Colangiocarcinoma “on the rise” - AISF · D. ALVARO, Univ. Sapienza, Rome, Italy. MONOTEMATICA...
31
D. ALVARO, Univ. Sapienza, Rome, Italy. MONOTEMATICA AISF, The future of Liver Diseases, Milano 13-15 Ottobre 2016 Colangiocarcinoma “on the rise” !
Transcript of Colangiocarcinoma “on the rise” - AISF · D. ALVARO, Univ. Sapienza, Rome, Italy. MONOTEMATICA...

D. ALVARO, Univ. Sapienza, Rome, Italy.
MONOTEMATICA AISF, The future of Liver Diseases,
Milano 13-15 Ottobre 2016
Colangiocarcinoma “on the rise” !

Domenico ALVARO, MD.SAPIENZA, ROMA
Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi
12 mesi conflitto d’interesse in relazione a questa presentazione
e
che la presentazione non contiene/contiene discussione
di farmaci in studio o ad uso off-label

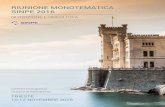
Distal (dCCA)
2-5%
INTRAHEPATIC
(iCCA)
10-20%
CHOLANGIOCARCINOMA (CCA): a more recent classification
based on anatomic location (EASL, ILCA guidelines 2013/2014, ENS-CCA))
Perihilar
(pCCA)
70-85%
Klatskin t.
second-order bile ducts
This classification overcomes the difficulties in classifying pCCA
as intra- or extra-hepatic
but ..
In ICD-O3, CCA is topographically classified as
C22 ‘‘liver and intrahepatic bile ducts’’ or
C24 ‘‘other and unspecified parts of the biliary tract’’.
Current epidemiological data evaluate only iCCA and eCCA !
Therefore, CCA classification in iCCA,
pCCA, dCCA is clinically useful
but ..
clashes with current epidemiologic
studies…… including risk factors!

2014
CCA: Worldwide incidence (cases/100,000), Banales JM…Alvaro D. Nature Rev. 2016.

Temporal trends in IH- and EH-CCA
incidence/mortality in 1980-2009.
In different countries, 1980-2009 yrs
incidence/mortality…
↑ for IH-CCA
=↓ for EH-CCA
Real or false increasing
incidence of IH-CCA ?
Bias ???

The reported increasing incidence of IH-CCA is biased
by:
- misclassification of perihilar-CCA as IH-CCA ?
- improved diagnostic tools ?
- less diagnosis of carcinoma of unknown primary site
(CUP).
Real or false increasing
incidence of IH-CCA ?
Bias ???

CHOLANGIOCARCINOMA: epidemiology !
Biases and criticisms !
USA SEER-9 registries, Welzel TM et al. (J Natl Cancer Inst 2006)
ICD-02: overreporting of IH-CCA by 13%
underreporting of EH-CCA by 15 %
IH-CCA
EH-CCA
Morphology
Morphology+
topography
Italian Cancer registries
(Capocaccia P. et al. DLD 2010)
IH-CCA = 20-30 %
EH-CCA = 40-50 %
NOS = 20-40%

13 SEER registries
(9,840 CC cases, 1992–2007)
90 % Klatskin ..as ICC 1992–2000
45% “ 2001–2007


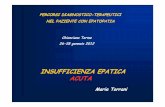
TASSI DI INCIDENZA STANDARDIZZATI PER IH-CCA
ED EH-CCA NELLE POPOLAZIONI OSSERVATE DA
9 REGISTRI (PERIODO 1988-2002) E DA 13 REGISTRI
(PERIODO 1997-2005) ITALIANI. (Alvaro D. et al. DLD 2009)
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
18,0
20,0
1988 1990 1992 1994 1996 1998 2000 2002 2004
anno di diagnosi
tass
o s
tan
dar
diz
zato
x m
ilio
ne
Extra-Epatico9 registri 13 registri
Intra-Epatico
+ 3%/anno
+ 6%/anno + 4%/anno

Cancer Deaths in USA in 2030 Liver and intrahepatic bile ducts

2014

The reported increasing incidence of IH-CCA is biased
by:
- misclassification of perihilar-CCA as IH-CCA ?
- improved diagnostic tools ?
- less diagnosis of carcinoma of unknown primary site
(CUP).
Real or false increasing
incidence of IH-CCA ?
Bias ???

The proportion of patients with different disease stages
shown in successive 5-year cohorts(Shaib Y. J. Hepatology 2004).

The reported increasing incidence of IH-CCA is biased
by:
- missclassification of perihilar-CCA as IH-CCA ?
- improved diagnostic tools ?
- less diagnosis of carcinoma of unknown primary site
(CUP).
Real or false increasing
incidence of IH-CCA ?
Bias ???


American Hepato-Pancreato-Biliary Association

92-gene biomarker panel (RT-PCR–based protocol) and
computational approach ….

American Hepato-Pancreato-Biliary Association2015
ICCs N. 83
HCC N. 42
Non hepatic origin N. 332
(perihilar-CCA, pancreas, stomach, esophagus, colon, breast, ovary,
endometrium, kidney, and urinary bladder)
Albumin RNA ISH positive in 82 (99 %) ICCs and in
42 (100 %) HCC
Perihilar and distal-CCA = 100% negative
22 % of previously diagnosed CUP
tested positive for albumin-RNA !
IH-CCA 22% of CUP !!!!!!!

The reported increasing incidence of IH-CCA is biased
by:
- misclassification of perihilar-CCA as IH-CCA ?
- improved diagnostic tools ?
- less diagnosis of carcinoma of unknown primary site
(CUP).
Real or false increasing
incidence of IH-CCA ?
Bias ???

Real increasing
incidence of IH-CCA !
Why ??

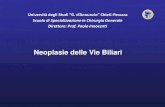
PSC
O.Viverrini
C. Sinensis
Choledochal
cysts , Caroli’s
Thorotrast
pCCA
22.92A meta-analysis of risk factors for
intrahepatic cholangiocarcinoma.
Palmer WC, Patel T. J. Hepatology 2012
AISF commissione colangiocarcinoma, DLD 2009.
IH-CCA EH-CCAn= 116 n= 102
Cirrhosis 16 (13.8%) 5 (4.3%)
Cirrhosis viral 12 (10.3%) 3 (2.9%)
HCV-Ab+ 18 (15.5%) 8 (7.8%)
HBsAg+ 17 (14.6%) 10 (9.8%)

2016
Experimental Diabetes
Human Diabetes2016
Metabolic Syndrome and Gastrointestinal Cancer Risk !
Working Hypothesis
Activation of stem/progenitor cells in PBGs, pancreatic duct
glands and colon crypts, and differentiation toward insulin-
producing cells, could represent the biologic basis for GI cancer
risk ?

CCA risk factors
iCCA pCCA
n= 116 n= 102
Positive hepatitis
virus markers 35 (30.2%) 19 (18.6%) p= 0.048
No putative risk factorin 60% CCA !

CCA: probable risk factors
Biliary-enteric
drainage
Toxins: dioxins,
asbestos
Choledocolithiasis
Cholangitis
Liver
Cirrhosis Cholelithiasis/cholecystectomy
Diabetes, Alcohol
Obesity, tobacco
IBD
Hepatic
Schistosmiasis
EH-CCA
IH-CCA



Chronic inflammation and CCA
Chronic
Inflammation
(flukes,PSC..)
Apoptosis
Proliferation
iNOS
NO
Nitrosylation DNA basis
and DNA repair proteins, caspase 9
Mutagenesis
IL6
TNF
COX-2
PgE2



Prof. E. Gaudio
Acknowledgments
Prof L. Reid at UNC
Dr V. CardinaleThanks for the attention
Dr G. Carpino
Prof. P. Berloco Prof. M. Nuti/Dr. Napolitano
Prof. A.F. Attili/Prof. A. DeSantis