BPCO e disturbi del sonno: più che una associazione · BPCO e disturbi del sonno: più che una...
39
BPCO e disturbi del sonno: più che una associazione Riccardo Drigo
Transcript of BPCO e disturbi del sonno: più che una associazione · BPCO e disturbi del sonno: più che una...

BPCO e disturbi del sonno:
più che una associazione
Riccardo Drigo

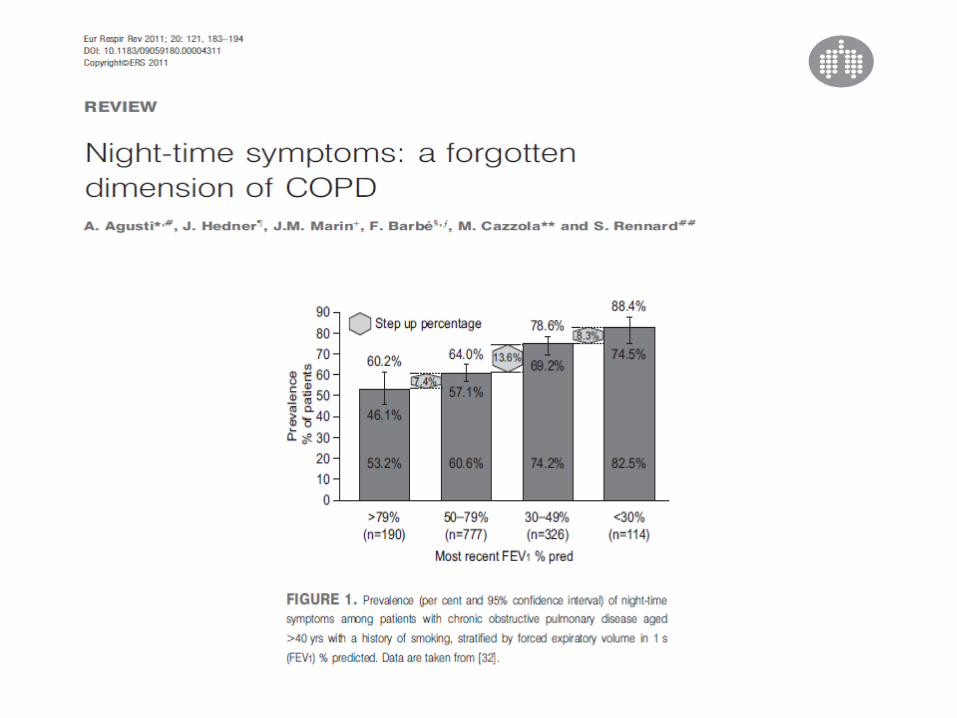
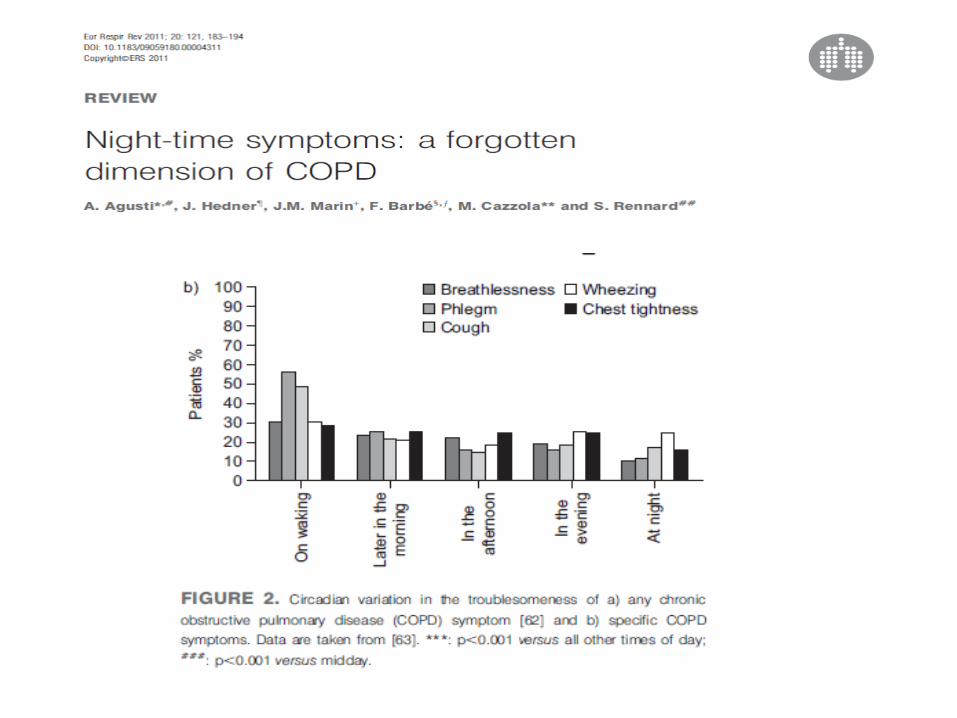
BPCO: quale impatto sul sonno
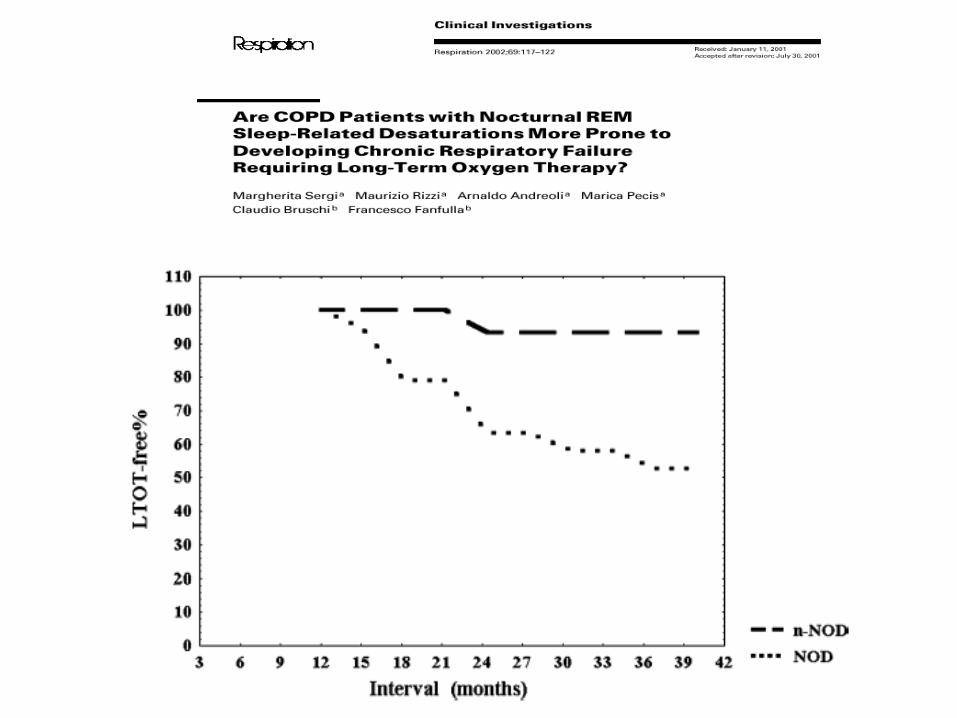
Sonno: quale impatto sulla BPCO
Overlap OSA e BPCO

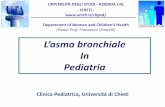
Demographic parameters Our cohort Normative population (Walsleben et al.) Number of subjects 106 197 Age (years) 66.4 + 7.3 55-69 Male (%) 67 33 BMI 25.1 + 5.1 Male 25.9 +2.5 Female 24.7 + 2.8 Sleep parameters %TST (Mean + SD) %TST (mean 10th;90th percentile) Stage 1 16.9 + 14.3 4.1 (1.5;6.9) Stage 2 54.7 + 16.8 55.1 (43.5;66.9) Stage ¾ 14.9 + 15.0 19.4 (6.8;30.5) Stage REM 12.7 + 8.3 21.4 (14.8;28.9) TST (min) 272.5 + 86.6 372 (306;450) Latency to persistent sleep (min) 36.8 + 33.9 19.4 (5.5;37.6) Sleep efficiency (%) 66 + 17 86 (77;95) Arousal index (n/h) 16.2 + 14.1 14.3 (7.5;23.3)
Sleep quality in chronic obstructive pulmonary disease David G. McSharry, Silke Ryan, Peter Calverley, J. Colin Edwaords, Walter T. McNicholas
Respirology, October 2012; 17 (7): 1119-1124




BPCO: quale impatto sul sonno
Sonno: quale impatto sulla BPCO
Overlap OSA e BPCO

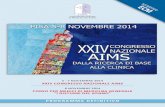
ALTERAZIONI FUNZIONALI NEL SONNO
NELLA BPCO
Perdita di tono dei
muscoli intercostali e dei
muscoli respiratori accessori
indotta dal sonno REM
Diminuzione di
sensibilità dei
chemorecettori
respiratori
Aumento delle
resistenze delle
alte e basse
vie aeree
Curva di
saturazione
ossiemoglobinica
Ipoventilazione
Squilibrio ventilo- perfusorio
INSUFFICIENZA RESPIRATORIA
Diminuzione
della capacità
funzionale
residua



Ore 22 Ore 6
SPO2 90%
veglia
SPO2 DURANTE IL SONNO NELLA BPCO NON
COMPLICATA DA OSA
Soggetto normale
REM REM REM REM

Ore 22 Ore 6
SPO2 90%
veglia
SPO2 DURANTE IL SONNO NELLA BPCO NON
COMPLICATA DA OSA
Soggetto normale
REM REM REM REM
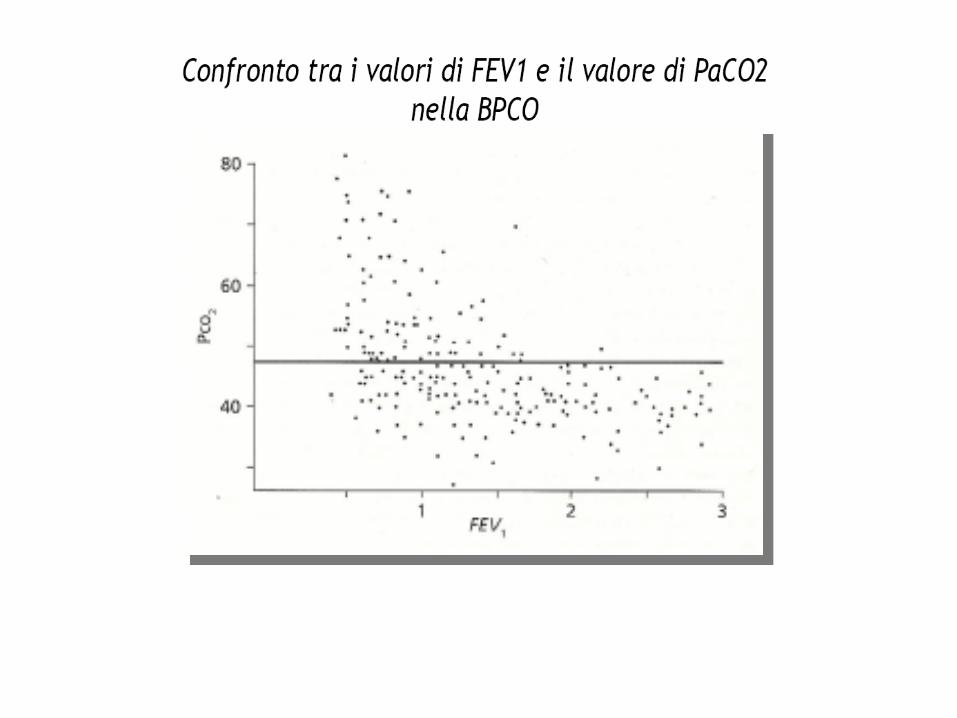
Prevedibile in base ai valori emogasanalitici di base
Non prevedibile in base ai valori emogasanalitici e
spirometrici di base


Linee guida italiane per l’ ossigenoterapia
domiciliare a lungo termine (aggiornamento 2004)
“sono necessari ulteriori studi prospettici che dimostrino il reale
beneficio dell’O2 terapia soprattutto in termini di sopravvivenza”
“e’ possibile prescrivere l’ossigenoterapia quando la SPO2 si
mantenga < 90 % per almeno il 30 % del tempo e se si dimostra
che l’O2 terapia a bassi flussi corregge l’ipossiemia”

BPCO e insonnia: qualche consiglio
di buon senso
• Evitare se possibile farmaci a lunga durata d’azione
• Preferire farmaci non BDZ (?)
• Non sospendere improvvisamente una BDZ in un paziente con BPCO stabile normocapnico
• Sospendere le BDZ negli ipercapnici acuti (?)
• Considerare altre categorie di farmaci (Trazodone, antidepressivi, agonisti della melatonina)
• Considerare terapie al bisogno

BPCO: quale impatto sul sonno
Sonno: quale impatto sulla BPCO
Overlap OSA e BPCO
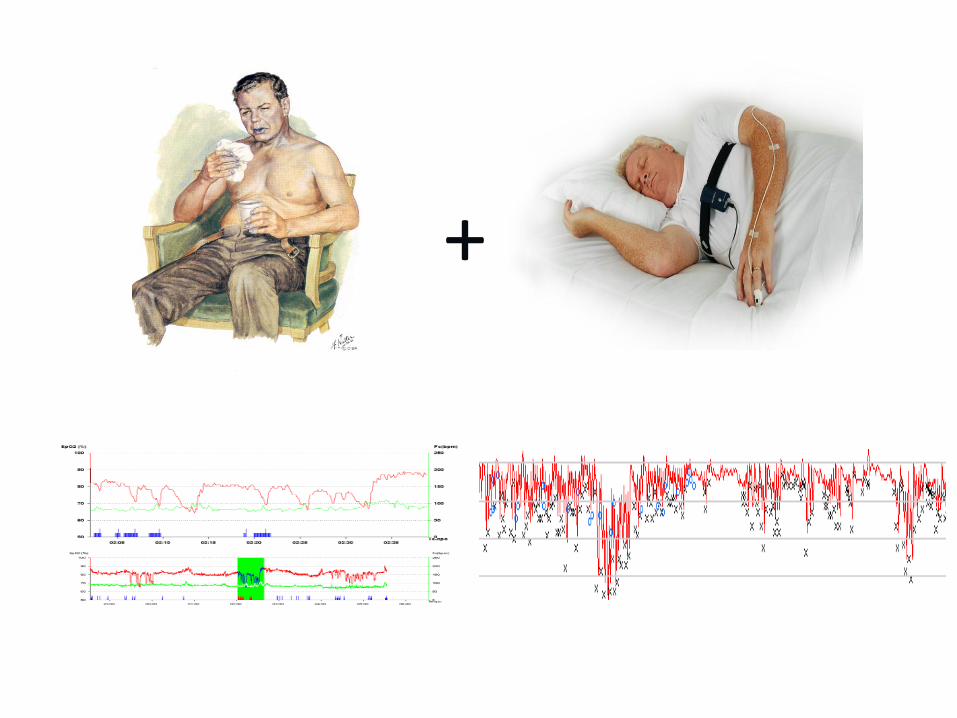
+ +

Association of chronic obstructive pulmonary disease and
obstructive sleep apnea consequences
Carlos Zamarron, Vanesa Garcia Paz, Emilio Morete and Felix del Campo Matias
Int J Chron Obstruct Pulmon Dis. 2008 December; 3(4): 671–682.

+ ipercapnia
+ ipossia
+ ipertensione polmonare
Fletcher EC et Al.: Long-term cardiopulmonary
sequelae in patients with sleep apnea and chronic
lung disease.
Am Rev Respir Dis 1987; 135:525-33
…in COPD patients who had concurrent OSA, the hemodynamic status was more severe than in patients with “pure” COPD with a similar degree of respiratory function impairment

osa + bpco solo osa solo bpco

Weitzenblun E et al. Proc AmThorac Soc 2008 ;5:237-248
PULMONARY HYPERTENSION

Health-related quality of life in patients with obstructive sleep apnoea and chronic obstructive pulmonary disease (overlap syndrome) C. Mermigkis1, A. Kopanakis2, N. Foldvary-Schaefer1, J. Golish1, V. Polychronopoulos2, S. Schiza3, A. Amfilochiou2, N. Siafakas3, D. Bouros4
The aim of this study was to determine the effect of OSA on quality of life (QOL) in patients with overlap syndrome (OVS). Thirty subjects with OVS and 15 control
subjects participated. The St George's Respiratory Questionnaire (SGRQ) was used to determine QOL. The control group included subjects with COPD and no
evidence of OSA by overnight polysomnography. All subjects were habitual snorers with normal Epworth Sleepiness Scale scores. Significant differences were found between the groups for the total score and each of the three components of the SGRQ suggesting worse QOL in OVS patients (symptoms 54.9 ± 18.9 vs. 38.2 ± 19.3, p = 0.008; activity 59.2 ± 16.2 vs. 44.4 ± 11.3, p = 0.003; impacts 35.2 ± 23 vs. 20.8 ± 8.7, p = 0.025 and total 45.7 ± 17.7 vs. 30.9 ± 8.7, p = 0.004 in OVS
patients and control group, respectively). Obstructive sleep apnoea has a major impact on QOL in patients with OVS and can exist in COPD patients with habitual snoring even in the absence of daytime sleepiness.
Int J Clin Pract 2007; 61 (2): 207-211






Am. J. Respir. Crit. Care Med. 2009; 180: 692-700
Chronic Obstructive Pulmonary Disease and Obstructive Sleep Apnea Overlaps in Pathophysiology, Systemic Inflammation, and Cardiovascular Disease Walter T. McNicholas

Indicazioni alla diagnostica strumentale
notturna nella BPCO
la polisonnografia è indicata nella BPCO:
• qualora coesistano sintomi di OSA
• qualora ipertensione polmonare, policitemia o
scompenso cardiaco dx siano presenti in un
paziente con PaO2 in veglia > 55 mmHg
American Thoracic Society, 1989



John William Waterhouse
Ipnos e Thanatos