Tidi d iTerapia radiante dopo ripresa biochimica post-prostatectomia · filippo alongi direttore...
36
T i di d i T erapia radiante dopo ripresa biochimica post-prostatectomia FILIPPO ALONGI DIRETTORE UOC RADIOTERAPIA ONCOLOGICA DIRETTORE UOC RADIOTERAPIA ONCOLOGICA, OSPEDALE SACRO CUORE-DON CALABRIA, NEGRAR-VERONA
Transcript of Tidi d iTerapia radiante dopo ripresa biochimica post-prostatectomia · filippo alongi direttore...

T i di d iTerapia radiante dopo ripresabiochimica post-prostatectomiaFILIPPO ALONGI
DIRETTORE UOC RADIOTERAPIA ONCOLOGICADIRETTORE UOC RADIOTERAPIA ONCOLOGICA,OSPEDALE SACRO CUORE-DON CALABRIA, NEGRAR-VERONA
NOTE ANAMNESTICHE E SITUAZIONE CLINICA ATTUALEATTUALE
• 68 i i t di b ti P• 68 anni, iperteso, non diabetico. Pregressa appendicectomia.
• Mitto ipovalido.• iPSA di 27 6ng/MLiPSA di 27,6ng/ML. • Biopsia prostatica con esito di adenocarcinoma 3+4
di Gl d bi i l bidi Gleason ad entrambi i lobi.• TC addome e Scintigrafia ossea negativi per g g p
secondarismi
NOTE ANAMNESTICHE E SITUAZIONE CLINICA ATTUALEATTUALE
• 68 anni, iperteso, non diabetico. Pregressa appendicectomiaappendicectomia
• Mitto ipovalido.• iPSA di 27,6ng/ML. • Biopsia prostatica con esito di adenocarcinoma 3+4Biopsia prostatica con esito di adenocarcinoma 3+4
di Gleason ad entrambi i lobi.TC dd S i i fi i i• TC addome e Scintigrafia ossea negativi per secondarismi
TERAPIA PER UN RISCHIO ALTO?
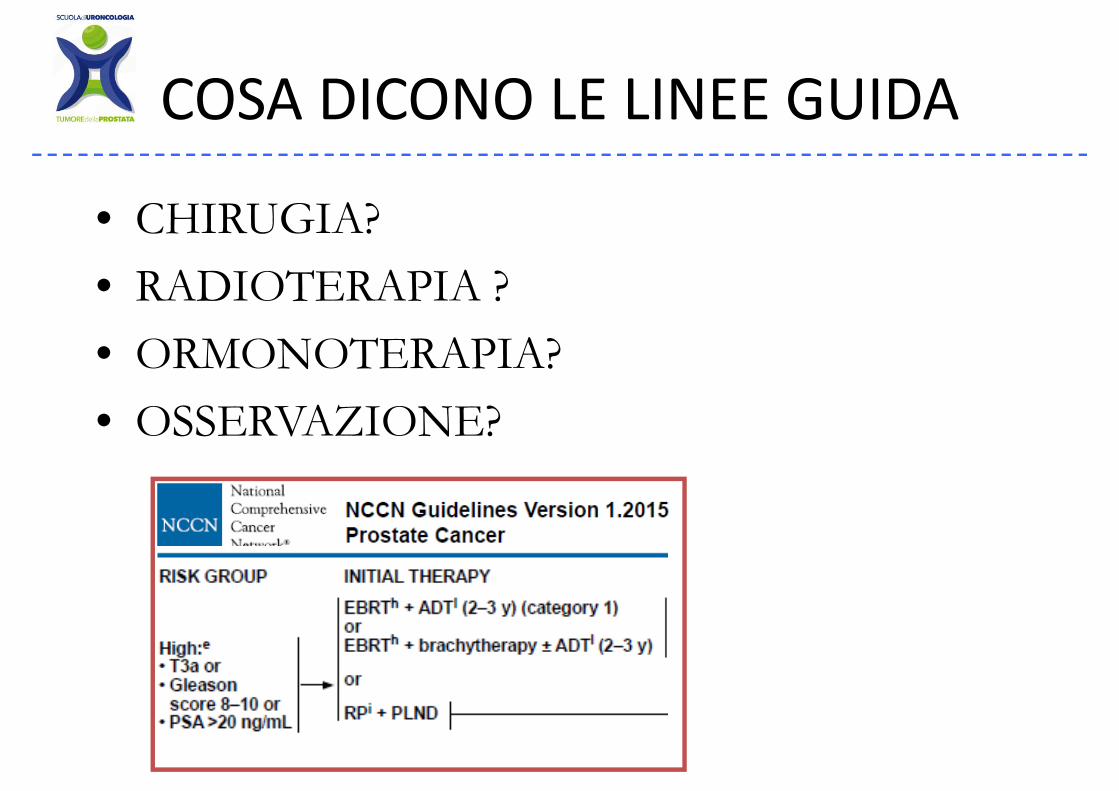
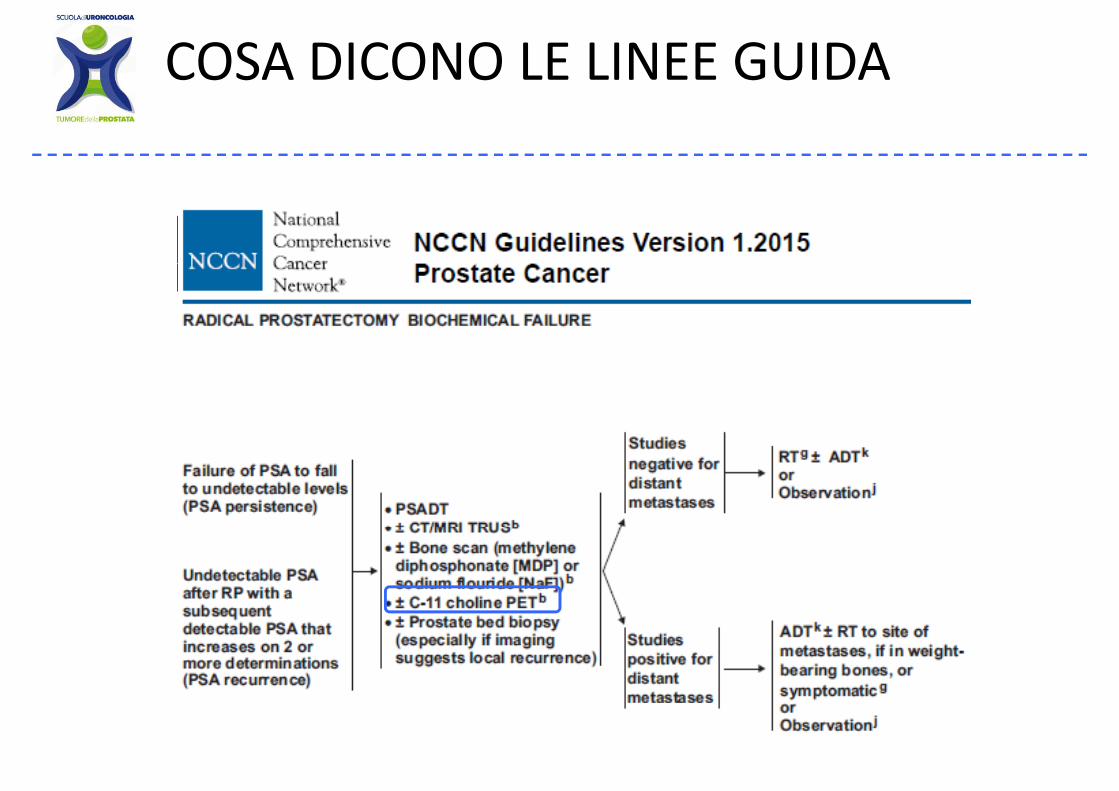
COSA DICONO LE LINEE GUIDACOSA DICONO LE LINEE GUIDA
• CHIRUGIA?• RADIOTERAPIA ?• ORMONOTERAPIA?• ORMONOTERAPIA?• OSSERVAZIONE?
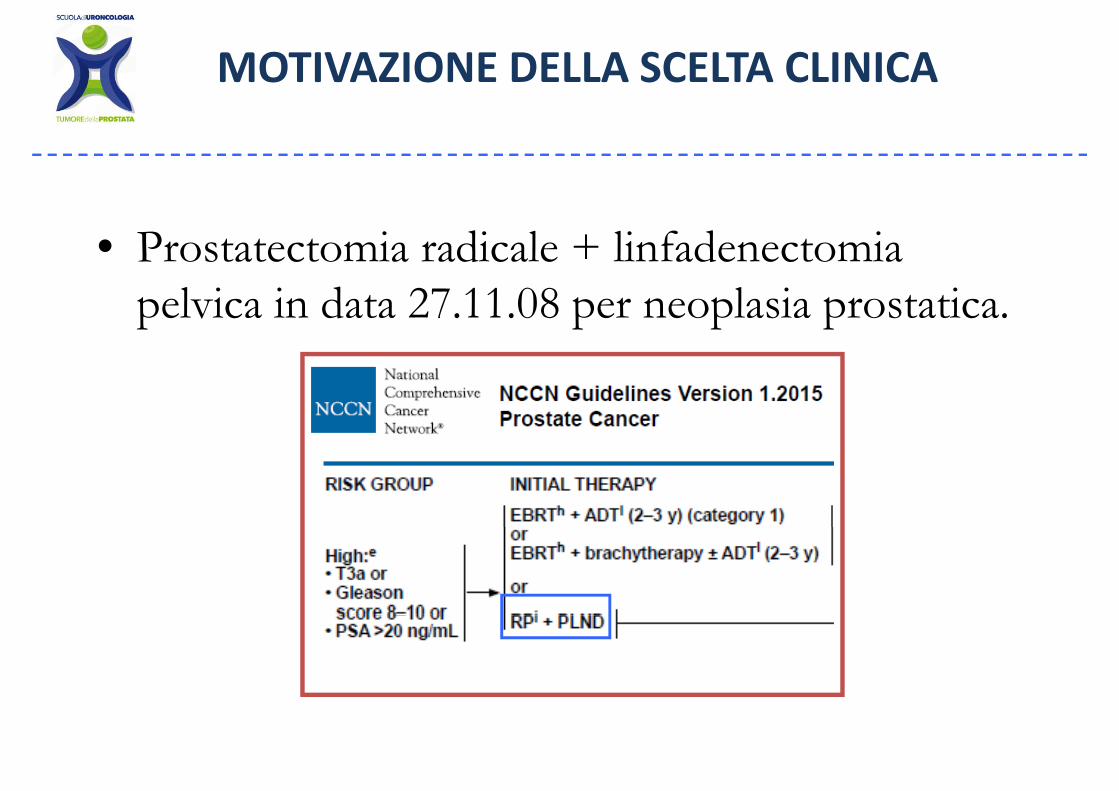
MOTIVAZIONE DELLA SCELTA CLINICA
• Prostatectomia radicale + linfadenectomia pelvica in data 27.11.08 per neoplasia prostatica.
MOTIVAZIONE DELLA SCELTA CLINICA
• Prostatectomia radicale + linfadenectomia pelvica in data 27.11.08 per neoplasia prostatica.
• EI: adenoca gleason 3+4=7 dell'emiprostata destra e sinistra con estensione extra prostaticadestra e sinistra con estensione extra prostatica ed infiltrazione della vescicola seminale sinistra.
T3b N M M i i hi i i i d ipT3b,No, Mx. Margini chirurgici indenni.
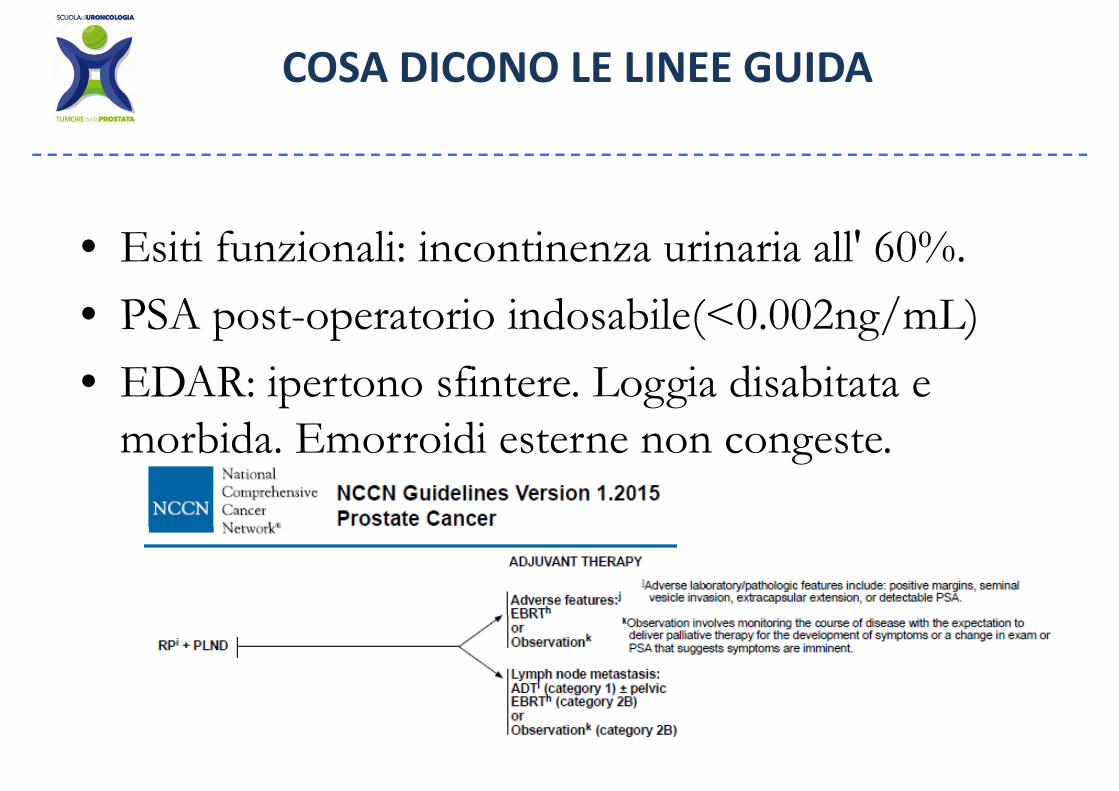
COSA DICONO LE LINEE GUIDA
TERAPIA ADIUVANTE?• RADIOTERAPIA?
ORMONOTERAPIA?• ORMONOTERAPIA?• FOLLOW UP?FOLLOW UP?
COSA DICONO LE LINEE GUIDA
• Esiti funzionali: incontinenza urinaria all' 60%.• PSA post-operatorio indosabile(<0.002ng/mL)• EDAR: ipertono sfintere. Loggia disabitata e
morbida Emorroidi esterne non congestemorbida. Emorroidi esterne non congeste.
COSA DICONO LE LINEE GUIDA
TERAPIA ADIUVANTE?• RADIOTERAPIA?...quindi SI
ORMONOTERAPIA? Q i di NO• ORMONOTERAPIA?...Quindi NO• FOLLOW UP? DOPO RT!!!!!FOLLOW UP?..DOPO RT!!!!!
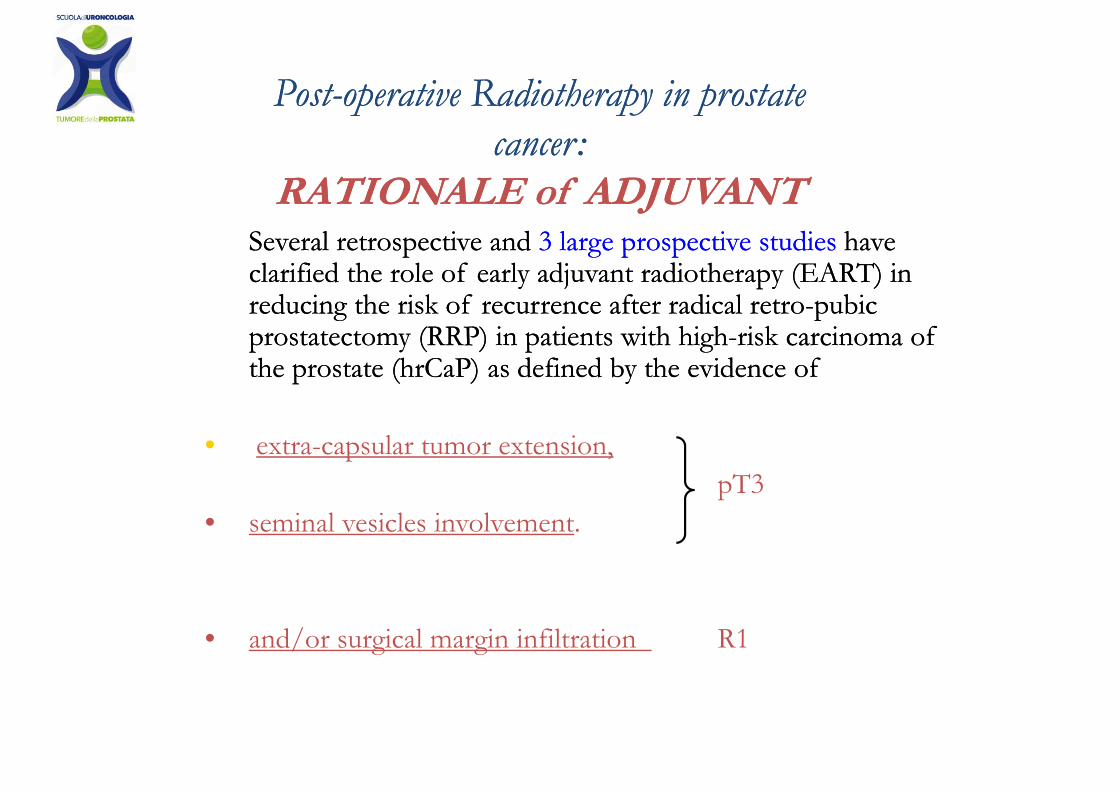
P tP t p tip ti R di th pR di th p i p t ti p t tPostPost--operativeoperative RadiotherapyRadiotherapy in prostate in prostate cancercancer: :
Several retrospective and Several retrospective and 3 large prospective studies3 large prospective studies have have l ifi d h l f l dj di h (EART) il ifi d h l f l dj di h (EART) i
RATIONALE RATIONALE ofof ADJUVANTADJUVANT
clarified the role of early adjuvant radiotherapy (EART) in clarified the role of early adjuvant radiotherapy (EART) in reducing the risk of recurrence after radical retroreducing the risk of recurrence after radical retro--pubic pubic prostatectomy (RRP) in patients with highprostatectomy (RRP) in patients with high--risk carcinoma of risk carcinoma of p y ( ) p gp y ( ) p gthe prostate (the prostate (hrCaPhrCaP) as defined by the evidence of ) as defined by the evidence of
l i• extra-capsular tumor extension, pT3
• seminal vesicles involvementseminal vesicles involvement.
• and/or surgical margin infiltration R1
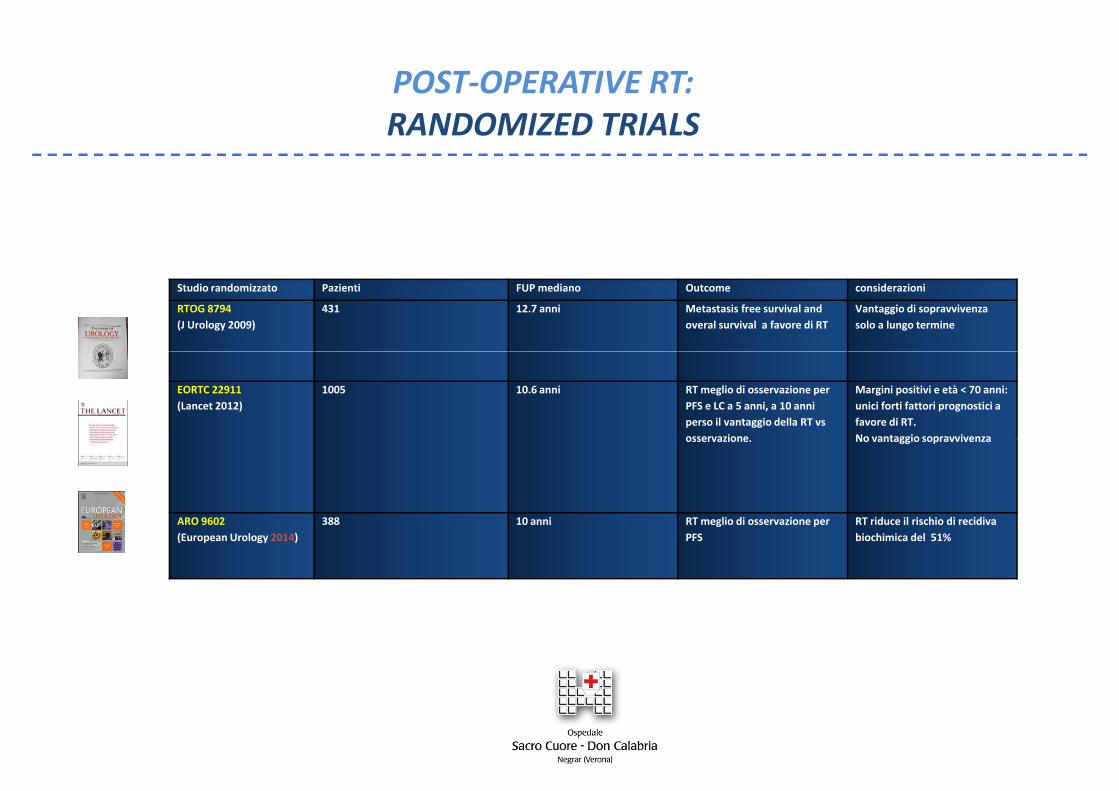
POST‐OPERATIVE RT:POST OPERATIVE RT:RANDOMIZED TRIALS
Studio randomizzato Pazienti FUP mediano Outcome considerazioni
RTOG 8794(J Urology 2009)
431 12.7 anni Metastasis free survival and overal survival a favore di RT
Vantaggio di sopravvivenza solo a lungo termine
EORTC 22911(Lancet 2012)
1005 10.6 anni RT meglio di osservazione per PFS e LC a 5 anni, a 10 anni perso il vantaggio della RT vs osservazione
Margini positivi e età < 70 anni: unici forti fattori prognostici a favore di RT.No vantaggio sopravvivenzaosservazione. No vantaggio sopravvivenza
ARO 9602 388 10 anni RT meglio di osservazione per RT riduce il rischio di recidiva (European Urology 2014) PFS biochimica del 51%
MOTIVAZIONE DELLA SCELTA CLINICA
• RADIOTERAPIA?...sconsigliata dall’urologo per timori di peggioramento incontinenzaper timori di peggioramento incontinenza urinaria
• Attiva FOLLOW UP?..visita urologica ogni 6 i PSA i 3mesi e PSA ogni 3…
SITUAZIONE CLINICA ATTUALEFOLL0W UP
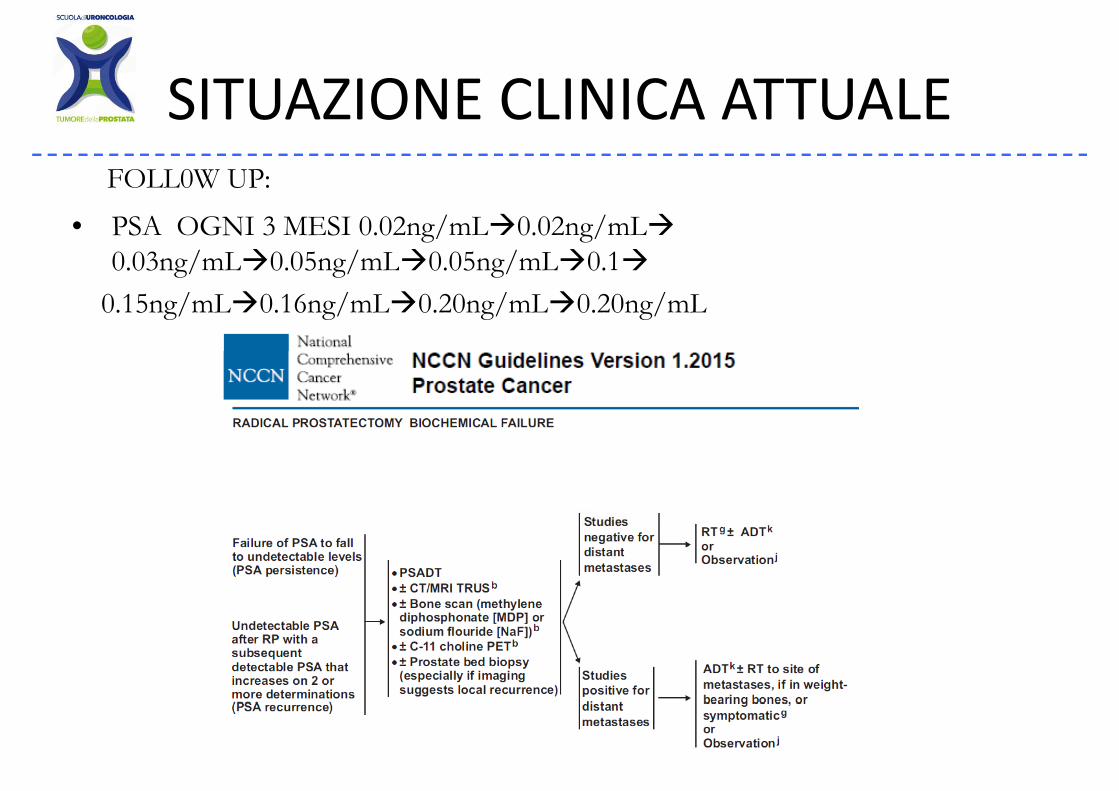
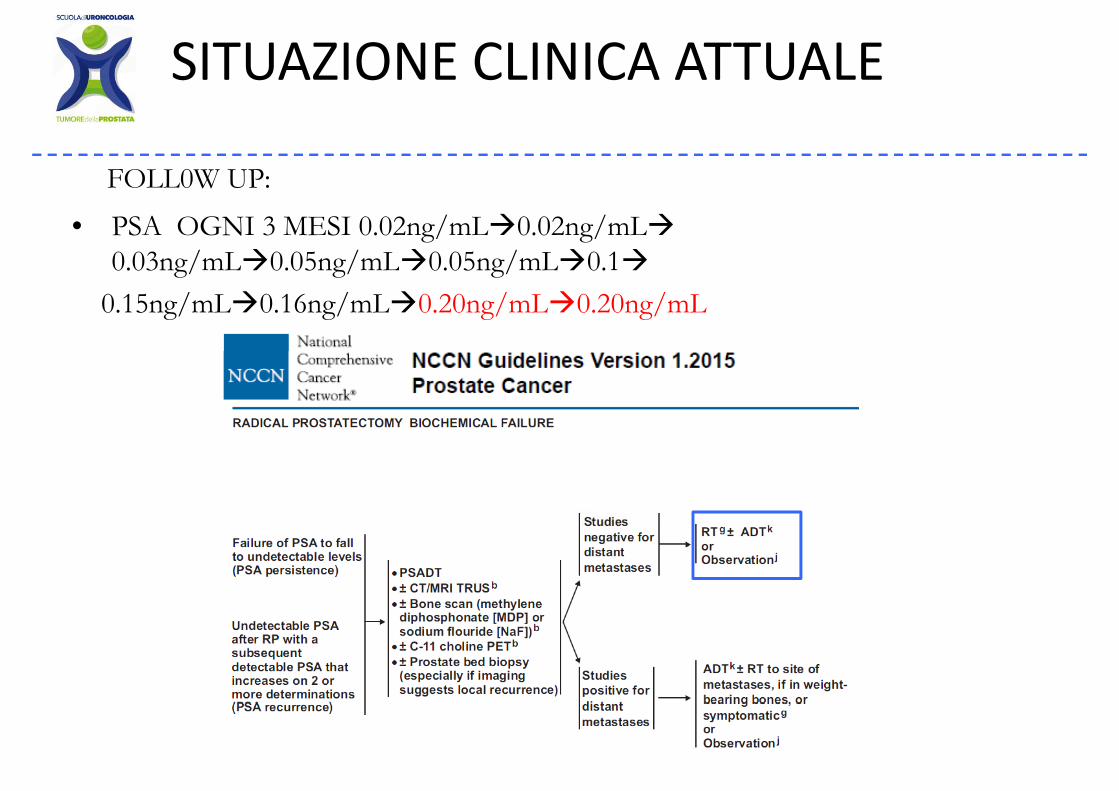
SITUAZIONE CLINICA ATTUALEFOLL0W UP:
• PSA OGNI 3 MESI 0.02ng/mL 0.02ng/mL0 03ng/mL 0 05ng/mL 0 05ng/mL 0 10.03ng/mL 0.05ng/mL 0.05ng/mL 0.1
0.15ng/mL 0.16ng/mL 0.20ng/mL 0.20ng/mL
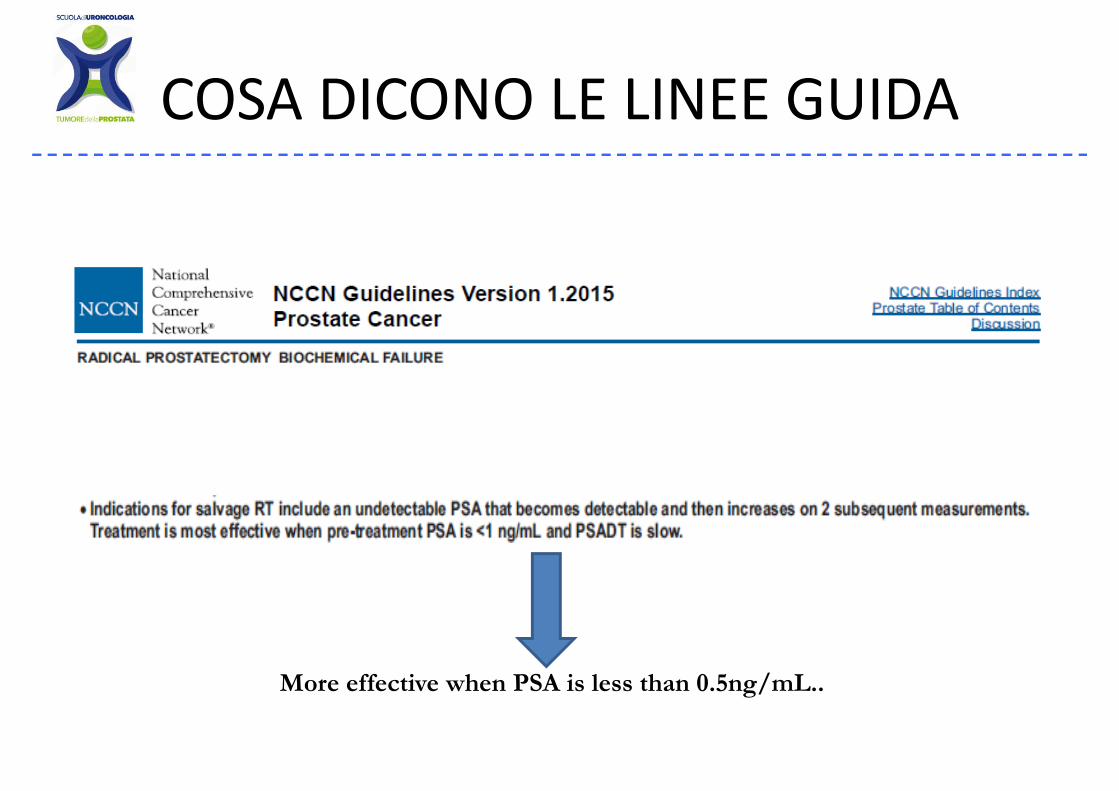
COSA DICONO LE LINEE GUIDACOSA DICONO LE LINEE GUIDA
More effective when PSA is less than 0.5ng/mL..
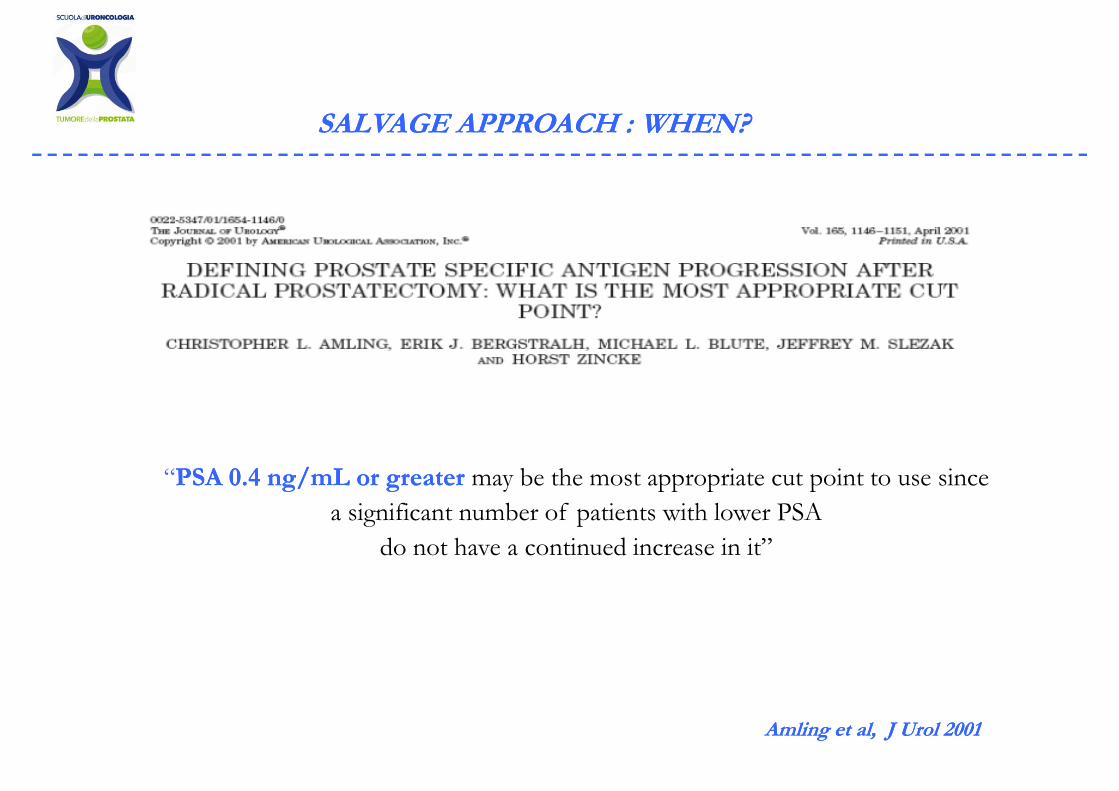
SALVAGE APPROACH : WHEN?SALVAGE APPROACH : WHEN?
“PSA 0.4 ng/mL or greaterPSA 0.4 ng/mL or greater may be the most appropriate cut point to use since a significant number of patients with lower PSA
do not have a continued increase in it”
Amling et al, J Urol 2001Amling et al, J Urol 2001
POST‐OPERATIVE RTPOST OPERATIVE RTSALVAGE TIME?
SALVAGE RT FOR PSA RISE: WHAT IS THE CUT OFF???
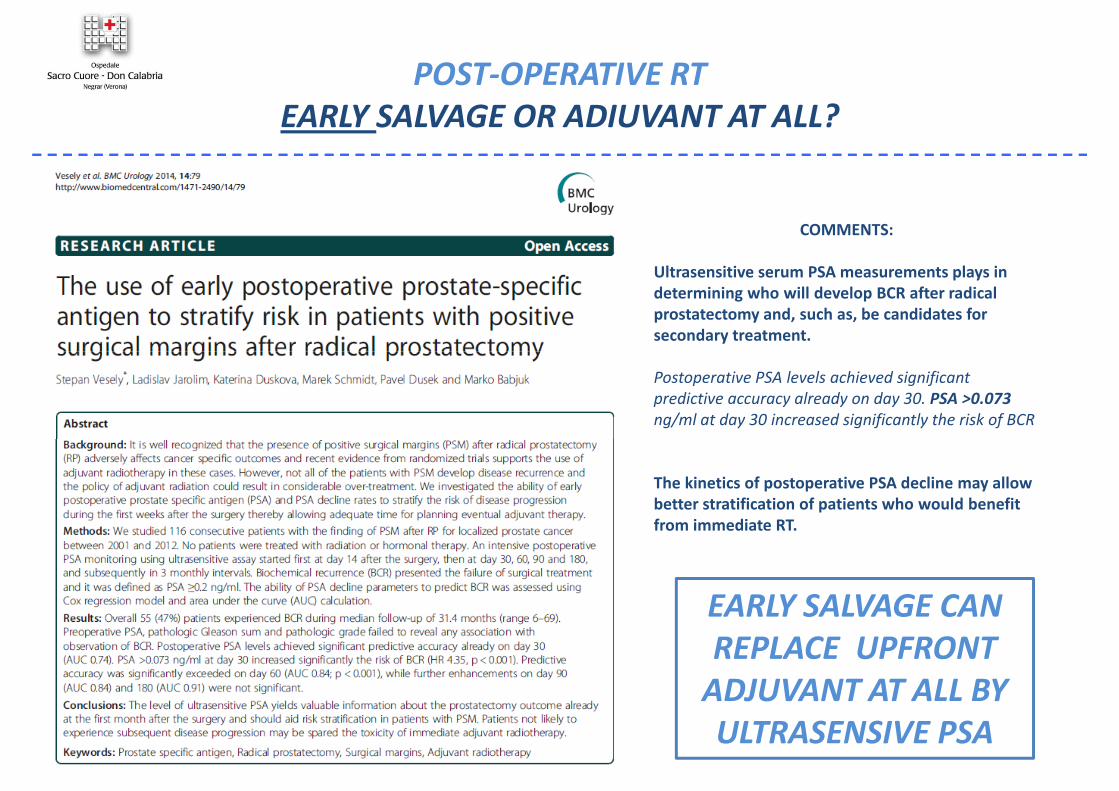
POST‐OPERATIVE RTEARLY SALVAGE OR ADIUVANT AT ALL?
COMMENTS:
Ultrasensitive serum PSA measurements plays in determining who will develop BCR after radical prostatectomy and, such as, be candidates for secondary treatment.
Postoperative PSA levels achieved significant predictive accuracy already on day 30. PSA >0.073 ng/ml at day 30 increased significantly the risk of BCR
The kinetics of postoperative PSA decline may allowbetter stratification of patients who would benefit from immediate RT
EARLY SALVAGE CAN
from immediate RT.
EARLY SALVAGE CAN REPLACE UPFRONT ADJUVANT AT ALL BY ULTRASENSIVE PSA
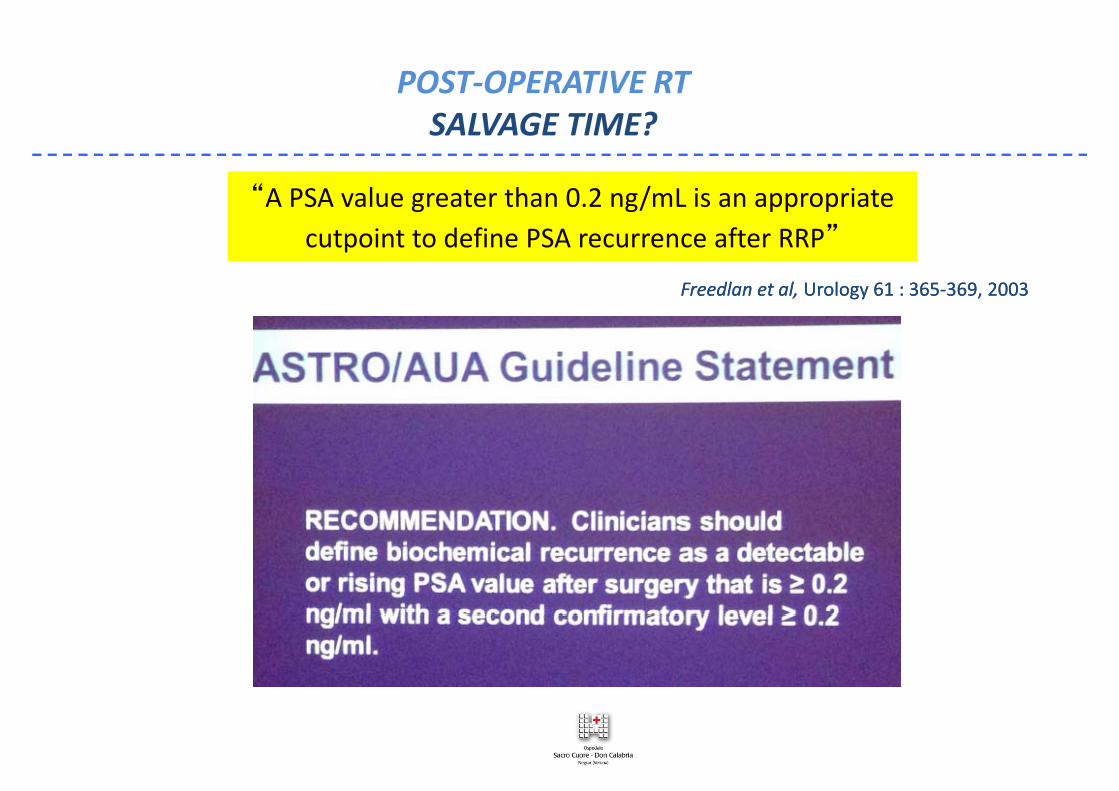
POST‐OPERATIVE RTPOST OPERATIVE RTSALVAGE TIME?
“A PSA value greater than 0.2 ng/mL is an appropriate cutpoint to define PSA recurrence after RRP”
Freedlan et al, Freedlan et al, Urology 61 : 365Urology 61 : 365‐‐369, 2003369, 2003
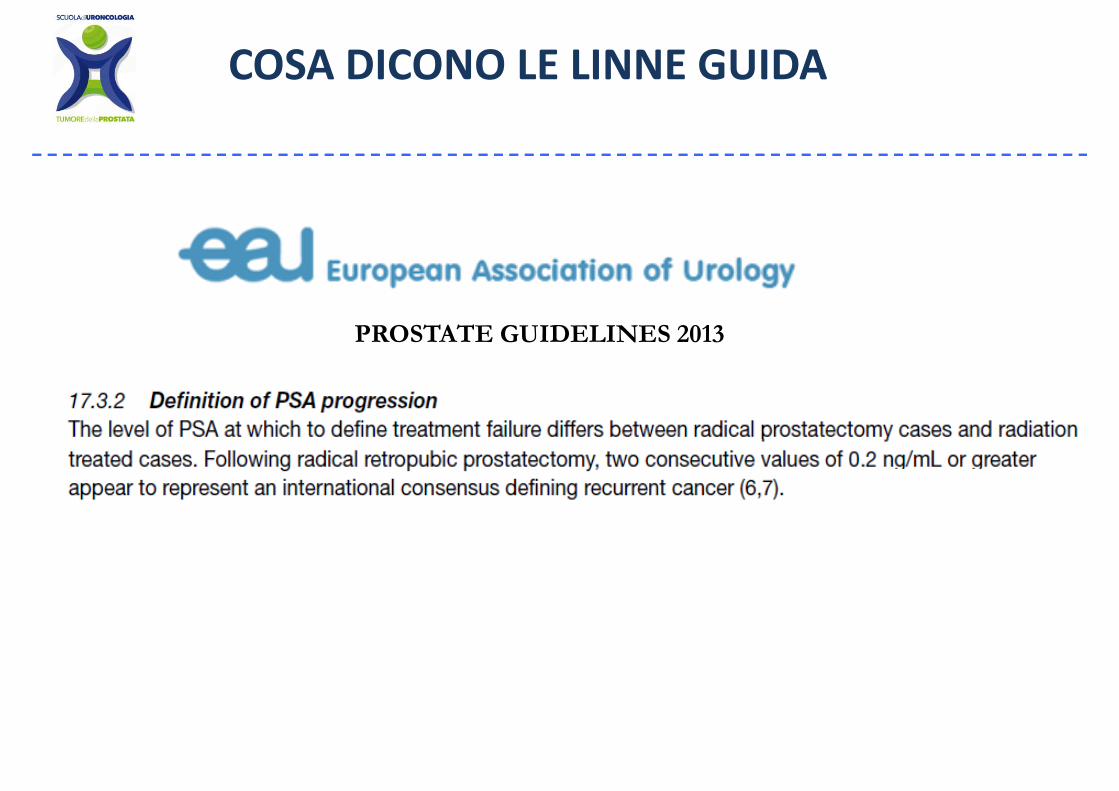
COSA DICONO LE LINNE GUIDA
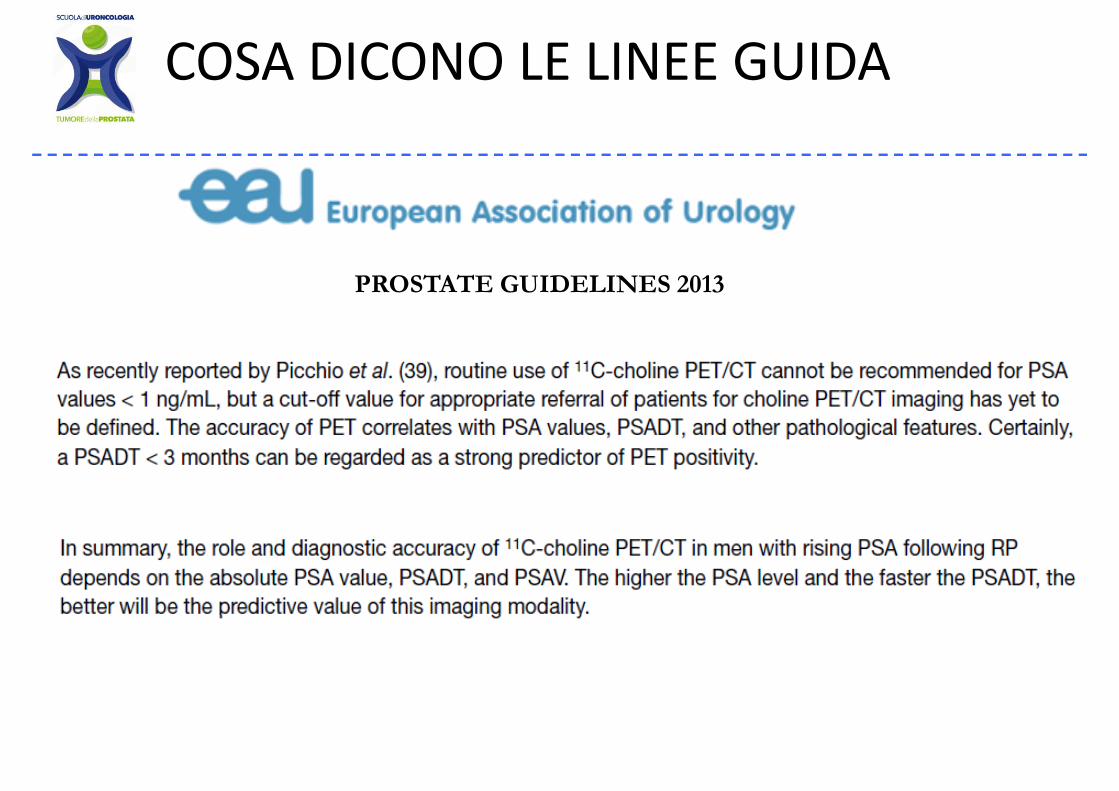
PROSTATE GUIDELINES 2013

SALVAGE APPROACH : WHEN?SALVAGE APPROACH : WHEN?
20122012
SITUAZIONE CLINICA ATTUALE
FOLL0W UPFOLL0W UP:
• PSA OGNI 3 MESI 0.02ng/mL 0.02ng/mL0 03ng/mL 0 05ng/mL 0 05ng/mL 0 10.03ng/mL 0.05ng/mL 0.05ng/mL 0.1
0.15ng/mL 0.16ng/mL 0.20ng/mL 0.20ng/mL
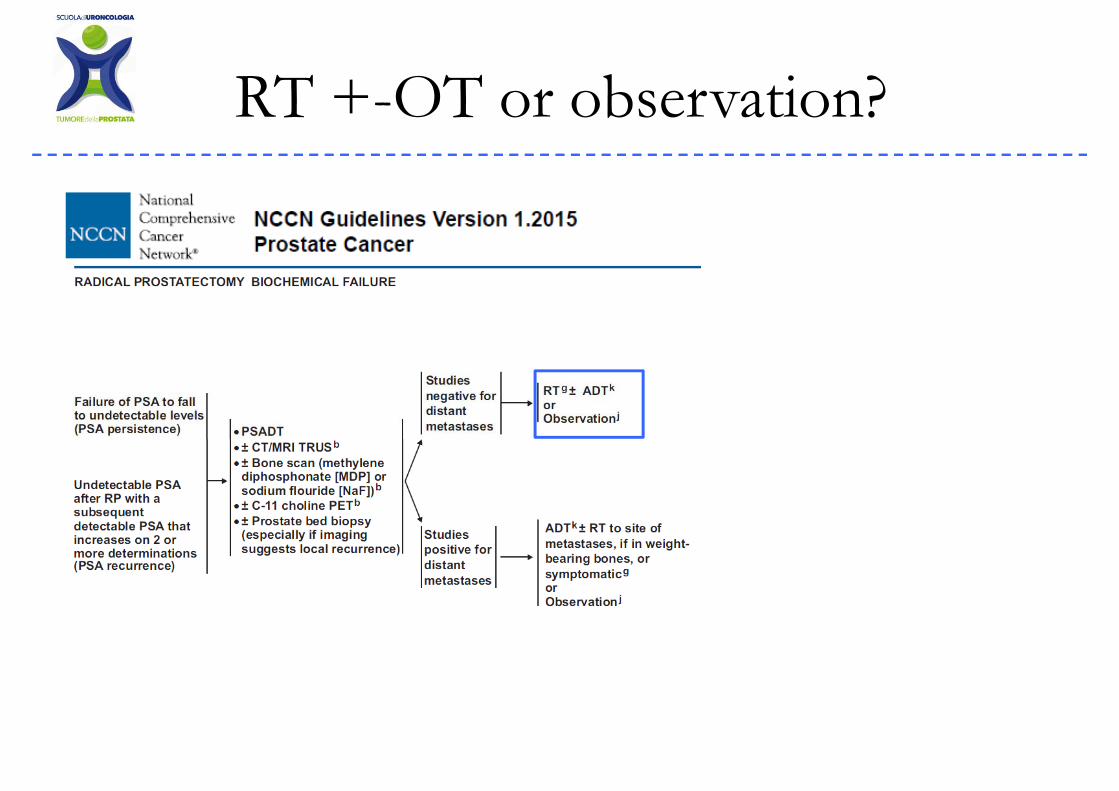
RT + OT b ti ?RT +-OT or observation?
20022002
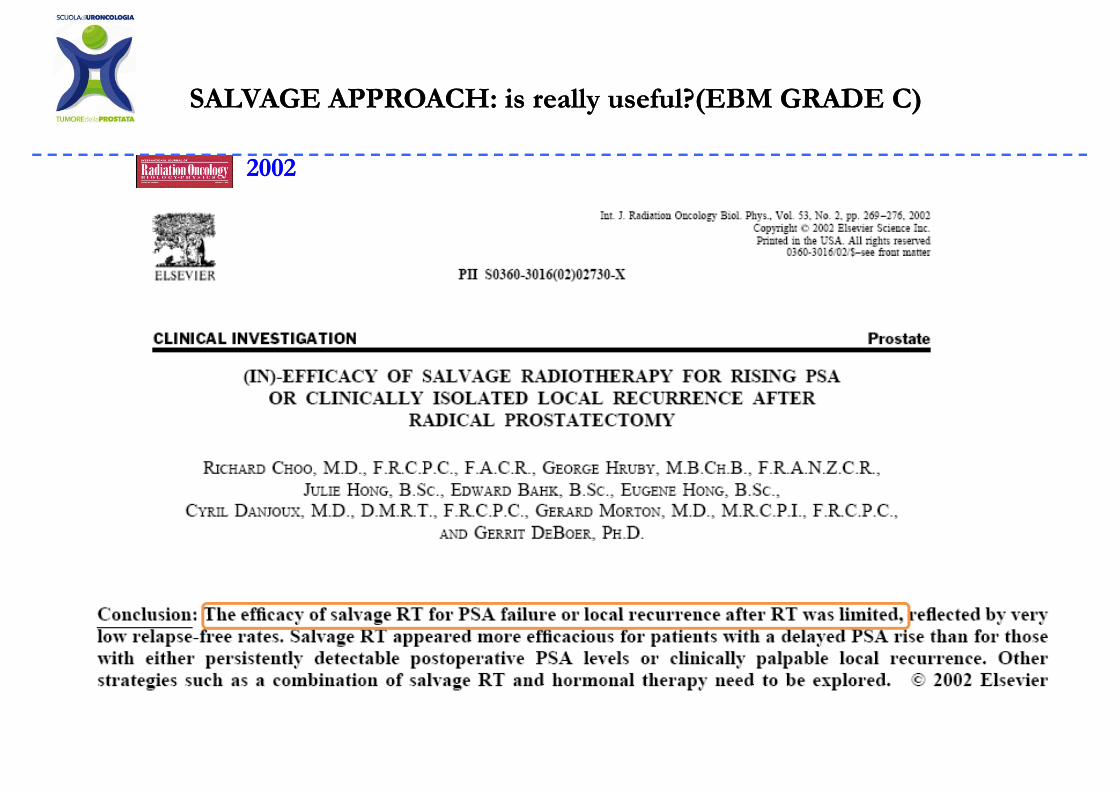
SALVAGE APPROACH: SALVAGE APPROACH: isis reallyreally usefuluseful?(EBM GRADE C) ?(EBM GRADE C)
20022002
SALVAGE APPROACH: SALVAGE APPROACH: isis reallyreally usefuluseful?(EBM GRADE C) ?(EBM GRADE C)
…HOWEVER..
For patients with recurrent prostate cancer after radical….For patients with recurrent prostate cancer after radicalprostatectomy, SALVAGE RT remains the only
potentially curative therapypotentially curative therapy.
Stephenson et al, JAMA 291 : 1325, 2004
C di l Li G idCosa dicono le Linee‐Guida
C di l Li G idCosa dicono le Linee‐Guida
HORMONAL THERAPY(CONCOMITANT/ADJUVANT)?HORMONAL THERAPY(CONCOMITANT/ADJUVANT)?
The potential benefit deriving The potential benefit deriving from the addition of adjuvant from the addition of adjuvant from the addition of adjuvant from the addition of adjuvant androgen deprivation (AAD) to androgen deprivation (AAD) to EART remains to be clarified in EART remains to be clarified in
ffterm of:term of:•• Timing Timing
D iD i•• DurationDuration•• TypeType•• Side effectsSide effects•• Side effectsSide effects
2004200419981998
SCELTA TERAPEUTICA
Effettua Radioterapia: 70 Gy in 35 sedute.L di i d i l iLamenta disuria e modesto tenesmo autorisolti.
• PSA ogni 3-4 mesi:0.1ng/mL 0.08ng/mL <0.01 ng/mL…•Dopo 1 anno dalla RT: PSA ogni 6 mesi …0.5ng/mL 0.6 0.8ng/mL 1.4ng/mL…0.5ng/mL 0.6 0.8ng/mL 1.4ng/mL
COSA DICONO LE LINEE GUIDA
COSA DICONO LE LINEE GUIDA
PROSTATE GUIDELINES 2013
SITUAZIONE CLINICA ATTUALE
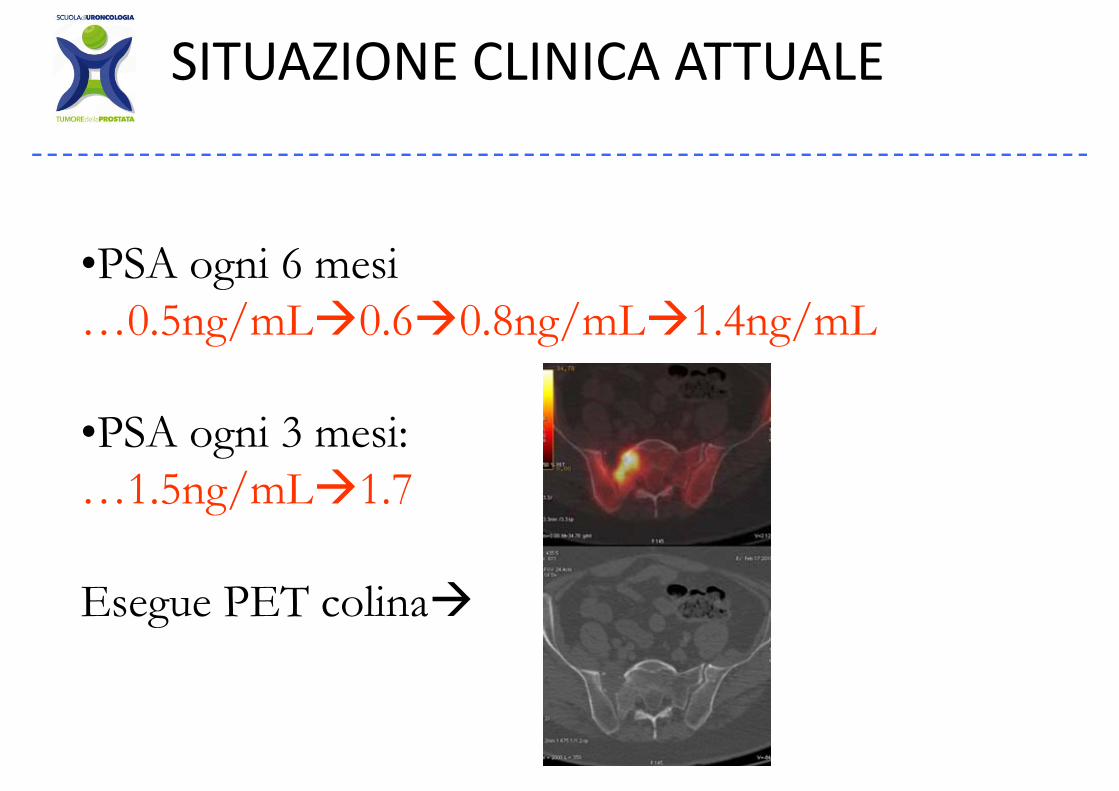
•PSA ogni 6 mesi•PSA ogni 6 mesi …0.5ng/mL 0.6 0.8ng/mL 1.4ng/mL
•PSA ogni 3 mesi:PSA ogni 3 mesi:…1.5ng/mL 1.7
Esegue PET colinaEsegue PET colina
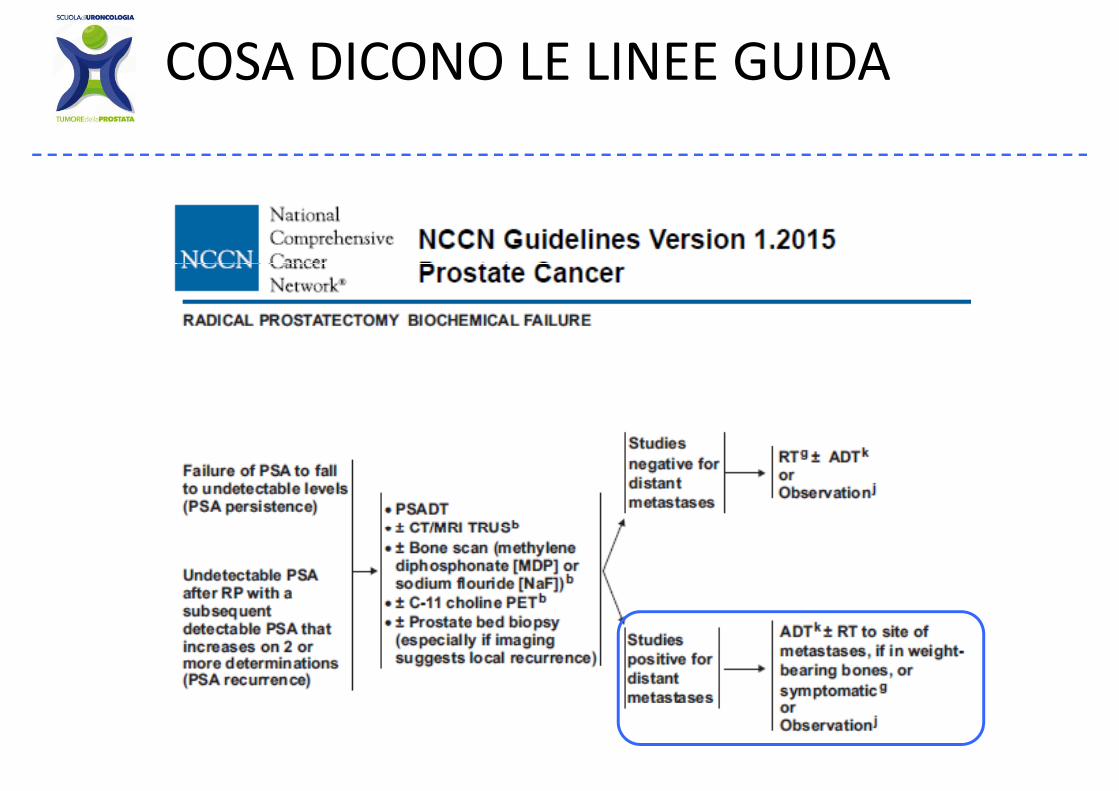
COSA DICONO LE LINEE GUIDA
Paziente di anni 68 anni
• Esegue PET colina che documenta i f l i iprogressione ossea focale non sintomatica e non
a rischio di frattura. • Attiva terapia ormonale con BAT, attualmente in
SA i d bilcorso con PSA indosabile.
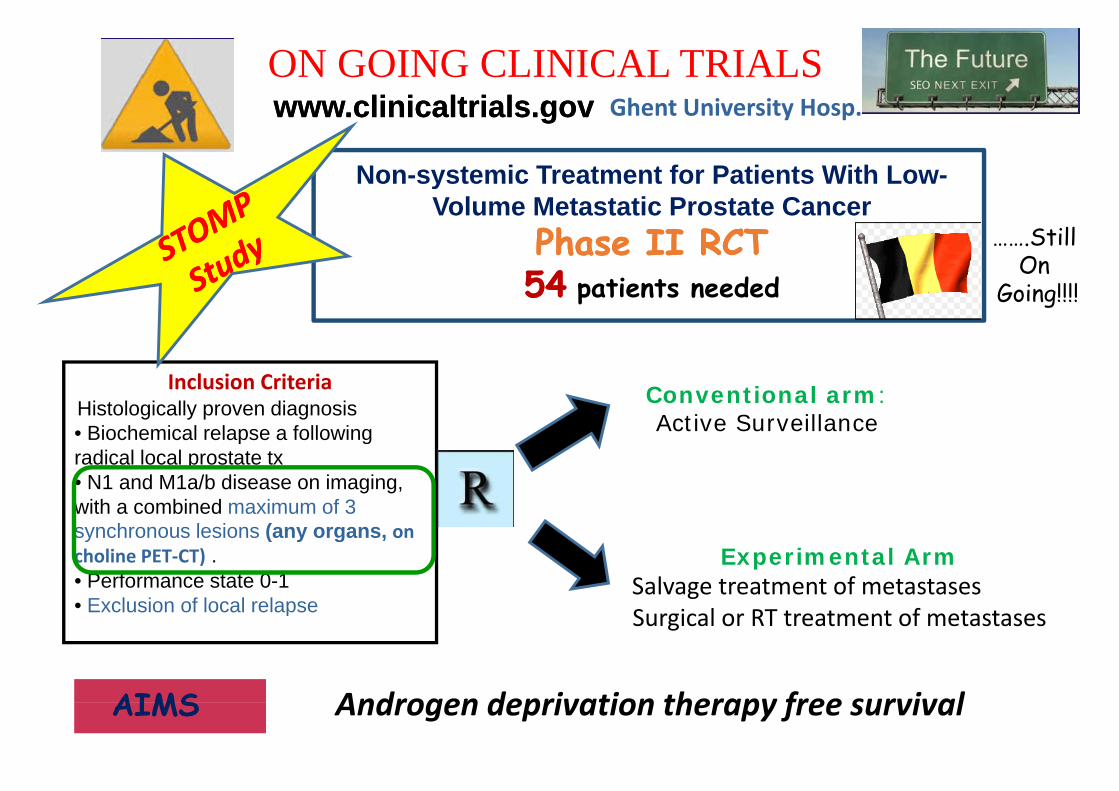
ON GOING CLINICAL TRIALSwww.clinicaltrials.govwww.clinicaltrials.gov
Non-systemic Treatment for Patients With Low-
Ghent University Hosp.
Non-systemic Treatment for Patients With Low-Volume Metastatic Prostate Cancer
Phase II RCTPhase II RCT …….StillOn5454 patients neededOn
Going!!!!
Inclusion CriteriaHistologically proven diagnosis• Biochemical relapse a following
Conventional arm: Active SurveillanceBiochemical relapse a following
radical local prostate tx• N1 and M1a/b disease on imaging, with a combined maximum of 3 s nchrono s lesions (an organssynchronous lesions (any organs, on choline PET‐CT) .• Performance state 0-1• Exclusion of local relapse
Experimental ArmSalvage treatment of metastasesSurgical or RT treatment of metastases
Androgen deprivation therapy free survivalAIMS
p Surgical or RT treatment of metastases
Androgen deprivation therapy free survivalAIMS
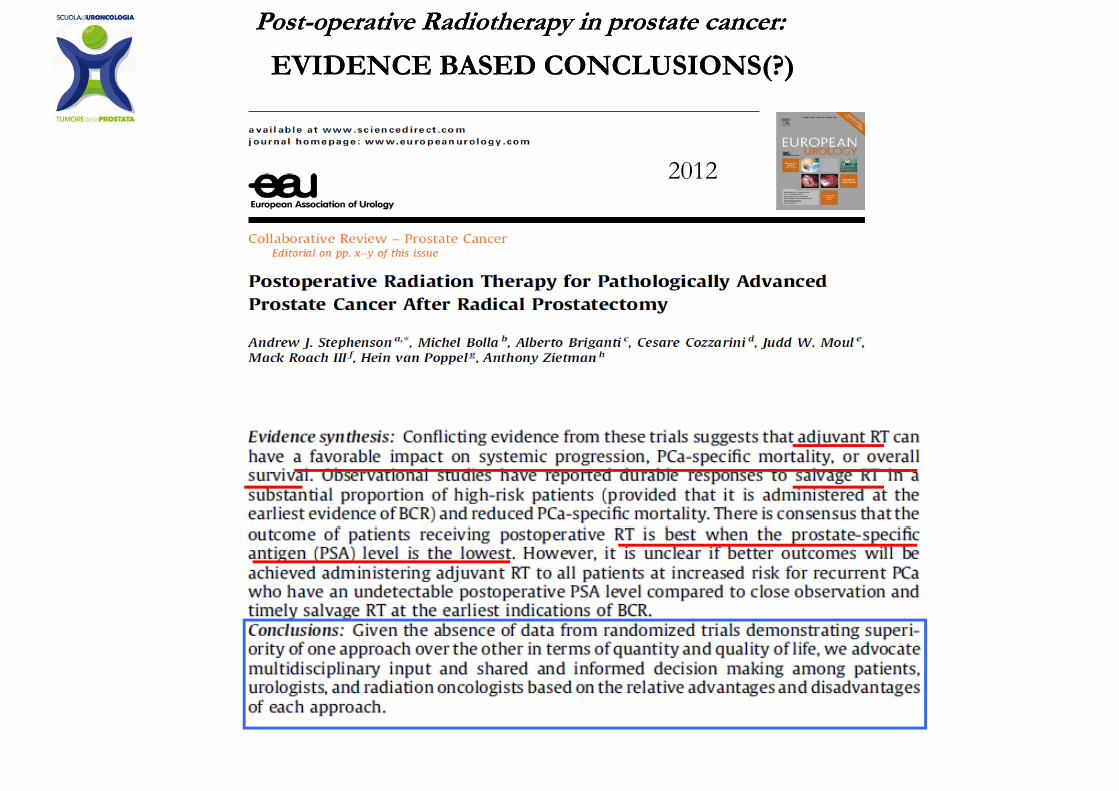
EVIDENCE BASED CONCLUSIONS(?)EVIDENCE BASED CONCLUSIONS(?)
PostPost--operativeoperative RadiotherapyRadiotherapy in prostate in prostate cancercancer::
20122012