of movement accuracy with fatigue Exp Brain Res (2008) 185:151–156
32. P. G. Martin, S. C. Gandevia and J. L. Taylor Muscle fatigue changes cutaneous suppression
of propriospinal drive to human upper limb muscles Physiol 580.1 (2007) pp 211–223
33. Kanekar a, Marcio J. Santos a, Alexander S. Aruin Anticipatory postural control following
fatigue of postural and focal muscles Neeta Clinical Neurophysiology 119 (2008) 2304–
2313
34. Mark P. Cote, Gregg Gomlinski, Jeremiah Tracy, Augustus D.Mazzocca Radiographic analysis
of commonly prescribed scapular exercises J Shoulder Elbow Surg (2009) 18, 311-316

30
35. John D. Borstad, Kimberly Szucs, Anand Navalgund Scapula kinematic alterations following
a modified push-up plus task Human Movement Science 28 (2009) 738–751
36. Kimberly Szucs, Anand Navalgund, John D. Borstad Scapular muscle activation and co-
activation following a fatigue task Med Biol Eng Comput (2009) 47:487–495
37. Roberto Merletti Elementi di elettromiografia di superficie: materiale didattico integrativo
alle Raccomandazioni Europee in Elettromiografia di superficie Novembre 2000 CLUT
Editrice
38. Merletti R., Rainoldi A., Farina D. Surface EMG for non invasive muscle characterization
Exercise and sport sciences reviews 2000a
39. Merletti R., Farina D., Gazzoni M., Schieroni M.P., Effect of age on muscle functions
investigated with surface electromyography Muscle & Nerve 2000c
40. Farina D., Fortunato E., Merletti R., Non invasive estimation of motor unit conduction
velocity distribuition using linear electrode arrays IEEE Trans Biomed Eng 47(3) 380-388
41. McQuade KJ, Dawson J, Smidt GL (1998) Scapulothoracic muscle fatigue associated with
alterations in scapulohumeral rhythm kinematics during maximum resistive shoulder
elevation. J Orthop Sports Phys Ther 28(2):74–80
42. Yoon, T., Schlinder Delap, B., Griffith, E. E., & Hunter, S. K. (2007). Mechanisms of fatigue
differ after low- and high-force fatiguing contractions in men and women. Muscle and
Nerve, 36, 515–524.
43. Dimitrova, Dimitrov Interpretation of EMG changes with fatigue: facts, pitfalls, and fallacies
of Electromyography and Kinesiology 13 (2003) 13-36












![Pentola a pressione elettria programmaile...Instant Pot® è una pentola fa ile e omoda da usare he fa risparmiare tempo in u ina. razie ai suoi 10 programmi intelligenti {1]ontrollati](https://static.fdocumenti.com/doc/165x107/6120bc1c344ade65351827b6/pentola-a-pressione-elettria-programmaile-instant-pot-una-pentola-fa-ile.jpg)





