
CORSO RESIDENZIALE Inquadramento e strategie terapeutiche ...

1
INNOVAZIONI TERAPEUTICHE IN ONCOLOGIA MEDICACAGLIARI 23-24 GIUGNO 2005Policlinico Universitario - Cagliari
MULTI TARGETED ANTIFOLATE
Elena MassaCATTEDRA DI ONCOLOGIA MEDICA
UNIVERSITA’ DEGLI STUDI DI CAGLIARI

2
Chemical Structure of ALIMTA (pemetrexed disodium, LY231514)
N-[4-[2-(2-amino-3,4-dihydro-4-oxo-7H-pyrrolo[2,3-d]pyrimidin-5-yl)ethyl]benzoyl]-L-
glutamic acid ALIMTA
HO
Methotrexate
O
N
NNN
NH2
NH2
NN
O
OHOH
N
OHO
OHO
NHN
O N SO
H
LometrexolNHN N
O
NH2
N
OHO
OHO
O
H
H
NH
N N
O
NH2
N
OHO
OH
O
O
H
H
Raltitrexed
NHHN
NHN
NH
NHCOOH
COOH
O
O
NH2
TH-FA
Taylor et al., J Med Chem 35: 4450-4454, 1992

ALIMTA: Key Intracellular Enzyme TargetsALIMTA: Key Intracellular Enzyme Targets
55--FU, FU, RaltitrexedRaltitrexedALIMTA
MethotrexateMethotrexate
dUMPdUMP
1010--CHOCHO--THFTHF DHFDHF
GARGAR
fGARfGARAMP, GMPAMP, GMP
NADPHNADPH5,105,10--CH2CH2--THFTHF
GARFTGARFTGARFT DHFRDHFRDHFR
TSTSTS
dTMPdTMP DNADNA
PRPPPRPP
THFTHF NADP+NADP+
DNA, RNA DNA, RNA TS: thymidylate synthase DHFR: dihydrofolate reductaseGARFT: glycinamide ribonucleotide formyltransferase

4
ALIMTA ALIMTA vsvs Other AntimetabolitesOther Antimetabolites
PURINE SYNTHESISPURINE SYNTHESISPYRIMYDINE SYNTHESISPYRIMYDINE SYNTHESIS
DNA, RNA biosynthesisDNA, RNA biosynthesis
like 5- FU/Leucovorin like Raltitrexedlike 5- FU/Leucovorin like Raltitrexed like Methotrexatelike Methotrexate unlike any other
marketed drugunlike any other marketed drug
ALIMTA inhibits
ALIMTA inhibits
ALIMTA inhibits
DNADNA
TSTS GARFTGARFTDHFRDHFRALIMTA inhibits
ALIMTA inhibits
ALIMTA inhibits
ALIMTA inhibits
5
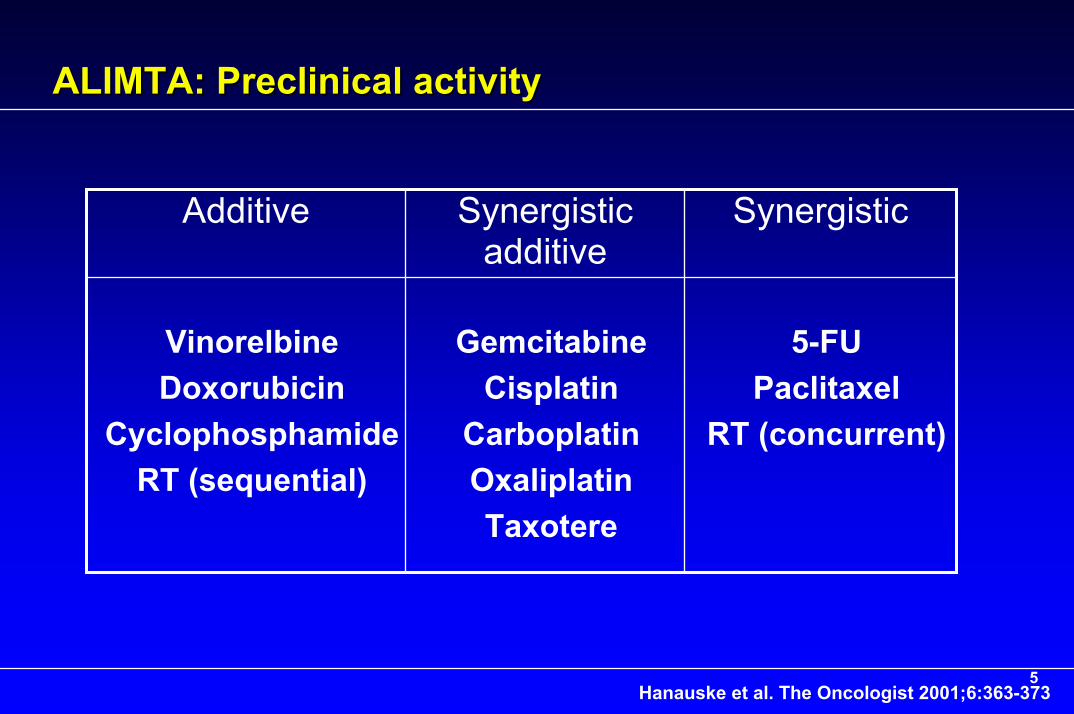
ALIMTA: Preclinical activityALIMTA: Preclinical activity
5-FUPaclitaxel
RT (concurrent)
GemcitabineCisplatin
CarboplatinOxaliplatinTaxotere
VinorelbineDoxorubicin
CyclophosphamideRT (sequential)
SynergisticSynergistic additive
Additive
Hanauske et al. The Oncologist 2001;6:363-373
6
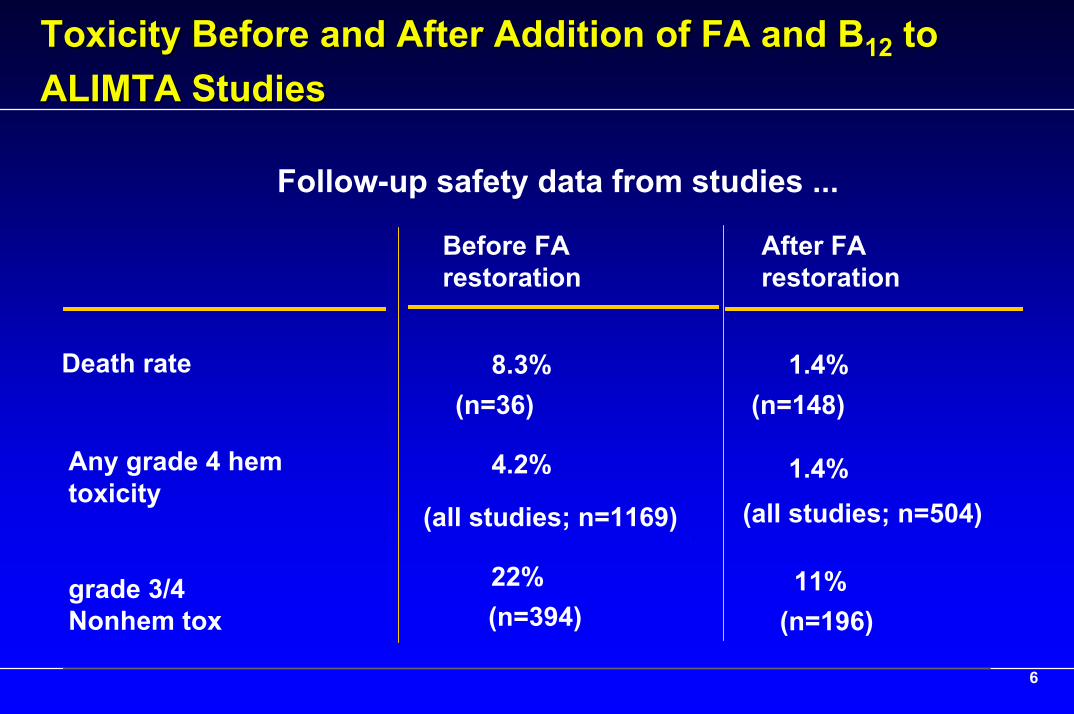
Toxicity Before and After Addition of FA and BToxicity Before and After Addition of FA and B1212 to to ALIMTA StudiesALIMTA Studies
Death rate
(all studies; n=1169)
1.4%(all studies; n=504)
Any grade 4 hemtoxicity
grade 3/4Nonhem tox
22%(n=394)
11%(n=196)
Follow-up safety data from studies ...
Before FArestoration
After FA restoration
8.3% 1.4%(n=36) (n=148)
4.2%
7
Folic Acid/Vitamin BFolic Acid/Vitamin B12 12 Supplementation RationaleSupplementation Rationale
• Folic acid is a supplement in cereal products in the US to reduce the incidence of neural tube defects.
• Plasma homocysteine concentration is a sensitive marker of folate and vitamin B12 status.
• Plasma homocysteine concentrations are associated with an increased risk of coronary artery disease and cerebral vascular mortality.
• Folic acid supplementation reduces toxicity without affecting efficacy in patients receiving low-dose methotrexate for rheumatoid arthritis and with B12/B6, reduces the rate of coronary restenosis .

8
Vitamin Supplementation InterventionVitamin Supplementation Intervention
Folic Acid: 350 - 1000 µg orally daily beginning 1-2 weeks prior to first dose of ALIMTA and continuing while the patient remains on study
Vitamin B12: 1000 µg im prior to the first dose of ALIMTA and repeated every 3 cycles while the patient remains on study
Bunn, et al. Proc Amer Soc Clin Oncol 76a: (abstr 300) 2001

9
ALIMTA SAFETY SUMMARYALIMTA SAFETY SUMMARY• Folic acid and vitamin B12 supplementation results in a dramatic reduction
in drug-related death.
• Folic acid and vitamin B12 supplementation significantly reduces the number of episodes of grade 4 hematologic or grade 3/4 nonhematologic toxicity associated with ALIMTA.
• The improved safety profile of ALIMTA may be attributed to the decrease in Hcys levels achieved through folic acid and vitamin B12supplementation.
• While folic acid and vitamin B12 supplementation has significantly reduced Hcy levels in all patients, the effect appears to be more pronounced in patients whose baseline Hcys ≥12 µmol.
• Patients with baseline Hcys ≤12 µmol benefit more from the FA and vitamin B12 supplementation.
Bunn P, et al. Proceedings of ASCO 2001: 76a:A300
10
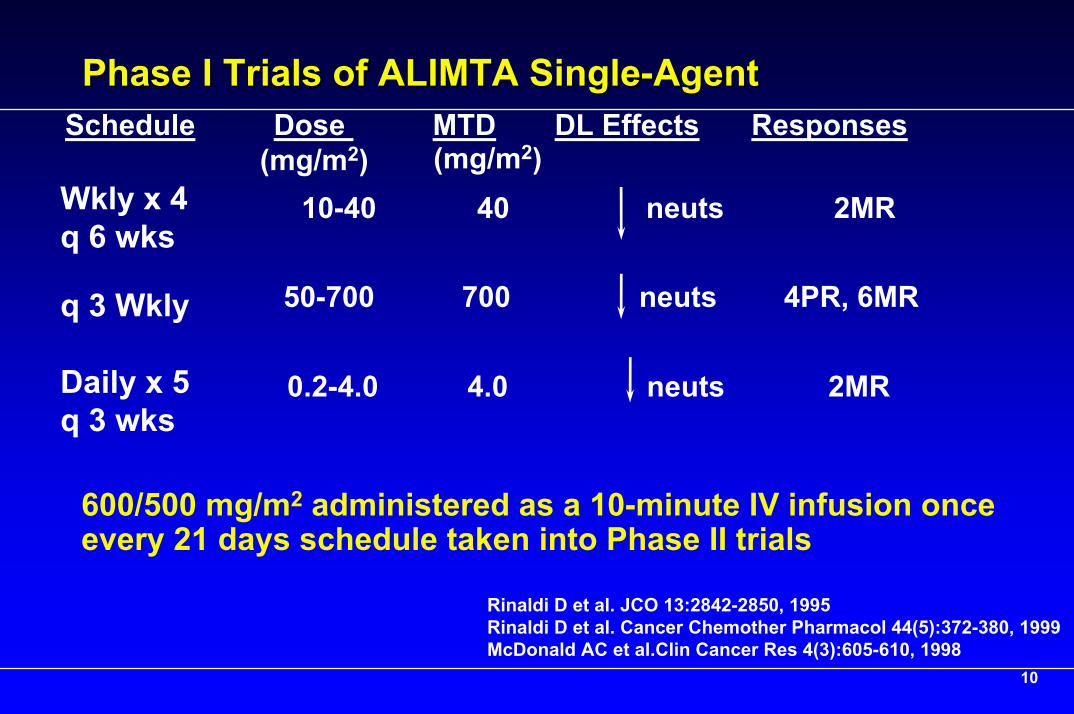
Phase I Trials of ALIMTA SinglePhase I Trials of ALIMTA Single--AgentAgentSchedule Dose MTD DL Effects Responses
(mg/m2)Wkly x 4 q 6 wks
q 3 Wkly
Daily x 5q 3 wks
10-40 40 neuts 2MR
50-700 700 neuts 4PR, 6MR
0.2-4.0 4.0 neuts 2MR
(mg/m2)
600/500 mg/m2 administered as a 10-minute IV infusion once every 21 days schedule taken into Phase II trials
Rinaldi D et al. JCO 13:2842-2850, 1995Rinaldi D et al. Cancer Chemother Pharmacol 44(5):372-380, 1999 McDonald AC et al.Clin Cancer Res 4(3):605-610, 1998
11
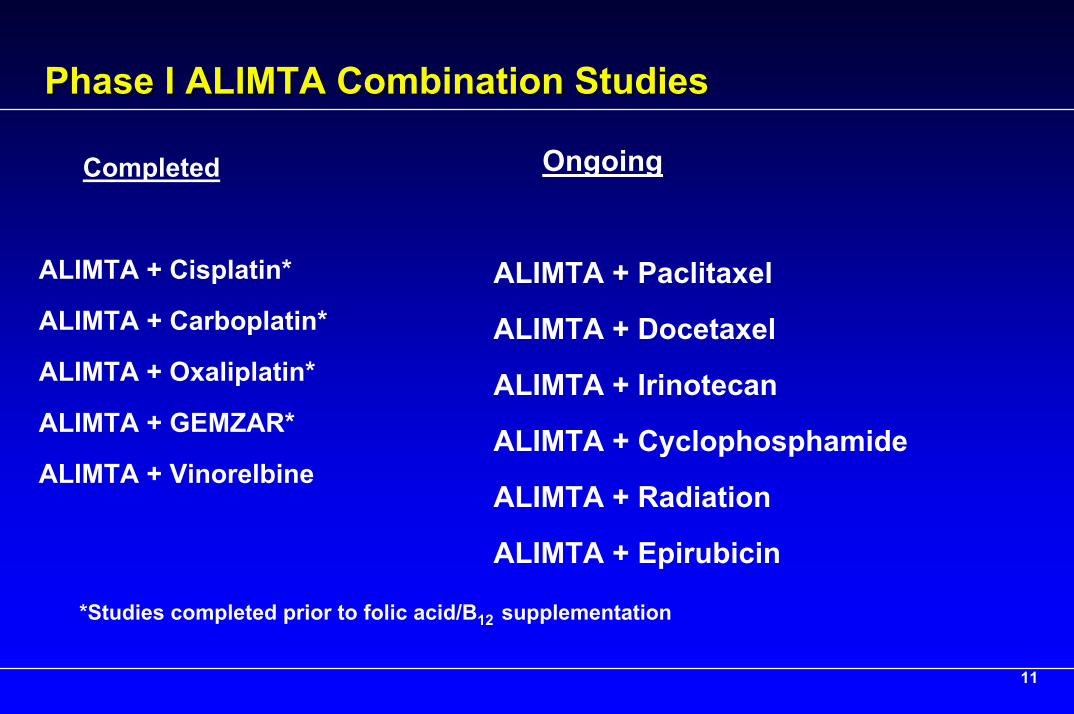
Phase I ALIMTA Combination StudiesPhase I ALIMTA Combination Studies
Completed Ongoing
ALIMTA + Paclitaxel
ALIMTA + Docetaxel
ALIMTA + Irinotecan
ALIMTA + Cyclophosphamide
ALIMTA + Radiation
ALIMTA + Epirubicin
*Studies completed prior to folic acid/B12 supplementation
ALIMTA + Cisplatin*
ALIMTA + Carboplatin*
ALIMTA + Oxaliplatin*
ALIMTA + GEMZAR*
ALIMTA + Vinorelbine
ALIMTA®
ACTIVITY IN PLEURAL MESOTHELIOMA
13
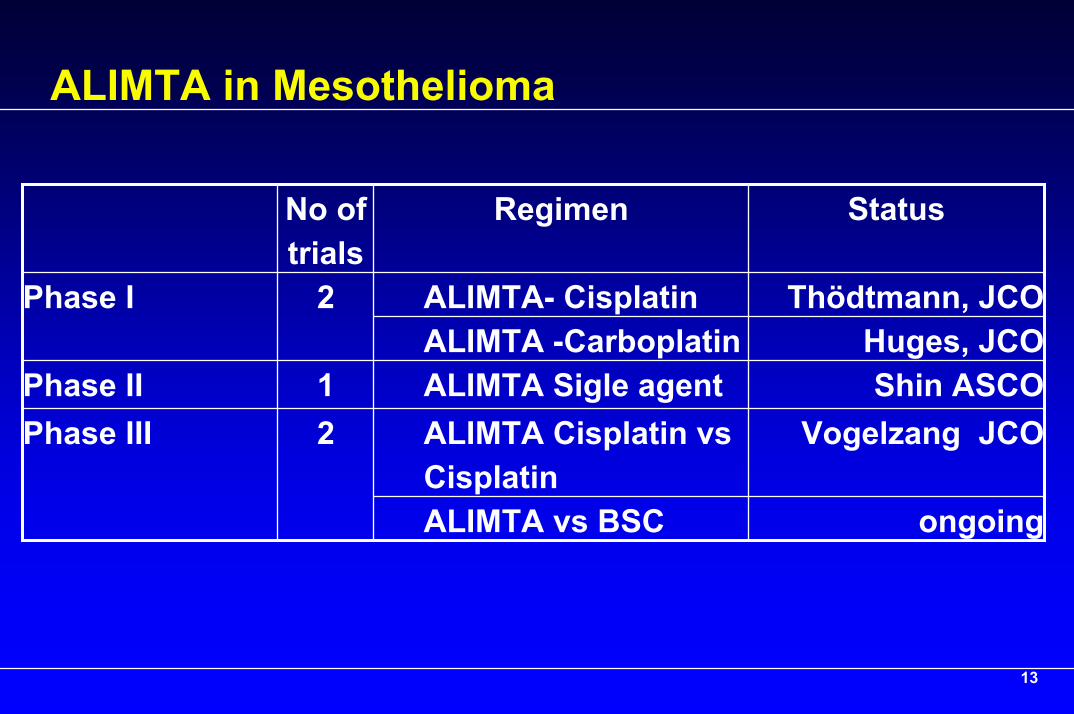
ALIMTA in Mesothelioma
ALIMTA vs BSC
ALIMTA Cisplatin vsCisplatin
ALIMTA Sigle agentALIMTA -CarboplatinALIMTA- Cisplatin
Regimen
ongoing
Vogelzang JCO2Phase IIIShin ASCO1Phase II
Huges, JCOThödtmann, JCO2Phase I
StatusNo of trials
14
Phase III, SinglePhase III, Single--Blinded Trial ofBlinded Trial of
ALIMTAALIMTA® ® ((pemetrexedpemetrexed) and ) and CisplatinCisplatinversusversus
CisplatinCisplatin AloneAlone
in in ChemonaiveChemonaive Patients with MalignantPatients with MalignantPleural Pleural MesotheliomaMesothelioma
Nicholas Vogelzang, et al. J Clin Oncol 2003; 21:2636–44
15
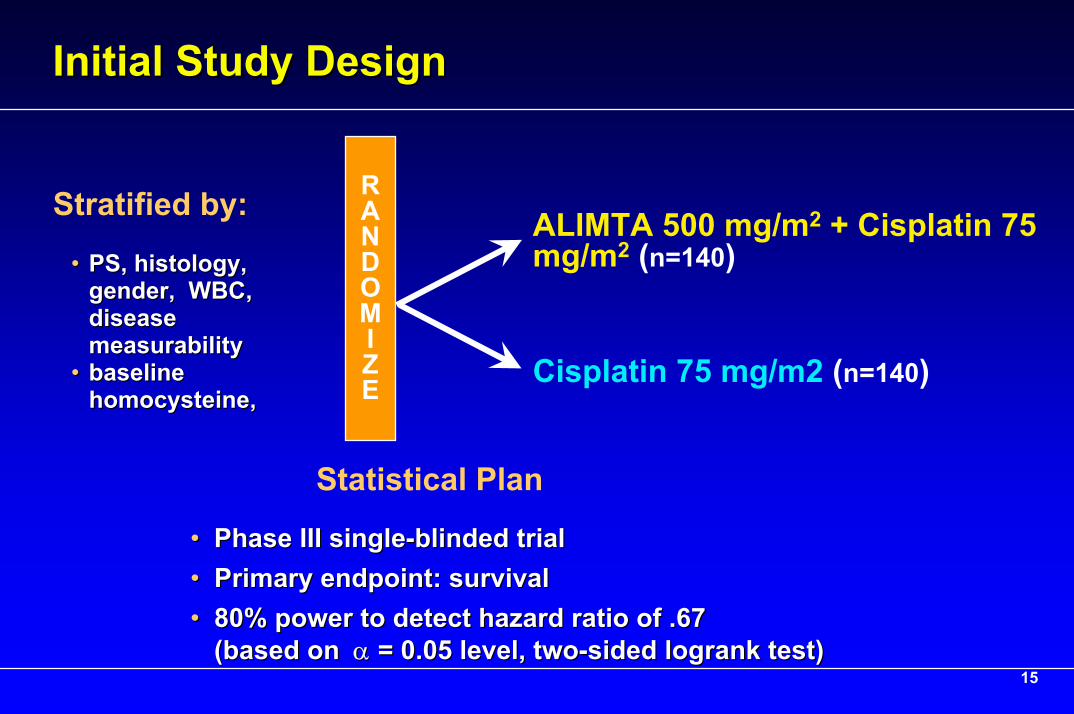
Initial Study DesignInitial Study Design
ALIMTA 500 mg/m2 + Cisplatin 75 mg/m2 (n=140)
Statistical Plan
•• Phase III singlePhase III single--blinded trialblinded trial•• Primary endpoint: survivalPrimary endpoint: survival•• 80% power to detect hazard ratio of .6780% power to detect hazard ratio of .67
(based on (based on α α = 0.05 level, two= 0.05 level, two--sided sided logranklogrank test)test)
RANDOMIZE
Stratified by:
•• PS, histology, PS, histology, gender, WBC, gender, WBC, disease disease measurabilitymeasurability
•• baseline baseline homocysteinehomocysteine,
Cisplatin 75 mg/m2 (n=140),
16
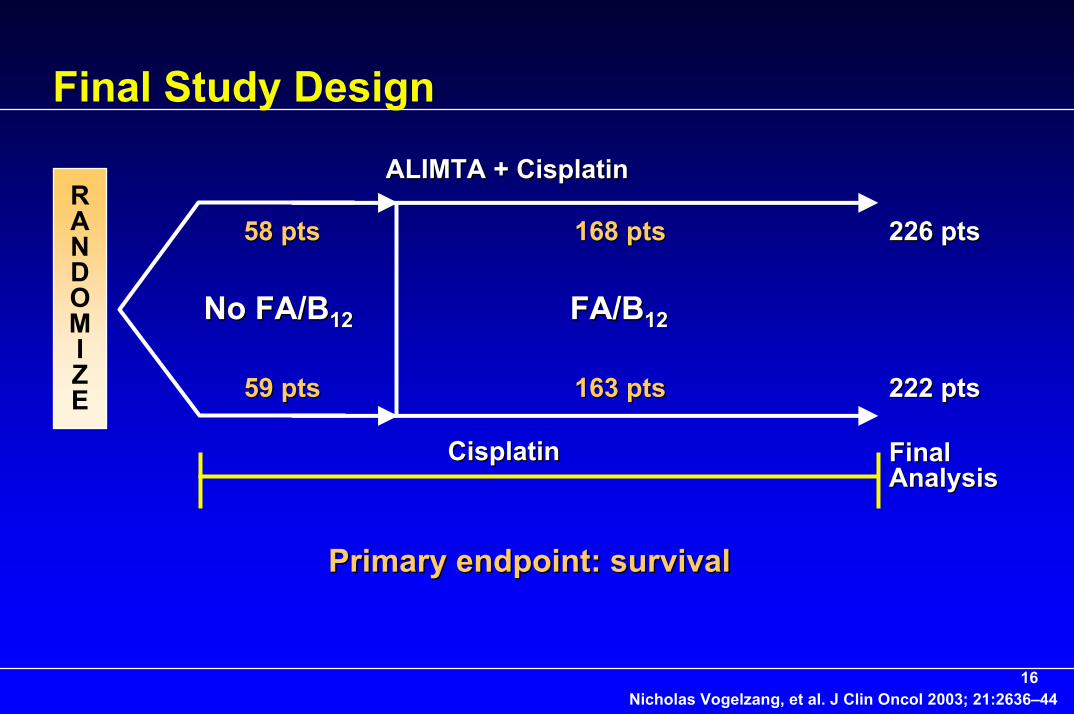
Final Study Design
ALIMTA + Cisplatin
Primary endpoint: survivalPrimary endpoint: survival
FinalFinalAnalysisAnalysis
58 pts58 pts
59 pts59 pts
No FA/BNo FA/B1212
CisplatinCisplatin
168 pts168 pts
163 pts163 pts
FA/BFA/B1212
ALIMTA + CisplatinRANDOMIZE
226 pts226 pts
222 pts222 pts
Nicholas Vogelzang, et al. J Clin Oncol 2003; 21:2636–44
17
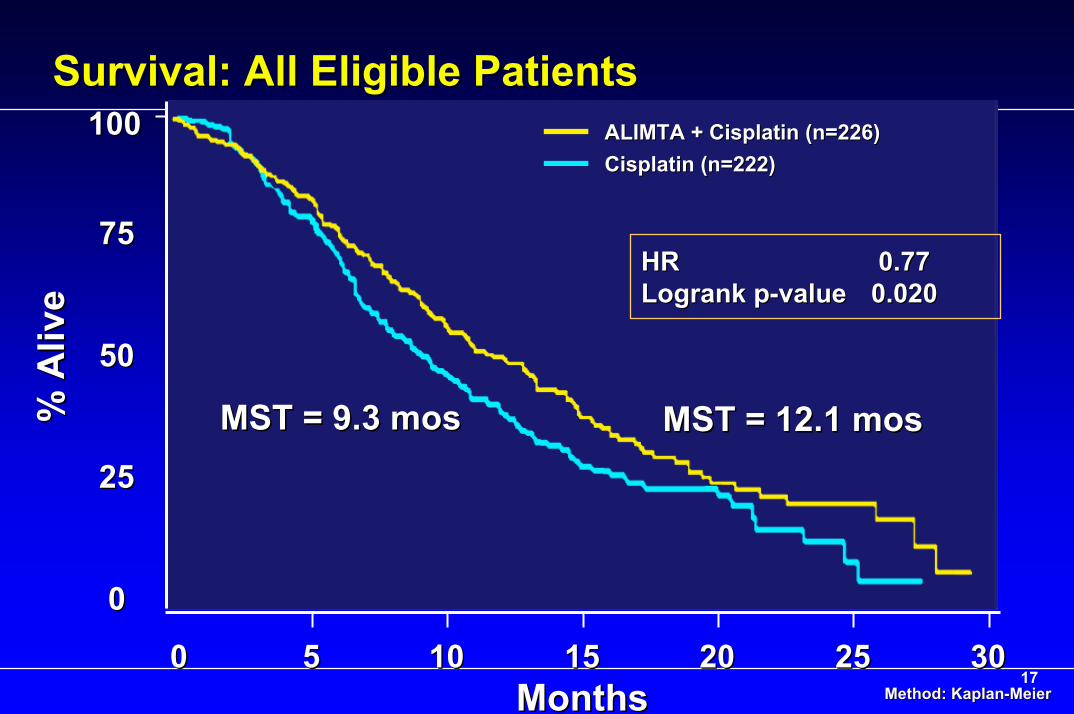
MST = 12.1 MST = 12.1 mosmos
HRHR 0.770.77LogrankLogrank pp--valuevalue 0.0200.020
MST = 9.3 MST = 9.3 mosmos
ALIMTA + ALIMTA + CisplatinCisplatin (n=226)(n=226)CisplatinCisplatin (n=222)(n=222)
00 55 1010 1515 2020 2525 3030
100100Survival: All Eligible PatientsSurvival: All Eligible Patients
7575
5050
2525
00
% A
live
% A
live
MonthsMonths Method: KaplanMethod: Kaplan--MeierMeier

18
Survival: Fully Supplemented PatientsSurvival: Fully Supplemented Patients
MST = 13.3 MST = 13.3 mosmosMST = 10.0 MST = 10.0 mosmos
HRHR 0.750.75LogrankLogrank pp--valuevalue 0.0510.051
ALIMTA + ALIMTA + CisplatinCisplatin (n=168)(n=168)CisplatinCisplatin (n=163)(n=163)
100
% A
live
% A
live
5050
2525
00
100
7575
00 55 1010 1515 2020 2525 3030MonthsMonths
19
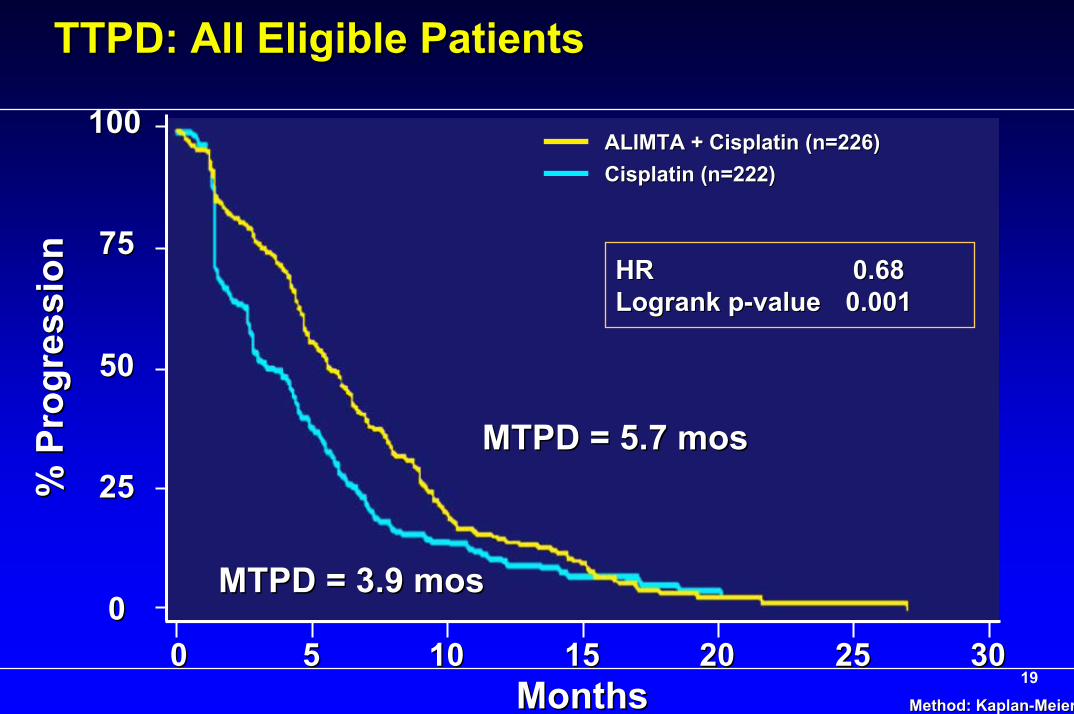
TTPD: All Eligible PatientsTTPD: All Eligible Patients
Method: KaplanMethod: Kaplan--MeierMeier
% P
rogr
essi
on%
Pro
gres
sion
00 55 1010 1515 2020 2525 3030
100100
7575
5050
2525
00
MonthsMonths
MTPD = 5.7 MTPD = 5.7 mosmos
MTPD = 3.9 MTPD = 3.9 mosmos
HRHR 0.680.68LogrankLogrank pp--valuevalue 0.0010.001
ALIMTA + ALIMTA + CisplatinCisplatin (n=226)(n=226)CisplatinCisplatin (n=222)(n=222)

20
TTPD: Fully Supplemented PatientsTTPD: Fully Supplemented Patients%
Pro
gres
sion
0 5 10 15 20 25
100
75
50
25
0
Months
MTPD = 6.1 mos
MTPD = 3.9 mos
HR 0.64Logrank p-value 0.008
ALIMTA + Cisplatin (n=168)Cisplatin (n=163)
21
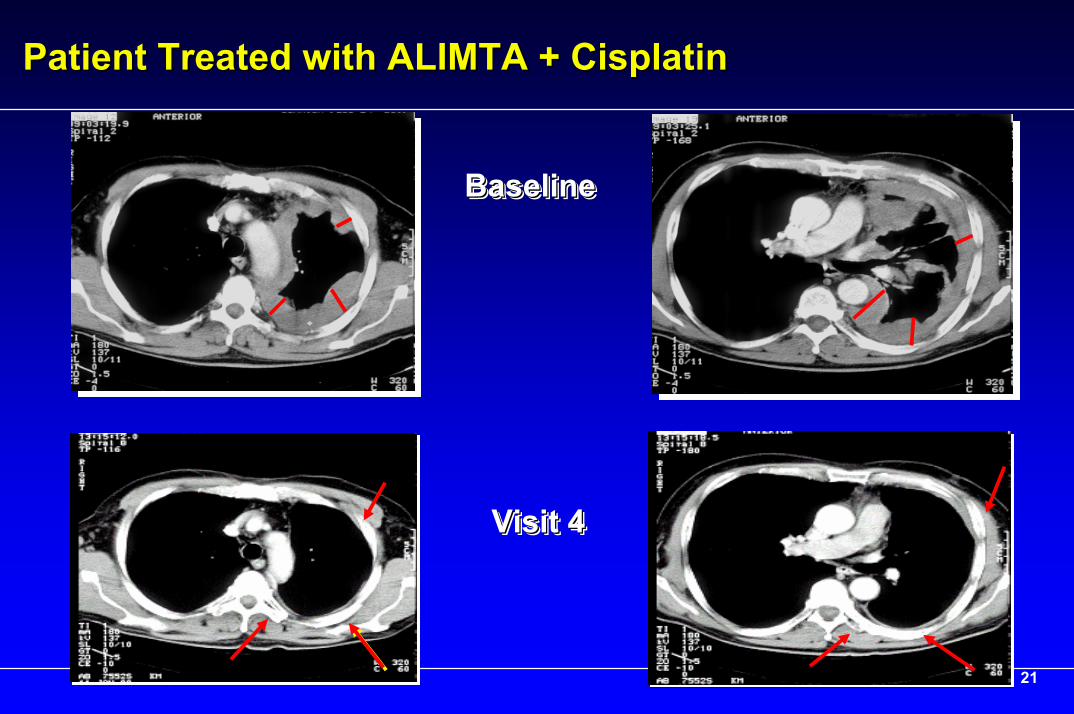
Patient Treated with ALIMTA + Patient Treated with ALIMTA + CisplatinCisplatin
BaselineBaselineBaseline
Visit 4Visit 4Visit 4

22
Tumor Response Rates Tumor Response Rates
50
40
30
20
10
0n=225 n=222
41
17
n=167 n=163
46
20
n=58 n=59
29
8
p <0.001 ALIMTA/Cisp <0.001%
Cis(CI 38-53)
(CI 35-48)p =0.005
(CI 18-43)
(CI 14-27)(CI 12-22)
(CI 3-19)
Partially and no FA/B12FA/B12All Eligible
23
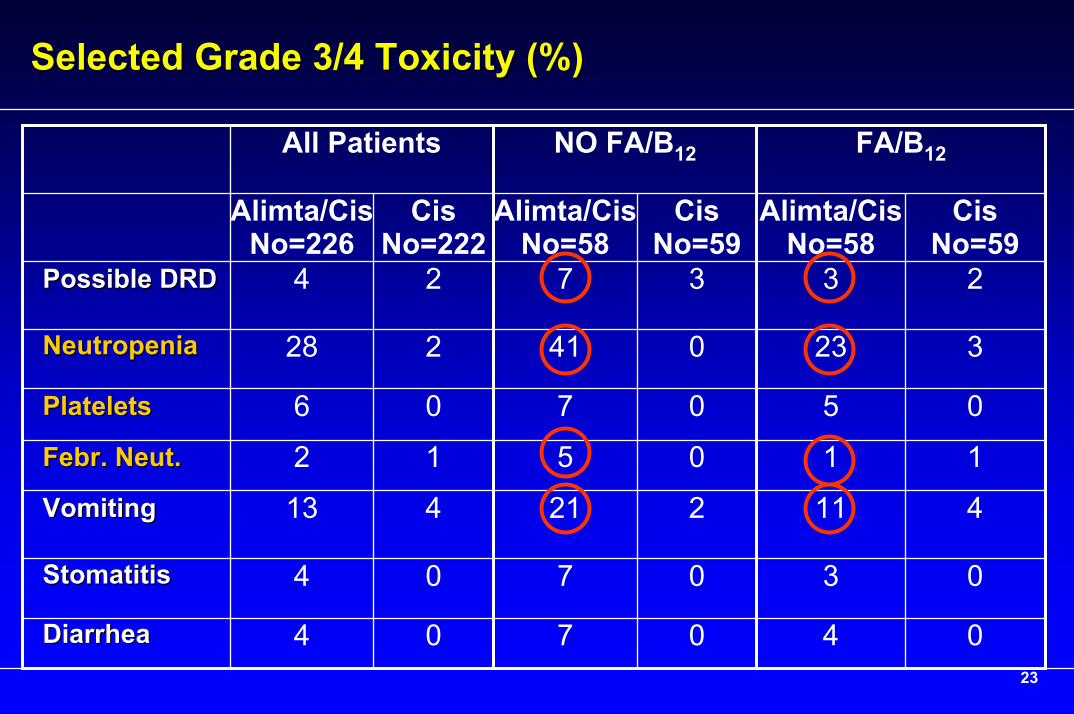
SSelected Grade 3/4 Toxicity (%) elected Grade 3/4 Toxicity (%)
All Patients
4
4
13
2
6
28
4
Alimta/CisNo=226 No=222
Cis
2NeutropeniaNeutropenia
0DiarrheaDiarrhea
0StomatitisStomatitis
4VomitingVomiting
1FebrFebr. . NeutNeut..
0PlateletsPlatelets
2Possible DRD
Alimta/Cis
Possible DRD
NO FA/B12
7
7
21
5
7
41
7No=58
CisNo=59
0
0
0
2
0
0
3
FA/B12
4
3
11
1
5
23
3
Alimta/CisNo=58
CisNo=59
3
0
0
4
1
0
2

24
Lung Function (Vital Capacity) by Treatment ArmLung Function (Vital Capacity) by Treatment Arm
p =0.324
p =0.034ALIMTA/Cis
Cis
p =0.002p =0.002
CycleCycle
VC (L
)
2.55
2.70
2.65
2.60
2.50
2.45
2.400 2 64

25
40
35
30
25
mm
Lung Cancer Symptom Scale: Lung Cancer Symptom Scale: DyspneaDyspnea
p =0.004
p =0.344p =0.476
ALIMTA/Cis
Cis
Worse
Better
Cycle0 2 4 6
26
Conclusions (1)Conclusions (1)
ALIMTA and cisplatin significantly improved survival compared to cisplatin alone
ALIMTA and cisplatin also significantly improved:
• Time to progressive disease• Tumor response rate • Lung function • Subjective indicators of quality of life
27
Conclusions (2)Conclusions (2)
Following the sequential, non-random addition of folic acid and B12:
• The improved efficacy of ALIMTA and cisplatin over cisplatin was maintained
• There was strong evidence of reduction in toxicity (including drug related deaths)
• Improved efficacy in FA/B12 – supplemented patients may be due to the higher median number of cycles delivered
28
Conclusions (3)Conclusions (3)
ALIMTA and cisplatin with FA/B12
should now be consideredstandard front-line therapy for patients with
malignant pleural mesothelioma

29
ALIMTA in NSCLCSingle Agent Studies
Two trials in previously untreated patients
Rusthoven et al, (NCIC), J Clin Oncol, 1999Clarke et al, (S.Africa/Australia), Ann Oncol 9:86, 1998
One trial in patients with one previous CT regimen
Postmus et al, Eur J Cancer, 35:249, 1999
No vitamin supplementation administered in these studiesNo vitamin supplementation administered in these studies
30
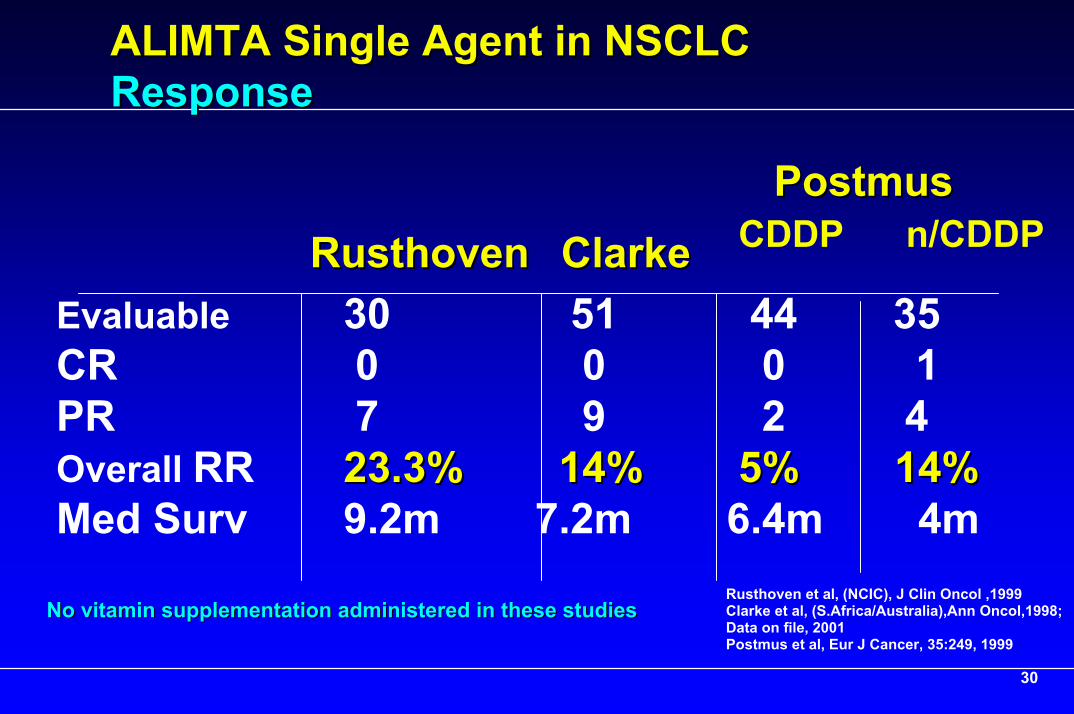
ALIMTA Single AgentALIMTA Single Agent in NSCLCin NSCLCResponseResponse
PostmusPostmusCDDP n/CDDP
Evaluable 30 51 44 35CR 0 0 0 1PR 7 9 2 4Overall RR 23.3%23.3% 14%14% 5% 14%5% 14%Med Surv 9.2m 7.2m 6.4m 4m
ClarkeClarkeRusthovenRusthoven
Rusthoven et al, (NCIC), J Clin Oncol ,1999Clarke et al, (S.Africa/Australia),Ann Oncol,1998; Data on file, 2001Postmus et al, Eur J Cancer, 35:249, 1999
No vitamin supplementation administered in these studiesNo vitamin supplementation administered in these studies
31
Phase II ALIMTA in NSCLCCombination Studies with Cisplatin
Two Phase II combination trials in untreated NSCLC
Shepherd et al, Cancer, 92(3):595-600, 2001Manegold et al, Ann Oncol, 11(4):435, 2000
No vitamin supplementation administered in these studiesNo vitamin supplementation administered in these studies
32
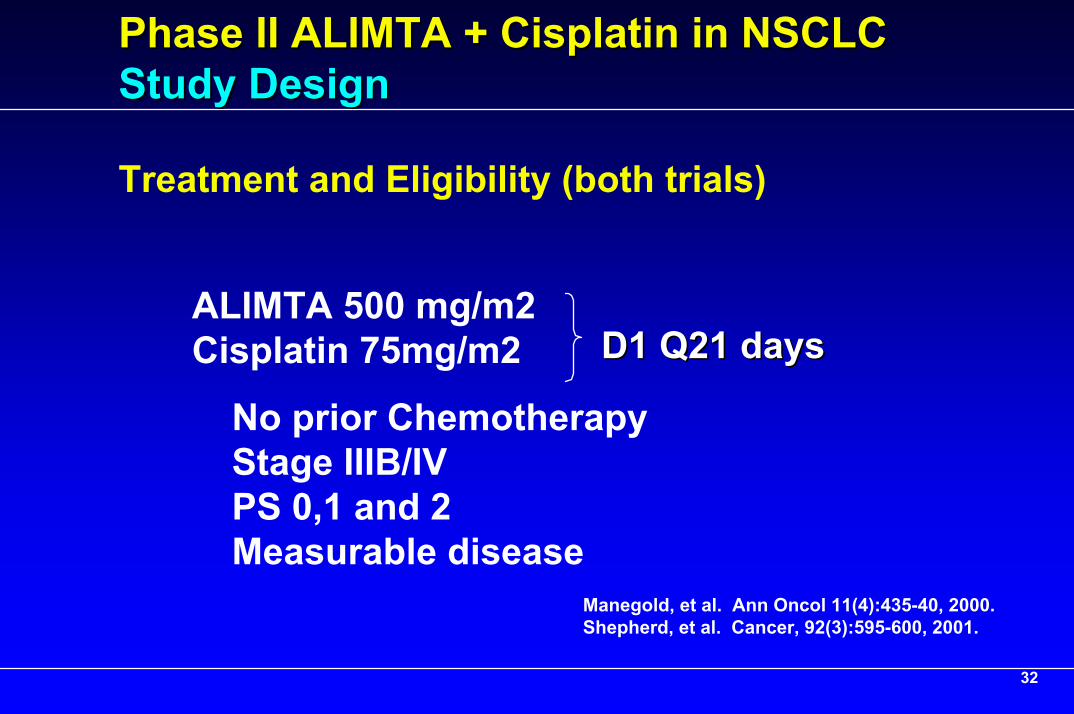
Phase II ALIMTA + Cisplatin in NSCLCPhase II ALIMTA + Cisplatin in NSCLCStudy DesignStudy Design
Treatment and Eligibility (both trials)
ALIMTA 500 mg/m2Cisplatin 75mg/m2 D1 Q21 daysD1 Q21 days
No prior ChemotherapyStage IIIB/IVPS 0,1 and 2Measurable disease
Manegold, et al. Ann Oncol 11(4):435-40, 2000. Shepherd, et al. Cancer, 92(3):595-600, 2001.

33
Phase II ALIMTA + Cisplatin in NSCLCPhase II ALIMTA + Cisplatin in NSCLCResultsResults
Shepherd ManegoldN° Evaluable 29 36PR 13 14SD 11 17RR 44.8% 38.9%Med Surv 8.9 mo 10.9 mo1-year Surv 49% 50%
No vitamin supplementatNo vitamin supplementation administered in these studieson administered in these studies
Shepherd, et al. Cancer, 92(3):595-600, 2001.Manegold, et al. Ann Oncol 11(4):435-40, 2000.

Randomized Phase III Trial of Randomized Phase III Trial of ALIMTA (ALIMTA (PemetrexedPemetrexed) vs. ) vs. DocetaxelDocetaxel inin
Patients with Locally Advanced or Patients with Locally Advanced or MetastaticMetastaticNSCLC Previously Treated with ChemotherapyNSCLC Previously Treated with Chemotherapy
Nasser Hanna, Frances Shepherd, Rafael Rosell, Jose Pereira, Filippo DeMarinis, Frank Fossella,
Louis Kayitalire, Sofia Paul, Lawrence Einhorn, Paul Bunn
HannaHanna N N etet al JCO 22:1589al JCO 22:1589--1597, 20041597, 2004

35
BackgroundBackground
Lung cancer is the leading cause of cancer-related death worldwide
1st-line chemotherapy offers a modest survival advantage over best supportive care (BSC)
Phase III studies have demonstrated docetaxelimproves 1 year survival by ~10-15% compared to BSC, ifosfamide or vinorelbine in the 2nd-line setting1,2
ALIMTA, a novel multi-targeted antifolate, shows activity as a single-agent in 1st-line and 2nd-line NSCLC
1 Fossella et. al., JCO 18(12):2354-2362, 20002 Shepherd et al., JCO 18(10):2095-2103, 2000
36
A Phase III Study of ALIMTA vs. A Phase III Study of ALIMTA vs. DocetaxelDocetaxel in in 22ndnd--line NSCLCline NSCLC
Primary Endpoint • Survival
Secondary Endpoints• Tumor Response Rate• Progression-free Survival• Toxicity
HannaHanna N N etet al JCO 22:1589al JCO 22:1589--1597, 20041597, 2004
37
Inclusion/Exclusion CriteriaInclusion/Exclusion CriteriaInclusion
• Histological/cytological NSCLC • Stage III or IV NSCLC• Previously treated with only 1 regimen for metastatic disease• ECOG PS 0-2• Adequate end organ function
Exclusion• Symptomatic brain metastasis• Grade 3 or 4 peripheral neuropathy• Weight loss > 10% over previous 6 weeks• Uncontrolled pleural effusions

38
ALIMTA vs. ALIMTA vs. DocetaxelDocetaxel in 2in 2ndnd--line NSCLCline NSCLC
ALIMTA 500 mg/m2 i.v. q3wks (n=283)(folic acid 350-1,000 µg daily + vitamin B12 1,000 µg q 9wks; dexamethasone 4mg bid on d-1,d0,d+1)
Stratified by:
• ECOG PS 0/1 vs. 2• Stage III vs. IV• # of prior chemo• Best response to prior
chemo• Time since last chemo • Prior platinum• Prior taxane• Homocysteine level • Center
Docetaxel75 mg/m2 i.v. q3wks (n=288)(dexamethasone 8 mg bid on d-1,d0,d+1)
RANDOMIZED
39
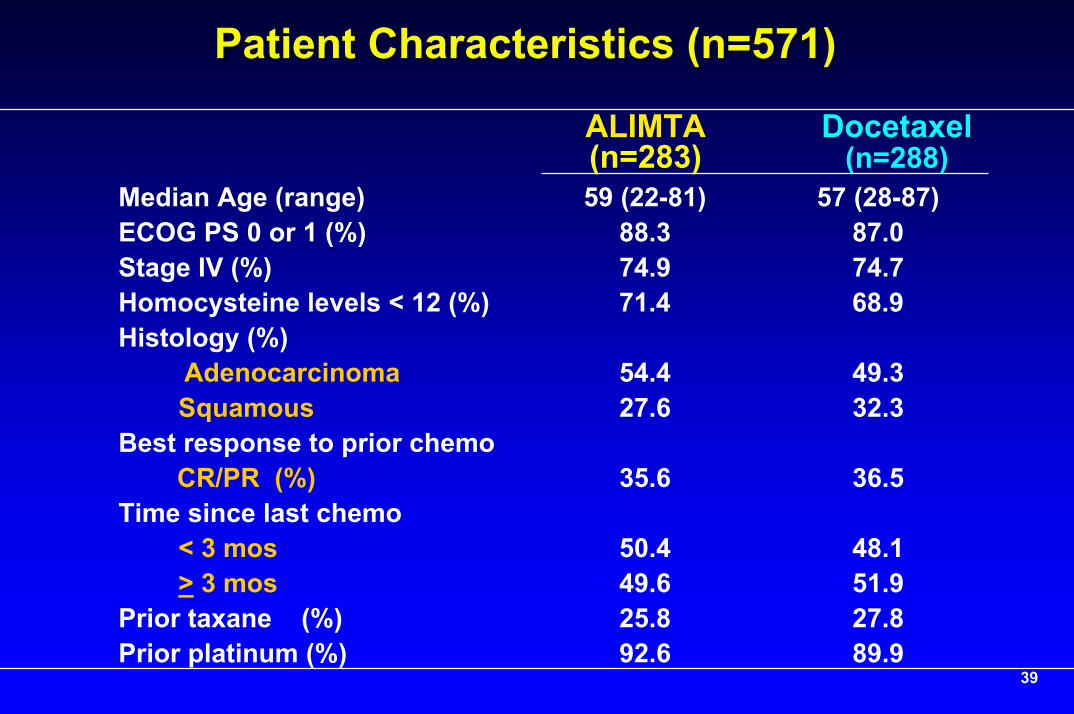
Patient Characteristics (n=571) Patient Characteristics (n=571)
ALIMTA Docetaxel(n=283) (n=288)
Median Age (range) 59 (22-81) 57 (28-87)ECOG PS 0 or 1 (%) 88.3 87.0Stage IV (%) 74.9 74.7Homocysteine levels < 12 (%) 71.4 68.9Histology (%)
Adenocarcinoma 54.4 49.3Squamous 27.6 32.3
Best response to prior chemoCR/PR (%) 35.6 36.5
Time since last chemo< 3 mos 50.4 48.1> 3 mos 49.6 51.9
Prior taxane (%) 25.8 27.8 Prior platinum (%) 92.6 89.9
40
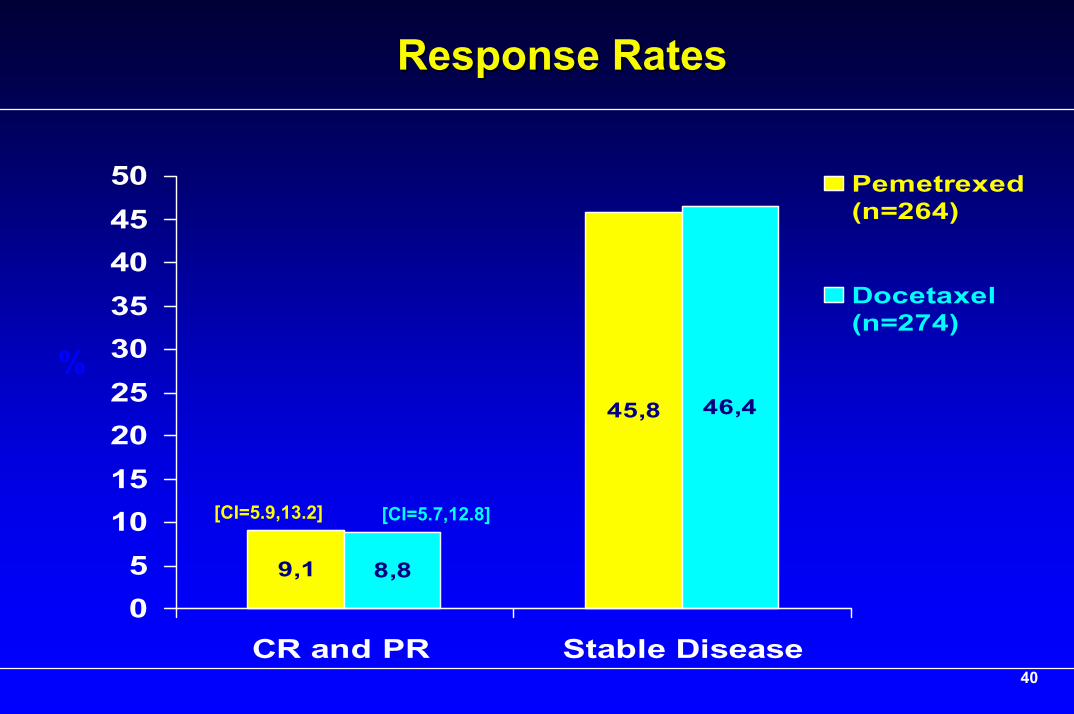
Response RatesResponse Rates
46,445,8
9,1 8,8
05
101520253035404550
CR and PR Stable Disease
Pemetrexed(n=264)
Docetaxel(n=274)
%
[CI=5.9,13.2] [CI=5.7,12.8]
41
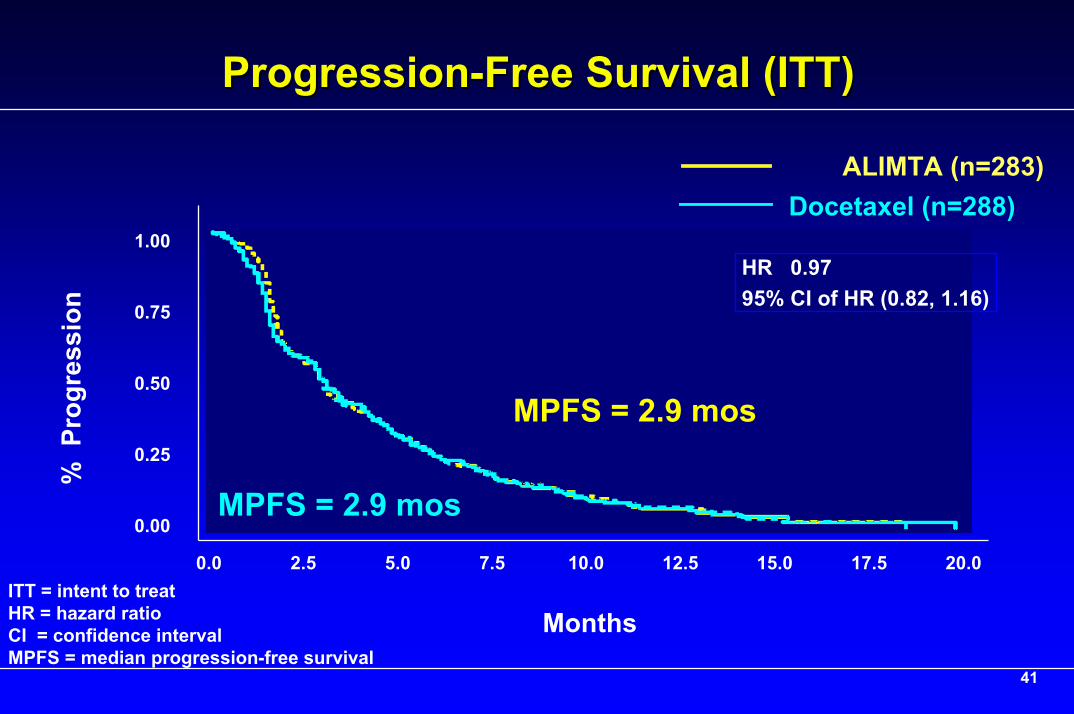
ProgressionProgression--Free Survival (ITT)Free Survival (ITT)
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Months
ALIMTA (n=283)Docetaxel (n=288)
% P
rogr
essi
on
MPFS = 2.9 mos
MPFS = 2.9 mos
ITT = intent to treatHR = hazard ratioCI = confidence intervalMPFS = median progression-free survival
HR 0.9795% CI of HR (0.82, 1.16)
42
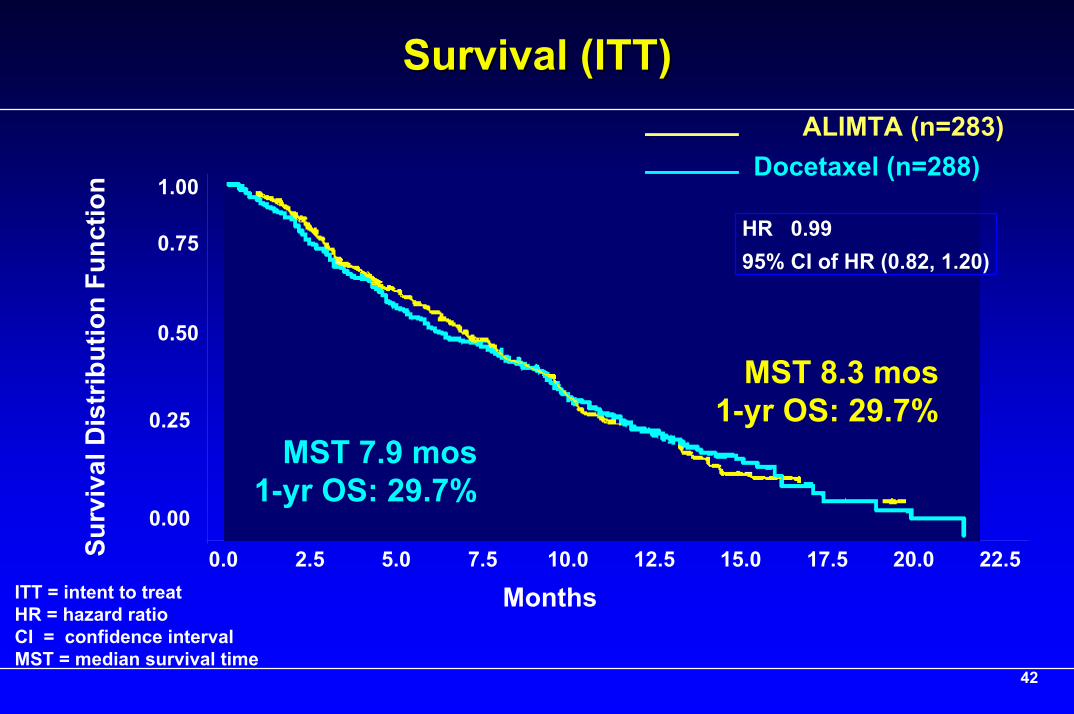
Survival (ITT)Survival (ITT)ALIMTA (n=283)
Docetaxel (n=288)
Surv
ival
Dis
trib
utio
n Fu
nctio
n
MonthsITT = intent to treatHR = hazard ratioCI = confidence intervalMST = median survival time
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0 22.5
MST 8.3 mos1-yr OS: 29.7%
HR 0.9995% CI of HR (0.82, 1.20)
MST 7.9 mos1-yr OS: 29.7%
43
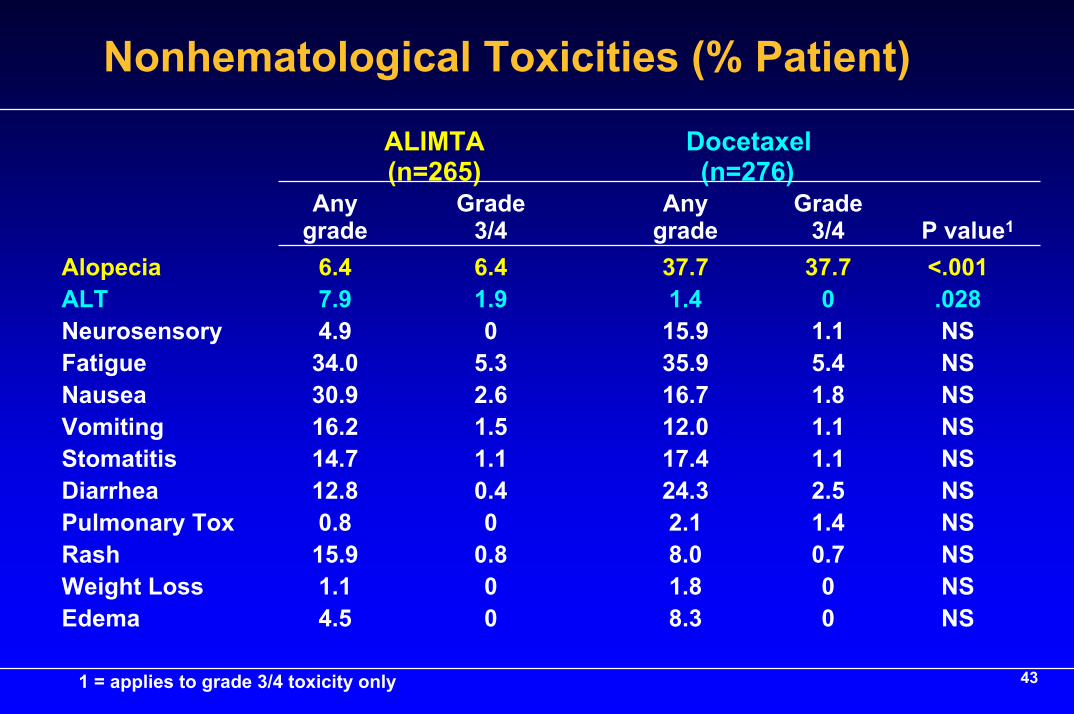
Nonhematological Toxicities (% Patient)
NS1.115.904.9Neurosensory
NS2.524.30.412.8DiarrheaNS1.117.41.114.7Stomatitis
.02801.41.97.9ALT<.00137.737.76.46.4Alopecia
NS08.304.5EdemaNS01.801.1Weight Loss
RashPulmonary Tox
NS0.78.00.815.9NS1.42.100.8
NS1.112.01.516.2VomitingNS1.816.72.630.9Nausea
Fatigue NS5.435.95.334.0
P value1Grade
3/4Any
gradeGrade
3/4
ALIMTA (n=265)
Docetaxel(n=276)
Any grade
1 = applies to grade 3/4 toxicity only
44
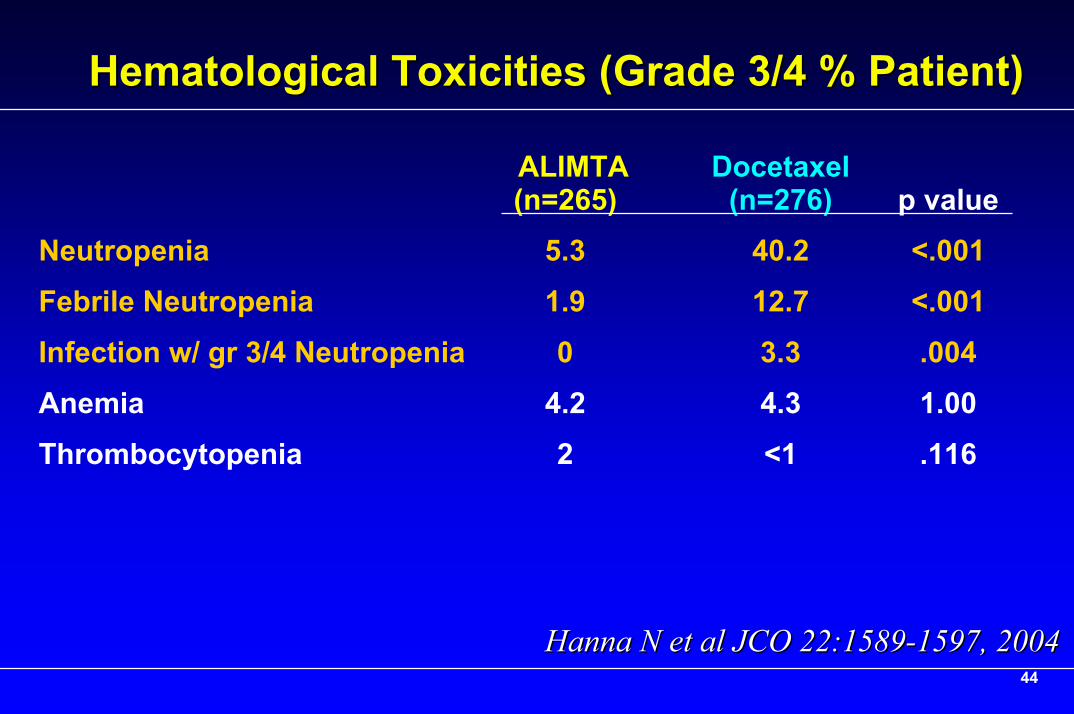
Hematological Toxicities (Grade 3/4 % Patient) Hematological Toxicities (Grade 3/4 % Patient)
ALIMTA Docetaxel(n=265) (n=276) p value
Neutropenia 5.3 40.2 <.001
Febrile Neutropenia 1.9 12.7 <.001
Infection w/ gr 3/4 Neutropenia 0 3.3 .004
Anemia 4.2 4.3 1.00
Thrombocytopenia 2 <1 .116
HannaHanna N N etet al JCO 22:1589al JCO 22:1589--1597, 20041597, 2004

45
Hospitalizations, Transfusions & Growth Factors Hospitalizations, Transfusions & Growth Factors ALIMTA Docetaxel(n=265) (n=276) p-value
Patients with > 1 hosp 31.7% 40.6% .032due to an adverse event
Total hospitalizations 1.5% 13.4% <.001 due to febrile neutropenia
G-CSF/GM-CSF 2.6% 19.2% <.001
Erythropoietin 6.8% 10.1% .169
Red blood cell 16.6% 11.6% .085Transfusions
46
Summary
• This is the largest phase III study ever reported for treatment in 2nd-line NSCLC
• ALIMTA and docetaxel have similar efficacy:
- response rates
- progression-free survival
- overall survival
47
SummarySummaryALIMTA had a more favorable hematological toxicity profile when compared with docetaxel:
− less severe neutropenia w/without fever and infections
− fewer hospitalizations
− less need for G-CSF/GM-CSF support
ALIMTA is an effective 2nd-line chemotherapy agent in NSCLC

48
Phase III ALIMTA Clinical TrialsPhase III ALIMTA Clinical Trials
ALIMTA + Cisplatin vs. Cisplatin in mesothelioma:−Completed; ALIMTA + Cisplatin showed survival advantage
ALIMTA vs. Docetaxel for 2nd Line NSCLC−Completed; ALIMTA showed equal efficacy but more favorable hematological toxicity profile
ALIMTA + GEMZAR vs. GEMZAR in Pancreatic Cancer−Completed accrual; awaiting data analysis
49
Conclusions IConclusions I
ALIMTA is an unique antifolate that inhibits several different enzymes in the DNA and RNA biosynthesis pathway
ALIMTA has activity in a number of solid tumors: NSCLC, pancreas, breast, colorectal, bladder and mesothelioma
In malignant pleural mesothelioma, a hard to-treat cancer, ALIMTA became the first agent that demonstrated superior survival and this represents a significant advance
In addition to survival benefits, ALIMTA also reduces disease-related symptoms and produces significantly higher objective response rates than the control arm in a phase III study
50
Conclusions IIConclusions II
ALIMTA is an effective 2nd-line chemotherapy agent in NSCLC
ALIMTA had a more favorable hematological toxicity profile when compared with control arm in a phase III study on 2nd line NSCLC
ALIMTA has an easy-to-control toxicity profile; physicians can deliver the planned course of therapy with simple folic acid and vitamin B12 supplementation
The antitumor activity of ALIMTA is retained or enhanced by folic acid and vitamin B12 supplementation
ALIMTA has a simple, brief outpatient administration and can easily be combined with other cytotoxic drugs


















