Complicanze cardiache dell ipertiroidismo - … · Roma, 9-11 novembre 2012 Complicanze cardiache...
10
Roma, 9-11 novembre 2012 Complicanze cardiache dell’ipertiroidismo gestione nei diversi setting assistenziali perché?
Transcript of Complicanze cardiache dell ipertiroidismo - … · Roma, 9-11 novembre 2012 Complicanze cardiache...

Roma, 9-11 novembre 2012
Complicanze cardiache dell’ipertiroidismo
gestione nei diversi setting assistenziali
perché?

Roma, 9-11 novembre 2012
• Ambulatorio MMG • Ambulatorio specialistico territoriale • Ambulatorio specialistico ospedaliero • Day Service • Day Hospital • Ricovero ordinario specialistico (“a gestione diretta”)
• Ricovero ordinario interspecialistico (“consulenza”)
setting assistenziali
INTEGRAZIONE fra le SPECIALIZZAZIONI

Roma, 9-11 novembre 2012
Ospedali di prossimità
AO centri di riferimento
Ambulatori territoriali
Studi MMG
RETI INTEGRATE DI SERVIZI a varia complessità strutturale ed organizzativa
La medicina del futuro

Roma, 9-11 novembre 2012
superare “le mura” tra UO SPECIALISTICHE

Roma, 9-11 novembre 2012
“integrazione é
comunicazione efficace”

Roma, 9-11 novembre 2012
Comunicazione in Medicina
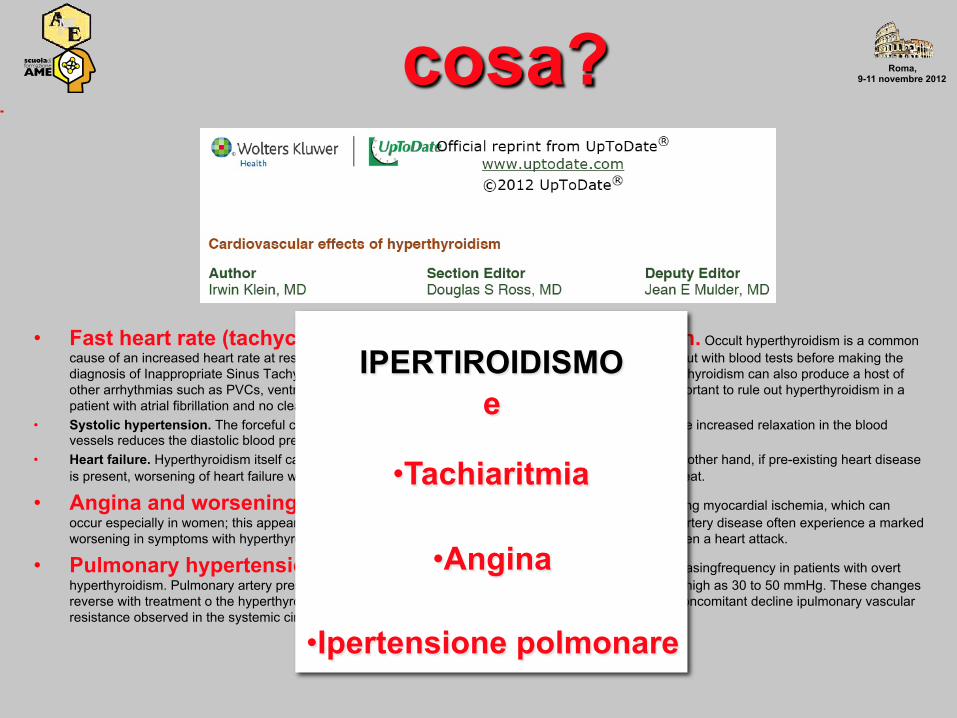
Roma, 9-11 novembre 2012 cosa?
• Fast heart rate (tachycardia) and palpitations, atrial fibrillation. Occult hyperthyroidism is a common cause of an increased heart rate at rest and with mild exertion. Hyperthyroidism should always be ruled out with blood tests before making the diagnosis of Inappropriate Sinus Tachycardia. Especially in patients with underlying heart disease, hyperthyroidism can also produce a host of other arrhythmias such as PVCs, ventricular tachycardia, and especially atrial fibrillation. Indeed, it is important to rule out hyperthyroidism in a patient with atrial fibrillation and no clear underlying cause.
• Systolic hypertension. The forceful cardiac contraction increases the systolic blood pressure, though the increased relaxation in the blood vessels reduces the diastolic blood pressure.
• Heart failure. Hyperthyroidism itself can produce heart failure, but this condition is relatively rare. On the other hand, if pre-existing heart disease is present, worsening of heart failure with hyperthyroidism is common, and can be extremely difficult to treat.
• Angina and worsening angina. Anginal-like chest pain, with EKG changes suggesting myocardial ischemia, which can occur especially in women; this appears to be the result of coronary vasospasm. Patients with coronary artery disease often experience a marked worsening in symptoms with hyperthyroidism. These can include an increase in chest pain (angina) or even a heart attack.
• Pulmonary hypertension — Pulmonary hypertension (PH) has been reported with increasingfrequency in patients with overt hyperthyroidism. Pulmonary artery pressures average twice normal v values (10 mmHg) and may be as high as 30 to 50 mmHg. These changes reverse with treatment o the hyperthyroidism and may reflect the increase in cardiac output without the concomitant decline ipulmonary vascular resistance observed in the systemic circulation
IPERTIROIDISMO e
• Tachiaritmia
• Angina
• Ipertensione polmonare

Roma, 9-11 novembre 2012 chi?
• Cappelli • De Biase • Deandrea • Limone • Piantoni • Tiratterra • Triggiani

Roma, 9-11 novembre 2012 come?
• Presentazione delle sessione 5 min– Giammarco • I parte - 40 min (tolleranza fino a 45) Endocrinologo e Cardiologo: ipertiroidismo e aritmia Conduce L. Piantoni Discussants: M. Deandrea, L. De Biase • II parte - 50 min (tolleranza fino a 55) Endocrinologo e Cardiologo: ipertiroidismo e dolore toracico Conduce V. Giammarco - V. Triggiani - relazione introduttiva - 10 min Discussants: C. Cappelli, F. Tiratterra -------------
Take-home messages P. Limone 10 min (tolleranza fino 15 min)
Roma, 9-11 novembre 2012
“standard” &“assolo”






![Tiroide ipotiroidismo e ipertiroidismo[1]](https://static.fdocumenti.com/doc/165x107/556db60bd8b42aed2e8b46a2/tiroide-ipotiroidismo-e-ipertiroidismo1.jpg)








![340]) - MIT - Massachusetts Institute of Technologyweb.mit.edu/asabatin/www/Med/SMC2/Anatomia-Patologica-Massi/... · Complicanze cardiache −Estensione peri-valvolare del processo](https://static.fdocumenti.com/doc/165x107/5c6d22ab09d3f2d9358b9b66/340-mit-massachusetts-institute-of-complicanze-cardiache-estensione.jpg)