A NARRATIVE MEDICINE PROJECT WITH PEOPLE LIVING ......
1
A NARRATIVE MEDICINE PROJECT WITH PEOPLE LIVING WITH A STOMA Antonini M. 1 , Botteselle E. 2 , Bullitta M. 3 , Caldarola D. 4 , Casoni L. 5 , Cilli D. 6 , Deledda MT. 7 , Eto L. 8 , Falco L. 9 , Ferruzzi A. 10 , Fiordispina G. 11 , Fodale C. 12 , Gaddoni E. 13 , Grassi M. 14 , Grezio M. 15 , Guerra E. 16 , Lungo P. 17 , Mazzotta L. 18 , Melis V. 19 , Palumbo G. 20 , Panarelli A. 21 , Pantano O. 22 , Sannicandro N. 23 , Sacchetti P. 24 , Tantulli Bartoli R. 25 , Tarantino A. 26 , Vivoli G. 27 . 1 USL Toscana Centro – Nuovo Ospedale San Giuseppe – Empoli; 2 °.O. Istituti Ospitalieri – Presidio di Cremona; 3 AOU Sassari; 4 Policlinico Universitario – Bari; 5 Azienda Ospedaliera di Reggio Emilia – Arcispedale Santa Maria Nuova; 6 AO San Giovanni Addolorata – Roma; 7 Ospedale SS Annunziata Sassari; 8 Istituto Nazionale Tumori Fondazione Pascale – Napoli; 9 ASL TO1 – Ospedale Martini - Torino; 10 Policlinico Universitario Campus Bio-Medico – Roma; 11 Ospedale Maria Vittoria – Torino; 12 AOU G. Martino – Messina; 13 AOU di Bologna - Policlinico Sant’Orsola-Malpighi – Bologna; 14 ASL TO2 – Ospedale San Giovanni Bosco - Torino; 15 AUSL Bologna – Ospedale Maggiore; 16 AO Spedali Civili di Brescia; 17 Ospedale Maggiore della Carità - Novara; 18 Poliambulatorio “Cittadella della Salute” Vito Fazzi” - Lecce; 19 A.O. Ospedali Riuniti di Bergamo – Ospedale Papa Giovanni XXIII; 18 I.C.P. E. Bassini – Cinisello; 21 Policlinico di Bari; 22 San Giovanni Battista “Molinette” – Torino; 23 AOU Ospedali Riuniti di Foggia; 24 San Filippo Neri – Roma; 25 Ospedale Santa Maria Annunziata – Bagno a Ripoli (FI); 26 I.E.O. Milano; 27 Azienda Ospedaliero-Universitaria Careggi – Firenze With support of DANSAC ITALY and ISTUD FOUNDATION KEY WORDS: NARRATIVE MEDICINE, OSTOMY INTRODUCTION Narrative medicine is what occurs between the health provider and the patient: from the collection of information of events before the occurrence of the disease, how the disease showed up, with attention to physical, psychological, social and ontological features. Attention is therefore to the Burden of Illness and to find the best way to personalize strategy of care. Greenhalgh and Hurtwitz of King’s College, BMJ , 1999: “Narrative based medicine in an evidence based world”. Among Disease, Illness and Sickness • DISEASE is the side of the mechanics, the performance and the causal effects of treatments bound primarily to the functionality of the "body" or even more of a “target organ”. Body as a “machine to be repaired” • ILLNESS concerns the conscious or unconscious perception that the subject has of the disease, how is the living with, thus transforming the patient from object of care to a human subject who feels and thinks and perceives the disease. Mind and Souls are embedded. • SICKNESS is the socially and culturally held conceptions of health conditions; these may influence how the patient reacts, as in the dread of cancer or the stigma of mental illness. The Others’ judgement. We have developed a project of Narrative Medicine with people living with a stoma, with the following aims: • Trace the pathway of care to understand the needs of the patients to hypothesize new services • Understand the emotional, social, relational impact of the ostomy • Draw the healthcare personnal’s profile • Understand the aspects of disease, of illness and sickness DISEASE: Professional perspective ILLNESS: First person perspective SICKNESS: Social perspective METHOD The narrative plot was created by the stoma therapy nurses with the support of ISTUD team. The Ostomy Centers involved in the research were 26. The goal was to collect the narratives of 100 adult patients. The patients involved were: • People who had the surgery at least 12 months before • People who wanted to tell their experience Three ways to gather the narratives: • The patients could bring back the narratives putting it in a box or in a closed envelope. • The patients could write in a specific online model www.medicinanarrativa.eu/diario-dna • The patients could write narratives in word file and send it by email RESULTS Between October and December 2015, we collected 151 narratives (50% above the expected number). In the narratives the encounter with the Surgeon it is a crucial event during the pathway of care. The ET nurse is the reference point for the patients. Degree/Master 14% High school graduatio n 43% Secondary school graduation 23% Primary school graduation 20% Educational qualification Degree/Master High school graduation Secondary school graduation Primary school graduation ENCOUNTERING THE SURGEON During the first meeting with the surgeon the person discovers: • That he/she will have a stoma surgery • The reason why he/she has to do this kind of surgery • In the majority of cases the patient discovers that he/she has a cancer and in many cases they don’t know if it is benign or malignant THE PROFILES OF SURGEON • The professional surgeon: gives information and psycological support to the patient • The technical surgeon: gives information in a technical way • The rushed surgeon: gives few information in a few minutes visit • Other case: emergency, there is no time to talk to the patient before the stoma surgery. Professional 29% Technical 30% Rushed 30% Emergency 11% Professional Technical Rushed Emergency ENCOUNTERING THE ET NURSE The stoma specialist nurse is the reference point for the patients, he/she deals with strengthening communication, calms and reassures the patient, opens up new possibilities for ostomy management, often he/she establishes a human relationship. In the majority of the narratives the good relationship with the nurse is emphasized. «Since the moment I have met the stoma therapy nurse mr. …, I felt reassured, because I received an answer for all my doubts» «I must admit that I didn’t feel ready from a psycological point of view to face this situation but, thanks to the support of the stoma therapy nurse I felt ready to face my new status with determination and serenity» “It‘s been nice because he is a very human person, understanding and calm. He gave me a lot of detailed information, and also a lot of confidence and calmness.” serene; 35%; 48% normal; 12%; 17% not good; 14%; 20% resignation; 11%; 15% serene normal not good resignation CONCLUSIONS • It has been the first Italian experience of Narrative Medicine with people from all regions who are living with a stoma. • The narrative plot has been evaluated by stoma therapy nurses as a useful tool to understand the soul, the organizational needs and the perception of the old/new identity of patients and their families. • The sharing of patients narratives can build up the dialogue among the different medical professionals as surgeons, stoma therapy nurses, nutritionists, psycologists, sexologists during the pathway of care . • The narrative plot used by the stoma therapy nurses in this project has turned into a diary that will be used by the stoma nurses in everyday clinical practice. FURTHER IDEAS • Engaging other countries in Narrative Medicine on people with stoma • Exploring the coping of living with temporary stoma vs the permanent stoma • Exploring the differences of living with ileo, colo, urostomy • Collecting narratives from healthcare professionals and caregivers • Focus on context of living with a permanent stoma FINDING AND ACTIONS Findings Actions The first encounter with the surgeon is a crucial event during which the diagnosis and the need of the ostomy are communicated The importance of the communication by the healthcare professionals, the use of the right words and the proper setting of the encounters that can help and foster the patient to cope. Time to cope with the stoma: The reaction to intestinal or urinary diversion surgery varies from one individual to the other. The importance of listening the needs and the feelings of the patients. Consider a physiological time of accommodation. The importance of the family, 62% would like to be assisted by a member of his/her a family Take care of the family/caregiver by the healthcare professionals: the ostomy has an impact not only on the patient but also on his/her family that are to help the patient to manage the stoma The stoma denial: • Patients don’t want information • Before the surgery patients don’t want or can’t imagine how the stoma will be • After the surgery the patients neither want to see the stoma nor manage it Give the opportunity to patients to share their own experience and meet people living with a stoma. Create awareness through press about stoma and living with since social information in Italy is totally lacking. REFERENCES 1. MacDonald, L. The Experience of Stigma: Living with Rectal Cancer. In: Anderson, P.; Bury, M., editors. Living with Chronic Illness: The Experience of Patients and Their Families. London: Unwin Hyman; 1988. p. 177-202. 2. Alexanderson K. Sickness absence: a review of performed studies with focus on levels of exposure and theories utilized. Scand J Soc Med 1998;26:241–9. 3. Charon R. Narrative Medicine. Honoring the stories of Illness”. Oxford University Press, Oxford 2006, p.3.
Transcript of A NARRATIVE MEDICINE PROJECT WITH PEOPLE LIVING ......

A NARRATIVE MEDICINE PROJECT WITH PEOPLE LIVING WITH A STOMAAntonini M.1, Botteselle E.2, Bullitta M.3, Caldarola D.4, Casoni L.5, Cilli D.6, Deledda MT.7, Eto L.8, Falco L.9, Ferruzzi A.10, Fiordispina G.11, Fodale C.12, Gaddoni E.13, Grassi M.14, Grezio M.15, Guerra E.16, Lungo P.17, Mazzotta L.18, Melis V.19, Palumbo G.20, Panarelli
A.21, Pantano O.22, Sannicandro N.23, Sacchetti P.24, Tantulli Bartoli R.25, Tarantino A.26, Vivoli G.27.
1USL Toscana Centro – Nuovo Ospedale San Giuseppe – Empoli; 2°.O. Istituti Ospitalieri – Presidio di Cremona; 3AOU Sassari; 4Policlinico Universitario – Bari; 5 Azienda Ospedaliera di Reggio Emilia – Arcispedale Santa Maria Nuova; 6AO San Giovanni Addolorata – Roma; 7Ospedale SS Annunziata Sassari; 8
Istituto Nazionale Tumori Fondazione Pascale – Napoli; 9ASL TO1 – Ospedale Martini - Torino; 10Policlinico Universitario Campus Bio-Medico – Roma; 11Ospedale Maria Vittoria – Torino; 12AOU G. Martino – Messina; 13 AOU di Bologna - Policlinico Sant’Orsola-Malpighi – Bologna; 14ASL TO2 – Ospedale San Giovanni Bosco - Torino; 15AUSL Bologna – Ospedale Maggiore; 16 AO Spedali Civili di Brescia; 17Ospedale Maggiore della Carità - Novara; 18Poliambulatorio “Cittadella della Salute” Vito Fazzi” - Lecce; 19A.O. Ospedali Riuniti di Bergamo – Ospedale Papa Giovanni XXIII; 18I.C.P. E. Bassini – Cinisello; 21Policlinico di Bari; 22San Giovanni Battista “Molinette” – Torino; 23AOU Ospedali Riuniti di Foggia; 24San Filippo Neri – Roma; 25Ospedale Santa Maria Annunziata – Bagno a Ripoli (FI); 26I.E.O. Milano; 27Azienda Ospedaliero-Universitaria Careggi – Firenze
With support of DANSAC ITALY and ISTUD FOUNDATION
KEY WORDS: NARRATIVE MEDICINE, OSTOMY
INTRODUCTION
Narrative medicine is what occurs between the health provider and the patient: from the collection of information of events before the occurrence of the disease, how the disease showed up, with attention to physical, psychological, social and ontological features. Attention is therefore to the Burden of Illness and to find the best way to personalize strategy of care. Greenhalgh and Hurtwitz of King’s College, BMJ , 1999: “Narrative based medicine in an evidence based world”.
Among Disease, Illness and Sickness
• DISEASE is the side of the mechanics, the performance and the causal effects of treatments bound primarily to the functionality of the "body" or even more of a “target organ”. Body as a “machine to be repaired”
• ILLNESS concerns the conscious or unconscious perception that the subject has of the disease, how is the living with, thus transforming the patient from object of care to a human subject who feels and thinks and perceives the disease. Mind and Souls are embedded.
• SICKNESS is the socially and culturally held conceptions of health conditions; these may influence how the patient reacts, as in the dread of cancer or the stigma of mental illness. The Others’ judgement.
We have developed a project of Narrative Medicine with people living with a stoma, with the following aims:• Trace the pathway of care to understand the needs of the patients to hypothesize new services • Understand the emotional, social, relational impact of the ostomy• Draw the healthcare personnal’s profile• Understand the aspects of disease, of illness and sickness
DISEASE: Professional perspective
ILLNESS: First person
perspective
SICKNESS: Social perspective
METHOD
The narrative plot was created by the stoma therapy nurses with the support of ISTUD team.
The Ostomy Centers involved in the research were 26.
The goal was to collect the narratives of 100 adult patients.
The patients involved were:• People who had the surgery at least 12 months before• People who wanted to tell their experience
Three ways to gather the narratives:• The patients could bring back the narratives putting it in a box or in a closed envelope.• The patients could write in a specific online model www.medicinanarrativa.eu/diario-dna• The patients could write narratives in word file and send it by email
RESULTS
Between October and December 2015, we collected 151 narratives (50% above the expected number).
In the narratives the encounter with the Surgeon it is a crucial eventduring the pathway of care. The ET nurse is the reference point for the patients.
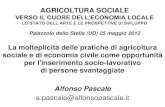
Degree/Master14%
High school
graduation
43%
Secondary school
graduation23%
Primary school graduation
20%
Educational qualification
Degree/Master High school graduation
Secondary school graduation Primary school graduation
ENCOUNTERING THE SURGEON
During the first meeting with the surgeon the person discovers:• That he/she will have a stoma surgery• The reason why he/she has to do this kind of surgery• In the majority of cases the patient discovers that he/she has a cancer and in many
cases they don’t know if it is benign or malignant
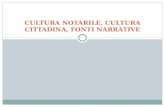
THE PROFILES OF SURGEON
• The professional surgeon: gives information and psycological support to the patient• The technical surgeon: gives information in a technical way• The rushed surgeon: gives few information in a few minutes visit• Other case: emergency, there is no time to talk to the patient before the stoma
surgery.
Professional29%
Technical30%
Rushed30%
Emergency11%
Professional
Technical
Rushed
Emergency
ENCOUNTERING THE ET NURSE
The stoma specialist nurse is the reference point for the patients, he/she deals with strengthening communication, calms and reassures the patient, opens up new possibilities for ostomy management, often he/she establishes a human relationship.
In the majority of the narratives the good relationship with the nurse is emphasized.
«Since the moment I have met the stoma therapy nurse mr. …, I felt reassured, because I received an answer for all my doubts»
«I must admit that I didn’t feel ready from a psycological point of view to face thissituation but, thanks to the support of the stoma therapy nurse I felt ready to face my new
status with determination and serenity»
“It‘s been nice because he is a very human person, understanding and calm. He gave me a lot of detailed information, and also a lot of confidence and calmness.”
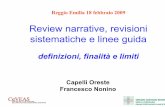
serene; 35%; 48%
normal; 12%; 17%
not good; 14%; 20%
resignation; 11%; 15%
serene
normal
not good
resignation
CONCLUSIONS
• It has been the first Italian experience of Narrative Medicine with people from all regions who are living with a stoma.• The narrative plot has been evaluated by stoma therapy nurses as a useful tool to understand the soul, the organizational needs and the perception of
the old/new identity of patients and their families.• The sharing of patients narratives can build up the dialogue among the different medical professionals as surgeons, stoma therapy nurses, nutritionists,
psycologists, sexologists during the pathway of care .• The narrative plot used by the stoma therapy nurses in this project has turned into a diary that will be used by the stoma nurses in everyday clinical
practice.
FURTHER IDEAS• Engaging other countries in Narrative Medicine on people with stoma• Exploring the coping of living with temporary stoma vs the permanent stoma• Exploring the differences of living with ileo, colo, urostomy• Collecting narratives from healthcare professionals and caregivers• Focus on context of living with a permanent stoma
FINDING AND ACTIONS
Findings Actions
The first encounter with the surgeon is a crucial eventduring which the diagnosis and the need of the ostomy are communicated
The importance of the communication by the healthcare professionals, the use of the right wordsand the proper setting of the encounters that can help and foster the patient to cope.
Time to cope with the stoma: The reaction to intestinal or urinary diversion surgery varies from one individual to the other.
The importance of listening the needs and the feelings of the patients. Consider a physiological time of accommodation.
The importance of the family, 62% would like to be assisted by a member of his/her a family
Take care of the family/caregiver by the healthcareprofessionals: the ostomy has an impact not only on the patient but also on his/her family that are to help the patient to manage the stoma
The stoma denial:• Patients don’t want information• Before the surgery patients don’t want or can’t
imagine how the stoma will be• After the surgery the patients neither want to
see the stoma nor manage it
Give the opportunity to patients to share their ownexperience and meet people living with a stoma. Create awareness through press about stoma and living with since social information in Italy is totallylacking.
REFERENCES
1. MacDonald, L. The Experience of Stigma: Living with Rectal Cancer. In: Anderson, P.; Bury, M., editors. Living with Chronic Illness: The Experience of Patients and Their Families. London: Unwin Hyman; 1988. p. 177-202.
2. Alexanderson K. Sickness absence: a review of performed studies with focus on levels of exposure and theories utilized. Scand J Soc Med 1998;26:241–9.3. Charon R. Narrative Medicine. Honoring the stories of Illness”. Oxford University Press, Oxford 2006, p.3.