HOT TOPICS MALATTIA METASTATICA - Over Group Provider … · HOT TOPICS MALATTIA METASTATICA...
31
Transcript of HOT TOPICS MALATTIA METASTATICA - Over Group Provider … · HOT TOPICS MALATTIA METASTATICA...

HOT TOPICS MALATTIA METASTATICA
Terapia delle metastasi
Alfredo BerrutiUniversità degli Studi
di BresciaAzienda Ospedaliera
Spedali CiviliBrescia
Quando è indicato il trattamentoQuando è indicato il trattamento con ac. zoledronico?
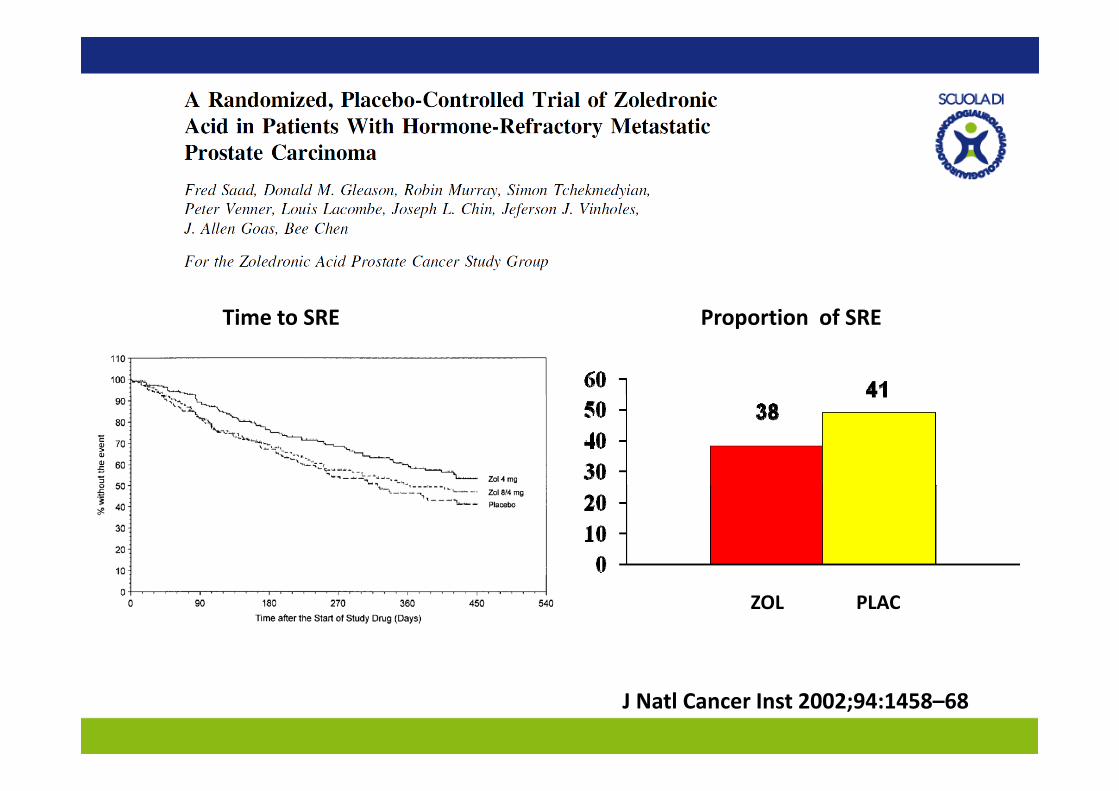
Time to SRE Proportion of SRE
ZOL PLAC
J Natl Cancer Inst 2002;94:1458–68

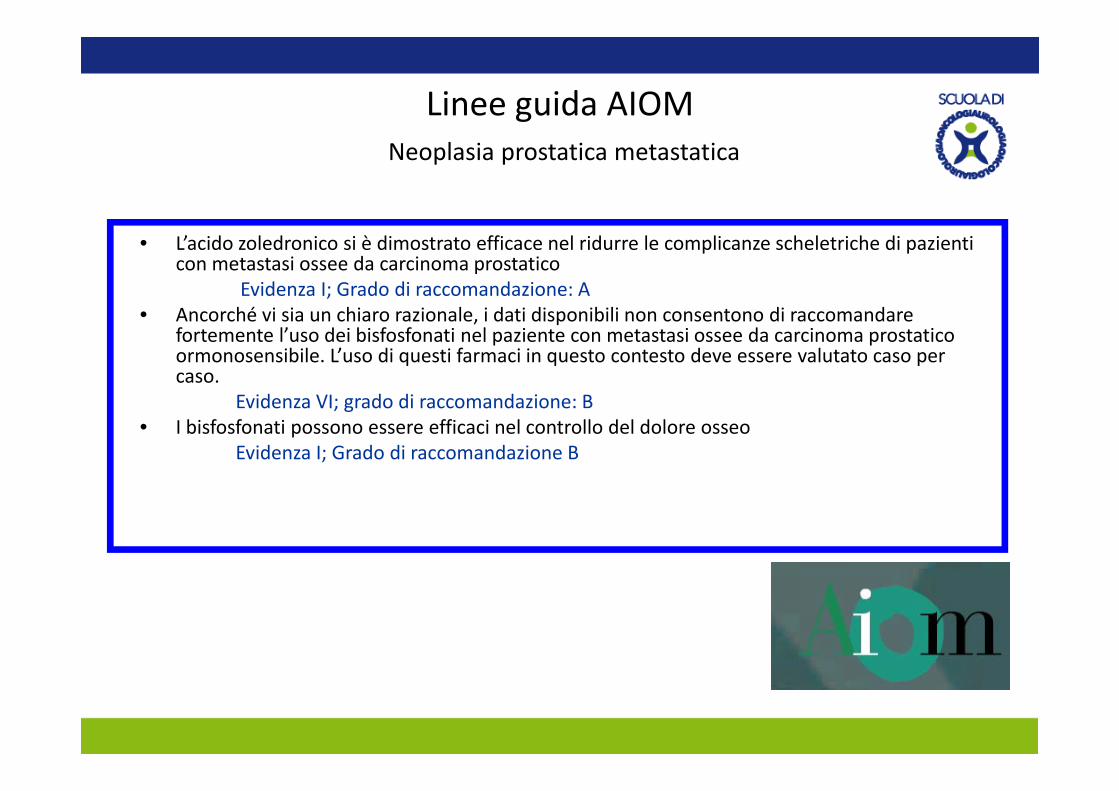
Linee guida AIOM Neoplasia prostatica metastatica
• L’acido zoledronico si è dimostrato efficace nel ridurre le complicanze scheletriche di pazienti con metastasi ossee da carcinoma prostatico
Evidenza I; Grado di raccomandazione: A• Ancorché vi sia un chiaro razionale, i dati disponibili non consentono di raccomandare
fortemente l’uso dei bisfosfonati nel paziente con metastasi ossee da carcinoma prostatico ormonosensibile. L’uso di questi farmaci in questo contesto deve essere valutato caso per caso.
E id VI d di d i BEvidenza VI; grado di raccomandazione: B• I bisfosfonati possono essere efficaci nel controllo del dolore osseo
Evidenza I; Grado di raccomandazione B
Quale paziente deve essere avviato a trattamento con acido zoledronico?a trattamento con acido oledronico?
Il paziente a rischio di complicanze scheletriche:Il paziente a rischio di complicanze scheletriche:
Estensione di malattiaEstensione di malattia
Dolore osseoDolore osseo
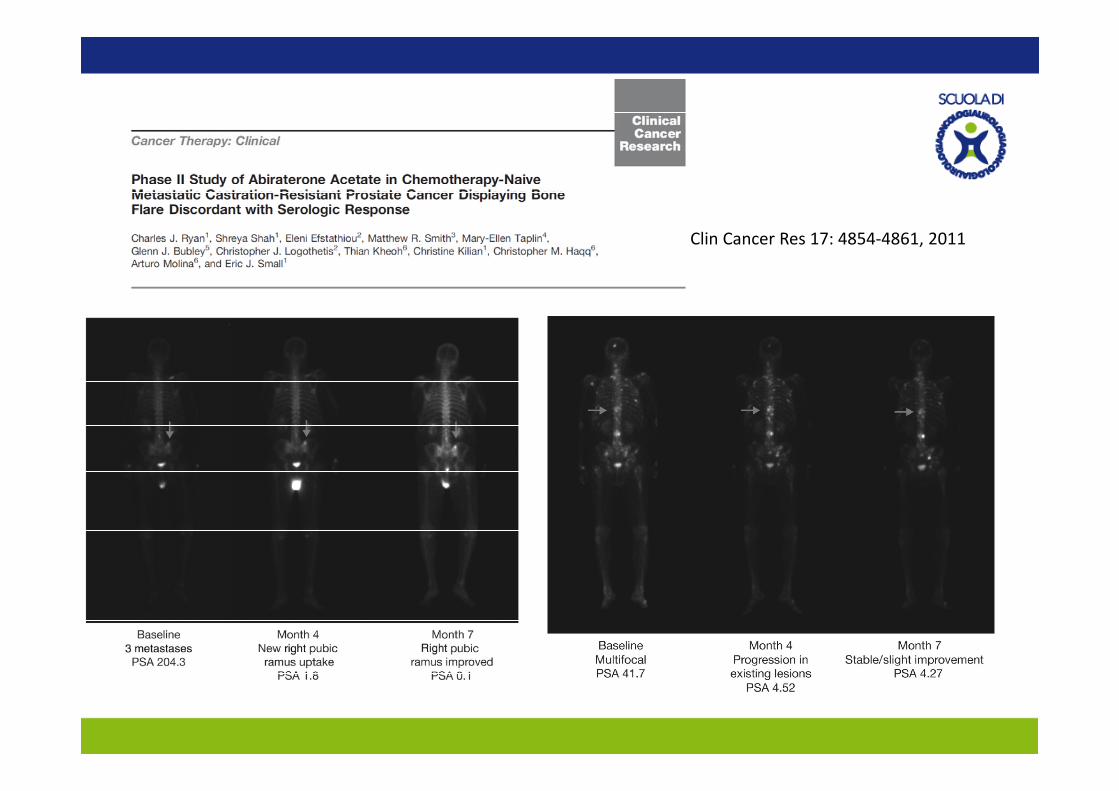
Clin Cancer Res 17: 4854‐4861, 2011
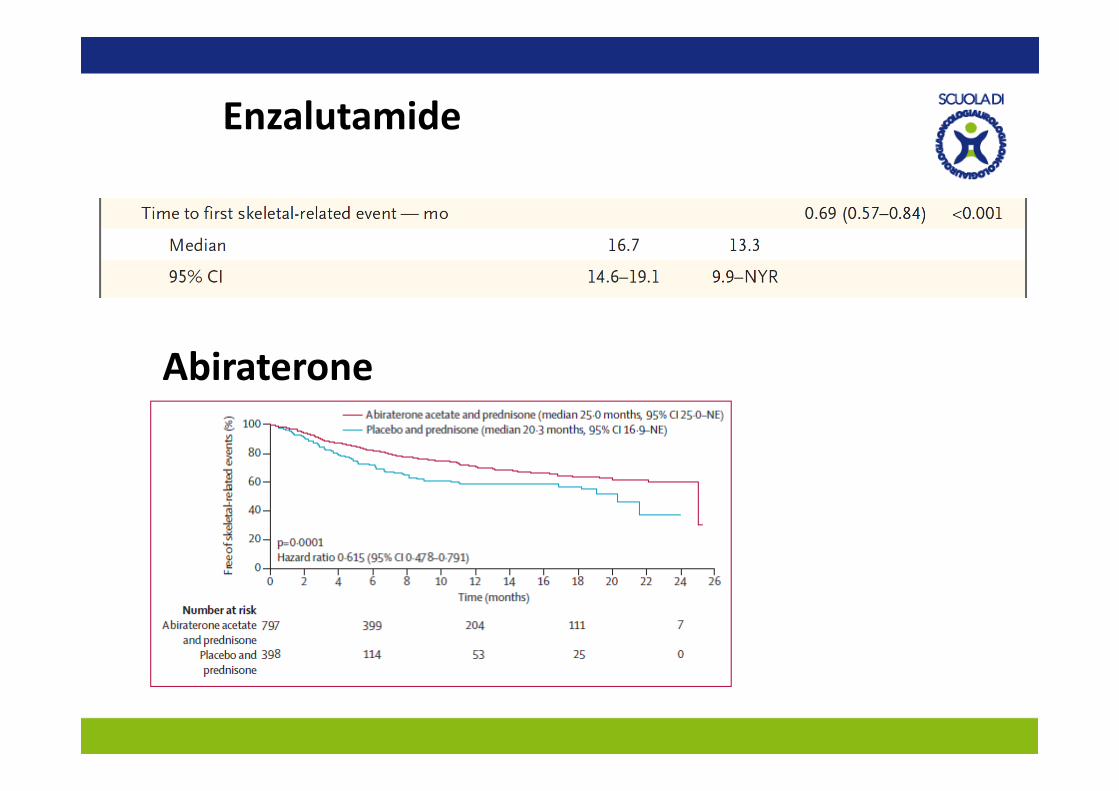
EnzalutamideEnzalutamide
Abiraterone
Bisogna utilizzare supplementazioni di calcio e vitamina D durante la terapia con difosfonati?
VITAMIN D SUPPLEMENTATION AND BISPHOSPHONATESVITAMIN D SUPPLEMENTATION AND BISPHOSPHONATES IN OSTEOPOROTIC PATIENTS
Vitamin D supplementation is mandatory in association withBisphosphonates in osteoporotic patients with vitamin D Deficiency and insufficiency
Controversial role in patients with vitamin D in the normal range
Carmel AS, Osteoporos Int. 2012; 23(10):2479-87Bourke S et al Osteoporos Int. 2013; 24(1):349-54
1. The total daily intake of elemental calcium (through diet and supplements) for individuals over age 50 should be 1200 mg [grade B].
2. For healthy adults at low risk of vitamin D deficiency, routine supplementation with 400–1000 IU (10–25 μg) vitamin D3 daily is recommended [grade D].
3 F d lt 50 t d t i k f it i D d fi i l t ti ith 8003. For adults over age 50 at moderate risk of vitamin D deficiency, supplementation with 800–1000 IU (20–25 μg) vita min D3 daily is recommended. To achieve optimal vitamin D status, daily supplementation with more than 1000 IU (25 μg) may be required. Daily doses up to 2000 IU (50μg) are safe and do not necessitate monitoring [grade C].( μg) g [g ]
4. For individuals receiving pharmacologic therapy for osteoporosis, measurement of serum 25-hydroxyvitamin D should follow three to four months of adequate supplementation and should
t b t d if ti l l l ( 75 l/L) i hi d [ d D]not be repeated if an optimal level (ε 75 nmol/L) is achieved [grade D].
Linee guida AIOMLinee guida AIOM
Take home message: A tutti i pazienti che effettuano bisfosfonati per via endovenosa o orale è raccomandata una supplementazione di calcio e vitamina D. E’ lt b bil h l d i d t 500 di l i 400 UIE’ molto probabile che le dosi raccomandate: 500 mg di calcio e 400 UI non siano adeguate e debbano essere raddoppiate. E’ consigliabile somministrare a tutti i pazienti oncologici che devono iniziare una terapia con bifosfonati una dose di 1000 UI al giorno di vitamina D p ge di 500 mg al giorno di calcio, possibilmente in formulazioni farmaceutiche separate. Utile monitoraggio di calcemia (ionizzata o corretta per albumina) durante il t tt t bi f f ti l fi di l i i l i i iil trattamento con bisfosfonati al fine di correggere valori ipocalcemici severi.
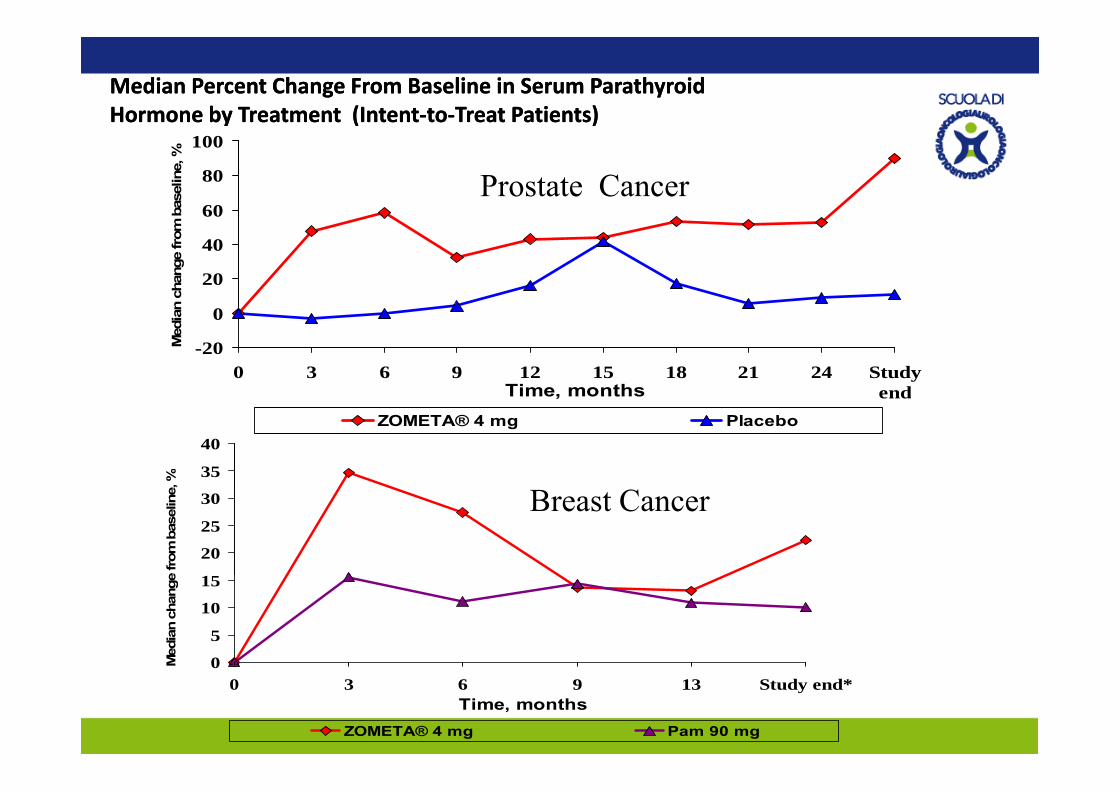
Median Percent Change From Baseline in Serum Parathyroid Median Percent Change From Baseline in Serum Parathyroid Hormone by Treatment (IntentHormone by Treatment (Intent‐‐toto‐‐Treat Patients)Treat Patients)
60
80
100
base
line,
%Prostate Cancer
20
40
60
n ch
ange
from
-20
0
0 3 6 9 12 15 18 21 24 StudyendTime, months
Med
ian
35
40
, %
endTime, monthsZOMETA® 4 mg Placebo
20
25
30
e fro
m b
asel
ine, Breast Cancer
0
5
10
15
Med
ian
chan
ge
00 3 6 9 13 Study end*
Time, months
M
ZOMETA® 4 mg Pam 90 mg
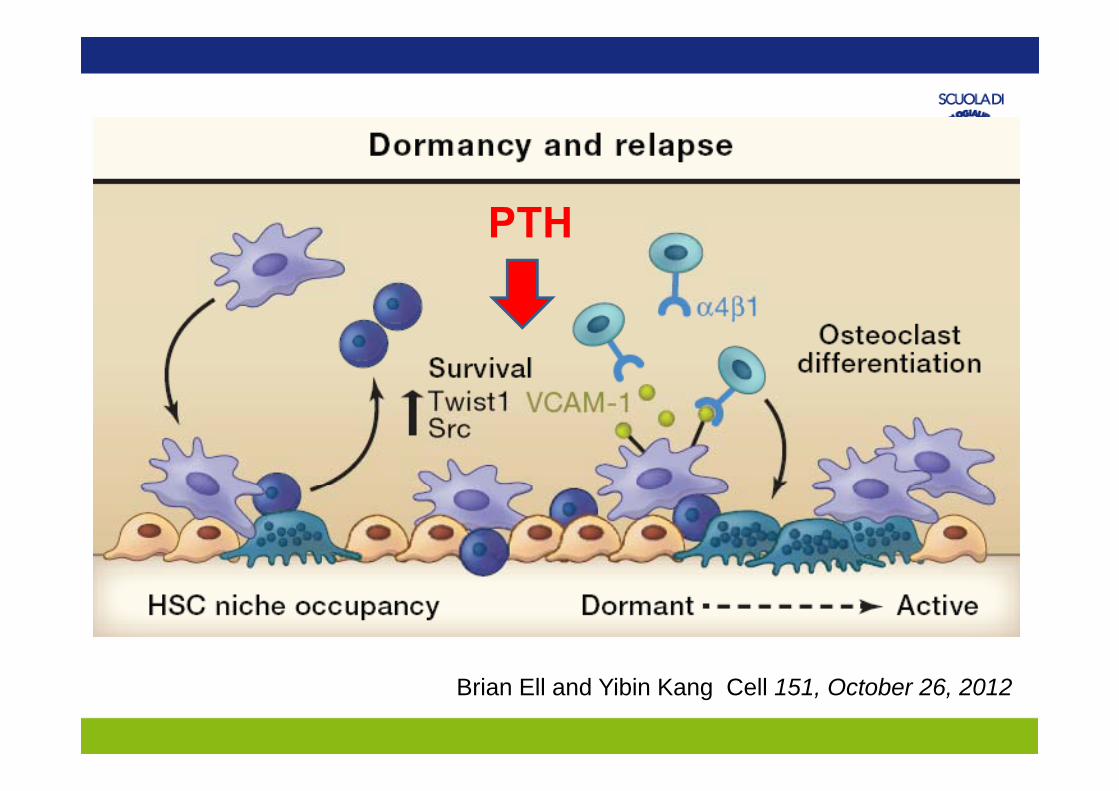
PTHPTH
Brian Ell and Yibin Kang Cell 151, October 26, 2012
2012;17: 645-652.
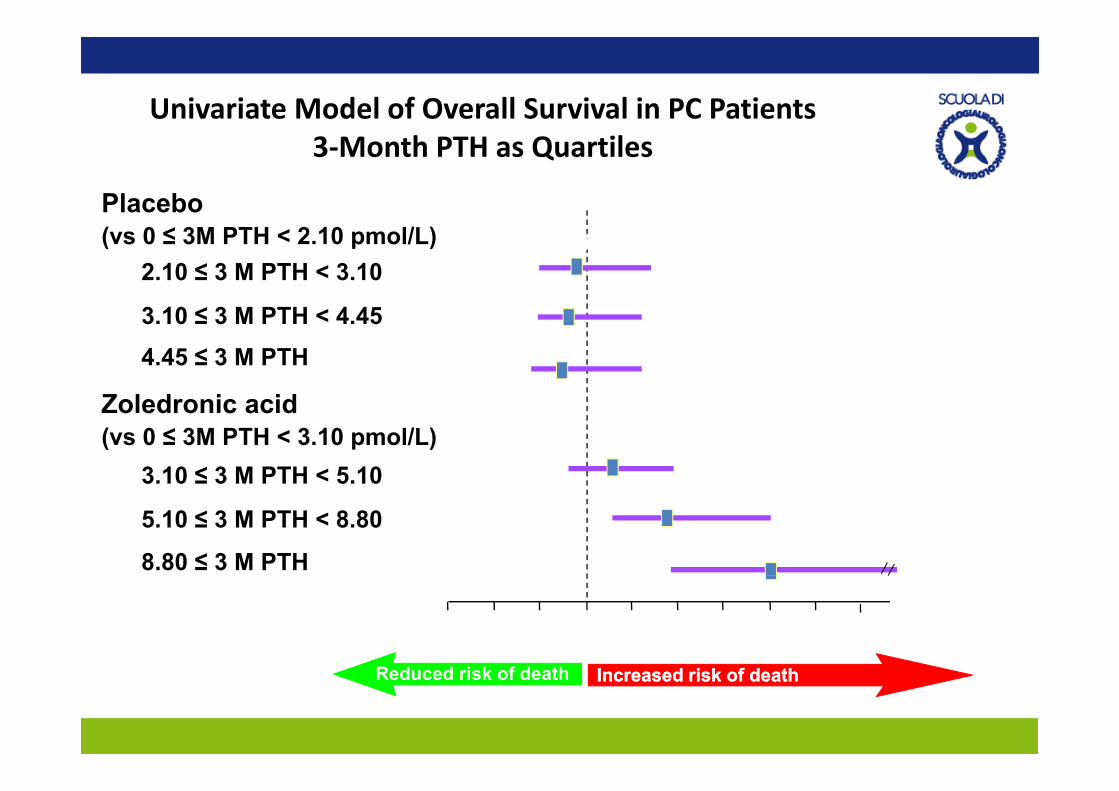
Univariate Model of Overall Survival in PC Patients3‐Month PTH as Quartiles
Placebo P value
.7040.89(vs 0 ≤ 3M PTH < 2.10 pmol/L)
4450.80
2.10 ≤ 3 M PTH < 3.10.445
.4010.77
3.10 ≤ 3 M PTH < 4.454.45 ≤ 3 M PTH
Z l d i id
.2741.30
Zoledronic acid(vs 0 ≤ 3M PTH < 3.10 pmol/L)
3.10 ≤ 3 M PTH < 5.10.006
1.88
<.00013.04
5.10 ≤ 3 M PTH < 8.80
8.80 ≤ 3 M PTH
0 1.0Risk ratio
2.0 3.0 4.0
(4.7)
Reduced risk of death Increased risk of deathIncreased risk of death
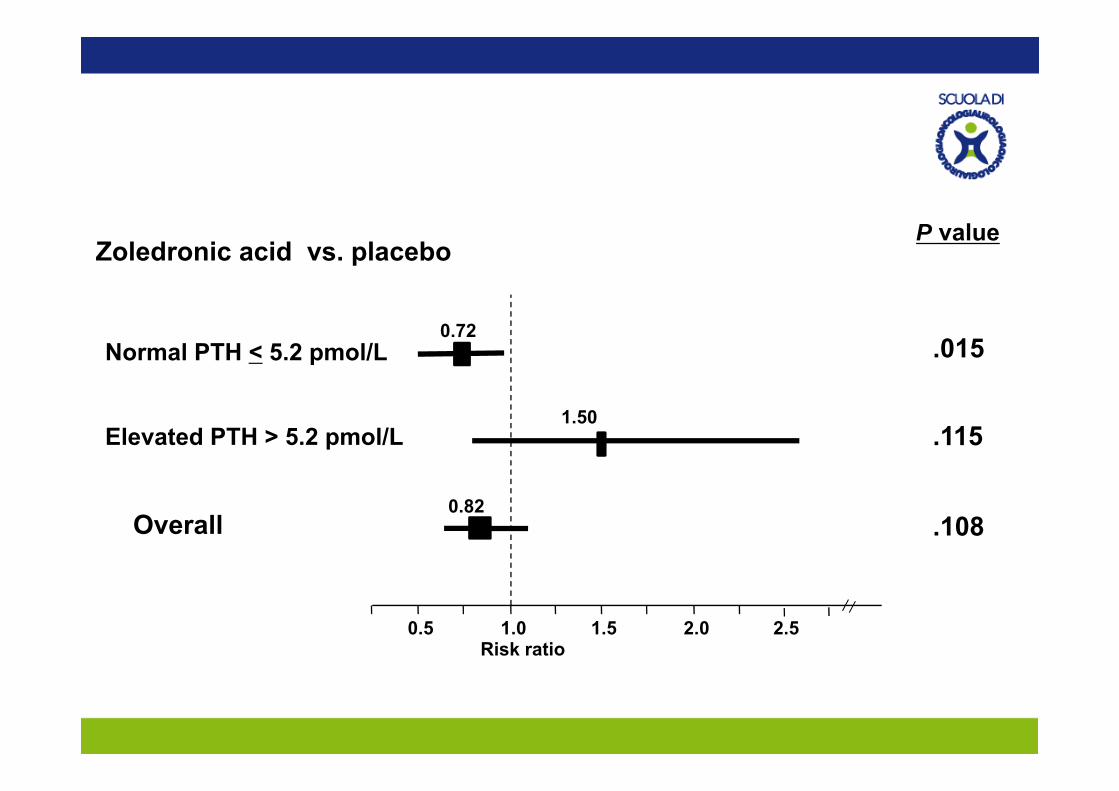
Zoledronic acid vs. placeboP value
.0150.72
Normal PTH < 5.2 pmol/L
.1151.50
Elevated PTH > 5.2 pmol/L
.1080.82
Overall
0.5 1.0Risk ratio
1.5 2.0 2.5
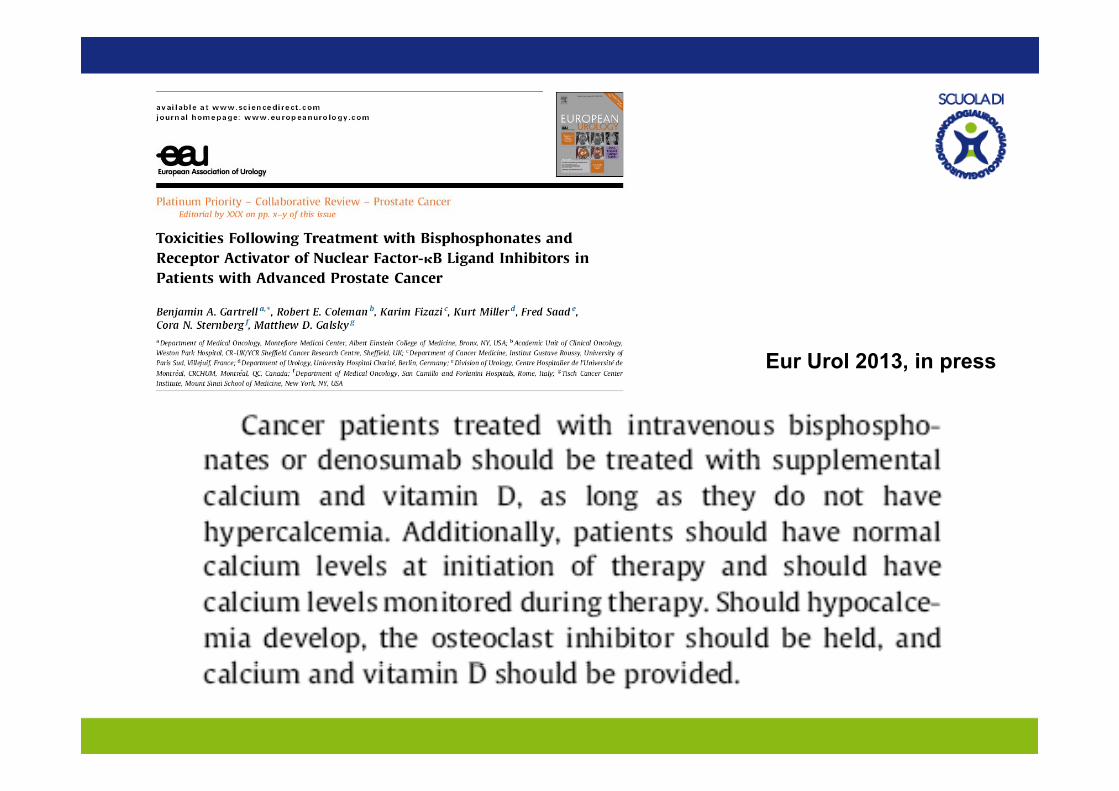
Eur Urol 2013, in press
Quale sarà il ruolo del Denosumab: la 1° linea di trattamento, l’associazione l’ac. zoledronico, o la 2° linea?
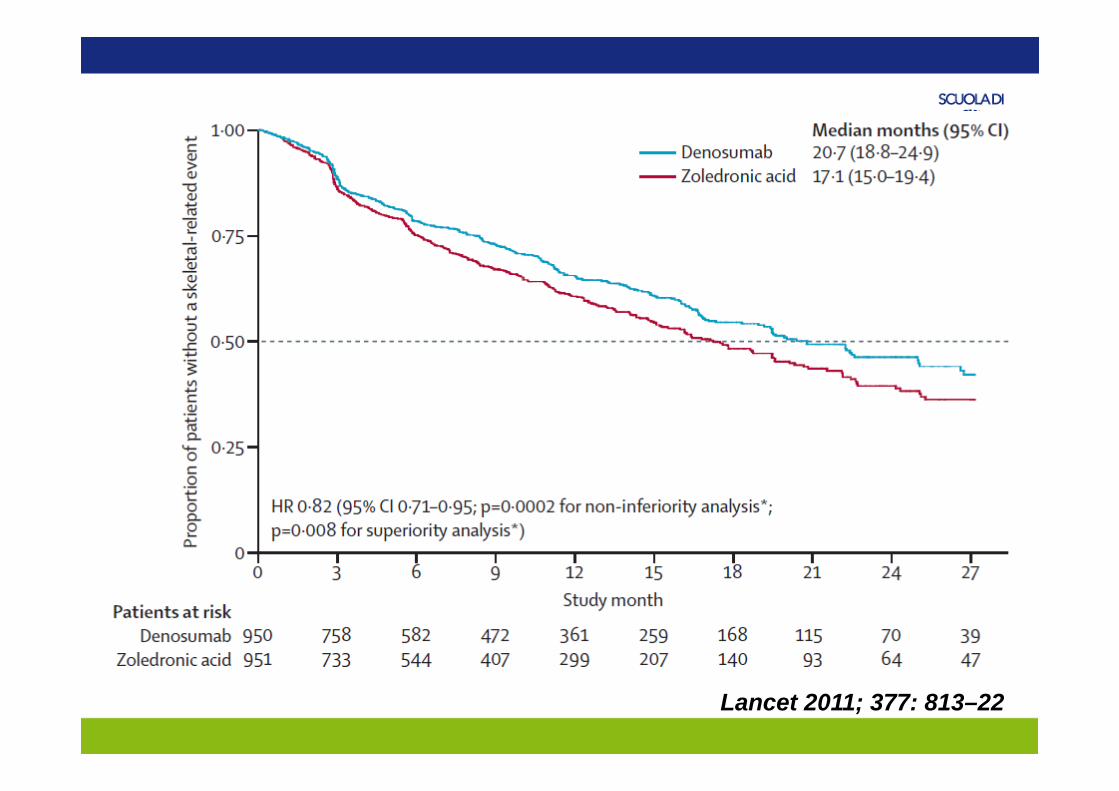
Lancet 2011; 377: 813–22
DenosumabMaggior efficacia
Ac ZoledronicoMinori costi
Denosumab is superior to zoledronic acid in delaying SREs. p y g
The toxicity profile of denosumab lacks nephrotoxicity and acute-phase reactions. However, hypocalcemia is more common with denosumab.
In patients with severe renal dysfunction (GFR <30 ml/min), zoledronic acid is contraindicated.
In patients with more modest degrees of renal impairment, if potential h t i it i th d b b f dnephrotoxicity is a concern, then denosumab may be favored.
While denosumab lacks nephrotoxicity and is not metabolized by the kidneys there is concern that rates of hypocalcemia may be higher in thekidneys, there is concern that rates of hypocalcemia may be higher in the setting of severe renal dysfunction.
PAZIENTE CON CARCINOMA PROSTATICOCON METASTASI OSSEECON METASTASI OSSEE
QUALI INDICAZIONI PER DENOSUMAB?
Alto rischio di SRE
Insufficienza renale
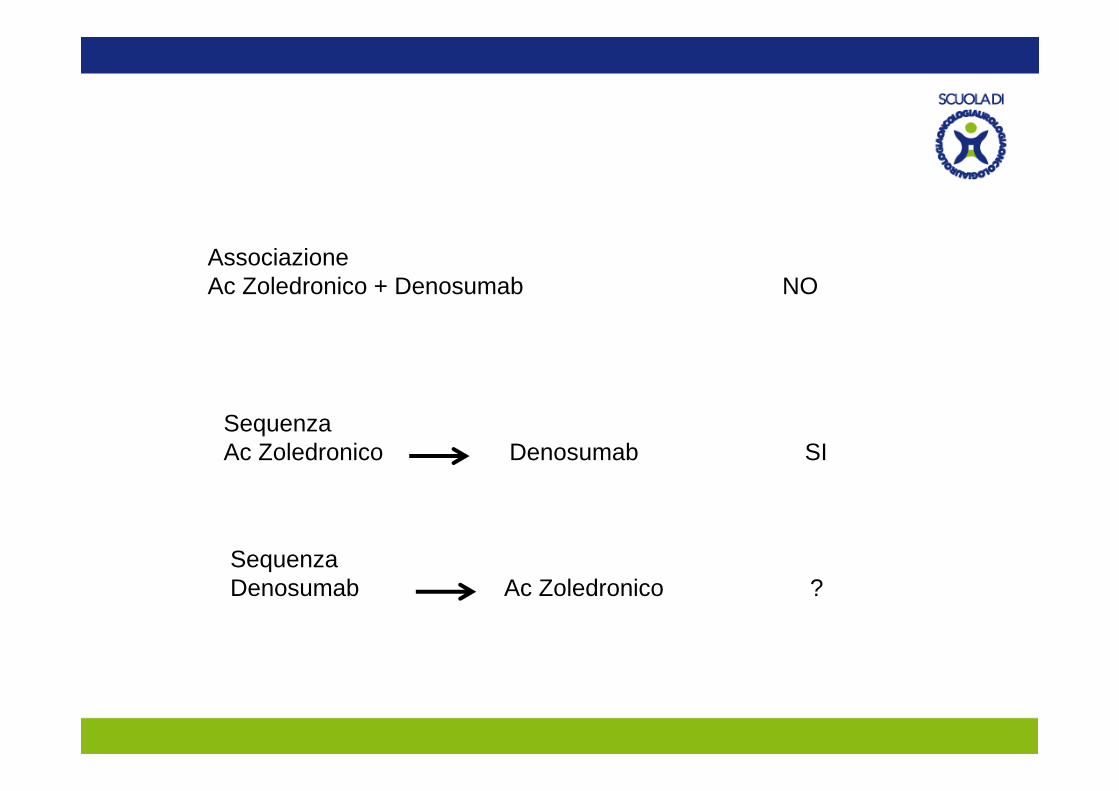
AssociazioneAc Zoledronico + Denosumab NO
SequenzaAc Zoledronico Denosumab SI
SequenzaDenosumab Ac Zoledronico ?
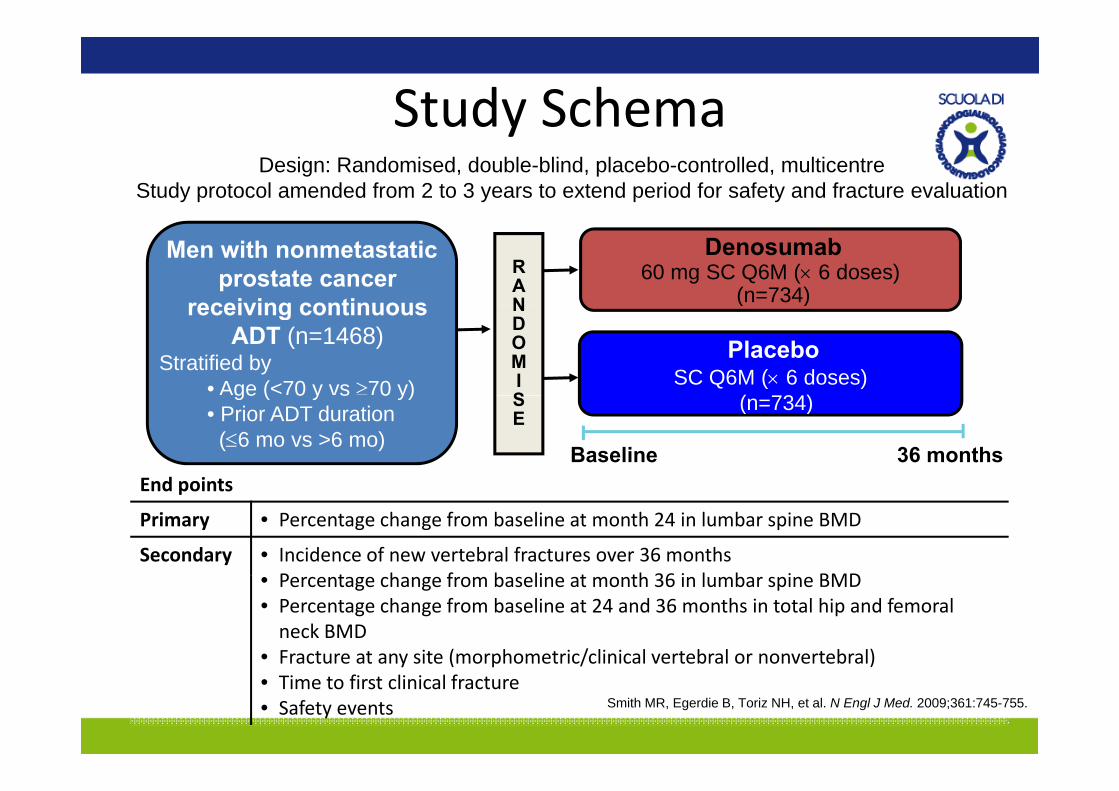
Study SchemaStudy SchemaDesign: Randomised, double-blind, placebo-controlled, multicentre
Study protocol amended from 2 to 3 years to extend period for safety and fracture evaluation
RAN
Men with nonmetastatic prostate cancer
receiving continuous
Denosumab60 mg SC Q6M (× 6 doses)
(n=734)NDOMIS
receiving continuous ADT (n=1468)
Stratified by• Age (<70 y vs ≥70 y)
( )
PlaceboSC Q6M (× 6 doses)
( 734)
Baseline 36 months
SE
ge ( 0 y s 0 y)• Prior ADT duration
(≤6 mo vs >6 mo)
(n=734)
End points
Supplemental calcium and vitamin D
End points
Primary • Percentage change from baseline at month 24 in lumbar spine BMD
Secondary • Incidence of new vertebral fractures over 36 months P t h f b li t th 36 i l b i BMD• Percentage change from baseline at month 36 in lumbar spine BMD
• Percentage change from baseline at 24 and 36 months in total hip and femoral neck BMD
• Fracture at any site (morphometric/clinical vertebral or nonvertebral)y ( p / )• Time to first clinical fracture• Safety events Smith MR, Egerdie B, Toriz NH, et al. N Engl J Med. 2009;361:745-755.
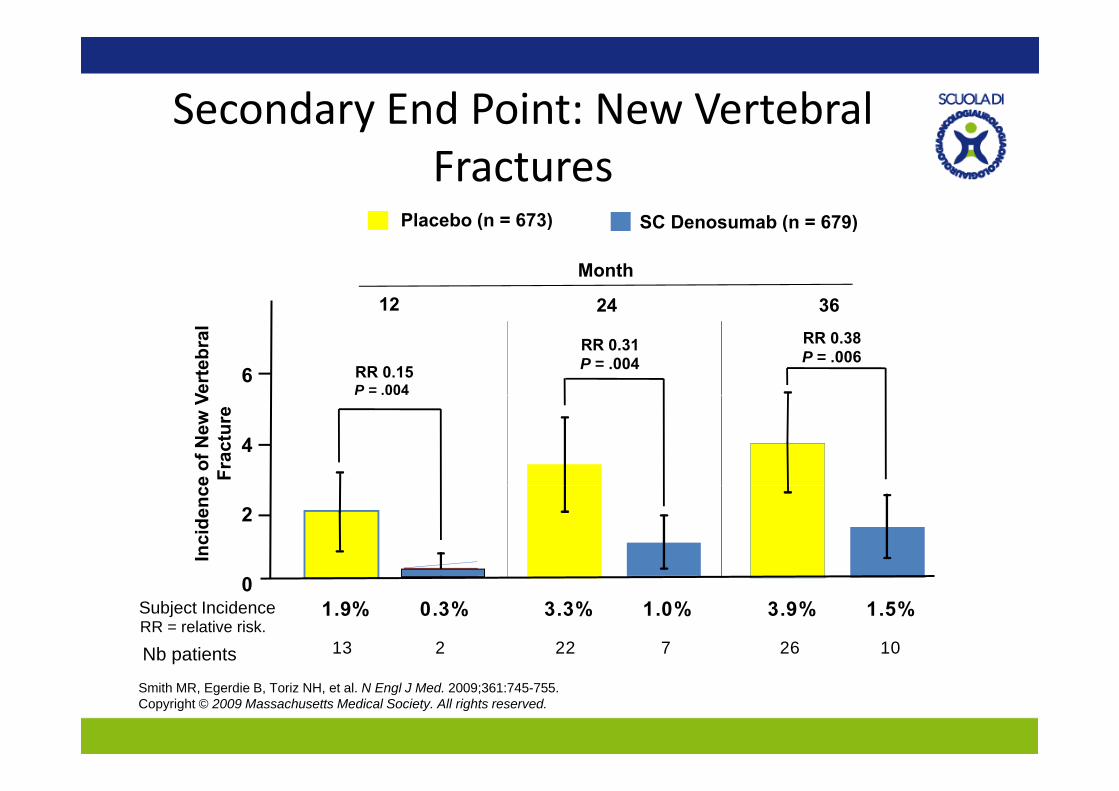
Secondary End Point: New Vertebral yFractures
SC D b ( 679)Pl b ( 673) SC Denosumab (n = 679)Placebo (n = 673)
12 24 36
Month
6 RR 0.15P = .004
RR 0.31P = .004
RR 0.38P = .006
Vert
ebra
l
12 24 36
4
e of
New
VFr
actu
re
2
Inci
denc
e
01.9% 0.3% 3.3% 1.0% 3.9% 1.5%Subject Incidence
26 1013 2 22 7RR = relative risk.
Nb patients
Smith MR, Egerdie B, Toriz NH, et al. N Engl J Med. 2009;361:745-755. Copyright © 2009 Massachusetts Medical Society. All rights reserved.