






Le lingue
Pagine
Legale


Strategie diagnostiche ed impiego delle risorse
nel mondo reale
Andrea Rubboli
Unità Operativa di Cardiologia
Ospedale Maggiore
Bologna
Evento Formativo ANMCO
14 dicembre 2006
Bologna

Erogazione media della gestione raccomandata
54.9% (IC 95% 54.3-55.5)
(N Engl J Med 2003; 348: 2635-2645)

Physician-related
Lack of awareness/familiarity with guidelines Lack of agreement with guidelines Negative attitudes to guidelines Pressure of time Forgetfulness Perceived lack of support from peers Lack of confidence in performing procedure Lack of outcome expectancy Inertia of previous practice
Guideline-related
Evidence insufficiently strong Difficult to understand/inconvenient Inconsistent
Environmental
Inappropriate skill mix/lack of staff Lack of forcing strategies Lack of reminder system Increased costs Patient preferences
Ostacoli all’attuazione delle linee guida
(modificata da Caprini JA et al, Manag Care 2006; 15: 49-66)

Nell’Embolia Polmonare Acuta:
quadro clinico proteiforme
coinvolgimento di numerose e differenti
professionalità
necessità di tecnologia sofisticata
numerosità/ridondanza delle linee guida

Anno Società Scientifica Rivista
1999 American Thoracic Society Am J Respir Crit Care Med160: 1043-1066
2000 European Society of Cardiology Eur Heart J21: 1301-1336
2001 ANMCO-SIC Ital Heart J Suppl2: 1342-1356
2003 American Collegeof Emergency Physicians
Ann Emerg Med 200341: 257-270
2003 British Thoracic Society Thorax 58: 470-484
2004 Spanish Society of Pulmonologyand Thoracic Surgery
Arch Bronconeumol 40: 580-594
Linee Guida recenti per la diagnosi ed il trattamento
dell’Embolia Polmonare Acuta

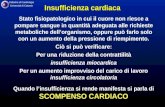
82,9
0,6
7,94,4 3,2
63,5
22,8
4,82,1
6,8
0
20
40
60
80
100
RVQ RVQ-SOD RVQ-PAG RVQ-CVG Other
Test sequences
(%)
1988 1991
Changing Practice Patterns in the Workup of Pulmonary EmbolismClaudia I. Henshke, MD, PhD; Ion Mateescu, BS; and David F. Yankelevitz, MD
(Chest 1995; 107: 940-945)
RVQ: scintigrafia polmonare
SOD: Ecodoppler AAII
PAG: angiopneumografia
CVG: flebografia

(Ital Heart J 2000; 1: 585-594)
Autore Tipo studio Centri partecipanti Durata studio Numero pz.
Ferrari E et al.(1997)
Registro prospettico 16 centri francesi 30 mesi 387
Kasper W et al.(1997)
Registro prospettico 204 centri tedeschi 16 mesi 1001
Rubboli A et al. (1998)
Analisi retrospettiva Ospedale Maggiore, Bologna
24 mesi 127
Goldhaber SZ et al. (1999)
Registro prospettico 52 centri europei e nordamericani
22 mesi 2454
Roncon L et al.(1999)
Registro prospettico 191 Unità Operative nella Regione Veneto
12 mesi 880
Saro et al.(1999)
Analisi retrospettiva Ospedale Valdecilla, Santander
24 mesi 251
Burkill GJ et al.(1999)
Inchiesta mediante questionario
327 centri nel Regno Unito e EIRE
-- --

(Rubboli A & Euler DE, Ital Heart J 2000; 1: 585-594)

“There is no doubt that CT pulmonary
angiography should now be considered the
central imaging investigation in suspected
pulmonary embolism”
(Miller AC & Boldy DAR, Thorax 2003; 58: 463)

Diagnosis of pulmonary embolism: a cost-effectiveness analysis
(Doyle NM et al, Am J Obst Gynecol 2004; 191: 1019-1023)
ECOGRAFIA VENOSA AAII
200 $
SCINTIGRAFIA POLMONARE V/Q
400 $
ANGIO TC
500 $
se + anticoagulazione se + anticoagulazione se – test aggiuntivo (V/Q o angio TC)
se alta probabilità anticoagulazione se bassa probabilità no anticoagulazione se intermedia probabilità test aggiuntivo
(angio TC o angiopneumografia)
Indagine di imaging iniziale
Costo per vita salvata
24.004 $ 35.906 $ 17.208 $

CT Pulmonary Angiography is the First-Line
Imaging Test for Acute Pulmonary Embolism:
A Survey of US Clinicians
Clifford R. Weiss, MD, John C. Scatarige, MD, Gregory B. Diette, MD, MHS, Edward F. Haponik, MDBarry Merriman, MD, Elliott K. Fishman, MD
Russell H. Morgan Department of Radiology and Radiological Sciences, and Department of Medicine, Division of Pulmonary and Critical Care Medicine
The Johns Hopkins University School of Medicine, Baltimore, MD
(Acad Radiol 2006; 13: 434-446)
86,7
8,3
0,0 2,5 0,00
20
40
60
80
100
CTPA V-P US PA Other
Imaging Test
71,4
19,7
5,81,7 1,0
0
20
40
60
80
100
CTPA V-P US PA Other
Imaging Test
Most useful imaging test First imaging test ordered

Question Percent
Severity of illness 87.5%
Pre-test clinical probability of PE 84.6%
Degree to which a test is validated in the literature 82.5%
How soon the results will be available 72.1%
Risk of adverse reaction during the test 53.8%
Confidence in interpreting physician 52.9%
Additional information, not related to PE, that the test may provide 49.2%
Degree of resistance received from imaging facility or personnel 16.3%
Time of day/day of week 14.2%
Examination covered by insurance 7.9%
Radiation dose to patient 6.7%
Importance of selected factors when ordering a first imaging test
(Clifford RW et al, Acad Radiol 2006; 13: 434-446)

Casistica Ospedale Maggiore - BolognaAnno 2004
Analisi retrospettiva codice di dimissione 415.1
68 pazienti: M/F 33/35; età media: 72.5 14 anni; range 28-97
Totale: 166 indagini di imaging (2.5/paziente)
0
10
20
30
40
50
60
Angio TC Scintigrafia EcodoppAAI I Ecocardio
1° indagine 2° indagine 3° indagine 4° indagine

0 5 10 15 20 25 30 35
EcodopplerAAII
Scintigrafia
Angio TC
NO indagini aggiuntive SI indagini aggiuntive
9%
27%
75%
Indagini aggiuntive dopo 1° test diagnostico
Casistica Ospedale Maggiore - Bologna, Anno 2004

Present diagnostic strategies for acute pulmonary thromboembolism; results of a
questionnaire in a restrospective trial conducted by the Respiratory Nuclear Medicine
Working Group of the Japanese Society of Nuclear Medicine
(Kawamoto M et al, Ann Nucl Med 2002; 8: 549-555)
9%
43%
25%
23%
agree undetermined disagree no opinion
Question # 6.
In the situation in which V/P lung scintigraphy is
performed as the 1st method for evaluating
pulmonary thromboembolism, and the results
suggest pulmonary thromboembolism we do not
perform further examinations

Strategie per incrementare l’aderenza alle linee guida
1. Raise awareness of acute PE in own practice
2. Create initiatives to improve knowledge of
management processes
3. Implement a process to facilitate and simplify
ordering
4. Incorporate a feedback process to assess impact
of changes and detect improvements in clinical
practice and outcomes
local audit
CME
ordering and monitoring charts
audit and feedback,linking back to stage 1
(modificata da Caprini JA et al, Manag Care 2006; 15: 49-66)

Ecodoppler AAII
D-dimero
Angiografia
Angio-TC
Ecocardiogramma
Troponine, BNP
ECG, Rx Torace, EGA
Scintigrafia
Relazione fra costo e informatività delle varie
indagini diagnostiche
Costo
Informazioni


Symtom Klyniska fynd Riskfaktorer
EKG Blodgas
Instabil Hemodynamik Stabil hemodynamik Lungröntgen
Ekokardiografi hjärt-ljungsjd ej hjärt-ljungsjd
högerkammarsvikt neg Spiral CT Lungscint (Spiral CT)
TROMBOLYS Spiral CT pos neg hög intermediär låg normal
pos neg HEPARIN HEPARIN STOPP
Spiral CT
hjärt-ljungsjd ej hjärt-ljungsjd stark svag-måttlig Angio
klin misstanke (Spiral CT,
Angio Sök alternativ diag Ultraljud ben bilat)
(ultraljud ben bilat) Angio neg pos
(Ultraljud ben bilat) Ultraljud ben bilat HEPARIN
pos neg
(Lapidus L, et al. 1997) HEPARIN STOPP

(Rubboli A & Euler DE, Ital Heart J 2000; 1: 585-594)
Top Related