L’UTILIZZO DEI DAAs NEI CONSUMATORI DI SOSTANZE ......Iceland Dramatic reduction in community...
46
L’UTILIZZO DEI DAAs NEI CONSUMATORI DI SOSTANZE : EFFICACIA E SICUREZZA Giorgio Barbarini Già responsabile Unità Semplice “Diagnosi e terapia delle Malattie Infettive correlate alla Tossicodipendenza” DIPARTIMENTO MALATTIE INFETTIVE E TROPICALI
Transcript of L’UTILIZZO DEI DAAs NEI CONSUMATORI DI SOSTANZE ......Iceland Dramatic reduction in community...

L’UTILIZZO DEI DAAs NEI CONSUMATORI DI SOSTANZE : EFFICACIA E SICUREZZA Giorgio BarbariniGià responsabile Unità Semplice “Diagnosi e terapia delle Malattie Infettive correlate alla Tossicodipendenza”DIPARTIMENTO MALATTIE INFETTIVE E TROPICALI

DisclosuresI have received funding in the past 2 years for membership ofAdvisory Boards, for membership of speaker panels and forsupport for travel to conferences from the following companies:Abbvie Gilead Sciences

April 21, 1989

Seroprevalence of Hepatitis C: 150 to 200 Million WorldwideWestern Pacific60 MWestern Europe 5 MEastern Europe 10 MUnited States5MAmericas12-15 M Africa 30-40M Australia.2 M
5 M Southeast Asia30-35 M1. World Health Organization. Wkly Epidemiol Rec. 2000;75:17-28.2. Edlin B et al. AASLD; November 11-15; 2005 San Francisco, California. Oral Presentation #44. 3. Fontanet A. Annual Report of Emerging Diseases for Year 2005. Accessed 03/13/06 athttp://www.pasteur.fr/recherche/RAR/RAR2005/Epimal-en.html
Highest Prevalence: Egypt-4M(45% adults >40y)

Hepatitis C is the silent global epidemic of the 21st Century2015• ~72 million people with viraemic HCV
Blach S, et al. Lancet Gastroenterol Hepatol 2017;2:161–76; The Polaris Observatory. Hepatitis C. Available at: http://polarisobservatory.org/polaris/hepC.htm (accessed April 2017)0.0–<0.6%0.6–<0.8%0.8–<1.3%1.3–<2.9%2.9–<6.7%
Viraemic prevalence• ~72 million people with viraemic HCV• ~8.1 million people with HCV-related liver cirrhosis• ~261,000 people with HCV-related HCC• ~7000 HCV-related liver transplants• ~370,000 HCV liver-related deaths


The Lancet Global Health – 23 October, 2017• Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Louisa Degenhardt et al.• 179 of 206 countries or territories report IDU (31 new compared to 2008)• 15.6 million PWID worldwide– 17.8% HIV+ ( 2.77 million people )– 52.3% HCV+ (8.2 million people)– 9% Hepatitis B surface antigen (HBsAg)+– 83% mainly opioids– 33% mainly stimulants– 58% history of incarceration

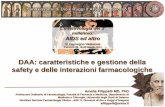
Proportion of HCV disease burden attributable to injecting drug use1990 2013Mean DALYs 1990 Population attributable factor Mean DALYs 2013 Population attributable factor
Degenhardt L, et al. Lancet Infect Dis 2016;16:1385–98© 2016 The Authors. Published by Elsevier Ltd.
Western Europe 376,000 44% 705,000 64%Eastern Europe 73,000 32% 605,000 68%Global 2,095,000 23% 7,046,000 38%

Lifecycle of the Hepatitis C VirusAssemblyAssemblyFusion andFusion and Viral RNAViral RNA
EntryGolgi complexGolgi complex
Differently from HIV and HBV:• HCV replication occurs only in cytoplasm• Viral genome is no archived into the 1. Asselah and Marcellin. Liver Int. 2011;31(suppl 1):68; 2. Scheel and Rice. Nat Med. 2013;19:837.
TranslationTranslationFusion anduncoatingFusion anduncoating
RNARNAViral RNAreplicationViral RNAreplicationNS5BNS5BNS5ANS5ANS3-NS4ANS3-NS4ANS4BNS4B ProcessingProcessing � Nonstructural proteins play a key role in the replication and assembly of new virions� Nonstructural proteins play a key role in the replication and assembly of new virionsReplicationcomplexReplicationcomplex EndoplasmicreticulumEndoplasmicreticulum• Viral genome is no archived into the genome of infected cells This makes HCV curable!!!!

Manns, von Hahn, Nat Rev Drug Discov 2013

TelaprevirBoceprevirSimeprevir SofosbuvirLedipasvirDaclatasvirVedroprevirAsunaprevirParitaprevir Ombitasvir DasabuvirAL-516Grazoprevir ElbasvirSamatasvirBeclabuvirUprifosbuvir
SovaprevirVelpatasvirOdalasvir ACH-3422 RadalbuvirGS- 9669Voxilaprevir TegobuvirVaniprevir
AL-335IDX- 459 MK- 8876Ravidasvir TMC-055/rPibrentasvirGlecaprevir
Updated to 2018 SeptemberRuzasvir

Peginterferon100 2013 Current98+All-OralTherapyDirect-Acting Antivirals
Nearly Everyone With HCV Can Now Be Treated Successfully• Very high SVR rates; therapies highly tolerable• All-oral therapy for almost every pt• Treatment generally just 12 wksPegIFN/RBV12 MosIFNIFN 6Mos 12Mos IFN/RBV12 Mos PegIFN12 Mos
20011998Standard Interferon Ribavirin Peginterferon1991
PegIFN/ RBV + DAAIFN/RBV6 Mos16 34 42 39 55 70+6020406080100
DAA +RBV ±PegIFN
90+2013All–Oral DAA±RBV
98+s2011


• Reduce necroinflammation• Stop fibrosis progression• Prevent cirrhosis & complications• Prevent hepatocellular carcinomaGoals obtained by achieving Sustained Virological Response (SVR) ≈ cure
• Prevent hepatocellular carcinoma• Reduce extra-hepatic manifestations • Increase survival• No AEAdapted by Schinazi & Asselah. From HCV to HBV cure. Liver Int. 2017;37 S1:73-80. Eradicate the virus (HCV clearance)

Global Call for HCV EliminationVision: “A world where viral hepatitis transmission is stopped and everyone has access to safe, affordable, and effective treatment and care”2020 target: 3 million HCV infections treatedFeasible by scaling up 6 key interventions to high coverage:Feasible by scaling up 6 key interventions to high coverage:Hepatitis B vaccination (including birth dose)Safe injection practices and safe bloodHarm reduction for injecting drug usersSafer sex (including condom promotion)Hepatitis B treatment Hepatitis C cure WHO. Towards the elimination of hepatitis B and C by 2030. Draft WHO Global Hepatitis Strategy, 2016-2021.2030 Targets90% Diagnosed80% Treated65% Reduced Mortality

Potential benefits of treatment in PWID : Societal benefits and Individual benefits• Target therapy to those at greatest risk of transmitting infection (younger injectors or newer initiates to injecting)Grebely J, Dore GJ. Antiviral Res 2014;104:62–72


PWID populations included in clinical trials withDAAsTreatment of HCV in PWIDLifetime PWIDOST OST and ongoingdrug useOngoingdrug use
Dore G, et al. Ann Intern Med 2016;165:625–34; Grebely J, et al. EASL 2017; Poster #FRI234 DAA: direct-acting antiviral agent; OST: opioid substitution therapy;PWID: people who inject drugs
drug use▪ PWID populations included in clinical trials with DAAs
− Patients on OST (Phase 2 AbbVie trial; ION-1, 2 and 3, ASTRAL-1, 2 and 3)− Patients on stable OST, ongoing injection use permitted (C-EDGE CO-STAR)− Patients on and not on OST with ongoing injection use (SIMPLIFY)Lalezari J, et al. J Hepatol 2015;63:364–9; Grebely J, et al. Clin Infect Dis 2016;63:1405–11; Grebely J, et al. Clin Infect Dis 2016;63:1479–81;





247 4 4 4
19 84 6468
1012Real-World Impact of SVR12 on PROs and Clinical Symptoms in OST Patients: DHC-R
Percen t No OST: BaselineWeek 24OST: BaselineWeek 24
Clinical Symptoms and Well-Being of OST Patients after SOF–Based Regimens: DHC-R ‡Clinical Symptoms30 24 19
26
2 2 2 2 2 0 3 02 1 1 0 1 1 0 0 0 1 0 0 00 2 0 2 2 2 0 0 02 0 0 0 2 0 0 0 0 0 0 0 0024
In OST patients, a number of clinical symptoms had decreased compared to baseline, including fatigue, abdominal pain, and depression/depressive moodChristensen S, INHSU 2017, Poster #92

Real-World Effectiveness of SOF-Based Regimens in Patients with OST� High SVR rates were achieved inOST and Non-OST patients� Alcohol consumption had noimpact on SVR12 rates
SVR rate by alcohol consumption (ITT)German Hepatitis C – Registry (DHC-R)
90 85 91 93 9284 88 82 88 88020406080100
SVR (%) 380421 4250
P=0.215 P=1.000 P=0.123 P=0.013 P=0.004
4553 1416 335368 2834 28343055 225255 32253488 267305
‡
27Günther, INHSU 2017, Poster #91 SOF-based therapies resulted in high SVR rates in OST and Non-OST patients.Consumption of alcohol and cannabis had no impact on SVR12SVR rate by cannabis consumption (ITT)
� SVR rates were comparable inpatients with and without OST� Cannabis consumption had noimpact on SVR12 rates
0 421 50Yes >40 g/day/men>30g/day women No Total≤40 g/day/men≤ 30g/day women53 16 368 34 3055 255 3488 30588 93 9283 88 88
020406080100
SVR (%) 8293 3441P=0.420 P=0.016 P=0.004
Yes 31423394 233264 33253488 267305No Total

TraP HepC: 2-Yr Results From HCV Treatment as Prevention in PWID in Iceland� Dramatic reduction in community viral load and HCV incidence between 2015-2017 at National Addiction Hospital– 53% reduction in new HCV infections– 53% reduction in new HCV infections– 72% reduction in HCV PCR positivity among PWID from 43% to 12%
Tyrffingsson T, et al. EASL 2018.Abstract PS-095. SVR12, % Treated Pts (N = 518) PCurrent IVD use (last 6 mos)Not currently using IVD 8795 .0033HomelessNot homeless 7494 .0005

Epatite C. Lorenzin: "Nuovi farmaci per tutti, nessuna selezione dei pazienti. Piano nazionale per eradicare la malattia : 80.000 trattati l’anno x 3 anni (1.500.000 E in bilancio).”

Criteri AIFA da marzo 2017Criterio 1: Pazienti con cirrosi in classe di Child A o B e/o con HCC con risposta completa a terapie resettive chirurgiche o loco-regionali non candidabili a trapianto epatico nei quali la malattia epatica sia determinante per la prognosi.Criterio 2: Epatite ricorrente HCV-RNA positiva del fegato trapiantato in paziente stabile clinicamente e con livelli ottimali di immunosoppressione.Criterio 3: Epatite cronica con gravi manifestazioni extra-epatiche HCV-correlate (sindrome crioglobulinemica con danno d'organo, sindromi linfoproliferative a cellule B, insufficienza renale). Criterio 4: Epatite cronica con fibrosi METAVIR F3 (o corrispondente Ishack).Criterio 5: In lista per trapianto di fegato con cirrosi MELD <25 e/o con HCC all'interno dei criteri di Milano con la possibilità di una attesa in lista di almeno 2 mesi.Criterio 6: Epatite cronica dopo trapianto di organo solido (non fegato) o di midollo in paziente stabileclinicamente e con livelli ottimali di immunosoppressione.clinicamente e con livelli ottimali di immunosoppressione.Criterio 7: Epatite cronica con fibrosi METAVIR F2 (o corrispondente Ishack) e/o comorbilità a rischio di progressione del danno epatico [coinfezione HBV, coinfezione HIV, malattie croniche di fegato non virali, diabete mellito in trattamento farmacologico, obesità (body mass index ≥30 kg/m2), emoglobinopatie e coagulopatie congenite].Criterio 8: Epatite cronica con fibrosi METAVIR F0-F1 (o corrispondente Ishack) e/o comorbilità a rischio di progressione del danno epatico [coinfezione HBV, coinfezione HIV, malattie croniche di fegato non virali, diabete mellito in trattamento farmacologico, obesità (body mass index ≥30 kg/m2), emoglobinopatie e coagulopatie congenite].Criterio 9: Operatori sanitari infetti.Criterio 10: Epatite cronica o cirrosi epatica in paziente con insufficienza renale cronica in trattamentoemodialitico.Criterio 11: Epatite cronica nel paziente in lista d'attesa per trapianto di organo solido (non fegato) o di midollo.

� Regimi terapeutici IFN-free approvati e rimborsati in Italia per la terapia anti HCVSofosbuvir + Velpatasvir (± RBV)
GTAll Glecaprevir + Pibrentasvir All
Sofosbuvir + Velpatasvir + VoxilaprevirSofosbuvir + Velpatasvir + VoxilaprevirGrazoprevir + Elbasvir (± RBV) 1All
1, 4
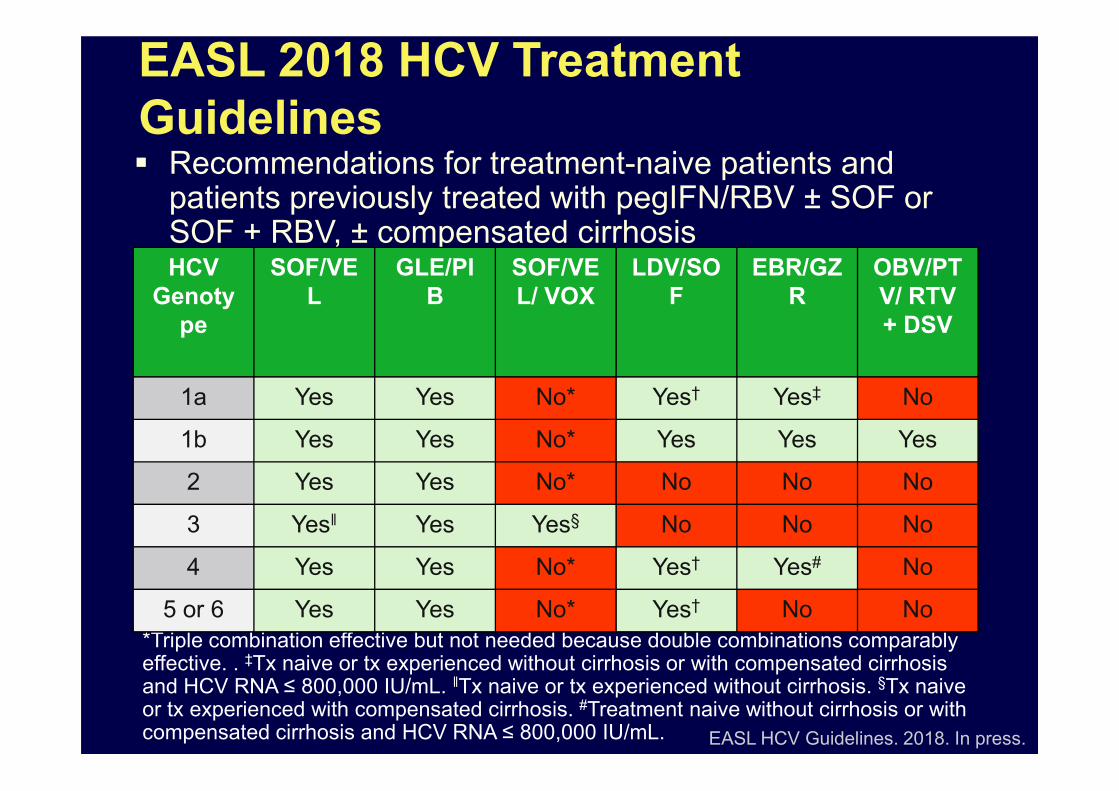
EASL 2018 HCV Treatment Guidelines� Recommendations for treatment-naive patients and patients previously treated with pegIFN/RBV ± SOF or SOF + RBV, ± compensated cirrhosisHCV Genotype SOF/VEL GLE/PIB SOF/VEL/ VOX LDV/SOF EBR/GZR OBV/PTV/ RTV + DSV1a Yes Yes No* Yes† Yes‡ No
EASL HCV Guidelines. 2018. In press.*Triple combination effective but not needed because double combinations comparably effective. . ‡Tx naive or tx experienced without cirrhosis or with compensated cirrhosis and HCV RNA ≤ 800,000 IU/mL. ǁTx naive or tx experienced without cirrhosis. §Tx naive or tx experienced with compensated cirrhosis. #Treatment naive without cirrhosis or with compensated cirrhosis and HCV RNA ≤ 800,000 IU/mL.
1a Yes Yes No* Yes† Yes‡ No1b Yes Yes No* Yes Yes Yes2 Yes Yes No* No No No3 Yesǁ Yes Yes§ No No No4 Yes Yes No* Yes† Yes# No5 or 6 Yes Yes No* Yes† No No


Lifetime PWIDCurrent PWIDMarginalized:- Socioeconomic- Prisoners- Indigenous
PWID Population DefinitionsPWIDPWID in OST

Past times PWIDPast PWIDPWID Population Definitions
PWIDPWID in OST

Snapshot of PWIDAlcohol consumptionMale SingleHomeless or living in temporary accommodation (shelters, prison)Poor quality of life Limited accessto healthcareUse of
Sris M, Rhodes T. Harm Reduction J 2013;10:7 Profile based on findings of two Canadian studies.PWID: people who inject drugs
Poorly educated (secondaryeducation or less) Use of multiple substances▪ Psychiatric disorders that are common among PWID include:
− Anxiety− Bipolar disorder− Depression− Post-traumatic stress− SchizophreniaBamvita JM, et al. Hepat Res Treat 2014;2014:631481;
HIV and/or HBV coinfection



TrattamentoPresenza criteri clinici
Valutazione: Genotipo, Fibroscan (cirrosi/no cirrosi), trattamenti farmacologici, comorbidità, consumo alcol e/o sostanze Presenza criteri comportamentali e motivazionali Scelta DAAHCV RNA + Harm Reduction Program:Training abilitàKit Riduzione del danno
Epatologi-Infettivologi + Ser.D.
infettivologico (SVR, comorbidità extraepatiche) di consumo e comorbidità psichiatriche/comportamentali Verifica apprendimento/utilizzo misure di riduzione del danno (con specifica scheda di valutazione) 3 e 6 mesi dall’EOTValutazione QOL a 3 e 6 mesi dall’EOT
Inizio trattamentoScelta DAAMonitoraggio Compliance (entrambi gli specialisti)Outcome Controllo virologico a 3 e 6 mesi dall’EOT Follow upa 3 e 6 mesi
Termine del Trattamento Harm Reduction Program:Questionario verifica HR

GESTIONE MULTIDISCIPLINAREINTEGRATA (non solo collaborativa)LA DECISIONE DI EFFETTUARE IL TRATTAMENTO VIENE ASSUNTA CONGIUNTAMENTE DAL CENTRO SPECIALISTICO E DAL SERD.CENTRO SPECIALISTICO E DAL SERD.IL PAZIENTE VIENE TRATTATO NEL SERD, DAGLI OPERATORI DEL SERD DI CONCERTO CON IL CONSULENTE SERD (DOT)IL MONITORAGGIO SUCCESSIVO AL TERMINE DELLA TERAPIA VIENE ESEGUITO PRESSO IL SERD


Reinfection following successful HCV DAA therapy among people with recent injecting drug use: the SIMPLIFY and D3FEAT studies7th International Symposium on Hepatitis Care in Substance UsersCascais, Portugal19 - 21 September 2018Evan Cunningham, Grebely J, Dalgard O, Hajarizadeh B, Conway B, Powis J, Bruneau J, Feld JJ, Read P, Cooper C, Amin J, Bruggmann P, Lacombe K, Stedman C, Hellard ME, Marks P, Dunlop A, Quiene S, Moriggia A, Applegate TL, Litwin AH, Matthews GV, and Dore GJ on behalf of the SIMPLIFY and D3FEAT Study Groups

“Reinfections are simply an indicator that we are treating the right population. People who become reinfected are not only at risk of HCV infection but likely HCV transmission as well and so treatment among this population is crucial in order to reduce the incidence of new HCV cases. It’s population is crucial in order to reduce the incidence of new HCV cases. It’s important that reinfection cases are seen in this framework and patients areA. H . Litwin given access to timely retreatment without any stigma or discrimination.”

Medications don’t work in patients who don’t take themtake them- C. Everett Koop, MD

The good physician treats the disease ;the best physician treats the patients with the disease William Osler

ORA…….LAVORIAMOINSIEME !!!!!