La prevenzione alimentare dell’osteoporosi - DIETA live convegno OPBG_Vescini.pdf · La...
38
La prevenzione alimentare dell’osteoporosi Fabio Vescini
Transcript of La prevenzione alimentare dell’osteoporosi - DIETA live convegno OPBG_Vescini.pdf · La...

La prevenzione alimentare dell’osteoporosi
Fabio Vescini

NORMALE OSTEOPOROSI

Nutrienti fondamentali per il mantenimento dell’omeostasi ossea
• Calcio
• Vitamina D• Fosforo
• Magnesio
• Sodio
• Potassio
• Fluoro
• Proteine (animali/vegetali)
• Vitamina K

Nutrienti fondamentali per il mantenimento dell’omeostasi ossea
• Calcio• Vitamina D
• Fosforo
• Magnesio
• Sodio
• Potassio
• Fluoro
• Proteine (animali/vegetali)
• Vitamina K

Distribuzione del calcio nell’organismo
Intracellulare 9,2 g
Fluidi extracellulari 1 g (0.1%)
Scheletro 1-2 Kg (99%)
Solubile 0.2 mg Insolubile 9 g
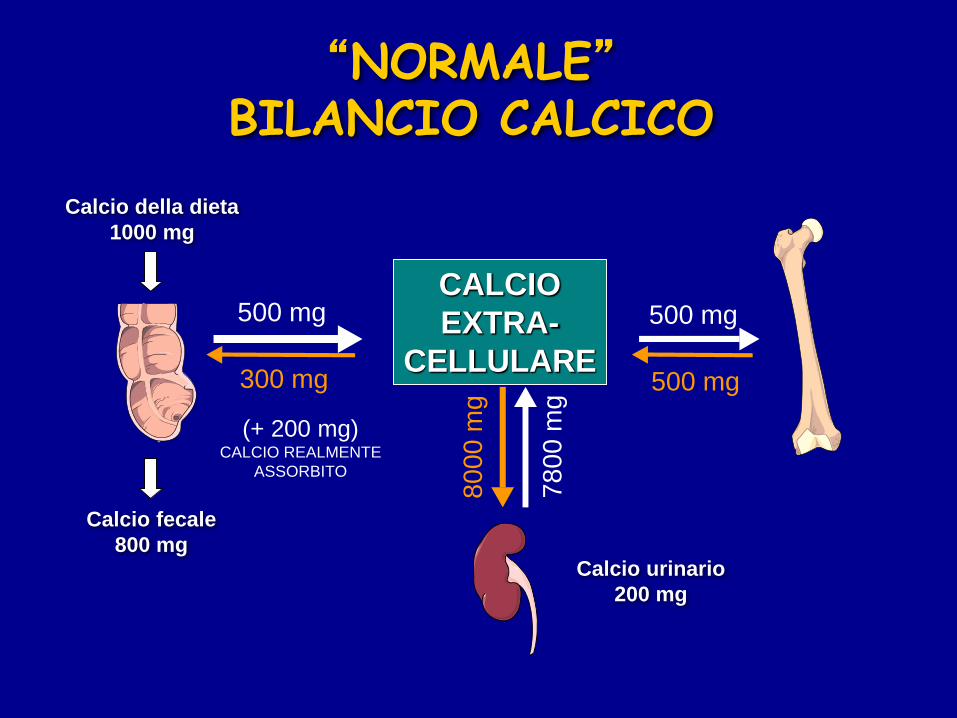
500 mg
500 mg
500 mg
300 mg
(+ 200 mg)CALCIO REALMENTE
ASSORBITO8
00
0 m
g
78
00
mg
Calcio urinario
200 mg
Calcio fecale
800 mg
Calcio della dieta
1000 mg
CALCIO
EXTRA-
CELLULARE
“NORMALE”BILANCIO CALCICO

0 20 40 60 80
Età (anni)
Femmine
Maschi
Orwoll ES. et al. Endocr Rev. 1995
PMO
Andamento fisiologico della massa ossea
60-70 % GENETICA
30-40 % AMBIENTE0,5 - 1 % per anno
10 30 50 70 900

PMO
Importanza del picco di massa ossea (PMO)
10 30 50 70 900

Massa ossea e apporto di calcio
0 10 20 30 40 50 60 70 80 Anni
Mass
a o
ssea
(uni
tà a
rbit
rari
e)
Ereditarietà
Assunzione di calcio
Errori strutturali
Adeguato
Inadeguato
PMO

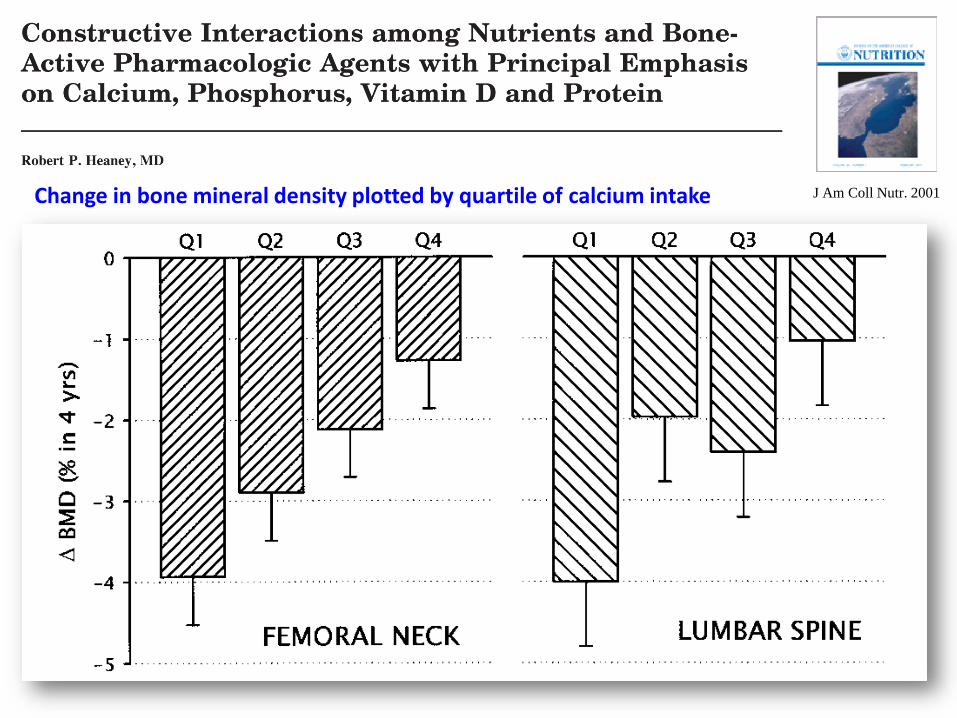
J Am Coll Nutr. 2001Change in bone mineral density plotted by quartile of calcium intake

J Am Coll Nutr. 2001Total body calcium measured by dual energy X-ray absorptiometry over a one-year period in 364 teenage girls progressing from pubertal stage 2 to 3
A mean increase of 108 g requires a daily positive Ca balance of about 300 mg, demonstrating the
importance of adequate calcium during growth
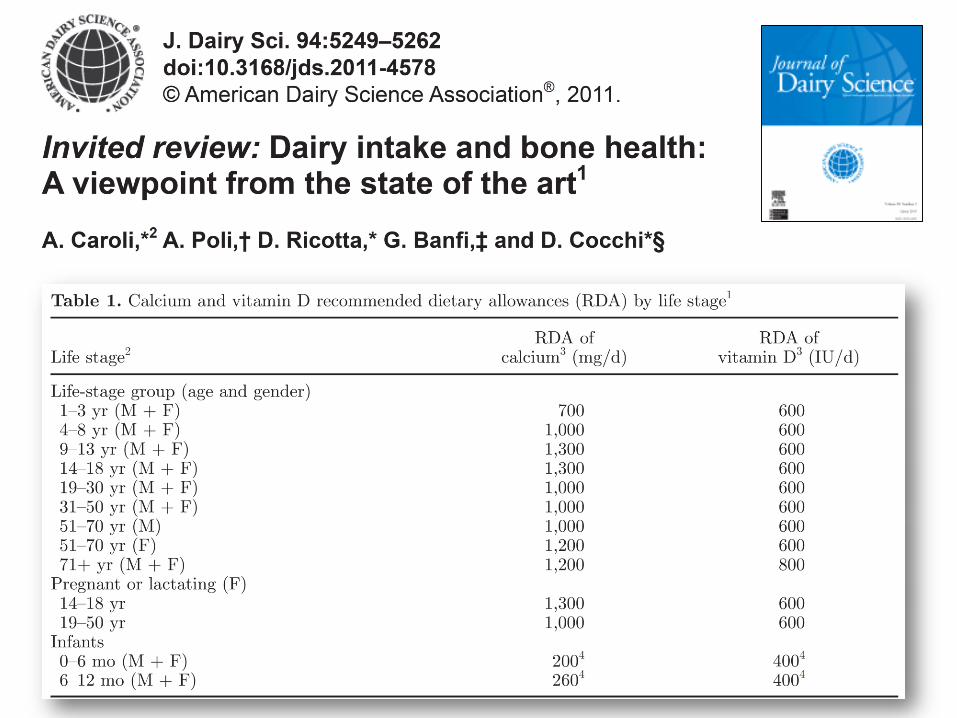
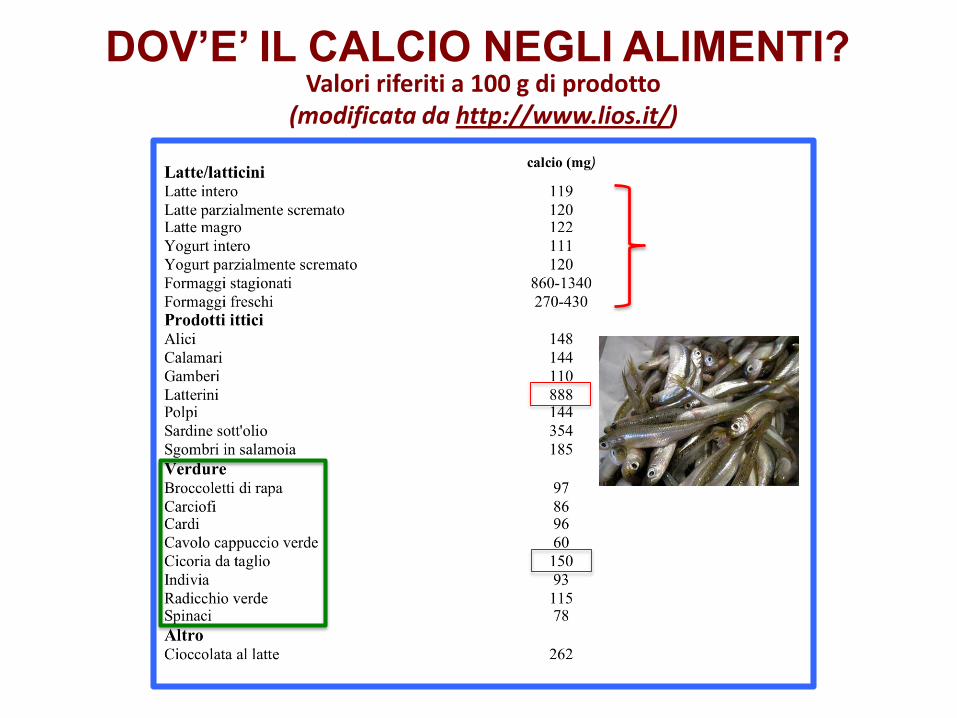
Valori riferiti a 100 g di prodotto(modificata da http://www.lios.it/)
DOV’E’ IL CALCIO NEGLI ALIMENTI?

Calcio (mg/l) sodio (mg/l) Bicarbonato (mg/l)
Levissima 19,5 1,8 56,8
Panna 30,2 6,5 100
Rocchetta 59 4,4 185
Vera 36,1 2 153
Cerelia 119 5,6 416
Ferrarelle 365 49 1342
Lete 321 4,9 1006
Sangemini 328 19 1042
Il calcio contenuto nell’acqua viene assorbito dall’intestino umano in misura sovrapponibile al calcio del latte
Acque con elevato HCO3- sono più efficaci nel ridurre il PTH e i BTMs

Povere ossa!Guardi signora
che il calcio le
può provocare
una calcolosi
renale
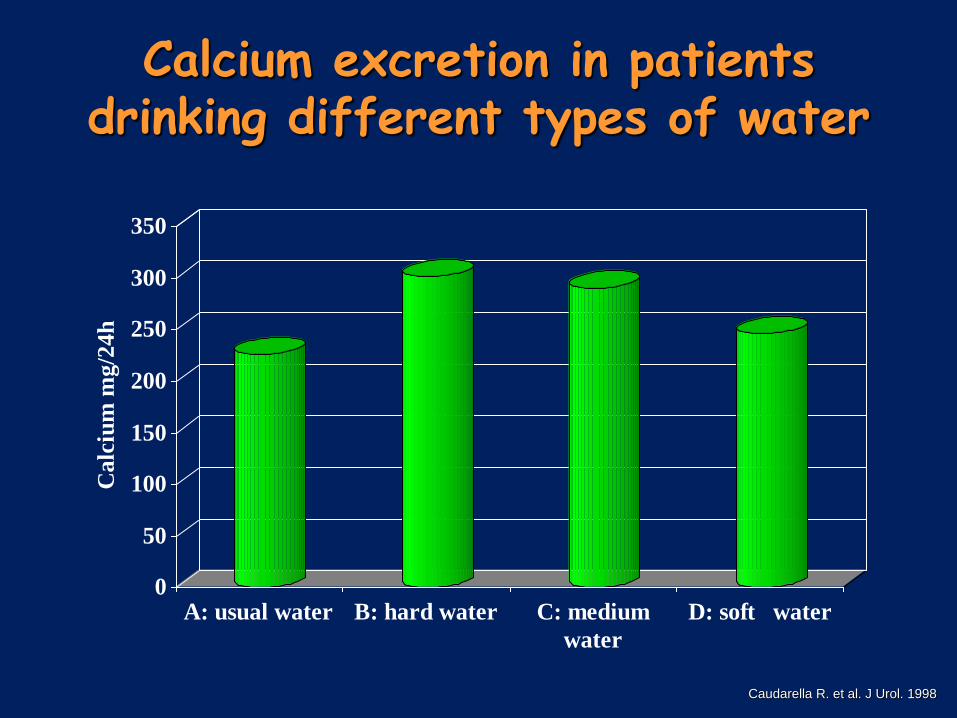
Calcium excretion in patients drinking different types of water
0
50
100
150
200
250
300
350
Ca
lciu
m m
g/2
4h
A: usual water B: hard water C: medium
water
D: soft water
Caudarella R. et al. J Urol. 1998

AP (CaOx) index in patients drinking different types of water
0
0,2
0,4
0,6
0,8
1
1,2
AP (CaOx) Index
Basal
High Ca
Medium Ca
Low Ca
Caudarella R. et al. J Urol. 1998

0
0,2
0,4
0,6
0,8
1
1,2
1,4
Baseline 1st Period 2nd Period
Healthy Subjects Stone Formers
*
*
Effects of 20 days of controlled diet (800 mg/day)
+ 20 days of diet and supplemental calcium (1000 mg CaCo3)
on urinary supersaturation for CaOx
Vescini F. et al. et al. 9° ESU 2001


Nutrienti fondamentali per il mantenimento dell’omeostasi ossea
• Calcio
• Vitamina D• Fosforo
• Magnesio
• Sodio
• Potassio
• Fluoro
• Proteine (animali/vegetali)
• Vitamina K

Percentuale di donne anziane con deficit subclinico di vitamina D in differenti paesi europei (inverno)
0
10
20
30
40
50
60
70
80
90
100
Gre
cia
Port
ogallo
Italia
Spag
na
Franci
a
Ungher
ia
Svi
zzer
a
Bel
gio
Dan
imar
ca
Norv
egia
%
Modificato da: Scharla SH. Ostepor Int. 1998
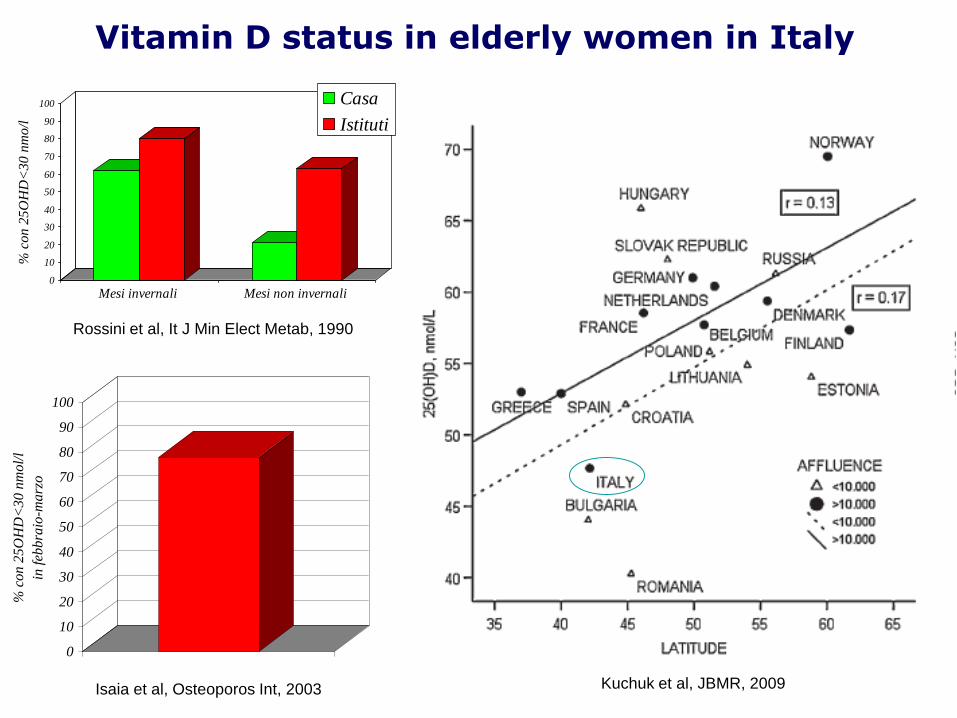
Kuchuk et al, JBMR, 2009
0
10
20
30
40
50
60
70
80
90
100
% c
on 2
5O
HD
<30 n
mo/l
Mesi invernali Mesi non invernali
Casa
Istituti
0
10
20
30
40
50
60
70
80
90
100
% c
on
25
OH
D<
30
nm
ol/
l
in f
ebb
raio
-ma
rzo
Rossini et al, It J Min Elect Metab, 1990
Isaia et al, Osteoporos Int, 2003
Vitamin D status in elderly women in Italy

Worldwide vitamin D statusNatasja M. van Schoor & Paul Lips.
Best Practice & Research Clinical Endocrinology & Metabolism 25 (2011) 671–680
Mean serum 25(OH)D levels in Europe

Prima descrizione del rachitismo
XVII secolo: prime descrizioni di bambini affetti da una malattia
che provoca ritardo della crescita, allargamento delle epifisi
delle ossa lunghe, deformità degli arti inferiori, scoliosi, gabbia
toracica “bitorzoluta”, debolezza e riduzione del tono muscolare
Holick, M. F. J. Clin. Invest. 2006;116:2062-2072

Gamgee, K.M.L. 1927. The artificial light treatment of children in rickets, anaemia & malnutrition. P.B. Hoeber Inc. New York, New York, USA. 172 pp
UV radiation therapy for rickets
Photograph from the 1920s of a child with rickets being exposed to UV
radiation 1 hour UV radiation 2 times a week for 8 weeks
Radiographs demonstrating florid rickets of the hand and wrist (left) and the same
wrist and hand taken after treatment. Note mineralization of the carpal bones
and epiphyseal plates
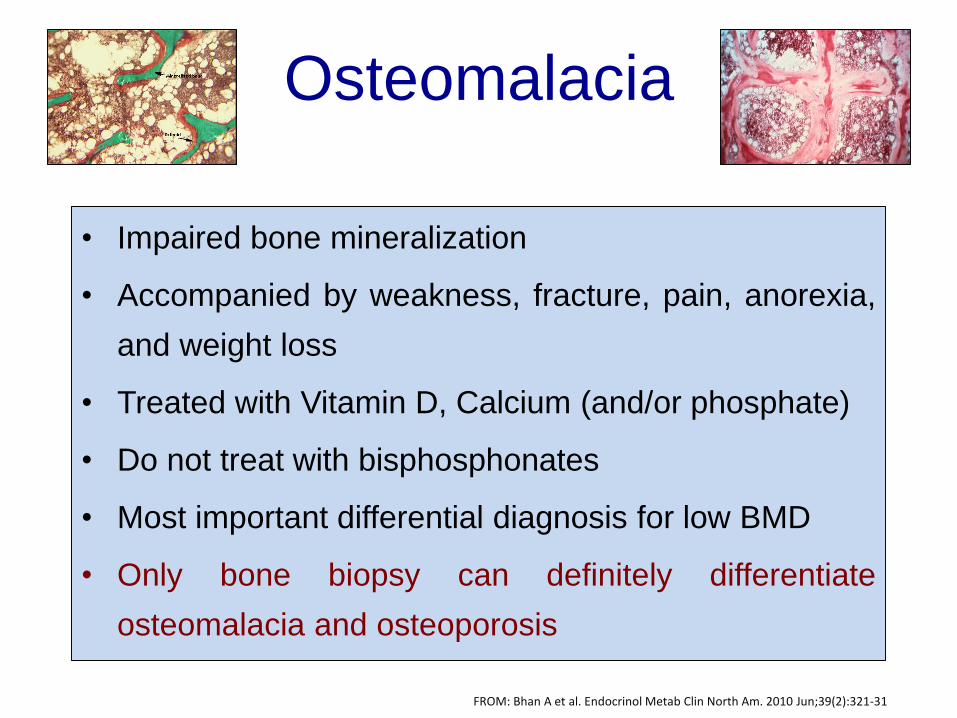
Osteomalacia
• Impaired bone mineralization
• Accompanied by weakness, fracture, pain, anorexia,
and weight loss
• Treated with Vitamin D, Calcium (and/or phosphate)
• Do not treat with bisphosphonates
• Most important differential diagnosis for low BMD
• Only bone biopsy can definitely differentiate
osteomalacia and osteoporosis
FROM: Bhan A et al. Endocrinol Metab Clin North Am. 2010 Jun;39(2):321-31
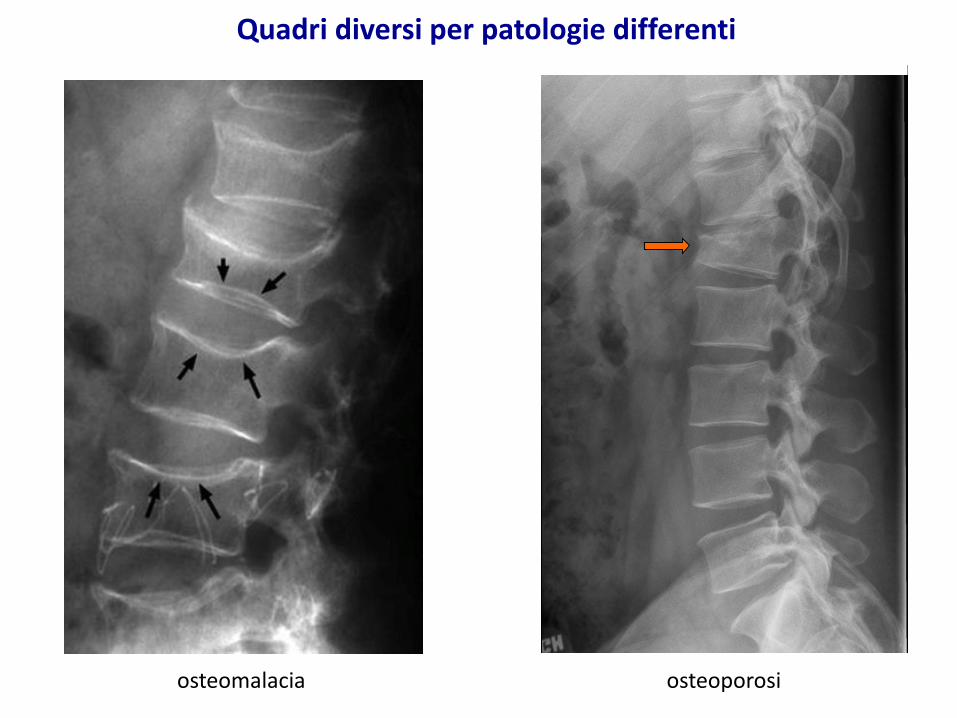
Quadri diversi per patologie differenti
osteomalacia osteoporosi

LA VITAMINA D NEGLI ALIMENTI
Alimento U.I. Vit D/100g
Salmone fresco
Olio di fegato di merluzzo
Uova
Latte vaccino
Latte umano
Formaggio Emmenthal
Burro
650
8500
200
0.5-4
0.4-9.7
100
40
L’80% del fabbisogno di vitamina D è garantito dalla irradiazione solare. La Vitamina D e’ contenuta soprattutto nei grassi animali

HO
7-DEIDROCOLESTEROLO
CUTEHO
HO
OH
HO
OH
OH
COLECALCIFEROLO
25-IDROSSI-COLECALCIFEROLO1,25-DI-IDROSSI-COLECALCIFEROLO
RAGGI ULTRAVIOLETTI (UVB)
FEGATO
25-IDROSSILASI
1-a-IDROSSILASI
RENE

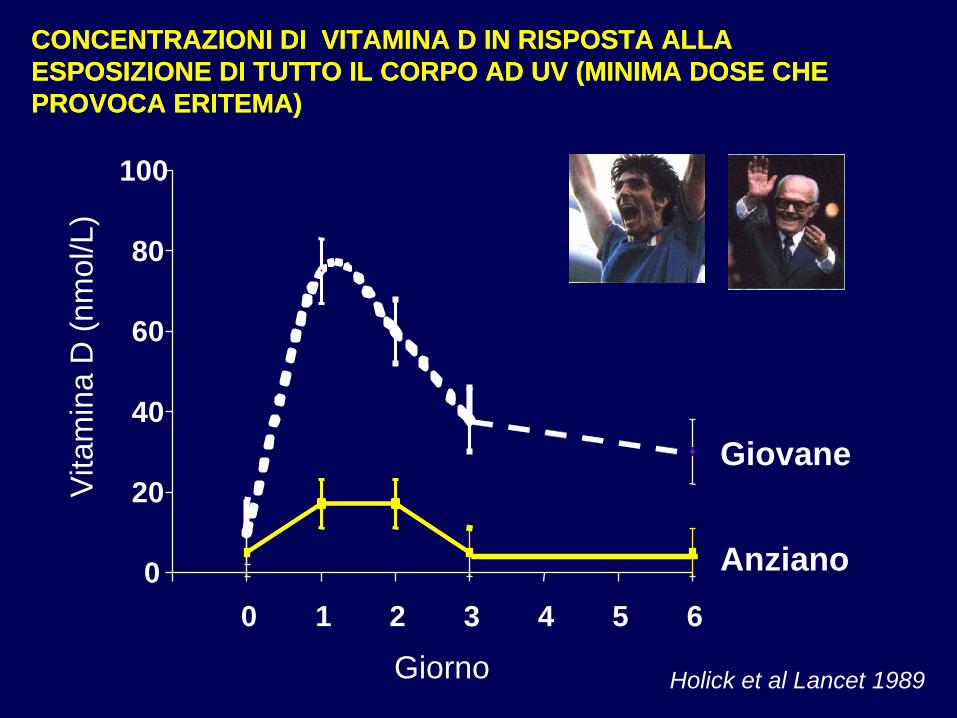
0
20
40
60
80
100
0 1 2 3 4 5 6
Giovane
Vitam
ina D
(nm
ol/L)
Giorno Holick et al Lancet 1989
CONCENTRAZIONI DI VITAMINA D IN RISPOSTA ALLA
ESPOSIZIONE DI TUTTO IL CORPO AD UV (MINIMA DOSE CHE
PROVOCA ERITEMA)
CONCENTRAZIONI DI VITAMINA D IN RISPOSTA ALLA
ESPOSIZIONE DI TUTTO IL CORPO AD UV (MINIMA DOSE CHE
PROVOCA ERITEMA)
0
20
40
60
80
100
0 1 2 3 4 5 6
Giovane
Anziano
Vitam
ina D
(nm
ol/L)
Giorno Holick et al Lancet 1989
CONCENTRAZIONI DI VITAMINA D IN RISPOSTA ALLA
ESPOSIZIONE DI TUTTO IL CORPO AD UV (MINIMA DOSE CHE
PROVOCA ERITEMA)
CONCENTRAZIONI DI VITAMINA D IN RISPOSTA ALLA
ESPOSIZIONE DI TUTTO IL CORPO AD UV (MINIMA DOSE CHE
PROVOCA ERITEMA)

Bischoff-Ferrari HA et al. Am J Clin Nutr. 2006;84(1):18-28
Optimal 25(OH)D3 serum concentration measured by multiple health
outcomes (BMD, fractures, colon cancer, muscular weakness,dental loss)

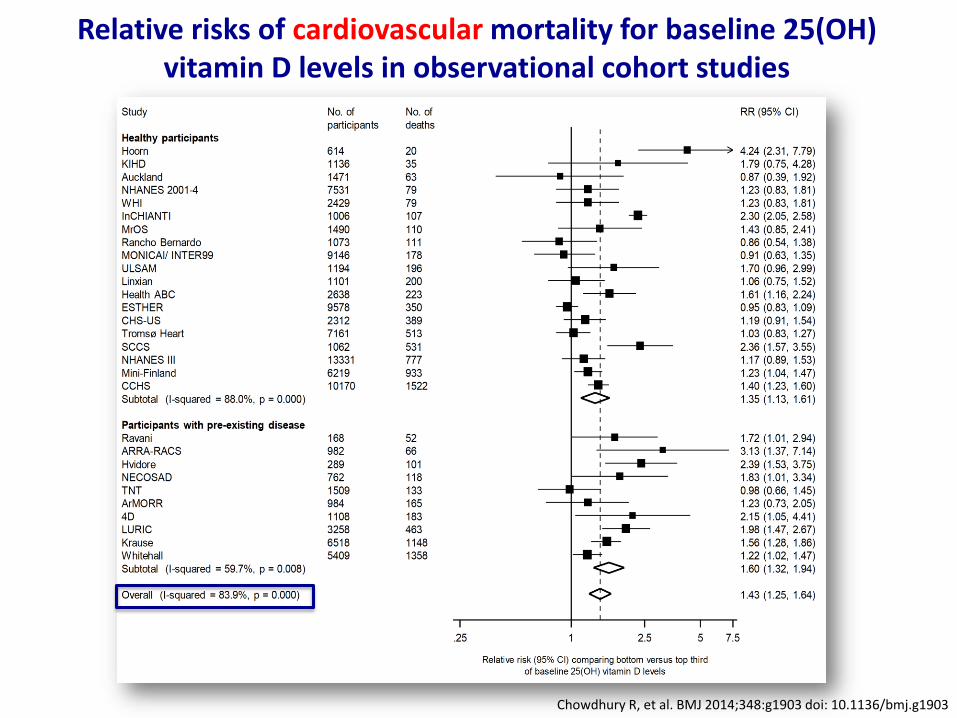
Chowdhury R, et al. BMJ 2014;348:g1903 doi: 10.1136/bmj.g1903
Relative risks of cancer mortality for baseline 25(OH) vitamin D levels in observational cohort studies
Chowdhury R, et al. BMJ 2014;348:g1903 doi: 10.1136/bmj.g1903
Relative risks of cardiovascular mortality for baseline 25(OH) vitamin D levels in observational cohort studies

Chowdhury R, et al. BMJ 2014;348:g1903 doi: 10.1136/bmj.g1903
Relative risks of nonvascular, noncancer mortality for baseline 25(OH) vitamin D levels in observational cohort studies

Chowdhury R, et al. BMJ 2014;348:g1903 doi: 10.1136/bmj.g1903
Relative risks of all cause mortality in vitamin D3 supplementation trials

Nutrizione corretta


















