Unità Operativa di Geriatria e Laboratorio di Ricerca ......IRCCS “Casa Sollievo della Sofferenza...
54
Greco A, Addante F, Longo MG, Scarcelli C, Niro V, Sancarlo D, D ’ Agostino MP, Paroni G, Seripa D Unità Operativa di Geriatria e Laboratorio di Ricerca Geriatria e Gerontologia IRCCS “ Casa Sollievo della Sofferenza” San Giovanni Rotondo (FG) Italia
Transcript of Unità Operativa di Geriatria e Laboratorio di Ricerca ......IRCCS “Casa Sollievo della Sofferenza...

Greco A, Addante F, Longo MG, Scarcelli C, Niro V, Sancarlo D, D’Agostino MP, Paroni G, Seripa D
Unità Operativa di Geriatria e Laboratorio di Ricerca Geriatria e Gerontologia IRCCS “Casa Sollievo della Sofferenza” San Giovanni Rotondo (FG) Italia

Can sarcopenia be reversed?

sarx – carne penia – perdita
riduzione della massa e/o della forza muscolare che si riscontra nel corso di invecchiamento
FATTORI CHE POSSONO CONTRIBUIRE ALLO SVILUPPO DELLA SARCOPENIA
- Diminuzione età correlata delle fibre muscolari
- Riduzione delle attività fisiche
- Declino ormonale: sia riproduttivi che dell’asse hypothalamic-GH-insulinlike growth factor
- Insufficienza nutrizionale
- È stata anche rilevata una componente genetica nella sarcopenia. [Roth SM, et al: j gerontol biol sci 2004;59a:10–5]

Sarcopenia compares with malnutrition and inactivity
• To fight against sarcopenia, one needs to:
– Screen
–Treat

Screening strategy
Cruz-Jentoft et al. Age Ageing 2010

• ↓ forza, potenza e resistenza muscolare
• ↓ massa ossea
• ↓ equilibrio con instabilità posturale
• ↓ isolamento corporeo
• ↓ produzione basale di calore
• ↑ calore specifico
• ↓ contenuto corporeo acqua
• ↓ capacità dispersione cutanea calore
• ↓ metabolismo basale e aumento della massa grassa


Burton LA, Clinical Intervention in Aging 2010

Causes of sarcopenia: therapeutic approaches?
SARCOPENIA
Senescence
Inflammation
Disuse
Starvation
Endocrine
Insulin resistance
Vitamin D deficiency
Cederholm et al. Clin Geriatr Med 2011

Inactivity
Malnutrition
Balance
Synthesis
Breakdown
Muscle
growth
Muscle
loss
Nutrition
Exercise
Hormones
Maintaining Muscle Mass and
Function
Protein
Illness/Injury

Exercise – physical activity

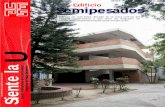
Inactivity and Aging Muscle
-1500
-1000
-750
-500
-250
0
250
Loss
of
lean
leg
mass
(g)
-2000
Healthy Young
28 Days Inactivity
2%
total lean leg mass
Healthy Elders
10 Days Inactivity
10%
total lean leg mass
Paddon-Jones et. al. 2004
Kortebein et al. 2007
3 times more
muscle loss
1/3 the time
All volunteers
consumed the
RDA for protein

Kortebein, P. et al. JAMA 2007
Effects of 10 Days of Bed Rest in Older Adults

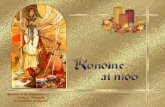
Randomized-controlled trials of exercise benefits on functional impairment (10 RCTs, 1150 persons)
Brown et al. 00 Buchner et al. 97 Cress et al. 99 Fiatarone et al 94 Jette et al. 97 Jette et al. 99 Lord et al. 95 Pollock et al. 91 Rooks et al. 91 Wolfson et al. 96
84 frail m+w, 83 y 105 impaired m+w, 75 y 49 healthy m+w, 76 100 frail nursing home p, 87y 102 nondisabled m+w, 72 y 215 disabled m+w, 75 y 197 healthy w, 72 y 57 healthy m+w, 72 y 131 healthy m+w, 74 y 110 healty m+w, 80 y
muscle strength, reaction time, balance muscle strength muscle strength muscle strength muscle strength muscle strength muscle strength, balance muscle strength muscle strength, reaction time, balance muscle strength, balance

Adjusted % change in disability score
Ettinger et al. JAMA 1997;277:25
-10%
-5%
0%
5%
10%
15%
Control
Resistance exercise
Aerobic exercise
Follow up (months)
0 18 9 3
Exercise and Disability (FAST)
P<.001 vs. control
N=439

La revisione ha interessato 1021 studi per un totale di 6700 pazienti anziani. Dimostra che PRT è un intervento efficace per migliorare le funzionalità fisiche nelle persone anziane, tra cui l’aumento della forza e il miglioramento delle prestazioni nelle attività semplici e complesse
CONCLUSIONI DEGLI AUTORI

Is exercise a validated treatment for sarcopenia? Yes, in particular resistance training
Available evidence: Very good
Exercise – physical activity

Protein - Nutritional supplements

Inactivity reduces muscle protein
synthesis
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
Day 1 Day 10
Pro
tein
Synth
esis
(%
/h)
* 30%
Kortebein et al. 2007
24 h muscle protein synthesis during 10 day of inactivity in elders
(stable isotope methodology)

Protein combats inactivity-induced
muscle loss
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.1
Day 1 Day 10
Pro
tein
Syn
the
sis
(%
/h)
*
Normal Diet Normal Diet Normal Diet + Amino Acids
#
Normal Diet + Amino Acids
30%
Ferrando & Paddon-Jones et. al. 2009
- older adults -

Houston, D. K et al. Am J Clin Nutr 2008
Lean mass loss by quintile of energy-adjusted total protein intake

Muscle Protein Synthesis and Age
Symons et. al. AJCN, 2007
* *
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Fasting
Pro
tein
Synth
esis
(%
/h)
Young
Elderly
50% increase
30 g protein
* 10 g essential
amino acids
Building muscle in response to protein

Plasma leucine concentration and
protein synthesis rate
Rieu I et al. Nutrition 2007

How much protein do we need –
and when ?

Protein Synthesis and Portion Control - a message of moderation -
* *
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Fasting 30 g protein
Pro
tein
Syn
the
sis
(%
/h) * *
Fasting 90 g protein
Young
Old
~1.2 g/kg/day for 180 lb individual
90 g protein 30 g protein
Symons et. al. AJCN, 2007 Symons et. al. JADA. 2009

* *
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Fasting
Pro
tein
Synth
esis
(%
/h) 0.16
0.18 No age-related
impairment
Key points
Moderate protein meal
Symons et. al. AJCN, 2007

Ne
t M
uscle
Pro
tein
Syn
thesis
(m
g P
he/le
g)
More than ~25 g protein
Age-related dose-response
0
10
20
30
40
50
60
Young
Elderly
Less than ~15 g protein
Katsanos et. al. AJCN, 2005

Relationship between the amount of protein per meal and the resultant anabolic response
Adapted from Paddon-Jones, 2009

Daily protein distribution - typical ? -
Total Protein
90 g
Cat
abol
ism
A
nabol
ism
10 g
maximum rate of protein synthesis
15 g 65 g
A skewed daily protein distribution fails
to maximize potential for muscle growth

Daily protein distribution - Optimal -
Cat
abol
ism
A
nabol
ism
maximum rate of protein synthesis
30 g 30g 30 g
Total Protein
90 g
Repeated maximal stimulation of protein synthesis increase / maintenance of muscle mass
~ 1.3 g/kg/day

Protein-exercise interaction

Resistance exercise + nutrition (protein)
Adapted from Biolo, 1997

Physical Disability
Time (months)
0 6 12 18
Su
mm
ary
Dis
ab
ilit
y S
core
1.70
1.75
1.80
1.85
1.90
1.95
2.00
2.05
Healthy Lifestyle Control
Diet
Exercise
Diet + Exercise
*
Messier et al Arthritis & Rheumatism 2004;50:1501
ADAPT – Diet, exercise and
disability

Options to optimize post-prandial anabolic action of dietary proteins
• Increase protein intake
– Age-specific RDAs
• Increase amino acid bioavailability
– Distribution of protein intake
– Digestion rate
• Use specific substrates
– Leucine
– ß-hydroxy-ß-methylbutyrate (HMB)
– Vitamin D

Leucine-HMB Metabolic Pathway
HMB KIC
(Liver, Muscle)
Urine (10-40%)
95%
5%
Other pathway
Liver Circulates
Muscle:
- Cholesterol
synthesis
- NFkB
- mTOR
Leucine
(Diet only)
The is an amino acid metabolite that occurs naturally in human muscle cells.
Traditionally, HMB has been used by athletes to enhance performance and
build muscle mass. Recent studies have focused on the use of HMB to
preserve or rebuild muscle mass.

Role of HMB on muscle function

Studies in Elderly with HMB
Citation Population Intervention Results
Vukovich et al.
J Nutr 2001
31 elderly individuals 70 ± 1 years old
8-week study
CaHMB: 3 g/d or Placebo
Trained with walking and stretching
Greater reduction in % body fat*
Lean mass increased
Greater upper and lower body strength*
Panton et al.
Med Sci Sports Ex 1998
35 M/F elderly adults
8-week study
CaHMB group or Placebo group
Resistance training
Greater functional mobility*
Coelho et al.
Med Sci Sports Ex 2001
12 Males 50–72 years old with high cholesterol
3 grams CaHMB or Placebo
Endurance and resistance training
Reduced LDL-cholesterol
Increased LBM
Greater weight lifting and strength*
*P<0.05

Study in elderly subjects receiving HMB
• Objective:
– Can HMB increase LBM and strength in older
adults engaged in resistance training?
• Prospective, randomized, blinded, placebo-
controlled trial
• 31 subjects ( age > 70 yrs); male and female
• 8-week supplementation + exercise (5 d / wk)
• 3 g HMB/day versus placebo
Vukovich et al. J Nutr 2001

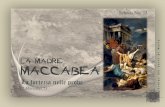
Improved LBM in elderly subjects receiving HMB (p=0.08)
Vukovich et al. J Nutr 2001
Reference: Vukovich et al J. Nutr. 2001;131:2049-2052
Ca HMB
55.2 kg
Mean
baseline
Placebo
54.7 kg
Ca HMB +
resistance training (n = 14)
Placebo +
resistance training (n = 14)

Mechanism of action Vitamin D
Role of Vitamin D on muscle function :

Vitamin D and muscle function
• Institutionalized elderly
• Vitamin D : 150,000 IU per month for 2 months, then 90,000 IU per month for 4 months
Moreira-Pfrimer et al. Ann Nutr Metab 2009

RCTs: Vitamin D and Physical Performance
Bischoff et al.
2003
122 ♀
85,3 y
NH
800 IU D3/d +Ca
vs. Ca, p.o.
3 months
+ Strength M. quadriceps, Handgrip,
TUG
Latham et al.
2003
243 ♀♂
79,1 y
Rehab
300000 IU D3
vs. Placebo, p.o.
3/6 months
- Strength M. quadriceps, TUG,
Balance
Dhesi et al.
2004
139 ♀♂
76,6 y
Amb
600000 IU D2
vs. Placebo, i.m.
6 months
+ Physical performance, Reaction
time, Body sway
- Strength
Pfeifer et al.
2009
242 ♀♂
77 y
Amb
800 IU D3/d +Ca
vs. Ca, p.o.
12 months
+ Strength M. quadriceps, TUG,
Body sway
Zhu et al.
2010
302 ♀
77 y
Amb, VD
deficient
1000 IU D3/d +Ca
vs. Ca, p.o.
12 months
+ Strength hip extensor and adductor,
TUG, Body sway

Meta-analysis: Fall prevention
n=1921
700-1000 IU Vitamin D/d
Bischoff-Ferrari et al. BMJ 2009





• Anticorpi della MIOSTATINA → inibisce rigenerazione muscolare
• CREATINA → aumenta la massa muscolare e le performance fisiche
• TRICOSTATINA A → antagonista della miostatina
• PGC-1α → regolatore della mitocondrogenesi
• Attivatori della AMP-activator protein
• CELLULE STAMINALI



• What should clinicians look for?
• Well recognized risk factors for sarcopenia include increasing age, low levels of physical activity, inadequate nutrition, and comorbidity.
• Identifying high risk groups of older people is straightforward, but making a diagnosis is more difficult.
• In the European guidelines, sarcopenia is diagnosed firstly on the basis of impaired physical performance, characterized by slow gait speed, and then either by low muscle strength assessed by handheld dynamometry or low muscle mass measured, for example, by bioimpedance.
Sayer AA. BMJ 2010; 341:952.

• In terms of managing sarcopenia, meta-analyses show that resistance exercise can improve muscle mass and strength in older adults.
• The evidence for the role of nutrition in the prevention and treatment of sarcopenia is less clear. In particular, more information is needed on protein and specific amino acids, such as leucine.
• Protein intake may become insufficient with the reduction in total food intake seen in later life and dietary reference intake for protein may be set too low to ensure optimal intake in healthy older adults.
Sayer AA. BMJ 2010; 341:952.

• Attempts to improve muscle mass and function with protein supplementation have had variable results.
• Similarly, findings from observational studies and randomized controlled trials reporting the effects of vitamin D on muscle strength have not been consistent, although some do report benefit.
• Sarcopenia is firmly on the agenda for research into ageing and now needs to be recognized in routine clinical practice.
Sayer AA. BMJ 2010; 341:952.

Il movimento è lo stato dell’uomo e la base della sua essenza. La vita umana non può essere concepibile in senso statico. Dal battere delle palpebre alla massima velocità in corsa, nel sonno o nella piena attività, l’uomo è in movimento.
(Kaplan A)