Combined large cell neuroendocrine carcinoma and papillary ......intestine, where they are often...
4
Combined large cell neuroendocrine carcinoma and papillary serous carcinoma of the endometrium rare type with literature review. Enaam M Junainah 1* , Hassan F Huwait 2 , Nisreen Khalid Aref Albezrah 3 , Ahmed S Bakr 4 , Hala Elnashar 5 , Saad Alawwad 6 , Haytham Dahlawi 7 , Rana Zaini 8 , Jamal Junainah 9 , Elaf Junainah 9 , Sahar Fattah 9 , Muhannad B Qarah 10 , Najd Alsekhairi 1 1 Pathology Department, Taif University, Saudi Arabia 2 Pathology Department, Umm AL-qura University, Saudi Arabia 3 Obstatric and Gynecology Department, Taif University, Saudi Arabia 4 Department of Microbiology, Alazhar University, Saudi Arabia 5 Histology Department, Suez Canal University, Saudi Arabia 6 King Faisal University, Saudi Arabia 7 Obstetric and Genecology Department, Aya Hospital, Saudi Arabia 8 Medicine Department, King Abdul-Aziz University, Saudi Arabia 9 Medicine Department, King Abdul Aziz Hospital, Jeddah, MOH, Kingdom of Saudi Arabia 10 Medicine Department, King Fasal Speciality Hospital, Kingdom of Saudi Arabia Abstract Neuroendocrine Tumours (NEC), are neoplasms that arise from cells of the endocrine (hormonal) and nervous systems. Many are benign, while some are malignant. They most commonly occur in the lung, intestine, where they are often called carcinoid tumours, but they are also found in the pancreas, and the rest of the body. The female genital counterpart is aggressive and uncommon, with propensity to involve the cervix and ovary, the endometrium variant is seldom occurring and tends to be of a conventional small cell type (up to 60 cases). Only twelve cases of large cell type NEC. In our centre, we diagnose a case of Large-Cell Neuroendocrine Carcinoma (LCNEC) of the, endometrium in an 82 y old female. It was report it as mixed type tumour papillary serous and large neuroendocrine, with FIGO nuclear grade III, the endocrine origin of the tumour was confirmed by immunohistochemically endocrine marker CD56 and NSE. Patient medical condition was unfit for surgery and she chose palliative treatment. Keywords: Endometrium, Large-cell neuroendocrine carcinoma, Neuroendocrine carcinoma. Accepted on August 16, 2017 Introduction Large Neuroendocrine Carcinoma (LNEC) tends to be high grade and is known to behave in aggressive fashion. It is predominantly occurring in the lung. Recently few cases been reported in the female genital tract, most commonly in the cervix [1-3]. Although the primary (LNEC) of the endometrium is quite rare, the age of presentation is usually between 30-90 y, however, the presentation of endometrial (LNEC) is related to metastases [4], and some time to associated symptom of concomitant paraneoplastic syndromes such as [5], Cushing syndrome due to ectopic ACTH production [6]. We discuss the pathological aspect and diagnostic tool of immunohistochemically stain in 83 y old woman who present with postmenopausal bleeding, in which her histopathology diagnosis was issued as mixed type tumour papillary serous and large neuroendocrine, with FIGO nuclear grade III. Case Presentation 83 y old Saudi woman complains of post-menopausal bleeding since six months. She soaks medical advice in Aya Hospital. At presentation, on physical examination was unremarkable, and ISSN 0970-938X www.biomedres.info Biomed Res 2017 Volume 28 Issue 19 Biomedical Research 2017; 28 (19): 8165-8168 8165
Transcript of Combined large cell neuroendocrine carcinoma and papillary ......intestine, where they are often...

Combined large cell neuroendocrine carcinoma and papillary serouscarcinoma of the endometrium rare type with literature review.
Enaam M Junainah1*, Hassan F Huwait2, Nisreen Khalid Aref Albezrah3, Ahmed S Bakr4, HalaElnashar5, Saad Alawwad6, Haytham Dahlawi7, Rana Zaini8, Jamal Junainah9, Elaf Junainah9, SaharFattah9, Muhannad B Qarah10, Najd Alsekhairi1
1Pathology Department, Taif University, Saudi Arabia2Pathology Department, Umm AL-qura University, Saudi Arabia3Obstatric and Gynecology Department, Taif University, Saudi Arabia4Department of Microbiology, Alazhar University, Saudi Arabia5Histology Department, Suez Canal University, Saudi Arabia6King Faisal University, Saudi Arabia7Obstetric and Genecology Department, Aya Hospital, Saudi Arabia8Medicine Department, King Abdul-Aziz University, Saudi Arabia9Medicine Department, King Abdul Aziz Hospital, Jeddah, MOH, Kingdom of Saudi Arabia10Medicine Department, King Fasal Speciality Hospital, Kingdom of Saudi Arabia
Abstract
Neuroendocrine Tumours (NEC), are neoplasms that arise from cells of the endocrine (hormonal) andnervous systems. Many are benign, while some are malignant. They most commonly occur in the lung,intestine, where they are often called carcinoid tumours, but they are also found in the pancreas, and therest of the body. The female genital counterpart is aggressive and uncommon, with propensity to involvethe cervix and ovary, the endometrium variant is seldom occurring and tends to be of a conventionalsmall cell type (up to 60 cases). Only twelve cases of large cell type NEC. In our centre, we diagnose acase of Large-Cell Neuroendocrine Carcinoma (LCNEC) of the, endometrium in an 82 y old female. Itwas report it as mixed type tumour papillary serous and large neuroendocrine, with FIGO nucleargrade III, the endocrine origin of the tumour was confirmed by immunohistochemically endocrinemarker CD56 and NSE. Patient medical condition was unfit for surgery and she chose palliativetreatment.
Keywords: Endometrium, Large-cell neuroendocrine carcinoma, Neuroendocrine carcinoma.Accepted on August 16, 2017
IntroductionLarge Neuroendocrine Carcinoma (LNEC) tends to be highgrade and is known to behave in aggressive fashion. It ispredominantly occurring in the lung. Recently few cases beenreported in the female genital tract, most commonly in thecervix [1-3]. Although the primary (LNEC) of theendometrium is quite rare, the age of presentation is usuallybetween 30-90 y, however, the presentation of endometrial(LNEC) is related to metastases [4], and some time toassociated symptom of concomitant paraneoplastic syndromessuch as [5], Cushing syndrome due to ectopic ACTH
production [6]. We discuss the pathological aspect anddiagnostic tool of immunohistochemically stain in 83 y oldwoman who present with postmenopausal bleeding, in whichher histopathology diagnosis was issued as mixed type tumourpapillary serous and large neuroendocrine, with FIGO nucleargrade III.
Case Presentation83 y old Saudi woman complains of post-menopausal bleedingsince six months. She soaks medical advice in Aya Hospital. Atpresentation, on physical examination was unremarkable, and
ISSN 0970-938Xwww.biomedres.info
Biomed Res 2017 Volume 28 Issue 19
Biomedical Research 2017; 28 (19): 8165-8168
8165

the results of routine serum biochemistry are within normallimit, apart from CBC, HB show mild normocyticnormochromic anaemia, per vaginal examination show noabnormality regardless the complain of PV bleeding cytologywas negative at admission. Ultrasound examinations revealedthick endometrium in which hysteroscopy biopsy waspreformed, multiple fragment of greyish brown andheomhargic tissue was obtained measuring in aggregate 7 × 4 ×3 cm. Microscopic examination revealed multiple fragments ofendometrial tissue and, report was issued with a diagnosis ofcombined endometrial carcinoma with a component ofpapillary serous endometroid and large neuroendocrinecarcinoma. Patient underwent radical hysterectomy, bilateralsalpingo oophorectomy, bilateral pelvic lymph nodesdissection, and omenectomy. On gross pathologic examination,the uterus weighed 100 g, measures 4.5 cm from Cronus toCronus, 3.5 cm anterior to posterior and body cavity measures5 cm, there was large haemorrhagic mass seen involving thewhole posterior endometrium and part of the anterior surfacemeasuring 3 × 3 cm it was away from the cervical canal andvaginal vault by 4 cm, although grossly there was brownishirregular area seen along the endo cervical canal. 14 bulkypelvic lymph nodes measuring up to 3 cm was obtained. Theovaries, tubes and omenum are grossly free. On microscopicexamination shows diffuse neoplastic growth, comprised of anadmixture of combined papillary serous carcinoma and largecell neuroendocrine carcinoma (Figure 1). Both componentsare typically high-grade, exhibit solid sheets, island and focalareas of papillary pattern floated in lakes of mucin. The tumourcells made up of medium to large polygonal cells with scant tomoderate amphiphilic cytoplasm, grow in cords and trabeculaepattern and focal pseudo rosette formation. Abundant mitoticfigures are seen, (up to 19 mitoses per 10 high-power fields),as well as numerous apoptotic bodies a foci of geographicnecrosis. Nuclear melding and crush artefact were focallynoticed, and some of the large cells were multinucleated. Areaof papillary serous carcinoma was present I (constituting 30%of the tumour). The surrounding area show poorlydifferentiated component, (about 10%), there is evidence ofvascular invasion. The tumour involved 50% thickness of themyometrium (1 mm away from the serosal surface) as well asthe cervical stromal connective tissue, and bilateral ovaries andtubes. Lymphovascular space invasion was present. Tow of 14pelvic lymph nodes was positive for metastasis. The omentumwas free from tumour deposit. Immunohistochemistry wasperformed. CK, P53, (Figure 2) neuroendocrine marker CD56and NSE, (Figure3) were performed using manual procedureencompasses antigen retrieval and applying the labelledantibody. Control used is breast, tonsil and appendix. CK showstrong positive expression of the epithelial cells,neuroendocrine marker (CD56 and NSE) show strong positiveexpression of the epithelial cells with large neuroendocrinefeature, while negative in the endometrial component. P53show strong positive nuclear expression of the epithelial cells(95%), indicate high grade lesion. Her final FIGO histologicalgrade was III. Pathological staging (pTNM) stage was pT3a,pN1, pMx. Patient receives chemotherapy treatment and she isdoing well and alive up to date.
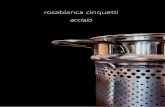
Figure 1. A: Note the papillary serous carcinoma component formingirregular islands and trabeculae (hematoxylin-eosin, originalmagnifications X400); B: Large cell neuroendocrine carcinoma. Noteneuroendocrine component with large cells and amophilic cytoplasm(hematoxylin-eosin, original magnifications X400); C:Neuroendocrine component grows in cords and trabeculae patternand focal pseudo rosette formation (hematoxylin-eosin, originalmagnifications X400).
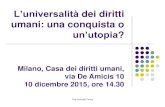
Figure 2. A show positive immunostaining for Pan CK,(Immunoperoxidase stain, original magnifications X400); B: Showpositive immunostaining for P53, (Immunoperoxidase stain, originalmagnifications X400).
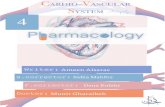
Figure 3. A show positive immunostaining for neuroendocrine markerCD56, (Immunoperoxidase stain, original magnifications X400); B:Show strong positive immunostaining for neuroendocrine markerNSE, (Immunoperoxidase stain, original magnifications X400).
DiscussionThe most common site of developing LNEC is the lung, andgastrointestinal tract. Extra-pulmonary LNEC comprises lessthan 4% of all LNECs. The female genital organs are a veryrare site for LNEC to occur and majority are seen in the cervixand ovary [1,3,5,7]. Primary endometrial LNEC is extremely
Junainah/Huwait/Albezrah/Bakr/Elnashar/Alawwad/Dahlawi/Zaini/Junainah/Junainah/Fattah/Qarah/Alsekhairi
8166 Biomed Res 2017 Volume 28 Issue 19

rare [2,8,9], accounting for about 0.78% of all endometrialcarcinomas. The primary uterine variant is tending to be veryaggressive and mostly combined with other high grade variantof endometrial carcinoma [13,14,16]. This tumour has a highpropensity for systemic spread, therefore it carries poorprognosis. the age prevalence is usually between 40-90 y moreoften seen in postmenopausal women who presented clinicallywith history of per vaginal (postmenopausal) bleeding,sometime the symptom may be related to paraneoplasticsyndrome that is commonly associated with this tumour,particularly Cushing syndrome, due to ACTH, [5,6,17].Radiologically, transvaginal ultrasound is the initial imaginginvestigation of choice for patients presenting with the usualsymptom of a postmenopausal bleed. A thickenedendometrium requires endometrial sampling. MRI isconsidered superior to CT for local staging [1,6]. Contrastenhanced MRI imaging improves accuracy in detectingmyometrial invasion. Endometrial cytopathology is a powerfultool for the detection of a wide variety of benign atypia’s,inflammatory changes, and infectious organisms. It is alsohelpful for the cytohormonal evaluation of patients and thedetection of endometrial malignancies. The cytologicalsensitivity in detecting endometrial carcinoma is about 30%therefore the literature review document only two cases ofendometrial LNEC in cytology. Pathological examination theoptimal procedure is the radical hysterectomy, in order to do aproper histopathological staging of the myometrial depth ofinvasion and subsequent cervical, vaginal and adnexalextension. Unfortunately, in our case the patient was old andrefused to do operation. So our microscopic evaluation wasbased mainly on endometrial solid sheets of pleomorphic cellswith frequent large polygonal cells, that exhibit scant tomoderate amphiphilic cytoplasm, foci with cords andtrabeculae and pseudo rosette formation are noticed, abundantmitotic figures are seen, (up to 19 mitoses per 10 high-powerfields), as well as numerous apoptotic bodies a foci ofgeographic necrosis. Nuclear melding and crush artefact werefocally noticed; area of papillary serous carcinoma was presentI (constituting 30% of the tumour). The surrounding area showpoorly differentiated component, (about 10%), there isevidence of vascular invasion.
Immunohistochemical stain is considered as the best ancillarytool for diagnosing confirmation of neuroendocrinehistogenesis origin of the tumour cells. The commonly usedneuroendocrine marker is synaptophysin, chromogranin andCD56 and NSE. Approximately 25 to 38% of cases expressingchromogranin and synpatophysin [9-12]. While (NSE) and(CD56) show constant strong positive stain in the NEC cells inabout 90-100% of the cases. Expression of broad-spectrumcytokeratins is usually present. Staging of endometrialcarcinoma is a based on the FIGO staging system, which is asurgical and pathological staging following total abdominalhysterectomy, salpingo-oopherectomy, lymphadenectomy andperitoneal washings.
The differential diagnosis, of primary endometrial LNEC ismetastatic spread from the cervix, however other endometrialcarcinomas (Carcinosarcomas, stromal sarcomas and primitive
neuroectodermal tumors of the uterus), which containargyrophil cells. Undifferentiated and dedifferentiatedendometrioid carcinomas also included in deferential list of theLNEC [16,17], in contrast to the genetic progression ofcarcinomas [18,19]. Recently study on massively number ofendometrial carcinoma, finally authors end up by fact thatTP53 mutation is commonly expressed in higher grade group,therefore our case shows strong P53 expression>than 98% ofthe cells which is correlated with poor prognosis andaggressive behaviour.
AcknowledgementsSpecial thanks for Almamlka Labs for their support.
References1. Atienza-Amores M, Guerini-Rocco E, Soslow RA, Park
KJ, Weigelt B. Small cell carcinoma of the gynecologictract: a multifaceted spectrum of lesions. Gynecol Oncol2014; 134: 410-418.
2. Crowder S, Tuller E. Small cell carcinoma of the femalegenital tract. Sem Oncol 2007; 34: 57-63.
3. Eichhorn JH, Young RH. Neuroendocrine tumors of thegenital tract. Am J Clin Pathol 2001; 115: 94-112.
4. Katahira A, Akahira J, Niikura H, Ito K, Moriya T,Matsuzawa S, Makinoda S, Oda T, Fujiwara K, YaegashiN. Small cell carcinoma of the endometrium: report ofthree cases and literature review. Int J Gynecol Cancer2004; 14: 1018-1023.
5. Campo E, Brunier MN, Merino MJ. Small cell carcinomaof the endometrium with associated ocular paraneoplasticsyndrome. Cancer 1992; 69: 2283-2288.
6. Sato H, Kanai G, Kajiwara H, Itoh J, Osamura RY. Small-cell carcinoma of the endometrium presenting as Cushingssyndrome. Endocrine J 2010; 57: 31-38.
7. van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet 2011; 378: 1741-1755.
8. Marioni G, Savastano M, Mattiello L, Koussis H, CarpeneS, Marino F, Staffieri A. Tongue base metastasis fromneuroendocrine endometrial small cell carcinoma. Am JOtolaryngol 2007; 28: 284-287.
9. Sakamoto H, Takenaka M, Ushimaru K, Tanaka T. Use ofLiquid-Based Cytology (LBC) and cell blocks from cellremnants for cytologic, immunohistochemical, andimmunocytochemical diagnosis of malignancy. Open JPathol 2012; 2 58-65.
10. Ishida M, Iwamoto N, Nakagawa T, Kaku S, Iwai M,Kagotani A, Takahashi K, Murakami T, Okabe H. Smallcell carcinoma of the endometrium: a case report withemphasis on the cytological features. Int J Clin Exp Pathol2014; 7: 3332-3337.
11. Proca D, Keyhani-Rofagha S, Copeland LJ, Hameed A.Exfoliative cytology of neuroendocrine small cellcarcinoma of the endometrium. A report of two cases. ActaCytologica 1998; 42: 978-982.
Combined large cell neuroendocrine carcinoma and papillary serous carcinoma of the endometrium rare type withliterature review
Biomed Res 2017 Volume 28 Issue 19 8167

12. Kurman RJ, Carcangiu ML, Herrington CS, Young RH.WHO classification of tumours of female reproductiveorgans. IARC Press Lyon 2014.
13. van Hoeven KH, Hudock JA, Woodruff JM, Suhrland MJ.Small cell neuroendocrine carcinoma of the endometrium.Int J Gynecol Pathol 1995; 14: 21-29.
14. Huntsman DG, Clement PB, Gilks CB, Scully RE. Small-cell carcinoma of the endometrium. A clinicopathologicalstudy of sixteen cases. Am J Surg Pathol 1994; 18:364-375.
15. Albores-Saavedra J, Martinez-Benitez B, Luevano E. Smallcell carcinomas and large cell neuroendocrine carcinomasof the endometrium and cervix: polypoid tumors and thosearising in polyps may have a favorable prognosis. Int JGynecol Pathol 2008; 27: 333-339.
16. Tafe LJ, Garg K, Chew I, Tornos C, Soslow RA.Endometrial and ovarian carcinomas with undifferentiatedcomponents: clinically aggressive and frequently
underrecognized neoplasms. Mod Pathol 2010; 23:781-789.
17. Silva EG, Deavers MT, Malpica A. Undifferentiatedcarcinoma of the endometrium: a review. Pathology 2007;39: 134-138.
18. Frazier SR, Kaplan PA, Loy TS. The pathology ofextrapulmonary small cell carcinoma. Sem Oncol 2007; 34:30-38.
19. Pearse AG. The diffuse endocrine system and theimplications of the APUD concept. Int Surg 1979.
*Correspondence toEnaam M Junainah
Pathology Department
Taif University
Saudi Arabia
Junainah/Huwait/Albezrah/Bakr/Elnashar/Alawwad/Dahlawi/Zaini/Junainah/Junainah/Fattah/Qarah/Alsekhairi
8168 Biomed Res 2017 Volume 28 Issue 19