
Prof. Sonia Bergamaschi Università degli Studi di Modena e Reggio Emilia
Ospedale di Circolo e Fondazione Macchi,Varese
9 Novembre 2011
Dott. Luigi Ruffo Codecasa, Responsabile Centro Regionale di Riferimento per la
Tubercolosi, Villa Marelli, A.O. Ospedale Niguarda Cà Granda, Milano
Dott. Giorgio Crosta, Dirigente Medico U.O. Pneumologia, A.O. Ospedale di
Circolo e Fondazione Macchi, Varese
Dott. Giovanni Gesu, Direttore Laboratorio Virologia e Microbiologia
A.O. Ospedale Niguarda Cà Granda, Milano
Dott.ssa Ester Mazzola, Dirigente Medico, Laboratorio di Virologia e Microbiologia
A.O. Ospedale Niguarda Cà Granda, Milano
Prof. Luigi Nespoli, Direttore Clinical Pediatrica - Ospedale F. del Ponte, Ospedale
di Circolo e Fondazione Macchi, Varese
Dott. Agostino Rossi, Dirigente Medico, Laboratorio di Microbiologia,
A.O. Ospedale di Circolo e Fondazione Macchi, Varese
Dott.ssa Franca Sambo, Responsabile Servizio di Medicina Preventiva delle
Comunità, ASL Varese
Prof. Antonio Toniolo, Direttore Laboratorio di Microbiologia, Ospedale di Circolo e
Fondazione Macchi, Varese
14.15 Saluto del Direttore Generale - Walter Bergamaschi
14.30 Introduzione scientifica - Antonio Toniolo
14.45 Diffusione della tubercolosi nella Provincia di Varese - Franca Sambo
15.15 La malattia tubercolare: aspetti clinici - Luigi Ruffo Codecasa
15.45 La malattia tubercolare nel paziente pediatrico - Luigi Nespoli
16.15 La malattia tubercolare: epidemiologia e diagnostica - Giorgio Crosta
16.45 Screening immunologico della infezione tubercolare - Giovanni Gesu
17.15 Discussione
17.25 Pausa
17.40 Diagnostica microbiologica e antibiogramma - Agostino Rossi
18.00 Aspetti molecolari: diagnostica, antibiogramma,epidemiologia –
Ester Mazzola
18.25 Discussione e conclusioni
18.45 Compilazione customer satisfaction
Laboratory diagnosis of TB infection
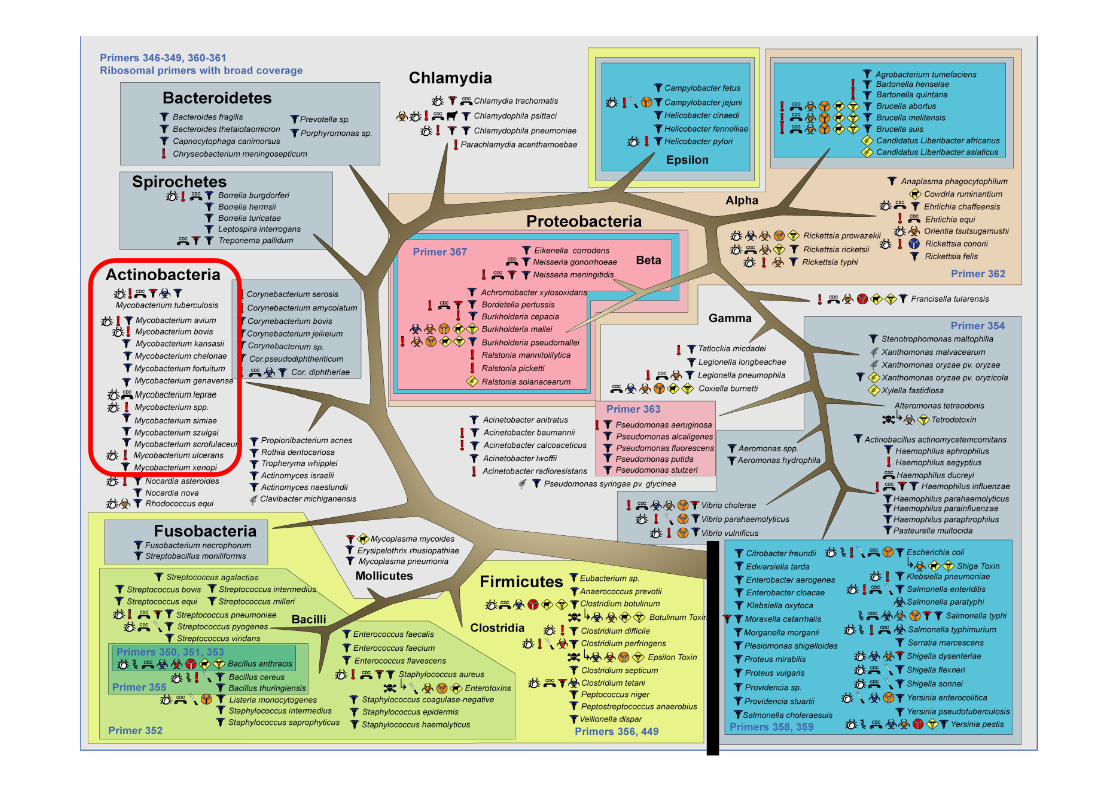

One third of the world’s population is infected with organisms of the Mycobacterium tuberculosis complex
Each year:
- Two million people die
- Eight million people are newly infected
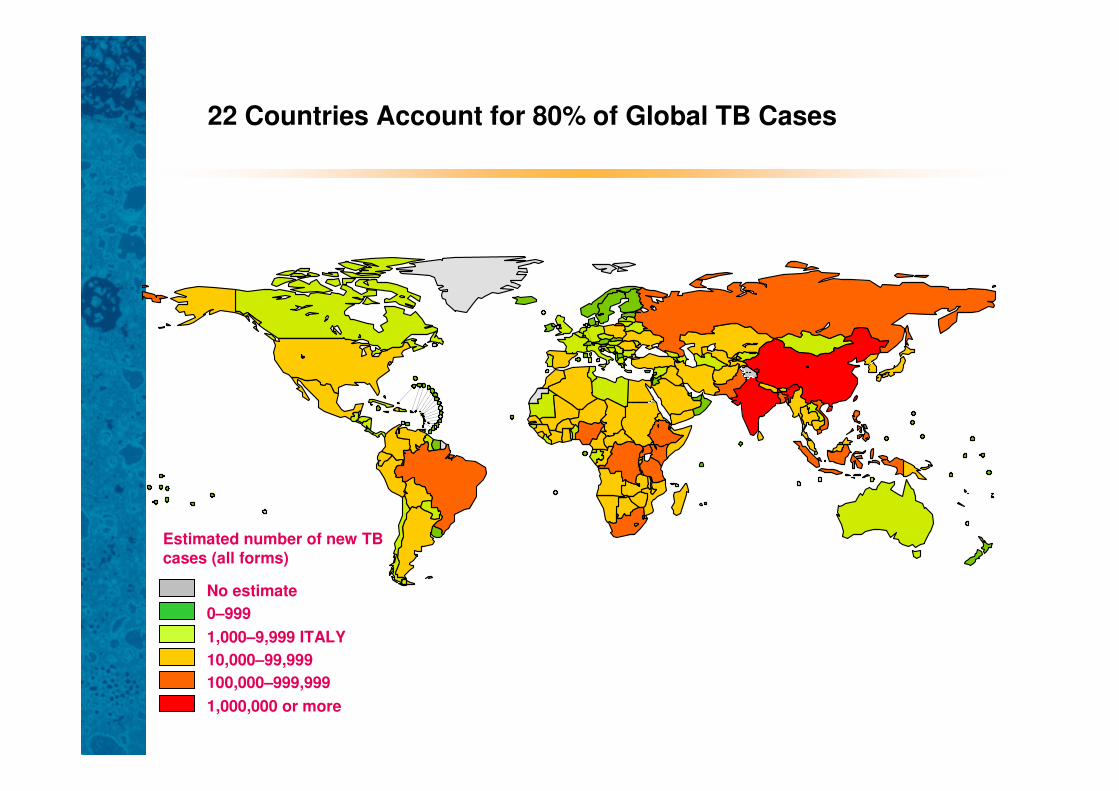
22 Countries Account for 80% of Global TB Cases
No estimate
0–999
10,000–99,999
100,000–999,999
1,000,000 or more
1,000–9,999 ITALY
Estimated number of new TB cases (all forms)
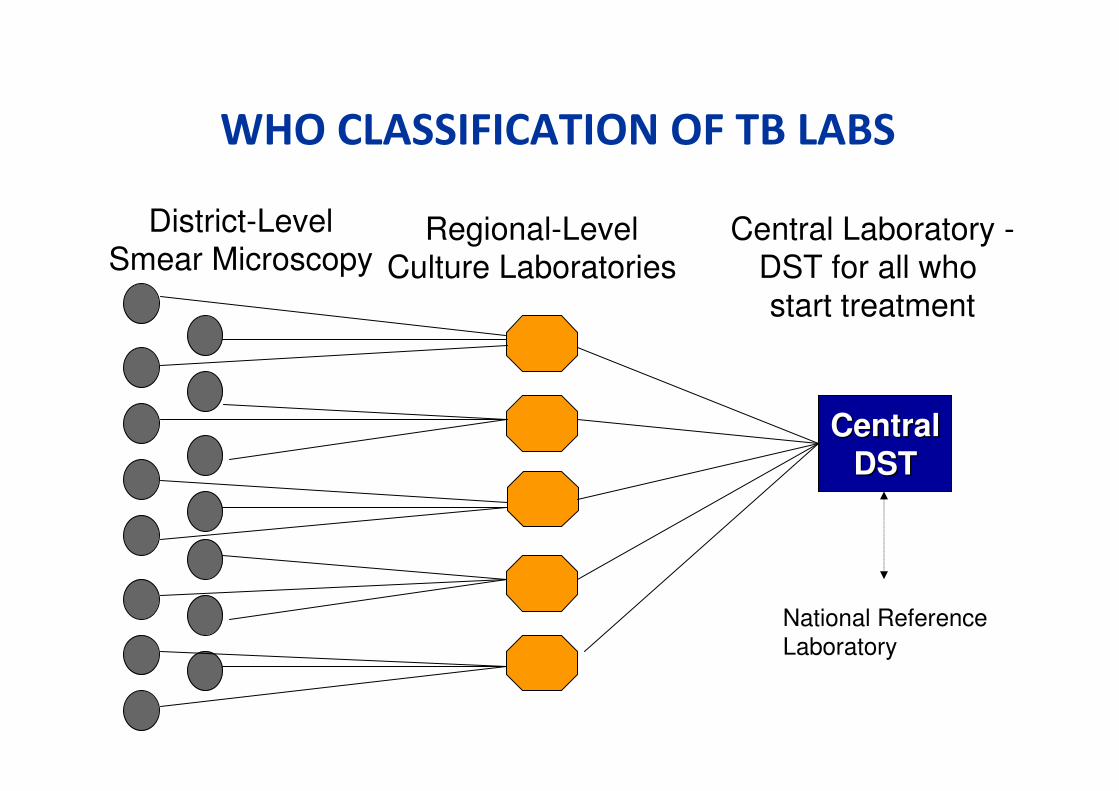
WHO CLASSIFICATION OF TB LABS
District-LevelSmear Microscopy
Regional-LevelCulture Laboratories
Central Laboratory -DST for all who
start treatment
CentralCentral
DSTDST
National Reference
Laboratory
Standards for Laboratory
Diagnosis of Tuberculosis
TB diagnosis and management depend
upon a reliable and prompt laboratory
service
Guidance and Standards
• National SOP
– How to do the tests
• NICE guidance
– How to manage the patient
• DH programme
– What service should be delivered
– 3 working groups
TB monitoring and laboratory services
working group
• Surveillance standards
• Standards for laboratory diagnosis
– Current best practice
– Simple and straightforward
– Not replicate or replace the National SOP

Standards to cover
• Samples
• Transfer to laboratory
• Immediate tests
– Microscopy
• Culture, isolation and
identification
• Laboratory facilities and
expertise
• Transport
• Susceptibility testing
• Molecular
fingerprinting/typing
• Notification
• PCR detection of Mtb
• Immunodiagnostic tests
• Histopathology
Samples
• Type of sample
– Sputum (resp. sample), CSF (spinal/para-spinal/intra-cerebral), gastric washings, lymph nodes (tissues), urine, faeces
• Number of samples
– 2 or 3 for sputum? Consecutive days.
– Early morning or any time?
– True LRT specimen
• Documentation
Transfer to laboratory
• Within 24h (or 1 working day, max 48h)
– Minimise overgrowth
– Maintain AFB character
• Potentially infected clinical sample
– Routine procedure
Immediate tests
• Microscopy
– Auramine fluorescent staining
– 6-day service (not on call)
– Perform microscopy and issue result within 24h (1 working
day) of receipt
– Telephone positive result to senior member of clinical
team
– Notify lead TB nurse, lead clinician, CCDC
• Accreditation; IQC programme; satisfactory EQA
performance; staff CPD/peer review
Culture, isolation and identification
• Automated liquid culture on all samples
– Set up within 24h of receipt (6 day service)
– Plus conventional solid culture
• Send all isolates to RCM on day found to be
positive
– Reach RCM within 24h
• Complete identification of most mycobacterial
isolates within 21 days
Identification and reporting
• NAAT (PCR, LCR) or hybridisation gene probe
for MTB complex
– On the day culture shows positive OR
– Within 24h of receipt at RCM
• Other probes and/or phenotypic tests
• Report on day of test to
– Senior member of clinical team
– Lead TB nurse, lead TB clinician, CCDC
Laboratory facilities and expertise
• Safety – Category 3 for culture
– HSE approved
– Contingency plan for accidental dispersal
– Continuity plan for closure
• Accredited
– IQC programme, satisfactory EQA
• Sufficient number – daily service, competence
• Named Consultant and BMS for advice
Transport
• Samples
– Potentially infected samples (routine)
• Positive cultures
– Category A but exemption to treat as B for clinical
and diagnostic purposes
• UN 3373 – marked Diagnostic or Clinical
• P650 packaging
• Do not send by Royal Mail
Susceptibility testing
• Complete within 30 days of initial receipt of clinical
sample for primary agents
– Isoniazid, rifampicin, pyrazinamide, ethambutol
• Takes 10-20 days by liquid proportion (automated) or resistance
ratio
• Molecular detection
– Rifampicin within 24h if MDRTB suspected
– Isoniazid under development
• Done at RCM with accreditation, IQC, EQA
Molecular fingerprinting/typing
• ALL ISOLATES
– 15-loci MIRU-VNTR
• Mycobacterial Interspersed Repetitive Units – Variable
Number Tandem Repeats
– Results to national database
– Other techniques as appropriate
• Done at RCM
Laboratory notification
• HPA
– Via CoSurv from laboratory that identifies a
positive culture
– Confirmation of positive from RCM within 24h (1
working day) of receipt
– RCM reports culture and susceptibility results to
MycobNET within 24h of report to clinician
PCR detection of MTB
• Not routine
• Available from RCM for particular samples
– High suspicion
– Definitive diagnosis deemed to be urgent
– Liaise in advance – Consultany Microbiologist to
RCM
Immunodiagnostic tests
• Interferon γ (QuantiFERON-TB Gold)
• Activated specific T-cells (T-SPOT.TB)
– Standard under development
• Which patients?
• How long should it take?
• Who provides it?
• What do the results mean and who interprets them?
Histopathology
• Report within 3 days of receipt
• Inform the Microbiology service
– Ensure same reporting as for positive microscopy
and culture results
• Send autopsy samples to Microbiology
without formalin!!
• [Role of PCR to be determined]
Implementation of standards
• Local responsibility
– What is done where?
• Microscopy; culture; identification
– What throughput is needed?
– Equipment – cost-effectiveness
– Personnel
• Maintain skills; CPD; peer review
• Named individuals for advice
• Back-up and cover
– IQC, EQA
Standards for Quality
Only do what you can do properly!


















