Sandro Mazzaferro Il Trattamento dei Disturbi del Metabolismo Minerale nell’IRC AGGIORNAMENTI IN...
56
Sandro Mazzaferro Il Trattamento dei Disturbi del Metabolismo Minerale nell’IRC AGGIORNAMENTI IN NEFROLOGIA CLINICA XIII Incontro Teramo, 11-12 ottobre 2013 Aula Convegni II Lotto Aspetti fisiopatologici ed epidemiologici (Manoppello – PE)
-
Upload
william-norman -
Category
Documents
-
view
216 -
download
0
Transcript of Sandro Mazzaferro Il Trattamento dei Disturbi del Metabolismo Minerale nell’IRC AGGIORNAMENTI IN...

Sandro Mazzaferro
Il Trattamento dei Disturbi del Metabolismo Minerale nell’IRC
AGGIORNAMENTIIN NEFROLOGIA CLINICA
XIII IncontroTeramo, 11-12 ottobre 2013
Aula Convegni II Lotto
Aspetti fisiopatologici ed epidemiologici
(Manoppello – PE)
Disturbances of Mineral Metabolism in CRF involve … …
2
A possible «rule of … … …»
3
IONS
At least …
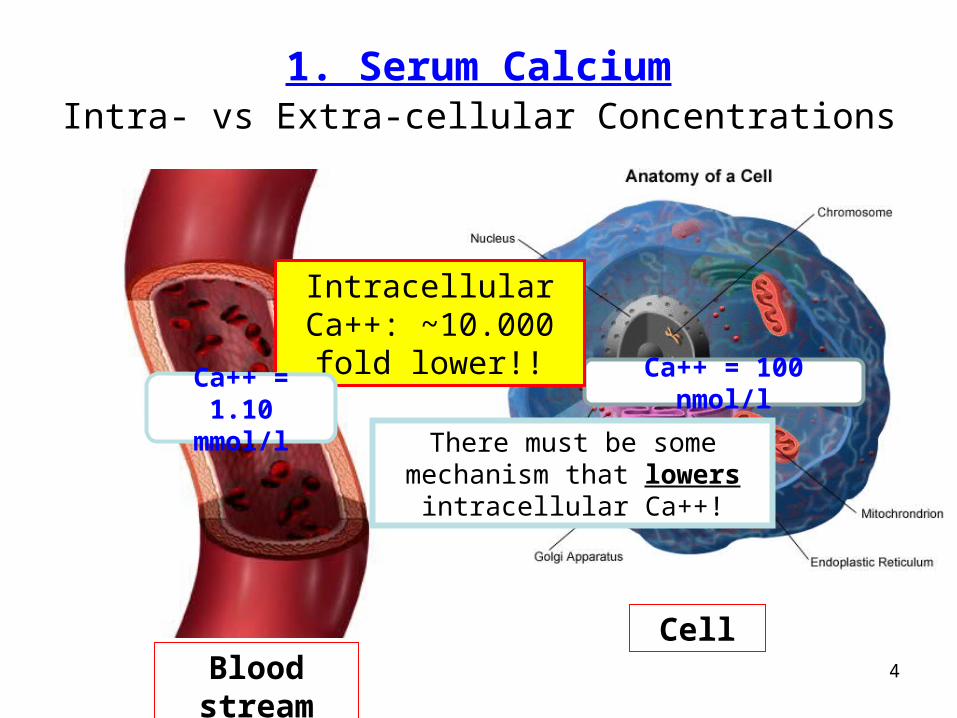
1. Serum CalciumIntra- vs Extra-cellular Concentrations
Blood streamCell
Ca++ = 100 nmol/l
Intracellular Ca++: ~10.000 fold lower!!
Ca++ = 1.10 mmol/l
4
There must be some mechanism that lowers
intracellular Ca++!
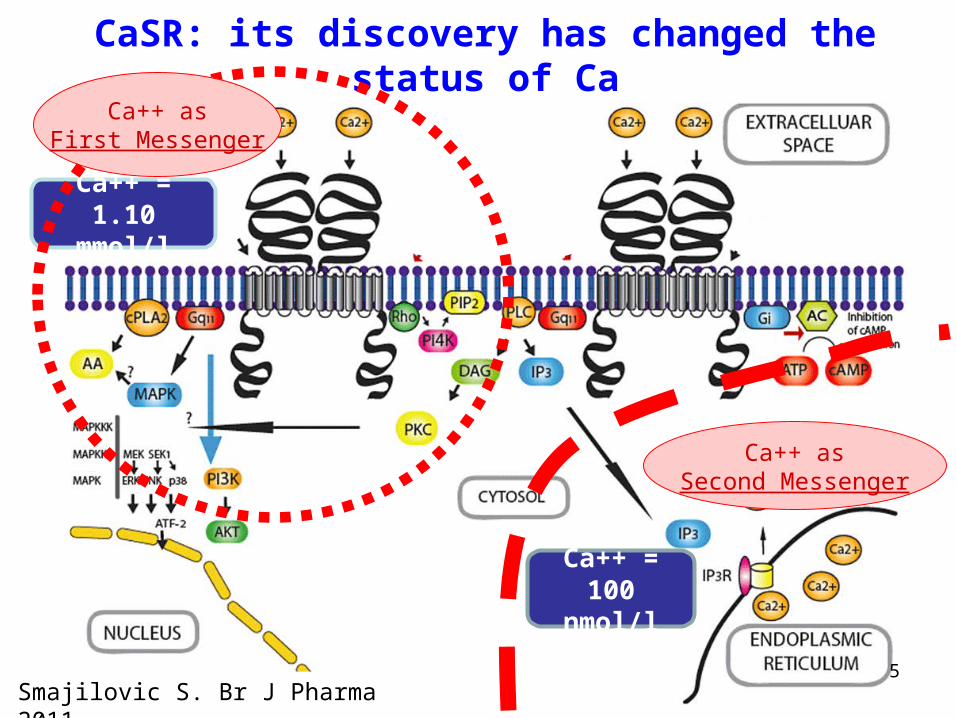
Ca++ asSecond Messenger
Smajilovic S. Br J Pharma 2011
CaSR: its discovery has changed the status of Ca
5
Ca++ = 100 nmol/l
Ca++ = 1.10 mmol/l
Ca++ asFirst Messenger
Ca derangements in CRF• Hypo-Calcemia and/or negative Ca
balance:– Anxiety, Paresthesias, Cramps, Tetany, Seizures,
Abdominal pain, Congestive heart failure, Calcifications, etc.
– High PTH, High turnover bone, Osteopenia• Hyper-Calcemia and/or positive Ca
balance:– Weakness, Nausea, Vomiting, Polyuria,
Polydipsia, Hypertension, Lethargy, Coma– Low PTH, Low turnover bone, Calcifications
6
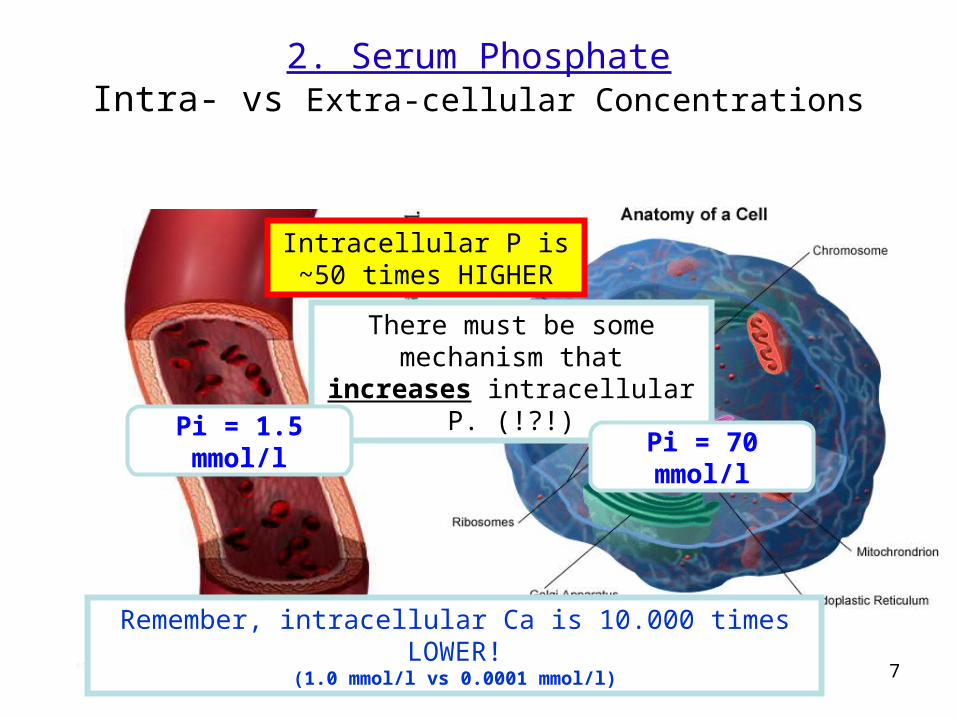
2. Serum PhosphateIntra- vs Extra-cellular Concentrations
Intracellular P is ~50 times HIGHER
Blood streamCell
Remember, intracellular Ca is 10.000 times LOWER!(1.0 mmol/l vs 0.0001 mmol/l)
There must be some mechanism that increases
intracellular P. (!?!)
7
Pi = 1.5 mmol/lPi = 70 mmol/l
Pi Receptor?
8
No Pi Receptor identified so far.
Derangements of Pi in CRF• Hypo-Phosphatemia and/or negative Pi
balance:– Low cardiac output, Arrhytmia, Hypotension,
Astenia, Confusion, Seizures, Coma– High insulin, Low PTH, Pseudofractures,
Osteomalacia• Hyper-Phosphatemia and/or positive Pi
balance:– Hypocalcemia, Hypotension, Excitability,– High PTH, High turnover, Calcification
9
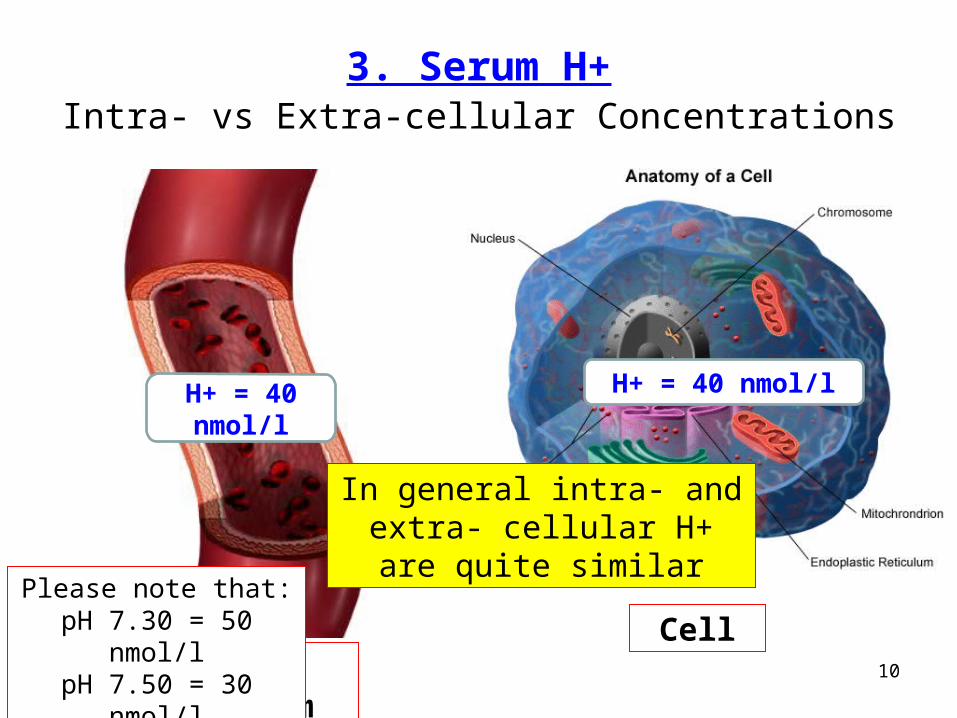
3. Serum H+Intra- vs Extra-cellular Concentrations
Blood streamCell
H+ = 40 nmol/l
In general intra- and extra- cellular H+ are quite similar
H+ = 40 nmol/l
10
Please note that:pH 7.30 = 50 nmol/lpH 7.50 = 30 nmol/l
Derangements of H+ in CRF
• Acidosis and/or Acidemia:– Fatigue, tachipnea, sleepness, confusion,
coma– Osteopenia/Malacia
• Alkalosis and/or Alkalemia:– Anxiety, nausea, tremor, twitching, spasm,
numbness, dizziness, coma – Calcifications
11

12
HORMONES
At least …
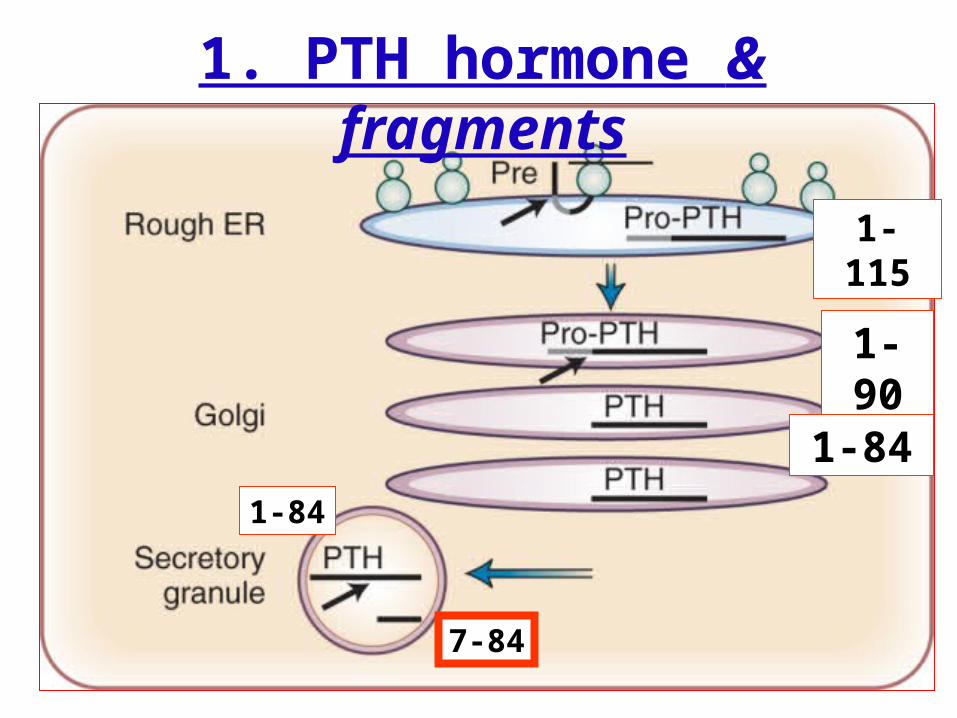
1. PTH hormone & fragments
1-115
1-90
1-84
1-84
7-84
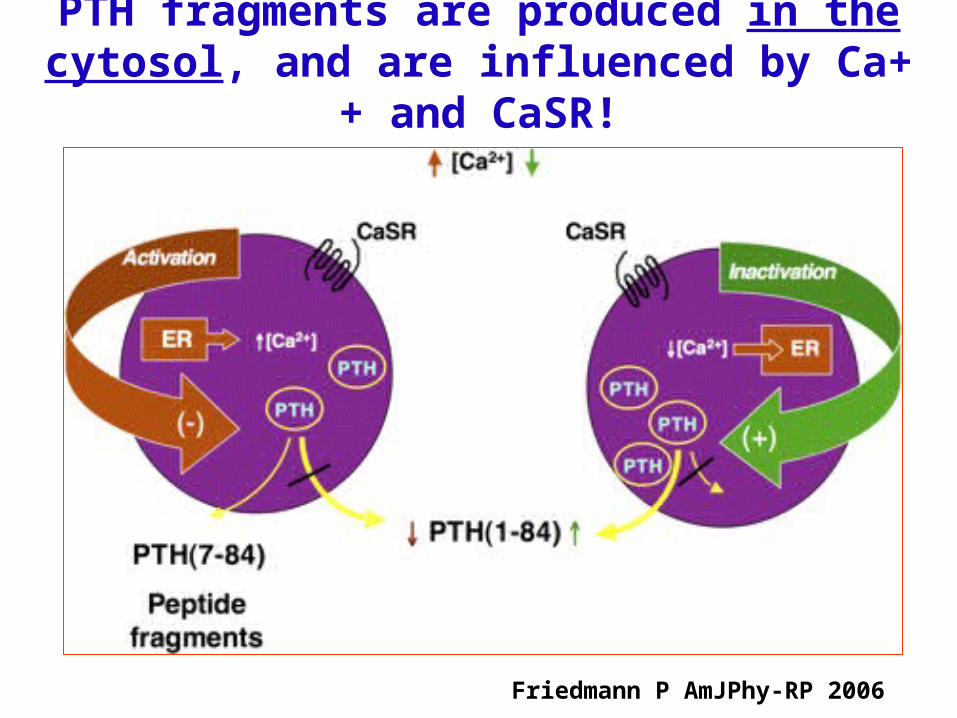
PTH fragments are produced in the cytosol, and are influenced by Ca++ and CaSR!
Friedmann P AmJPhy-RP 2006
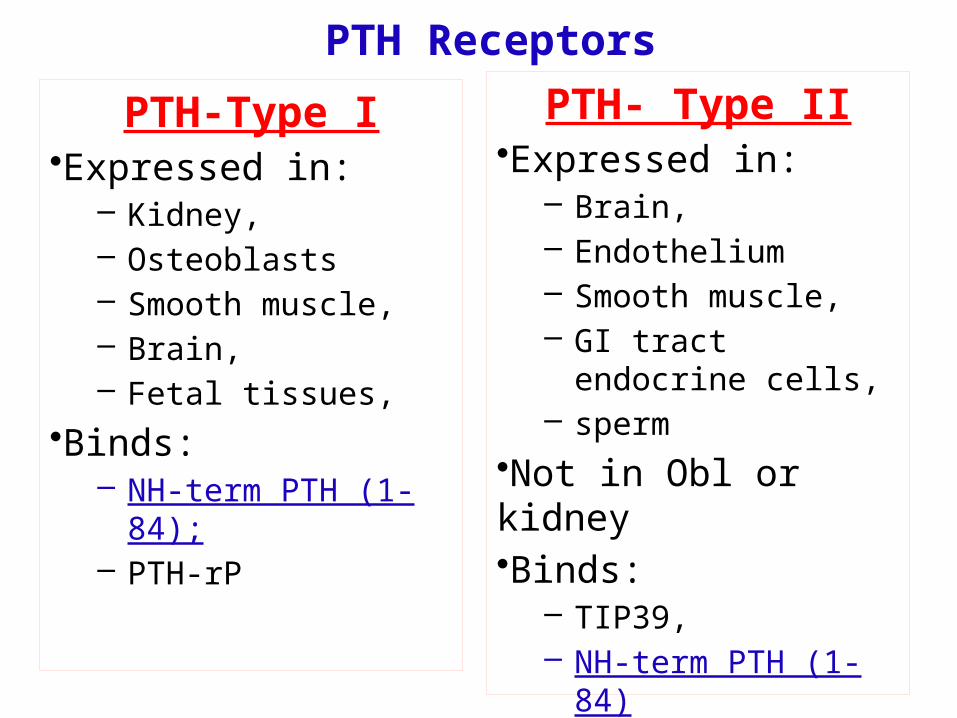
PTH-Type I•Expressed in:
– Kidney, – Osteoblasts– Smooth muscle,– Brain,– Fetal tissues,
•Binds:– NH-term PTH (1-84);– PTH-rP
PTH- Type II•Expressed in:
– Brain,– Endothelium– Smooth muscle,– GI tract endocrine
cells,– sperm
•Not in Obl or kidney•Binds:
– TIP39,– NH-term PTH (1-84)
PTH Receptors
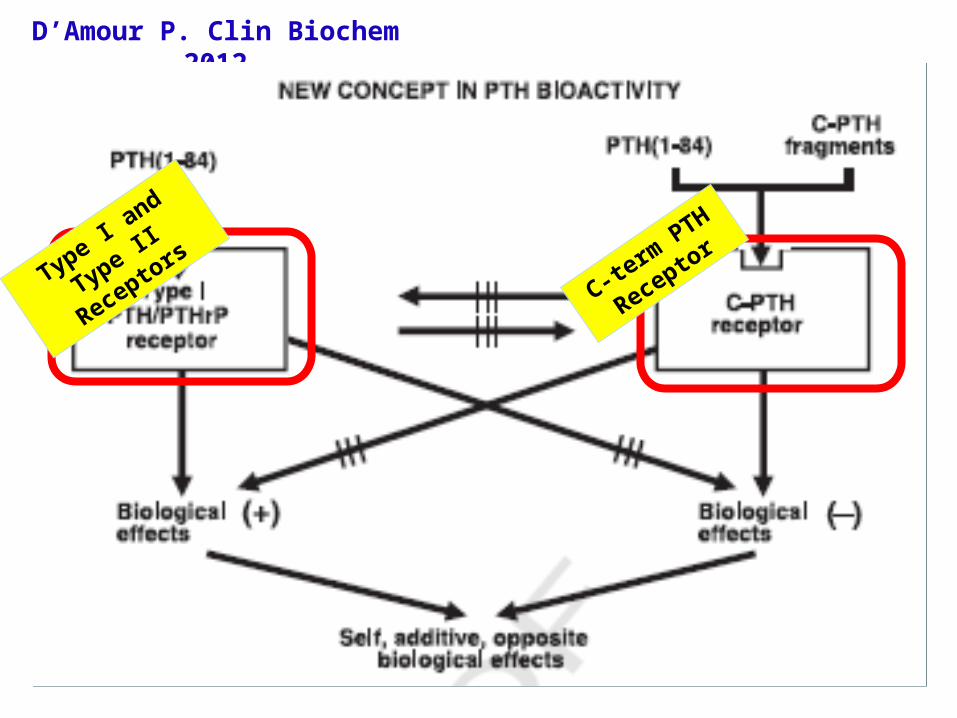
D’Amour P. Clin Biochem 2012
Type I and Type
II Receptors
C-term
PTH
Receptor
Derangements of PTH in CRF
• Hypoparathyroidism:– Low Ca, high Pi, low AP – Low turnover bone, Ectopic calcification
• Hyperparathyroidism:– High Ca, high Pi, high AP– High turnover bone, Ectopic calcification
17
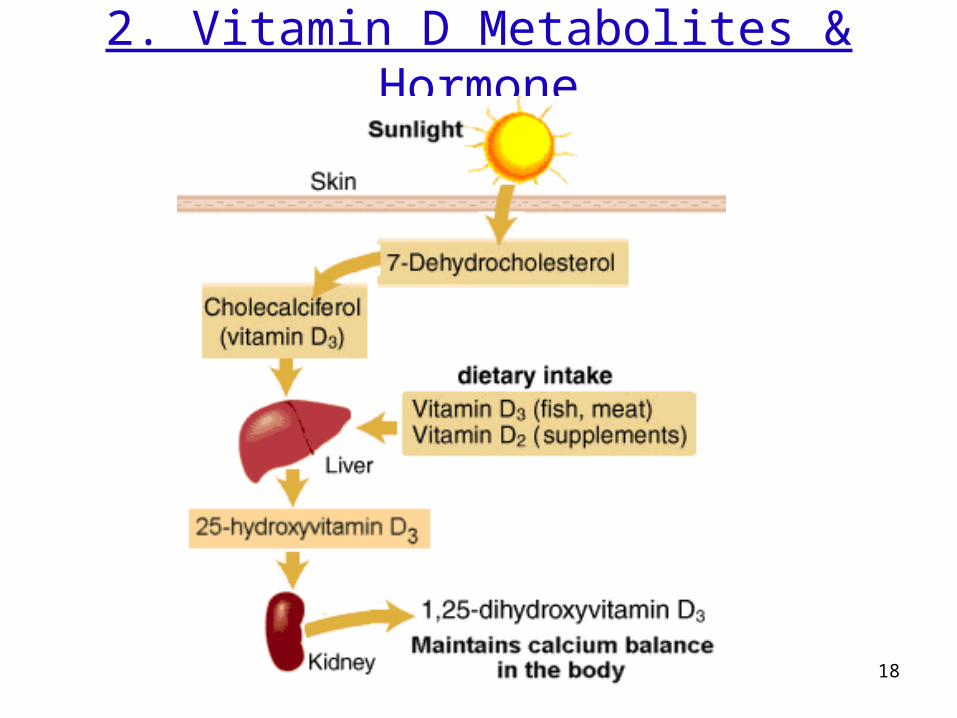
2. Vitamin D Metabolites & Hormone
18
19
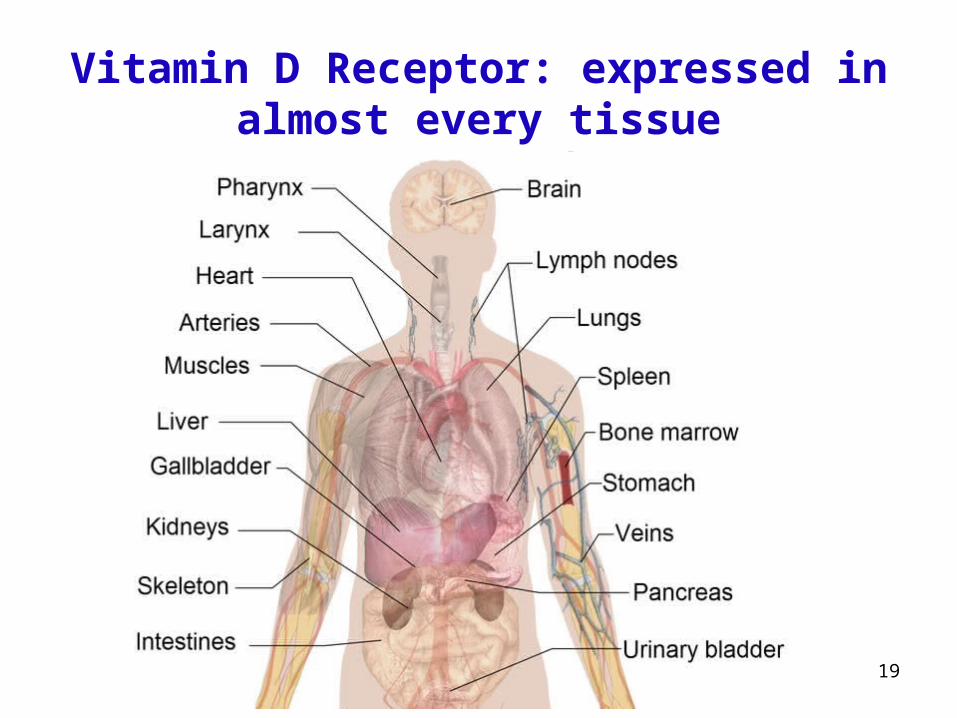
Vitamin D Receptor: expressed in almost every tissue
Derangements of Vitamin D in CRF
• Hypovitaminosis D:– HypoCa, high PTH, high AP– Bone Resorption/Osteomalacia/Penia– Other (pleiotropic?)
• Hypervitaminosis D:– Hyper Ca, low-high PTH, low-high AP– Bone mineralization, low turnover– Ectopic Calcifications– Other (pleiotropic?)
20
3. FGF23-Klotho
Why together?
• FGF23 null vs Klotho null transgenic mice
21
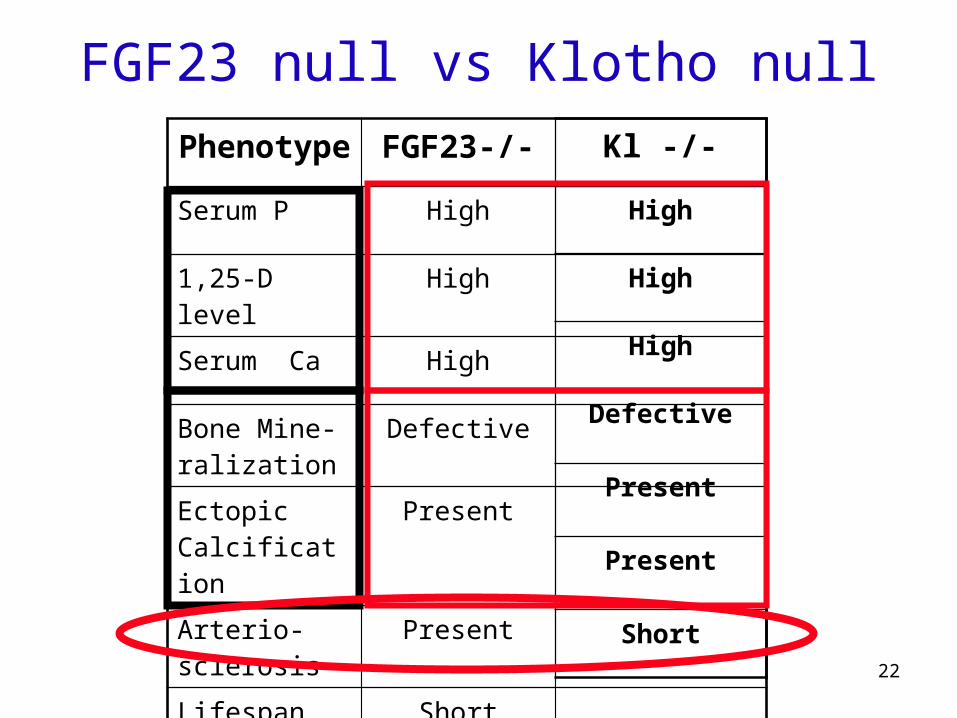
FGF23 null vs Klotho null
22
Phenotype FGF23-/-
Serum P High
1,25-D level High
Serum Ca High
Bone Mine-ralization
Defective
Ectopic Calcification
Present
Arterio- sclerosis
Present
Lifespan Short
Kl -/-
High
High
High
Defective
Present
Present
Short
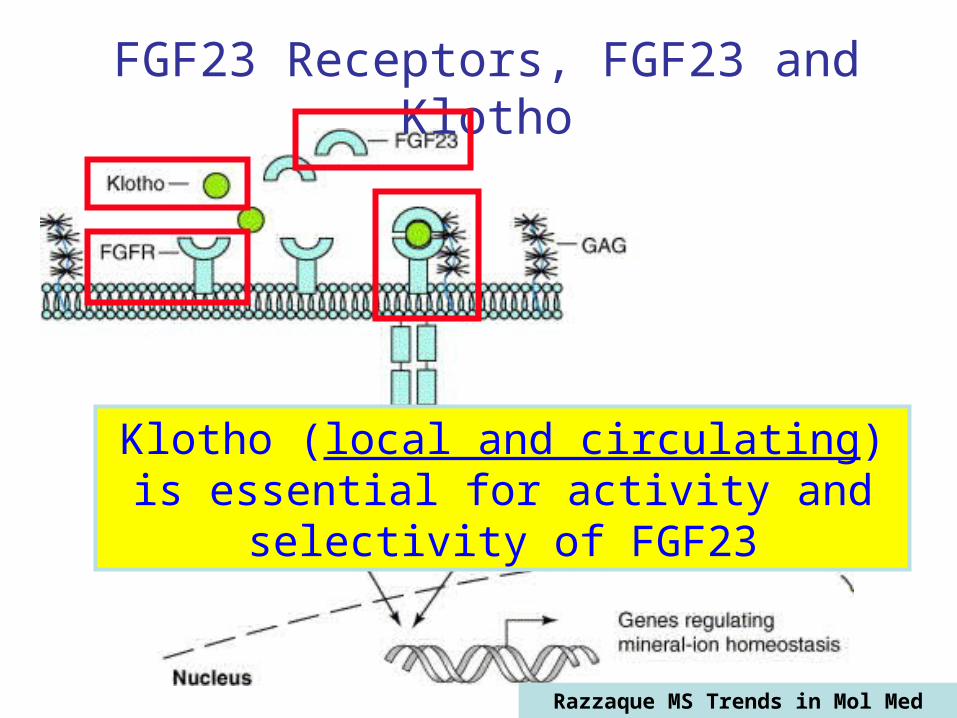
FGF23 Receptors, FGF23 and Klotho
Razzaque MS Trends in Mol Med 2006
Klotho (local and circulating) is essential for activity and selectivity of FGF23

Blood
[ H +]
[ Ca++]
[ P++]
[1,25D]
[PTH]
From Kidney to Bone and viceversa
Klotho
FGF23
Mazzaferro S. et al Arch. Biochem. Biophys. (2010)

Possible differences between the two?
25
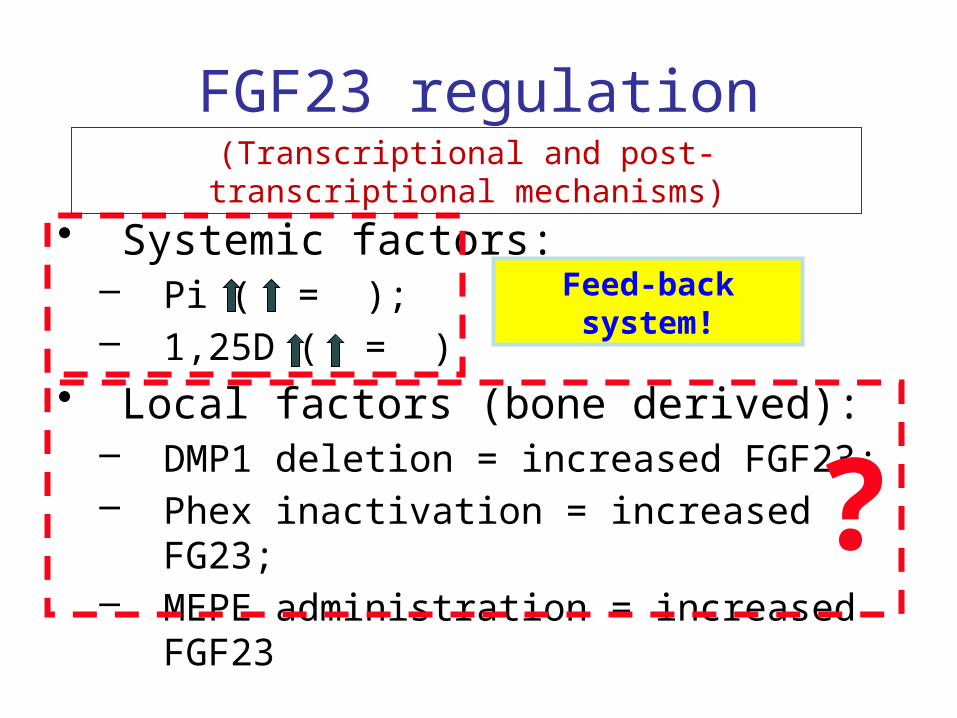
FGF23 regulation
• Systemic factors:– Pi ( = );– 1,25D ( = )
• Local factors (bone derived):– DMP1 deletion = increased FGF23;– Phex inactivation = increased FG23;– MEPE administration = increased FGF23
(Transcriptional and post-transcriptional mechanisms)
?
Feed-back system!
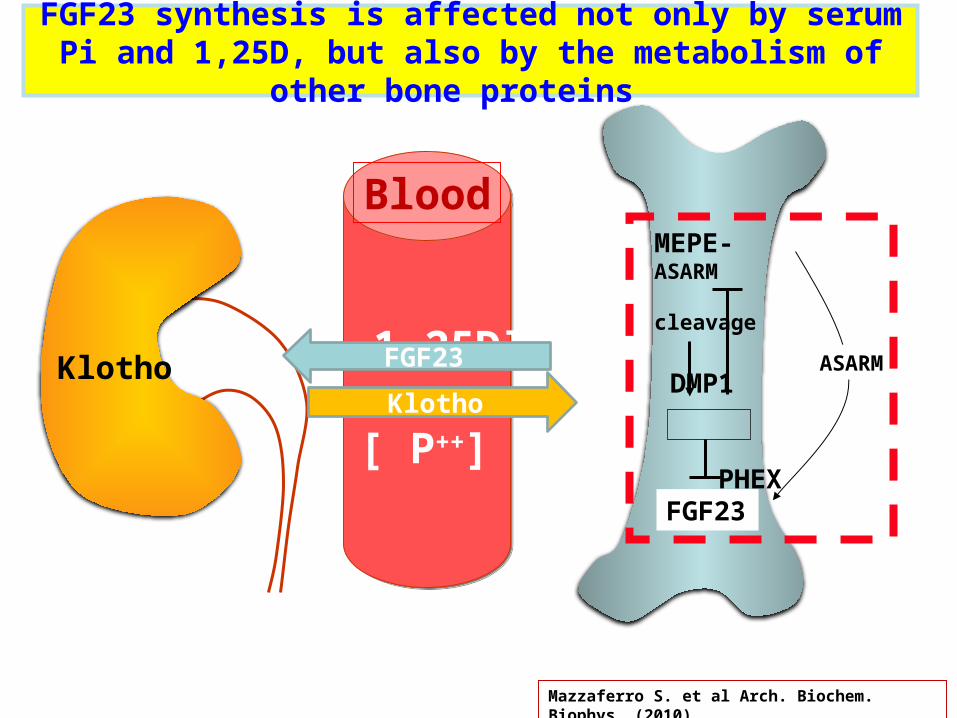
Blood
[ 1,25D]
[ P++]
From Bone to Kidney
FGF23
MEPE-ASARM cleavage
DMP1
PHEX
ASARM
Klotho
FGF23
FGF23 synthesis is affected not only by serum Pi and 1,25D, but also by the metabolism of other bone proteins
Mazzaferro S. et al Arch. Biochem. Biophys. (2010)
Klotho

Klotho functions outside FGF23Organ Activity Effect
Kidney NaPi2a/2c inactivation Hypophosphatemia
Renal TRPV5/6 Activation Ca reabsorption
Renal ROMK1 Activation Potassium secretion
Na/K ATPase Activation Ca homeostasis
Parathyroids Na/K ATPase Activation PTH stimulation
Choroid Plexus
Na/K ATPase Activation Ca homeostasis
Sytemic NaPi3 Reduction Vascular Calcification inhibition
Insulin/IGF-1 inhibition Insulin resistance – Anti-age
Wnt suppression Anti-age
Endothelial NO Up-regulation
Endothelial dysfunction protection
PiCaK
PTH
VC
InsAge
29
S-K
loth
o, p
g/m
l
FG
F23
, pg
/ml
N CKD 2 CKD 3 CKD 4CKD 2 CKD 3 CKD 4
* **
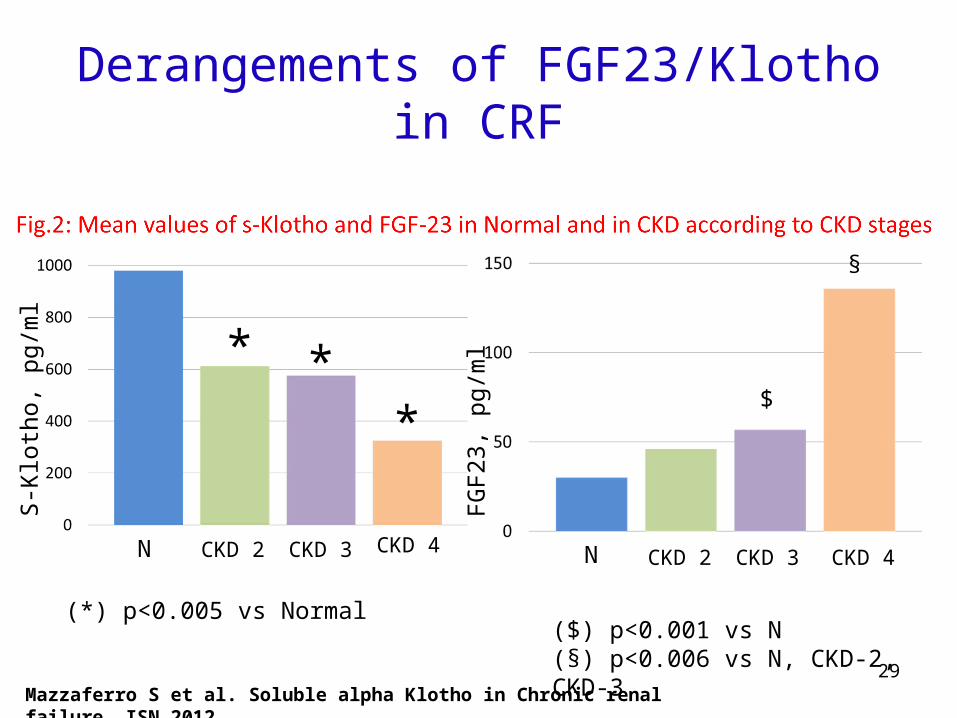
(*) p<0.005 vs Normal
$
N
§
($) p<0.001 vs N(§) p<0.006 vs N, CKD-2, CKD-3
Mazzaferro S et al. Soluble alpha Klotho in Chronic renal failure. ISN 2012
Derangements of FGF23/Klotho in CRF
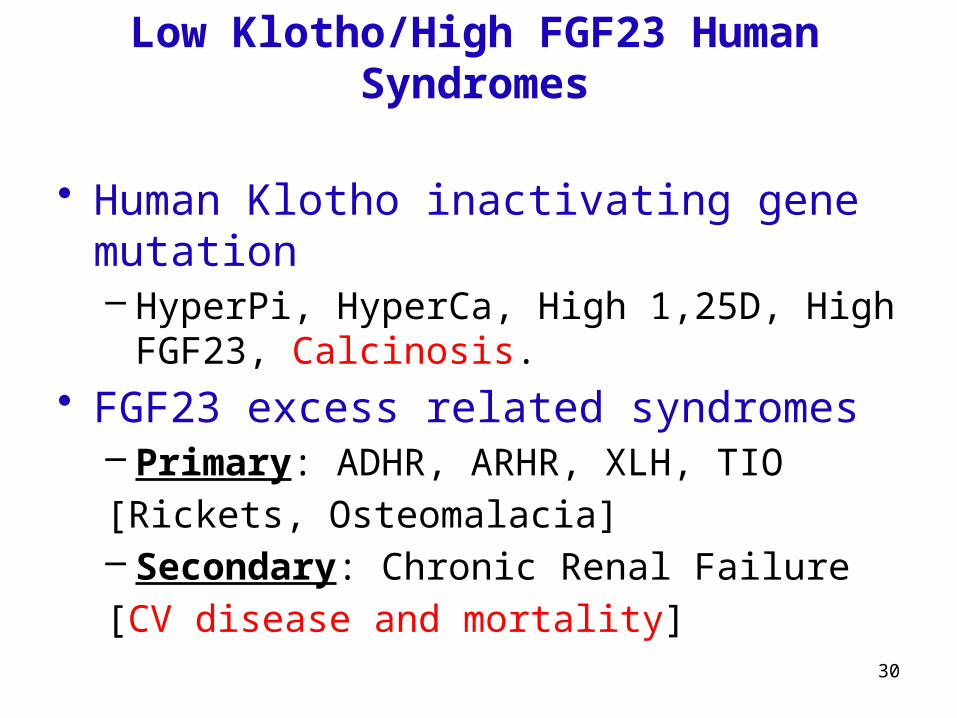
Low Klotho/High FGF23 Human Syndromes
• Human Klotho inactivating gene mutation– HyperPi, HyperCa, High 1,25D, High FGF23,
Calcinosis. • FGF23 excess related syndromes
– Primary: ADHR, ARHR, XLH, TIO
[Rickets, Osteomalacia]– Secondary: Chronic Renal Failure
[CV disease and mortality]
30
31
ORGANS
At least …
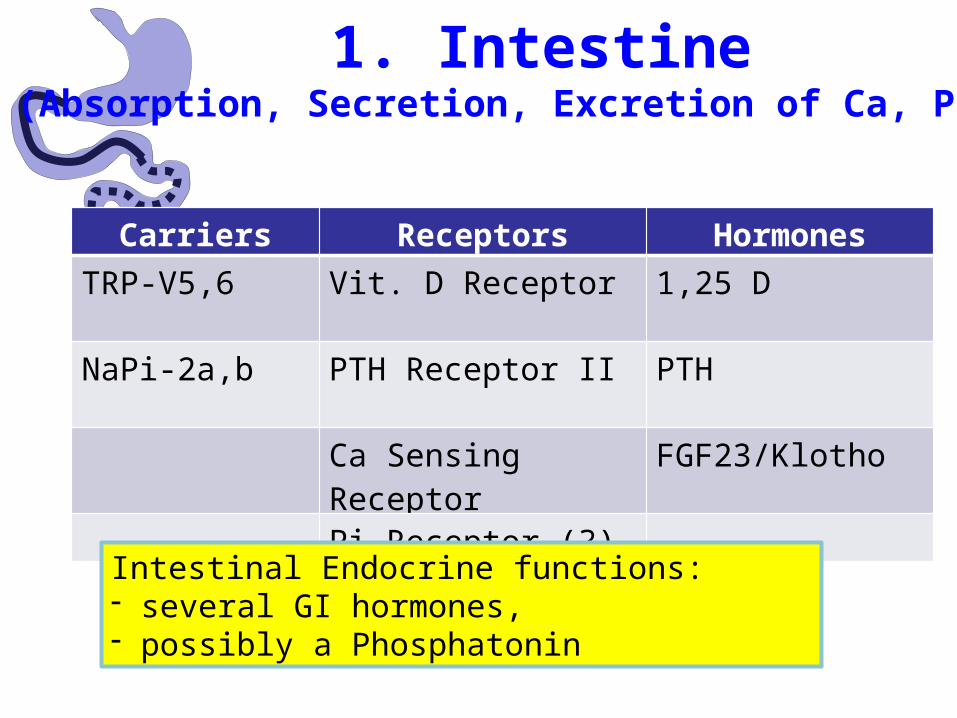
1. Intestine(Absorption, Secretion, Excretion of Ca, Pi, H)
Carriers Receptors Hormones
TRP-V5,6 Vit. D Receptor 1,25 D
NaPi-2a,b PTH Receptor II PTH
Ca Sensing Receptor FGF23/Klotho
Pi Receptor (?)
Intestinal Endocrine functions:- several GI hormones,- possibly a Phosphatonin

2. Kidney(Filtration, Reabsorption, Excretion of Ca, Pi, H)
Carriers Receptors Hormones
TRP-V5,6 Vit. D Receptor 1,25 D
NaPi-2a,b PTH Receptor I PTH
Ca Sensing Receptor FGF23/Klotho
Pi Receptor (?)
Renal Endocrine functions:- Renin, Epo, Calcitriol,- Klotho
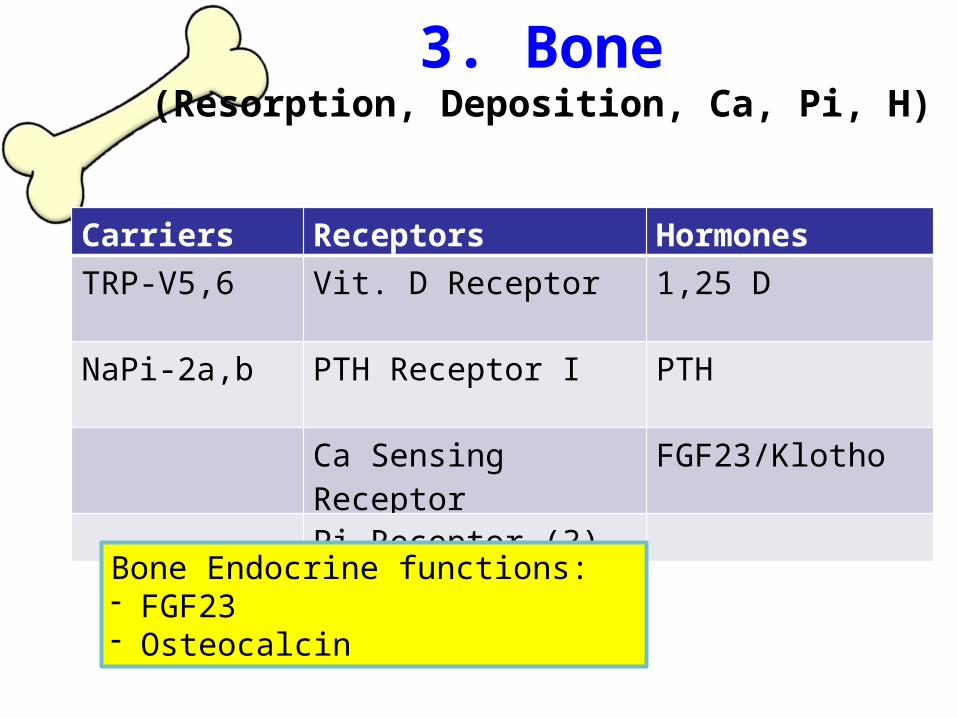
3. Bone(Resorption, Deposition, Ca, Pi, H)
Carriers Receptors Hormones
TRP-V5,6 Vit. D Receptor 1,25 D
NaPi-2a,b PTH Receptor I PTH
Ca Sensing Receptor FGF23/Klotho
Pi Receptor (?)
Bone Endocrine functions:- FGF23- Osteocalcin
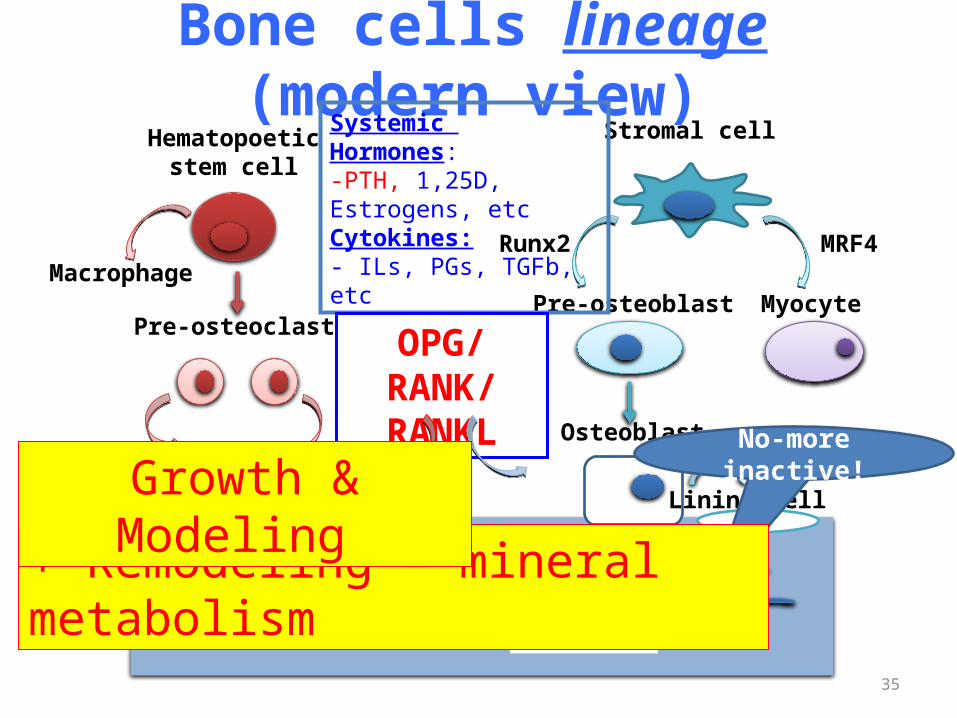
Bone cells lineage (modern view)Hematopoetic
stem cell
Pre-osteoclast
Macrophage
Osteoclast
Pre-osteoblast
Osteoblast
Runx2
Stromal cell
Lining cell
Osteocyte
Systemic Hormones:-PTH, 1,25D, Estrogens, etcCytokines:- ILs, PGs, TGFb, etc
OPG/RANK/RANKL
Myocyte
MRF4
35
No-more inactive!
+ Remodeling = mineral metabolism
Growth & Modeling
Organic Matrix- Non Collagenous Proteins (11%)
1. GAGs: - Proteoglycans, Hyaluronan;
2. Glycoproteins:- ON, SIBLINGs (OPN; BSP; DMP1; SPP1; MEPE), OPG, SOST, RDG contaning proteins, Thrombospondin
3. Γ-Carboxylic Acid containing:- MGP, OC
4. Other Proteins:- Growth factors (BMPs, FGFs), Enzymes (AP, TRAP, PHEX, MMPs), Absorbed from circulation (Albumin, Fetuin)
36
Non-collagenous bone protein contribute to Ca and Pi fluxes from and into bone
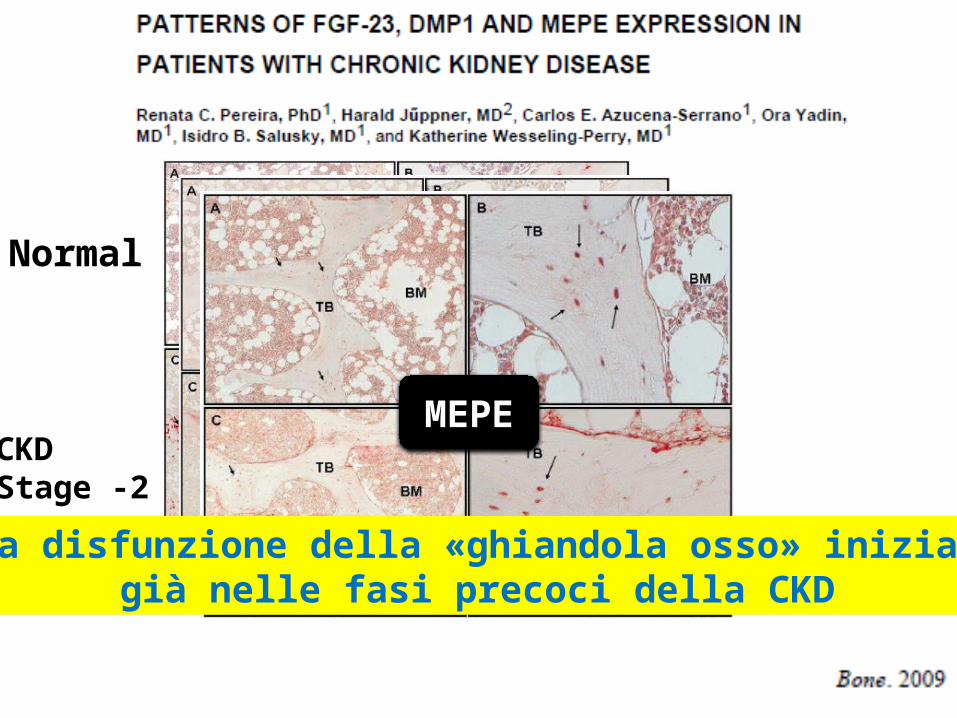
Normal
CKDStage -2
FGF23DMP1MEPE
La disfunzione della «ghiandola osso» inizia già nelle fasi precoci della CKD
39
A possible «rule of … … …»
IONS
ORGANS
HORMONESSystemic (CV) involvement or CKD-MBD
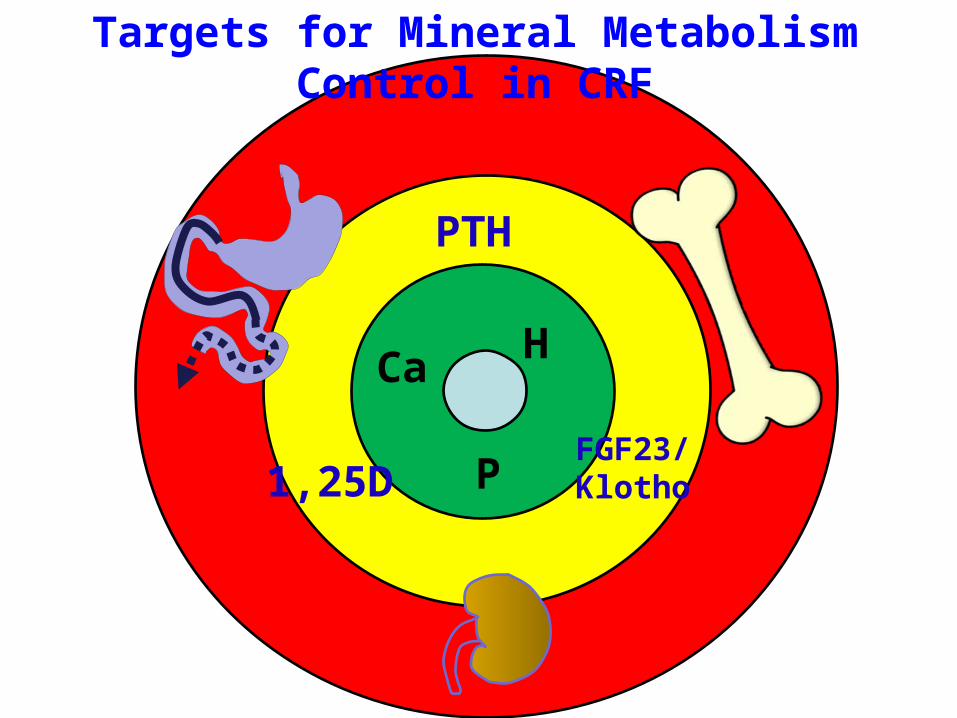
Targets for Mineral Metabolism Control in CRF
PTH
1,25DFGF23/Klotho
Ca
P
H
Available drugs for CKD-MBD
1. Phosphate binders
2. Vitamin D and analogs
3. Calcimimetics
41
(again … … … )
Epidemiologic aspects
(in Dialysis)
Aim of the study:To evaluate- Drug prescription policy,- Biochemical control of SH,with new available drugs (from 2006 to 2008)
1. Drug Prescription policy:(a.) PTH inhibitors
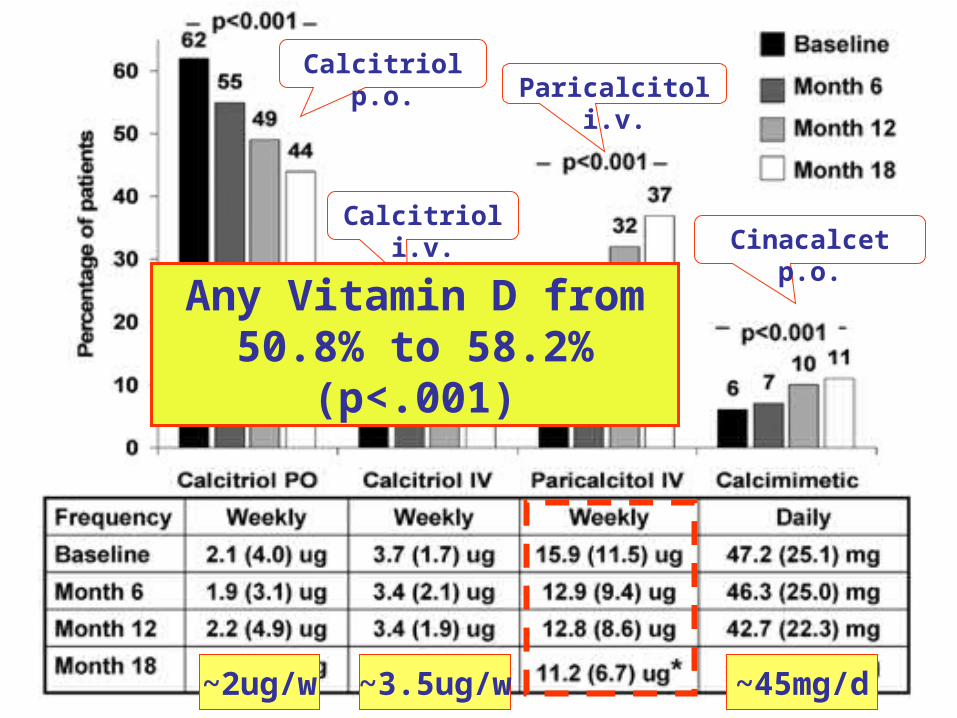
Calcitriol p.o.
Calcitriol i.v.
Paricalcitol i.v.
Cinacalcet p.o.
Any Vitamin D from 50.8% to 58.2% (p<.001)
~2ug/w ~3.5ug/w ~45mg/d
1. Drug Prescription policy:(b.) Phosphate Binders
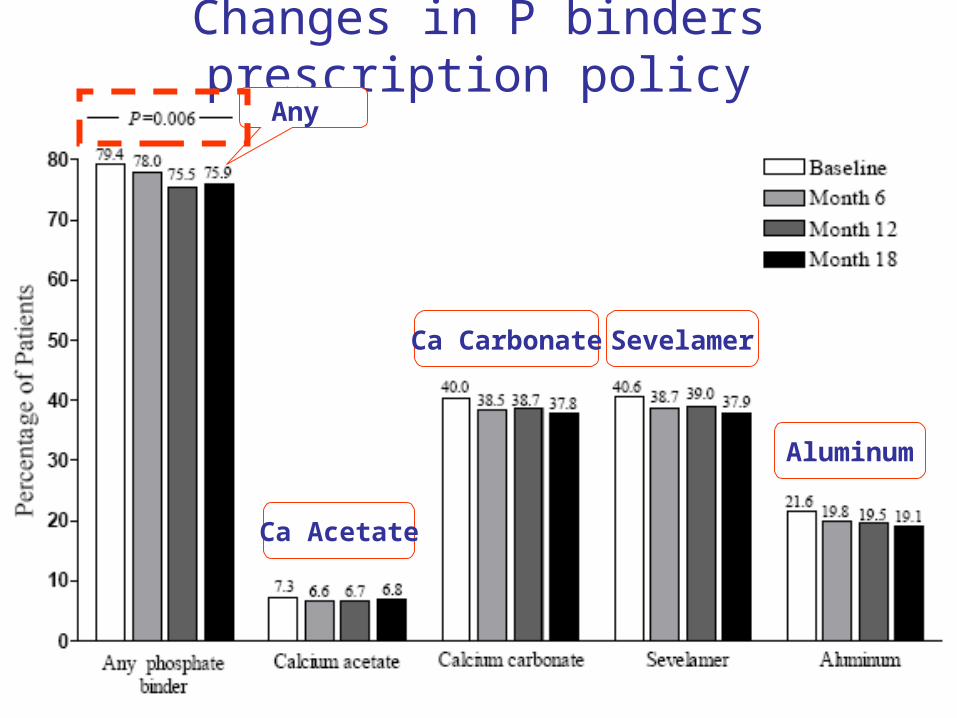
Changes in P binders prescription policyAny
Ca Acetate
Ca Carbonate Sevelamer
Aluminum

Average doses of P binders
Ca Acetate Ca Carbonate Sevelamer Aluminum
~2g/day ~2g/day ~2g/day~4g/day
2. Biochemical control of SH
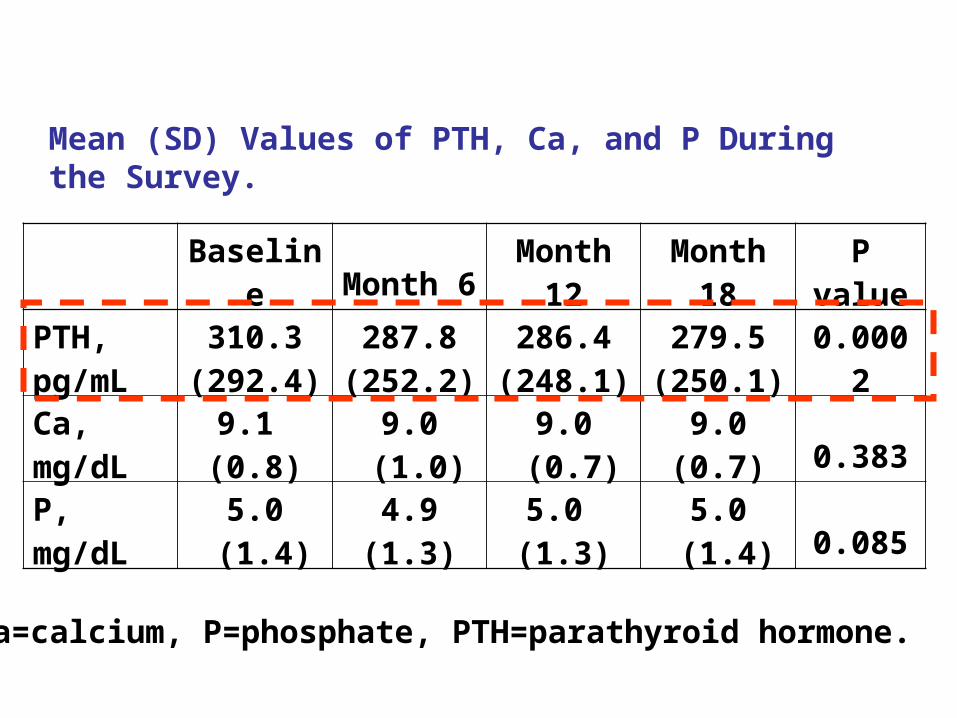
Mean (SD) Values of PTH, Ca, and P During the Survey.
Baseline Month 6Month
12Month
18P
value
PTH, pg/mL
310.3 (292.4)
287.8 (252.2)
286.4 (248.1)
279.5 (250.1) 0.0002
Ca, mg/dL
9.1 (0.8)
9.0 (1.0)
9.0 (0.7)
9.0(0.7) 0.383
P, mg/dL
5.0 (1.4)
4.9(1.3)
5.0 (1.3)
5.0 (1.4) 0.085
Ca=calcium, P=phosphate, PTH=parathyroid hormone.
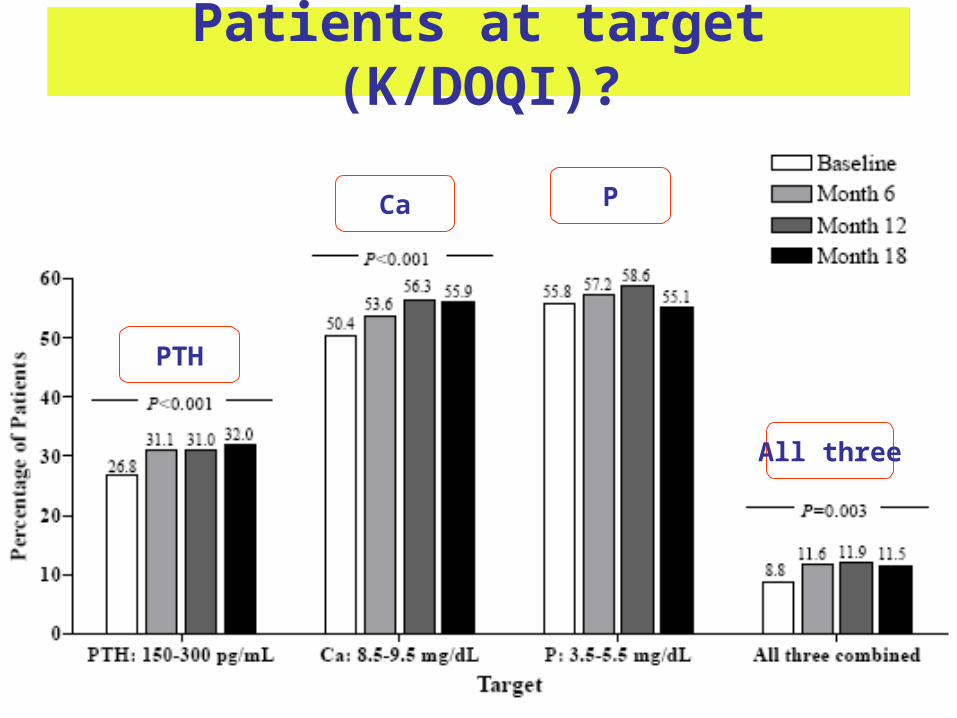
Patients at target (K/DOQI)?
PTH
Ca P
All three

Conclusions
• CKD-MBD = complex metabolic derangement of renal failure, with significant systemic involvement and morbidity/mortality.
• Its therapeutic management is rather difficult, even with new drugs,
• The «rule of 3» seems cute, but insufficient to help manage it properly
52

EVOLVE: Study Design
Screening Phase
Up to 30 Days
TitrationPhase(Visits Q2
Wks)
Follow up Phase(Visits Q8 Wks)
Follow-up period = ~ 2.5 yearsEnrollment = ~ 1.5 years
Day 1 Week 20 Week 52
Event-driven study that concludes when approximately 1,882 subjects have experienced a primary composite event
Placebo plus standard of care(n = 1,900)
Cinacalcet plus standard of care (n = 1,900)
Adapted from: Chertow GM, et al. Clin J Am Soc Nephrol. 2007;2:898-905.
All patients could receive vitamin D sterols and phosphate binders, as necessary, at the discretion of the physician.
Trial Population• Hemodialysis • iPTH 300 pg/mL• Ca 8.4 mg/dL• Ca x P 45 mg2/dL2
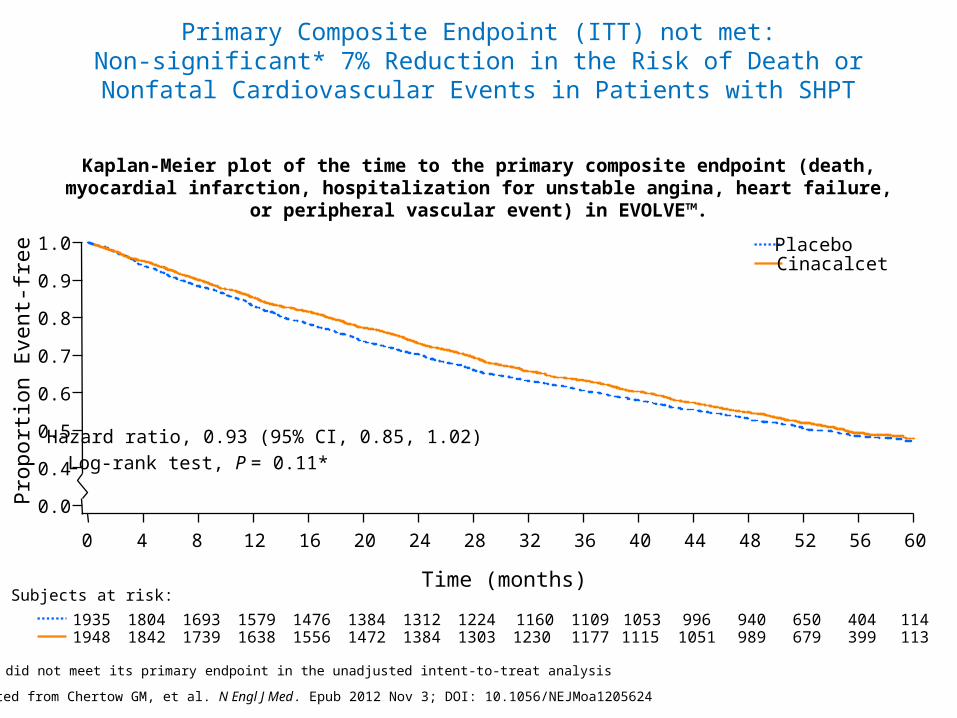
Primary Composite Endpoint (ITT) not met:Non-significant* 7% Reduction in the Risk of Death or Nonfatal Cardiovascular Events in Patients with SHPT
Pro
port
ion
Eve
nt-f
ree
0.0
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (months)
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Hazard ratio, 0.93 (95% CI, 0.85, 1.02)
Log-rank test, P = 0.11*
Subjects at risk:
19481935
18421804
17391693
16381579
15561476
14721384
13841312
13031224
12301160
11771109
11151053
1051996
989940
679650
399404
113114
CinacalcetPlacebo
Kaplan-Meier plot of the time to the primary composite endpoint (death, myocardial infarction, hospitalization for unstable angina, heart failure, or peripheral vascular event) in EVOLVE™.
Adapted from Chertow GM, et al. N Engl J Med. Epub 2012 Nov 3; DOI: 10.1056/NEJMoa1205624
* The trial did not meet its primary endpoint in the unadjusted intent-to-treat analysis
CKD-MBD Working Group ERA-EDTA
55
56