Vantaggi e limiti della terapia di rivascolarizzazione...
49
1 Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial Appropriatezza in terapia della cardiopatia ischemica cronica TIGULLIO CARDIOLOGIA 2010 Walter Pitscheider – Cardiologia BOLZANO
Transcript of Vantaggi e limiti della terapia di rivascolarizzazione...
1
Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial
Appropriatezza in terapia della cardiopatia ischemica cronicaTIGULLIO CARDIOLOGIA 2010
Walter Pitscheider – Cardiologia BOLZANO
2
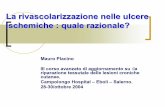
Appropriatezza in terapia della cardiopatia ischemica cronica2004 U.S.A. - Circa un milione di procedure di PCI
• 85% delle procedure in pazienti con “STABLE CAD”
– The New York State Angioplasty Registry -Feldman DN Am J Cardiol 2006;98:1334-9
• 58% delle procedure in pazienti con “STABLE CAD”
– American College of Cardiology National CV Data Registry. Durham, NC: Duke Clinical Research Institute, 2009.
• In quali casi è teoricamente giustificata la rivascolarizzazione ?
• In quanti di questi casi i rischi ed i costi sono compensati dai benefici ?
Rosamond W, et al. Heart disease and stroke statistics — 2007 update: a report from the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Circulation 2007;115(5) :e69-e171.
3
PCI on top of the Medical Tx in non acute CAD - Metanalisi
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
4
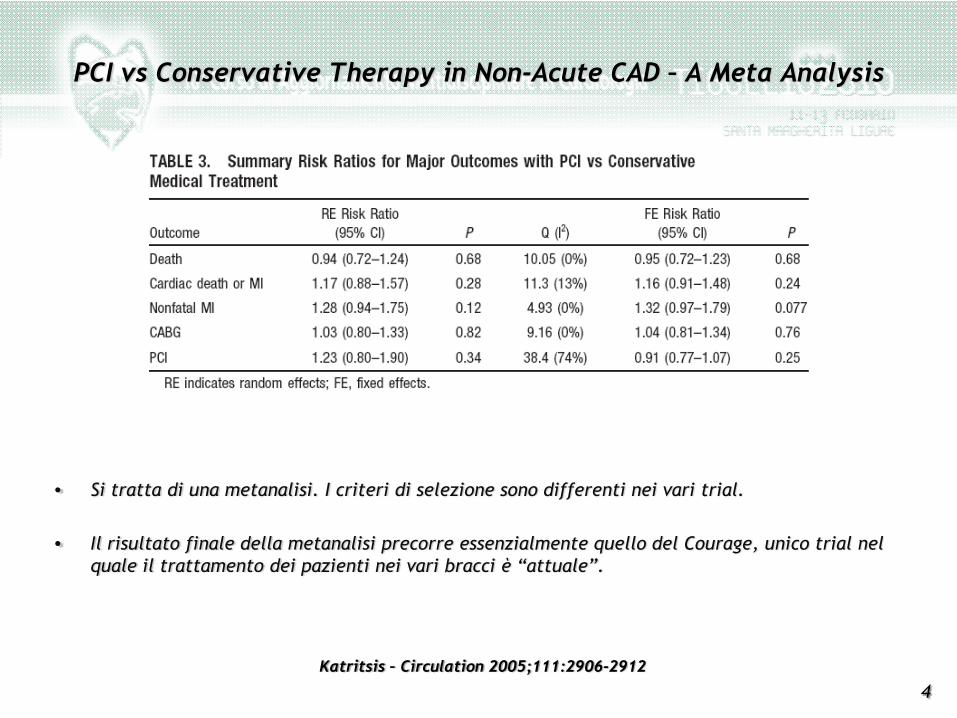
PCI vs Conservative Therapy in Non-Acute CAD – A Meta Analysis
• Si tratta di una metanalisi. I criteri di selezione sono differenti nei vari trial.
• Il risultato finale della metanalisi precorre essenzialmente quello del Courage, unico trial nel quale il trattamento dei pazienti nei vari bracci è “attuale”.
Katritsis – Circulation 2005;111:2906-2912
5
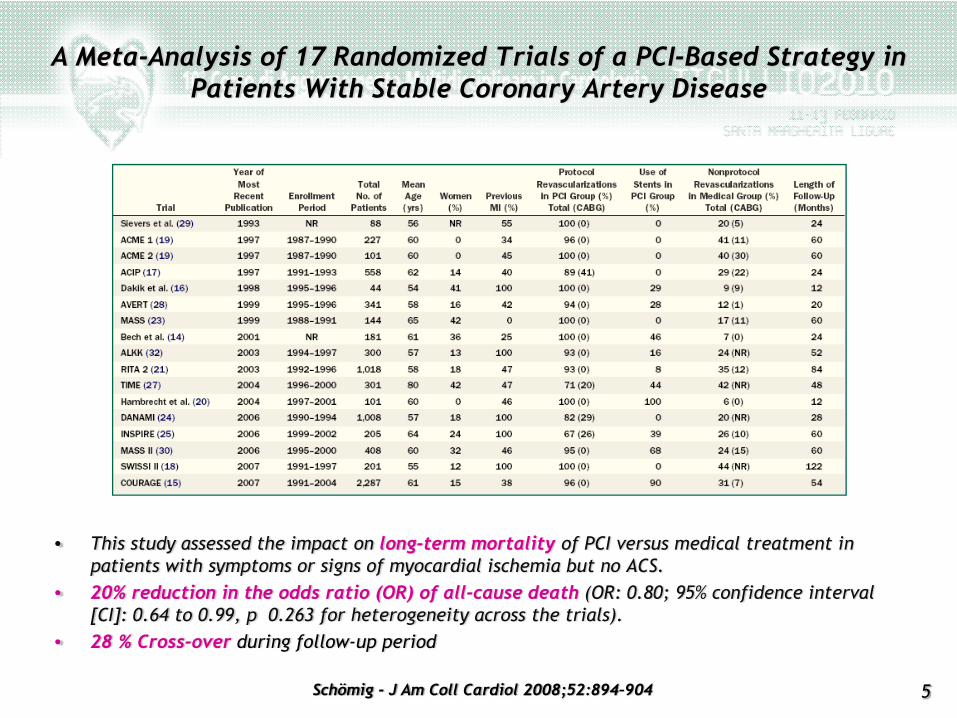
A Meta-Analysis of 17 Randomized Trials of a PCI-Based Strategy in Patients With Stable Coronary Artery Disease
• This study assessed the impact on long-term mortality of PCI versus medical treatment in patients with symptoms or signs of myocardial ischemia but no ACS.
• 20% reduction in the odds ratio (OR) of all-cause death (OR: 0.80; 95% confidence interval [CI]: 0.64 to 0.99, p 0.263 for heterogeneity across the trials).
• 28 % Cross-over during follow-up period
Schömig - J Am Coll Cardiol 2008;52:894–904
6
• CRITICA– I trial della metanalisi (ad eccezione del Courage) riguardano un periodo di oltre 17 anni :
nella maggior parte dei casi la terapia medica non è attuale - Zadeh JACC 2009;53:526
• REPLICA– Non si tratta di un confronto testa a testa fra terapia medica e PCI. – Nessun singolo trial ha dimensioni sufficienti per il target di mortalità. Questa è l’unica
metanalisi in grado di rispondere al questa domanda - Schömig JACC 2009;53:529
• Ordine di grandezza della riduzione di “Mortality Odds Ratio”– 20 % per la PCI nella stable CAD (Schoemig)– 16 % per le Statine (WILT – Arch Intern Med 2004)– 23 % per i Betabloccanti (Freemantle - BMJ 1999)
A Meta-Analysis of 17 Randomized Trials of a PCI-Based Strategy in Patients With Stable Coronary Artery Disease
7
COURAGE TRIAL
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
8
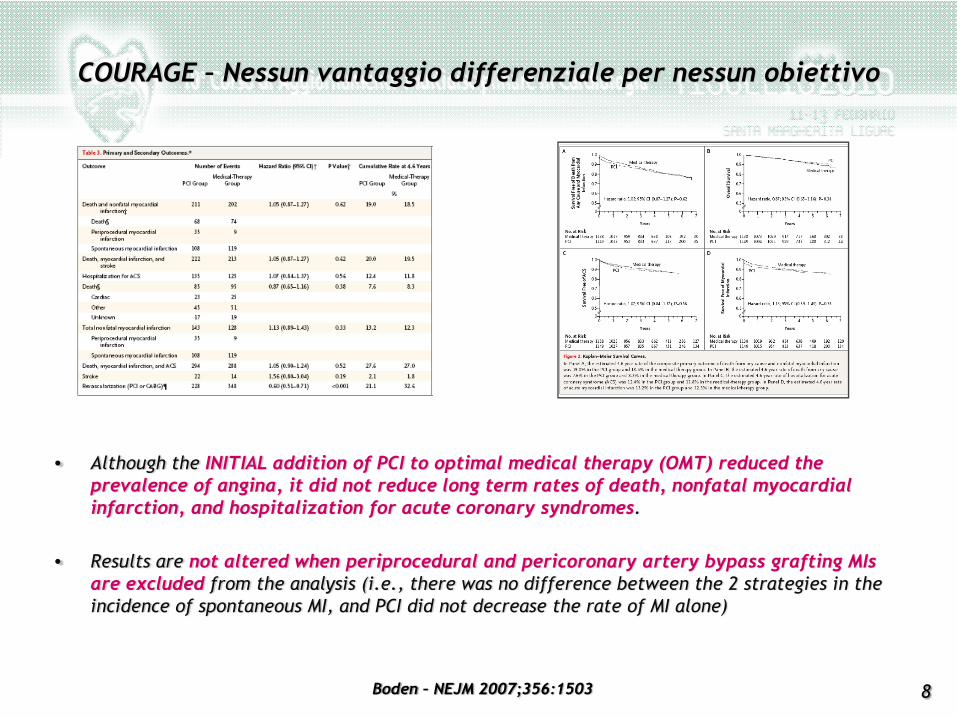
COURAGE – Nessun vantaggio differenziale per nessun obiettivo
Boden – NEJM 2007;356:1503
• Although the INITIAL addition of PCI to optimal medical therapy (OMT) reduced the prevalence of angina, it did not reduce long term rates of death, nonfatal myocardial infarction, and hospitalization for acute coronary syndromes.
• Results are not altered when periprocedural and pericoronary artery bypass grafting MIs are excluded from the analysis (i.e., there was no difference between the 2 strategies in the incidence of spontaneous MI, and PCI did not decrease the rate of MI alone)
9
• ENTRY CRITERIA– Stenosis of at least 70% in at least one proximal epicardial coronary artery and objective
evidence of myocardial ischemia or at least one coronary stenosis of at least 80% and classic angina without provocative testing.
• EXCLUSION CRITERIA– Persistent CCS class IV angina– Markedly positive stress test– Refractory CHF or Cardiogenic Shock– EF < 30%– Revasc. within the previous 6 months– Coronary anatomy not suitable for PCI.
• HIGH SELECTED POPULATION– > 90% of the pts excluded– EF = 60.8 ± 11.2 %
Clinical Outcomes Utilizing Revascularization and AggressiveDruG Evaluation (COURAGE) Trial
Boden – NEJM 2007;356:1503
10
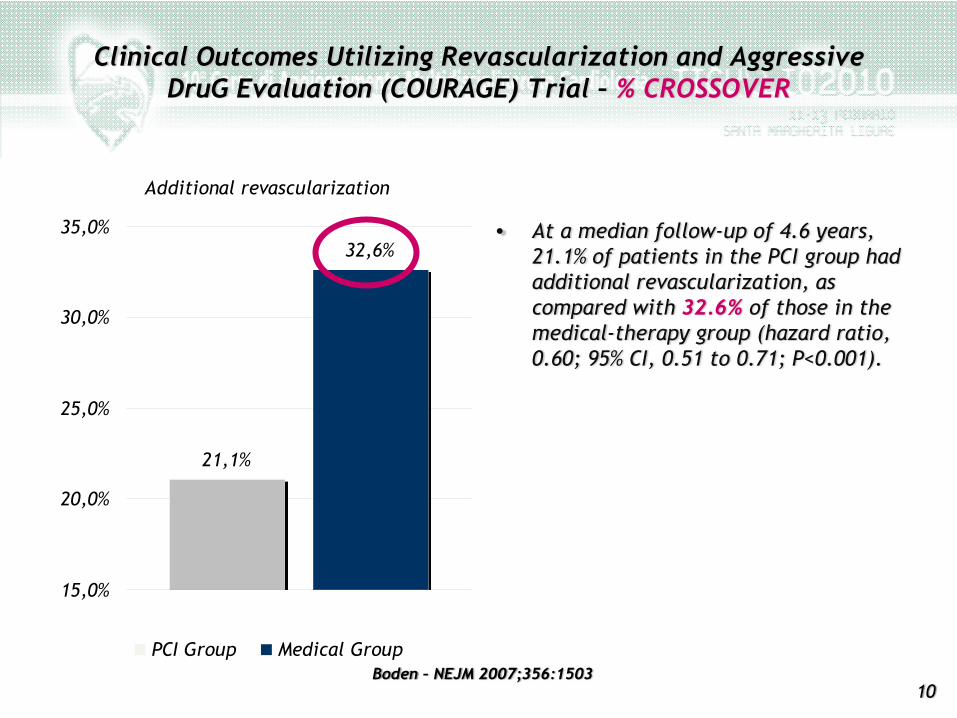
Additional revascularization
21,1%
32,6%
15,0%
20,0%
25,0%
30,0%
35,0%
PCI Group Medical Group
• At a median follow-up of 4.6 years, 21.1% of patients in the PCI group had additional revascularization, as compared with 32.6% of those in the medical-therapy group (hazard ratio, 0.60; 95% CI, 0.51 to 0.71; P<0.001).
Clinical Outcomes Utilizing Revascularization and AggressiveDruG Evaluation (COURAGE) Trial – % CROSSOVER
Boden – NEJM 2007;356:1503
11
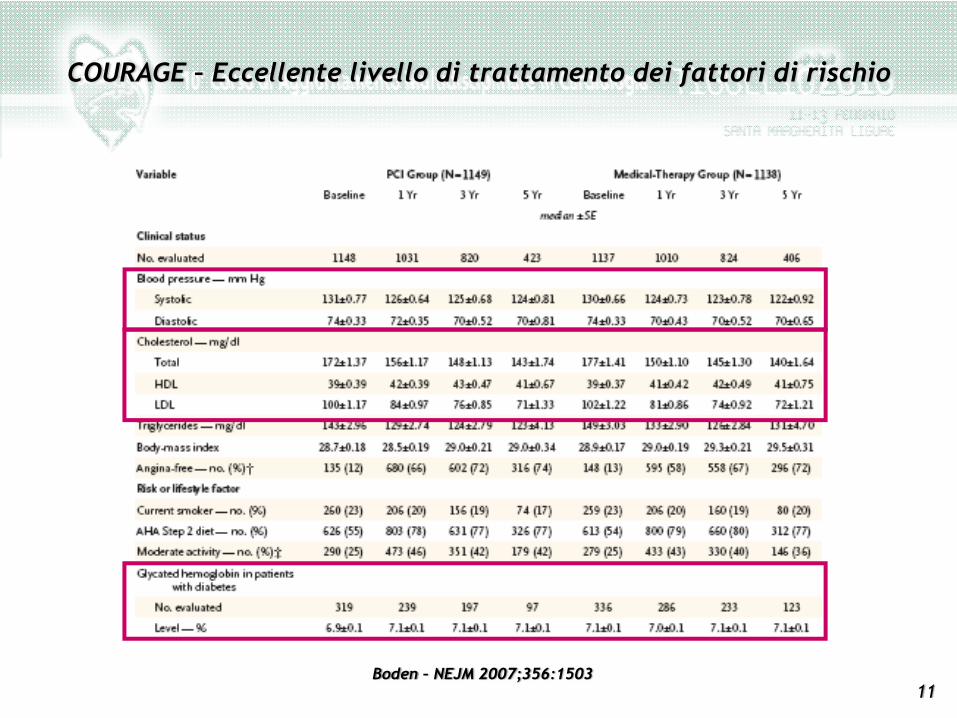
COURAGE – Eccellente livello di trattamento dei fattori di rischio
Boden – NEJM 2007;356:1503
12
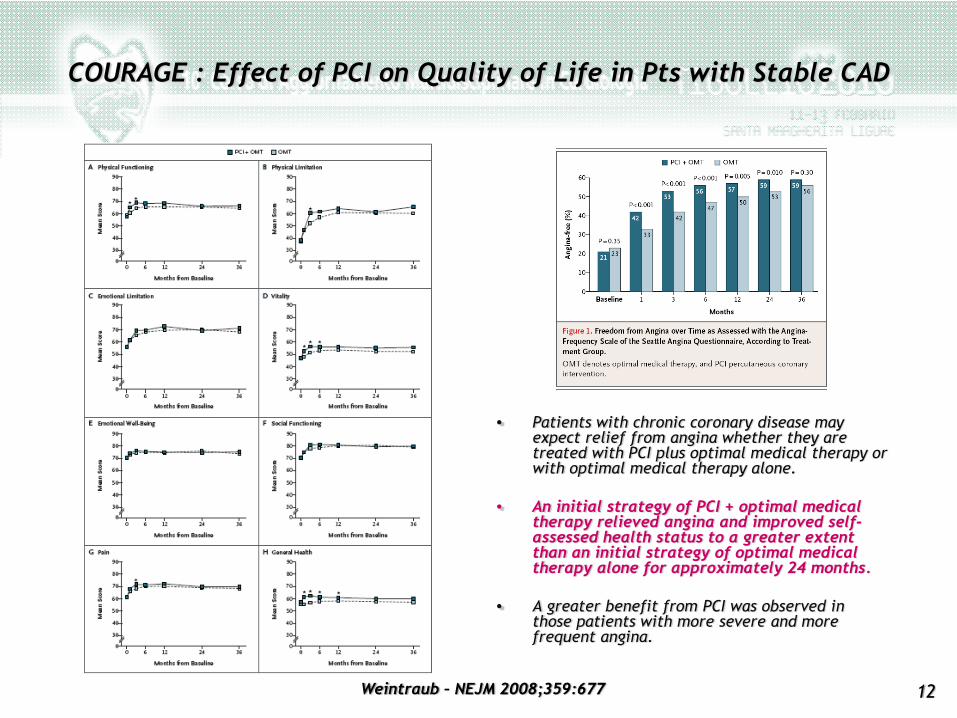
COURAGE : Effect of PCI on Quality of Life in Pts with Stable CAD
• Patients with chronic coronary disease may expect relief from angina whether they are treated with PCI plus optimal medical therapy or with optimal medical therapy alone.
• An initial strategy of PCI + optimal medical therapy relieved angina and improved self-assessed health status to a greater extent than an initial strategy of optimal medical therapy alone for approximately 24 months.
• A greater benefit from PCI was observed in those patients with more severe and more frequent angina.
Weintraub – NEJM 2008;359:677
13
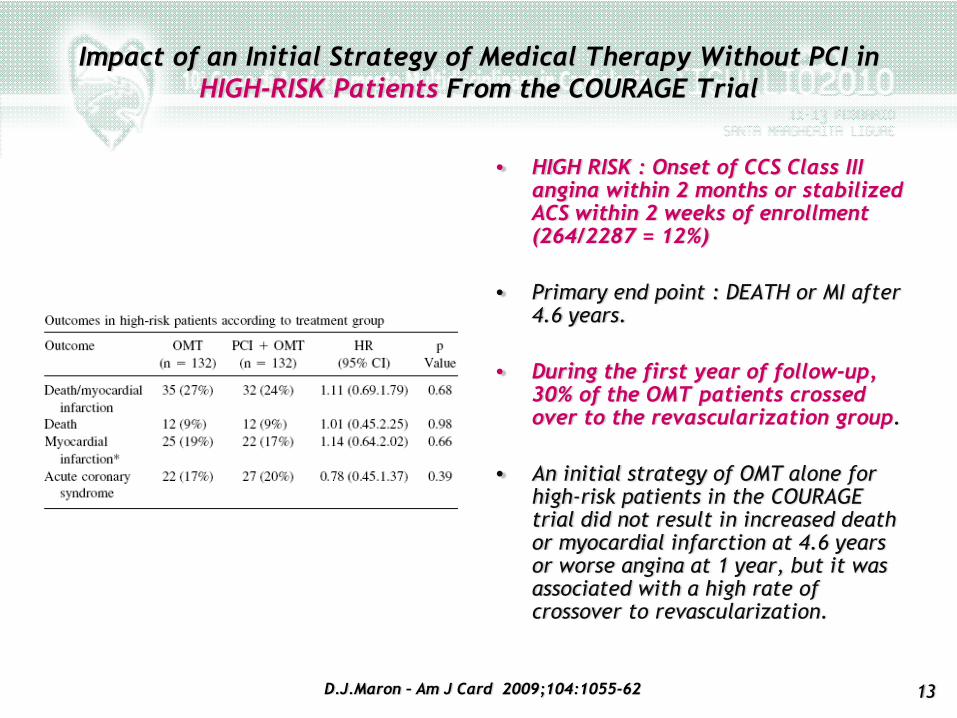
• HIGH RISK : Onset of CCS Class III angina within 2 months or stabilized ACS within 2 weeks of enrollment (264/2287 = 12%)
• Primary end point : DEATH or MI after 4.6 years.
• During the first year of follow-up, 30% of the OMT patients crossed over to the revascularization group.
• An initial strategy of OMT alone for high-risk patients in the COURAGE trial did not result in increased death or myocardial infarction at 4.6 years or worse angina at 1 year, but it was associated with a high rate of crossover to revascularization.
Impact of an Initial Strategy of Medical Therapy Without PCI inHIGH-RISK Patients From the COURAGE Trial
D.J.Maron – Am J Card 2009;104:1055-62
14
Inutile, e spesso dannoso, trattare le lesioni angiograficamente critiche, ma non ischemizzantiDEFER , FAME
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
15
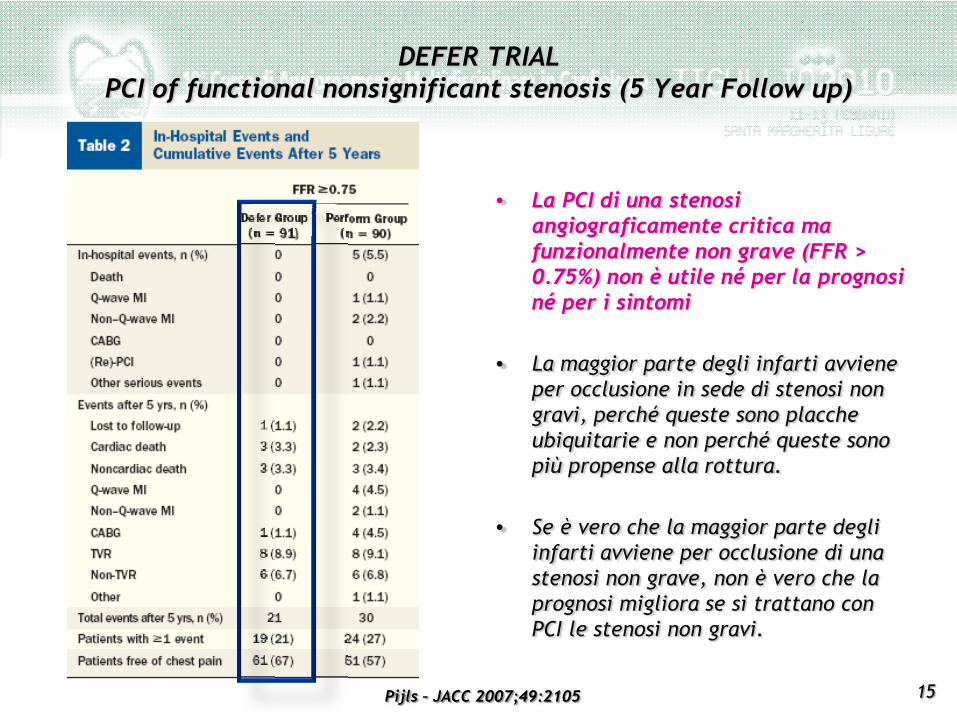
• La PCI di una stenosi angiograficamente critica ma funzionalmente non grave (FFR > 0.75%) non è utile né per la prognosi né per i sintomi
• La maggior parte degli infarti avviene per occlusione in sede di stenosi non gravi, perché queste sono placche ubiquitarie e non perché queste sono più propense alla rottura.
• Se è vero che la maggior parte degli infarti avviene per occlusione di una stenosi non grave, non è vero che la prognosi migliora se si trattano con PCI le stenosi non gravi.
DEFER TRIALPCI of functional nonsignificant stenosis (5 Year Follow up)
Pijls – JACC 2007;49:2105
16
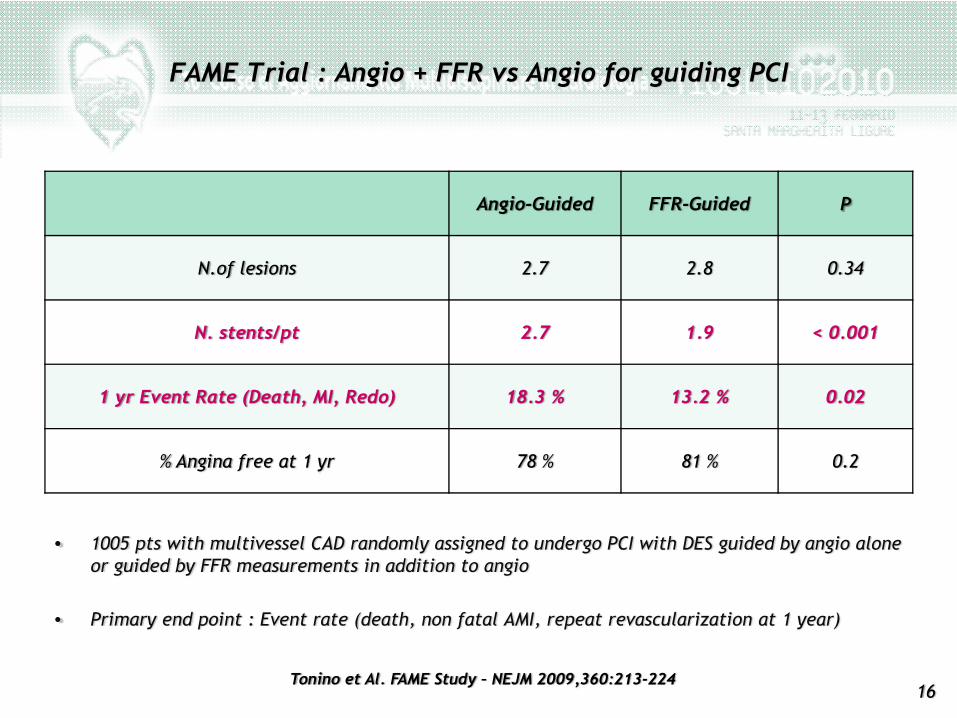
FAME Trial : Angio + FFR vs Angio for guiding PCI
Angio-Guided FFR-Guided P
N.of lesions 2.7 2.8 0.34
N. stents/pt 2.7 1.9 < 0.001
1 yr Event Rate (Death, MI, Redo) 18.3 % 13.2 % 0.02
% Angina free at 1 yr 78 % 81 % 0.2
• 1005 pts with multivessel CAD randomly assigned to undergo PCI with DES guided by angio alone or guided by FFR measurements in addition to angio
• Primary end point : Event rate (death, non fatal AMI, repeat revascularization at 1 year)
Tonino et Al. FAME Study – NEJM 2009,360:213-224
17
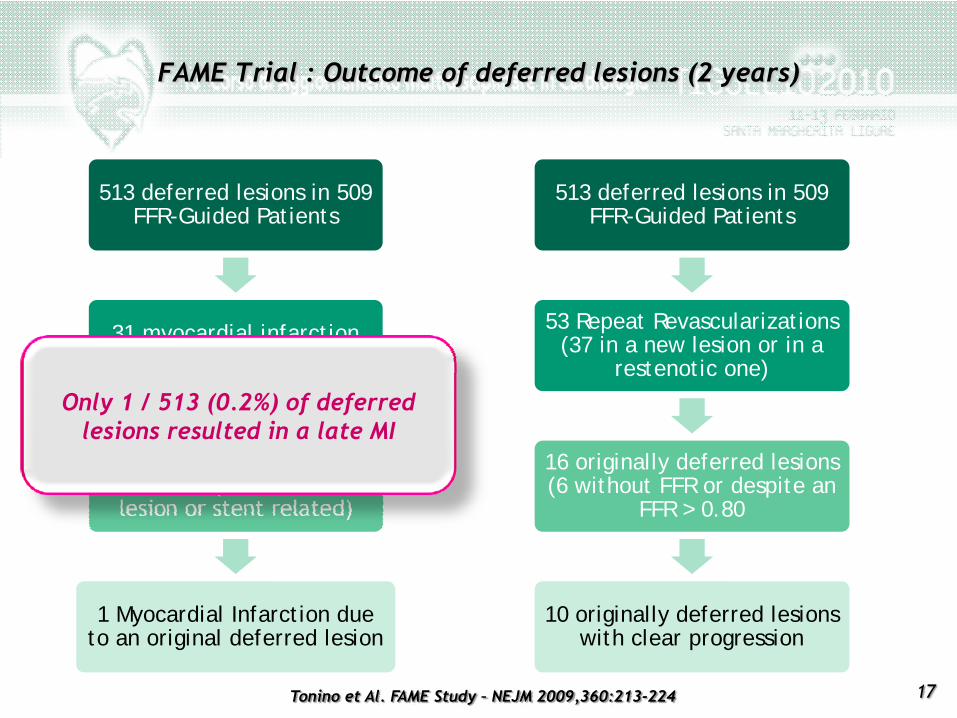
FAME Trial : Outcome of deferred lesions (2 years)
513 deferred lesions in 509 FFR-Guided Patients
31 myocardial infarction(22 periprocedural)
9 late myocardialinfarctions (8 due to a new
lesion or stent related)
1 Myocardial Infarction due to an original deferred lesion
513 deferred lesions in 509 FFR-Guided Patients
53 Repeat Revascularizations(37 in a new lesion or in a
restenotic one)
16 originally deferred lesions(6 without FFR or despite an
FFR > 0.80
10 originally deferred lesionswith clear progression
Only 1 / 513 (0.2%) of deferredlesions resulted in a late MI
Tonino et Al. FAME Study – NEJM 2009,360:213-224
18
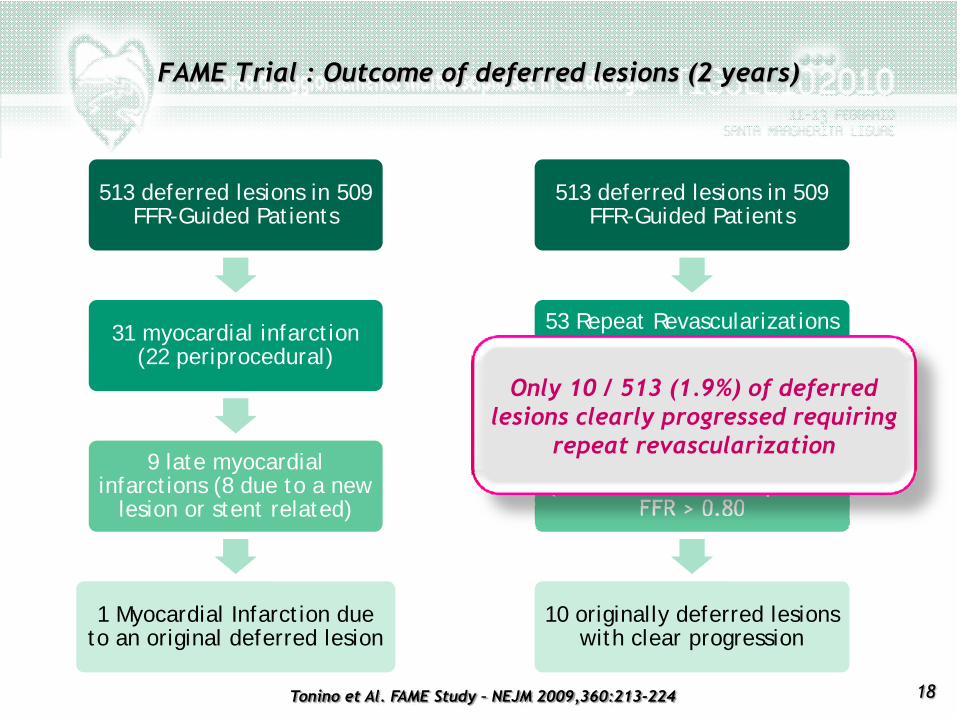
FAME Trial : Outcome of deferred lesions (2 years)
513 deferred lesions in 509 FFR-Guided Patients
31 myocardial infarction(22 periprocedural)
9 late myocardialinfarctions (8 due to a new
lesion or stent related)
1 Myocardial Infarction due to an original deferred lesion
513 deferred lesions in 509 FFR-Guided Patients
53 Repeat Revascularizations(37 in a new lesion or in a
restenotic one)
16 originally deferred lesions(6 without FFR or despite an
FFR > 0.80
10 originally deferred lesionswith clear progression
Only 10 / 513 (1.9%) of deferredlesions clearly progressed requiring
repeat revascularization
Tonino et Al. FAME Study – NEJM 2009,360:213-224
19
Pazienti “stabili” dopo un infarto miocardicoInspire – Swiss II
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
20
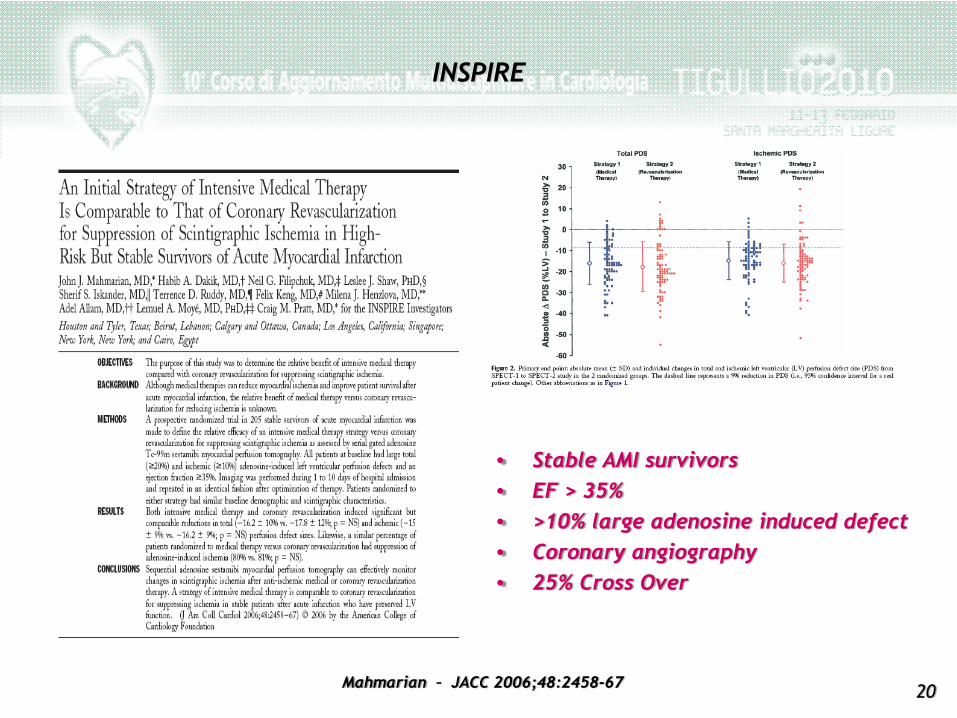
INSPIRE
• Stable AMI survivors• EF > 35%• >10% large adenosine induced defect• Coronary angiography• 25% Cross Over
Mahmarian – JACC 2006;48:2458-67
21
• OBJECTIVES– to determine the relative benefit of intensive medical therapy compared with coronary
revascularization for suppressing scintigraphic ischemia.
• RESULTS– Both intensive medical therapy and coronary revascularization induced significant but
comparable reductions in total (16.2 10% vs. 17.8 12%; p NS) and ischemic (15.9% vs. 16.2 9%; p NS) perfusion defect sizes. Likewise, a similar percentage of patients randomized to medical therapy versus coronary revascularization had suppression of adenosine-induced ischemia (80% vs. 81%; p NS).
CONCLUSIONS
• A strategy of intensive medical therapy is comparable to coronary revascularization for suppressing ischemia in stable patients after acute infarction who have preserved LV function.
• Ischemia suppression was achieved in 80% of patients randomized to either strategy.
• Consistent with the similarity in scintigraphic treatment effects, 1-year cardiac event rates were comparable between strategies.
INSPIRE
Mahmarian – JACC 2006;48:2458-67
22
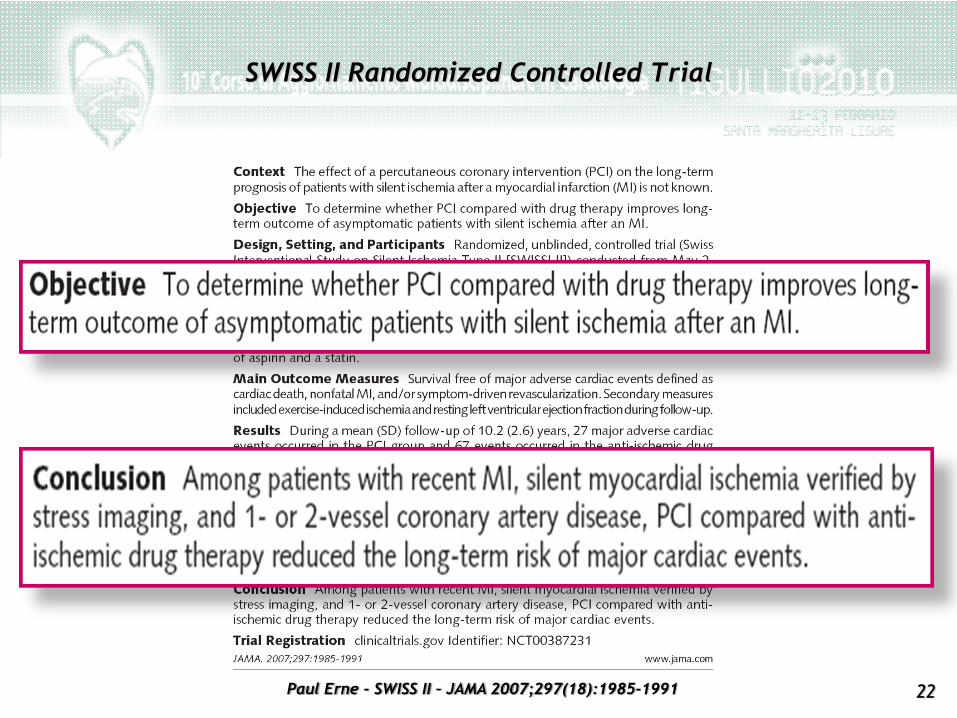
SWISS II Randomized Controlled Trial
Paul Erne - SWISS II – JAMA 2007;297(18):1985-1991
23
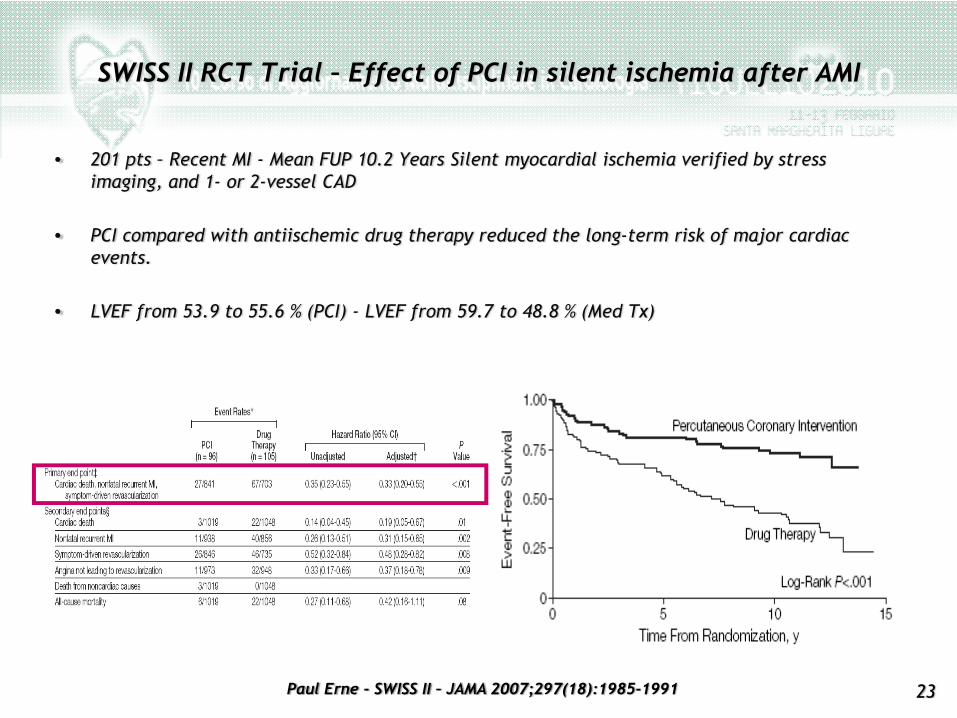
SWISS II RCT Trial – Effect of PCI in silent ischemia after AMI
• 201 pts – Recent MI - Mean FUP 10.2 Years Silent myocardial ischemia verified by stress imaging, and 1- or 2-vessel CAD
• PCI compared with antiischemic drug therapy reduced the long-term risk of major cardiac events.
• LVEF from 53.9 to 55.6 % (PCI) - LVEF from 59.7 to 48.8 % (Med Tx)
Paul Erne - SWISS II – JAMA 2007;297(18):1985-1991
24
Pazienti con diabete mellito – BARI 2D
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
25
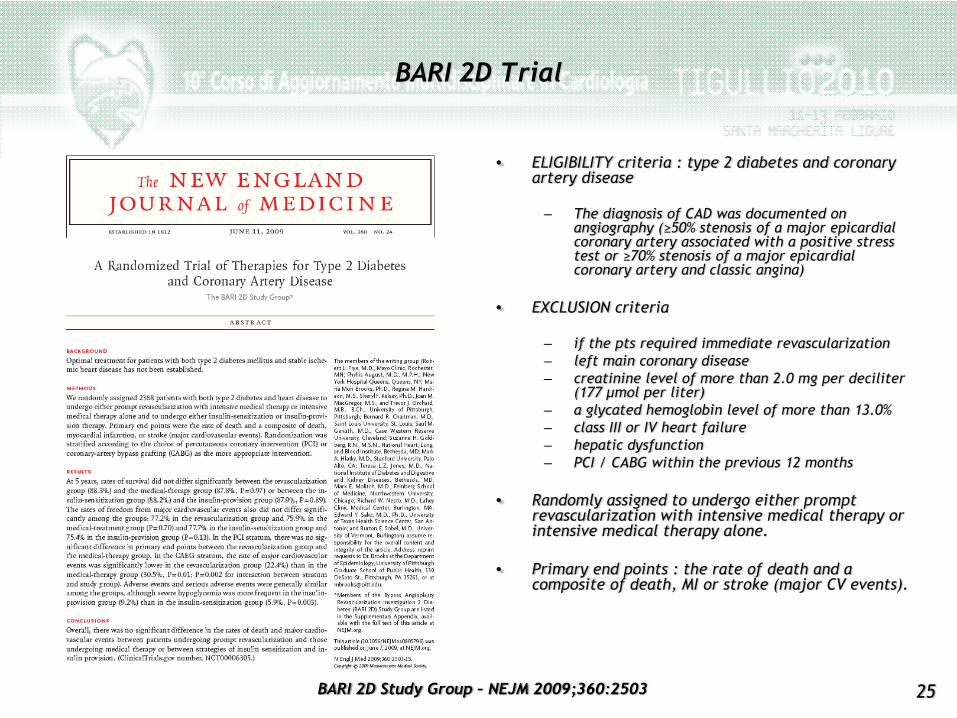
• ELIGIBILITY criteria : type 2 diabetes and coronary artery disease
– The diagnosis of CAD was documented on angiography (≥50% stenosis of a major epicardialcoronary artery associated with a positive stress test or ≥70% stenosis of a major epicardialcoronary artery and classic angina)
• EXCLUSION criteria
– if the pts required immediate revascularization– left main coronary disease– creatinine level of more than 2.0 mg per deciliter
(177 μmol per liter)– a glycated hemoglobin level of more than 13.0%– class III or IV heart failure– hepatic dysfunction– PCI / CABG within the previous 12 months
• Randomly assigned to undergo either prompt revascularization with intensive medical therapy or intensive medical therapy alone.
• Primary end points : the rate of death and a composite of death, MI or stroke (major CV events).
BARI 2D Trial
BARI 2D Study Group – NEJM 2009;360:2503
26
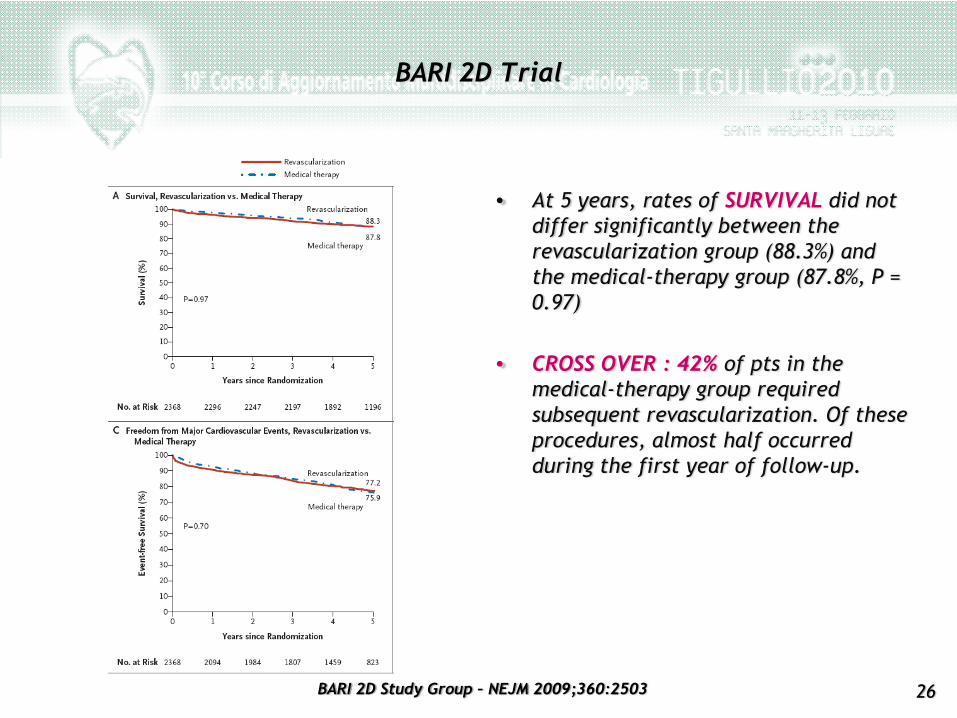
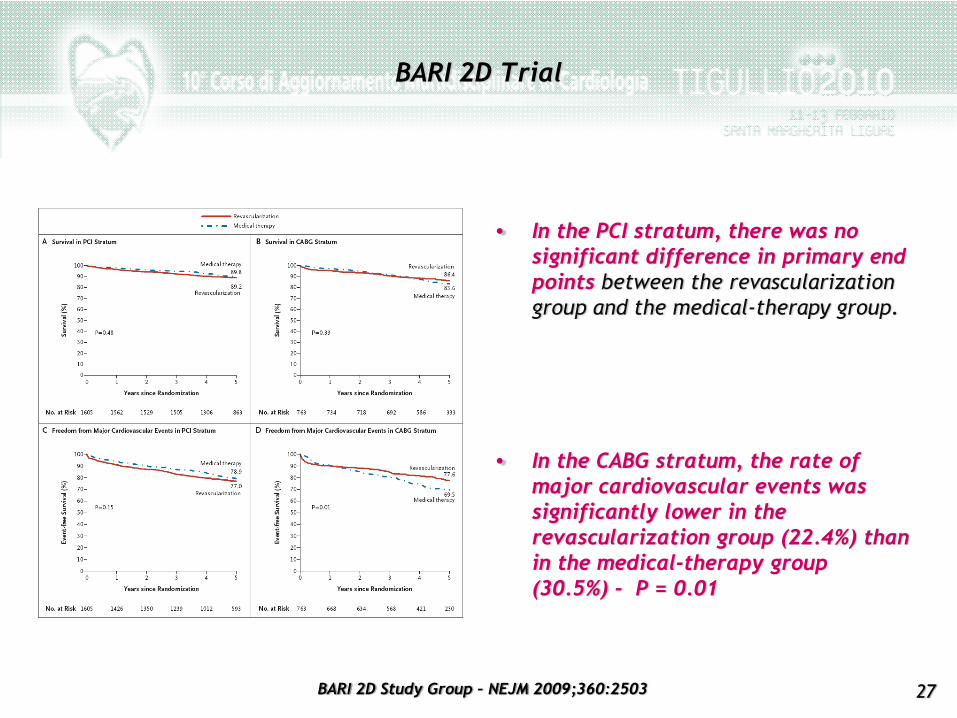
• At 5 years, rates of SURVIVAL did not differ significantly between the revascularization group (88.3%) and the medical-therapy group (87.8%, P = 0.97)
• CROSS OVER : 42% of pts in the medical-therapy group required subsequent revascularization. Of these procedures, almost half occurred during the first year of follow-up.
BARI 2D Trial
BARI 2D Study Group – NEJM 2009;360:2503
27
• In the PCI stratum, there was no significant difference in primary end points between the revascularization group and the medical-therapy group.
• In the CABG stratum, the rate of major cardiovascular events was significantly lower in the revascularization group (22.4%) than in the medical-therapy group (30.5%) - P = 0.01
BARI 2D Trial
BARI 2D Study Group – NEJM 2009;360:2503
28
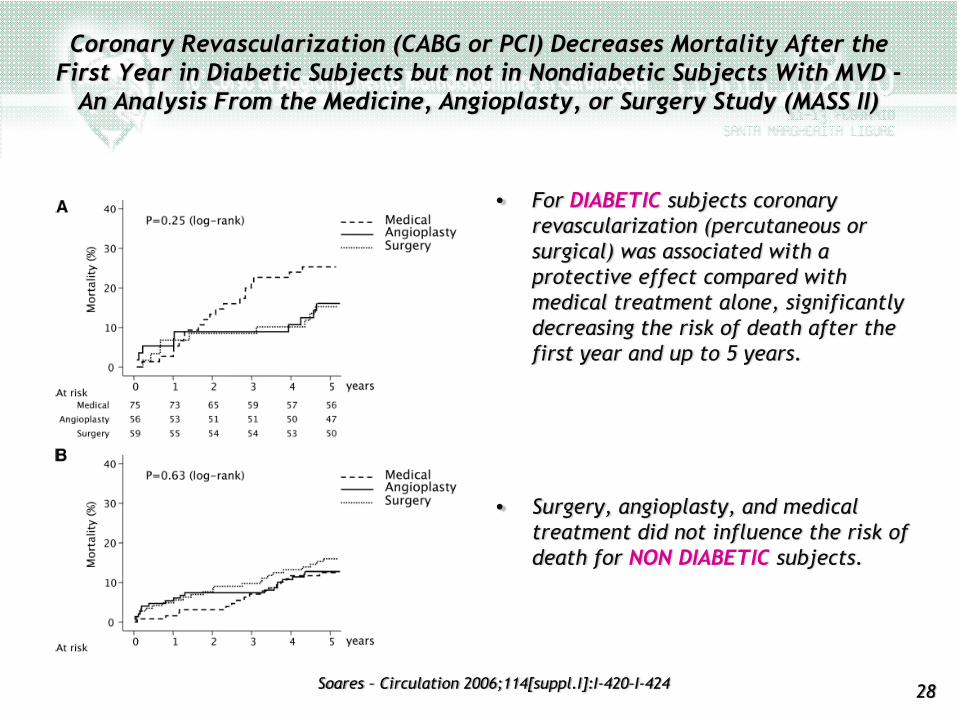
• For DIABETIC subjects coronary revascularization (percutaneous or surgical) was associated with a protective effect compared with medical treatment alone, significantly decreasing the risk of death after the first year and up to 5 years.
• Surgery, angioplasty, and medical treatment did not influence the risk of death for NON DIABETIC subjects.
Coronary Revascularization (CABG or PCI) Decreases Mortality After the First Year in Diabetic Subjects but not in Nondiabetic Subjects With MVD -
An Analysis From the Medicine, Angioplasty, or Surgery Study (MASS II)
Soares – Circulation 2006;114[suppl.I]:I-420–I-424
29
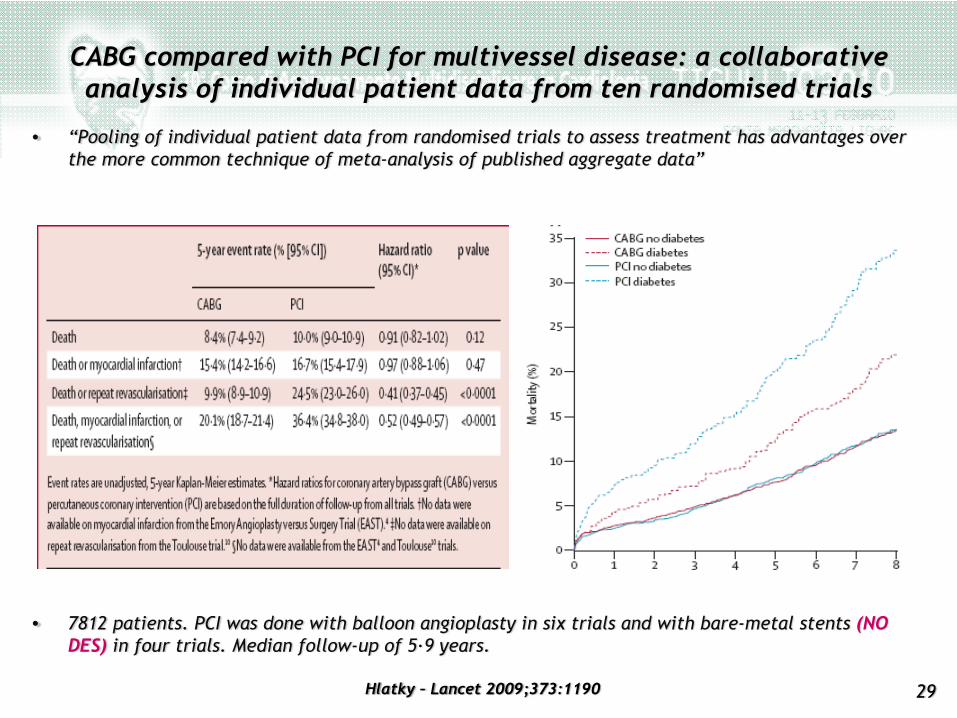
CABG compared with PCI for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials
Hlatky – Lancet 2009;373:1190
• 7812 patients. PCI was done with balloon angioplasty in six trials and with bare-metal stents (NO DES) in four trials. Median follow-up of 5·9 years.
• “Pooling of individual patient data from randomised trials to assess treatment has advantages over the more common technique of meta-analysis of published aggregate data”
30
Se è clinicamente giustificata la rivascolarizzazione ……CABG o PCI ?
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
31
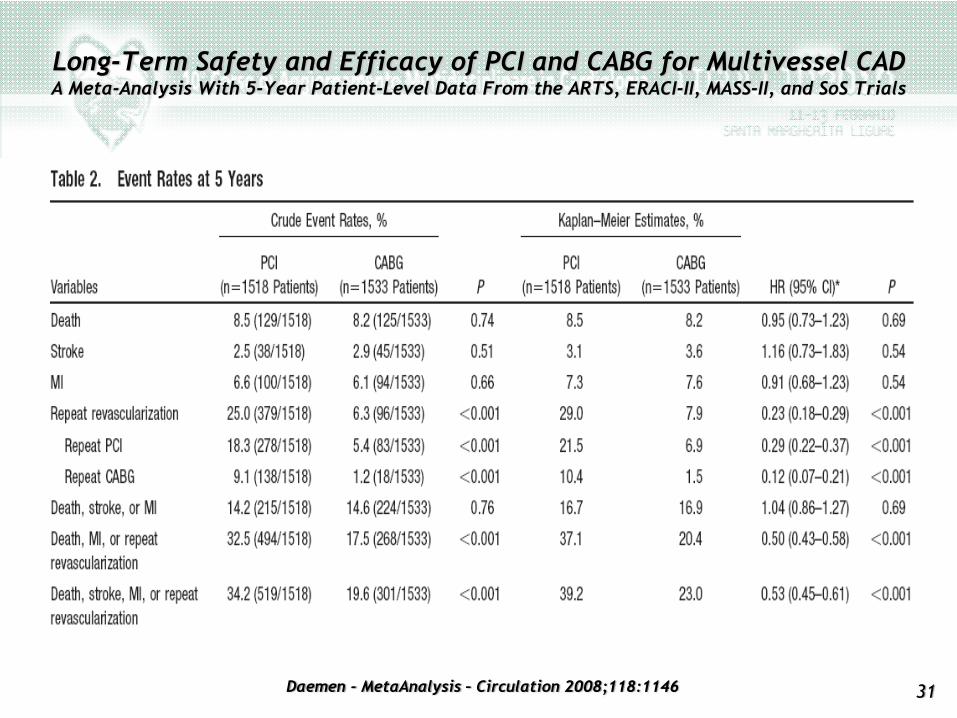
Long-Term Safety and Efficacy of PCI and CABG for Multivessel CADA Meta-Analysis With 5-Year Patient-Level Data From the ARTS, ERACI-II, MASS-II, and SoS Trials
Daemen - MetaAnalysis – Circulation 2008;118:1146

32
Systematic Review : The Comparative Effectiveness of PCI and CABG23 RCTs in which 5019 patients were randomly assigned to PCI and 4944 patients were randomly assigned to CABG
Bravata – Annals Intern Med 2007;147:703
• The difference in SURVIVAL after PCI or CABG was less than 1% over 10 years of follow-up
• Procedure-related STROKES were more common after CABG than after PCI (1.2% vs. 0.6%; risk difference, 0.6%; P 0.002).
• ANGINA RELIEF was greater after CABG than after PCI, with risk differences ranging from 5% to 8% at 1 to 5 years (P 0.001).
• REPEAT REVASCULARIZATION was more common after PCI than after CABG (risk difference, 24% at 1 year and 33% at 5 years; P 0.001); the absolute rates at 5 years were 46.1% after balloon angioplasty, 40.1% after PCI with stents, and 9.8% after CABG.
• CONCLUSION : Compared with PCI, CABG was more effective in relieving angina and led to fewer repeated revascularizations but had a higher risk for procedural stroke. Survival to 10 years was similar for both procedures.
33
NOTABLE STRENGHTS
• Prospective, multicenter trial (85 centers in Europe and USA).
• It attempted to include “all comers” with left main or three-vessel coronary artery disease. (71% of screened patients enrolled in the randomized or registry cohorts)
• State of-the-art CABG and PCI (arterial grafts and DES) both with excellent results.
• A “heart team” consisting of an interventional cardiologist and cardiac surgeon reviewed each subject’s data (angio included), after which they reached agreement on which procedure or procedures should be offered to that subject.
LIMITATIONS
• Follow-up period only 12 months (the outcomes a longer period in pts with severe CAD are unknown)
• 78% men
• CABG patients were significantly undertreated with aspirin (84% vs91%), thienopyridine (15% vs 71%), and statin drugs (75% vs 87%) compared with PCI patients. These factors may be relevant to the 50% of CABG strokes that occurred more than 30 days after operation.
SYNTAX : 1.800 pts with LM or 3VD randomly assigned to CABG or PCI (with DES) to determine which was the better revasc. strategy
Lange and Hillis – Editorial – NEJM 2009;360,10:1024-1026
34
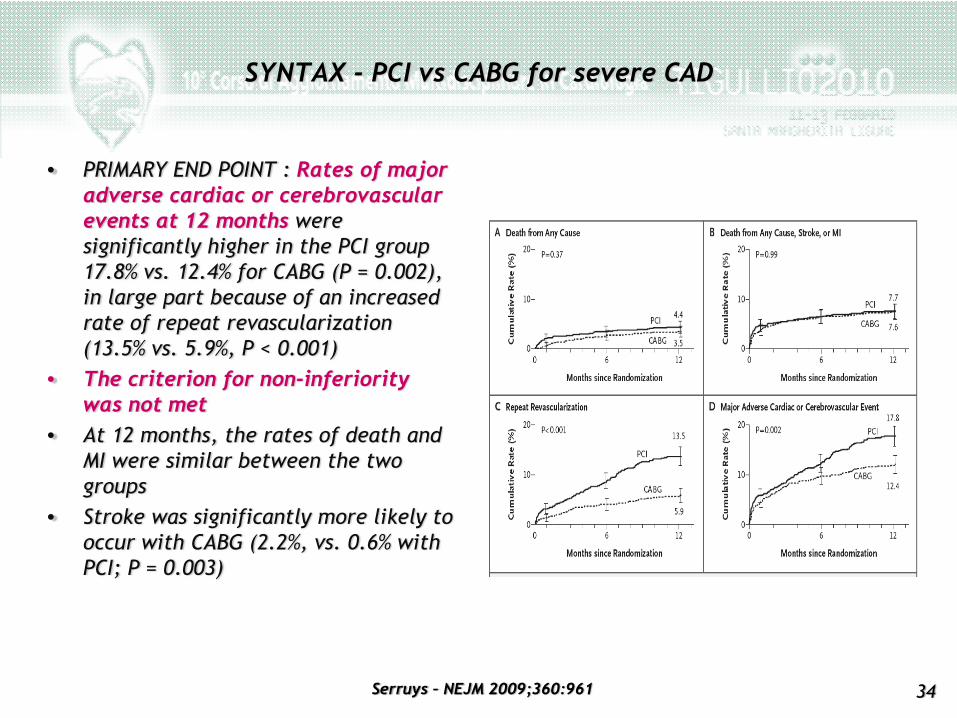
SYNTAX - PCI vs CABG for severe CAD
Serruys – NEJM 2009;360:961
• PRIMARY END POINT : Rates of major adverse cardiac or cerebrovascularevents at 12 months were significantly higher in the PCI group 17.8% vs. 12.4% for CABG (P = 0.002), in large part because of an increased rate of repeat revascularization (13.5% vs. 5.9%, P < 0.001)
• The criterion for non-inferiority was not met
• At 12 months, the rates of death and MI were similar between the two groups
• Stroke was significantly more likely to occur with CABG (2.2%, vs. 0.6% with PCI; P = 0.003)
35
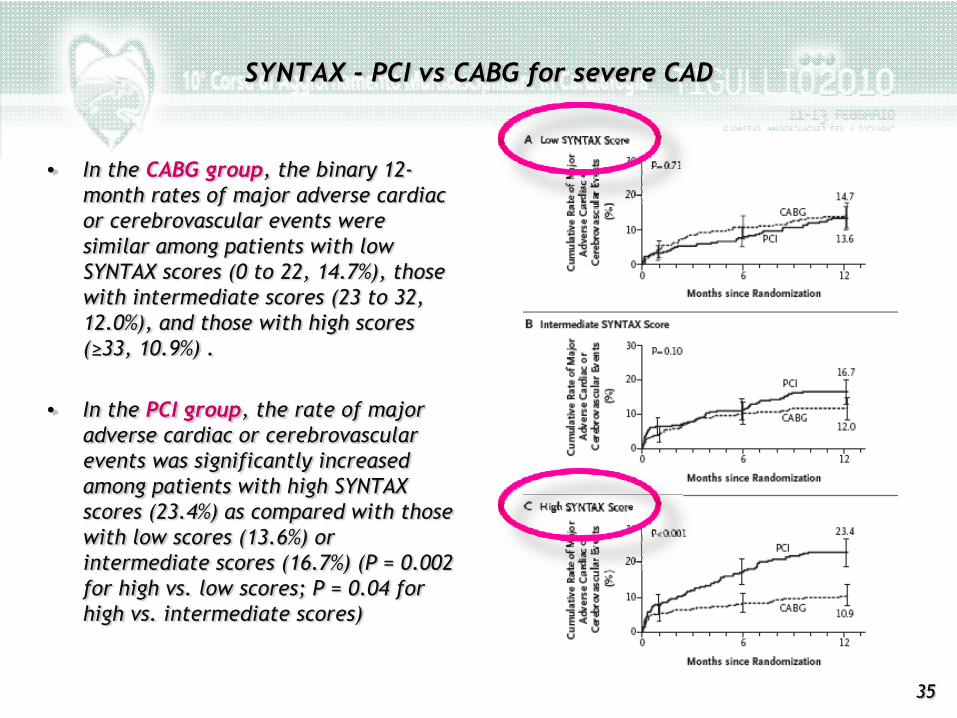
• In the CABG group, the binary 12-month rates of major adverse cardiac or cerebrovascular events were similar among patients with low SYNTAX scores (0 to 22, 14.7%), those with intermediate scores (23 to 32, 12.0%), and those with high scores (≥33, 10.9%) .
• In the PCI group, the rate of major adverse cardiac or cerebrovascularevents was significantly increased among patients with high SYNTAX scores (23.4%) as compared with those with low scores (13.6%) or intermediate scores (16.7%) (P = 0.002 for high vs. low scores; P = 0.04 for high vs. intermediate scores)
SYNTAX - PCI vs CABG for severe CAD
36
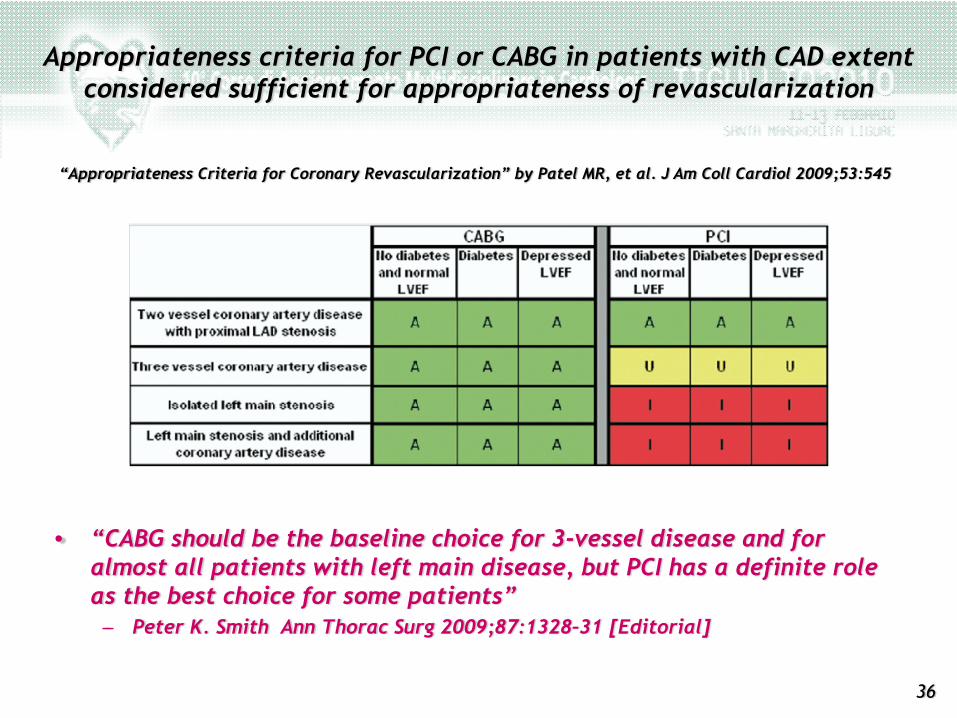
Appropriateness criteria for PCI or CABG in patients with CAD extent considered sufficient for appropriateness of revascularization
• “CABG should be the baseline choice for 3-vessel disease and for almost all patients with left main disease, but PCI has a definite role as the best choice for some patients” – Peter K. Smith Ann Thorac Surg 2009;87:1328–31 [Editorial]
“Appropriateness Criteria for Coronary Revascularization” by Patel MR, et al. J Am Coll Cardiol 2009;53:545
37
Attenzione fisiopatologica- alla entità della ischemia ed - alla funzione VSx
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
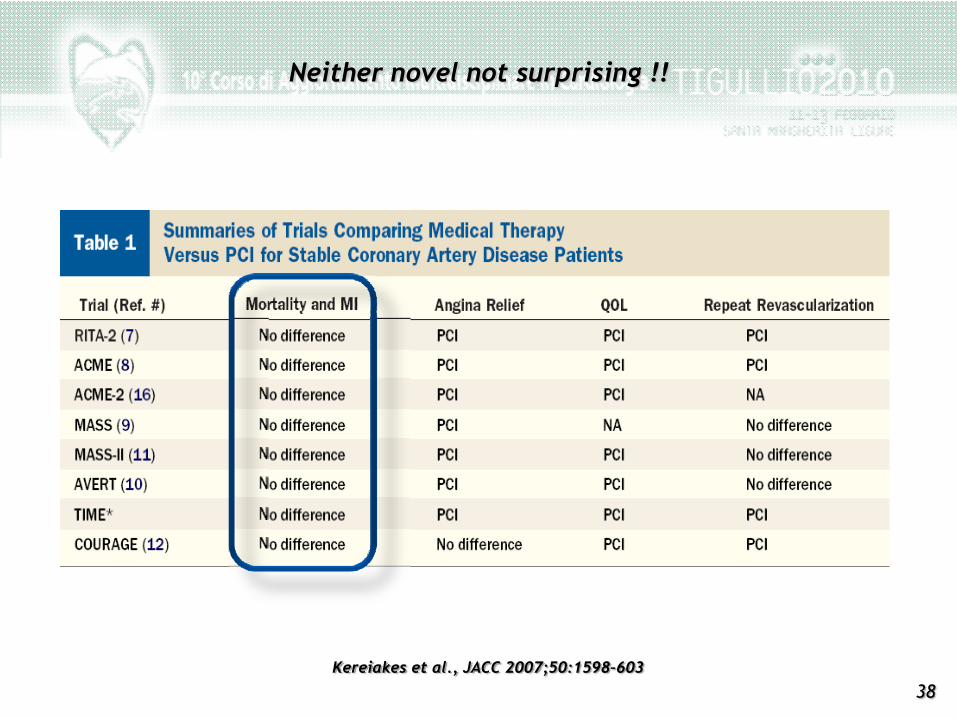
38Kereiakes et al., JACC 2007;50:1598–603
Neither novel not surprising !!
39
• Nelle forme ACUTE la rivascolarizzazione risolve l’ISCHEMIA, che, in questo contesto, è la causa principale di mortalità
• Nelle forme CRONICHE (stabili) la mortalità è principalmente dovuta a– Funzione ventricolare (frazione di eiezione)– Ischemia inducibile (entità)– Pregresso infarto miocardico– Gravità e SEDE delle stenosi coronariche
Perché nessuna differenza nella mortalità ?
40Rory Hachamovitch – Circulation 2003;107:2900-2906
• A total of 10.627 consecutive patients who underwent exercise or adenosine MPS and had no prior myocardial infarction or revascularization were followed up (90.6% complete; mean: 1.9 ± 0.6 years)…
• Patients undergoing Medical Therapy demonstrated a survival advantageover patients undergoing revasc. in the setting of no or mild ischemia...
• whereas patients undergoing revascularization had an increasing survival benefit over patients undergoing MT when moderate to severe ischemia was present
Comparison of the Short-Term Survival Benefit Associated With Revascularization Compared With Medical Therapy in Pts With No
Prior CAD Undergoing Stress Myocardial Perfusion SPECT
41
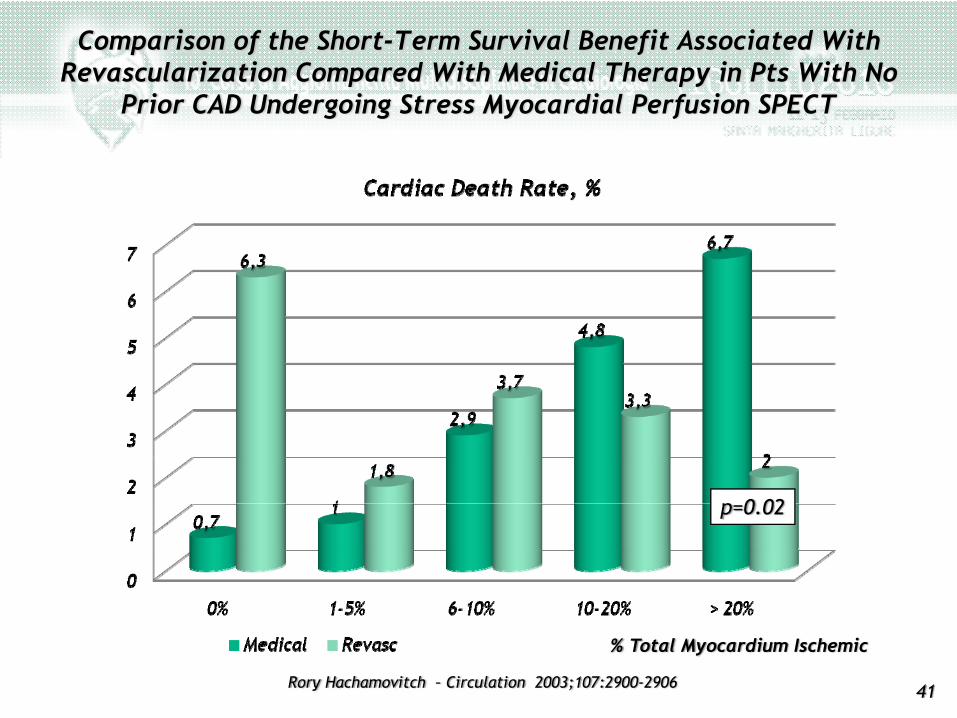
Comparison of the Short-Term Survival Benefit Associated WithRevascularization Compared With Medical Therapy in Pts With No
Prior CAD Undergoing Stress Myocardial Perfusion SPECT
p=0.02
% Total Myocardium Ischemic
Rory Hachamovitch – Circulation 2003;107:2900-2906
42
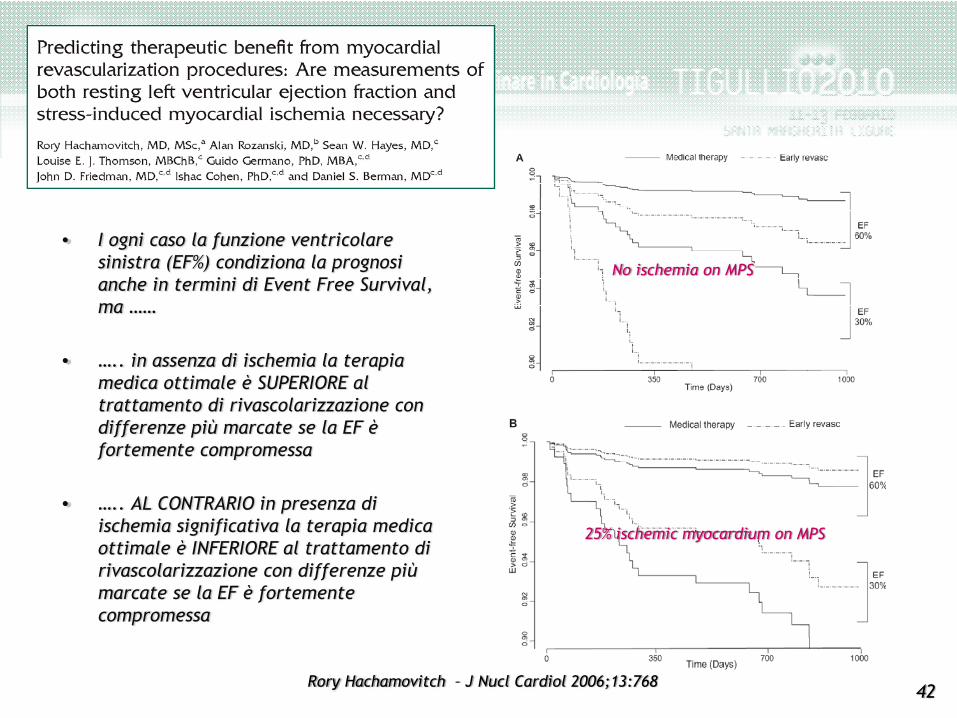
• I ogni caso la funzione ventricolare sinistra (EF%) condiziona la prognosi anche in termini di Event Free Survival, ma ……
• ….. in assenza di ischemia la terapia medica ottimale è SUPERIORE al trattamento di rivascolarizzazione con differenze più marcate se la EF è fortemente compromessa
• ….. AL CONTRARIO in presenza di ischemia significativa la terapia medica ottimale è INFERIORE al trattamento di rivascolarizzazione con differenze più marcate se la EF è fortemente compromessa
No ischemia on MPS
25% ischemic myocardium on MPS
Rory Hachamovitch – J Nucl Cardiol 2006;13:768
43
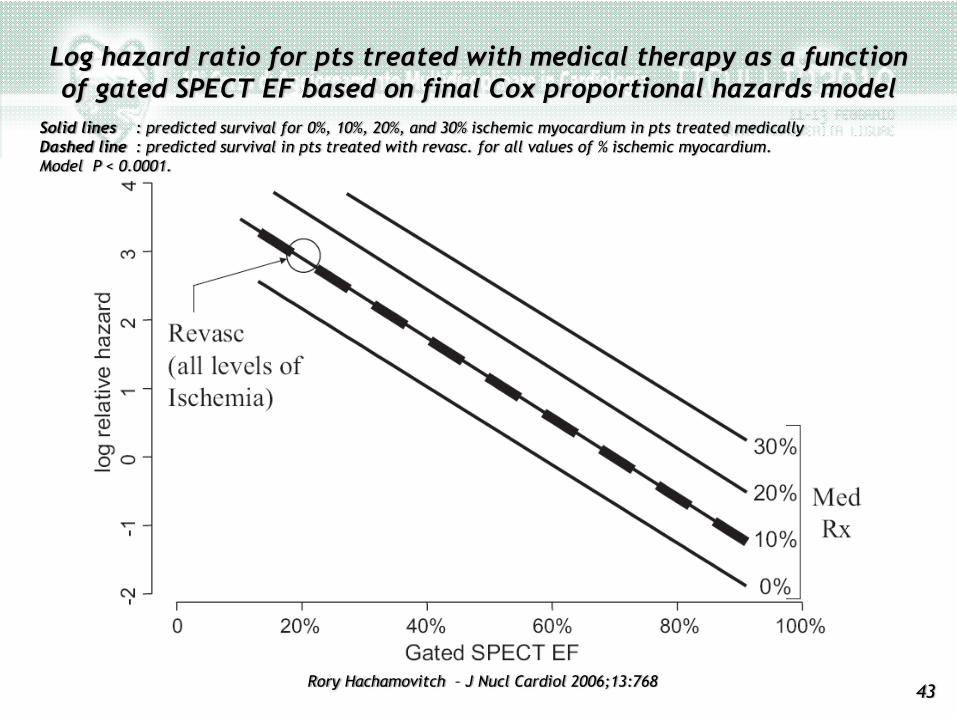
Log hazard ratio for pts treated with medical therapy as a function of gated SPECT EF based on final Cox proportional hazards model
Solid lines : predicted survival for 0%, 10%, 20%, and 30% ischemic myocardium in pts treated medicallyDashed line : predicted survival in pts treated with revasc. for all values of % ischemic myocardium. Model P < 0.0001.
Rory Hachamovitch – J Nucl Cardiol 2006;13:768
44
• The only patients who had a statistically significant SURVIVAL BENEFIT from early revascularization were those who had myocardial ischemia (10%) and left ventricular dysfunction.
• For patients without significant impairment of fractional flow reserve who were randomized to undergo PCI versus a deferred procedure, there was no improvement in event-free survival rate.
• Patients with a reduced EF stand to benefit the most from revascularization in terms of absolute survival improvement but, at the same time, are at greater risk for a poor procedure outcome in the absence of ischemia.
Revascularize only for ischemia, especially if LV function is poor
Mark I. Travin - J Nucl Cardiol 2006;13:742 [ Editorial]
45
Conclusioni
Appropriatezza in terapia della cardiopatia ischemica cronica. Vantaggi e limiti della terapia di rivascolarizzazione.
46
Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial
KEY POINTS
Nei pazienti con Cardiopatia Ischemica Stabile
1. La rivascolarizzazione migliora temporaneamente i sintomi (se questi ci sono)
2. Il solo trattamento farmacologico ottimale è competitivo ….– Se la terapia medica è ottimale con target simili a quelli raggiunti nel Courage – Se il follow up è stretto e riconosce la instabilizzazione da trattare in modo invasivo– Se c’è liberalità di cross over ( > 30% in 4.6 anni nel Courage, ma 30% in un anno per i pt più gravi )– Se l’anatomia coronarica è nota
3. La rivascolarizzazione può migliorare la sopravvivenza e ridurre i MACE ….– Se il paziente ha avuto un infarto miocardico significativo– Se l’area di ischemia inducibile è ≥10 % e se si ottiene una riduzione dell’ischemia inducibile > 5 %– Se la EF è molto ridotta e di conseguenza aumenta la efficacia della riduzione di ischemia
4. Il trattamento farmacologico ottimale va garantito anche al paziente rivascolarizzato
47
Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial
KEY POINTS
Nei pazienti con Cardiopatia Ischemica Stabile
1. La rivascolarizzazione migliora temporaneamente i sintomi (se questi ci sono)
2. Il solo trattamento farmacologico ottimale è competitivo ….– Se la terapia medica è ottimale con target simili a quelli raggiunti nel Courage– Se il follow up è stretto e riconosce la instabilizzazione da trattare in modo invasivo– Se c’è liberalità di cross over ( > 30% in 4.6 anni nel Courage, ma 30% in un anno per i pt più gravi )– Se l’anatomia coronarica è nota
3. La rivascolarizzazione può migliorare la sopravvivenza e ridurre i MACE ….– Se il paziente ha avuto un infarto miocardico significativo– Se l’area di ischemia inducibile è ≥10 % e se si ottiene una riduzione dell’ischemia inducibile > 5 %– Se la EF è molto ridotta e di conseguenza aumenta la efficacia della riduzione di ischemia
4. Il trattamento farmacologico ottimale va garantito anche al paziente rivascolarizzato
48
Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial
KEY POINTS
Nei pazienti con Cardiopatia Ischemica Stabile
1. La rivascolarizzazione migliora temporaneamente i sintomi (se questi ci sono)
2. Il solo trattamento farmacologico ottimale è competitivo ….– Se la terapia medica è ottimale con target simili a quelli raggiunti nel Courage– Se il follow up è stretto e riconosce la instabilizzazione da trattare in modo invasivo– Se c’è liberalità di cross over ( > 30% in 4.6 anni nel Courage, ma 30% in un anno per i pt più gravi )– Se l’anatomia coronarica è nota
3. La rivascolarizzazione può migliorare la sopravvivenza e ridurre i MACE ….– Se il paziente ha avuto un infarto miocardico significativo– Se l’area di ischemia inducibile è ≥10 % e se si ottiene una riduzione dell’ischemia inducibile > 5 %– Se la EF è molto ridotta e di conseguenza aumenta la efficacia della riduzione di ischemia
4. Il trattamento farmacologico ottimale va garantito anche al paziente rivascolarizzato
49
Vantaggi e limiti della terapia di rivascolarizzazione alla luce dei recenti trial
KEY POINTS
Nei pazienti con Cardiopatia Ischemica Stabile
1. La rivascolarizzazione migliora temporaneamente i sintomi (se questi ci sono)
2. Il solo trattamento farmacologico ottimale è competitivo ….– Se la terapia medica è ottimale con target simili a quelli raggiunti nel Courage– Se il follow up è stretto e riconosce la instabilizzazione da trattare in modo invasivo– Se c’è liberalità di cross over ( > 30% in 4.6 anni nel Courage, ma 30% in un anno per i pt più gravi )– Se l’anatomia coronarica è nota
3. La rivascolarizzazione può migliorare la sopravvivenza e ridurre i MACE ….– Se il paziente ha avuto un infarto miocardico significativo– Se l’area di ischemia inducibile è ≥10 % e se si ottiene una riduzione dell’ischemia inducibile > 5 %– Se la EF è molto ridotta e di conseguenza aumenta la efficacia della riduzione di ischemia
4. Il trattamento farmacologico ottimale va garantito anche al paziente rivascolarizzato