REGIONE del VENETO - formazionesostenibile.it · REGIONE del VENETO ’AZIENDA OSPEDALIERA -...
99
REGIONE del VENETO REGIONE del VENETO AZIENDA OSPEDALIERA - UNIVERSITA AZIENDA OSPEDALIERA - UNIVERSITA ’ ’ DI PADOVA DI PADOVA UNITA’ OPERATIVA COMPLESSA UNITA’ OPERATIVA COMPLESSA Chirurgia del Rachide Chirurgia del Rachide “ “ Sandro Agostini Sandro Agostini ” ” ( ( Dir.: dr Daniele Fabris Monterumici Dir.: dr Daniele Fabris Monterumici ) )
Transcript of REGIONE del VENETO - formazionesostenibile.it · REGIONE del VENETO ’AZIENDA OSPEDALIERA -...
REGIONE del VENETOREGIONE del VENETO
AZIENDA OSPEDALIERA - UNIVERSITAAZIENDA OSPEDALIERA - UNIVERSITA’’DI PADOVADI PADOVA
UNITA’ OPERATIVA COMPLESSAUNITA’ OPERATIVA COMPLESSAChirurgia del RachideChirurgia del Rachide
““Sandro AgostiniSandro Agostini””((Dir.: dr Daniele Fabris MonterumiciDir.: dr Daniele Fabris Monterumici))

IL TRATTAMENTO CHIRURGICO
DELLE
SPONDILOLISTESI LOMBO – SACRALI(GRADO III° e IV°)
Daniele Fabris Monterumici
IN TEMA DI TRATTAMENTO CHIRURGICOIN TEMA DI TRATTAMENTO CHIRURGICO
DELLE SPONDILOLISTESI LOMBO - SACRALIDELLE SPONDILOLISTESI LOMBO - SACRALI
SI PUO’ SOSTENERE ESSERVI OGGI SI PUO’ SOSTENERE ESSERVI OGGI
UN GENERALE CONSENSOUN GENERALE CONSENSO
SULLESULLE

INDICAZIONIINDICAZIONIINDICAZIONIINDICAZIONI
SOGGETTI IN ACCRESCIMENTOSOGGETTI IN ACCRESCIMENTO
PROGRESSIONE DOCUMENTATAPROGRESSIONE DOCUMENTATA DELL’OLISTESIDELL’OLISTESI
PROGRESSIONE DOCUMENTATA (RX)PROGRESSIONE DOCUMENTATA (RX)
OLISTESI OLISTESI >> 20 - 25 % 20 - 25 % POSITIVITA’ ELEMENTI POSITIVITA’ ELEMENTI RADIOGRAFICIRADIOGRAFICI
OLISTESI OLISTESI >> 50% ? 50% ?

INDICAZIONIINDICAZIONIINDICAZIONIINDICAZIONI
SOGGETTI IN ACCRESCIMENTOSOGGETTI IN ACCRESCIMENTO
PROGRESSIONE DOCUMENTATAPROGRESSIONE DOCUMENTATA DELL’OLISTESIDELL’OLISTESI
Spondylolysis and spondylolisthesis during growthSpondylolysis and spondylolisthesis during growthHasler C, Dick W.Hasler C, Dick W.
Orthopade, 2002 Jan;31(1):78-87Orthopade, 2002 Jan;31(1):78-87
Patients with low grade Spondylolisthesis (Meyerding I, II) Patients with low grade Spondylolisthesis (Meyerding I, II) require repeated radiological follow-up during growth require repeated radiological follow-up during growth
because of the inherent risk of slip progression. because of the inherent risk of slip progression. If a slip of more than 50% is detected before the end of growth, If a slip of more than 50% is detected before the end of growth,
operative treatment is indicatedoperative treatment is indicated

INDICAZIONIINDICAZIONIINDICAZIONIINDICAZIONI
SOGGETTI IN ACCRESCIMENTOSOGGETTI IN ACCRESCIMENTO
PROGRESSIONE DOCUMENTATAPROGRESSIONE DOCUMENTATA DELL’OLISTESIDELL’OLISTESI
SOGGETTI IN FASE DI ACCRESCIMENTOSOGGETTI IN FASE DI ACCRESCIMENTO
CON OLISTESI CON OLISTESI >> 25 - 30%25 - 30%
SEGNI RADIOGRAFICISEGNI RADIOGRAFICIPROGNOSTICAMENTE POSITIVIPROGNOSTICAMENTE POSITIVI
ANCHE NON IN PRESENZAANCHE NON IN PRESENZA
INDICAZIONIINDICAZIONIINDICAZIONIINDICAZIONI
SOGGETTI IN ACCRESCIMENTOSOGGETTI IN ACCRESCIMENTO
PROGRESSIONE DOCUMENTATAPROGRESSIONE DOCUMENTATA DELL’OLISTESIDELL’OLISTESI
SOGGETTI IN FASE DI ACCRESCIMENTOSOGGETTI IN FASE DI ACCRESCIMENTO
CON OLISTESI CON OLISTESI >> 25 - 30%25 - 30%
SEGNI RADIOGRAFICISEGNI RADIOGRAFICIPROGNOSTICAMENTE POSITIVIPROGNOSTICAMENTE POSITIVI
QUADRI CLINICI EVIDENTIQUADRI CLINICI EVIDENTI
ANCHE NON IN PRESENZAANCHE NON IN PRESENZA
DEBBANO ESSERE CONSIDERATIDEBBANO ESSERE CONSIDERATI
PER IL TRATTAMENTOPER IL TRATTAMENTO
CHIRURGICOCHIRURGICO
DELLA DEFORMITA’DELLA DEFORMITA’

OBIETTIVIOBIETTIVIOBIETTIVIOBIETTIVI
RIPRISTINO RAPPORTI CONTENENTE - CONTENUTORIPRISTINO RAPPORTI CONTENENTE - CONTENUTO
STABILITA’STABILITA’
OBIETTIVIOBIETTIVIOBIETTIVIOBIETTIVI
RAGGIUNGIMENTORAGGIUNGIMENTODEGLIDEGLI
OBIETTIVIOBIETTIVI
RAGGIUNGIMENTORAGGIUNGIMENTODEGLIDEGLI
OBIETTIVIOBIETTIVI
RIDUZIONERIDUZIONE
ARTRODESIARTRODESI
RAGGIUNGIMENTORAGGIUNGIMENTODEGLIDEGLI
OBIETTIVIOBIETTIVI
RAGGIUNGIMENTORAGGIUNGIMENTODEGLIDEGLI
OBIETTIVIOBIETTIVI
ANCOR OGGI UN VI E’ DIBATTITOANCOR OGGI UN VI E’ DIBATTITOPER QUANTO CONCERNEPER QUANTO CONCERNE
VIA CHIRURGICAANTERIORE - POSTERIORE - COMBINATAANTERIORE - POSTERIORE - COMBINATA
RIDUZIONESI NO QUANDO?SI NO QUANDO?
TIPO DI ARTRODESIPOSTERO LATERALE IN SITU - INTERSOMATICA - PLIFPOSTERO LATERALE IN SITU - INTERSOMATICA - PLIF
QUESTO DIBATTITO ASSUME CONTORNIQUESTO DIBATTITO ASSUME CONTORNI
DIVERSIDIVERSI
QUANDO SI DISCUTA SU OLISTESIQUANDO SI DISCUTA SU OLISTESI
NEI SOGGETTI IN ACCRESCIMENTONEI SOGGETTI IN ACCRESCIMENTO
OO
NEI SOGGETTI ADULTINEI SOGGETTI ADULTI
DIVERSO PERCHE’DIVERSO PERCHE’
DIVERSIDIVERSI
APPAIONOAPPAIONO
GLI OBIETTIVI DEL TRATTAMENTOGLI OBIETTIVI DEL TRATTAMENTO
MA NON E’ QUESTO IL COMPITOMA NON E’ QUESTO IL COMPITO
OGGI A ME AFFIDATOOGGI A ME AFFIDATO
IL COMPITO OGGI A ME AFFIDATOIL COMPITO OGGI A ME AFFIDATO
RIGUARDARIGUARDA
LE METODICHE DILE METODICHE DI
TRATTAMENTO CHIRURGICOTRATTAMENTO CHIRURGICO
DELLE SPONDILOLISTESI GRAVIDELLE SPONDILOLISTESI GRAVI

RIDUZIONERIDUZIONE
ARTRODESIARTRODESI
RAGGIUNGIMENTORAGGIUNGIMENTORAGGIUNGIMENTORAGGIUNGIMENTO
RIPRISTINO RAPPORTI CONTENENTE - CONTENUTORIPRISTINO RAPPORTI CONTENENTE - CONTENUTO
STABILITA’STABILITA’
OBIETTIVIOBIETTIVIOBIETTIVIOBIETTIVI

ARTRODESIARTRODESISOPPRESSIONE DEL MOVIMENTOSOPPRESSIONE DEL MOVIMENTO
TRAMITE ARTRODESITRAMITE ARTRODESI
POSTERO - LATERALE “IN SITU”POSTERO - LATERALE “IN SITU”
POSTERO - LATERALE STRUMENTATAPOSTERO - LATERALE STRUMENTATA
INTERSOMATICA + PL STRUMENTATAINTERSOMATICA + PL STRUMENTATA
ARTRODESI POSTERO – LATERALE ARTRODESI POSTERO – LATERALE
““IN SITU” IN SITU”
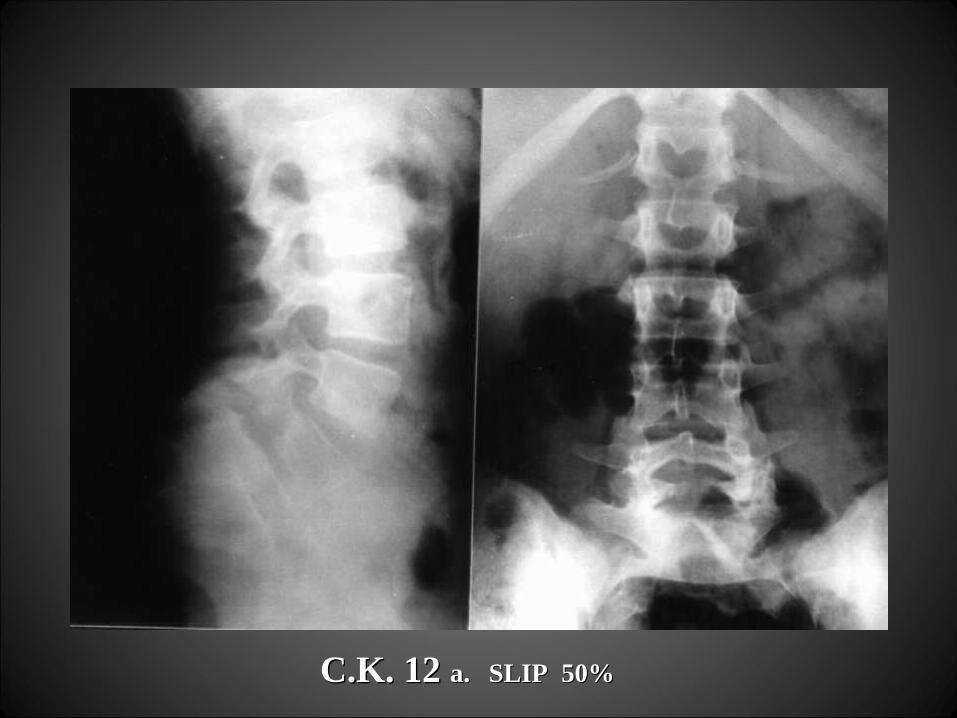
C.K. 12 C.K. 12 a.a. SLIP 50%SLIP 50%

C.K. C.K. ARTRODESI POST - LAT. L3 - S1 ARTRODESI POST - LAT. L3 - S1

L’ARTRODESI POSTERO - LATERALE “IN SITU”L’ARTRODESI POSTERO - LATERALE “IN SITU”
E’ STATA PER MOLTI ANNIE’ STATA PER MOLTI ANNI
CONSIDERATACONSIDERATA
IL “GOLD STANDARD”IL “GOLD STANDARD”
ANCHE SE NUMEROSI STUDI COMPARATIVIANCHE SE NUMEROSI STUDI COMPARATIVI
TENDONO A SOVVERTIRETENDONO A SOVVERTIRE
TALE ASSUNTOTALE ASSUNTO
Grzegorzewski A; Kumar SJ In situ posterolateral spine arthrodesis for grades III, IV, and V spondylolisthesis in children and adolescents. J Pediatr Orthop., Jul-Aug 2000, 20(4) p506-11
Suk KS, Jeon CH, Park MS, Moon SH, Kim NH, Lee HM. Comparison between posterolateral fusion with pedicle screw fixation and anterior interbody fusion with pedicle screw fixation in adult spondylolytic spondylolisthesis.Yonsei Med J. 2001 Jun;42(3):316-23
Madan S. - Boeree N.R.Outcome of posterior lumbar interbody fusion versus posterolateral fusion for spondylolytic spondylolisthesis. Spine, Jul 15 2002, 27(14), 1536-42
Molinari RW; Bridwell KH; Lenke LG; Baldus C Anterior column support in surgery for high-grade, isthmic spondylolisthesis. Clin Orthop., Jan 2002, (394), 109-120
Christensen FB Lumbar spinal fusion. Outcome in relation to surgical methods, choice of implant and postoperative rehabilitationActa Orthop Scand Suppl. 2004 Oct;75(313):2-43
Madan S. - Boeree N.R.Outcome of posterior lumbar interbody fusion versus posterolateral fusion for spondylolytic spondylolisthesis. Spine, Jul 15 2002, 27(14), 1536-42
Posterolateral fusion has a better clinical outcome
in low grades of isthmic spondylolisthesis, although
posterior lumbar interbody fusion is more predictable
in maintaining correction and achieving union
Madan S. - Boeree N.R.Outcome of posterior lumbar interbody fusion versus posterolateral fusion for spondylolytic spondylolisthesis. Spine, Jul 15 2002, 27(14), 1536-42
Posterolateral fusion has a better clinical outcome
in low grades of isthmic spondylolisthesis, although although
posterior lumbar interbody fusion is more predictable posterior lumbar interbody fusion is more predictable
in maintaining correction and achieving unionin maintaining correction and achieving union
Molinari RW; Bridwell KH; Lenke LG; Baldus C Molinari RW; Bridwell KH; Lenke LG; Baldus C Anterior column support in surgery for high-grade, isthmic spondylolisthesis. Anterior column support in surgery for high-grade, isthmic spondylolisthesis. Clin Orthop., Jan 2002, (394), 109-120 Clin Orthop., Jan 2002, (394), 109-120
Group 1 consisted of 18 patients treated only with posterior surgery without anterior structural
Group 2 consisted of 19 patients who had a reduction and circumferential fusion including anterior structural support.
The incidence of pseudarthrosis was The incidence of pseudarthrosis was
39% (seven of 18 patients) in Group 139% (seven of 18 patients) in Group 1
and 0% (0 of 19) in Group 2.and 0% (0 of 19) in Group 2.
All seven patients who had pseudarthrosis achieved solid fusion with a second procedure involving circumferential fusion
with anterior column structural grafting.
Group 1 consisted of 18 patients treated only with posterior
surgery without anterior structural
Group 2 consisted of 19 patients who had a reduction and circumferential fusion including anterior structural support.
The incidence of pseudarthrosis was The incidence of pseudarthrosis was
39% (seven of 18 patients) in Group 139% (seven of 18 patients) in Group 1
and 0% (0 of 19) in Group 2.and 0% (0 of 19) in Group 2. All seven patients who had pseudarthrosis achieved solid fusion
with a second procedure involving circumferential fusion with anterior column structural grafting.
Molinari RW; Bridwell KH; Lenke LG; Baldus C Molinari RW; Bridwell KH; Lenke LG; Baldus C Anterior column support in surgery for high-grade, isthmic spondylolisthesis. Anterior column support in surgery for high-grade, isthmic spondylolisthesis. Clin Orthop., Jan 2002, (394), 109-120 Clin Orthop., Jan 2002, (394), 109-120
Group 1 consisted of 18 patients treated only with posterior
surgery without anterior structural
Group 2 consisted of 19 patients who had a reduction and circumferential fusion including anterior structural support.
The incidence of pseudarthrosis was The incidence of pseudarthrosis was
39% (seven of 18 patients) in Group 139% (seven of 18 patients) in Group 1
and 0% (0 of 19) in Group 2.and 0% (0 of 19) in Group 2. All seven patients who had pseudarthrosis achieved solid fusion
with a second procedure involving circumferential fusion with anterior column structural grafting.
Grzegorzewski A; Kumar SJ In situ posterolateral spine arthrodesis for grades III, IV, and V spondylolisthesis in children and adolescents. J Pediatr Orthop., Jul-Aug 2000, 20(4) p506-11
The study population consisted of 21 patients who underwent an in situ posterolateral spinal fusion from L4 to S1
with autogenous iliac bone graft and were immobilized in a pantaloon cast for 4 months
After surgery there were no motor deficits, incontinence of bowel or bladder, or sexual dysfunction.
Roentgenographic findings showed progression of the slip showed progression of the slip in five patients and increase of the slip angle in five patients and increase of the slip angle and the displacement index in two patientsand the displacement index in two patients
Grzegorzewski A; Kumar SJ In situ posterolateral spine arthrodesis for grades III, IV, and V spondylolisthesis in children and adolescents. J Pediatr Orthop., Jul-Aug 2000, 20(4) p506-11
The study population consisted of 21 patients who underwent an in situ posterolateral spinal fusion from L4 to S1
with autogenous iliac bone graft and were immobilized in a pantaloon cast for 4 months
After surgery there were no motor deficits, incontinence of bowel or bladder, or sexual dysfunction.
Roentgenographic findings showed progression of the slip showed progression of the slip in five patients and increase of the slip angle in five patients and increase of the slip angle and the displacement index in two patientsand the displacement index in two patients
Suk KS et Al.Comparison between posterolateral fusion with pedicle screw fixation and anterior interbody fusion with pedicle screw fixation in adult spondylolytic spondylolisthesis.Yonsei Med J. 2001 Jun;42(3):316-23
In conclusion, PLF with PSF was just as effective as ALIF with PSFIn conclusion, PLF with PSF was just as effective as ALIF with PSF
in terms of clinical outcomes, but ALIF with PSF was superior to in terms of clinical outcomes, but ALIF with PSF was superior to
PLF with PSF in terms of the prevention of reduction loss.PLF with PSF in terms of the prevention of reduction loss.
Anterior support would be helpful for preventing reduction loss Anterior support would be helpful for preventing reduction loss
in cases of spondylolytic spondylolisthesis of the lumbar spinein cases of spondylolytic spondylolisthesis of the lumbar spine
Suk KS et Al.Comparison between posterolateral fusion with pedicle screw fixation and anterior interbody fusion with pedicle screw fixation in adult spondylolytic spondylolisthesis.Yonsei Med J. 2001 Jun;42(3):316-23
In conclusion, PLF with PSF was just as effective as ALIF with PSFIn conclusion, PLF with PSF was just as effective as ALIF with PSF
in terms of clinical outcomes, but ALIF with PSF was superior to in terms of clinical outcomes, but ALIF with PSF was superior to
PLF with PSF in terms of the prevention of reduction loss.PLF with PSF in terms of the prevention of reduction loss.
Anterior support would be helpful for preventing reduction loss Anterior support would be helpful for preventing reduction loss
in cases of spondylolytic spondylolisthesis of the lumbar spinein cases of spondylolytic spondylolisthesis of the lumbar spine
Christensen FB Lumbar spinal fusion. Outcome in relation to surgical methods, choice of implant and postoperative rehabilitationActa Orthop Scand Suppl. 2004 Oct;75(313):2-43
The choice of surgical procedure should relate to the diagnosis, as patients
with isthmic spondylolisthesis (Grades I and II) are best served with posterolateral fusion
without instrumentation, and patients with disc degeneration seem to gain most
from instrumented posterolateral fusion or circumferential fusion
Christensen FB Lumbar spinal fusion. Outcome in relation to surgical methods, choice of implant and postoperative rehabilitationActa Orthop Scand Suppl. 2004 Oct;75(313):2-43
The choice of surgical procedure should relate to the diagnosis, as patients
with isthmic spondylolisthesis (Grades I and II) are best served with posterolateral fusion
without instrumentation, and patients with disc degeneration seem to gain most
from instrumented posterolateral fusion or circumferential fusion
Christensen FB Lumbar spinal fusion. Outcome in relation to surgical methods, choice of implant and postoperative rehabilitationActa Orthop Scand Suppl. 2004 Oct;75(313):2-43
The choice of surgical procedure should relate to the diagnosis, as patients
with isthmic spondylolisthesis (Grades I and II) are best served with posterolateral fusion
without instrumentation, and patients with disc degeneration seem to gain most
from instrumented posterolateral fusion or circumferential fusion
SE INVECE, SE INVECE,
E TALE OPZIONE PARREBBEE TALE OPZIONE PARREBBE
DEL TUTTO LOGICA,DEL TUTTO LOGICA,
SI TENDA AL RIPRISTINOSI TENDA AL RIPRISTINO
DI RAPPORTI ANATOMICIDI RAPPORTI ANATOMICI
LOCALI, REGIONALI E GLOBALILOCALI, REGIONALI E GLOBALI
PERDUTI IN RAGIONE DELL’OLISTESIPERDUTI IN RAGIONE DELL’OLISTESI
APPARE ALLORA NECESSARIOAPPARE ALLORA NECESSARIO
DISCUTERE SULLADISCUTERE SULLA
RIDUZIONERIDUZIONE
PERCHE’ SOLAMENTE LA RIDUZIONEPERCHE’ SOLAMENTE LA RIDUZIONE
CONSENTECONSENTE
•RIEQUILIBRIO ASSETTO SAGITTALERIEQUILIBRIO ASSETTO SAGITTALE
•STABILITA’STABILITA’
•ARTRODESI INTERSOMATICAARTRODESI INTERSOMATICA
STRATEGIE CHIRURGICHE STRATEGIE CHIRURGICHE
DIDI
ARTRODESI E STRUMENTAZIONEARTRODESI E STRUMENTAZIONE
TECNICHE DI RIDUZIONETECNICHE DI RIDUZIONE
MOLTE SONO STATE LE TECNICHEMOLTE SONO STATE LE TECNICHE
PROPOSTE ALLO SCOPO DI OTTENEREPROPOSTE ALLO SCOPO DI OTTENERE
LA RIDUZIONE DELL’OLISTESILA RIDUZIONE DELL’OLISTESI
CORREZIONE INTRA – OPERATORIACORREZIONE INTRA – OPERATORIA - VITI A DOPPIA FILETTATURA- VITI A DOPPIA FILETTATURA- EFFETTO CANTILEVER- EFFETTO CANTILEVER
CORREZIONE PRE - OPERATORIA CORREZIONE PRE - OPERATORIA - GESSO- GESSO

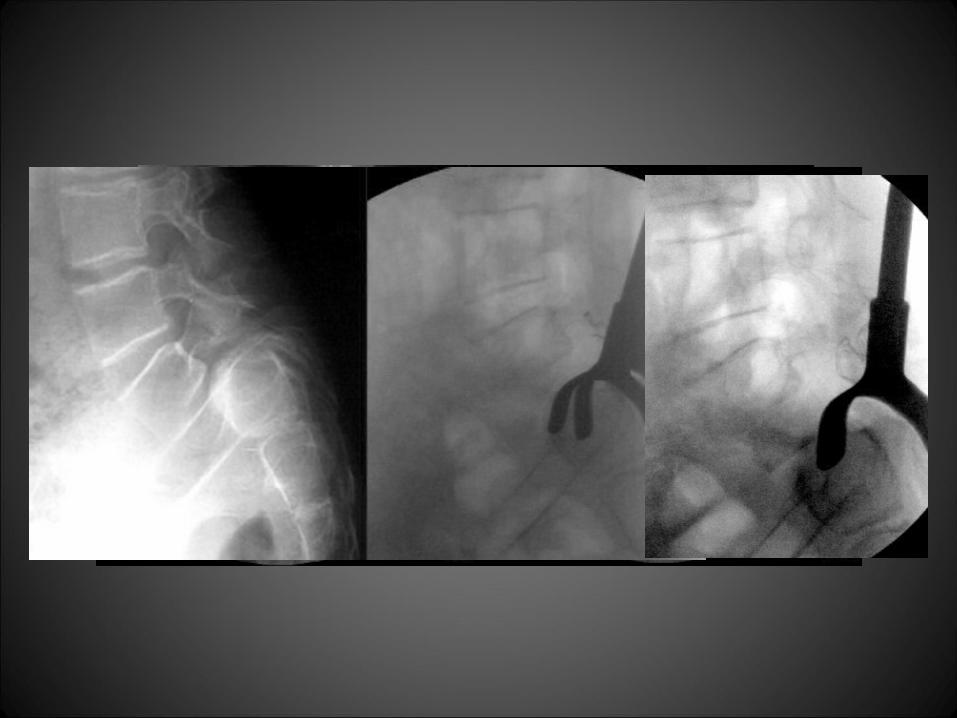
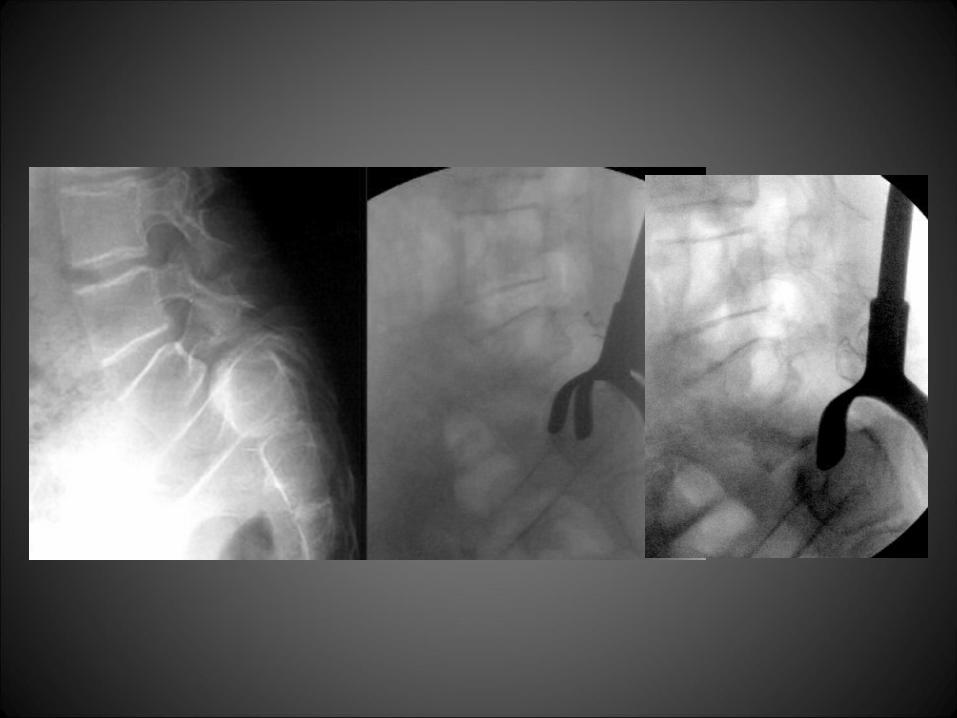
CORREZIONE INTRA - OPERATORIACORREZIONE INTRA - OPERATORIA
DISTRAZIONE REGIONALE LOMBAREDISTRAZIONE REGIONALE LOMBARE

CORREZIONE INTRA - OPERATORIACORREZIONE INTRA - OPERATORIA
DISTRAZIONE REGIONALE LOMBAREDISTRAZIONE REGIONALE LOMBARE

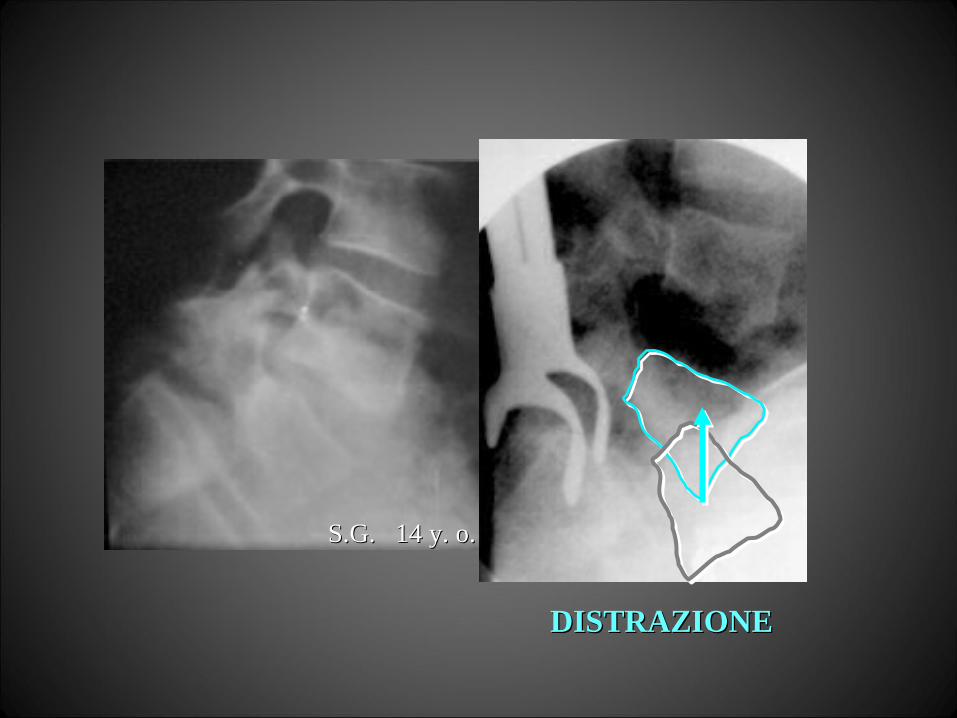
CORREZIONE INTRA - OPERATORIACORREZIONE INTRA - OPERATORIA
DISTRAZIONE REGIONALE LOMBAREDISTRAZIONE REGIONALE LOMBARE
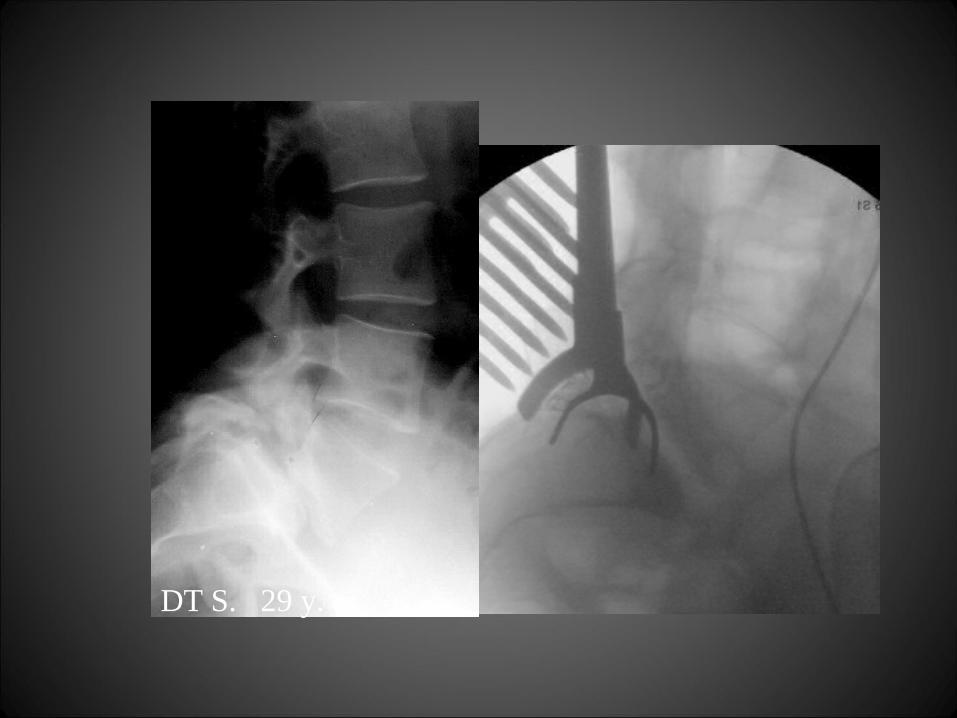
DT S. 29 y. o.

S.G. 14 y. o.S.G. 14 y. o.
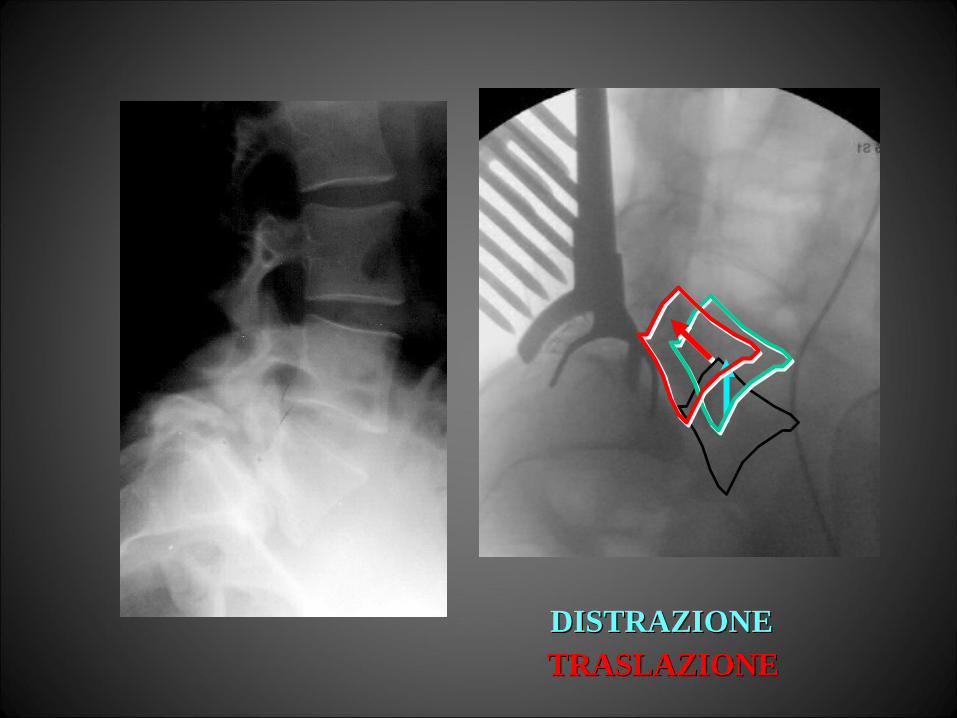
DISTRAZIONEDISTRAZIONETRASLAZIONETRASLAZIONE
S.G. 14 y. o.S.G. 14 y. o.
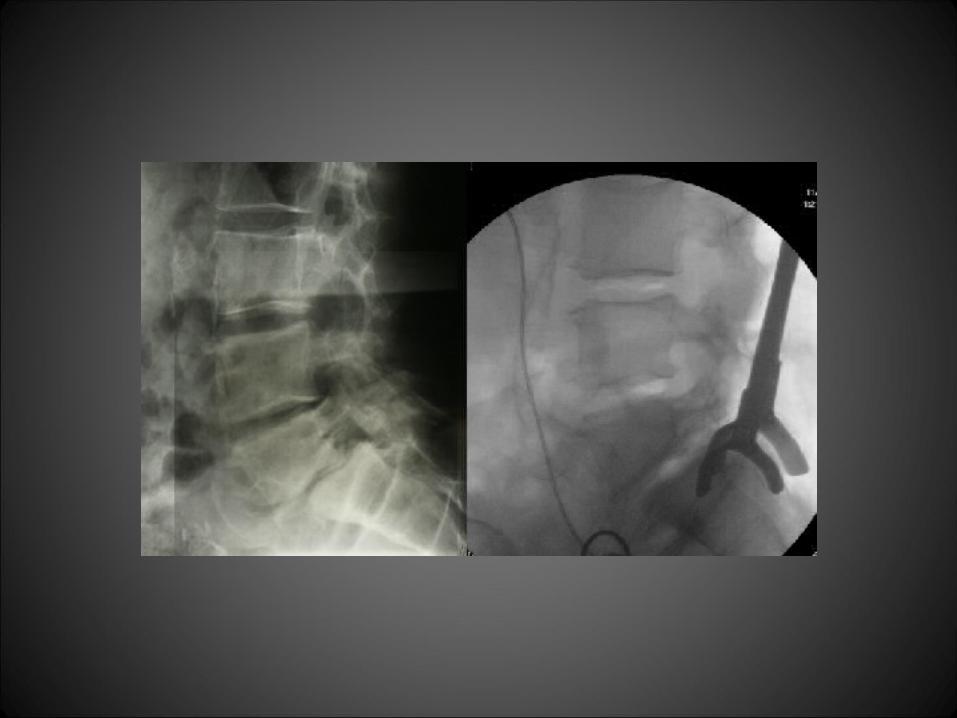
DISTRAZIONEDISTRAZIONE
RIDUZIONE INTRA-OPERATORIARIDUZIONE INTRA-OPERATORIA
"Extremely challenging and with a high "Extremely challenging and with a high rate of complications”rate of complications”
Grobler and Wiltze '91Grobler and Wiltze '91
Anterior spondylodesis including posterior instrumentation Anterior spondylodesis including posterior instrumentation
and reduction was superior to the simple anterior fusion and reduction was superior to the simple anterior fusion
in situ for normalization of the lumbosacral profile and osseous in situ for normalization of the lumbosacral profile and osseous
consolidation of the spondylodesis.consolidation of the spondylodesis.
Muschik M. et al. Spine, Sep 1997Muschik M. et al. Spine, Sep 1997
Anterior spondylodesis including posterior instrumentation Anterior spondylodesis including posterior instrumentation
and reduction was superior to the simple anterior fusion and reduction was superior to the simple anterior fusion
in situ for normalization of the lumbosacral profile and osseous in situ for normalization of the lumbosacral profile and osseous
consolidation of the spondylodesis.consolidation of the spondylodesis.
Muschik M. et al. Spine, Sep 1997Muschik M. et al. Spine, Sep 1997
RIDUZIONE INTRA-OPERATORIARIDUZIONE INTRA-OPERATORIA

COMPLICANZE RADICOLARICOMPLICANZE RADICOLARI
“ “ There were as many neurological deficits after in situThere were as many neurological deficits after in situposterior procedures as there were with operations thatposterior procedures as there were with operations thatinvolved reduction of the deformity.”involved reduction of the deformity.”
Morbidity report on surgical treatment of spondylolisthesisMorbidity report on surgical treatment of spondylolisthesis
Scoliosis Research Society (1988)Scoliosis Research Society (1988)
LUMBO-SACRAL SPONDYLOLISTHESISLUMBO-SACRAL SPONDYLOLISTHESISRoot ComplicationsRoot Complications
INSTRUMENTATION - FUSIONINSTRUMENTATION - FUSION
““IN SITU” FUSIONSIN SITU” FUSIONS 960960 8 cases (0.8%)8 cases (0.8%)
REDUCTION - FUSIONREDUCTION - FUSION 237237 3 cases (1.2%)3 cases (1.2%)
Morbidity report on surgical treatment of spondylolisthesisMorbidity report on surgical treatment of spondylolisthesis
Scoliosis Research Society (1997)Scoliosis Research Society (1997)
LUMBO-SACRAL SPONDYLOLISTHESISLUMBO-SACRAL SPONDYLOLISTHESISRoot ComplicationsRoot Complications
INSTRUMENTATION - FUSIONINSTRUMENTATION - FUSION
Anatomic evaluation of L5 nerve stretchAnatomic evaluation of L5 nerve stretchin spondylolisthesis reductionin spondylolisthesis reduction
D.M. Petraco et al.,D.M. Petraco et al.,Spine, XXI, 10, 1996Spine, XXI, 10, 1996
Anatomic evaluation of L5 nerve stretchAnatomic evaluation of L5 nerve stretchin spondylolisthesis reductionin spondylolisthesis reduction
D.M. Petraco et al.,D.M. Petraco et al.,Spine, XXI, 10, 1996Spine, XXI, 10, 1996
RIDUZIONE INTRAOPERATORIARIDUZIONE INTRAOPERATORIA
COMPLICANZE RADICOLARICOMPLICANZE RADICOLARI
RIDUZIONE INTRAOPERATORIARIDUZIONE INTRAOPERATORIA
COMPLICANZE RADICOLARICOMPLICANZE RADICOLARI
SOLO IL 29% DELLA TENSIONE SULLE RADICI
PER UNA COMPLETA RIDUZIONEDI UNO SCIVOLAMENTO DEL 100%
AVVIENE NEL CORSO DELLA PRIMA META’DELLA RIDUZIONE
D. M. Petraco 1996D. M. Petraco 1996
..
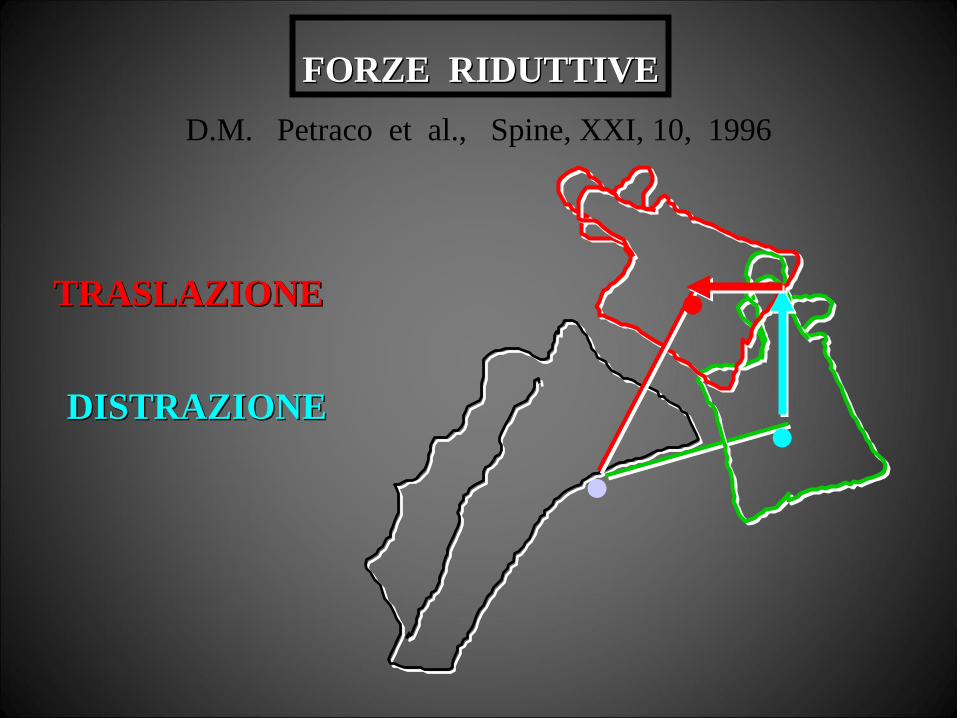
.DISTRAZIONEDISTRAZIONE
FORZE RIDUTTIVEFORZE RIDUTTIVE
TRASLAZIONETRASLAZIONE
D.M. Petraco et al., Spine, XXI, 10, 1996
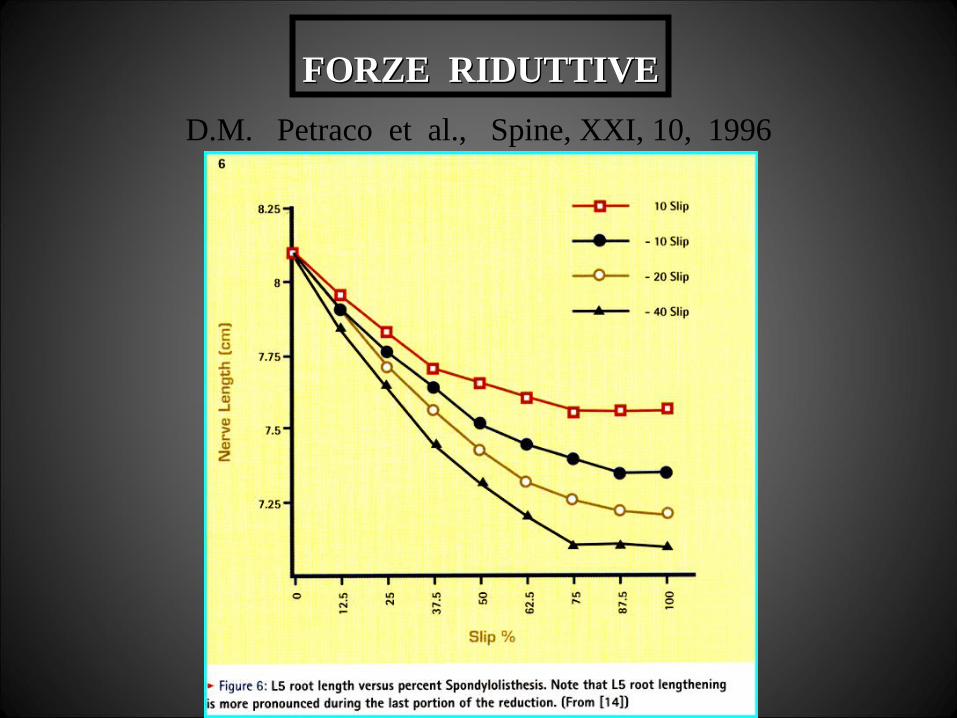
FORZE RIDUTTIVEFORZE RIDUTTIVE
D.M. Petraco et al., Spine, XXI, 10, 1996

...
DISTRAZIONE ∆ +
TRASLAZIONE ∆ -
.
DISTRAZIONE ∆ -
TRASLAZIONE ∆ +
PRIMA PARTEPRIMA PARTE DELLA RIDUZIONEDELLA RIDUZIONE
SECONDA PARTESECONDA PARTEDELLA RIDUZIONEDELLA RIDUZIONE
TRASLAZIONETRASLAZIONE
(SECONDA PARTE DELLA RIDUZIONE)(SECONDA PARTE DELLA RIDUZIONE)
E’ POTENZIALMENTE LA PIU’ PERICOLOSA E’ POTENZIALMENTE LA PIU’ PERICOLOSA
D.M. Petraco et al., Spine, XXI, 10, 1996D.M. Petraco et al., Spine, XXI, 10, 1996
LA RIDUZIONE DEVE ESSERELA RIDUZIONE DEVE ESSERE
VALUTATA CONSIDERANDOVALUTATA CONSIDERANDO
IL BILANCIAMENTO TRIDIMENSIONALEIL BILANCIAMENTO TRIDIMENSIONALE
DI TUTTO IL RACHIDEDI TUTTO IL RACHIDE
E CIO’ COINVOLGE LA SCELTAE CIO’ COINVOLGE LA SCELTA
SULL’ESTENSIONE PROSSIMALESULL’ESTENSIONE PROSSIMALE
DELL’ARTRODESI - STRUMENTAZIONEDELL’ARTRODESI - STRUMENTAZIONE
ARTRODESIARTRODESI
TIPO DI ARTRODESITIPO DI ARTRODESI
ARTRODESI ARTRODESI INTERSOMATICAINTERSOMATICA
ARTRODESI ARTRODESI INTERSOMATICAINTERSOMATICA
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
> 25 35 a.> 25 35 a.
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
> 25 35 a.> 25 35 a.
CAGES CAGES
> 25 35 a.> 25 35 a.
CAGES CAGES
> 25 35 a.> 25 35 a.
IN RAGIONE DELIN RAGIONE DEL
POSSIBILE COLLASSO DELL’INNESTOPOSSIBILE COLLASSO DELL’INNESTO
CORTICO - SPONGIOSOCORTICO - SPONGIOSO
TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
PRELEVATO DALL’ILEOPRELEVATO DALL’ILEORAGGIUNTO PER VIA SOTTOCUTANEARAGGIUNTO PER VIA SOTTOCUTANEA
DALL’INCISIONE MEDIANADALL’INCISIONE MEDIANA
TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO

TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
DUE OSTEOTOMI DI EGUALE LUNGHEZZA FORMANODUE OSTEOTOMI DI EGUALE LUNGHEZZA FORMANOUN DIEDRO ORTOGONALE CHE CONSENTE DI RICAVAREUN DIEDRO ORTOGONALE CHE CONSENTE DI RICAVARE
UN INNESTO CORTINO - SPONGIOSO DI ALTEZZA UN INNESTO CORTINO - SPONGIOSO DI ALTEZZA E PROFONDITA’ PRE DETERMINATEE PROFONDITA’ PRE DETERMINATE

TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
PRELEVATO DALL’ILEORAGGIUNTO PER VIA SOTTOCUTANEA
DALL’INCISIONE MEDIANA

TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
L’INNESTO VIENE QUINDI RIDOTTOIN DUE META’ SECONDO L’ALTEZZA
DETERMINATA DA UNA PROBE
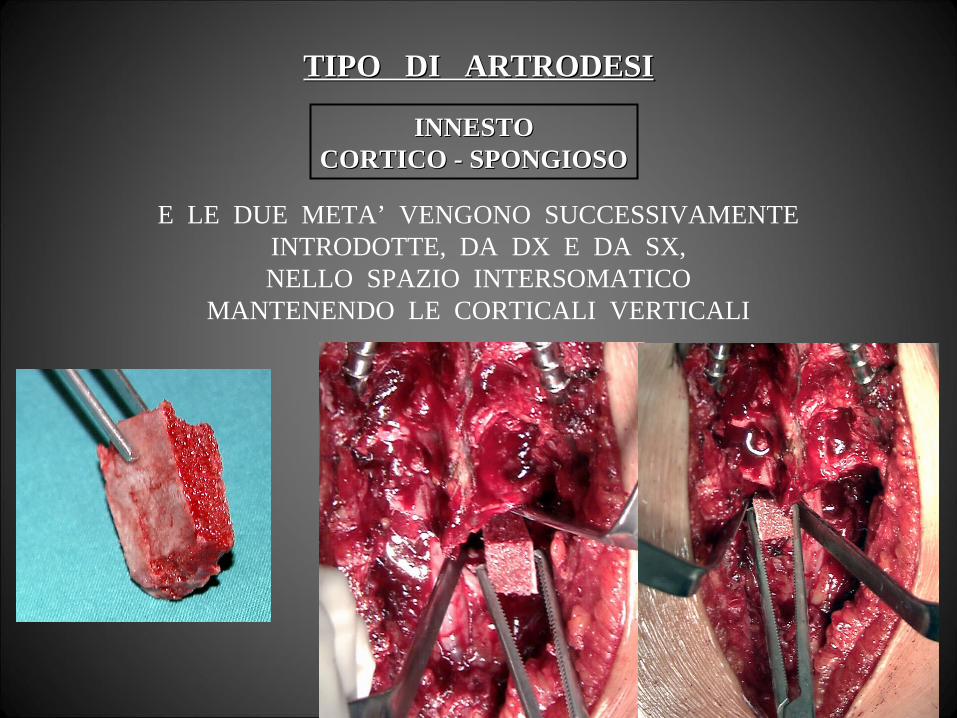
TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
E LE DUE META’ VENGONO SUCCESSIVAMENTEINTRODOTTE, DA DX E DA SX,NELLO SPAZIO INTERSOMATICO
MANTENENDO LE CORTICALI VERTICALI
TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
MENTRE LA RIDUZIONE VIENE MANTENUTADAL SISTEMA PROVVISORIO

TIPO DI ARTRODESITIPO DI ARTRODESI
INNESTOINNESTOCORTICO - SPONGIOSOCORTICO - SPONGIOSO
MENTRE LA RIDUZIONE VIENE MANTENUTAMENTRE LA RIDUZIONE VIENE MANTENUTADAL SISTEMA PROVVISORIODAL SISTEMA PROVVISORIO
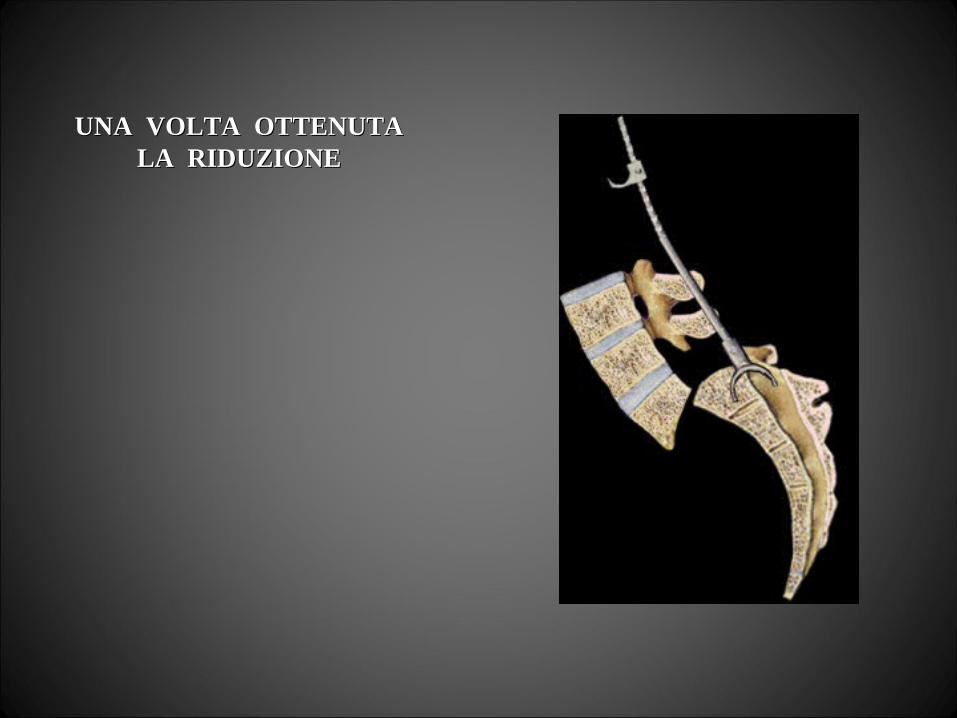
UNA VOLTA OTTENUTAUNA VOLTA OTTENUTALA RIDUZIONELA RIDUZIONE
UNA VOLTA OTTENUTAUNA VOLTA OTTENUTALA RIDUZIONELA RIDUZIONE
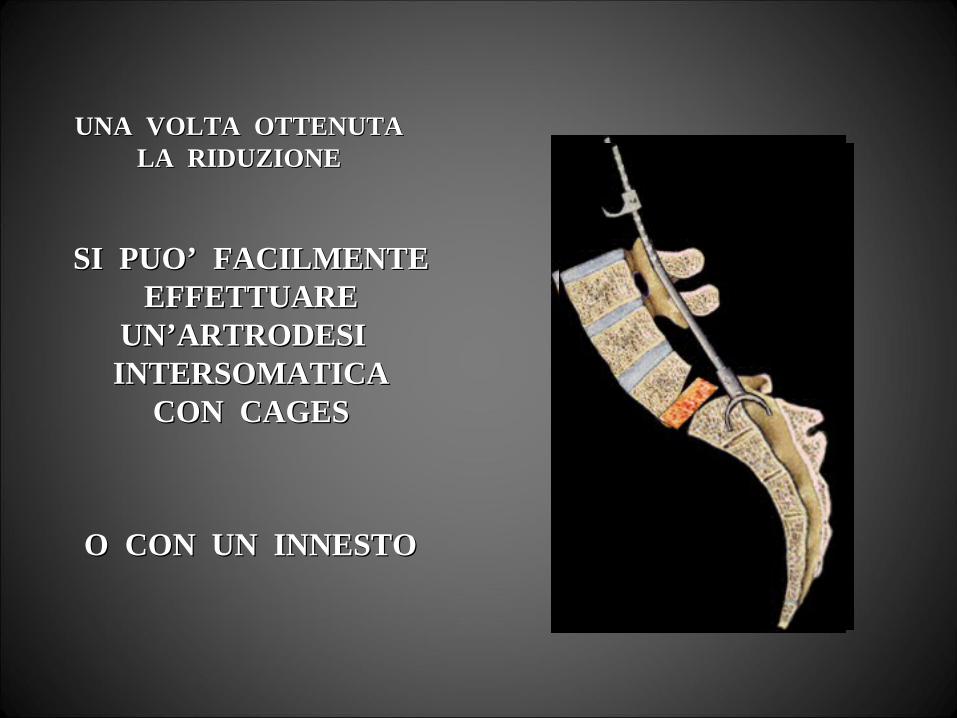
SI PUO’ FACILMENTESI PUO’ FACILMENTEEFFETTUAREEFFETTUARE
UN’ARTRODESI UN’ARTRODESI INTERSOMATICAINTERSOMATICA
CON CAGESCON CAGES
O CON UN INNESTOO CON UN INNESTO

ED UNA STABILIZZAZIONEED UNA STABILIZZAZIONE SEGMENTARIASEGMENTARIA
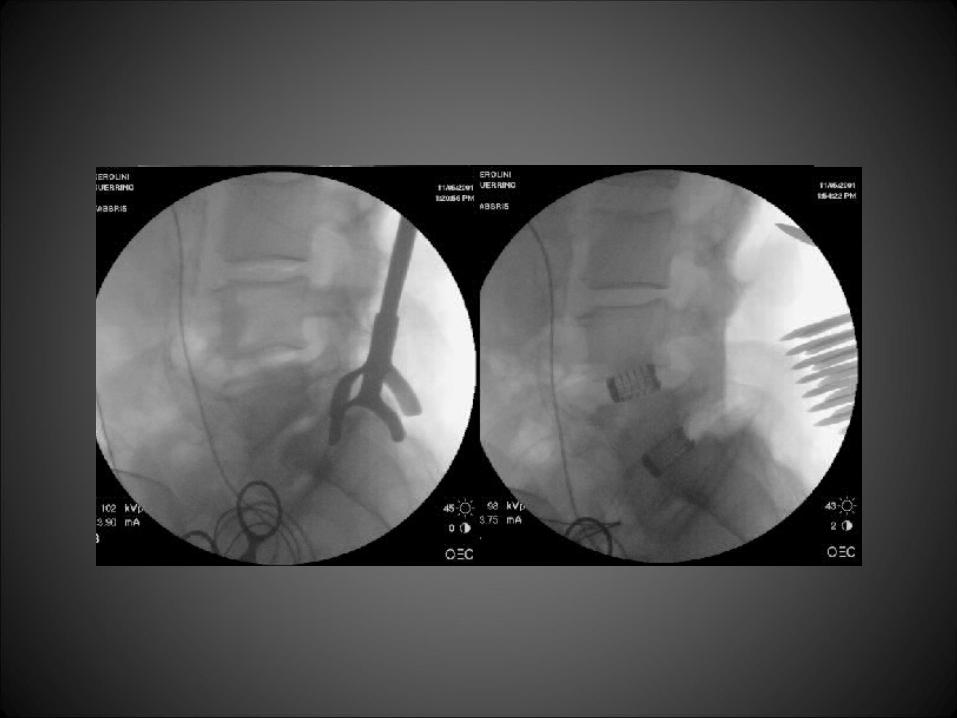

E QUINDI RIMUOVEREE QUINDI RIMUOVEREIL SISTEMA TEMPORANEOIL SISTEMA TEMPORANEO
DI DISTRAZIONEDI DISTRAZIONE
ESTENSIONE DELL’ ARTRODESIESTENSIONE DELL’ ARTRODESI
ESTENSIONE DELL’ ARTRODESIESTENSIONE DELL’ ARTRODESI
ASSETTO SAGITTALEASSETTO SAGITTALE
LSLSRACHIDERACHIDE
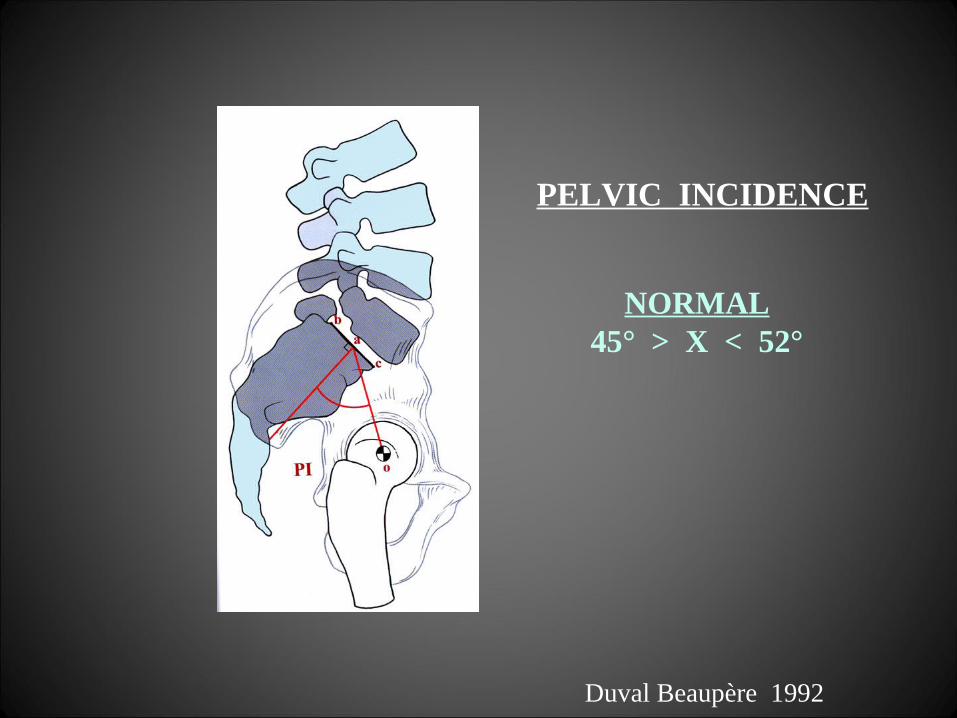
PELVIC INCIDENCE
NORMAL45° > X < 52°
Duval Beaupère 1992
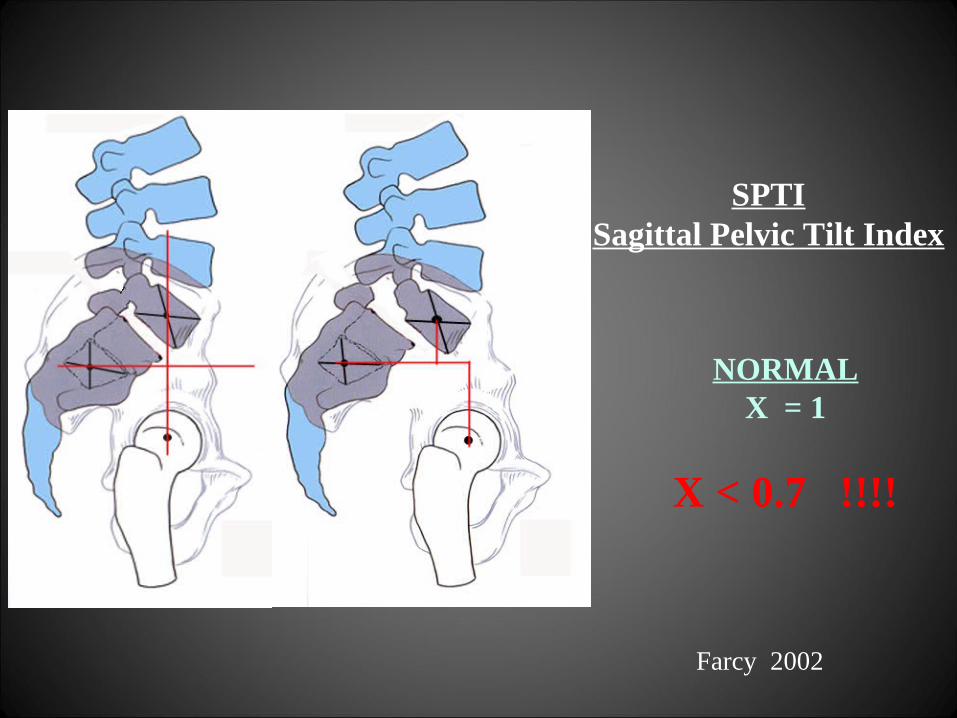
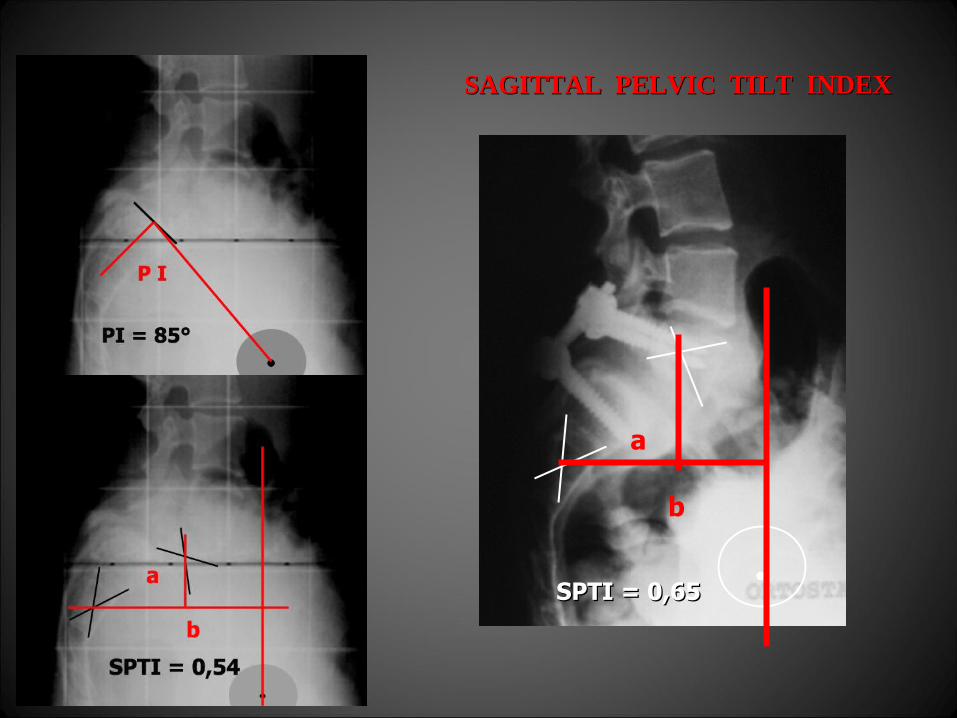
SPTISagittal Pelvic Tilt Index
NORMALX = 1
X < 0.7 !!!!
Farcy 2002

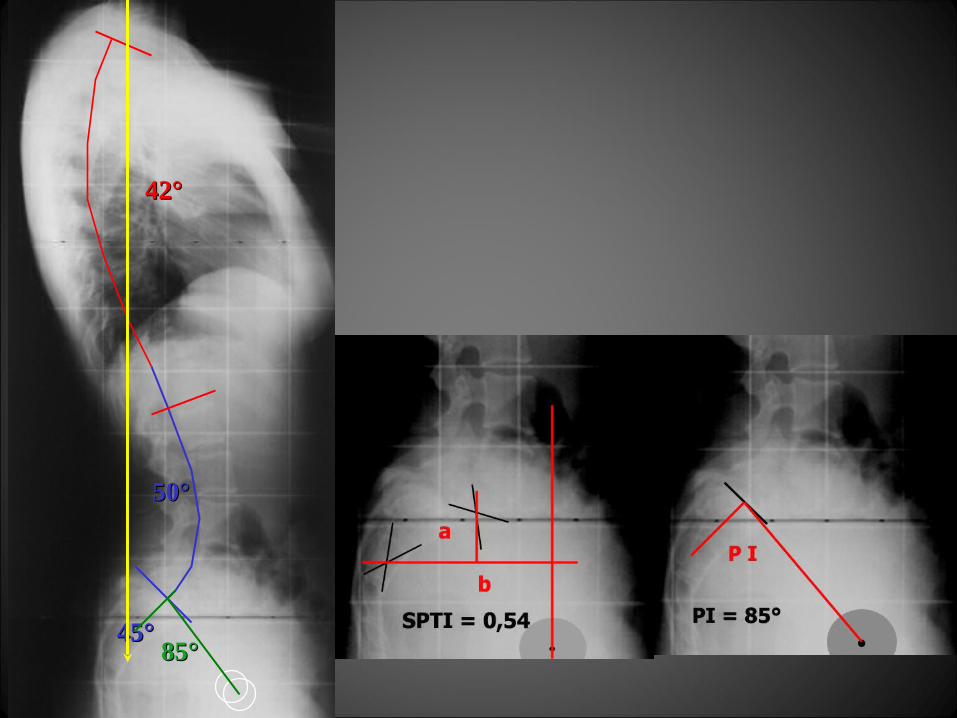
ESTENSIONE DELL’ ARTRODESIESTENSIONE DELL’ ARTRODESI
MISURAZIONI RADIOGRAFICHEMISURAZIONI RADIOGRAFICHE(P.I. - S.P.T.I.)(P.I. - S.P.T.I.)

ESTENSIONE dell’ ARTRODESI
ASSETTO SAGITTALEASSETTO SAGITTALE
RX STANDARDRX STANDARD
L’INTER RELAZIONE TRA ASSETTO L’INTER RELAZIONE TRA ASSETTO SAGITTALE DEL RACHIDE E SAGITTALE DEL RACHIDE E
PARAMETRIPARAMETRIRADIOGRAFICI LOMBO - SACRALIRADIOGRAFICI LOMBO - SACRALI
PUO’ CONDIZIONALE LA SCELTA CIRCAPUO’ CONDIZIONALE LA SCELTA CIRCAL’ESTENSIONE PROSSIMALE DELLAL’ESTENSIONE PROSSIMALE DELLA
ARTRODESI - STABILIZZAZIONEARTRODESI - STABILIZZAZIONE
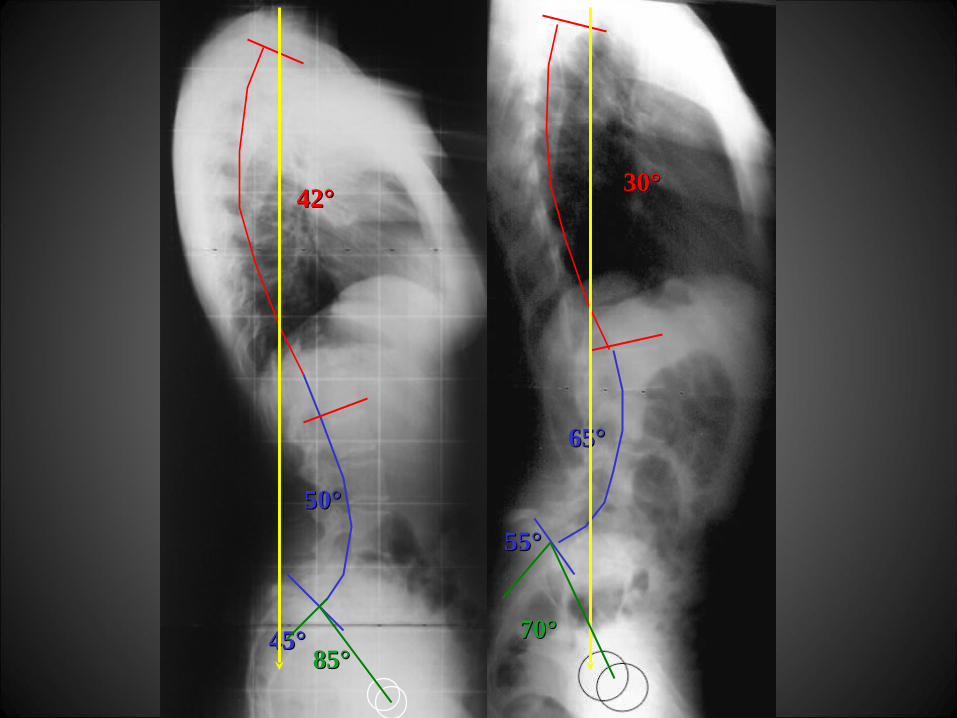
ESTENSIONE dell’ ARTRODESI
RX STANDARDRX STANDARD
45°45°
50°50°
42°42° 30°30°
65°65°
55°55°
85°85°70°70°
45°45°
50°50°
42°42°
85°85°
ESTENSIONE dell’ ARTRODESI
RX STANDARDRX STANDARD
45°45°
50°50°
42°42°
85°85°
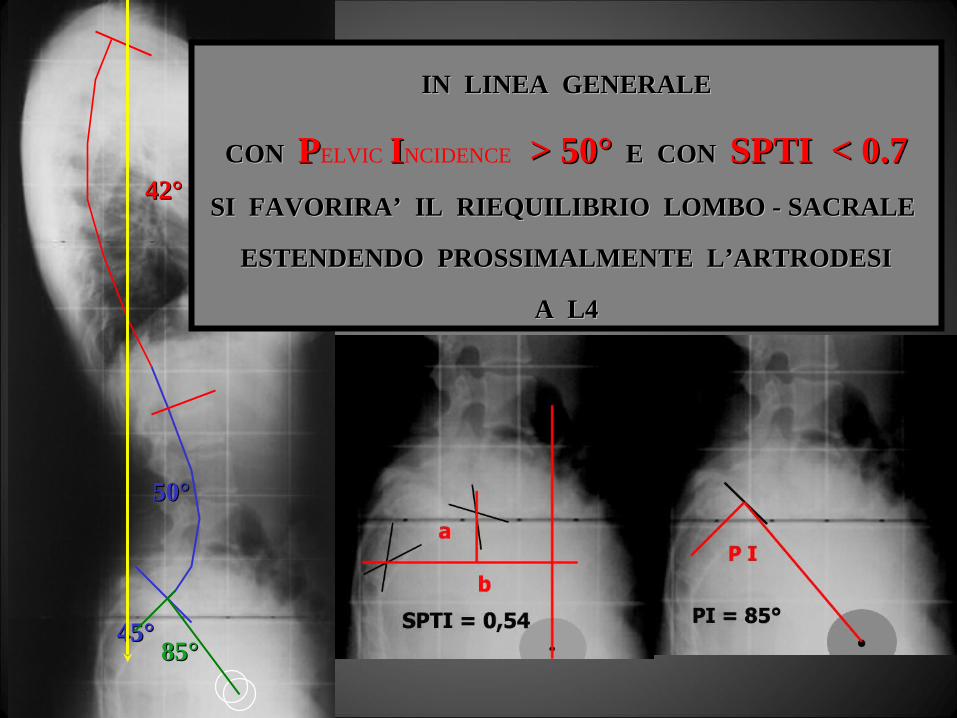
IN LINEA GENERALEIN LINEA GENERALE
CON CON PPELVIC IINCIDENCE > 50° > 50° E CON E CON SPTI < 0.7SPTI < 0.7
SI FAVORIRA’ IL RIEQUILIBRIO LOMBO - SACRALE SI FAVORIRA’ IL RIEQUILIBRIO LOMBO - SACRALE
ESTENDENDO PROSSIMALMENTE L’ARTRODESIESTENDENDO PROSSIMALMENTE L’ARTRODESI
A L4A L4
.
a
b
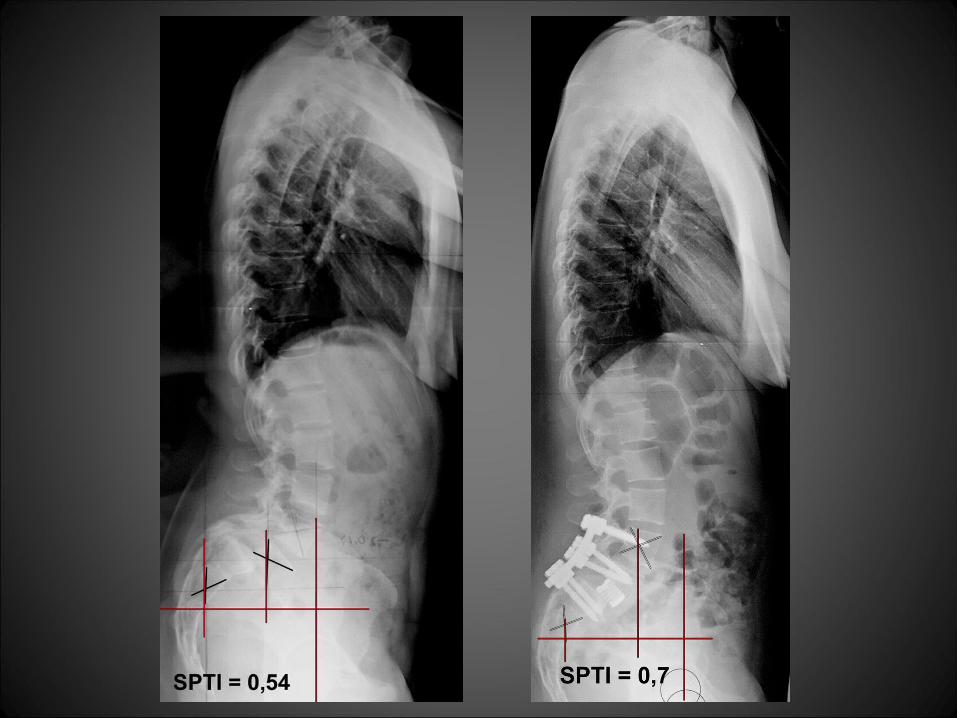
SPTI = 0,65SPTI = 0,65
SAGITTAL PELVIC TILT INDEXSAGITTAL PELVIC TILT INDEX
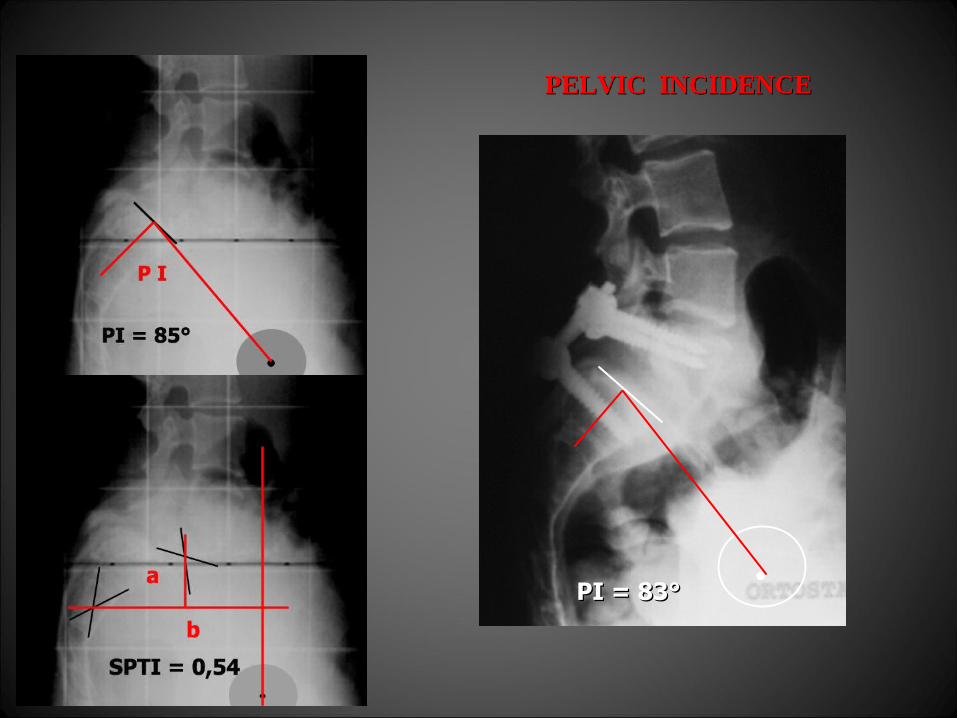
.PI = 83°PI = 83°
PELVIC INCIDENCEPELVIC INCIDENCE
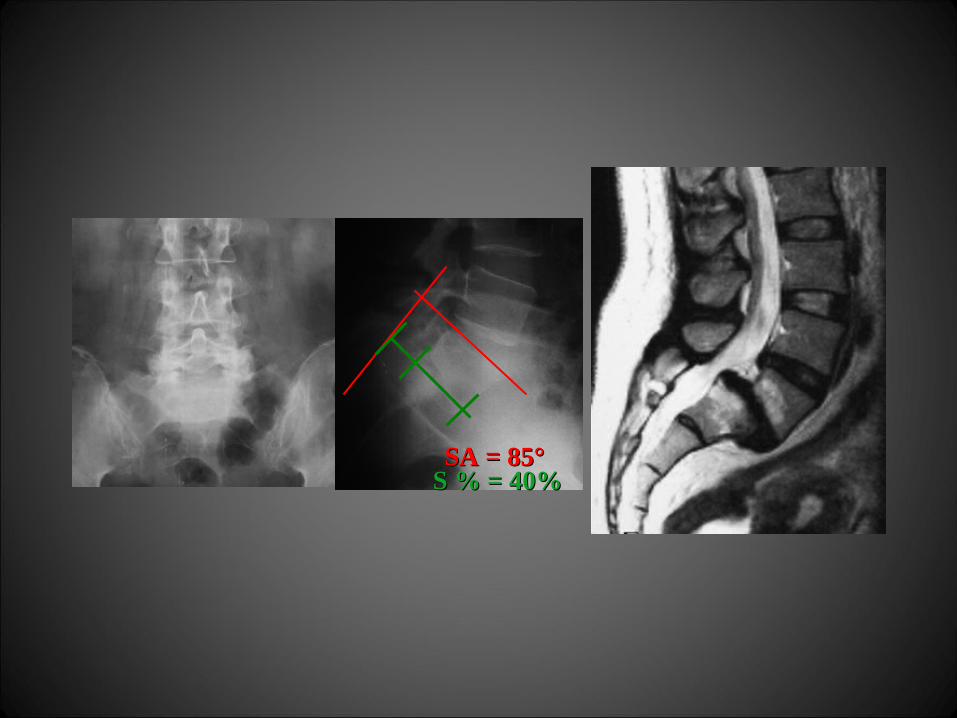
SA = 85°SA = 85°S % = 40%S % = 40%
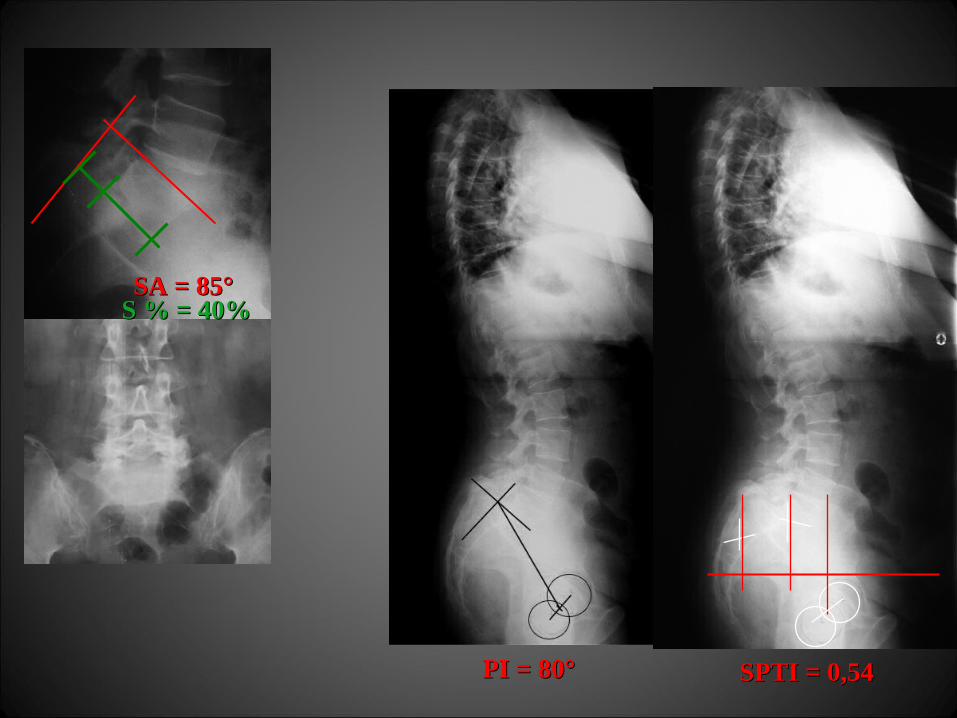
SPTI = 0,54SPTI = 0,54PI = 80°PI = 80°
SA = 85°SA = 85°S % = 40%S % = 40%
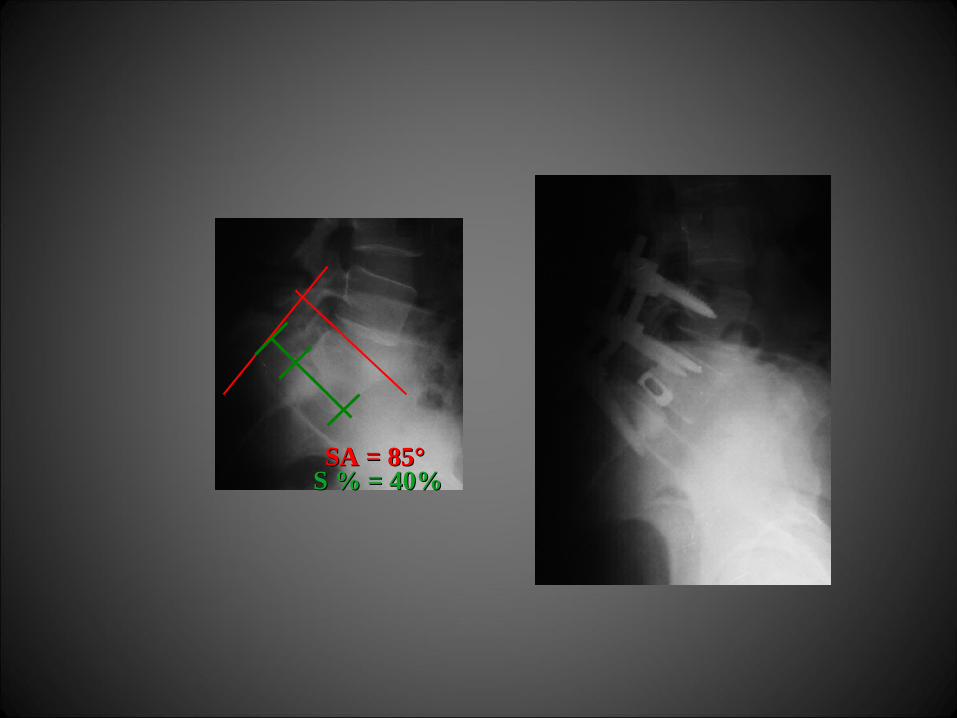
SA = 85°SA = 85°S % = 40%S % = 40%

T.G. a.18T.G. a.18 f. up 9 a.f. up 9 a.
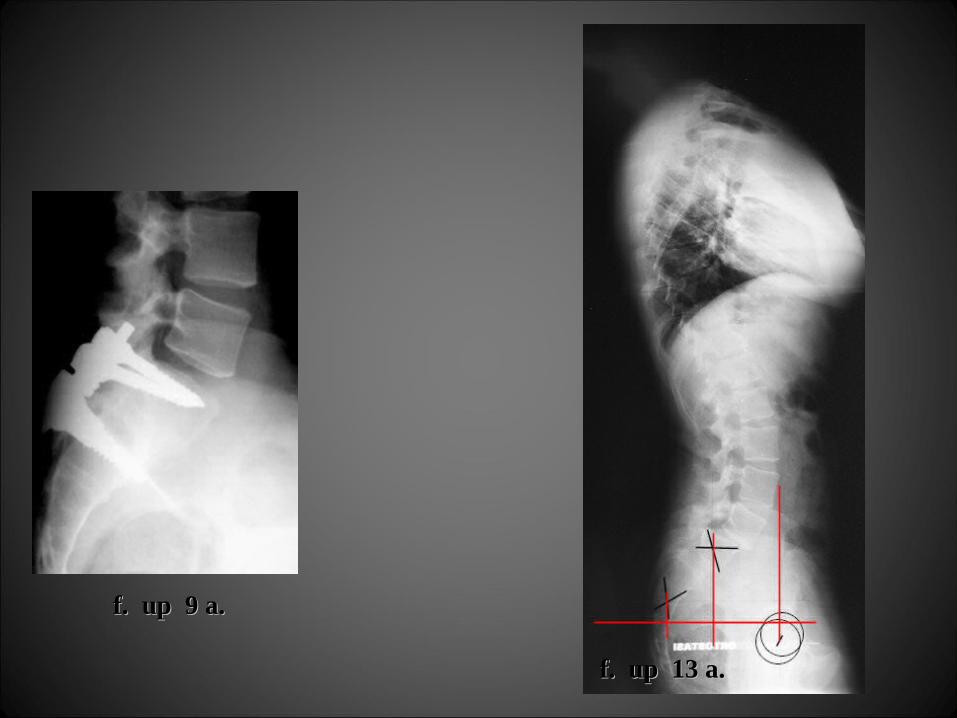
f. up 9 a.f. up 9 a.
f. up 13 a.f. up 13 a.

T.G. a.18T.G. a.18
f. up 13 a.f. up 13 a.
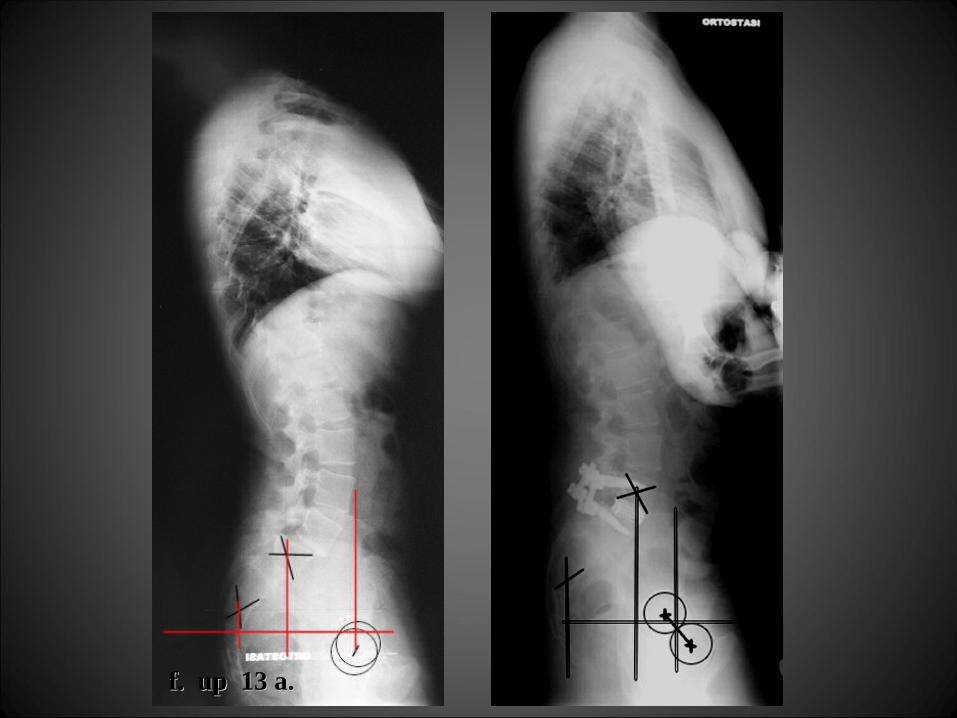
f. up 13 a.f. up 13 a.
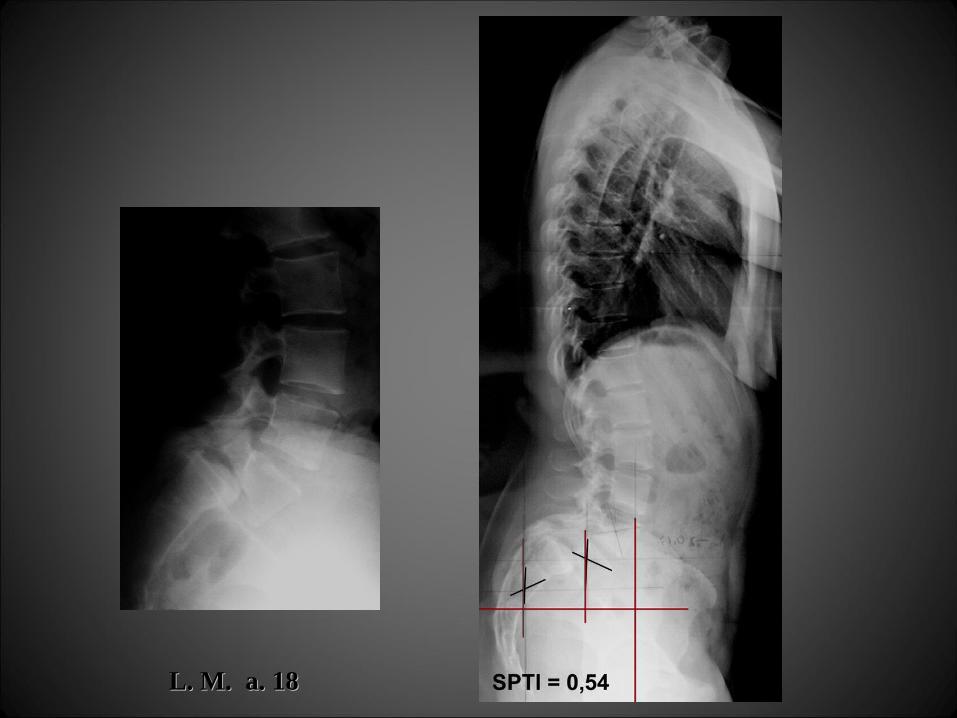
L. M. a. 18L. M. a. 18
LA STRATEGIA DITRATTAMENTO CHIRURGICO
DELLE SPONDILOLISTESI GRAVINON PUO’ PRESCINDERE
DALLO STUDIO DELLE CARATTERISTICHE
- DELL’ASSETTO SAGITTALE DEL RACHIDE IN TOTO
- DEI RAPPORTI LOMBO - PELVICI
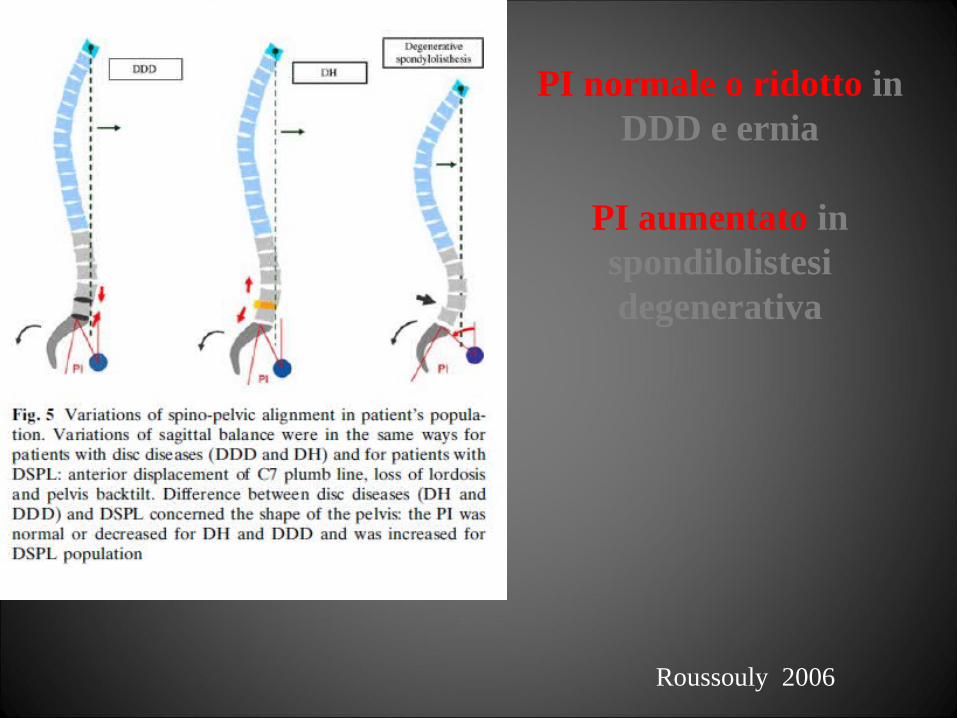
PI normale o ridotto in DDD e ernia
PI aumentato in spondilolistesi degenerativa
Roussouly 2006