Prolasso e chirurgia fasciale: steps ed evidenze - COMPARTIMENTO ANTERIORE
58
Prolasso e chirurgia fasciale: steps ed evidenze COMPARTIMENTO ANTERIORE GF. MININI
-
Upload
glup2010 -
Category
Health & Medicine
-
view
164 -
download
1
Transcript of Prolasso e chirurgia fasciale: steps ed evidenze - COMPARTIMENTO ANTERIORE
Prolasso e chirurgia fasciale:steps ed evidenze
COMPARTIMENTO ANTERIORE
GF. MININI
Shull 1992, Baden 1992Shull 1992, Baden 1992
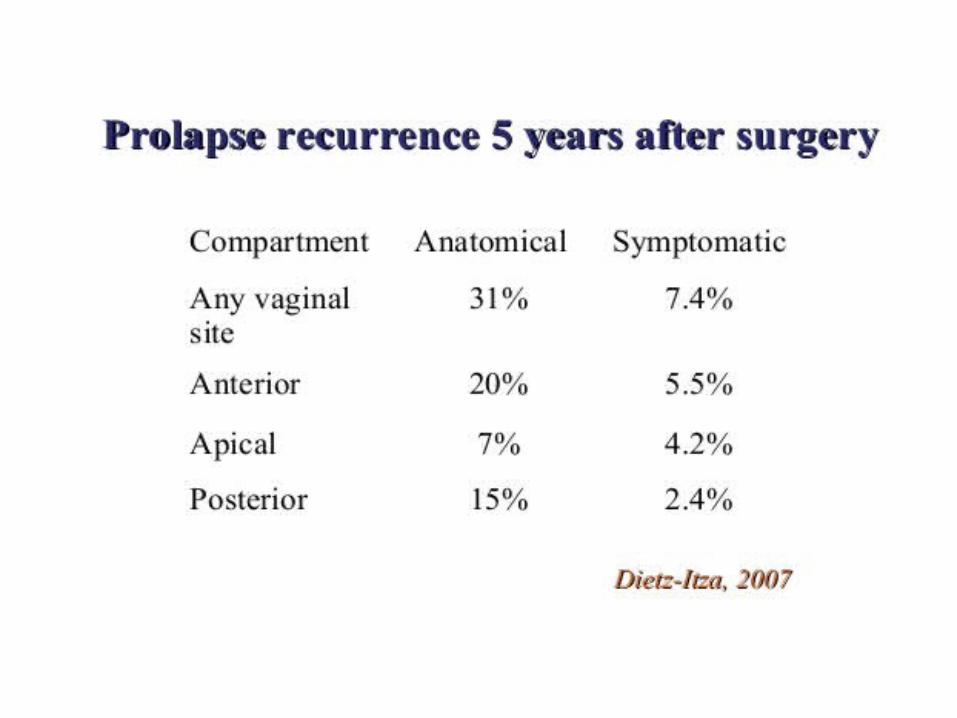
Alla fine del secolo scorso alcuni Autori rilevavano la difficoltà nello stabilizzare un risultato efficace della chirurgia vaginale del prolasso con una possibilità di recidiva variabile dal 20% al 40%
CHIRURGIA “TRADIZIONALE” RECIDIVE
1997 OLSEN 29%
2004 TEGERSTEDT 44%
2007 DIETZ-ITZA 31%

Data 22.06.2009
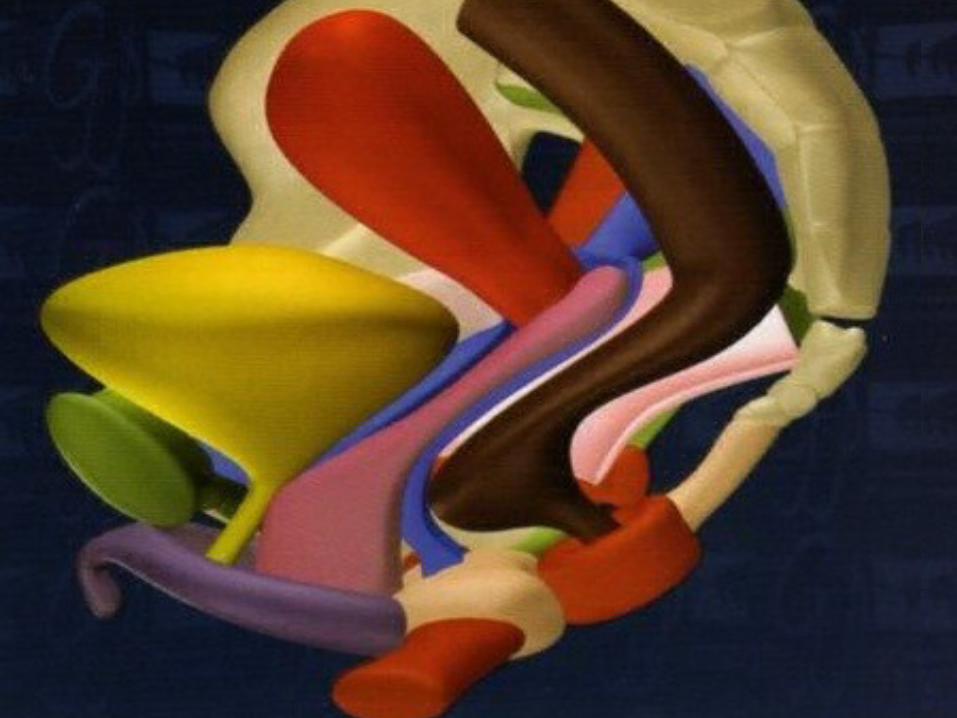
La fascia endopelvica
Courtesy by Dr. T. Mouchel
“Fin de Siècle” Anatomy
• Livelli di DeLancey• Riparazione di difetto sito-specifico• Fossa Ischiorettale• Fossa Otturatoria• Arco Tendineo della Fascia Pelvica• Legamento Sacrospinoso
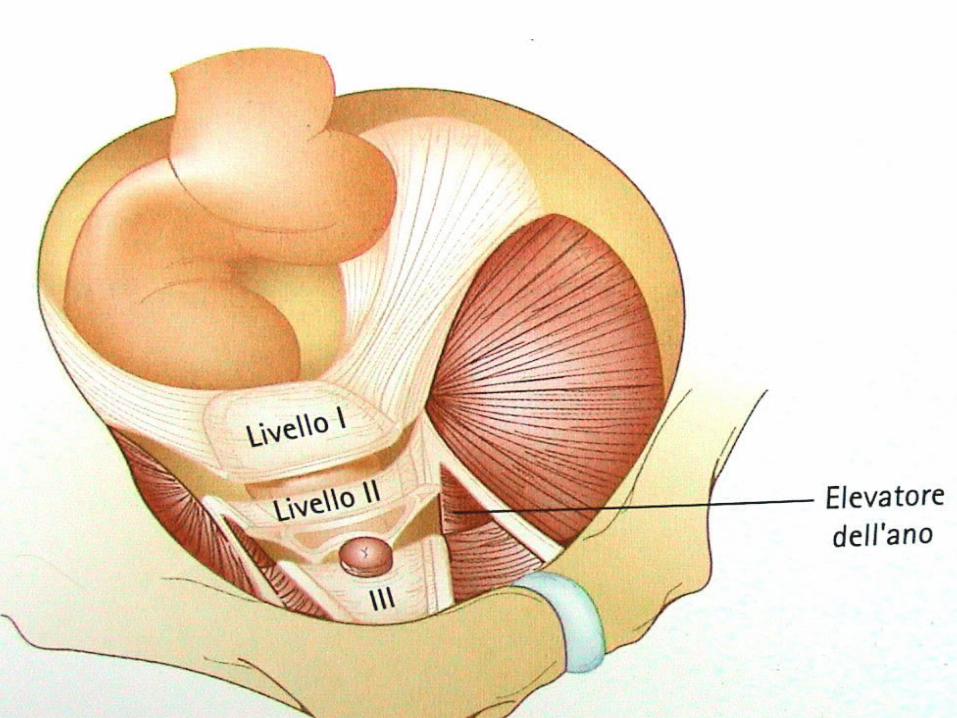
DeLancey
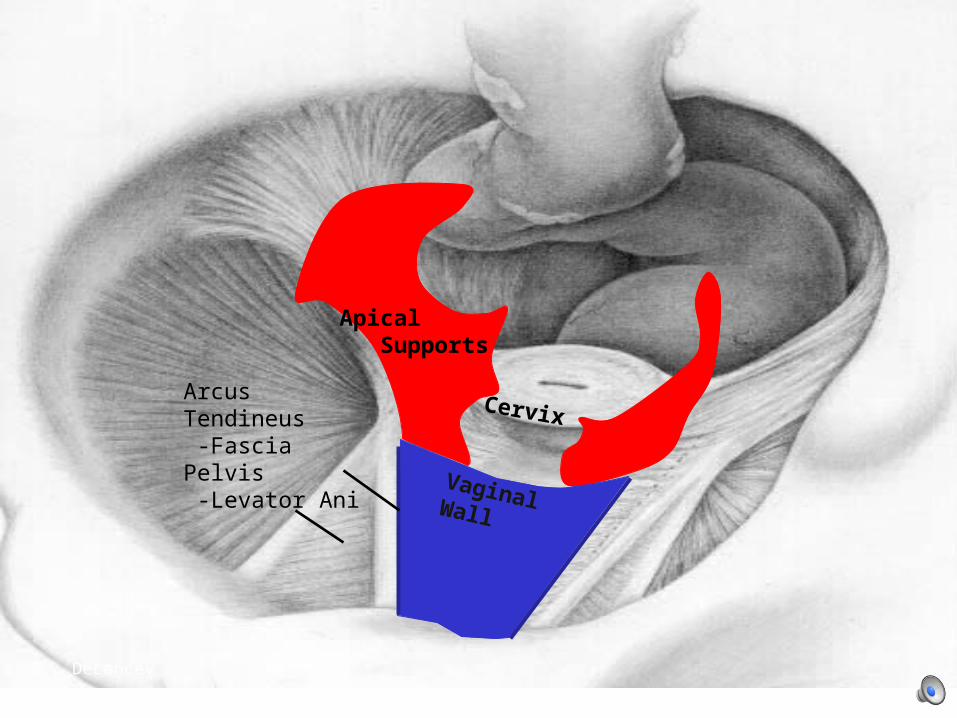
Apical Supports
Vaginal Wall
CervixArcusTendineus -Fascia Pelvis -Levator Ani
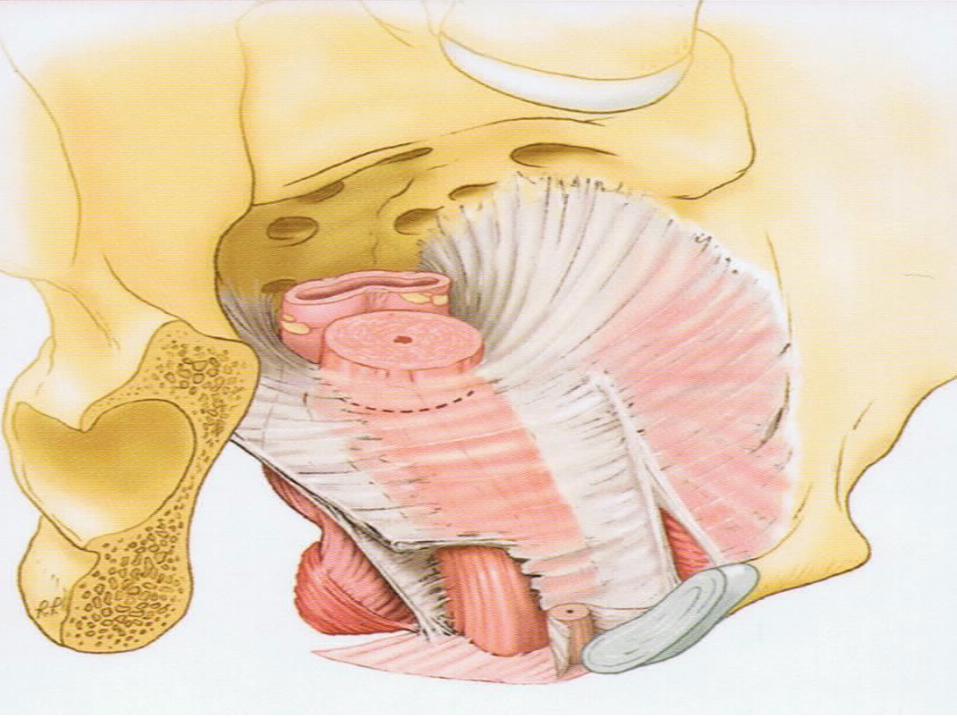
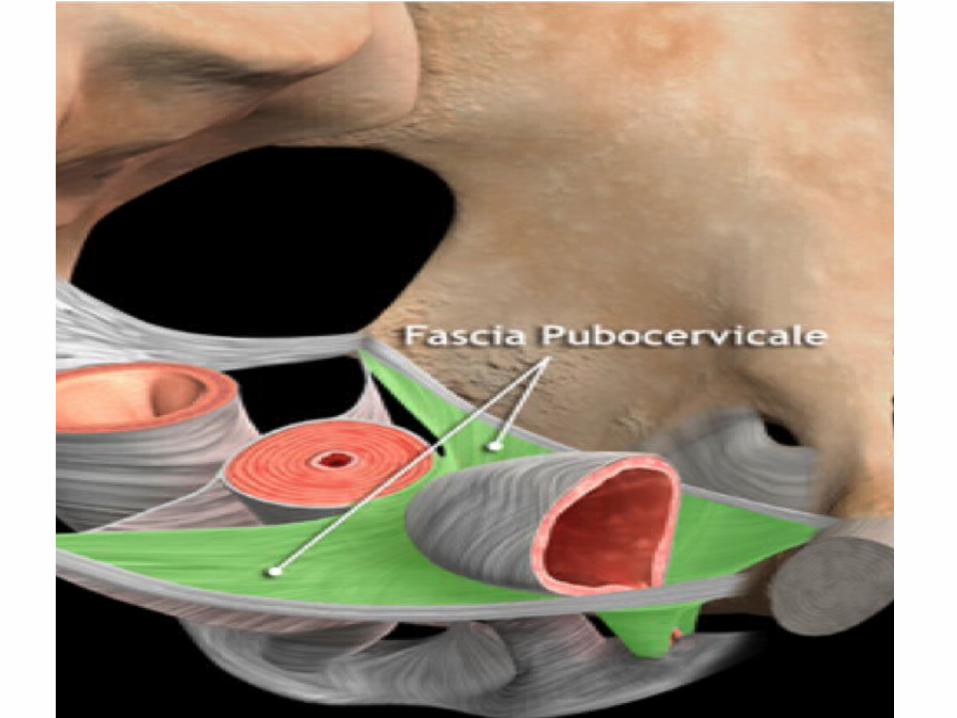

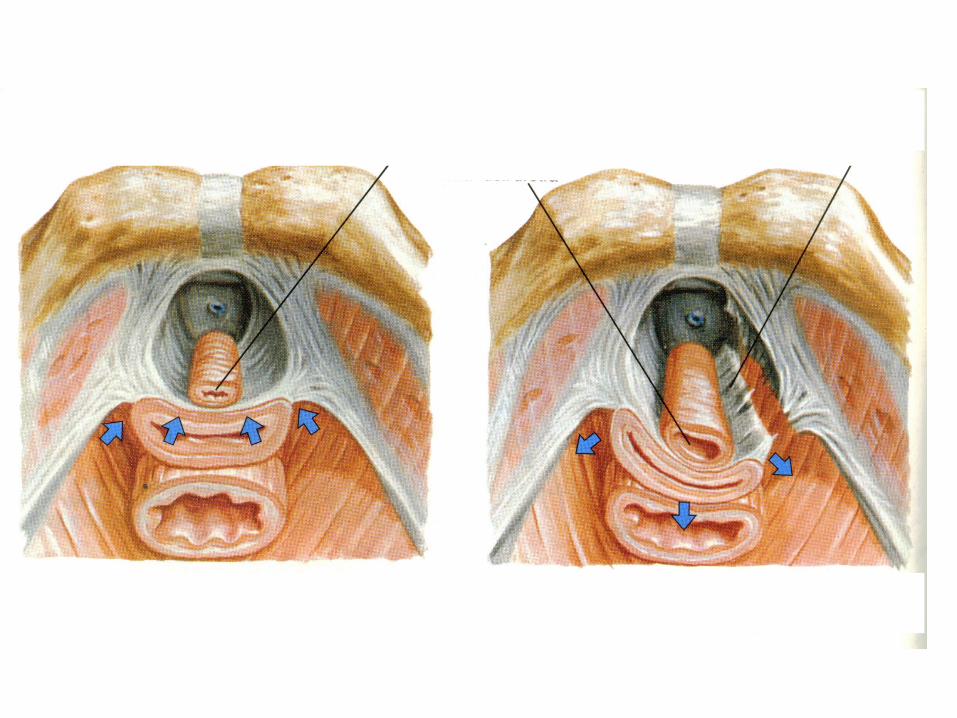
Fascia Pubocervicale e Rettovaginale
II° Livello di supporto nella pelvi
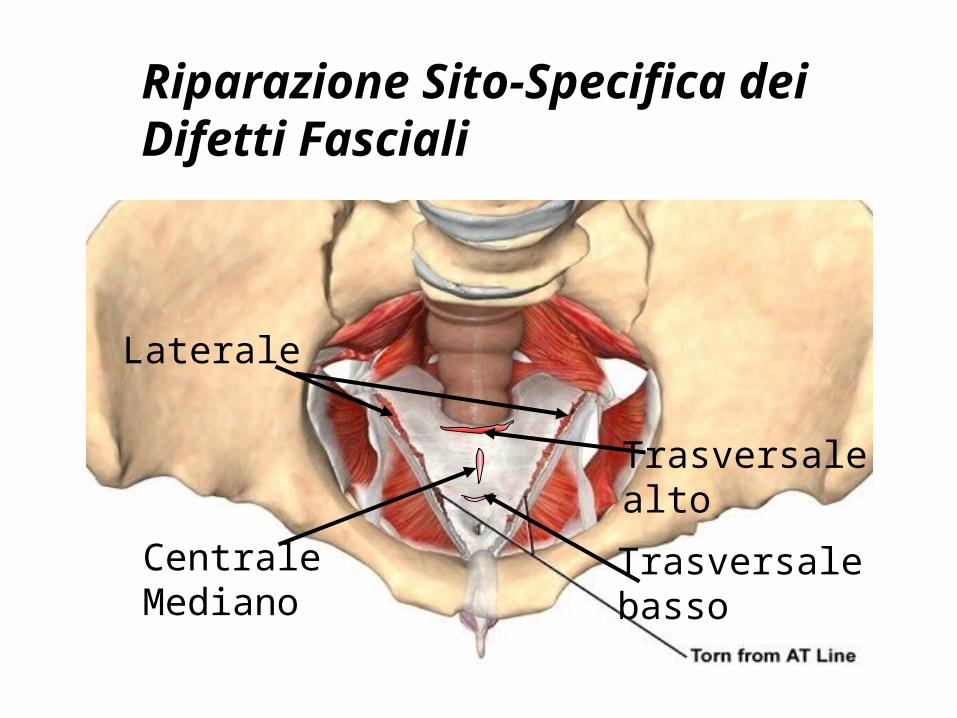
CentraleMediano
Trasversalebasso
Laterale
Trasversalealto
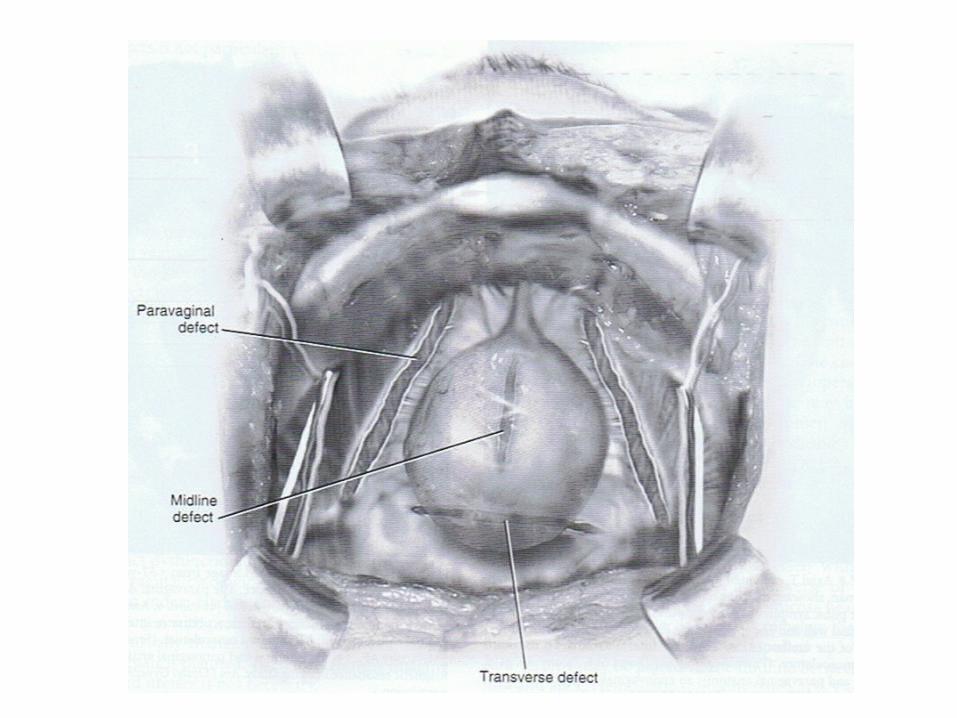
Riparazione Sito-Specifica dei Difetti Fasciali
I DIFETTI FASCIALI• Difetti fasciali del segmento anteriore
laterale dxlaterale sinmedianotrasversalepubouretrali
• Difetti fasciali del segmento superiorecomplesso cardinale/uterosacraleParacolpo superiore (1° livello di Delancey)
• Difetti fasciali del segmento posteriorelaterale dxlaterale sinmedianotrasversale altotrasversale basso

RICOSTRUZIONE FASCIALE“sito-specifica”
Identification and repair of each Identification and repair of each individual anatomical defect is individual anatomical defect is
essentialessential
““Leave the Leave the totaltotal tract intact” tract intact”
(Bob L. Shull)(Bob L. Shull)
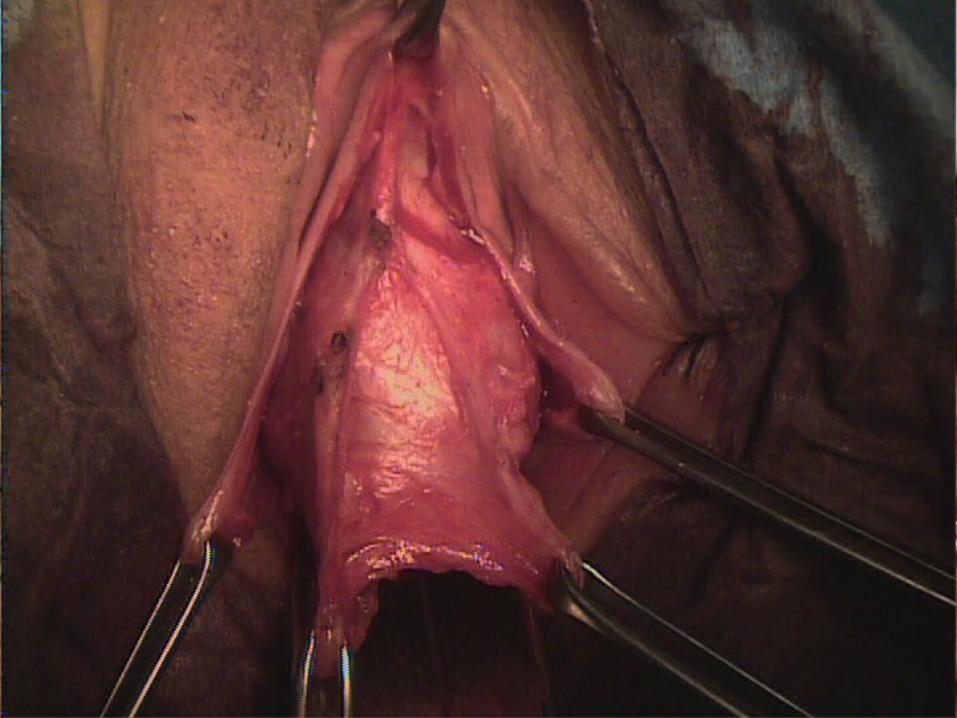
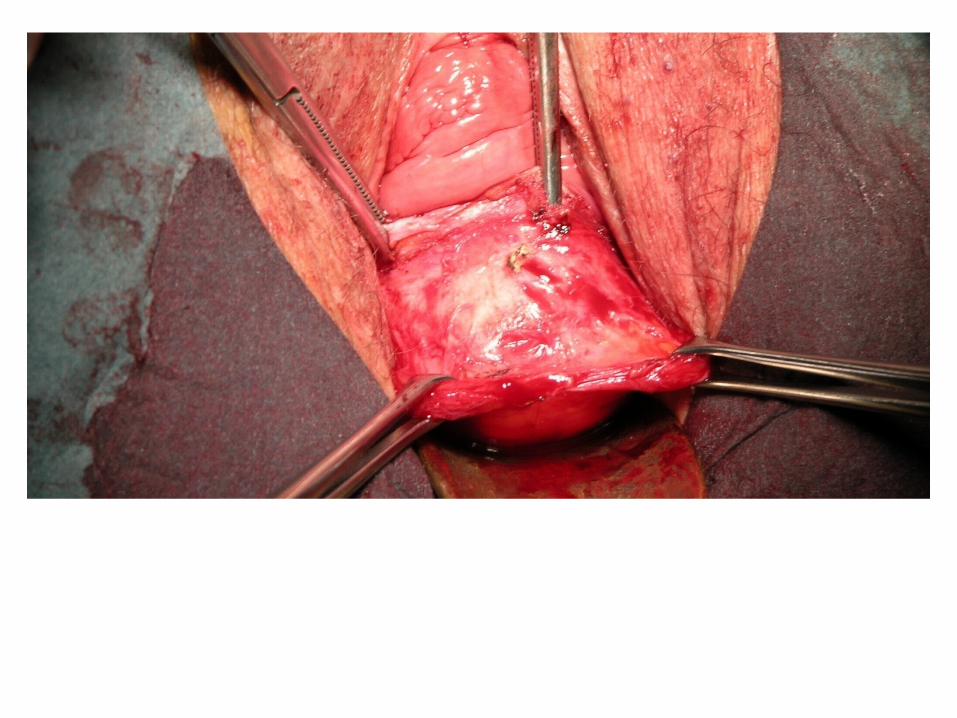
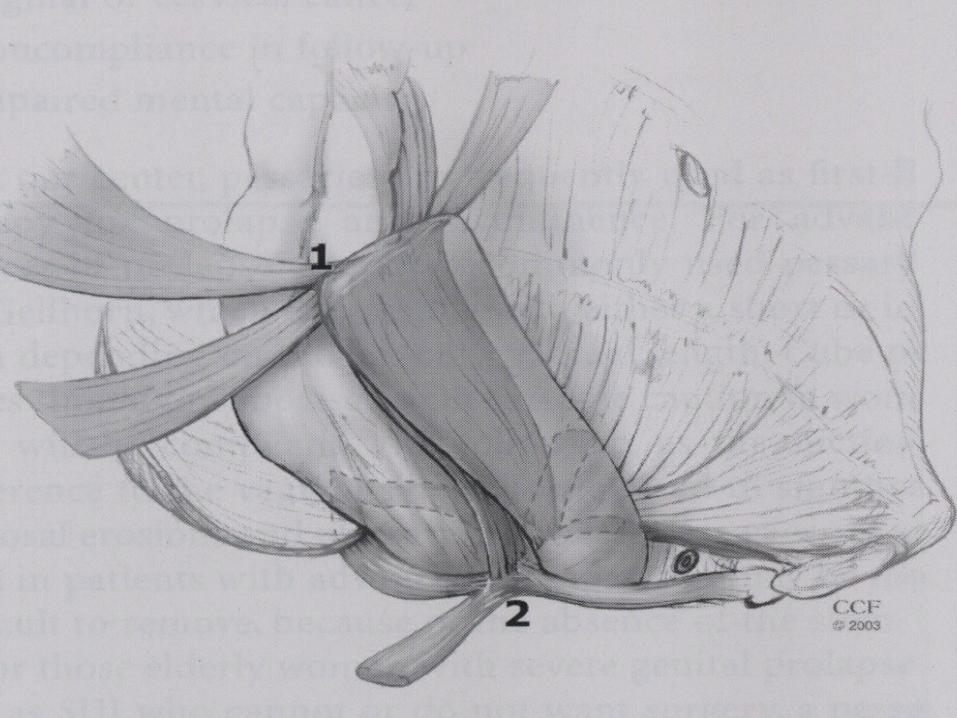
Objective of anterior colporraphy is to plicate the layers of vaginal muscolaris and adventitia overlying the bladder (pubocervical fascia) or to plicate and reattach
the paravaginal tissue in such a way as to reduce the protrusion of the bladder and vagina.
Modifications of the standard repair
M.D.Walters –M.M.Karram Urogynecology and Reconstructive Pelvic Surgery 2007
Modifications of the technique depend on how lateral the dissection is carried, where the plicating sutures are placed, whether additional layers are placed in the pubocervical fascia for extra support.

The dissection should be carried further laterally to the ischiopubic rami with more advanced prolapse
Using sharp dissection is also important to mobilize the bladder base from the vaginal apex
M.D. Walters; M.M. Karram: Urogynecology and reconstructive pelvic surgery ( 2007 )
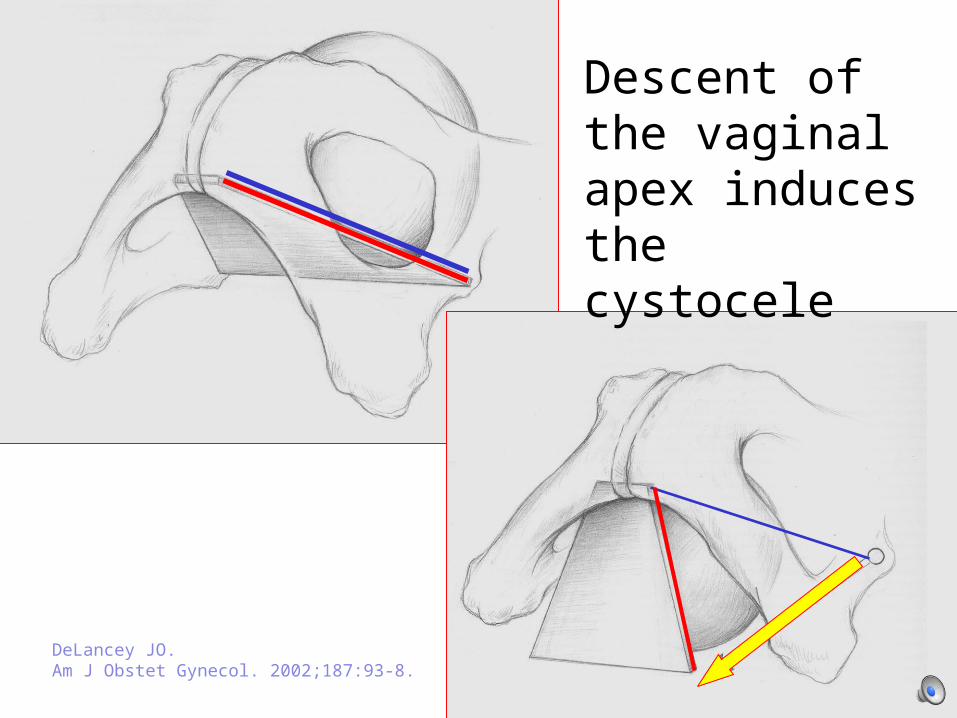
Descent of the vaginal apex induces the cystocele
DeLancey JO.Am J Obstet Gynecol. 2002;187:93-8.
60% OF BLADDER DESCENT EXPLAINED BY APICAL DESCENT


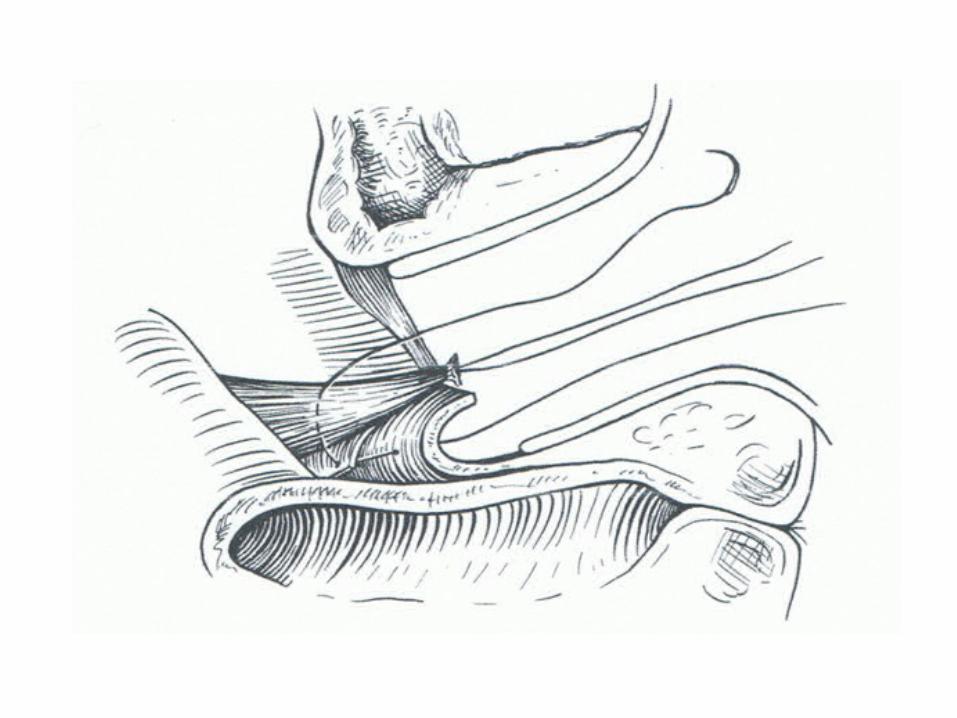
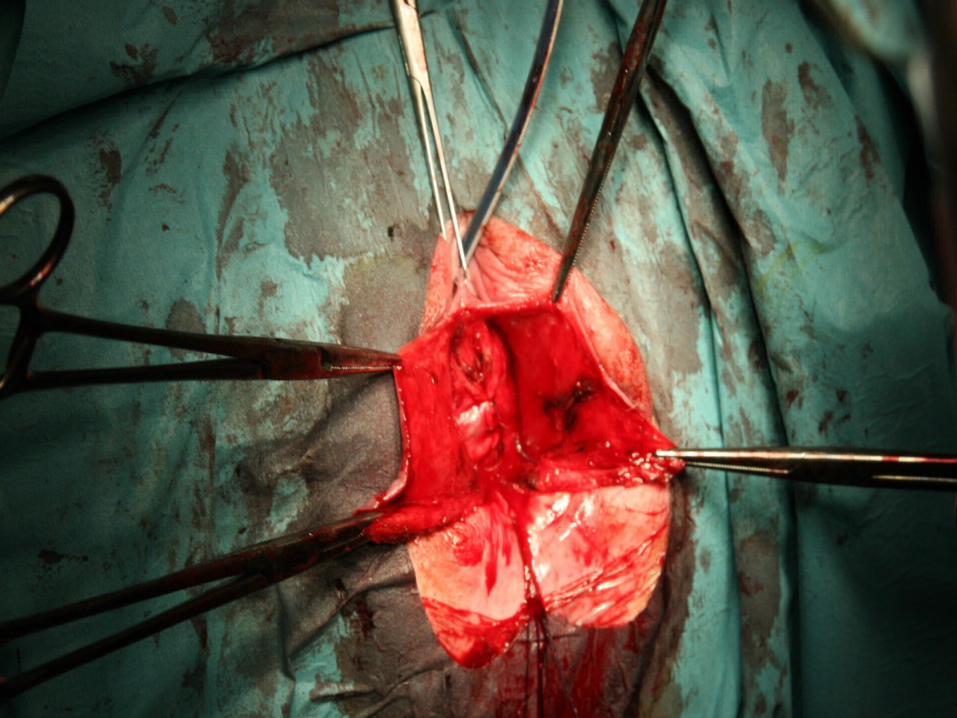
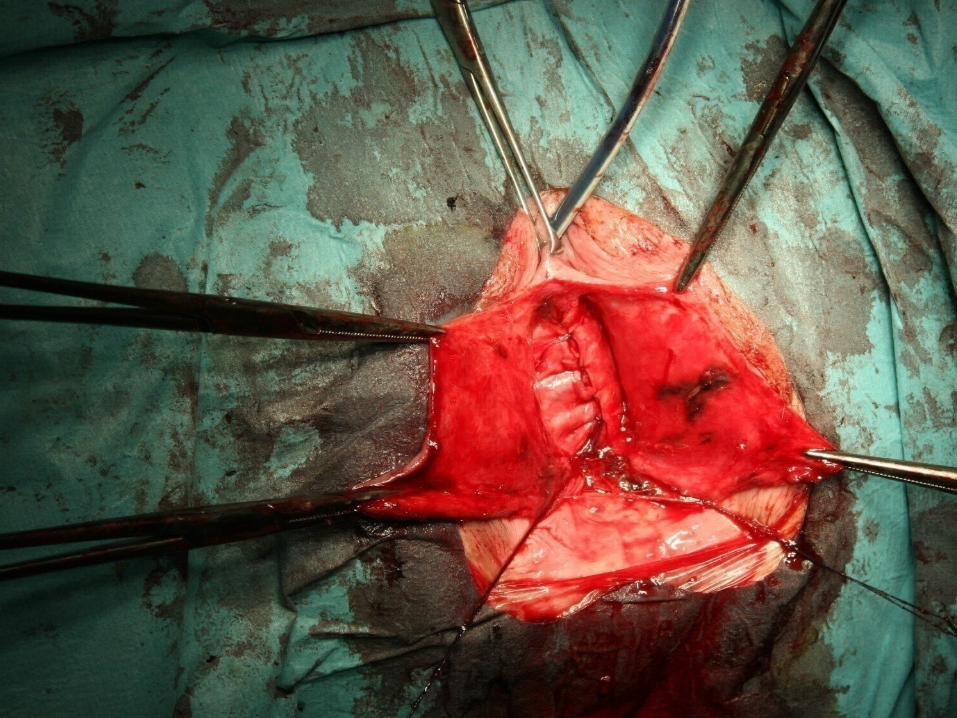
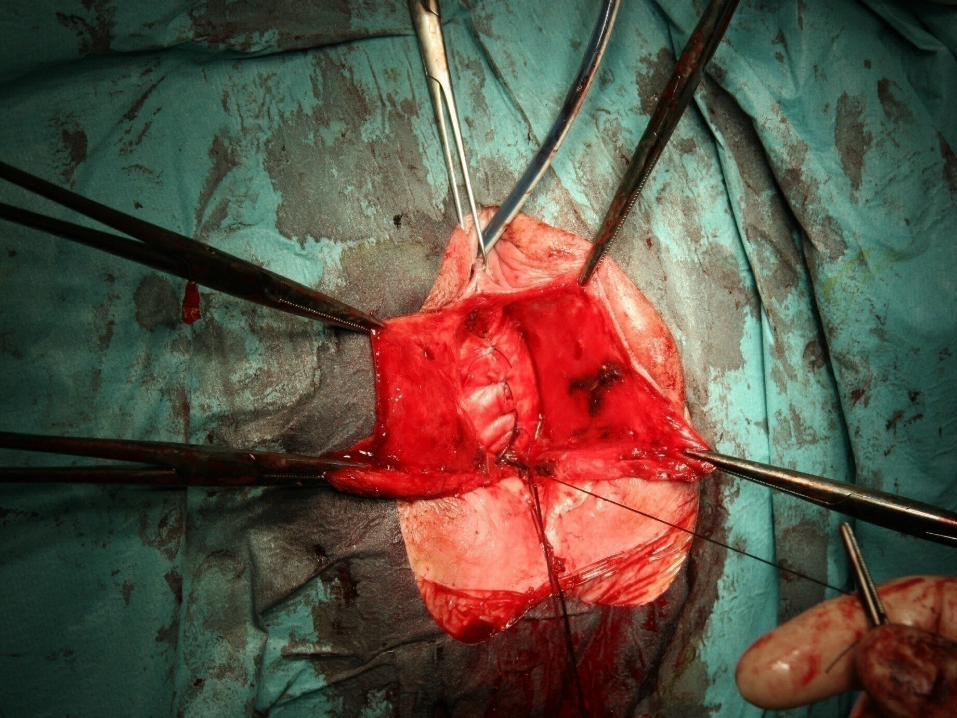
Fixation of the inferior part of the pubo-cervical fascia to the structures included in Mac Call stitches ( round, cardinal and utero-sacral ligaments )
Pubo-cervical fascia is so fixed to the perivaginal ring and the recto-vaginal septum
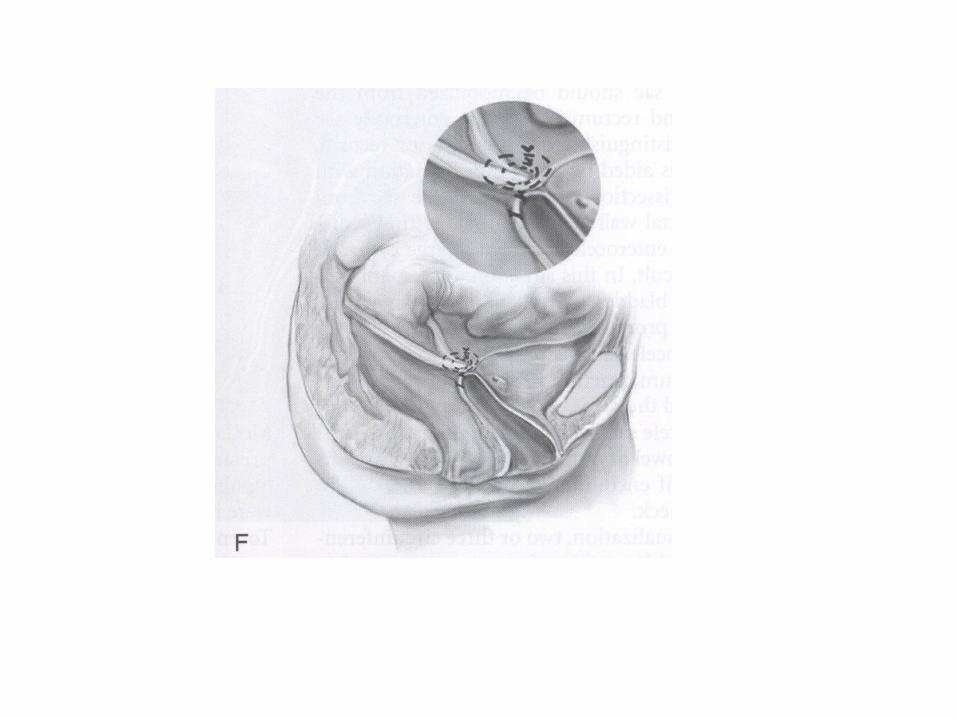
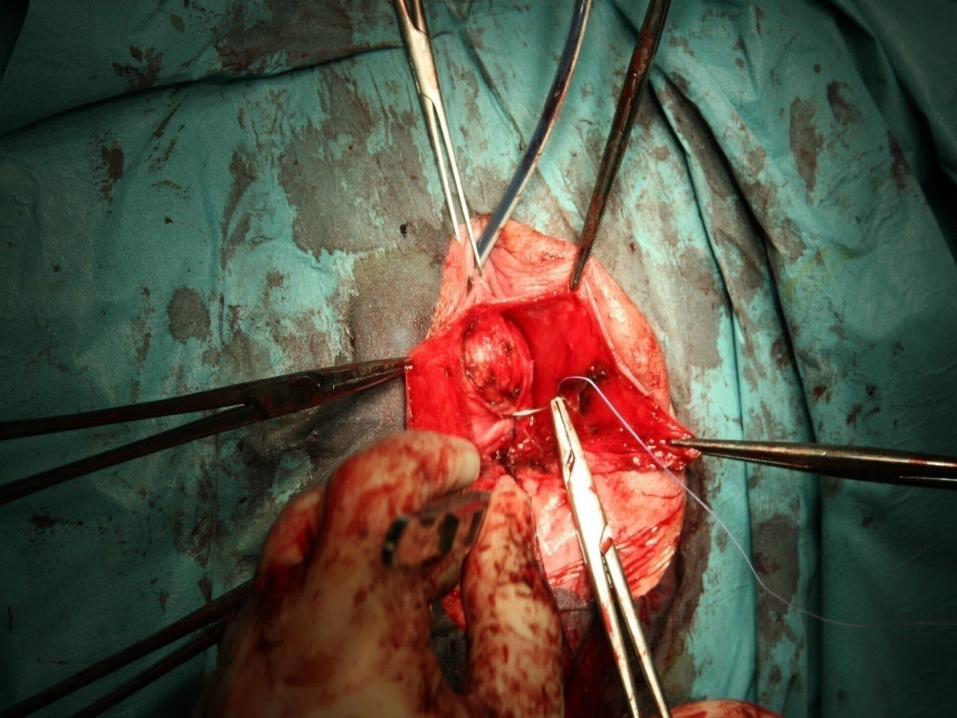
Further suspension is finally obtained using bilateral peritoneal sutures transfixed through the anterior vaginal wall
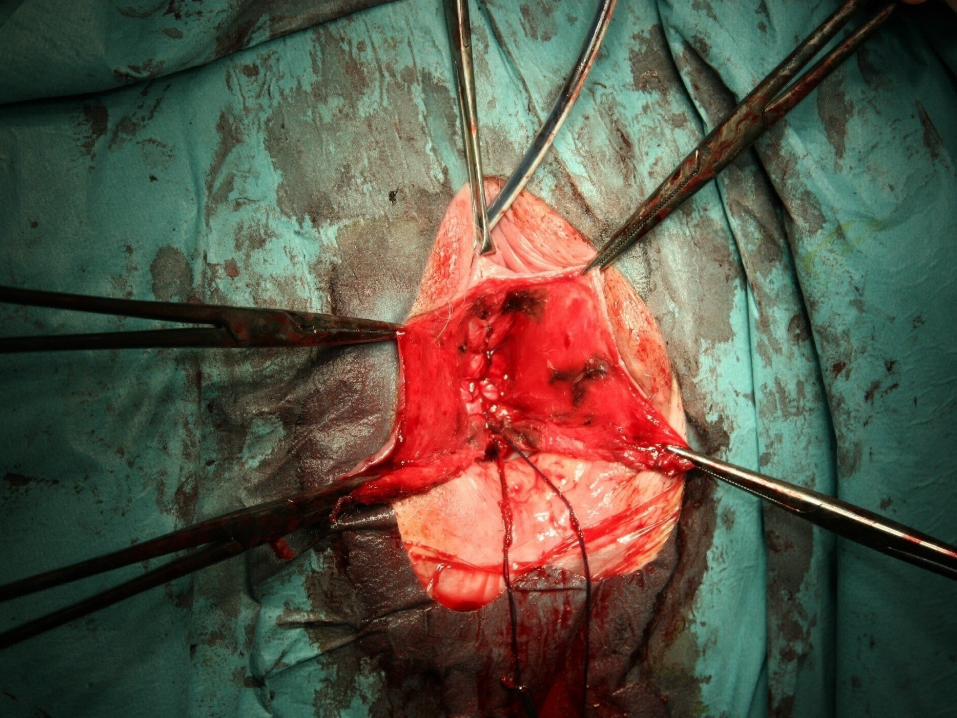
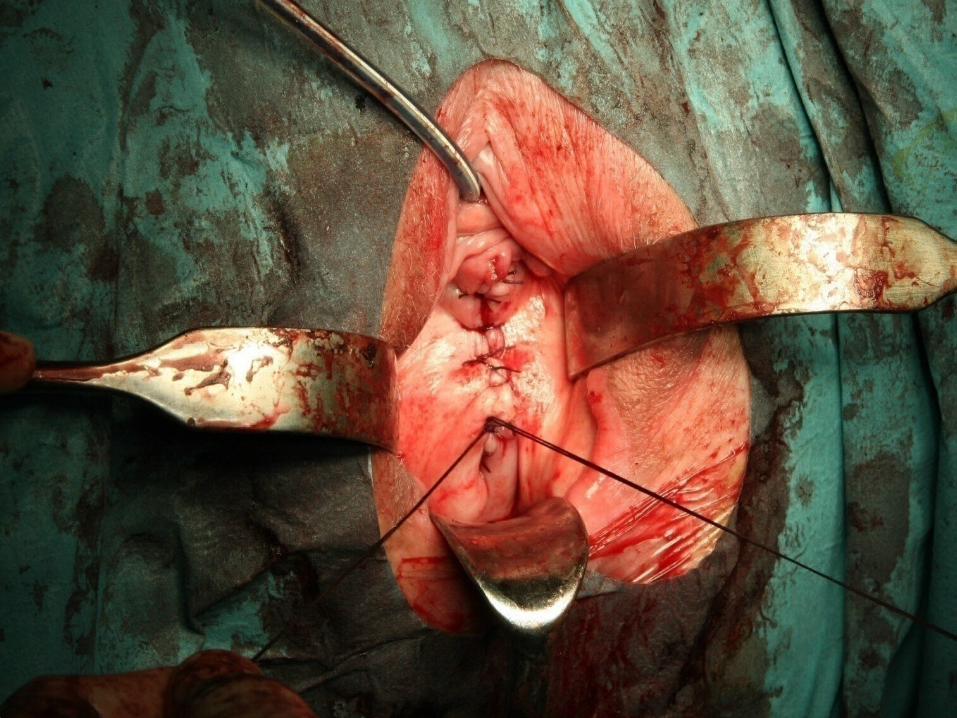
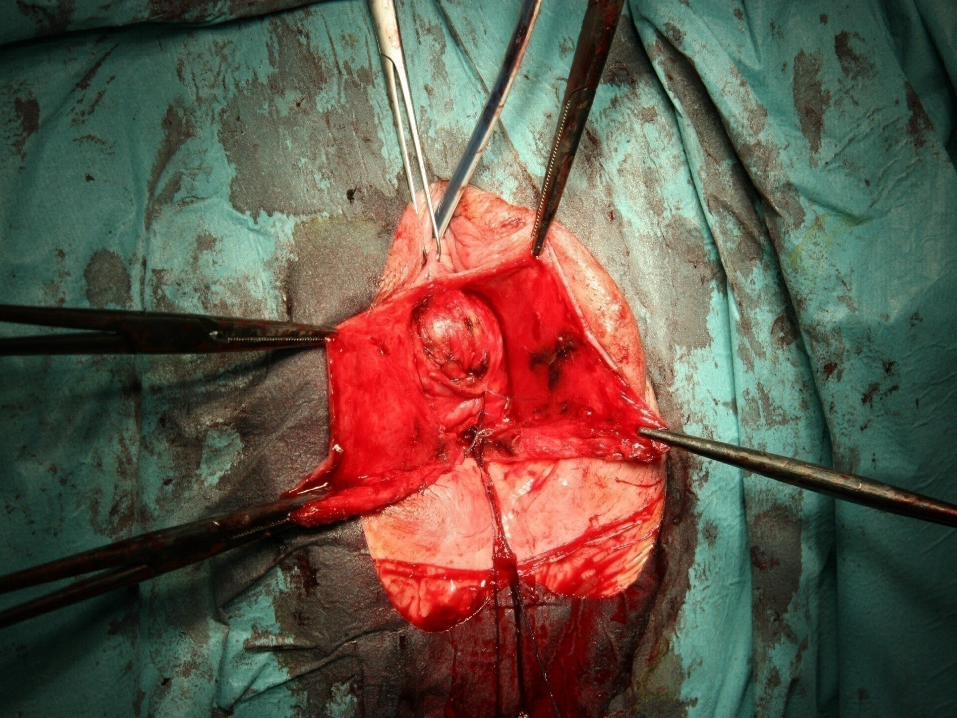
The anterior vaginal wall is closed with interrupted mattress sutures that include the underlying connective tissue.
M.D. Walters; M.M. Karram: Urogynecology and Reconstructive Pelvic Surgery ( 2007 )