![[1616-Trasfusioni Sicure Integrate][Fondazione IRCCS Istituto Nazionale dei Tumori]](https://static.fdocumenti.com/doc/165x107/558e997b1a28aba3708b46e9/1616-trasfusioni-sicure-integratefondazione-irccs-istituto-nazionale-dei-tumori.jpg)
[1616-Trasfusioni Sicure Integrate][Fondazione IRCCS Istituto Nazionale dei Tumori]
Carlo Garufi Oncologia Medica AIstituto Nazionale Tumori Regina ElenaRoma
Esempi di Ricerca Traslazionale:POCHER 1 e POCHER 2
Come nasce e cosa è POCHER
• Si tratta dell’evoluzione di due linee di ricerca integrate
A) la cronobiologia e la cronoterapia
B) il trattamento delle metastasi epatiche da CRC
• Come inserire tutto ciò nel contesto delle conoscenze attuali e del trattamento del CRC
Come nasce e cosa è POCHER
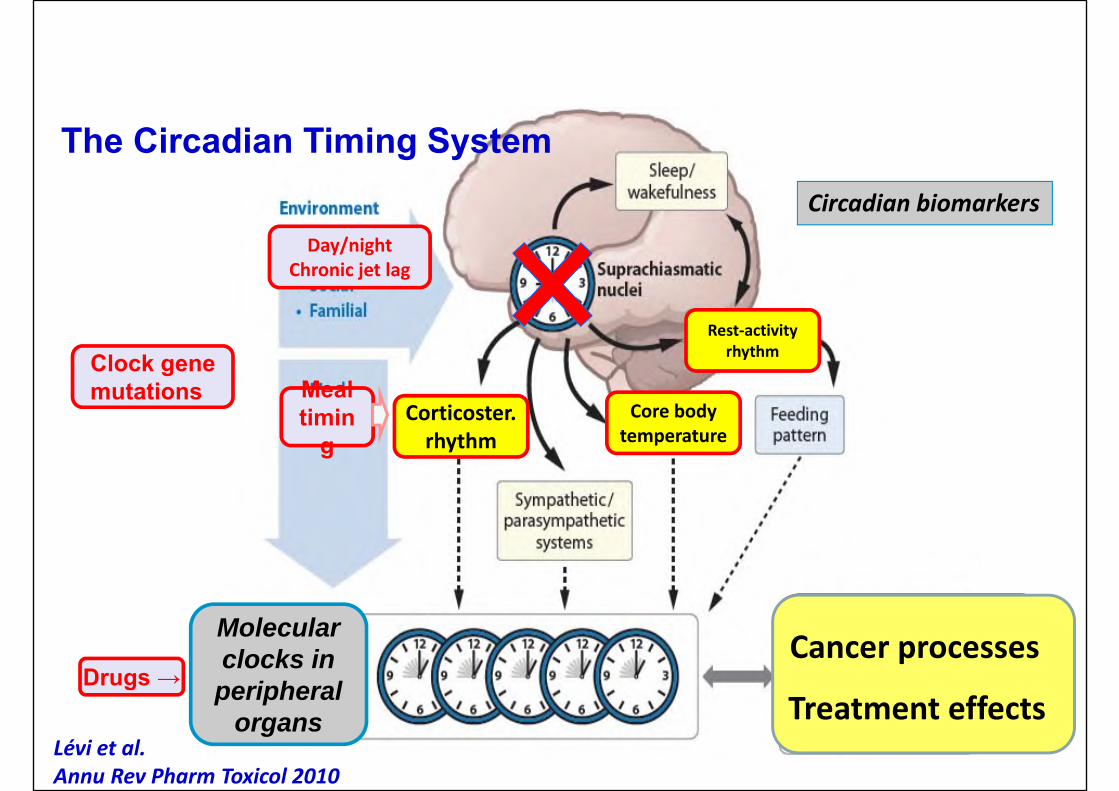
Rest‐activity rhythm
Molecularclocks in
peripheralorgans
• Cell cycle & DNA repair• Metabolism• Drug detoxification• Angiogenesis
Circadian biomarkers
Lévi et al.Annu Rev Pharm Toxicol 2010
Core bodytemperature
Corticoster. rhythm
Day/nightChronic jet lag
Cancer processes
Treatment effects
Mealtimin
g
Clock genemutations
The Circadian Timing System
Drugs →
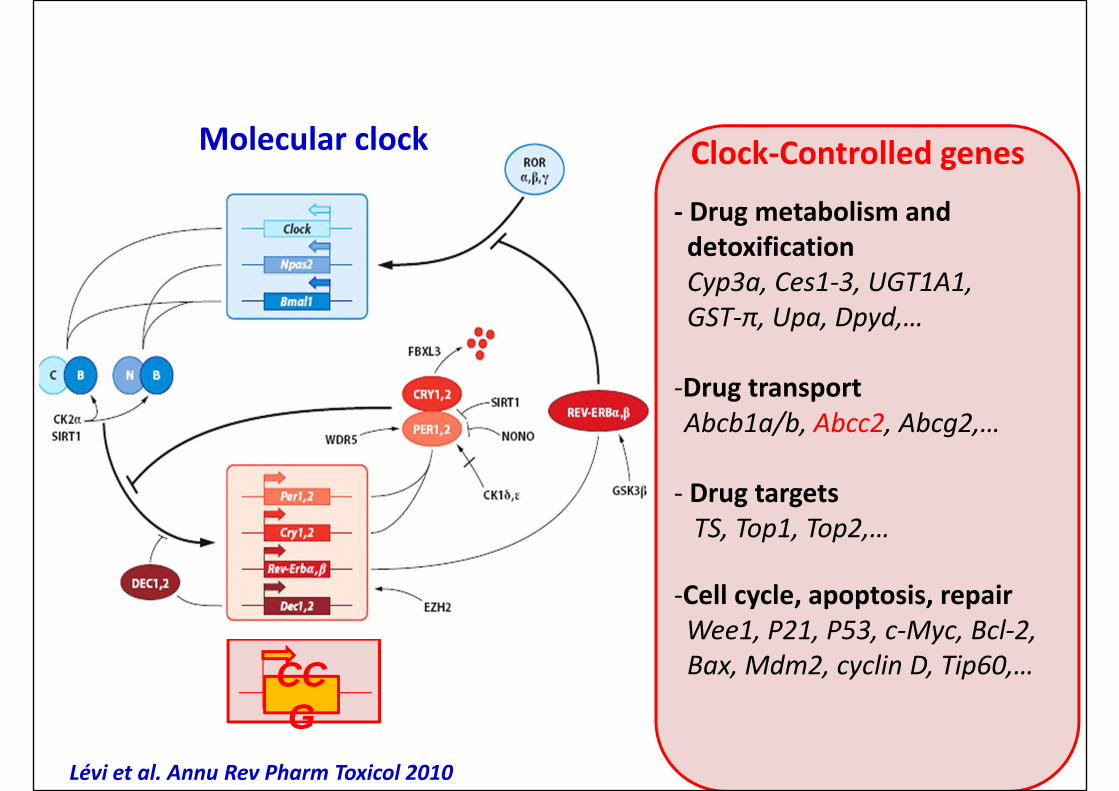
Lévi et al. Annu Rev Pharm Toxicol 2010
Molecular clock
Bjarnason et al. Am. J Pathology 2001
hBmal1
0.2
0.4
0.6
0.8
1
0.008 12 16 20 00 04
hPer1 hBmal1
Clock gene transcriptionrhythms in human oral mucosa
Time (clock hours)CCG
Clock‐Controlled genes
‐ Drug metabolism anddetoxificationCyp3a, Ces1‐3, UGT1A1, GST‐π, Upa, Dpyd,…
‐Drug transportAbcb1a/b, Abcc2, Abcg2,…
‐ Drug targetsTS, Top1, Top2,…
‐Cell cycle, apoptosis, repairWee1, P21, P53, c‐Myc, Bcl‐2,Bax, Mdm2, cyclin D, Tip60,…
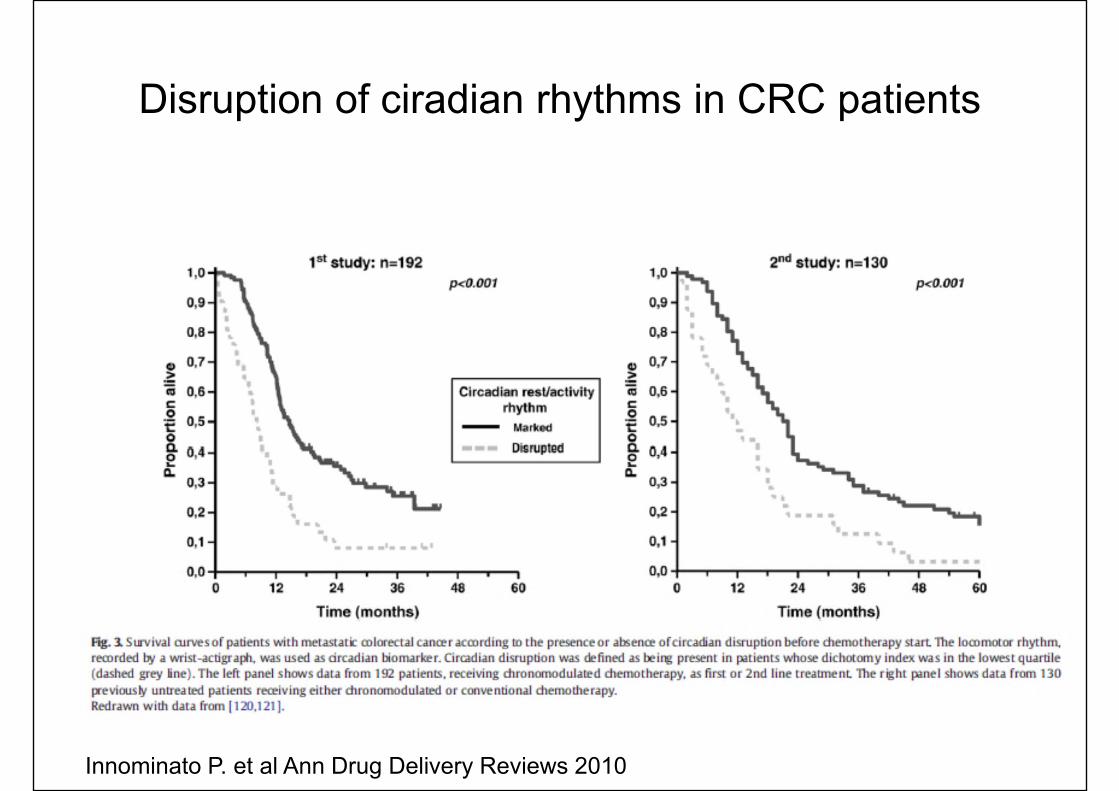
Disruption of ciradian rhythms in CRC patients
Innominato P. et al Ann Drug Delivery Reviews 2010
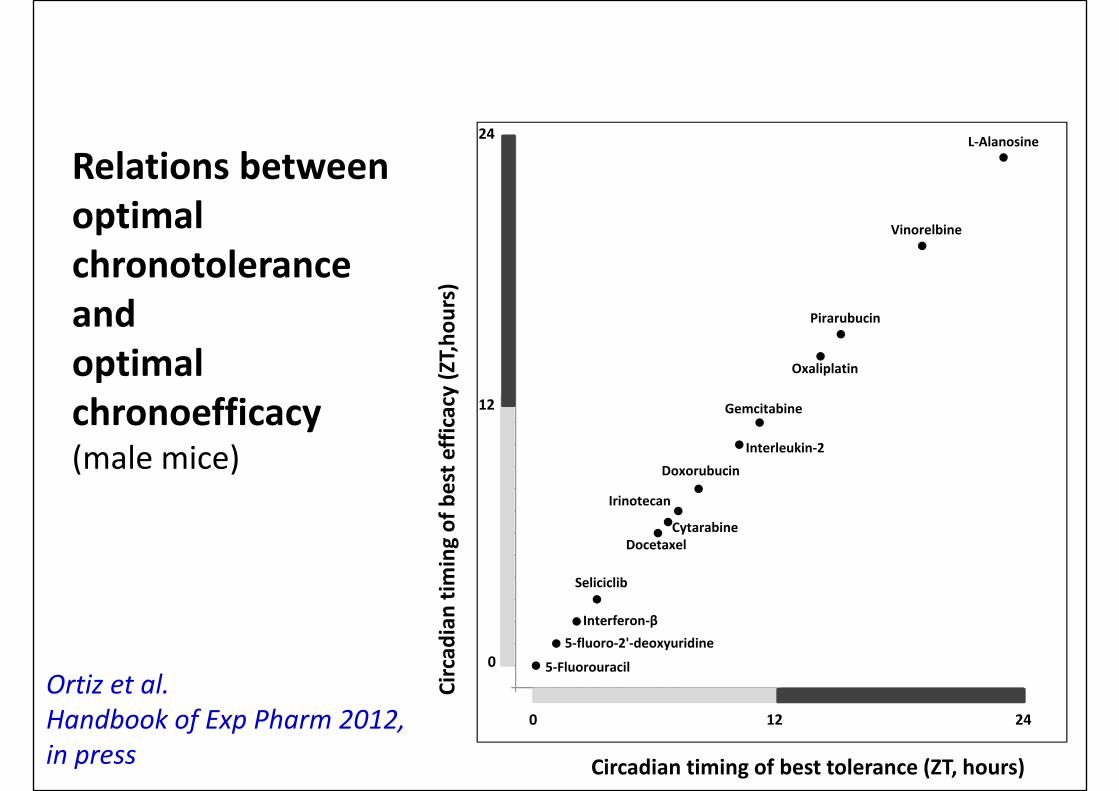
Relations betweenoptimalchronotoleranceandoptimalchronoefficacy(male mice)
Ortiz et al.Handbook of Exp Pharm 2012,in press
L‐Alanosine
Vinorelbine
Pirarubucin
Oxaliplatin
Gemcitabine
Interleukin‐2Doxorubucin
Irinotecan
CytarabineDocetaxel
Seliciclib
Interferon‐β5‐fluoro‐2'‐deoxyuridine
0 12 24
0
12
24
5‐Fluorouracil
Circadian timing of best tolerance (ZT, hours)
Circad
ian tim
ing of best e
fficacy (ZT,ho
urs)
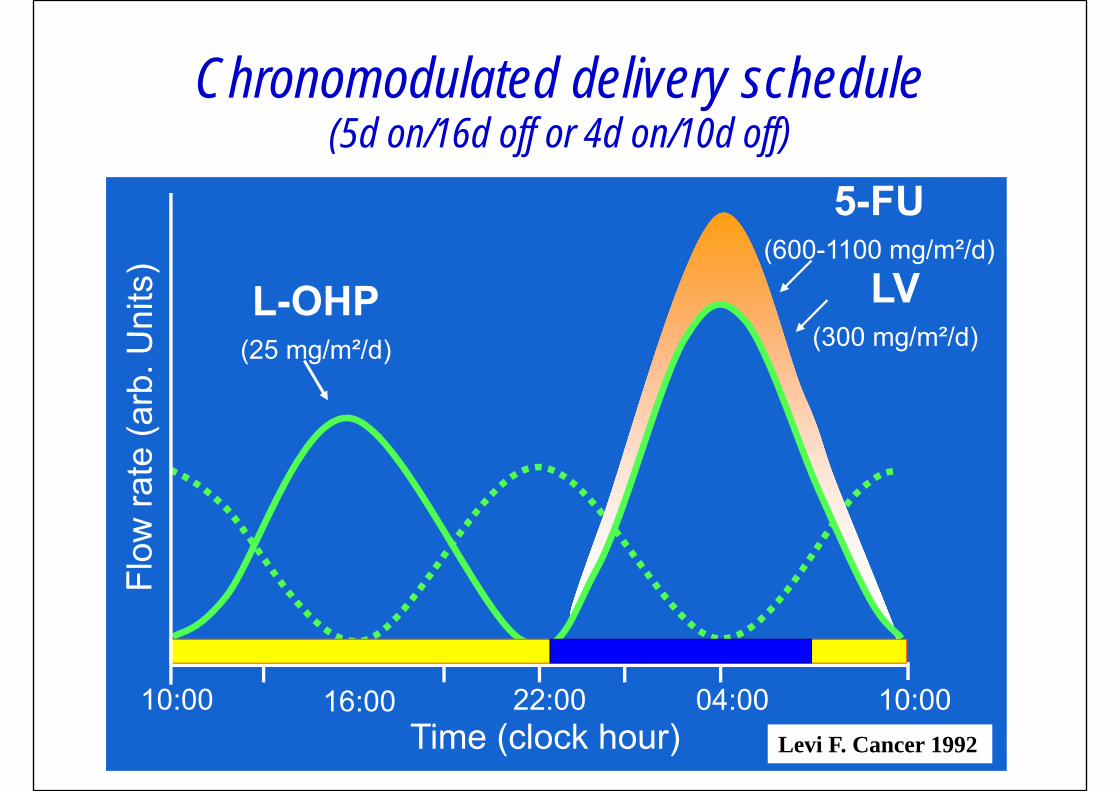
Chronomodulated delivery schedule(5d on/16d off or 4d on/10d off)
Time (clock hour)10:00 16:00 22:00 04:00 10:00
5-FU(600-1100 mg/m²/d)
LV(300 mg/m²/d)
L-OHP(25 mg/m²/d)
Levi F. Cancer 1992
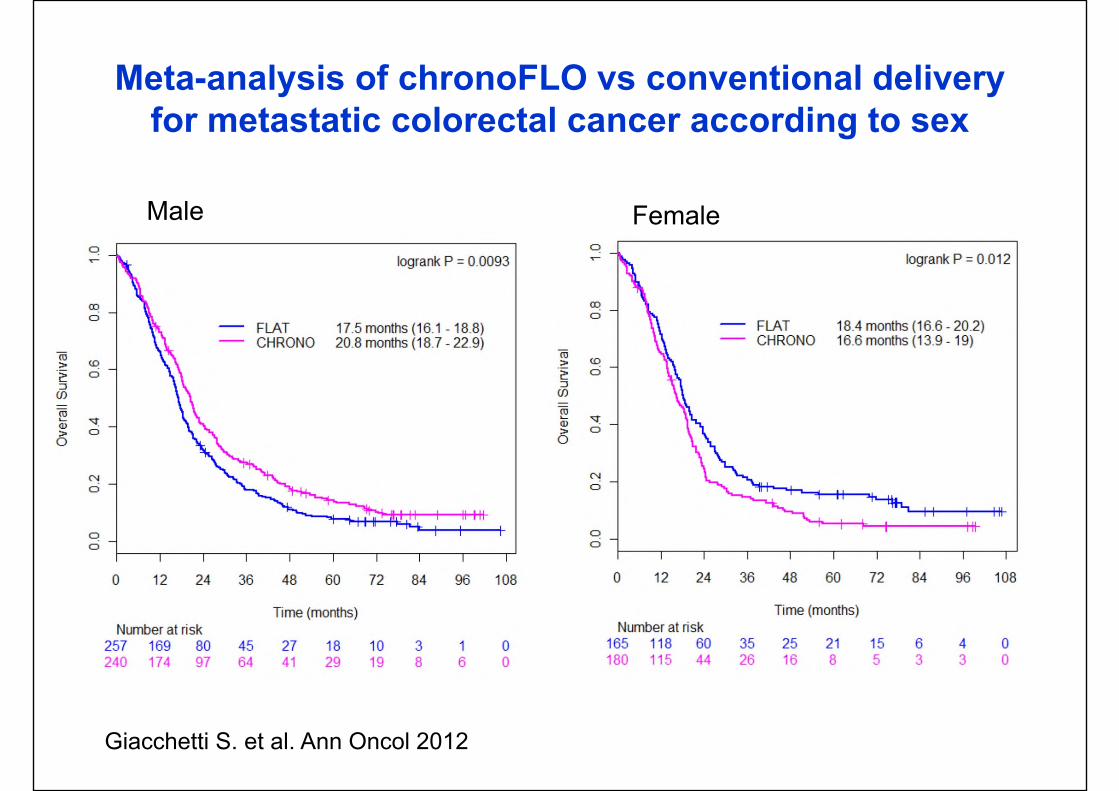
Male Female
Giacchetti S. et al. Ann Oncol 2012
Meta-analysis of chronoFLO vs conventional deliveryfor metastatic colorectal cancer according to sex
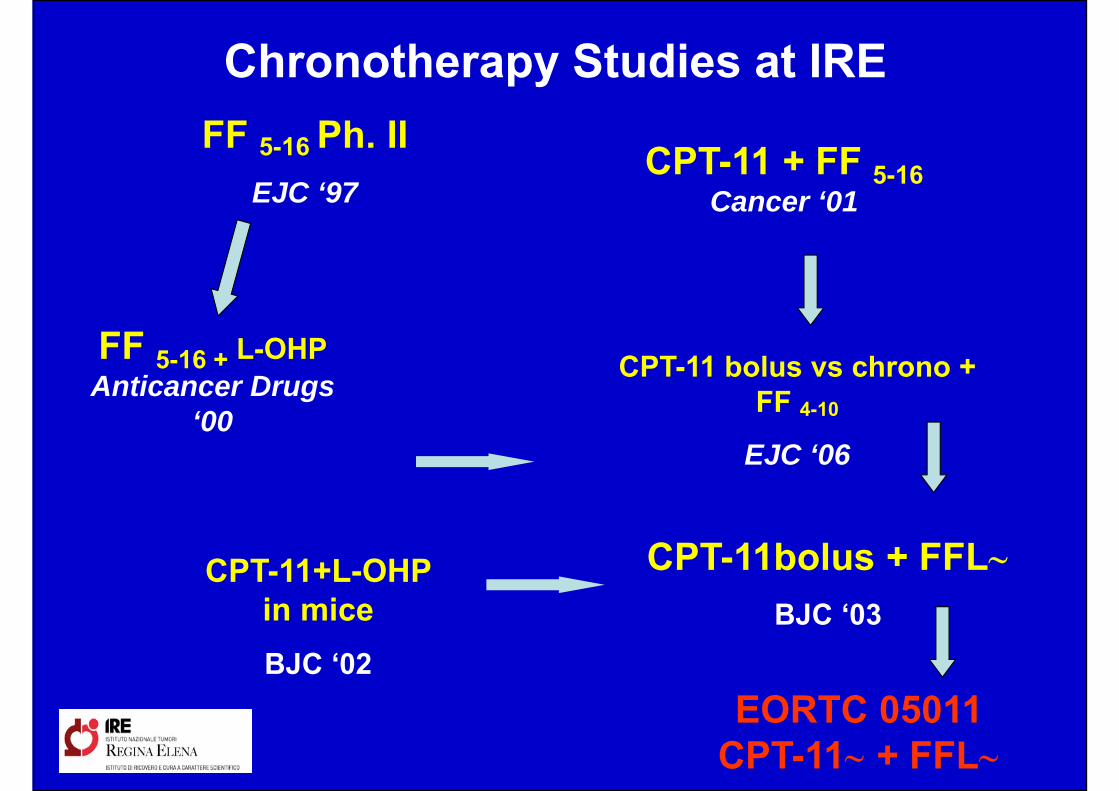
FF 5-16 Ph. IIEJC ‘97
FF 5-16 + L-OHP Anticancer Drugs
‘00
CPT-11+L-OHP in miceBJC ‘02
CPT-11 bolus vs chrono + FF 4-10
EJC ‘06
CPT-11 + FF 5-16Cancer ‘01
EORTC 05011 CPT-11∼ + FFL∼
Chronotherapy Studies at IRE
CPT-11bolus + FFL∼BJC ‘03
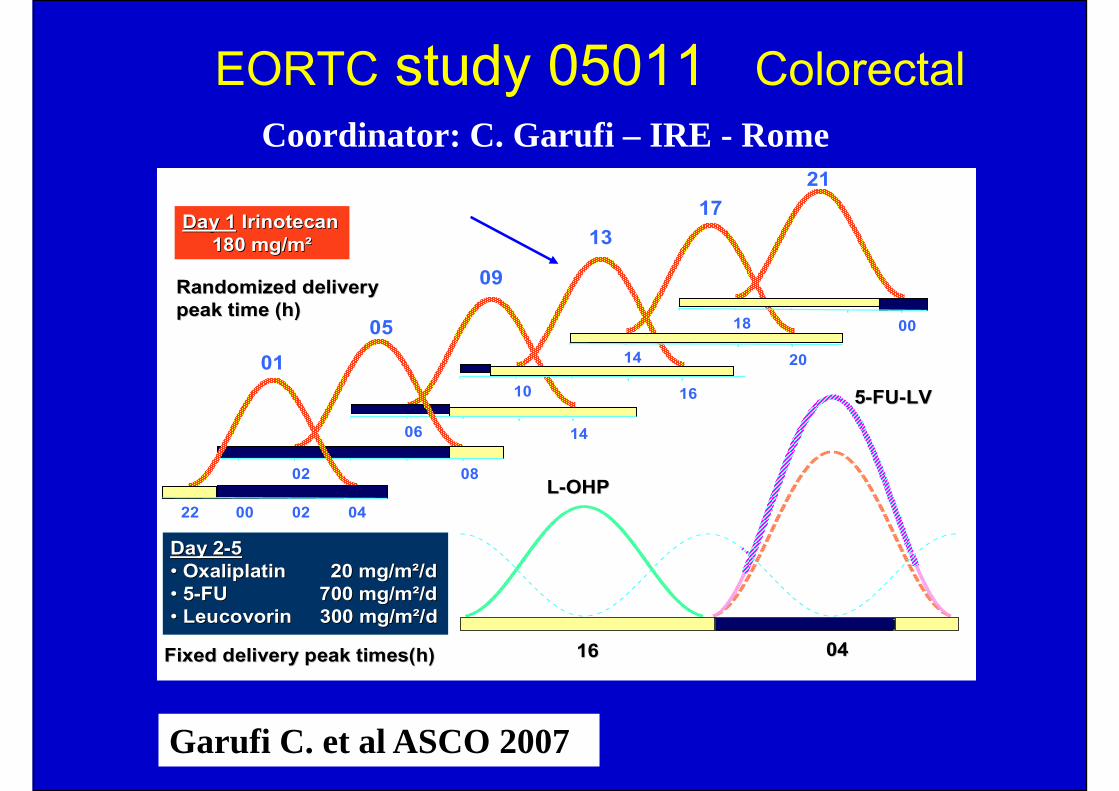
EORTC study 05011 Colorectal
DayDay 22--55•• OxaliplatinOxaliplatin 20 mg/m²/d20 mg/m²/d•• 55--FU FU 700 mg/m²/d700 mg/m²/d•• LeucovorinLeucovorin 300 mg/m²/d300 mg/m²/d
1616 0404
55--FUFU--LVLV
DayDay 11 IrinotecanIrinotecan180 mg/m²180 mg/m²
LL--OHPOHP
05
06
09
14
02 08
00 02 0422
0110
13
16
14
17
20
18
21
00
Randomized deliveryRandomized deliverypeakpeak time (h)time (h)
Fixed delivery peak timesFixed delivery peak times(h)(h)
Coordinator: C. Garufi – IRE - Rome
Garufi C. et al ASCO 2007
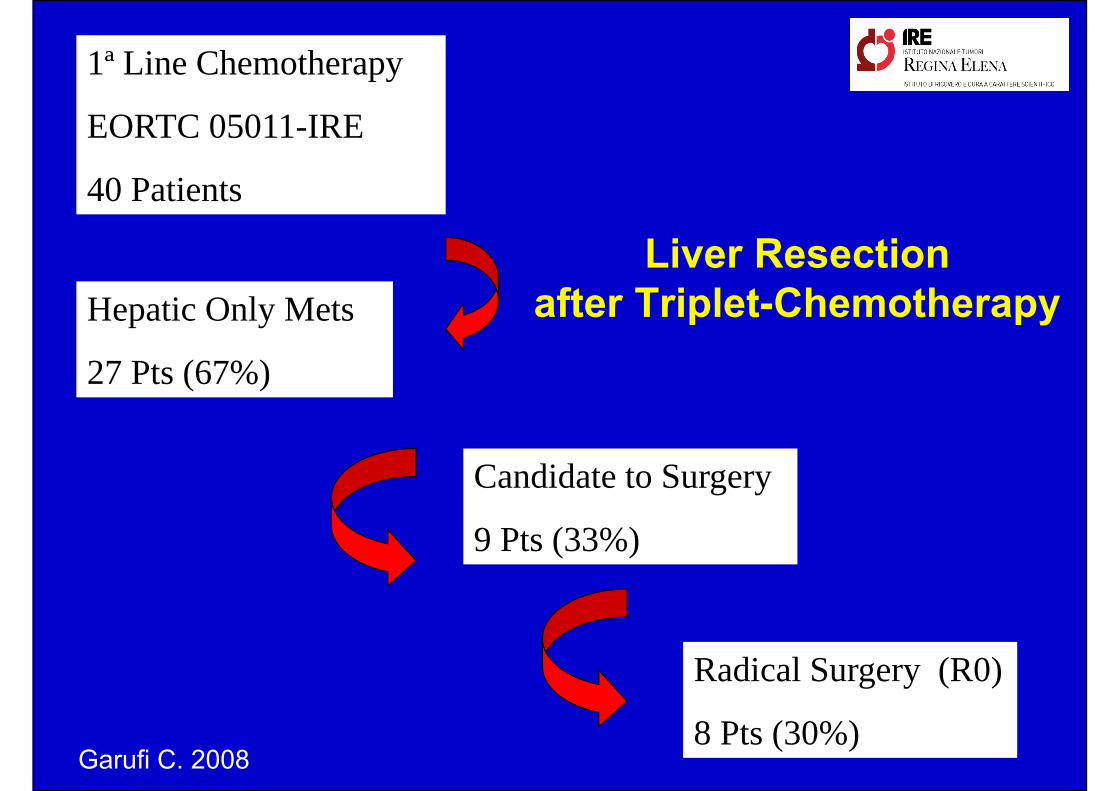
Liver Resection after Triplet-Chemotherapy
1ª Line Chemotherapy
EORTC 05011-IRE
40 Patients
Candidate to Surgery
9 Pts (33%)
Radical Surgery (R0)
8 Pts (30%)
Hepatic Only Mets
27 Pts (67%)
Garufi C. 2008
• Do patients need chemotherapy for treatment of CRLMs? We think YES
• Aim: Cure or Increase of survival?• When deliver chemo? After, Before, Sandwich …• Which one? Chemo alone, chemo + Ab ….• How to deliver it? EV or IA or both?• How long after resection?? • Do all patients have the same biologic behaviour?
Clearly Not
Chemotherapy and Liver Metastases
Definition of “Curative Intent”
Cure: DFS at 3 years and not OS
OS can reflect tumor biology while DFSlikely reflects surgical cure
Not all patients who can be offered apossible R0 resection can be offered itwith realistic curative intent
Saltz L. ASCO – 2012
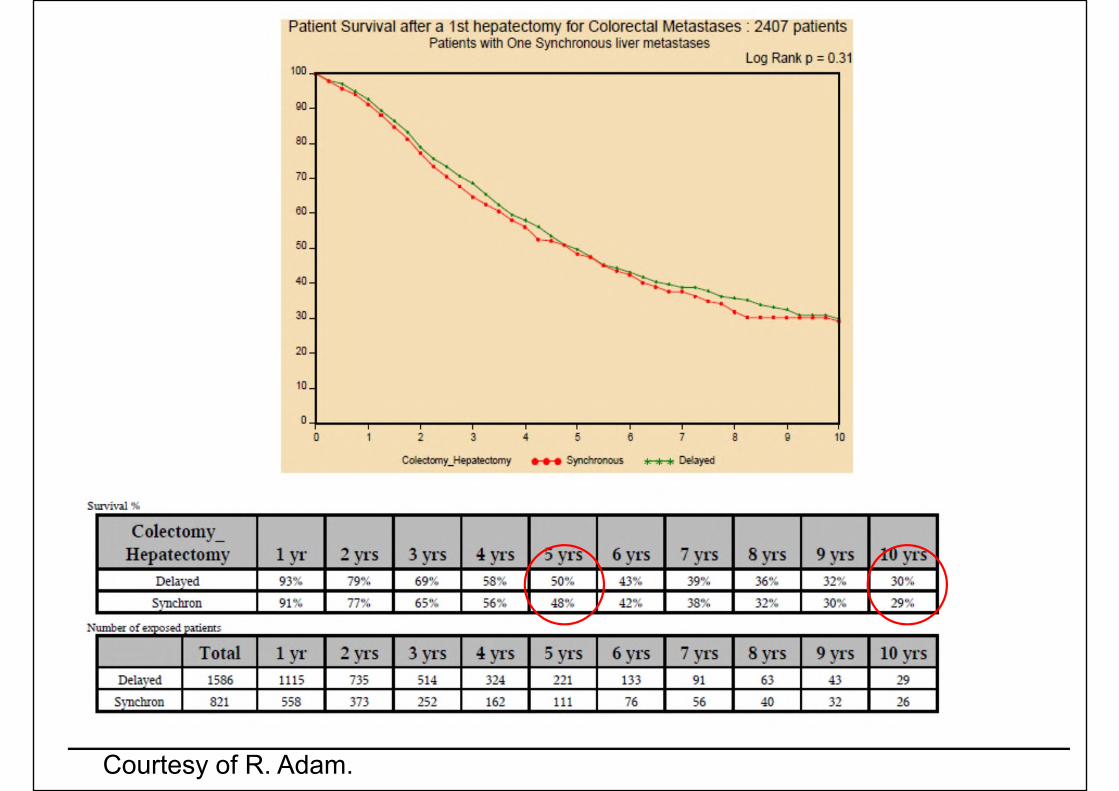
Courtesy of R. Adam.
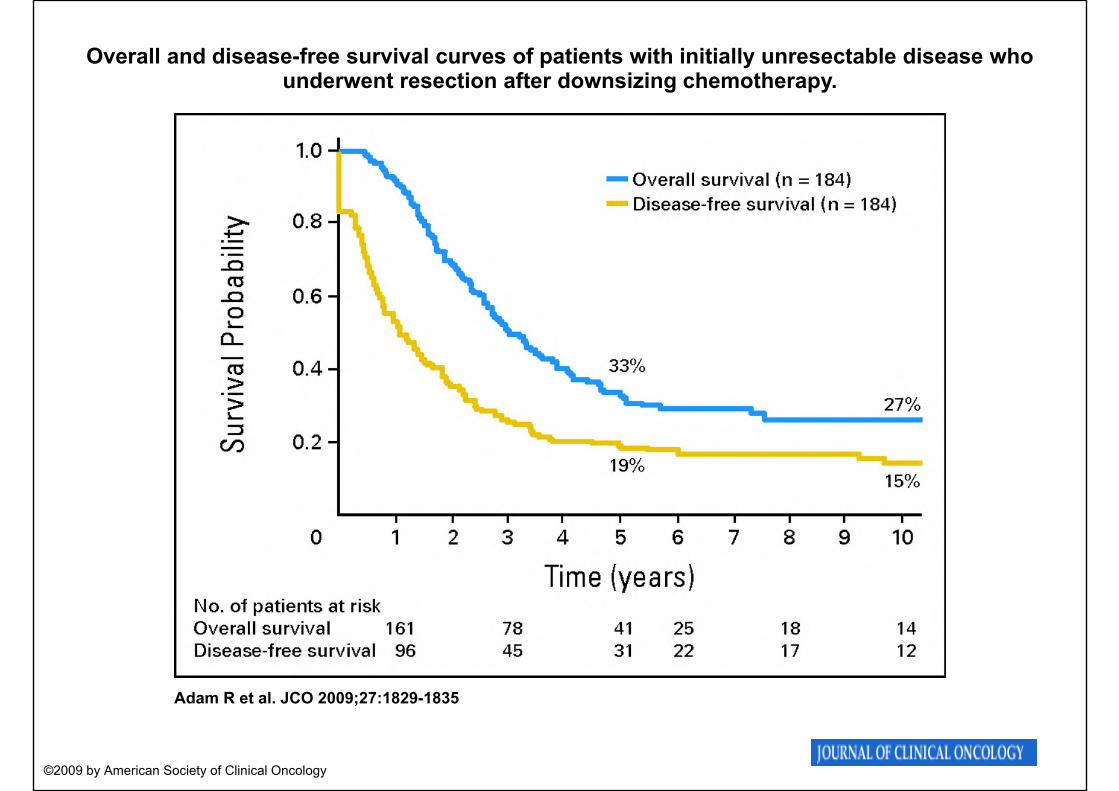
Overall and disease-free survival curves of patients with initially unresectable disease who underwent resection after downsizing chemotherapy.
Adam R et al. JCO 2009;27:1829-1835
©2009 by American Society of Clinical Oncology
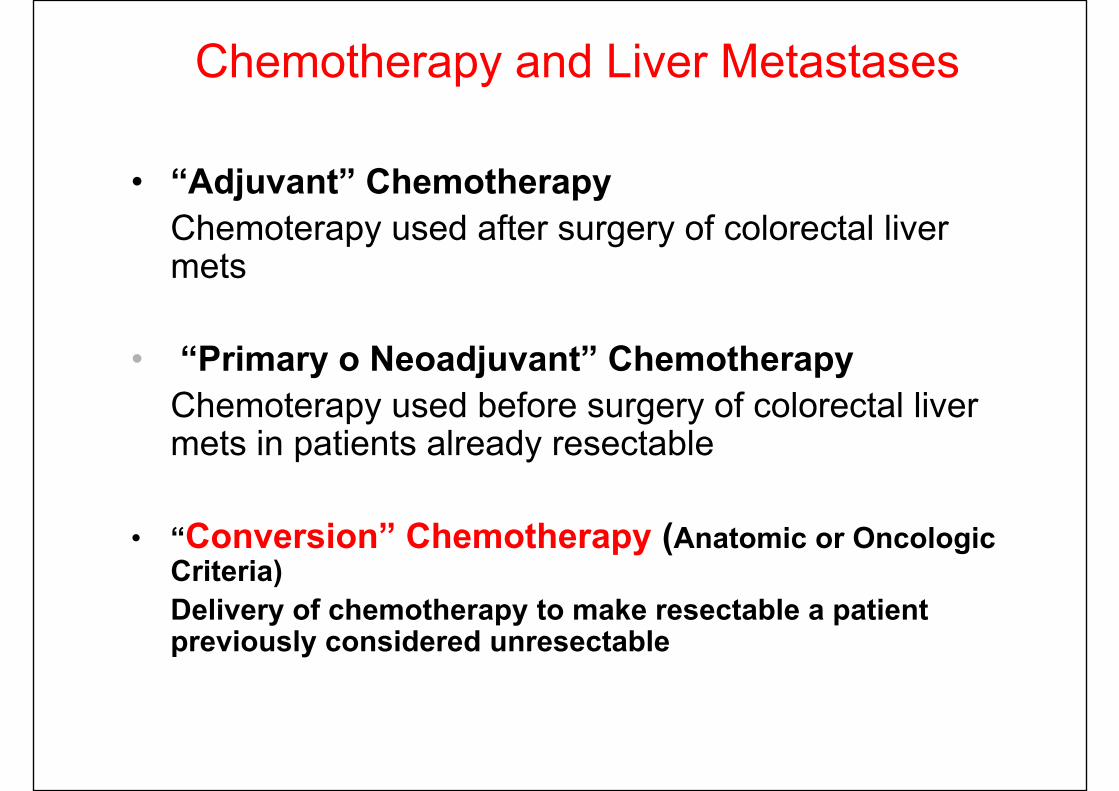
• “Adjuvant” Chemotherapy Chemoterapy used after surgery of colorectal liver mets
• “Primary o Neoadjuvant” ChemotherapyChemoterapy used before surgery of colorectal liver mets in patients already resectable
• “Conversion” Chemotherapy (Anatomic or Oncologic Criteria)Delivery of chemotherapy to make resectable a patient previously considered unresectable
Chemotherapy and Liver Metastases
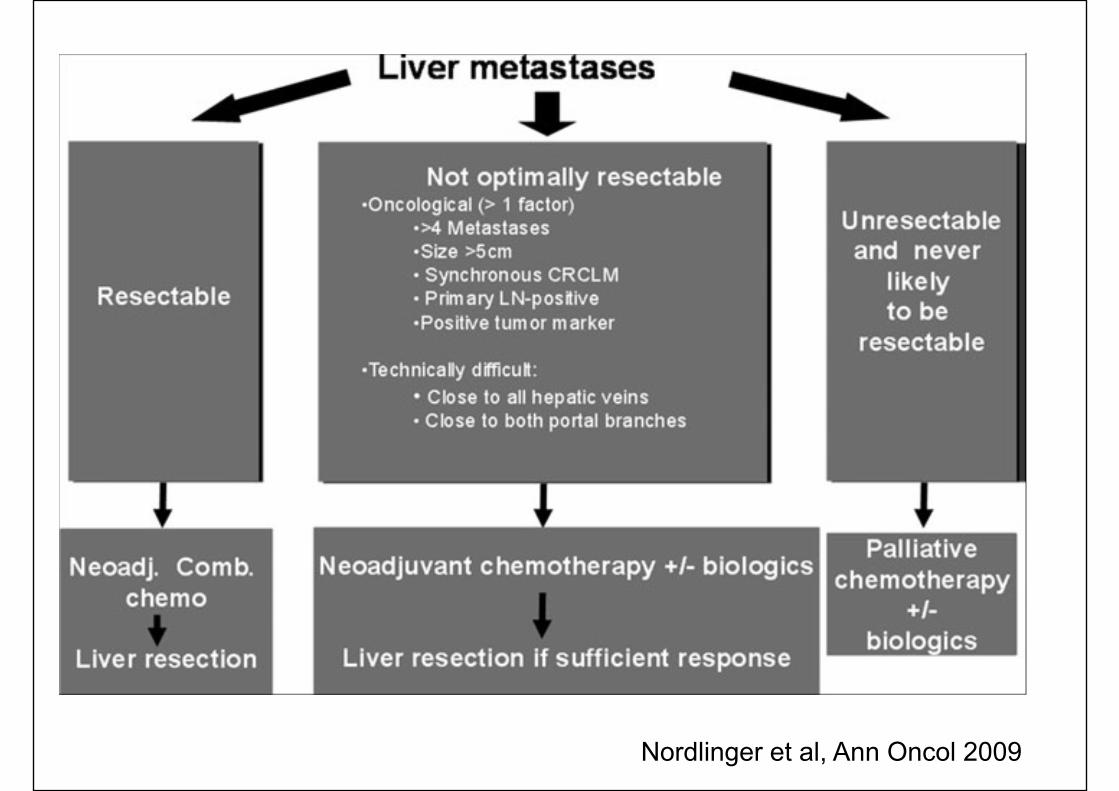
Nordlinger et al, Ann Oncol 2009
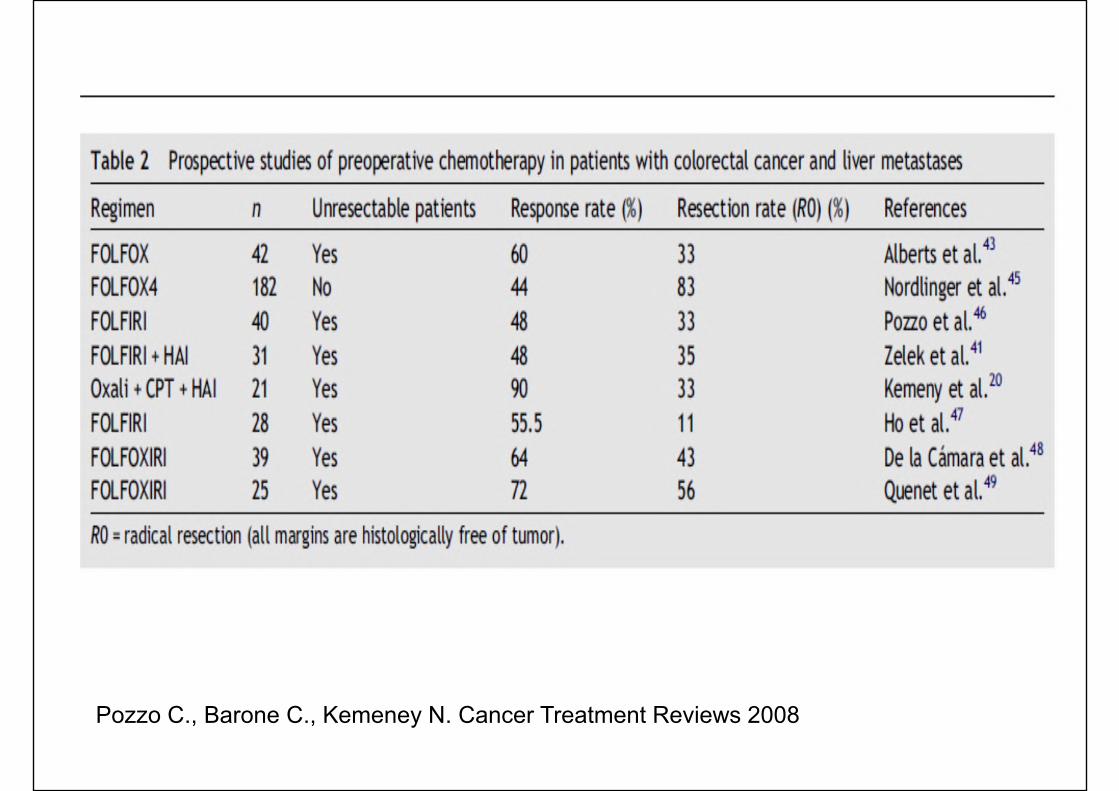
Pozzo C., Barone C., Kemeney N. Cancer Treatment Reviews 2008
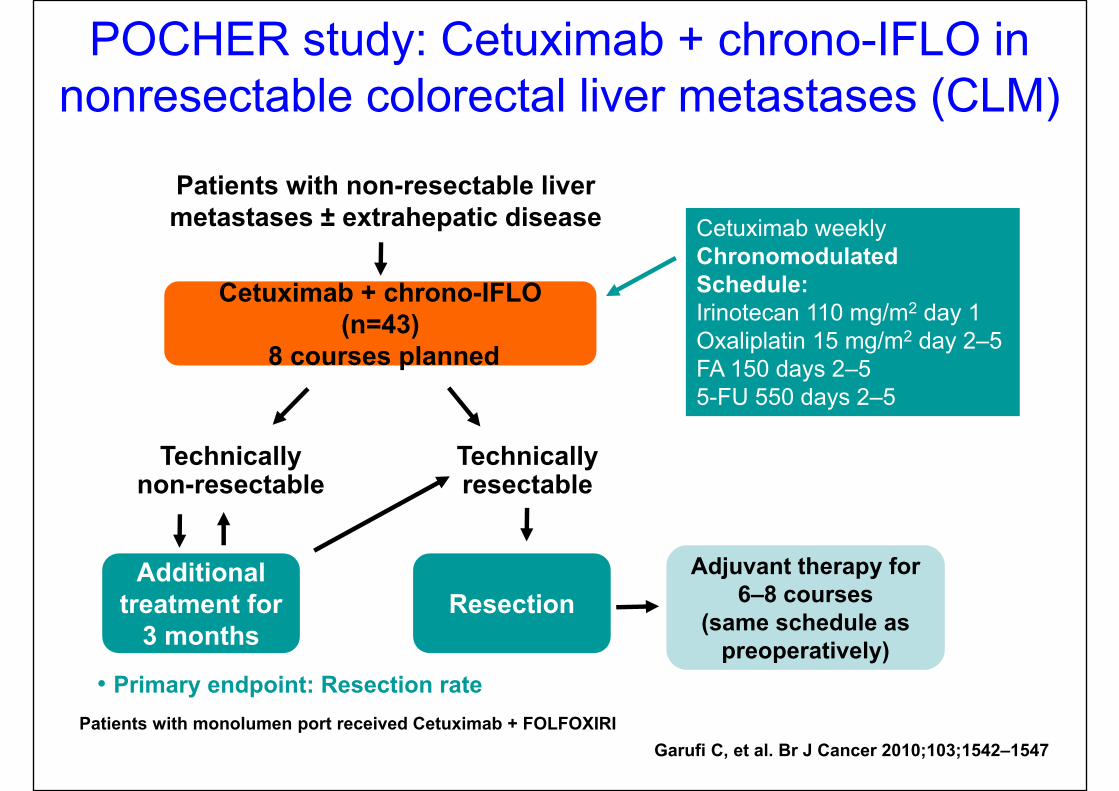
POCHER study: Cetuximab + chrono-IFLO in nonresectable colorectal liver metastases (CLM)
Adjuvant therapy for 6–8 courses
(same schedule as preoperatively)
Patients with non-resectable liver metastases ± extrahepatic disease
Cetuximab + chrono-IFLO (n=43)
8 courses planned
Technically resectable
• Primary endpoint: Resection rate
Additional treatment for
3 months
Technically non-resectable
Patients with monolumen port received Cetuximab + FOLFOXIRI
Resection
Cetuximab weeklyChronomodulated Schedule:Irinotecan 110 mg/m2 day 1Oxaliplatin 15 mg/m2 day 2–5 FA 150 days 2–55-FU 550 days 2–5
Garufi C, et al. Br J Cancer 2010;103;1542–1547
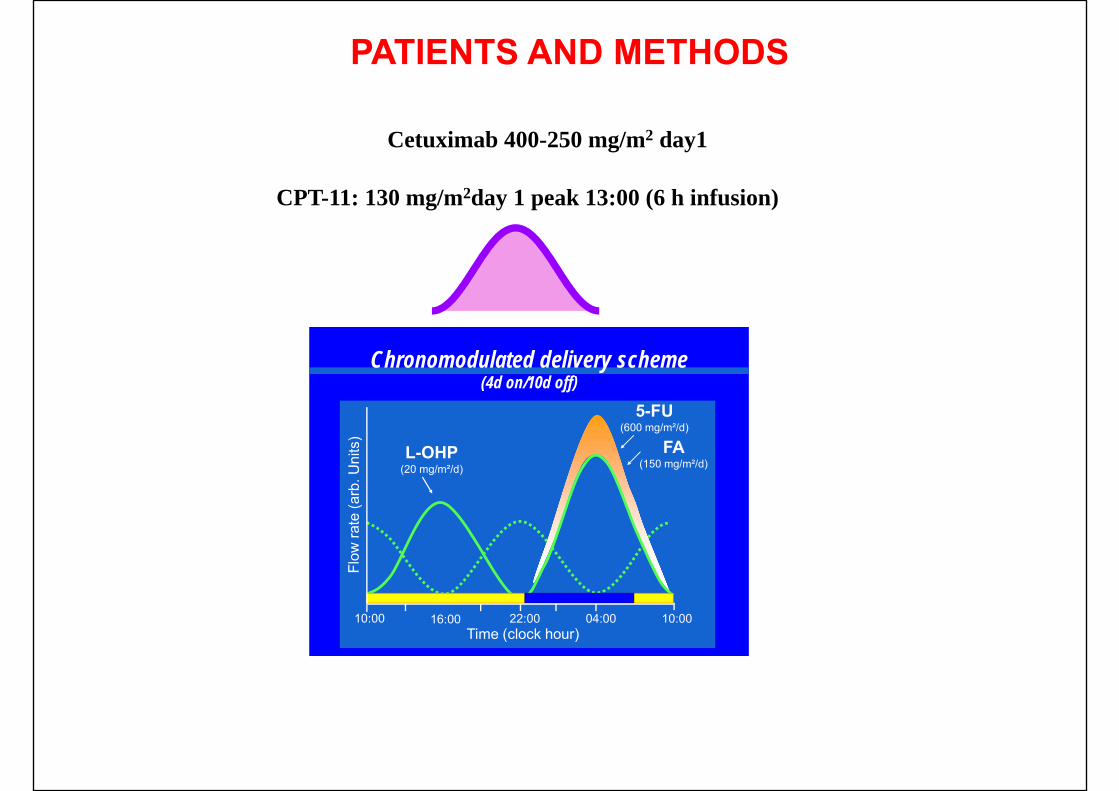
PATIENTS AND METHODS
Cetuximab plus chronomodulated CPT-FFL: first-line/patientswith unresectable CLM.
Schedule:a) weekly cetuximab (400 mg/m2 - w1, then 250 mg/m2)b) CPT-11 130 mg/m2/d1 (6-h infusion-peak 13:00), then 12-h
infusions of L-OHP 20/mg/m2/d (peak at 16:00), FA 150 mg/m2/dplus 5-FU 600 mg/m2/d (peak at 4:00), days 2-5 q2 weeks.
Cetuximab was given irrespective of EGFR IHC expression orK-RAS mutation status. Both were evaluated retrospectively.
After the first 17 patients 5-FU and the L-OHP daily dose werereduced from 600 to 550 mg/m2 and from 20 to 15 mg/m2
respectively with CPT-11 at 130 mg/m2/d1 (courses every 2wks). Two/ 43 patients received FOLFOXIRI instead of CPT-FFL.French recommendations and internal criteria were used toclassify liver metastases for resectability.
CPT-11: 130 mg/m2day 1 peak 13:00 (6 h infusion)
Chronomodulated delivery scheme(4d on/10d off)
Time (clock hour)10:00 16:00 22:00 04:00 10:00
5-FU(600 mg/m²/d)
FA(150 mg/m²/d)
L-OHP(20 mg/m²/d)
Cetuximab 400-250 mg/m2 day1
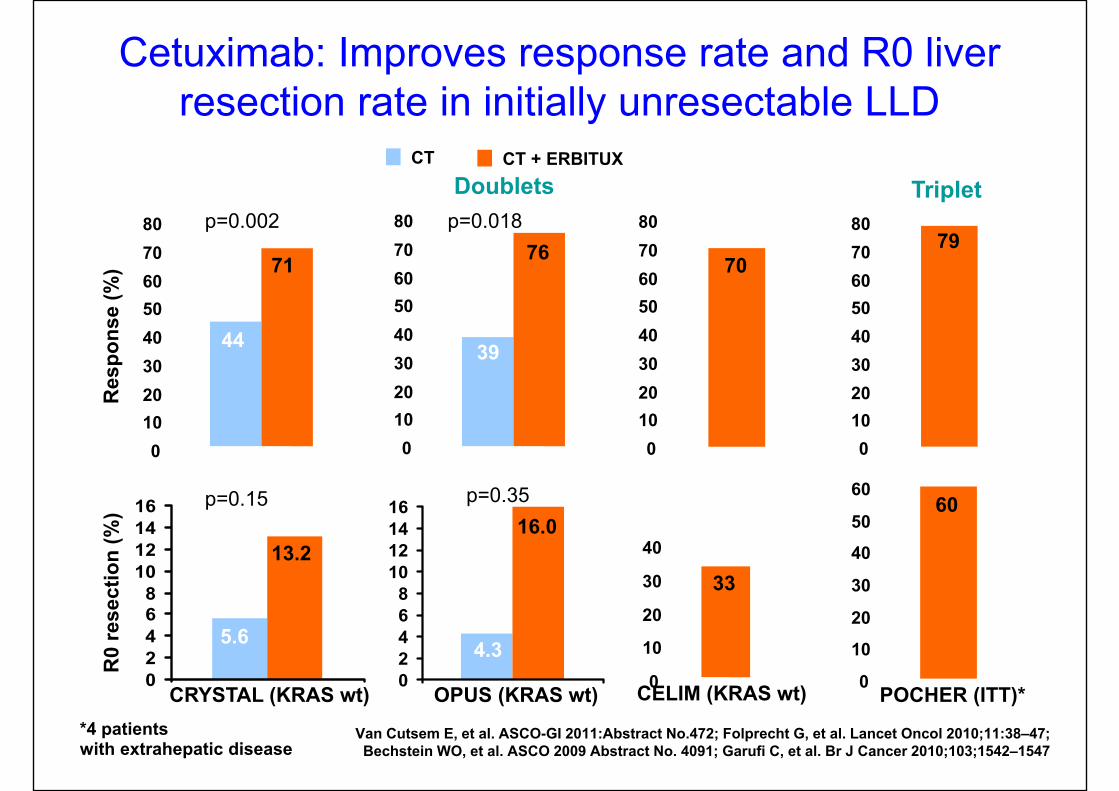
Cetuximab: Improves response rate and R0 liver resection rate in initially unresectable LLD
CT CT + ERBITUX
*4 patientswith extrahepatic disease
Res
pons
e (%
)R
0 re
sect
ion
(%) 60
0
10
20
30
40
50
60
POCHER (ITT)* 02468
10121416
CRYSTAL (KRAS wt)
5.6
13.2
01020304050607080
79
Triplet
CELIM (KRAS wt)
33
0
10
20
30
40
p=0.002Doublets
Van Cutsem E, et al. ASCO-GI 2011:Abstract No.472; Folprecht G, et al. Lancet Oncol 2010;11:38–47; Bechstein WO, et al. ASCO 2009 Abstract No. 4091; Garufi C, et al. Br J Cancer 2010;103;1542–1547
44
71
01020304050607080
70
01020304050607080
44
71
39
76
01020304050607080
39
76p=0.018
p=0.15
02468
10121416
OPUS (KRAS wt)
16.0
4.3
p=0.35
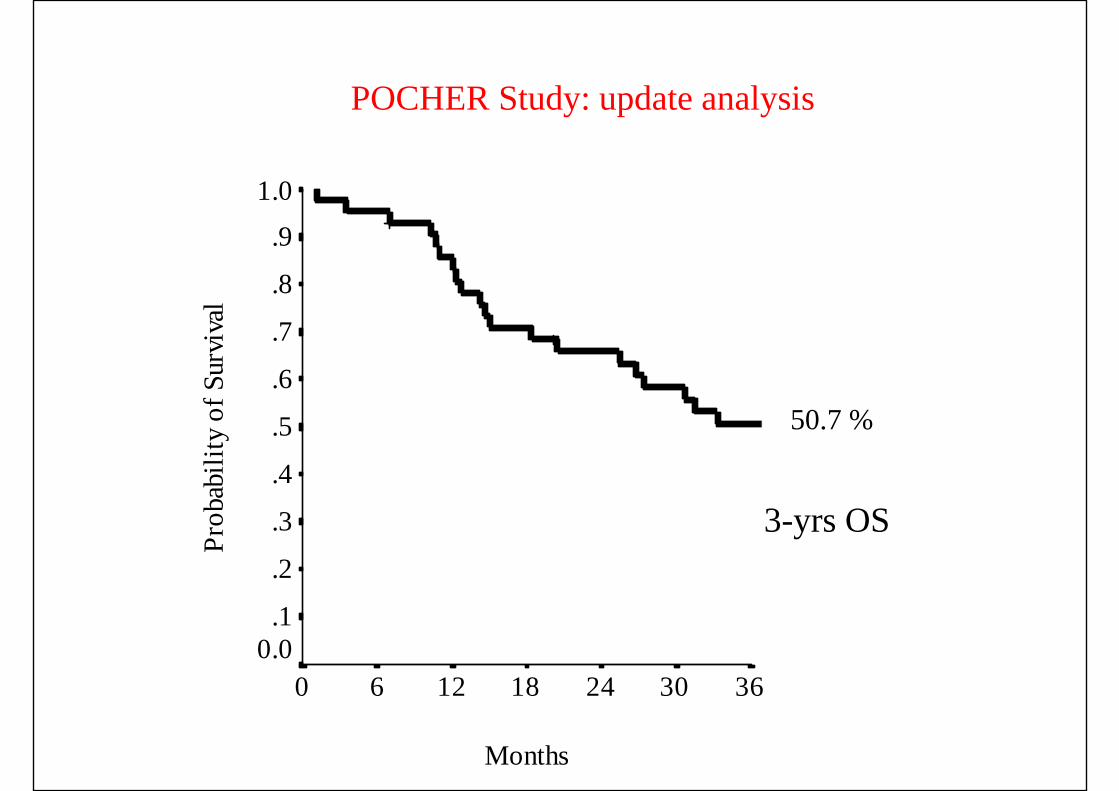
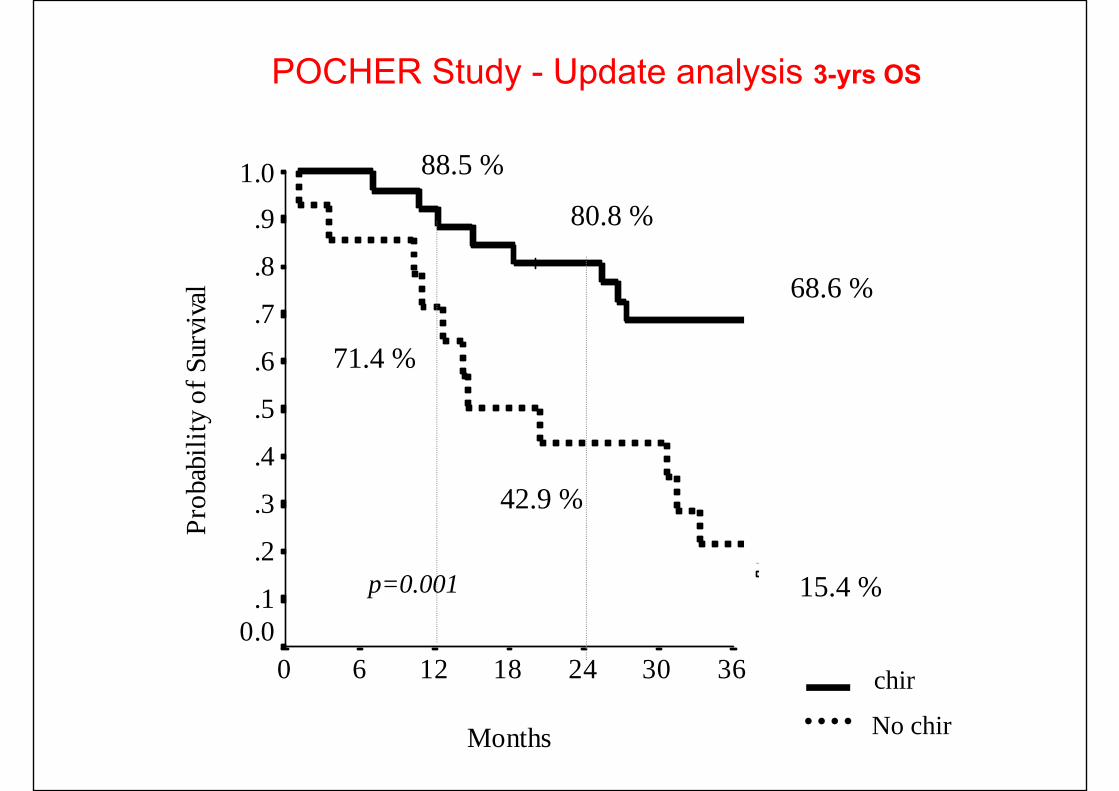
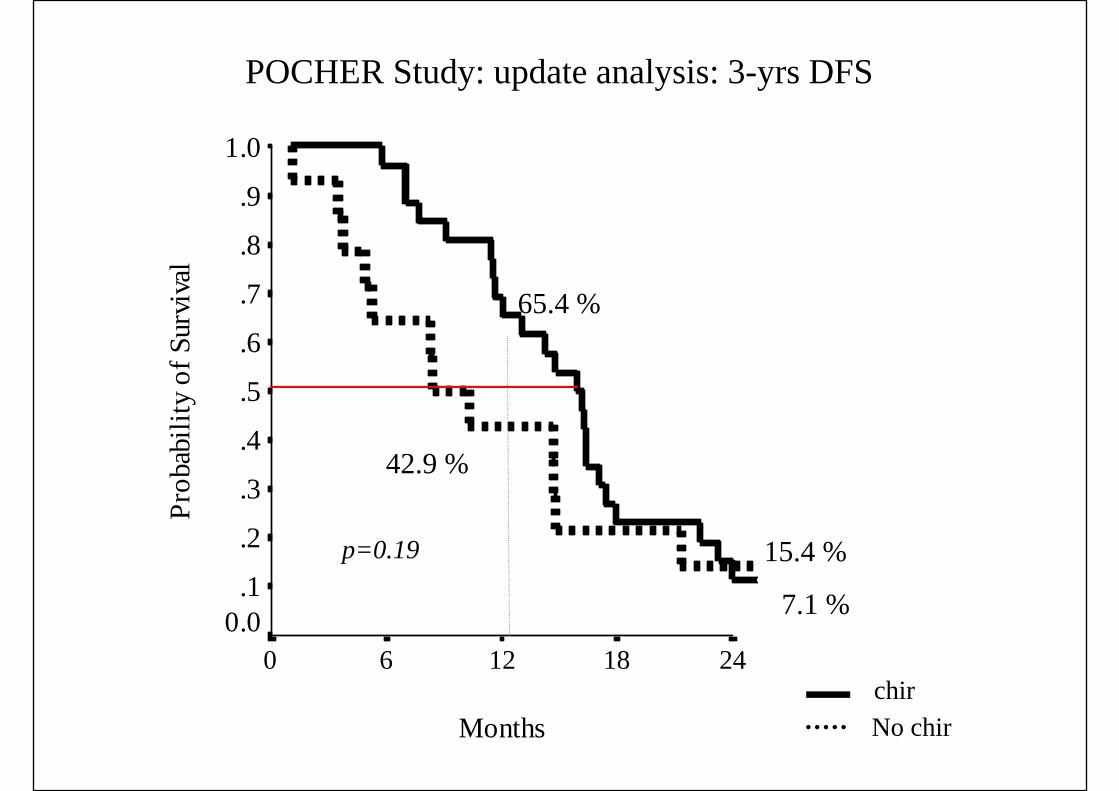
POCHER Study: update analysis
50.7 %
80.6 %
65.9 %
Months
363024181260
Prob
abili
ty o
f Sur
viva
l1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
3-yrs OS
Months
363024181260
Prob
abili
ty o
f Sur
viva
l1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
68.6 %
15.4 %
42.9 %
80.8 %
p=0.001
chir
No chir
88.5 %
71.4 %
POCHER Study - Update analysis 3-yrs OS
Months
24181260
Prob
abili
ty o
f Sur
viva
l1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0 7.1 %
15.4 %
42.9 %
65.4 %
p=0.19
chirNo chir
POCHER Study: update analysis: 3-yrs DFS
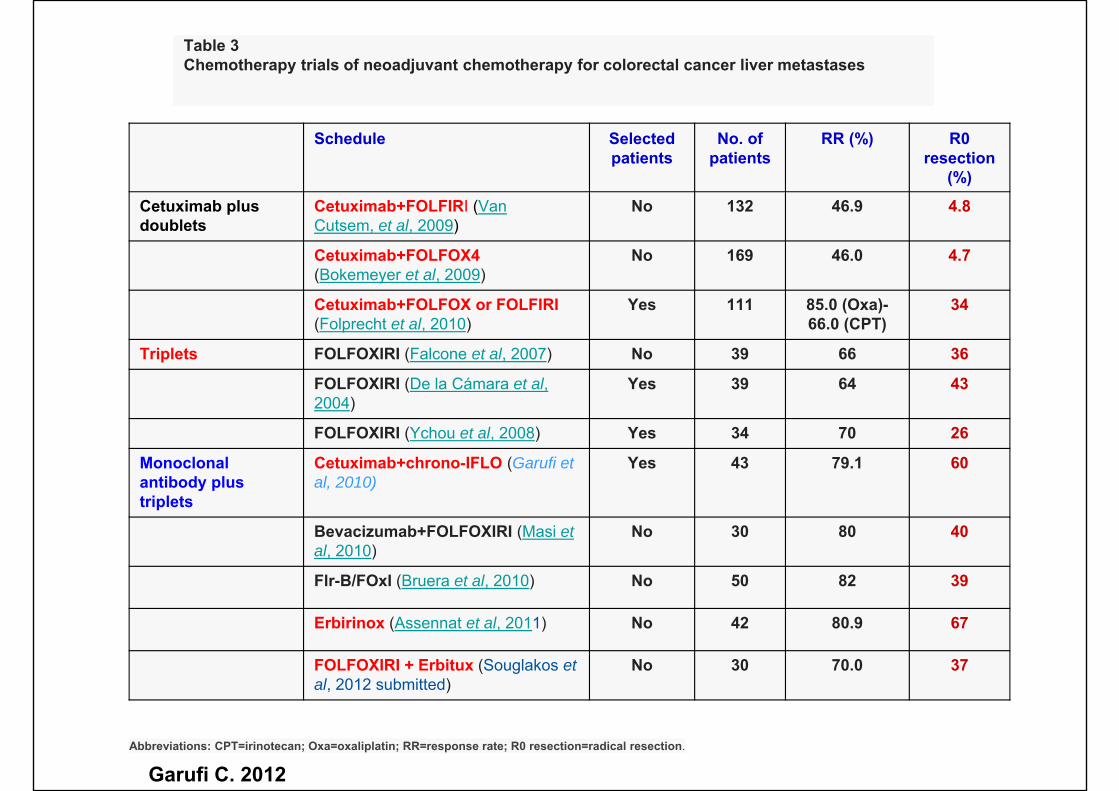
Table 3Chemotherapy trials of neoadjuvant chemotherapy for colorectal cancer liver metastases
Schedule Selected patients
No. of patients
RR (%) R0 resection
(%)
Cetuximab plus doublets
Cetuximab+FOLFIRI (Van Cutsem, et al, 2009)
No 132 46.9 4.8
Cetuximab+FOLFOX4 (Bokemeyer et al, 2009)
No 169 46.0 4.7
Cetuximab+FOLFOX or FOLFIRI(Folprecht et al, 2010)
Yes 111 85.0 (Oxa)-66.0 (CPT)
34
Triplets FOLFOXIRI (Falcone et al, 2007) No 39 66 36
FOLFOXIRI (De la Cámara et al, 2004)
Yes 39 64 43
FOLFOXIRI (Ychou et al, 2008) Yes 34 70 26
Monoclonal antibody plus triplets
Cetuximab+chrono-IFLO (Garufi et al, 2010)
Yes 43 79.1 60
Bevacizumab+FOLFOXIRI (Masi et al, 2010)
No 30 80 40
Flr-B/FOxI (Bruera et al, 2010) No 50 82 39
Erbirinox (Assennat et al, 2011) No 42 80.9 67
FOLFOXIRI + Erbitux (Souglakos et al, 2012 submitted)
No 30 70.0 37
Abbreviations: CPT=irinotecan; Oxa=oxaliplatin; RR=response rate; R0 resection=radical resection.
Garufi C. 2012
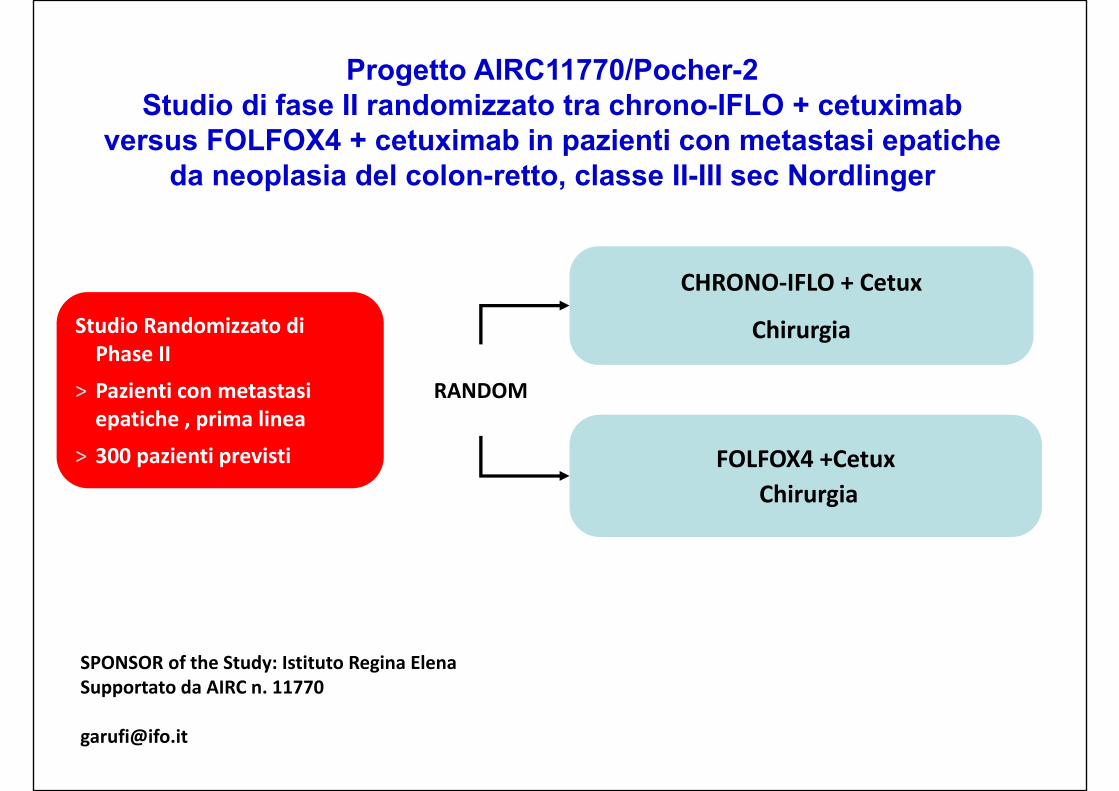
Progetto AIRC11770/Pocher-2 Studio di fase II randomizzato tra chrono-IFLO + cetuximab
versus FOLFOX4 + cetuximab in pazienti con metastasi epatiche da neoplasia del colon-retto, classe II-III sec Nordlinger
SPONSOR of the Study: Istituto Regina ElenaSupportato da AIRC n. 11770
CHRONO‐IFLO + Cetux
Chirurgia
FOLFOX4 +CetuxChirurgia
RANDOM
Studio Randomizzato di Phase II
> Pazienti con metastasi epatiche , prima linea
> 300 pazienti previsti
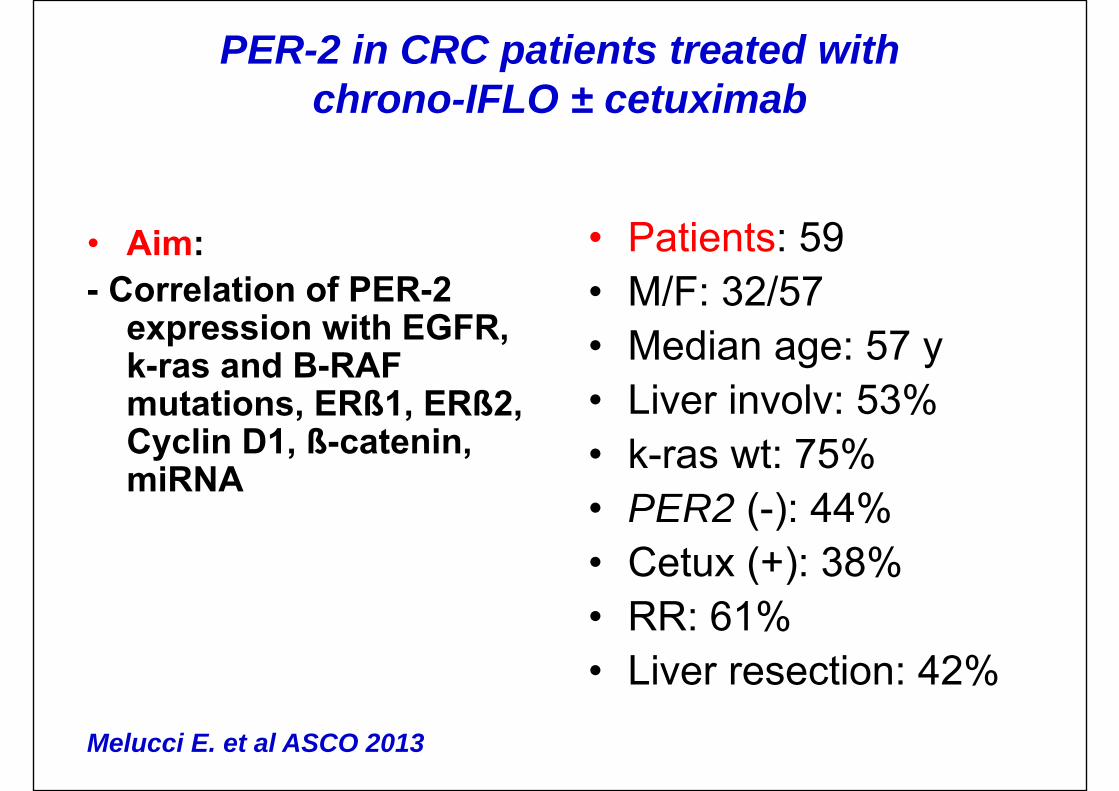
PER-2 in CRC patients treated with chrono-IFLO ± cetuximab
• Aim:- Correlation of PER-2
expression with EGFR, k-ras and B-RAF mutations, ERß1, ERß2, Cyclin D1, ß-catenin, miRNA
• Patients: 59• M/F: 32/57• Median age: 57 y• Liver involv: 53%• k-ras wt: 75%• PER2 (-): 44%• Cetux (+): 38%• RR: 61%• Liver resection: 42%
Melucci E. et al ASCO 2013
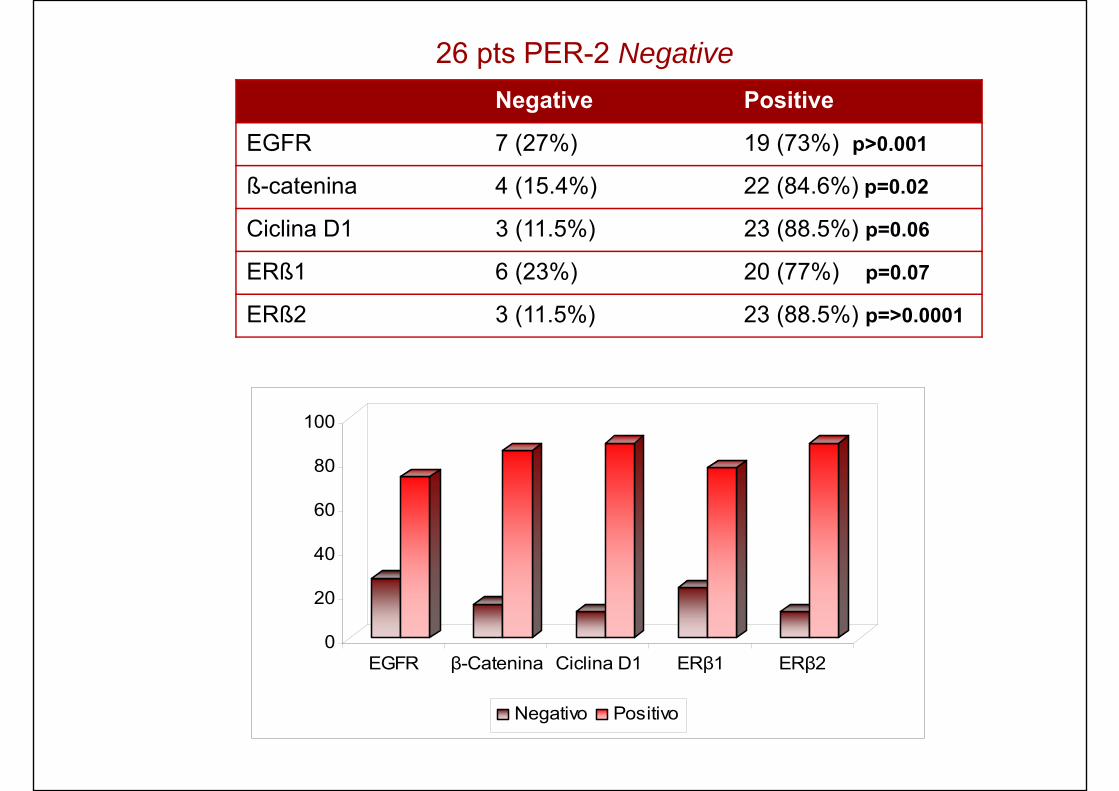
Negative Positive
EGFR 7 (27%) 19 (73%) p>0.001
ß-catenina 4 (15.4%) 22 (84.6%) p=0.02
Ciclina D1 3 (11.5%) 23 (88.5%) p=0.06
ERß1 6 (23%) 20 (77%) p=0.07
ERß2 3 (11.5%) 23 (88.5%) p=>0.0001
26 pts PER-2 Negative
0
20
40
60
80
100
EGFR β-Catenina Ciclina D1 ERβ1 ERβ2
Negativo Positivo
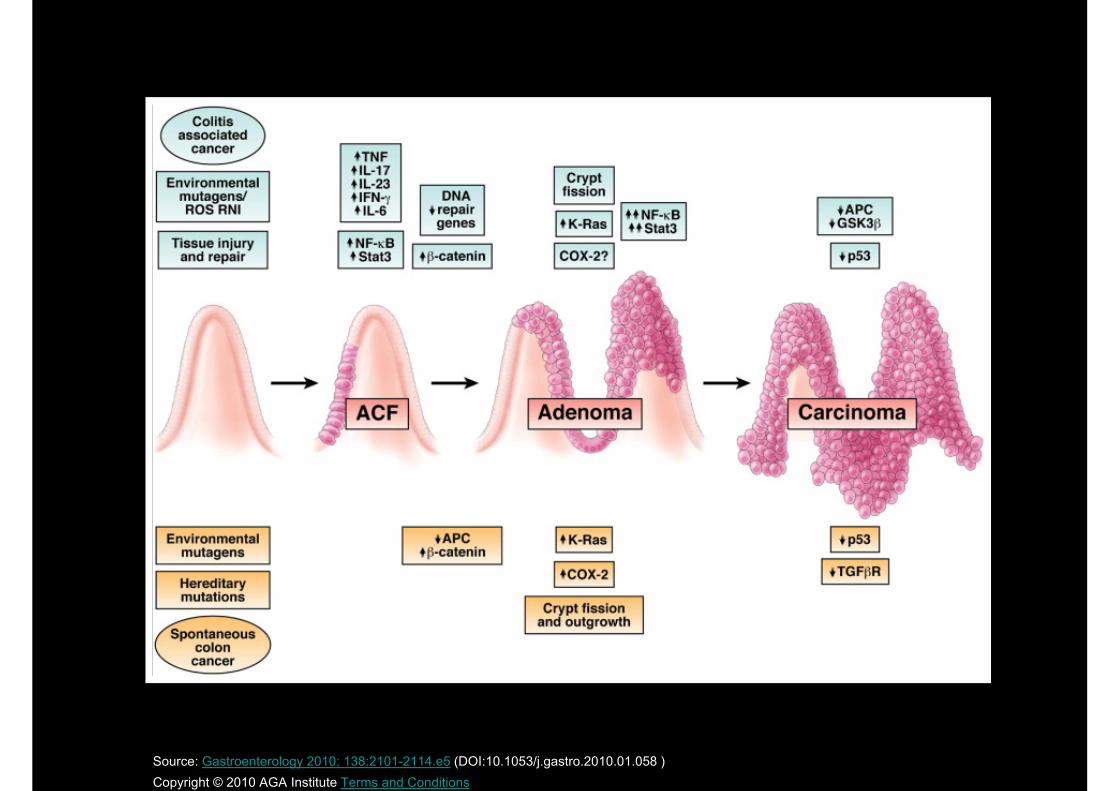
Source: Gastroenterology 2010; 138:2101-2114.e5 (DOI:10.1053/j.gastro.2010.01.058 )Copyright © 2010 AGA Institute Terms and Conditions
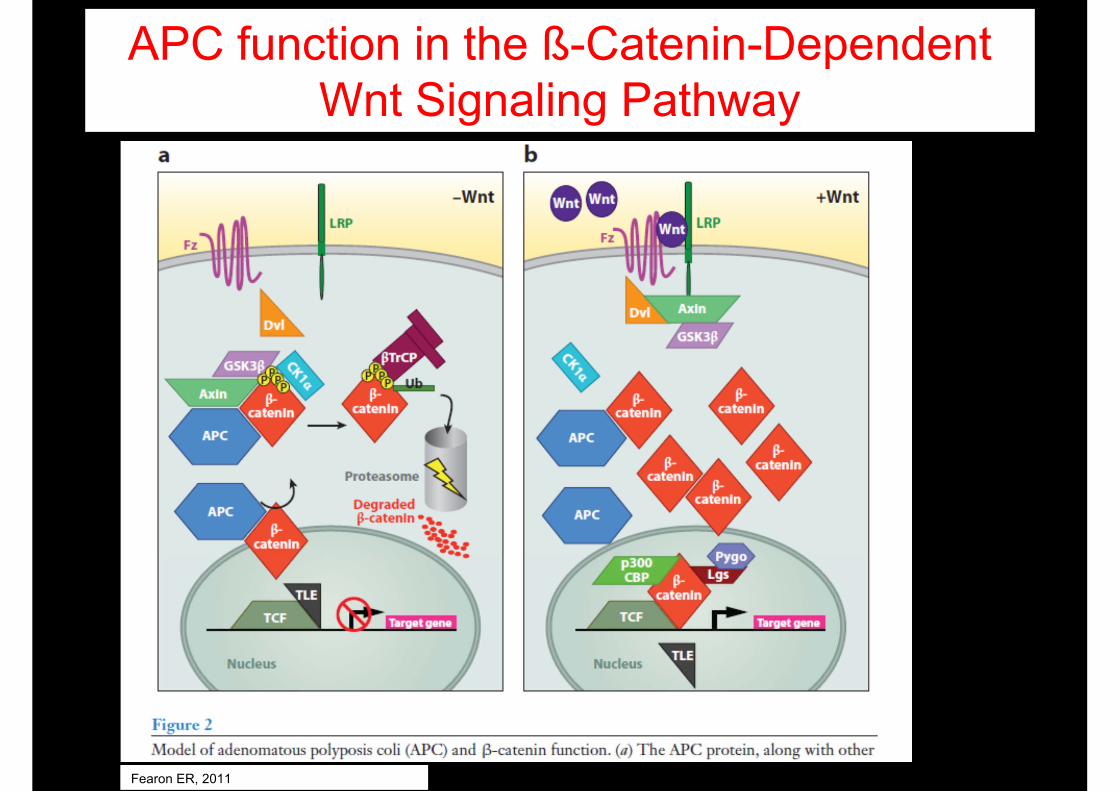
APC function in the ß-Catenin-Dependent Wnt Signaling Pathway
Fearon ER, 2011
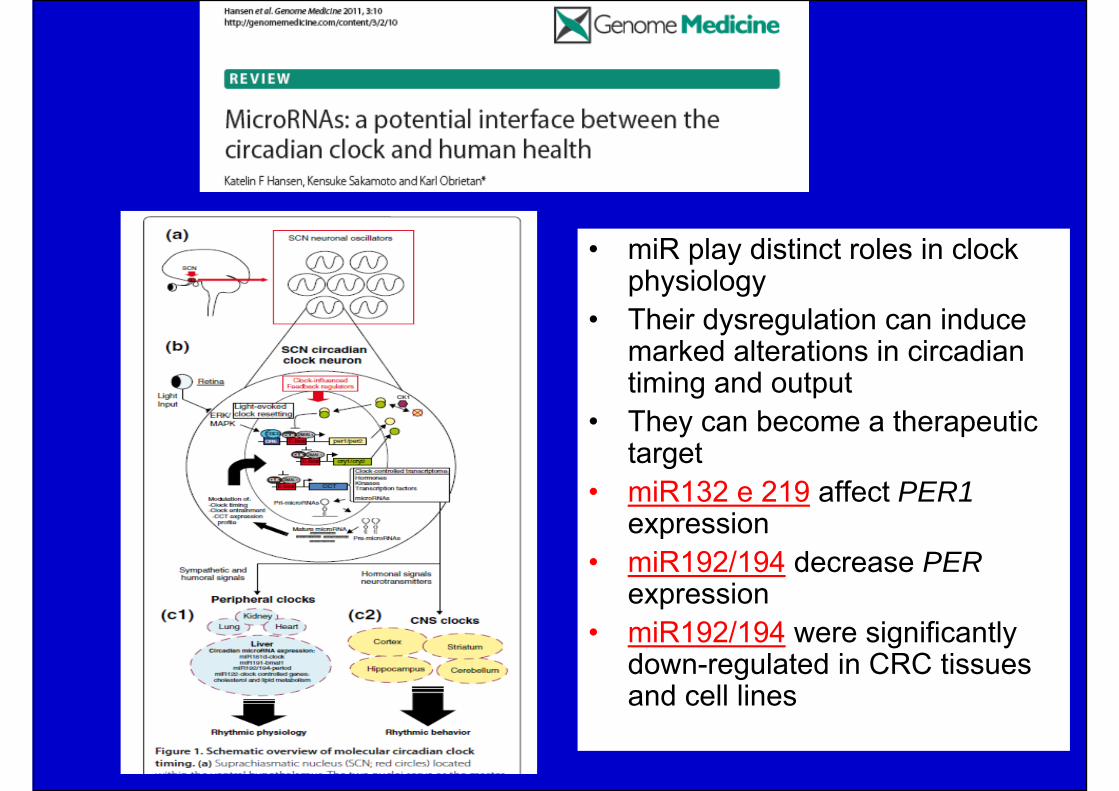
• miR play distinct roles in clock physiology
• Their dysregulation can induce marked alterations in circadian timing and output
• They can become a therapeutic target
• miR132 e 219 affect PER1expression
• miR192/194 decrease PERexpression
• miR192/194 were significantly down-regulated in CRC tissues and cell lines
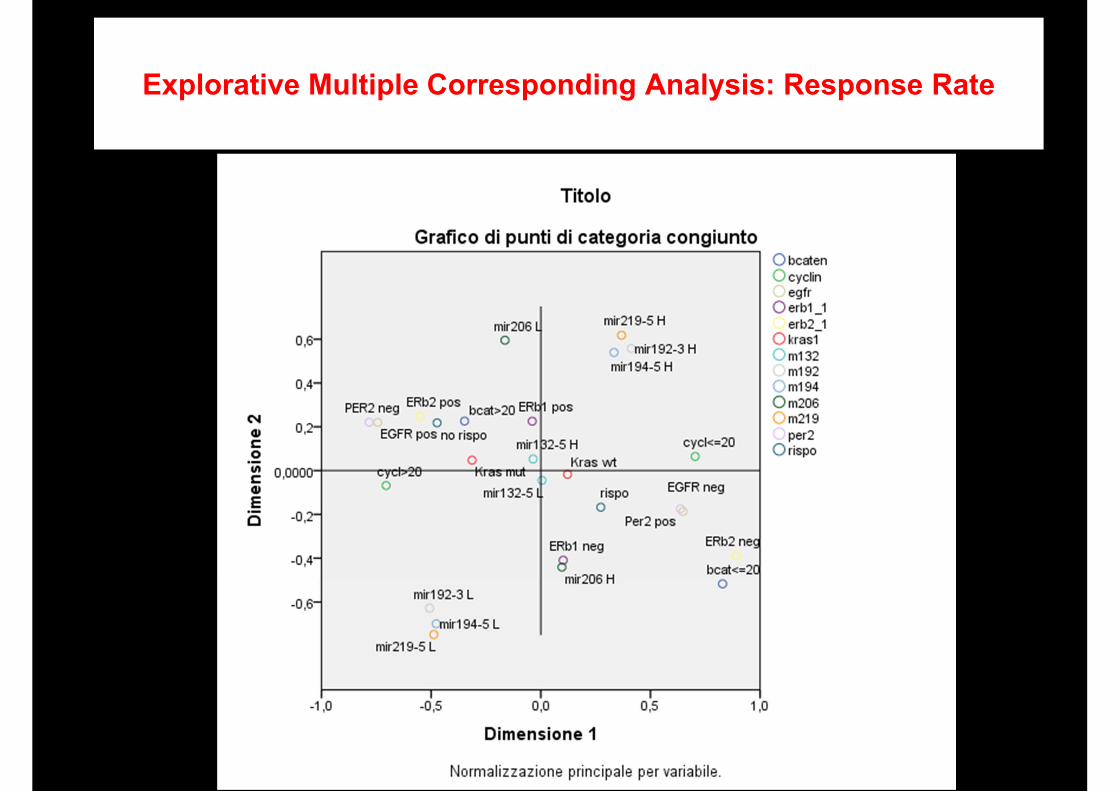
Explorative Multiple Corresponding Analysis: Response Rate
3
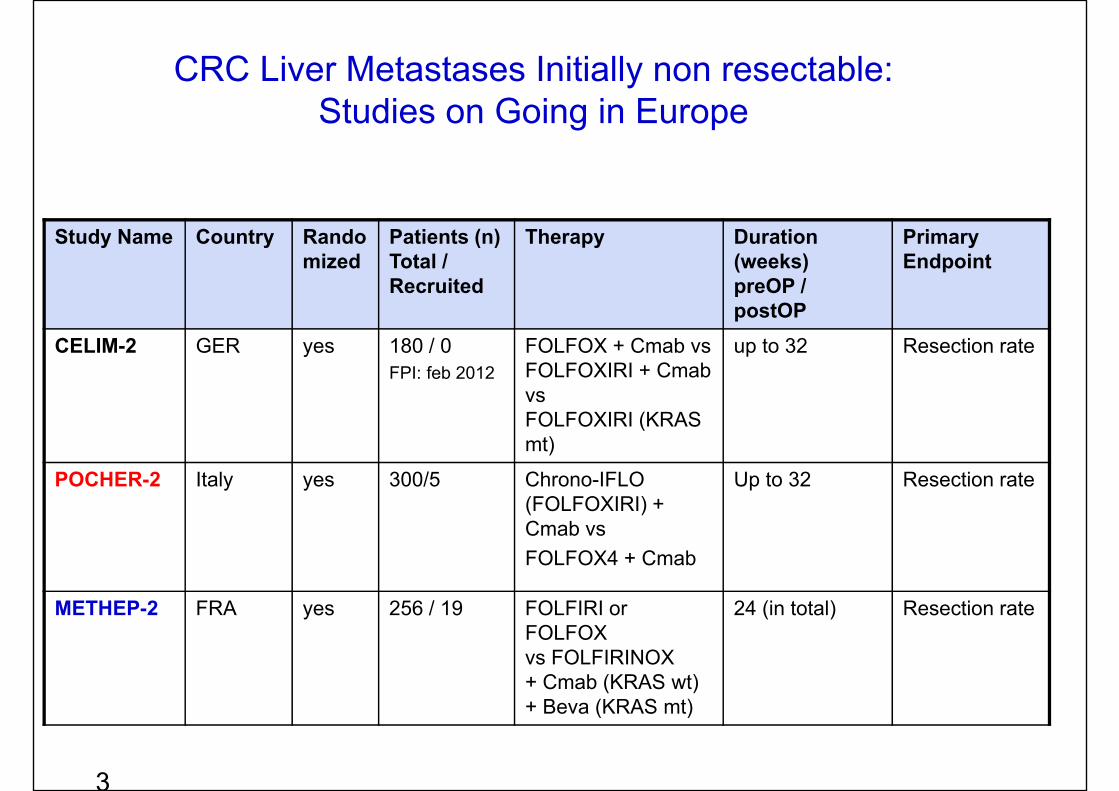
Study Name Country Randomized
Patients (n)Total / Recruited
Therapy Duration (weeks)preOP / postOP
Primary Endpoint
CELIM-2 GER yes 180 / 0FPI: feb 2012
FOLFOX + Cmab vsFOLFOXIRI + Cmab vsFOLFOXIRI (KRAS mt)
up to 32 Resection rate
POCHER-2 Italy yes 300/5 Chrono-IFLO (FOLFOXIRI) + Cmab vsFOLFOX4 + Cmab
Up to 32 Resection rate
METHEP-2 FRA yes 256 / 19 FOLFIRI orFOLFOXvs FOLFIRINOX+ Cmab (KRAS wt)+ Beva (KRAS mt)
24 (in total) Resection rate
CRC Liver Metastases Initially non resectable: Studies on Going in Europe