STATO NUTRIZIONALE Lo stato nutrizionale in provincia di ...
IL#TRATTAMENTO#NUTRIZIONALE#DELL’ECCESSO#PONDERALE#
Giorgio&Bedogni&
www.giorgiobedogni.it&
IL TRATTAMENTO NUTRIZIONALEDELL'ECCESSO PONDERALE
Giorgio Bedogni
www.giorgiobedogni.it
Obie5vo#
• Discutere&la&base&di&evidenza&disponibile&per&il&tra8amento&nutrizionale&dell’eccesso&ponderale&e&la&sua&implementazione&in&forma&di&linee&guida&per&la&pra<ca&professionale&(Academy&of&Nutri<on&and&Diete<cs,&AND&ex&American&Diete<c&Associa<on,&ADA)&
www.giorgiobedogni.it&
Obiettivo
• Discutere la base di evidenza disponibile per il trattamentonutrizionale dell'eccesso ponderale e la sua implementazionein forma di linee guida per la pratica professionale (Academyof Nutrition and Dietetics, AND ex American DieteticAssociation, ADA)
www.giorgiobedogni.it

Posizione#ADA#2009#
www.giorgiobedogni.it&
Posizione ADA 2009
from e associa ion
J Am Diet Assoc. 2009;109:330-346
Position of the American Dietetic Association:Weight Management
This paper endorsed by the American College of Sports Medicine
Classificazione#dell’evidenza#
A.#Grade& B.#Strength& C.#RecommendaKon&
I&=&Good& Strong& Condi<onal&
II&=&Fair& Fair& Impera<ve&
III&=&Limited& Weak&
IV&=&Expert&Opinion& Consensus&
V&=&Not&assignable& Insufficient&evidence&
Seagle et al. JADA 2009;109:330
www.giorgiobedogni.it&
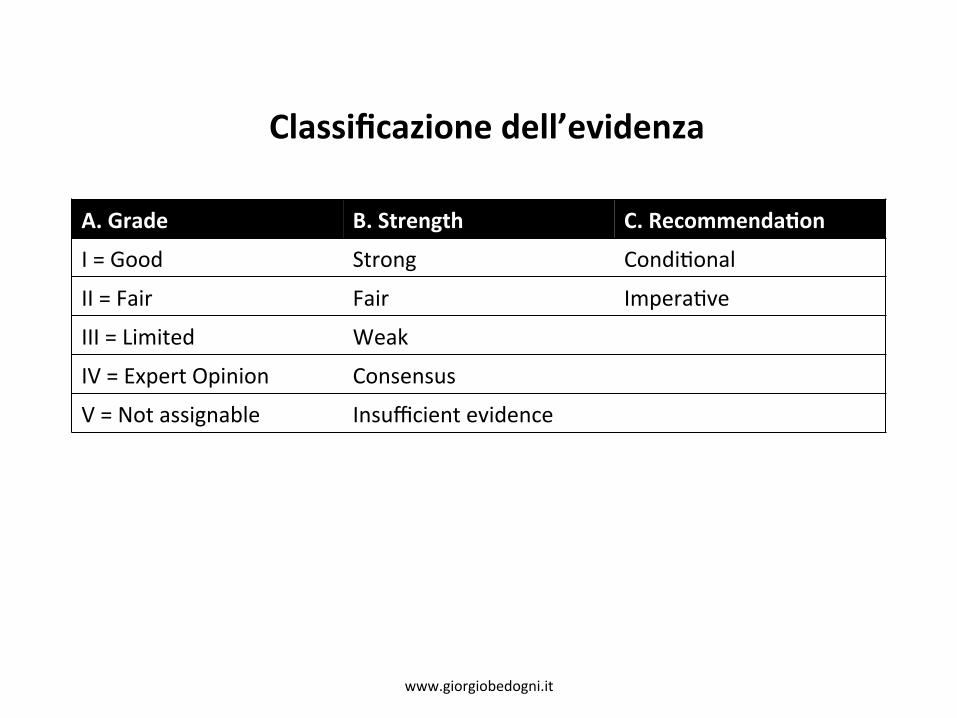
Classificazione delrevidenza
A. Grade B. Strength C. Recommendation
I = Good Strong Conditional
II = Fair Fair Imperative
III = Limited Weak
IV = Expert Opinion Consensus
V = Not assignable Insufficient evidence
www.giorgiobedogni.it

Posizione#ADA#2009#
• “It&is&the&posi<on&of&the&ADA&that&successful&weight&loss&management&to&improve&overall&health&for&adults&require&a&lifelong(commitment(to&healthful&lifestyle&behaviors&emphasizing&sustainable&and&enjoyable&ea<ng&prac<ces&and&daily&physical&ac<vity”&
&Seagle&et&al.&JADA&2009;109:330&&&&
www.giorgiobedogni.it&
Posizione ADA 2009
• " I t is the position of the ADA that successful weight lossmanagement to improve overall health for adults require alifelong commitment to healthful lifestyle behaviorsemphasizing sustainable and enjoyable eating practices anddaily physical activity"
www.giorgiobedogni.it

Obie5vi#
1. Prevenzione&o&arresto&dell’incremento&ponderale&2. Promozione&di&calo&ponderale&di&piccola&o&grande&en<tà&
(purché&mantenibile)&a8raverso&modificazione&dell’alimentazione&e&dell’aavità&fisica&&
3. Miglioramento&della&salute&fisica&ed&emozionale&4. Miglioramento&del&comportamento&rela<vo&all’alimentazione&
e&all’aavità&fisica&
&Seagle&et&al.&JADA&2009;109:331&
www.giorgiobedogni.it&
Obiettivi
1. Prevenzione o arrest° dell'incremento ponderale2. Promozione di cab o ponderale di piccola o grande entita
(purche mantenibile) attraverso modificazionedell'alimentazione e dell'attivita fisica
3. Miglioramento della salute fisica ed emozionale4. Miglioramento del comportamento relativo all'alimentazione
e all'attivita fisica
www.giorgiobedogni.it

ADA NCP Writing Group JADA 2008;108:1113. www.giorgiobedogni.it&
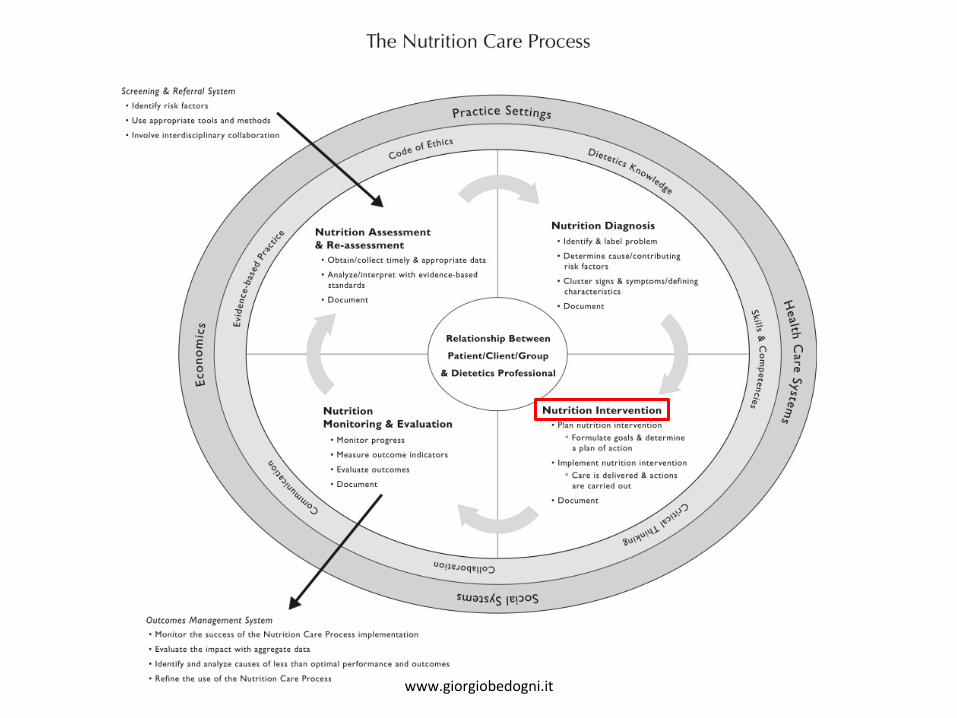
Screening & Referral System• Identify risk factors
• Use appropriate tools and methods
• Involve interdisciplinary collaboration
N u t r i t i o n Assessmen t& Re-assessment
• Obtain/collect timely & appropriate data
• Analyle/interpret with evidence-basedstandards
• Document
N u t r i t i o nM o n i t o r i n g & Eva lua t i on
• Moni tor progress
• Measure outcome indicators
• Evaluate outcomes
• Document
N u t r i t i o n Diagnos is• Identify & label problem
• Determine cause/contributingrisk factors
• Cluster signs & symptoms/definingcharacteristics
• Document
Relationship Between
Patient/Client/Group
& Dietet ics Professional
Nutrition Intervention• Plan nutr i t ion intervention
o Formulate goals & determinea plan of action
• Implement nutrit ion interventionCare is delivered & actionsare carried out
• Document
The Nutrition Care Process
e E t i n i C S
Outcomes Management System• Monitor the success o f the Nutr i t ion Care Process implementation
• Evaluate the impact with aggregate data
• Identify and analyze causes of less than optimal performance and outcomes
• Refine the use o f the Nutr i t ion Care Process
Practice Settings
uolaeJogepoD
SI-U93sAs ' e p o s
www.giorgiobedogni.it
sas'a'N.5.
LP

www.giorgiobedogni.it&
Screening & Referral System• Identify risk factors
• Use appropriate tools and methods
• Involve interdisciplinary collaboration
N u t r i t i o n Assessmen t I& Re-assessment
anvcollect timely & appropriate data
pie/interpret with evidence-baseddards
ument
N u t r i t i o nM o n i t o r i n g & Eva lua t i on
• monitor progress• Measure outcome indicators
• Evaluate outcomes
• Document
Relationship Between
Patient/Client/Group
& Dietet ics Professional
N u t r i t i o n Diagnos is• Identify & label problem
• Determine cause/contributingrisk factors
• Cluster signs & symptoms/definingcharacteristics
• Document
N u t r i t i o n I n t e r v e n t i o n• Plan nutr i t ion intervention
o Formulate goals & determinea plan of action
• Implement nutrit ion interventionCare is delivered & actionsare carried out
• Document
• AnalStan
• Doc
The Nutrition Care Process
e o i EtiniCs
Outcomes Management System• Monitor the success o f the Nutr i t ion Care Process implementation
• Evaluate the impact with aggregate data
• identify and analyze causes of less than optimal performance and outcomes
• Refine the use o f the Nutr i t ion Care Process
Practice Settings
LioneJoat i toD
sl-U93sAs ' e p o s
www.giorgiobedogni.it
,Ok.•>•\.5.
LP

BMI#e#circonferenza#vita#
• “BMI&and&waist&circumference&should&be&used&to&classify&overweight&and&obesity,&es-mate(risk(for(disease,&and&to&iden<fy&treatment&op<ons”&&&Ra<ng:&FAIR,&IMPERATIVE&
&Seagle&et&al.&JADA&2009;109:332&&
www.giorgiobedogni.it&
BM! e circonferenza vita
• "BMI and waist circumference should be used to classifyoverweight and obesity, estimate risk for disease, and toidentify treatment options"
Rating: FAIR, IMPERATIVE
www.giorgiobedogni.it
www.giorgiobedogni.it&
Screening & Referral System• Identify risk factors
• Use appropriate tools and methods
• Involve interdisciplinary collaboration
The Nutrition Care Process
<se.
N u t r i t i o n Assessmen t& Re-assessment
• Obtain/collect timely & appropriate data
• Analyze/interpret with evidence-basedstandards
• Document
N u t r i t i o nM o n i t o r i n g & Eva lua t i on
• monitor progress• Measure outcome indicators
• Evaluate outcomes
• Document
N u t r i t i o n Diagnos is• Identify & label problem
• Determine cause/contributingrisk factors
• Cluster signs & symptoms/definingcharacteristics
• Document
Relationship Between
Patient/Client/Group
& Dietet ics Professional
• Plan nutr i t ion interventiono Formulate goals & determine
a plan of action
• Implement nutrit ion interventionCare is delivered & actionsare carried out
• Document
Outcomes Management System• Monitor the success o f the Nutr i t ion Care Process implementation
• Evaluate the impact with aggregate data
• identify and analyze causes of less than optimal performance and outcomes
• Refine the use o f the Nutr i t ion Care Process
Practice Settings
www.giorgiobedogni.it
INutrit ion Intervention I

Approcci#disponibili#
1. Composizione&della&dieta&2. Controllo&delle&porzioni&3. Frequenza&dell’alimentazione&4. Pas<&sos<tu<vi&5. Dieta&fortemente&ipocalorica&6. Aavità&fisica&7. Interven<&comportamentali&8. Farmacoterapia&9. Chirurgia&
&Seagle&et&al.&JADA&2009;109:332&
www.giorgiobedogni.it&
1. Composizione della dieta2. Con t ro l lo delle porzioni3. Frequenza dell'alimentazione4. P a s t i sostitutivi5. D i e t a fortemente ipocalorica6. A t t i v i t a fisica7. In tervent i comportamentali8. Farmacoterapia9. Chirurgia
Approcci disponibili
www.giorgiobedogni.it
Composizione#della#dieta#
1. Composizione(della(dieta(2. Controllo&delle&porzioni&3. Frequenza&dell’alimentazione&4. Pas<&sos<tu<vi&5. Dieta&fortemente&ipocalorica&6. Aavità&fisica&7. Interven<&comportamentali&8. Farmacoterapia&9. Chirurgia&
www.giorgiobedogni.it&
1. Composizione dello dieto2. Con t ro l lo delle porzioni3. Frequenza dell'alimentazione4. P a s t i sostitutivi5. D i e t a fortemente ipocalorica6. A t t i v i t a fisica7. In tervent i comportamentali8. Farmacoterapia9. Chirurgia
Composizione della dieta
www.giorgiobedogni.it

Energia#
• “Reducing&dietary&fat&and/or&carbohydrates&&is&a&prac<cal&way&to&create&a&caloric&deficit&of&500&to&1000&kcal&below&es<mated&energy&needs&and&should&result&in&a&weight&loss&of&1*&to&2&lb&per&week”&&
&Ra<ng:&STRONG,&IMPERATIVE&&
&*&1&lb&=&0.45&kg&
&Seagle&et&al.&JADA&2009;109:334&&
www.giorgiobedogni.it&
• "Reducing dietary fat and/or carbohydrates is a practical wayto create a caloric deficit of 500 to 1000 kcal below estimatedenergy needs and should result in a weight loss of 1* to 2 lbper week"
Rating: STRONG, IMPERATIVE
* 1 lb = 0.45 kg
Energia
www.giorgiobedogni.it

CarboidraK#
• “...Consump<on&of&a&lowlcarbohydrate&diet&is&associated&with&a&greater&weight&and&fat&loss&than&tradi<onal&reducedlcalorie&diet&during&the&first&6&months,&but&these&differences&are¬&significant&aner&1&year”&&&Ra<ng:&FAIR,&CONDITIONAL&
&Seagle&et&al.&JADA&2009;109:334&&
www.giorgiobedogni.it&
Carboidrati
• "...Consumption of a low-carbohydrate diet is associated witha greater weight and fat loss than traditional reduced-caloriediet during the first 6 months, but these differences are notsignificant after 1 year"
Rating: FAIR, CONDITIONAL
www.giorgiobedogni.it

CarboidraK#
• “...The&safety&has¬&been&evaluated&for&longlterm&extreme&restric<ons&of&carbohydrates&(<35%&of&energy&from&carbohydrates)”&&&
&Seagle&et&al.&JADA&2009;109:334&&
www.giorgiobedogni.it&
Carboidrati
• "...The safety has not been evaluated for long-term extremerestrictions of carbohydrates (<35% of energy fromcarbohydrates)"
www.giorgiobedogni.it
*LowPcarb#vs#hiPcarb?#
www.giorgiobedogni.it&
ZJg
*Low-carb vs hi-carb?
American Journal of Epidemiologyr0 The Author 2012. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School ofPublic Health. All rights reserved. For permissions, please e-mail: [email protected].
Systematic Reviews and Meta- and Pooled Analyses
Effects of Low-Carbohydrate Diets Versus Low-Fat Diets on Metabolic RiskFactors: A Meta-Analysis of Randomized Controlled Clinical Trials
Tian Hu, Katherine T. Mills, Lu Yao, Kathryn Demanelis, Mohamed Eloustaz, William S. Yancy, Jr,Tanika N. Kelly, Jiang He, and Lydia A. Bazzano*
' Correspondence to Dr. Lydia A. Bazzano, Department of Epidemiology, Tulane University School of Public Health and TropicalMedicine. 1440 Canal Street, SL-18, Suite 2000, New Orleans, LA 70112 (e-mail: [email protected]).
Initially submitted December 16, 2011; accepted for publication May 11, 2012.
www.giorgiobedogni.it
Vol. 176. No. 7DOI: 10.1 93/aje/kws264
*LowPcarb#vs#hiPcarb?#
www.giorgiobedogni.it&
• “The&effects&of&lowlcarbohydrate&diets&(≤45%&of&energy&from&carbohydrates)&versus&lowlfat&diets&(≤30%&of&energy&from&fat)&on&metabolic&risk&factors&were&compared&in&a&metalanalysis&of&randomized&controlled&trials”&
*Low-carb vs hi-carb?
• "The effects of low-carbohydrate diets (45% of energy fromcarbohydrates) versus low-fat diets (30% of energy from fat)on metabolic risk factors were compared in a meta-analysis ofrandomized controlled trials"
www.giorgiobedogni.it

*LowPcarb#vs#hiPcarb?#
www.giorgiobedogni.it&
*Low-carb vs hi-carb?
778 potentially relevant 7 additional referencesreferences identified through identified through manualdatabase searching searches
503 remaining record A c r duplicates wereremoved
lull-text articles assessed for eligibility
23 trials included in meta-analysis
Figure 1. F l o w diagram of systematic review (from January 1, 1966 to June 20, 2011).
www.giorgiobedogni.it
466 articles excluded ny review of abstract or title:117 not randomized controlled trials116 intervention did not include a low-carbohydrate diet or
a low-fat diet13 inappropriate population13 no difference in dietary carbohydrate or fat.3 difference other than macronutrient intake
144 length of intervention was not lonser than 6 months.,difference other than macrontarient intake
74 . - t i l l - t e x t a r t i c l e s e x c l u d e d l ' o r t h e f o l l o w i n g reaSULIS:
5 duplicate reports12 not randomized controlled trials15 no metabolic risk factors were reported19 intenention did not include low-carbohydrate diet or
low-fat diet6 duration less than 6 months8 no difference in dietary carbohydrate or fat7 difference other than macronutrient intake2 no variance, standard error, standard deviation, or
confidence interval reported

*LowPcarb#vs#hiPcarb?#
www.giorgiobedogni.it&
*Low-carb vs hi-carb?
VariableAll Trials Trials With >70%
Completion RateTrials W i t h 20
Participants per GroupTrials With Healthy
Participants'
No. ofTrials
Net 95% ClChangeNo. ofTrials
NetChange 95n% Cl No. of
TrialsNet
Change 95% Cl No. ofTrials
NetChange 95% Cl
Weight, kg 22 1.0 -2.2, 0.2 12 -1.3 -2.8, 0.2 19 -1.3 -2.5, -0.1 18 -1.4 -2.6, -0.2WC, cm 10 0.1 -0.6, 0.4 8 -0.3 -1.0, 0.5 8 -0.2 -0.7, 0.3 8 -0.2 -0.7, 0.3TC, mg/dL 15 2.7 0.8, 4.6 9 3.5 0.1, 6.9 14 3.3 1.0, 5.5 13 2.7 0.6, 4,9WI_ mg/dL 19 3.7 1.0, 6.4 11 2.8 0.3, 5.3 18 3.7 1.0, 6.4 17 3.6 0.7, 6.4HDL, mg/dL 19 3.3 1.9, 4.7 11 3.0 1.9, 4.1 18 3.4 1.9,4.8 17 3.3 1.9, 4.8TC:HDL ratio 5 -0.1 -0.3, 0.1 1 -0.5 -0.8, -0.1 5 -0.1 -0.3, 0.1 5 -0.1 -0.3, 0.1TG, mg/dL 20 -14.0 -19.4, -8.7 12 -11.2 -16.9, -5.5 19 -13.4 -18.7, -8.1 18 -13.6 -19.2, -8.0SBP, mmHg 18 -1.0 -3.5, 1.5 10 -0.1 -2.5, 2.3 17 -1.4 -3.9, 1.2 17 -1.6 -4.2, 1.0DBP, mmHg 18 -0.7 -1,6, 0.2 10 -1.1 -2.4, 0.2 17 -0.8 -1.7, 0,2 17 -0.8 -1.7, 0,2Glucose, mg/dL 14 -0.3 -1.9, 1.3 10 -0.6 -2.7, 1.4 13 -0.4 -2.1, 1.4 13 -0.4 -2.1, 1.4Insulin, Iti/mL 12 -0.1 0.8, 0.6 8 -0.1 -1.0, OA 10 -0.1 -0.9, 0.7 10 -0.3 -0.9, 0.7
Table 3. M a i n Results and Results From Sensitivity Analyses, 1966-2011
Abbreviations: Cl, confidence interval; DBP, diastolic blood pressure; HDL, high density lipoprotein cholesterol; LDL, low density lipoproteincholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; WC, waist circumference.
a Trials with participants who had breast cancer, polycystic ovary syndrome, or coronary heart disease or who had undergone gastric bypasssurgery were excluded.
www.giorgiobedogni.it

*LowPcarb#vs#hiPcarb?#
• “In&the&present&metalanalysis&of&randomized&controlled&trials&comparing&lowlcarbohydrate&diets&with&lowlfat&diets,&we&found&that&both&diets&were&equally&effec<ve&at&reducing&body&weight&and&waist&circumference.&Both&diets&reduced&par<cipants’&blood&pressures,&total&to&HDL&cholesterol&ra<os,&and&total&cholesterol,&LDL&cholesterol,&triglycerides,&blood&glucose,&and&serum&insulin&levels&and&raised&HDL&cholesterol.”&
www.giorgiobedogni.it&
*Low-carb vs hi-carb?
• " I n the present meta-analysis of randomized controlled trialscomparing low-carbohydrate diets with low-fat diets, wefound that both diets were equally effective at reducing bodyweight and waist circumference. Both diets reducedparticipants' blood pressures, total to HDL cholesterol ratios,and total cholesterol, LDL cholesterol, triglycerides, bloodglucose, and serum insulin levels and raised HDL cholesterol."
www.giorgiobedogni.it

*LowPcarb#vs#hiPcarb?#
• “However,&par<cipants&on&lowlcarbohydrate&diets&had&greater&increases&in&HDL&cholesterol&and&greater&decreases&in&triglycerides&but(experienced(less(reduc-on(in(total(and(LDL(cholesterol(compared(with(persons(on(low(fat(diets”&
• “These&findings&have&important&clinical&and&public&health&implica<ons”&
www.giorgiobedogni.it&
*Low-carb vs hi-carb?
• "However, participants on low-carbohydrate diets had greaterincreases in HDL cholesterol and greater decreases intriglycerides but experienced less reduction in total and LDLcholesterol compared with persons on low fat diets"
• "These findings have important clinical and public healthimplications"
www.giorgiobedogni.it

*LowPcarb#vs#hiPcarb?#
• “Although&the&present&study&did¬&examine&longlterm&clinical&effects&on&cardiovascular&diseases,&these&findings&suggest&that&lowlcarbohydrate&diets&can&be&recommended&to&obese&persons&with&metabolic&risk&factors&for&the&purpose&of&weight&loss”&&
• “Dietary&recommenda<ons&for&weight&loss&should&be&revisited&to&consider&addi<onal&evidence&of&the&benefits&of&lowlcarbohydrate&diets”&
www.giorgiobedogni.it&
*Low-carb vs hi-carb?
• "Although the present study did not examine long-termclinical effects on cardiovascular diseases, these findingssuggest that low-carbohydrate diets can be recommended toobese persons with metabolic risk factors for the purpose ofweight loss"
• "Dietary recommendations for weight loss should be revisitedto consider additional evidence of the benefits of low-carbohydrate diets"
www.giorgiobedogni.it

*Modificazione#delle#HDL#e#rischio#cardiovascolare?#
www.giorgiobedogni.it&
*Modificazione delle HDL e rischio cardiovascolare?
BMJAssociation between change in high densitylipoprotein cholesterol and cardiovasculardisease morbidity and mortality: systematicreview and meta-regression analysisMatthias Brie!, Ignacio Ferreira-Gonzalez, John J You, Paul J Karanicolas,Elie A Akl. Ping Wu, Boris Blechacz, Dirk Bassler, Xinge Wei, AsheerSharman, Irene Whitt, Suzana Alves da Silva, Zahira Khalid, Alain JNordmann. Oi Zhou, Stephen D Walter, Noah Vale. Neera Bhatnagar,Christopher 01Regan. Edward J Mills, Heiner C Bucher, Victor M Montori andGordon H Guyatt
BMJ 2009;338:1392do1:10.1136/13mj.1392
www.giorgiobedogni.it

*Modificazione#delle#HDL#e#rischio#cardiovascolare?#
www.giorgiobedogni.it&
*Modificazione delle HDL e rischio cardiovascolare?
WHAT THIS STUDY ADDSNo association exists between treatment induced change in high density lipoproteincholesterol a nd risk ratios for coronary heart disease events, coronary heart disease deaths, ortotal deaths when changes in low density lipoprotein cholesterol are adjusted forWhereas change in high density lipoprotein cholesterolfailed to explain variability in risk ratiosfor coronary heart disease events across studies, change in low density lipoprotein cholesterolexplained about one third of the variability
Scepticism about interventions to lower coronary heart disease risk by increasing the amountof circulating high density lipoprotein cholesterol without considering effects on its function isreinforced
www.giorgiobedogni.it

*Modificazione#delle#HDL#e#rischio#cardiovascolare?#
www.giorgiobedogni.it&
*Modificazione delle HDL e rischio cardiovascolare?
ORIGINAL ARTICLE
Changes in HDL cholesterol and cardiovascularoutcomes after lipid modification therapyKausik Ray,1 Nick W J Wainwright,2 Loes Visser,3/1 Jacqueline Witteman,3Monique Breteler,3 Baishali Ambegaonkar,5 Albert Hotman,3 Bruno Stricker,3Nick Wareham,6 Kay Tee Khaw,7 Manjinder Sandhu2Heart 2012;98:780-785. doil 0.1136/heartjnI-2011-301405
www.giorgiobedogni.it
*Modificazione#delle#HDL#e#rischio#cardiovascolare?#
• “The&present&findings&give&limited&support&to&the&possibility&of&beneficial&effects&of&HDLlC&raising&in&ongoing&clinical&trials.&While&we&found&some&evidence&of&associa<on&between&changes&in&HDLlC&and&reduced&risk&of&CVD,&our&findings&suggest&that&these&effects&are(not(independent(of(non>LDL>C>lowering,(or(of(changes(in(conven-onal(non>lipid(CVD(risk(factors,&and&that&they&are&more&modest&than&those&previously&described”&
www.giorgiobedogni.it&
*Modificazione delle HDL e rischio cardiovascolare?
• "The present findings give limited support to the possibility ofbeneficial effects of HDL-C raising in ongoing clinical trials.While we found some evidence of association betweenchanges in HDL-C and reduced risk of CVD, our findingssuggest that these effects are not independent of non-LDL-C-lowering, or of changes in conventional non-lipid CVD riskfactors, and that they are more modest than those previouslydescribed"
www.giorgiobedogni.it

Indice#glicemico#
• “A&low&glycemic&index&diet&is¬(recommended&for&weight&loss&or&weight&maintenance&as&part&of&a&comprehensive&weight&management&program&since&it&has¬&been&shown&to&be&effec<ve&in&these&areas”&&&Ra<ng:&STRONG,&IMPERATIVE&
&Seagle&et&al.&JADA(2009;109:334&
www.giorgiobedogni.it&
Rating: STRONG, IMPERATIVE
Seagle et al. JADA 2009;109:334
Indice glicemico
• " A low glycemic index diet is not recommended for weightloss or weight maintenance as part of a comprehensiveweight management program since it has not been shown tobe effective in these areas"
www.giorgiobedogni.it

*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
Low glytaemic index or low glytaemic load diets foroverweight and obesity Low glytaemic index or low glytaernic
load diets for overweight and obesity (Review)
Thomas DE, Elliott El, Baur L
THE COCHRANECOLLABORATION'
r } b i . a , p r i m eel Cochrane review, prepared and maintained by I l Cochrane CoLtaboralio E p blished in t i e ( M u n e L i k e ,2007, :Naar 3
WILEYPublishers Since 1807
givesernit ;MCISL or km, girwrornic load diets ,or twororrigin rerd oborito Low otrolornit irobro or tow grrowerodo load dors rocor...weight . . , b . , fILorLwrlCorryrigtO 1.007 Tiro Cow/worm ColirOurotkor PoLlithrd by johoWlier A Som. Ltd
www.giorgiobedogni.it

*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
Figure 01. A d a p t e d Q U O R O M (qual i ty of report ing of meta-analyses) f low-chart o f study selection
Art ic les r e t n e v e d f o r m o r e deta i led eva luat ion:
68 publications(19 potentially relevant RCTs)
Studies that met inclusion criteria:
6 publications (6 RCTs)
Potentially relevant articles from electronic databases:
892 publications
www.giorgioloodogni.it
Titles or abstracts excludedbecause they did not fulfillinclusion criteria: 824
Full text articles excluded:62 publications(13 RCTs)

*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
Analysis 01.01. Comparison 01 Low glycaemic diet versus high glycaemic or other diet, Outcome 01 changein body mass (kg)
Review L o w glycaemic index or low glycaemic load diets for overweight and obesity
Comparison: 0 1 Low glycaemic diet versus high
Outcome: 0 1 change in body mass (kg)
Study I n t e r v e n t i o n
N M e a n ( S D )
glycaemic or other diet
Control
N M e a n ( S D )
Weighted Mean Difference (Fixed) W e i g h t
95% CI ( 9 6 )Weighted Mean Difference (Fixed)
95% Cl
0 I change In body mass (kg)Bouche 2002 1 1 -0.30 (9.60) II 050 (8.90) -0.80 [ -8.54. 6.941.4
McMillan-Nce 2006 3 2 -5.60 (4.00) 32 -4.30 (4.00) -1.30 [ -3.26, 0.66 I- E - - 21.4
Slabber 1994 1 6 -7.42 (2.49) 16 -4.48 (4.23) 14.2 -2.94 [ -5.35, -0.53 ]
Sloth 2004 2 3 -1.90 (2.40) 22 -1.30 (1.40) 63.0 -0.60 [ -1.74. 0.54 I
Total (95% CI) 8 2 81 ••• 100.0 -1.09 [ -1.99. -0.18 ]Test for heterogeneity chi-square=3.03 df=3 p=0.39 12=1.0%
Test for overall effect z=2.35 p=0.02
*Indice glicemico e cab ° ponderale
-10.0 - 5 . 0 0 5 . 0 1 0 . 0
Favours low glycem lc F a v o u r s control
www.giorgiobedogni.it

*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
Study InterventionMean(SD) N
ControMean(SD)
Weighted Mean Difference (Fixed) W e i g h t
95% CI ( 9 6 )
Weighted Mean Difference (Fixed)95% Cl
Ebbeling 2003 8 -1.20 (1.85) 8 0.60 (1.32) 22.7 -1.80 [ -3.37. -0.23 ]
Slabber 1994 16 -2.73 (0.85) 16 -1.61 (1.52) --E-- 77.3 -1.12 [-1.97,-0.27]
Total (95% Cl) 24 24 -401- 100.0 -1.27 [ -2.02, -0,52 ]Test for heterogeneity chi-square=0.55 df=1 p=0.46 P =00%Test for overall effect z=3,33 p=0.0009
Analysis 01.03. Comparison 01 Low glycaemic diet versus high glycaemic or other diet, Outcome 03 changein body mass index (BM! units)
Review: L o w glycaemic index or low glycaemic load d ets for overweight and obesityCompanson: 0 1 Low glycaemic diet versus high glycaemic or other diet
Outcome: 0 3 change in body mass index (BMI units)
-4,0 - 2 . 0 0 2 • 0 4 . 0
Favours low glycemic F a v o u r s control
www.giorgiobedogni.it
*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
Study I n t e r v e n t i o nN M e a n ( S D ) N
ControlMean(SD)
Weighted Mean Difference (Fixed) W e i g h t
95% Cl ( % )
We ghted Mean Difference (Fixed)95% CI
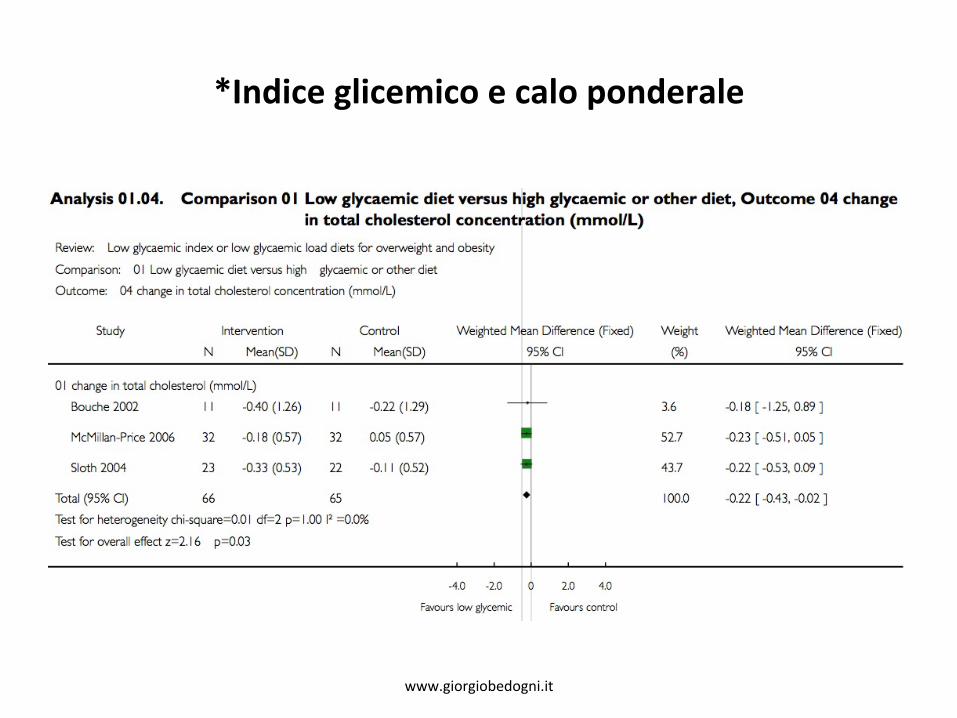
01 change n total cholestero (mmol/L)Bouche 2002 I I - 0 . 4 0 (1.26) I I -0.22 (1.29) 3.6 -018 [ 0.89 ]
McMillan-Price 2006 3 2 - 0 . 1 8 (0.57) 32 0.05 (0.57) 52.7 -0.23 [ -0.51. 0,05 ]
Sloth 2004 2 3 - 0 . 3 3 (0.53) 22 -0.11 (0.52) 43.7 -022 [ -0.53, 0.09]
Total (95% Cl) 6 6 65 • 100.0 -0.22 [ -0.43, -0.02 ]Test for heterogeneity chi-square=0.0 I df=2 p= ILO F =0.0%
Analysis 01.04. Comparison 01 Low glycaemic diet versus high glycaemic or other diet, Outcome 04 changein total cholesterol concentration (mmol/L)
Review: L o w glycaemic index or low glycaemic load diets for overweight and obesty
Compar son: 0 1 Low glycaemic diet versus high glycaem c or other diet
Outcome: 0 4 change in total cholesterol concentration (mmol/L)
Test for overall effect z=2. I 6 p=0.03
-4.0 - 2 . 0 D 2 . 0 4 , 0
Favours low glycemic F a v o u r s control
www.giorgiobedogni.it

*Indice#glicemico#e#calo#ponderale#
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
Review: L o w glycaemic index or low glycaemic load (lets for overweight and obesityComparison: 0 1 Low glycaemic diet versus high glycaemic or other diet
Outcome: 0 5 change in LDL cholesterol concentrat on (mmol/L)
Study I n t e r v e n t i o n C o n t r o l W e i g h t e d Mean Difference (Fixed) W e i g h tN M e a n ( S D ) N M e a n ( S D ) 9 5 % Cl ( % )
Weighted Mean Difference (Fixed)95% Cl
01 change n LDL chole5tera concentrat on (mmol/L)
Bouche 2002 1 I - 0 . 3 6 (1.06) I I -0.27 (0.70) 6.4 -0.09 [ -0.84. 0.66]
McMillan-Pnce 2006 3 2 - 0 . 1 7 (0.57) 32 0.04 (0.57) • 4 6 . 5 -0.21 [ -0.49, 0.07]
Sloth 2004 2 3 - 0 . 2 4 (0.48) 22 0.06 (0.47) 47.1 -0.30 [ -0.58, -0.02 ]
Total (95% Cl) 6 6 65 100.0 -0.24 [ -0.44. -0.05 ]Test for heterogeneity chi-square=0.37 df=2 p=0.83 V =0.0%Test for overall effect z=2.52 p=0.01
Analysis 01.05. Comparison 01 Low glycaemic diet versus high glycaemic or other diet, Outcome 05 changein LDL cholesterol concentration (mmol/L)
AC - 2 . 0 0 2 . 0 4 0
Favours low glycemic F a v o u r s control
www.giorgiobedogni.it
*Indice#glicemico#e#calo#ponderale#
• “Lowering&the&glycaemic&load&of&the&diet&appears&to&be&an&effec<ve&method&of&promo<ng&weight&loss&and&improving&lipid&proles&and&can&be&simply&incorporated&into&a&person's&lifestyle.&Further&research&with&longer&term&followlup&will&determine&whether&improvement&con<nues&longlterm&and&improves&quality&of&life.”&
• (Ci&sono&ancora&dubbi&sul&perché&è&indispensabile&valutare&la&dimensione&dell’effe8o?)&
www.giorgiobedogni.it&
*Indice glicemico e cab ° ponderale
• "Lowering the glycaemic load of the diet appears to be aneffective method of promoting weight loss and improvinglipid proles and can be simply incorporated into a person'slifestyle. Further research with longer term follow-up willdetermine whether improvement continues long-term andimproves quality of life."
• (Ci sono ancora dubbi sul perche e indispensabile valutare ladimensione dell'effetto?)
www.giorgiobedogni.it
LaSe#e#derivaK#
• “In&order&to&meet&nutri<onal&recommenda<ons,&incorporate&3l4&servings&of&lowlfat&dairy&foods&a&day&as&part&of&a&comprehensive&weight&management&program”&&&Ra<ng:&FAIR,&IMPERATIVE&
&Seagle&et&al.&JADA(2009;109:334&
www.giorgiobedogni.it&
• " I n order to meet nutritional recommendations, incorporate3-4 servings of low-fat dairy foods a day as part of acomprehensive weight management program"
Rating: FAIR, IMPERATIVE
Seagle et al. JADA 2009;109:334
Latte e derivati
www.giorgiobedogni.it

Calcio#
• “Research&suggests&that&calcium&intake&lower&than&the&recommended&intake&is&associated&with&increased&body&weight”&[OSSERVAZIONALE]&
• “However,&the&effect&of&dairy&and/or&calcium&at&above&recommended&levels&on&calcium&management&is&unclear”&[SPERIMENTALE]&
&Seagle&et&al.&JADA(2009;109:334&
www.giorgiobedogni.it&
• "Research suggests that calcium intake lower than therecommended intake is associated with increased bodyweight" [OSSERVAZIONALE]
• "However, the effect of dairy and/or calcium at aboverecommended levels on calcium management isunclear" [SPERIMENTALE]
Seagle et al. JADA 2009;109:334
Calcio
www.giorgiobedogni.it
www.giorgiobedogni.it&
A systematic review of the effects of calcium supplementation on body weight
Rebecca Trowmanl, Jo C. Dumvillel*, Seokyung Hahn2 and David J. Torgersonl1Seebohm Rowntree Building, Department of Health Sciences, University of York, York Y010 5DD, UK2Medical Research Collaborating Center, Seoul National University College of Medicine, Seoul National University Hospital,Seoul 110-744, Korea
(Received 28 June 2005 — Revised 8 December 2005 — Accepted 13 December 2005)
Animal studies and epidemiological studies have suggested that Ca supplementation (with Ca supplements or dairy products) may be associatedwith weight loss in human adults. We aimed to assess whether any association was present by reviewing relevant randomized controlled trials inhuman subjects. The study was a systematic review and subsequent meta-analysis of randomized controlled trials that used Ca supplementation asan intervention in persons 18 or more years of age, and that reported body weight as a final outcome. A total of thirteen randomized controlledtrials were included in the meta-analysis. There was no association between the increased consumption of either Ca supplements or dairy productsand weight loss after adjusting for differences in baseline weights between the control and intervention groups (P=0•19 and 0•85, respectively).We therefore concluded that Ca supplementation has no statistically significant association with a reduction in body weight.British Journal o f Nutrition (2006), 95, 1033-1038© The Authors 2006
www.giorgiobedogni.it

Controllo#delle#porzioni#
1. Composizione&della&dieta&2. Controllo(delle(porzioni(3. Frequenza&dell’alimentazione&4. Pas<&sos<tu<vi&5. Dieta&fortemente&ipocalorica&6. Aavità&fisica&7. Interven<&comportamentali&8. Farmacoterapia&9. Chirurgia&
www.giorgiobedogni.it&
1. Composizione della dieta2. C o n trollo delle porzioni3. Frequenza dell'alimentazione4. P a s t i sostitutivi5. D i e t a fortemente ipocalorica6. A t t i v i t a fisica7. In tervent i comportamentali8. Farmacoterapia9. Chirurgia
Controllo delle porzioni
www.giorgiobedogni.it

Controllo#delle#porzioni#
• “Por<on&control&should&be&included&as&part&of&comprehensive&weight&management&program.&Por<on&controls&at&meals&and&snacks&results&in&reduced&energy&intake&and&weight&loss”&&
&Ra<ng:&FAIR,&IMPERATIVE&
&Seagle&et&al.&JADA(2009;109:334&
www.giorgiobedogni.it&
Rating: FAIR, IMPERATIVE
Seagle et al. JADA 2009;109:334
Controllo delle porzioni
• "Portion control should be included as part of comprehensiveweight management program. Portion controls at meals andsnacks results in reduced energy intake and weight loss"
www.giorgiobedogni.it

Frequenza#dell’alimentazione#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza(dell’alimentazione(• Pas<&sos<tu<vi&• Dieta&fortemente&ipocalorica&• Aavità&fisica&• Interven<&comportamentali&• Farmacoterapia&• Chirurgia&
www.giorgiobedogni.it&
Frequenza dell'alimentazione
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dellialimentazione• Pas t ' sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• Intervent i comportamentali• Farmacoterapia• Chirurgia
www.giorgiobedogni.it
Frequenza#dell’alimentazione#
• “Total&caloric&intake&should&be&distributed&throughout&the&day,&with&the&consump<on&of&four&to&five&meals/snacks&including&breakfast.&Consump<on&of&greater&energy&intake&during&the&day&may&be&preferable&to&evening&consump<on”&
&Ra<ng:&FAIR,&IMPERATIVE&
www.giorgiobedogni.it&
Frequenza dell'alimentazione
• "Tota l caloric intake should be distributed throughout theday, with the consumption of four to five meals/snacksincluding breakfast. Consumption of greater energy intakeduring the day may be preferable to evening consumption"
Rating: FAIR, IMPERATIVE
www.giorgiobedogni.it

PasK#sosKtuKvi#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas-(sos-tu-vi(• Dieta&fortemente&ipocalorica&• Aavità&fisica&• Interven<&comportamentali&• Farmacoterapia&• Chirurgia&
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• P a s t sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• Intervent i comportamentali• Farmacoterapia• Chirurgia
Pasti sostitutivi
www.giorgiobedogni.it

PasK#sosKtuKvi#
• “For&people&who&have&difficulty(with&self>selec-on(and/or(por-on(control,(meal&replacements&may&be&used&as&part&of&the&diet&component&of&a&comprehensive&weight&management&program”&
&Ra<ng:&STRONG,&CONDITIONAL&&&
www.giorgiobedogni.it&
• "For people who have difficulty with self-selection and/orportion control, meal replacements may be used as part ofthe diet component of a comprehensive weightmanagement program"
Rating: STRONG, CONDITIONAL
Pasti sostitutivi
www.giorgiobedogni.it

Dieta#fortemente#ipocalorica#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas<&sos<tu<vi&• Dieta(fortemente(ipocalorica(• Aavità&fisica&• Interven<&comportamentali&• Farmacoterapia&• Chirurgia&
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• Pas t i sostitutivi• D i e t o fortemente ipocalorica• A t t i v i t a fisica• Intervent i comportamentali• Farmacoterapia• Chirurgia
Dieta fortemente ipocalorica
www.giorgiobedogni.it

Dieta#fortemente#ipocalorica##(<#800#kcal)#
• “Results&in&significant&weight&loss”&(Grade&I&=&Good)&
• “Results&in&significantly&greater&weight&loss&than&reducelcalorie&diets”&(Grade&I&=&Good)&
• “Studies&report&varying&levels&of&weight®ain&based&on&difference&in&weight&management&strategies”&(Grade&I&=&Good)&
&&&
&&
&&
www.giorgiobedogni.it&
Dieta fortemente ipocalorica(< 800 kcal)
• "Results in significant weight loss" (Grade I = Good)
• "Results in significantly greater weight loss than reduce-caloriediets" (Grade I = Good)
• "Studies report varying levels of weight regain based on differencein weight management strategies" (Grade I = Good)
www.giorgiobedogni.it
A5vità#fisica#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas<&sos<tu<vi&• Dieta&fortemente&ipocalorica&• AKvità(fisica(• Interven<&comportamentali&• Farmacoterapia&• Chirurgia&
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• Pas t i sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• In tervent i comportamentali• Farmacoterapia• Chirurgia
Attivita fisica
www.giorgiobedogni.it

A5vità#fisica#
www.giorgiobedogni.it&
J Am Diet Assoc. 2009;109:330-346
Attivita fisica
from the associa ionPosition of the American Dietetic Association:
Weight ManagementThis paper endorsed by the American College of Sports Medicine I
www.giorgiobedogni.it

A5vità#fisica#
• “Despite&its&modest(impact(on&weight&loss,&physical&ac<vity&is&important&for&improving&healthlrelated&outcomes”&
&Seagle&et&al.&JADA(2009;109:336&
www.giorgiobedogni.it&
• "Despite its modest impact on weight loss, physical activity isimportant for improving health-related outcomes"
Seagle et al. JADA 2009;109:336
Attivita fisica
www.giorgiobedogni.it
Quale#e#quanta#a5vità#fisica?#
Obie5vo# Indicazione#
Riduzione&del&rischio&di&malaaa&cronica& 30&minu<&di&aavità&fisica&moderata&per&la&“maggioranza”&dei&giorni&della&seamana&[≥4l5]&
O8enimento&di&calo&ponderale& 60&minu<&di&aavità&fisica&moderatalvigorosa&per&la&“maggioranza”&dei&giorni&della&seamana&[≥4l5]&
Mantenimento&di&calco&ponderale& 60l90&minu<&di&aavità&fisica&moderatalvigorosa&tua&i&giorni&della&seamana&&
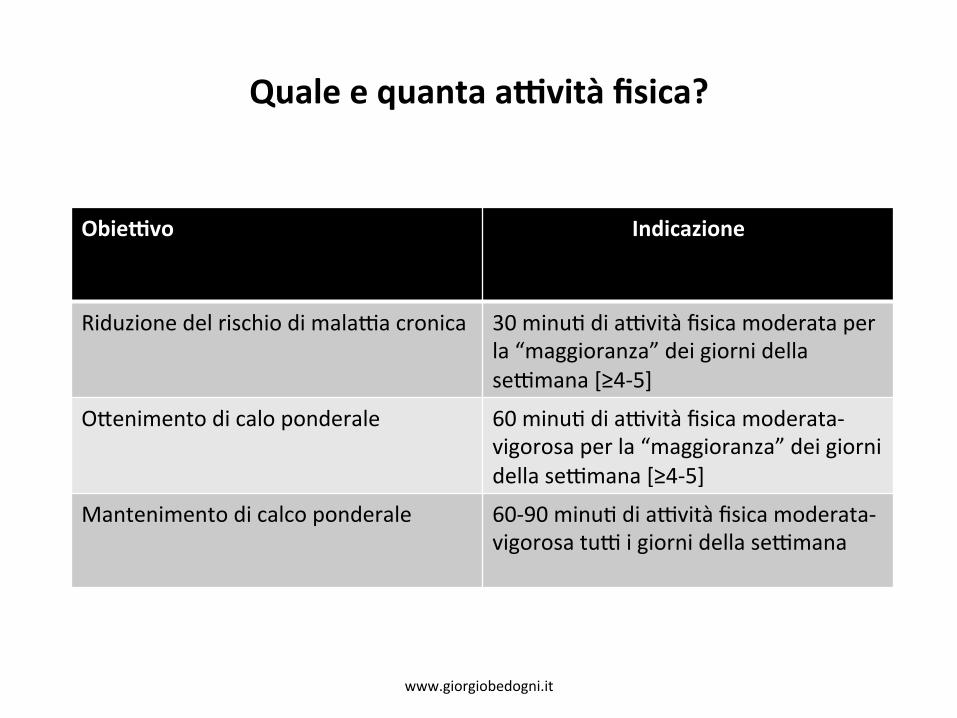
Seagle et al. JADA 2009;109:336 www.giorgiobedogni.it&
Quale e quanta attivita fisica?
Obiettivo Indicazione
Riduzione del rischio di malattia cronica 3 0 minuti di attivita fisica moderata perla "maggioranza" dei giorni dellasettimana [4 -5 ]
Ottenimento di cab o ponderale 6 0 minuti di attivita fisica moderata-vigorosa per la "maggioranza" dei giornidella settimana [4-5 ]
Mantenimento di calco ponderale
www.giorgiobedogni.it
60-90 minuti di attivita fisica moderata-vigorosa tutti i giorni della settimana

Evidenza#
• L’aavità&fisica&ha&un&chiaro&effe8o&proteavo&nei&confron<&della&mortalità&[OSSERVAZIONALE]&
• Inoltre,&il&principale&determinante&del&successo&nel&mantenimento&del&calo&ponderale&è&il&mantenimento&di&un’aavità&fisica®olare&[OSSERVAZIONALE]&
www.giorgiobedogni.it&
Evidenza
• Latt iv i ta fisica ha un chiaro effetto protettivo nei confrontidella mortalita [OSSERVAZIONALE]
• lnoltre, il principale determinante del success° nelmantenimento del cab ° ponderale e il mantenimento diun'attivita fisica regolare [OSSERVAZIONALE]
www.giorgiobedogni.it

IntervenK#comportamentali#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas<&sos<tu<vi&• Dieta&fortemente&ipocalorica&• Aavità&fisica&• Interven-(comportamentali(• Farmacoterapia&• Chirurgia&
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• Pas t i sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• In tervent i comportment-all• Farmacoterapia• Chirurgia
Interventi comportamentali
www.giorgiobedogni.it

IntervenK#comportamentali#
• “A&comprehensive&weight&management&program&should&make&maximum&use&of&the&mul<ple&strategies&for&behavioral&therapy&(i.e.&selflmonitoring,&stress&management,&s<mulus&control,&con<ngency&management,&cogni<ve&restructuring&and&social&support”&
www.giorgiobedogni.it&
Interventi comportamentali
• " A comprehensive weight management program should makemaximum use of the multiple strategies for behavioraltherapy (i.e. self-monitoring, stress management, stimuluscontrol, contingency management, cognitive restructuringand social support"
www.giorgiobedogni.it
IntervenK#comportamentali#
• “Cogni<ve&behavior&therapy&in&addi<on&to&diet&and&physical&ac<vity&leads&to&addi<onal&weight&loss.&Con<nued&behavioral&interven<ons&may&be&necessary&to&prevent&a&return&to&baseline&weight”&
&Ra<ng:&STRONG,&IMPERATIVE&
www.giorgiobedogni.it&
Interventi comportamentali
• "Cognitive behavior therapy in addition to diet and physicalactivity leads to additional weight loss. Continued behavioralinterventions may be necessary to prevent a return tobaseline weight"
Rating: STRONG, IMPERATIVE
www.giorgiobedogni.it

IntervenK#comportamentali##
• “It&is&possible&that&there&is&no&single&behavioral&tool&that&works&best.&Instead&it&may&be&more&important&to&match&behavioral&tools&with&each&individual’s&unique&set&of&characteris<cs.&These(are(the(type(of(ques-ons(than(need(further(aPen-on(and(research.”&
www.giorgiobedogni.it&
Interventi comportamentali
• " I t is possible that there is no single behavioral tool thatworks best. Instead it may be more important to matchbehavioral tools with each individual's unique set ofcharacteristics. These are the type of questions than needfurther attention and research."
www.giorgiobedogni.it

Farmacoterapia#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas<&sos<tu<vi&• Dieta&fortemente&ipocalorica&• Aavità&fisica&• Interven<&comportamentali&• Farmacoterapia(• Chirurgia&
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• Pas t i sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• Intervent i comportamentali• Formacoterapia• Chirurgia
Farmacoterapia
www.giorgiobedogni.it
Farmacoterapia#
• “FDAlapproved&weight&loss&medica<ons&may&be&part&of&a&comprehensive&weight&management&program.&Research&indicates&that&pharmacotherapy&may&enhance&weight&loss&in&some&overweight&and&obese&adults”&
&Ra<ng:&STRONG,&IMPERATIVE&
www.giorgiobedogni.it&
Farmacoterapia
• "FDA-approved weight loss medications may be part of acomprehensive weight management program. Researchindicates that pharmacotherapy may enhance weight loss insome overweight and obese adults"
Rating: STRONG, IMPERATIVE
www.giorgiobedogni.it

2009:#riKro#del#rimonabant#(Europa)#
• “The&Commi8ee&confirmed&that&the&risk&of&psychiatric&side&effects,&including&depression,&sleep&disorders,&anxiety&and&aggression,&is&approximately&doubled&in&pa<ents&taking&Acomplia,&compared&to&obese&or&overweight&pa<ents&taking&placebo&(a&dummy&treatment).&The&new&data&from&ongoing&studies&and&postlmarke<ng&reports&indicated&that&serious&psychiatric&disorders&may&be&more(common(than&in&the&clinical&trials&used&in&the&ini<al&assessment&of&the&medicine”&&h8p://www.ema.europa.eu/humandocs/PDFs/EPAR/acomplia/53715308en.pdf&
www.giorgiobedogni.it&
2009: ritiro del rimonabant (Europa)
• " T h e Committee confirmed that the risk of psychiatric side effects,including depression, sleep disorders, anxiety and aggression, isapproximately doubled in patients taking Acomplia, compared to obese oroverweight patients taking placebo (a dummy treatment). The new datafrom ongoing studies and post-marketing reports indicated that seriouspsychiatric disorders may be more common than in the clinical trials usedin the initial assessment of the medicine"
http://www.ema.europa.eu/humandocs/PDFs/EPAR/acomplia/53715308en.pdf
www.giorgiobedogni.it

2010:#riKro#della#sibutramina#(Europa)#
• “The&SCOUT&study&showed&an&increased&risk&of&serious&cardiovascular&events&(such&as&heart&a8ack&or&stroke)&in&pa<ents&with&known&cardiovascular&disease&taking&sibutramine”&&http://www.ema.europa.eu/pdfs/human/referral/sibutramine Sibutramine_Q&A_80817909en.pdf
www.giorgiobedogni.it&
2010: ritiro della sibutramina (Europa)
• " T h e SCOUT study showed an increased risk of serious cardiovascularevents (such as heart attack or stroke) in patients with knowncardiovascular disease taking sibutramine"
http://www.emaeuropaeuipdts/humanireferralisibutramine Sibutramine CAA 8081 7909en lodt
www.giorgiobedogni.it

2010:#riKro#della#sibutramina#(Europa)#
• “Most&of&the&pa<ents&in&the&SCOUT&study&would¬&normally&be&given&sibutramine,&as&the&medicine&is&contralindicated&in&pa<ents&with&cardiovascular&disease.&Nevertheless&the&Commi8ed&considered&that&an&increased&risk&can&also&apply&to&pa<ents&for&whom&sibutramine&can&be&prescribed&because&obese&and&overweight&pa<ents&are&likely&to&be&at&risk&of&cardiovascular&disease”&
http://www.ema.europa.eu/pdfs/human/referral/sibutramine Sibutramine_Q&A_80817909en.pdf&
www.giorgiobedogni.it&
2010: ritiro della sibutramina (Europa)
• " M o s t of the patients in the SCOUT study would not normally be givensibutramine, as the medicine is contra-indicated in patients withcardiovascular disease. Nevertheless the Committed considered that anincreased risk can also apply to patients for whom sibutramine can beprescribed because obese and overweight patients are likely to be at riskof cardiovascular disease"
http://www.emaeuropaeuipdts/humanireferralisibutramine Sibutramine CAA 8081 7909en lodt
www.giorgiobedogni.it
2010:#riKro#della#sibutramina#(Europa)#
• “Finally,&looking&at&all&of&the&studies&of&sibutramine&in&the&management&of&obesity,&the&weight&loss&achieved&with&sibutramine&treatment&is&modest&in&comparison&with&that&obtained&with&placebo,&with&pa<ents&losing&on&average&two&to&four&kilograms&more&than&with&placebo.&The&Commi8ee&also¬ed&that&it&is¬&clear&if&this&effect&on&weight&loss&can&be&maintained&when&sibutramine&treatment&is&stopped.”&
http://www.ema.europa.eu/pdfs/human/referral/sibutramine Sibutramine_Q&A_80817909en.pdf&
www.giorgiobedogni.it&
2010: ritiro della sibutramina (Europa)
• "Final ly, looking at all of the studies of sibutramine in the management ofobesity, the weight loss achieved with sibutramine treatment is modest incomparison with that obtained with placebo, with patients losing onaverage two to four kilograms more than with placebo. The Committeealso noted that it is not clear if this effect on weight loss can bemaintained when sibutramine treatment is stopped."
http://www.emaeuropaeuipdfsthumanireferraltsibutramine Si butrami ne_Q&A_8081 7909en.pdt
www.giorgiobedogni.it

Chirurgia#
• Composizione&della&dieta&• Controllo&delle&porzioni&• Frequenza&dell’alimentazione&• Pas<&sos<tu<vi&• Dieta&fortemente&ipocalorica&• Aavità&fisica&• Interven<&comportamentali&• Farmacoterapia&• Chirurgia(
www.giorgiobedogni.it&
• Composizione della dieta• Cont ro l lo delle porzioni• Frequenza dell'alimentazione• Pas t i sostitutivi• D i e t a fortemente ipocalorica• A t t i v i t a fisica• Intervent i comportamentali• Farmacoterapia• Ch i rurg la
Chirurgia
www.giorgiobedogni.it

Chirurgia#
• “Die<<ans&should&collaborate&with&other&members&of&the&health&care&team®arding&the&appropriateness&of&bariatric&surgery&for&people&who&have¬&achieved&weight&loss&goals&with&less&invasive&weight&loss&methods&and&who&meet&the&NHLBI&criteria”(((Ra<ng:&STRONG,&IMPERATIVE&
&&Seagle&et&al.&JADA(2009;109:339&
www.giorgiobedogni.it&
Rating: STRONG, IMPERATIVE
Seagle et al. JADA 2009;109:339
Chirurgia
• "Dietitians should collaborate with other members of thehealth care team regarding the appropriateness of bariatricsurgery for people who have not achieved weight loss goalswith less invasive weight loss methods and who meet theNFILEil criteria"
www.giorgiobedogni.it
ADA#Weight#Management#PracKce#Guideline#
h8p://andevidencelibrary.com/topic.cfm?cat=3014&(last&updated&2009;&under&revision)&
&
www.giorgiobedogni.it&
ADA Weight Management Practice Guideline
http://andevidencelibrary.comitopic.cfm?cat=3014(last updated 2009; under revision)
www.giorgiobedogni.it

ClassificaKon#of#Overweight#and#Obesity#
• Body&mass&index&(BMI)&and&waist&circumference&should&be&used&to&classify&overweight&and&obesity,&es<mate&risk&for&disease,&and&to&iden<fy&treatment&op<ons.&&
• BMI&and&waist&circumference&are&highly&correlated&to&obesity&or&fat&mass&and&risk&of&other&diseases&(NHLBI&report).&
• Fair,&Impera<ve&
www.giorgiobedogni.it&
Classification of Overweight and Obesity
• Body mass index (BMI) and waist circumference should beused to classify overweight and obesity, estimate risk fordisease, and to identify treatment options.
• B M I and waist circumference are highly correlated to obesityor fat mass and risk of other diseases (1\11-1LBI report).
• Fair, Imperative
www.giorgiobedogni.it

ClassificaKon#of#Overweight#and#Obesity#
• Body&weight&and&waist&circumference&should&be&used&to&determine&the&effec<veness&of&therapy&in&the&reassessment.&
• BMI&and&waist&circumference&are&highly&correlated&to&obesity&or&fat&mass&(NHLBI&report).&
• Fair,&Impera<ve&
www.giorgiobedogni.it&
Classification of Overweight and Obesity
• Body weight and waist circumference should be used todetermine the effectiveness of therapy in the reassessment.
• B M I and waist circumference are highly correlated to obesityor fat mass (1\11-1LBI report).
• Fair, Imperative
www.giorgiobedogni.it
Comprehensive#Weight#Management#Program#
• Weight&loss&and&weight&maintenance&therapy&should&be&based&on&a&comprehensive&weight&management&program&including&diet,&physical&ac<vity,&and&behavior&therapy.&&
• The&combina<on&therapy&is&more&successful&than&using&any&one&interven<on&alone.&
&• Strong,&Impera<ve&
www.giorgiobedogni.it&
Comprehensive Weight Management Program
• Weight loss and weight maintenance therapy should be basedon a comprehensive weight management program includingdiet, physical activity, and behavior therapy.
• The combination therapy is more successful than using anyone intervention alone.
• Strong, Imperative
www.giorgiobedogni.it

OpKmal#Length#of#Therapy#
• MNT&for&weight&loss&should&last&at&least&6&months&or&un<l&weight&loss&goals&are&achieved,&with&implementa<on&of&a&weight&maintenance&program&aner&that&<me.&&
• A&greater&frequency&of&contacts&between&the&pa<ent&and&prac<<oner&may&lead&to&more&successful&weight&loss&and&maintenance.&
&• Strong,&Impera<ve&
www.giorgiobedogni.it&
Optimal Length of Therapy
• M N I for weight loss should last at least 6 months or untilweight loss goals are achieved, with implementation of aweight maintenance program after that time.
• A greater frequency of contacts between the patient andpractitioner may lead to more successful weight loss andmaintenance.
• Strong, Imperative
www.giorgiobedogni.it

RealisKc#Weight#Goals#
• Individualized&goals&of&weight&loss&therapy&should&be&to&reduce&body&weight&at&an&op<mal&rate&of&1l2&lbs&per&week&for&the&first&6&months&and&to&achieve&an&ini<al&weight&loss&goal&of&up&to&10%&from&baseline.&&
• These&goals&are&realis<c,&achievable,&and&sustainable.&&• Strong,&Impera<ve&
www.giorgiobedogni.it&
Realistic Weight Goals
• Individualized goals of weight loss therapy should be toreduce body weight at an optimal rate of 1-2 lbs per week forthe first 6 months and to achieve an initial weight loss goal ofup to 10% from baseline.
• These goals are realistic, achievable, and sustainable.
• Strong, Imperative
www.giorgiobedogni.it

Determining#Energy#Needs#
• Es<mated&energy&needs&should&be&based&on&RMR.&If&possible,&RMR&should&be&measured&(e.g.,&indirect&calorimetry).&&
• If&RMR&cannot&be&measured,&then&the&MifflinlSt.&Jeor&equa<on&using&actual&weight&is&the&most&accurate&for&es<ma<ng&RMR&for&overweight&and&obese&individuals.&
&• Strong,&Condi<onal&
www.giorgiobedogni.it&
Determining Energy Needs
• Estimated energy needs should be based on RMR. If possible,RMR should be measured (e.g., indirect calorimetry).
• I f RMR cannot be measured, then the Mifflin-St. Jeor equationusing actual weight is the most accurate for estimating RMRfor overweight and obese individuals.
• Strong, Conditional
www.giorgiobedogni.it

*Formule#predi5ve#
www.giorgiobedogni.it&
*Formule predittive
Relationship Between Basal Metabolic Rate,Gender, Age, and Body Compositionin 8,780 White Obese SubjectsStefano Lazzer1'2, Giorgio Bedogni3, Claudio L. Lafortune, Nicoletta Marazzi', Carlo Busti',Raffaela Galli', Alessandra De Col', Florenza Agostil and Alessandro Sartorio'5
Obesity (2(109) 18, 71-78. dc4:1 a 1 038/oloy.2009.162
www.giorgiobedogni.it
*Formule#predi5ve#
www.giorgiobedogni.it&
*Formule predittive
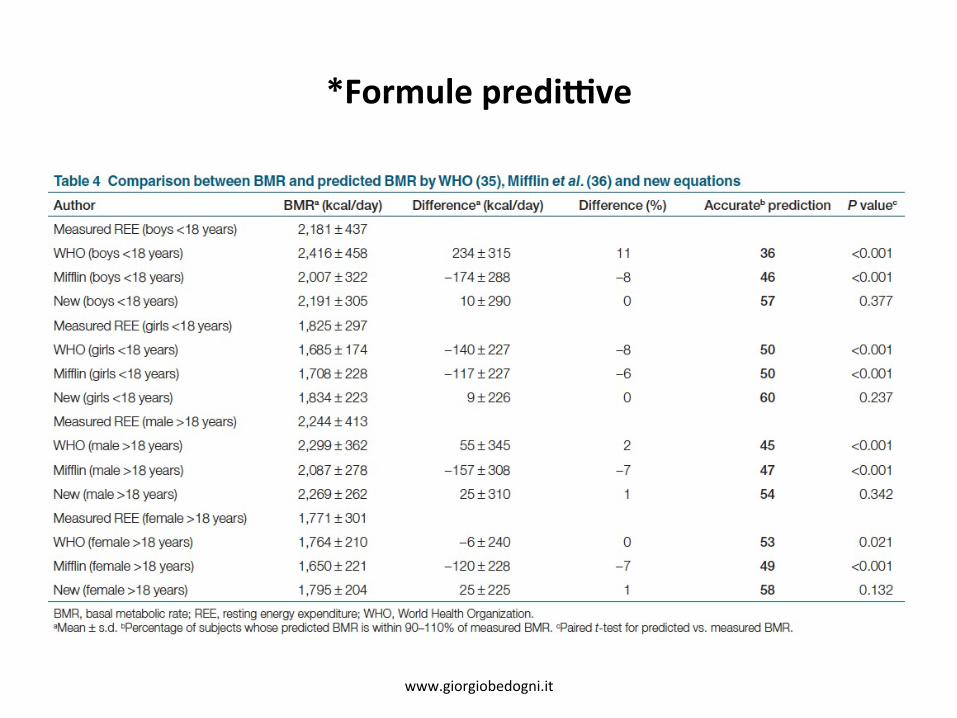
Author BMR (kcal/day) Difference' (kcal/day) Difference (%) Accurateb prediction P value'
Measured REE (boys <18 years) 2,181 ± 437
WHO (boys <18 years) 2,416 ± 458 234 ± 315 11 36 <0.001
Mifflin (boys <18 years) 2,007 ± 322 -174 ± 288 -8 46 <0.001
New (boys <18 years) 2,191 ± 305 10 ± 290 0 57 0.377
Measured REE (girls <18 years) 1,825 ± 297WHO (girls <18 years) 1,685± 174 -140 ± 227 -8 50 <0.001Mifflin (girls <18 years) 1,708 ± 228 -117±227 -6 50 <0.001
New (girls <18 years) 1,834 ± 223 9 ± 226 0 60 0.237
Measured REE (male >18 years) 2,244 ± 413WHO (male >18 years) 2,299 ± 362 55 ± 345 2 45 <0.001
Mifflin (male >18 years) 2,087 ± 278 -157± 308 -7 47 <0.001New (male >18 years) 2,269 ± 262 25± 310 1 54 0.342
Measured REE (female >18 years) 1,771 ± 301
WHO (female >18 years) 1,764 ± 210 -6 ± 240 0 53 0.021
Mifflin (female >18 years) 1,650 ± 221 -120 ± 228 -7 49 <0.001New (female >18 years) 1,795 ± 204 25 ± 225 1 58 0.132
Table 4 Comparison between BMR and predicted BMR by WHO (35). Mifflin etal. (36) and new equations
BMR, basal metabolic rate; REE, resting energy expenditure; WHO, World Health Organization.'Mean ± s.d, ,Percentage of subjects whose predicted BMR is within go--1-101'/o of measured BMR. 'Pared t-test for predicted vs. measured BMR.
www.glorglobedogni.it

Reduced#Calorie#Diet#
• An&individualized&reduced&calorie&diet&is&the&basis&of&the&dietary&component&of&a&comprehensive&weight&management&program.&&
• Reducing&dietary&fat&and/or&carbohydrates&is&a&prac<cal&way&to&create&a&caloric&deficit&of&500&–&1000&kcals&below&es<mated&energy&needs&and&should&result&in&a&weight&loss&of&1&–&2&lbs&per&week.&
&• Strong,&Impera<ve&
www.giorgiobedogni.it&
Reduced Calorie Diet
• A n individualized reduced calorie diet is the basis of thedietary component of a comprehensive weight managementprogram.
• Reducing dietary fat and/or carbohydrates is a practical wayto create a caloric deficit of 500 — 1000 kcals below estimatedenergy needs and should result in a weight loss of 1— 2 lbsper week.
• Strong, Imperative
www.giorgiobedogni.it
EaKng#Frequency#and#PaSerns#
• Total&caloric&intake&should&be&distributed&throughout&the&day,&with&the&consump<on&of&4&to&5&meals/snacks&per&day&including&breakfast.&&
• Consump<on&of&greater&energy&intake&during&the&day&may&be&preferable&to&evening&consump<on.&
&• Fair,&Impera<ve&
www.giorgiobedogni.it&
Eating Frequency and Patterns
• To ta l caloric intake should be distributed throughout the day,with the consumption of 4 to 5 meals/snacks per dayincluding breakfast.
• Consumption of greater energy intake during the day may bepreferable to evening consumption.
• Fair, Imperative
www.giorgiobedogni.it
PorKon#Control#
• Por<on&control&should&be&included&as&part&of&a&comprehensive&weight&management&program.&Por<on&control&at&meals&and&snacks&results&in&reduced&energy&intake&and&weight&loss.&
• Fair,&Impera<ve&
www.giorgiobedogni.it&
• Portion control should be included as part of a comprehensiveweight management program. Portion control at meals andsnacks results in reduced energy intake and weight loss.
• Fair, Imperative
Portion Control
www.giorgiobedogni.it
Meal#Replacements#
• For&people&who&have&difficulty&with&self&selec<on&and/or&por<on&control,&meal&replacements&(e.g.,&liquid&meals,&meal&bars,&calorielcontrolled&packaged&meals)&may&be&used&as&part&of&the&diet&component&of&a&comprehensive&weight&management&program.&&
• Subs<tu<ng&one&or&two&daily&meals&or&snacks&with&meal&replacements&is&a&successful&weight&loss&and&weight&maintenance&strategy.&
&• Strong,&Condi<onal&
www.giorgiobedogni.it&
• Strong, Conditional
Meal Replacements
• F o r people who have difficulty with self selection and/orportion control, meal replacements (e.g., liquid meals, mealbars, calorie-controlled packaged meals) may be used as partof the diet component of a comprehensive weightmanagement program.
• Substituting one or two daily meals or snacks with mealreplacements is a successful weight loss and weightmaintenance strategy.
www.giorgiobedogni.it
NutriKon#EducaKon#
• Nutri<on&educa<on&should&be&individualized&and&included&as&part&of&the&diet&component&of&a&comprehensive&weight&management&program.&&
• Short&term&studies&show&that&nutri<on&educa<on&(e.g.&reading&nutri<on&labels,&recipe&modifica<on,&cooking&classes)&increases&knowledge&and&may&lead&to&improved&food&choices.&
• Fair,&Impera<ve&
www.giorgiobedogni.it&
Nutrition Education
• Nutri t ion education should be individualized and included aspart of the diet component of a comprehensive weightmanagement program.
• Short term studies show that nutrition education (e.g. readingnutrition labels, recipe modification, cooking classes)increases knowledge and may lead to improved food choices.
• Fair, Imperative
www.giorgiobedogni.it

Low#Glycemic#Index#Diets#
• A&low&glycemic&index&diet&is¬&recommended&for&weight&loss&or&weight&maintenance&as&part&of&a&comprehensive&weight&management&program,&since&it&has¬&been&shown&to&be&effec<ve&in&these&areas.&
• Strong,&Impera<ve&
www.giorgiobedogni.it&
Low Glycemic Index Diets
• A low glycemic index diet is not recommended for weight lossor weight maintenance as part of a comprehensive weightmanagement program, since it has not been shown to beeffective in these areas.
• Strong, Imperative
www.giorgiobedogni.it

Dairy/Calcium#and#Weight#Management#
• In&order&to&meet¤t&nutri<onal&recommenda<ons,&incorporate&3l4&servings&of&low&fat&dairy&foods&a&day&as&part&of&the&diet&component&of&a&comprehensive&weight&management&program.&&
• Research&suggests&that&calcium&intake&lower&than&recommended&levels&is&associated&with&increased&body&weight.&&
• However,&the&effect&of&dairy&and/or&calcium&at&or&above&recommended&levels&on&weight&management&is&unclear.&
&• &Fair,&Impera<ve&
www.giorgiobedogni.it&
Dairy/Calcium and Weight Management
• I n order to meet current nutritional recommendations, incorporate3-4 servings of low fat dairy foods a day as part of the dietcomponent of a comprehensive weight management program.
• Research suggests that calcium intake lower than recommendedlevels is associated with increased body weight.
• However, the effect of dairy and/or calcium at or aboverecommended levels on weight management is unclear.
• F a i r , Imperative
www.giorgiobedogni.it
Low#Carbohydrate#Diet#
• Having&pa<ents&focus&on&reducing&carbohydrates&rather&than&reducing&calories&and/or&fat&may&be&a&short&term&strategy&for&some&individuals.&&
• Research&indicates&that&focusing&on&reducing&carbohydrate&intake&(<35%&of&kcals&from&carbohydrates)&results&in&reduced&energy&intake.&&
• Consump<on&of&a&lowlcarbohydrate&diet&is&associated&with&a&greater&weight&and&fat&loss&than&tradi<onal&reduced&calorie&diets&during&the&first&6&months,&but&these&differences&are¬&significant&aner&1&year.&
• Fair,&Condi<onal&
www.giorgiobedogni.it&
Low Carbohydrate Diet
• Having patients focus on reducing carbohydrates rather thanreducing calories and/or fat may be a short term strategy for someindividuals.
• Research indicates that focusing on reducing carbohydrate intake(<35% of kcals from carbohydrates) results in reduced energyintake.
• Consumption of a low-carbohydrate diet is associated with agreater weight and fat loss than traditional reduced calorie dietsduring the first 6 months, but these differences are not significantafter 1 year.
• Fa i r, Conditional
www.giorgiobedogni.it

Physical#AcKvity#
• Physical&ac<vity&should&be&part&of&a&comprehensive&weight&management&program.&Physical&ac<vity&level&should&be&assessed&and&individualized&longlterm&goals&established&to&accumulate&at&least&30&minutes&or&more&of&moderate&intensity&physical&ac<vity&on&most,&and&preferably,&all&days&of&the&week,&unless&medically&contraindicated.&&
• Physical&ac<vity&contributes&to&weight&loss,&may&decrease&abdominal&fat,&and&may&help&with&maintenance&of&weight&loss.&
• Strong,&Impera<ve&
www.giorgiobedogni.it&
• Strong, Imperative
Physical Activity
• Physical activity should be part of a comprehensive weightmanagement program. Physical activity level should beassessed and individualized long-term goals established toaccumulate at least 30 minutes or more of moderate intensityphysical activity on most, and preferably, all days of the week,unless medically contraindicated.
• Physical activity contributes to weight loss, may decreaseabdominal fat, and may help with maintenance of weight loss.
www.giorgiobedogni.it

MulKple#Behavior#Therapy#Strategies#
• A&comprehensive&weight&management&program&should&make&maximum&use&of&mul<ple&strategies&for&behavior&therapy&(e.g.&self&monitoring,&stress&management,&s<mulus&control,&problem&solving,&con<ngency&management,&cogni<ve&restructuring,&and&social&support).&&
• Behavior&therapy&in&addi<on&to&diet&and&physical&ac<vity&leads&to&addi<onal&weight&loss.&&
• Con<nued&behavioral&interven<ons&may&be&necessary&to&prevent&a&return&to&baseline&weight.&
• Strong,&Impera<ve&
www.giorgiobedogni.it&
• Strong, Imperative
Multiple Behavior Therapy Strategies
• A comprehensive weight management program should makemaximum use of multiple strategies for behavior therapy (e.g. selfmonitoring, stress management, stimulus control, problem solving,contingency management, cognitive restructuring, and socialsupport).
• Behavior therapy in addition to diet and physical activity leads toadditional weight loss.
• Continued behavioral interventions may be necessary to prevent areturn to baseline weight.
www.giorgiobedogni.it
Use#of#Weight#Loss#MedicaKons#
• FDAlapproved&weight&loss&medica<ons&may&be&part&of&a&comprehensive&weight&management&program.&&
• Die<<ans&should&collaborate&with&other&members&of&the&health&care&team®arding&the&use&of&FDAlapproved&weight&loss&medica<ons&for&people&who&meet&the&NHLBI&criteria.&
• Research&indicates&that&pharmacotherapy&may&enhance&weight&loss&in&some&overweight&and&obese&adults.&
www.giorgiobedogni.it&
Use of Weight Loss Medications
• FDA-approved weight loss medications may be part of acomprehensive weight management program.
• Dietitians should collaborate with other members of thehealth care team regarding the use of FDA-approved weightloss medications for people who meet the NHLBI criteria.
• Research indicates that pharmacotherapy may enhanceweight loss in some overweight and obese adults.
www.giorgiobedogni.it

Bariatric#Surgery#for#Weight#Loss#
• Die<<ans&should&collaborate&with&other&members&of&the&health&care&team®arding&the&appropriateness&of&bariatric&surgery&for&people&who&have¬&achieved&weight&loss&goals&with&less&invasive&weight&loss&methods&and&who&meet&the&NHLBI&criteria.&&
• Separate&ADA&evidence&based&guidelines&are&being&developed&on&nutri<on&care&in&bariatric&surgery.&
• &Strong,&Impera<ve&
www.giorgiobedogni.it&
Bariatric Surgery for Weight Loss
• Dietitians should collaborate with other members of thehealth care team regarding the appropriateness of bariatricsurgery for people who have not achieved weight loss goalswith less invasive weight loss methods and who meet theNFILEil criteria.
• Separate ADA evidence based guidelines are being developedon nutrition care in bariatric surgery.
• Strong, Imperative
www.giorgiobedogni.it

Grazie#
www.giorgiobedogni.it&
Grazie
www.giorgiobedogni.it