
Gianluca Aimaretti - old.iss.itold.iss.it/binary/rnoc/cont/Aimaretti_e_matarazzo.pdf · MAIN...
75
INCONTRO SU IPOPITUITARISMO E TERAPIA CON ORMONE SOMATOTROPO NELL’ADULTO Gianluca Aimaretti Endocrinologia, Dipartimento di Medicina Traslazionale Università A. Avogadro del Piemonte Orientale [email protected]
Transcript of Gianluca Aimaretti - old.iss.itold.iss.it/binary/rnoc/cont/Aimaretti_e_matarazzo.pdf · MAIN...
INCONTRO SU IPOPITUITARISMO E TERAPIA CON ORMONE SOMATOTROPO NELL’ADULTO
Gianluca Aimaretti
Endocrinologia, Dipartimento di Medicina Traslazionale
Università A. Avogadro del Piemonte Orientale
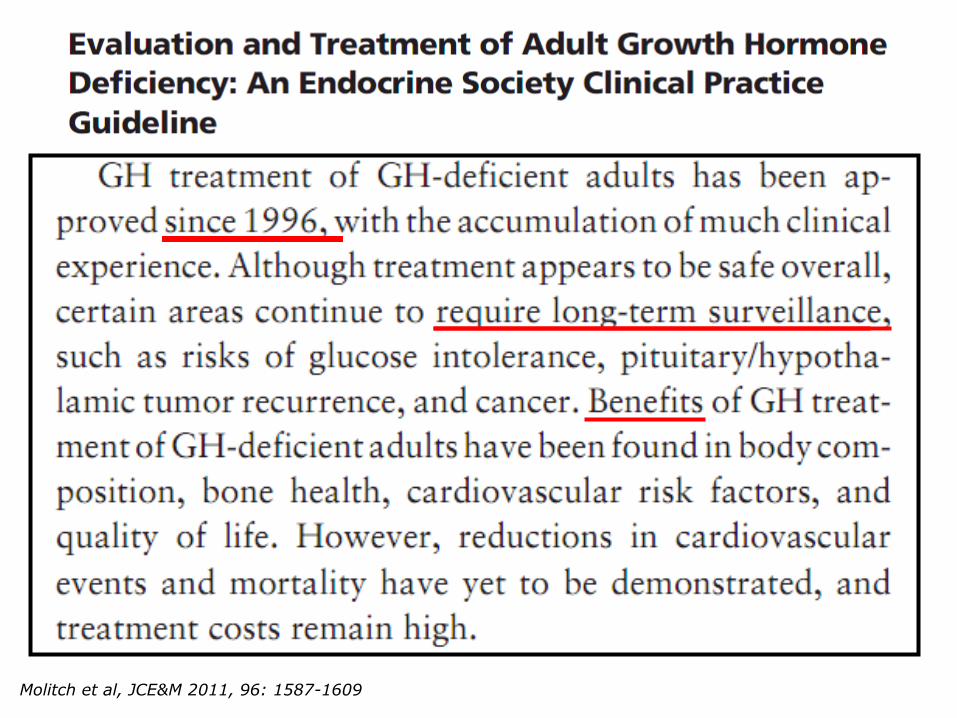
Molitch et al, JCE&M 2011, 96: 1587-1609
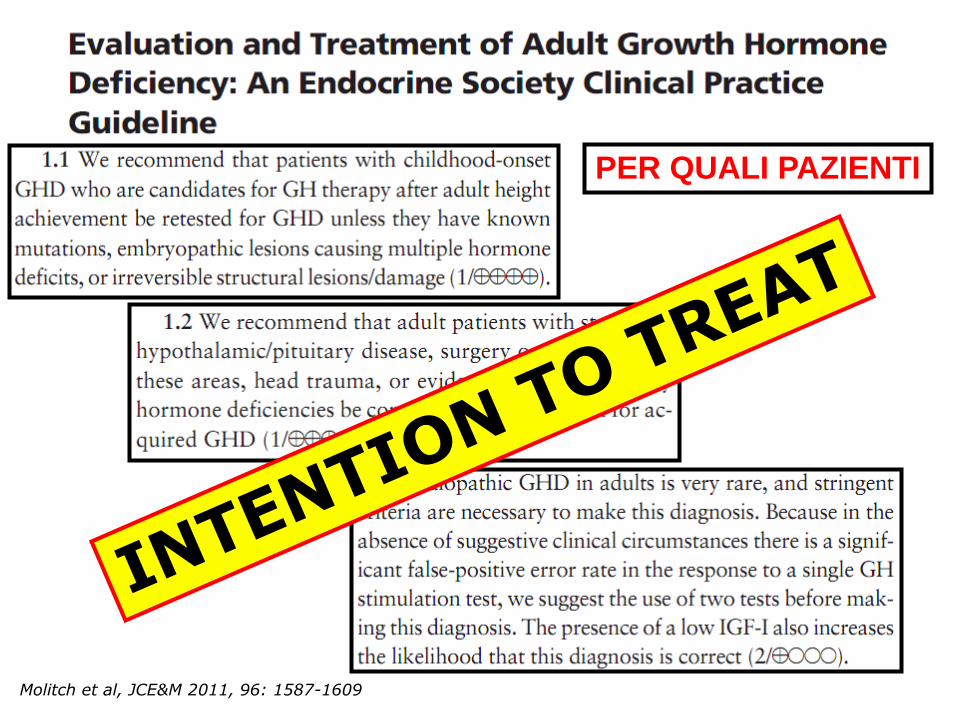
Molitch et al, JCE&M 2011, 96: 1587-1609
PER QUALI PAZIENTI
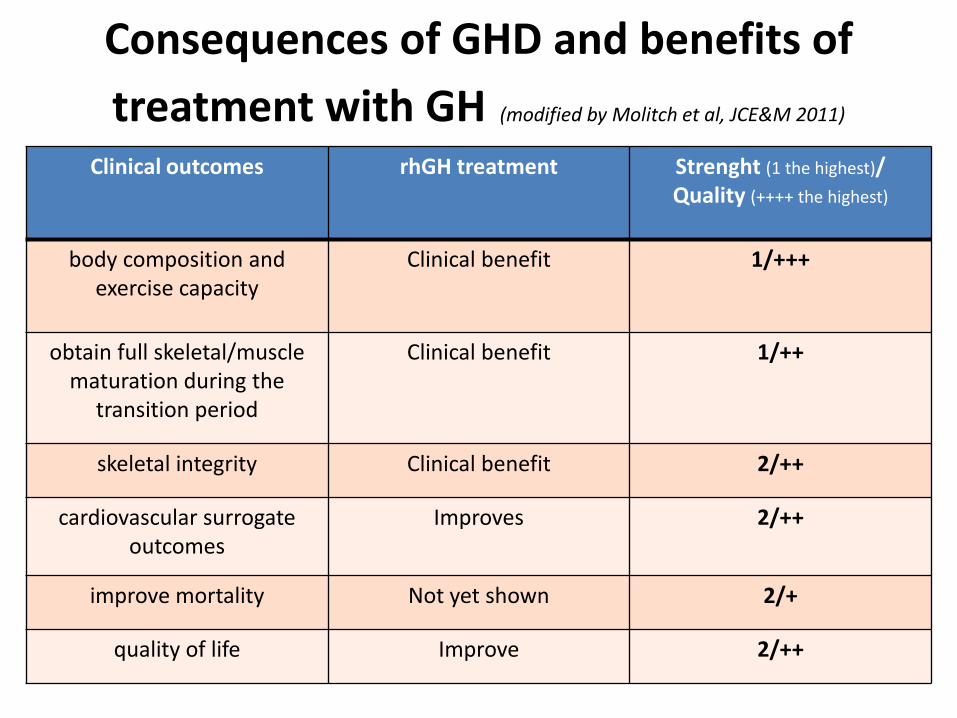
Consequences of GHD and benefits of
treatment with GH (modified by Molitch et al, JCE&M 2011)
Clinical outcomes rhGH treatment Strenght (1 the highest)/ Quality (++++ the highest)
body composition and exercise capacity
Clinical benefit 1/+++
obtain full skeletal/muscle maturation during the
transition period
Clinical benefit 1/++
skeletal integrity Clinical benefit 2/++
cardiovascular surrogate outcomes
Improves 2/++
improve mortality Not yet shown 2/+
quality of life Improve 2/++
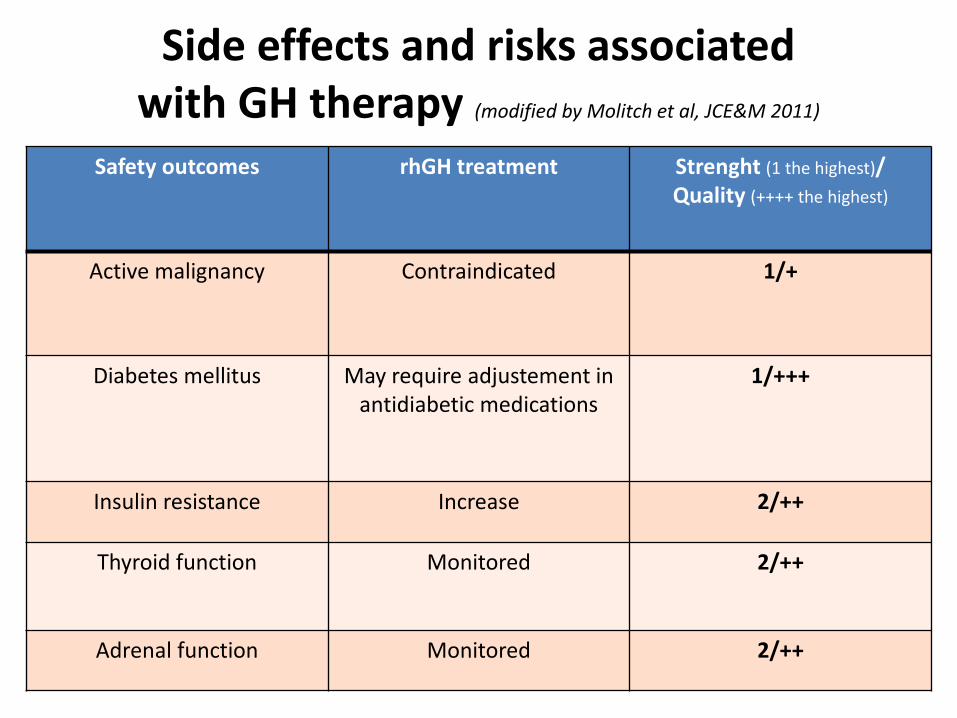
Side effects and risks associated with GH therapy (modified by Molitch et al, JCE&M 2011)
Safety outcomes rhGH treatment Strenght (1 the highest)/ Quality (++++ the highest)
Active malignancy Contraindicated 1/+
Diabetes mellitus May require adjustement in antidiabetic medications
1/+++
Insulin resistance Increase 2/++
Thyroid function Monitored 2/++
Adrenal function Monitored 2/++
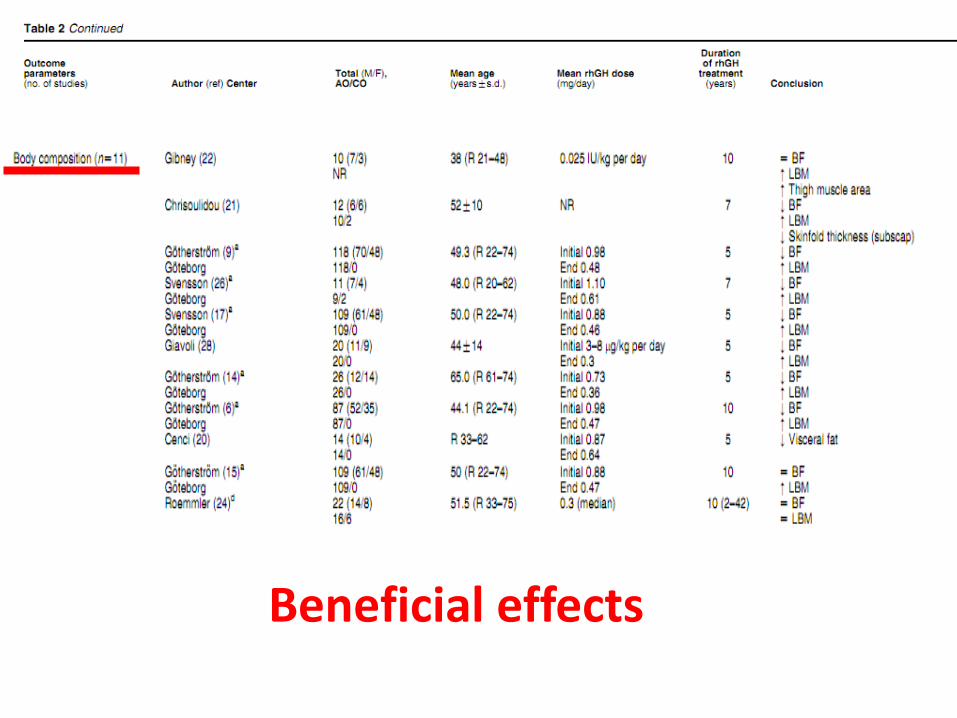
Beneficial effects

Beneficial effects
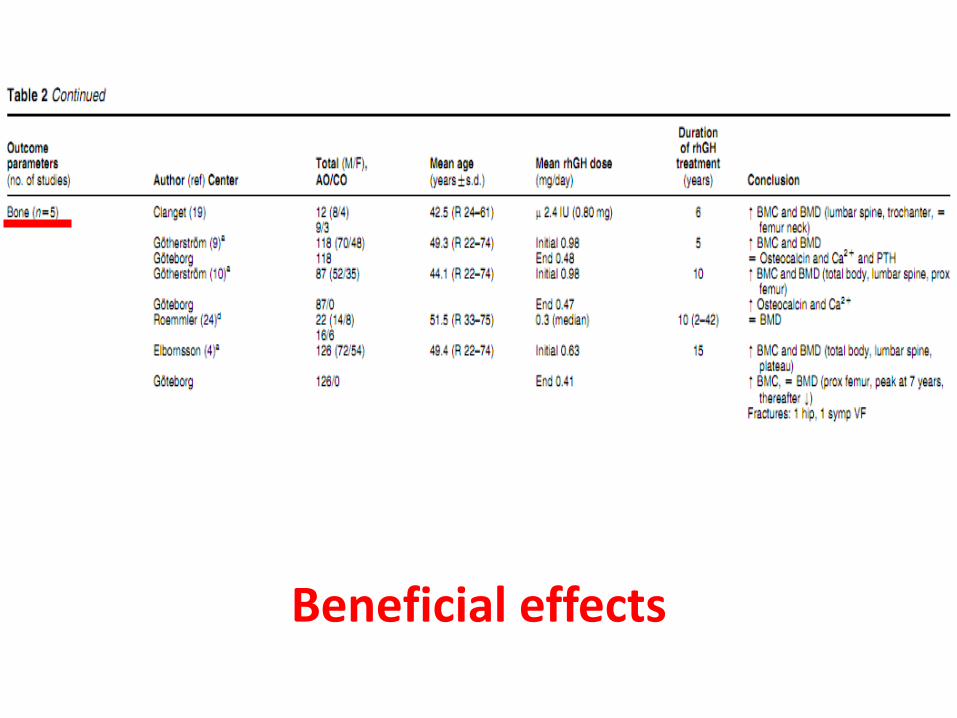
Beneficial effects
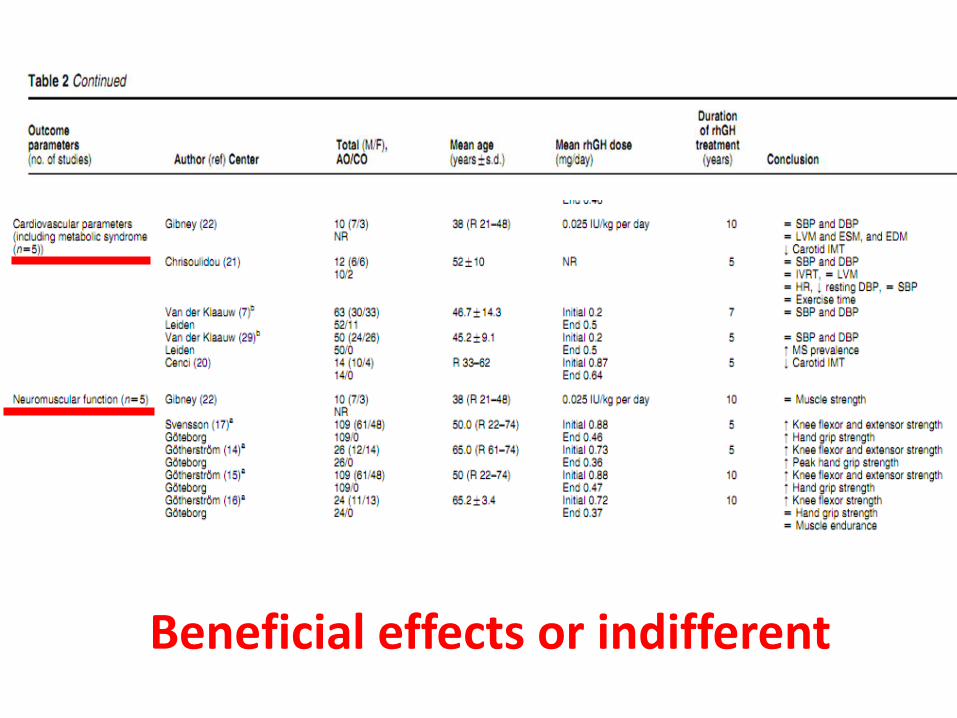
Beneficial effects or indifferent
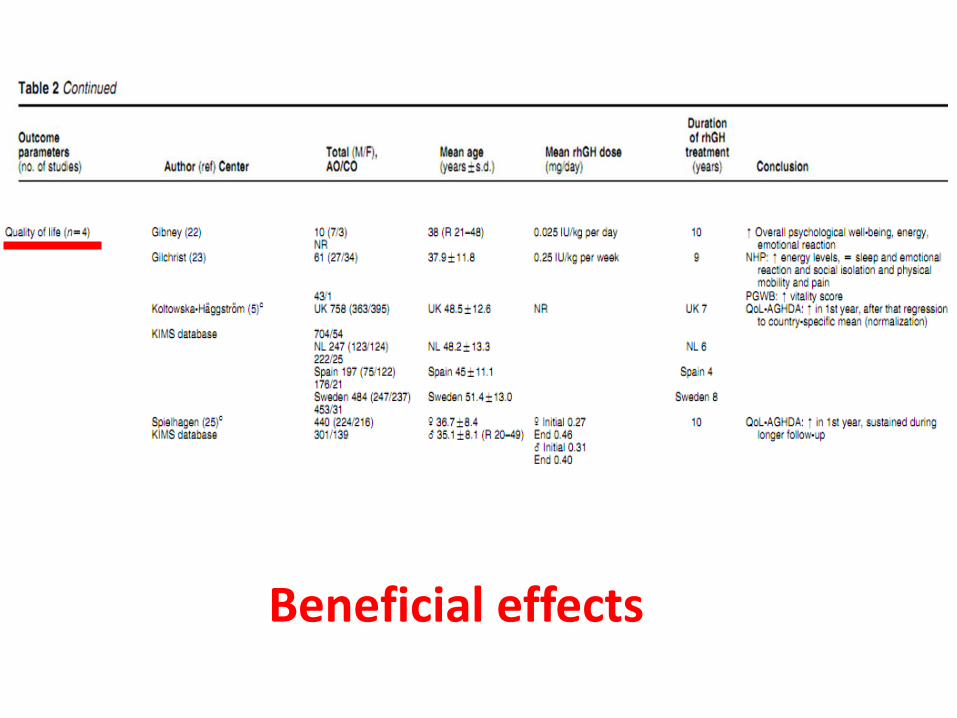
Beneficial effects
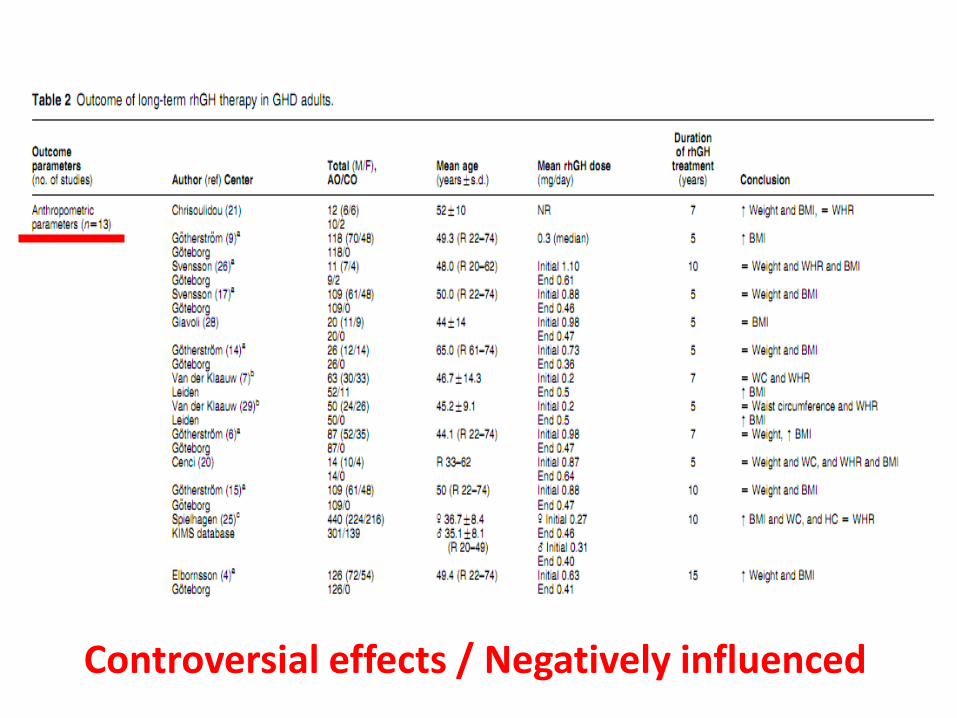
Controversial effects / Negatively influenced
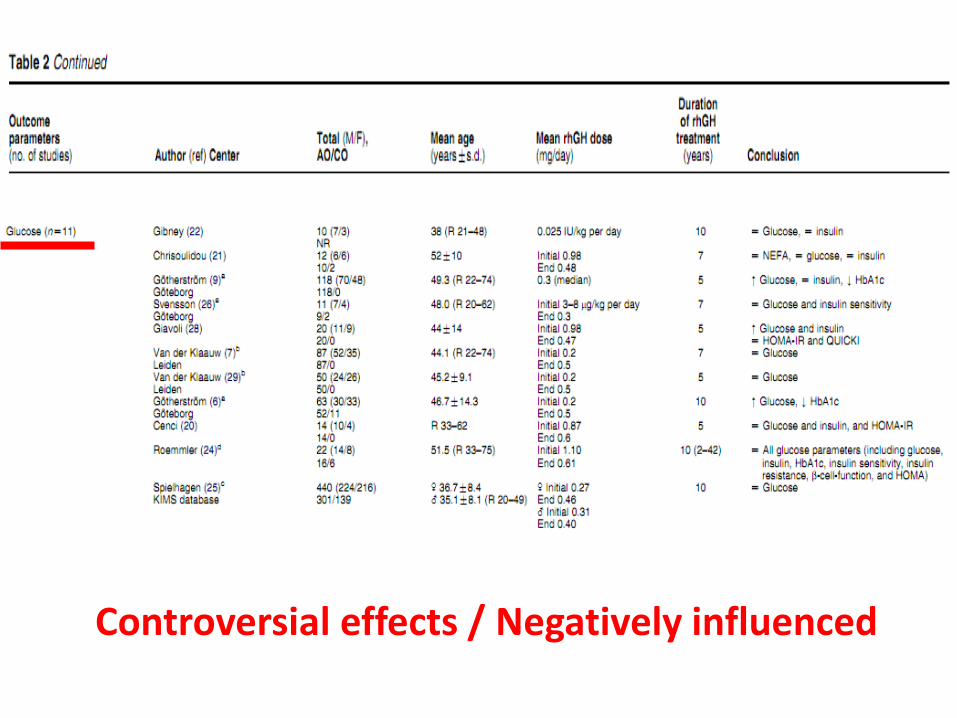
Controversial effects / Negatively influenced
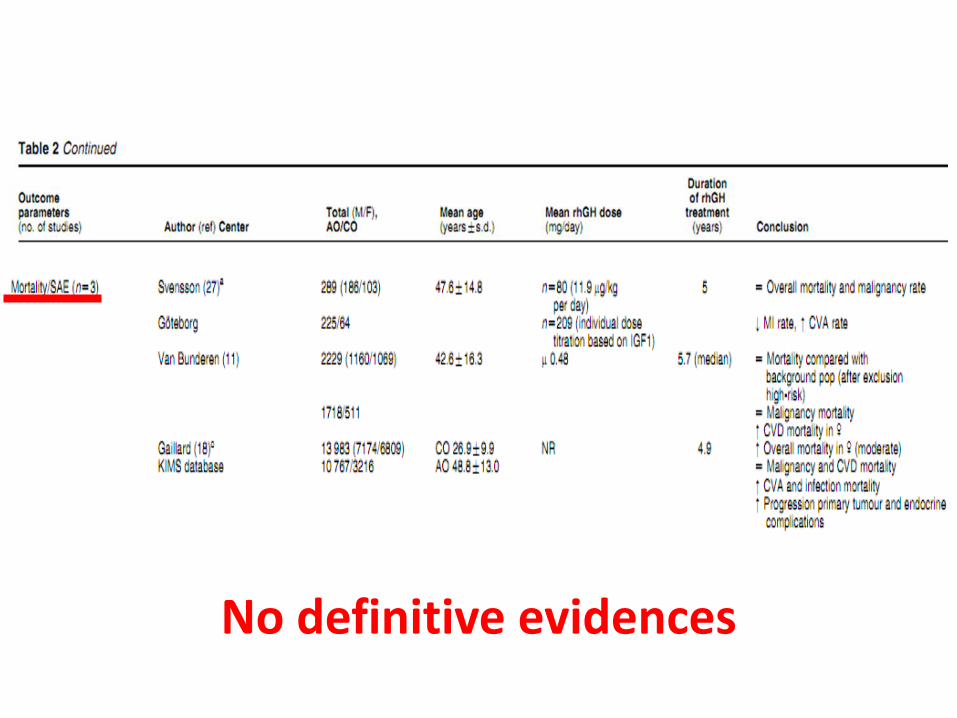
No definitive evidences
MAIN CONCLUSIONS (Appelman et al EJE 2013)
• …long-term studies were generally uncontrolled and lacked a control group (of non-treated GHD patients) enabling adjustment for subjective changes or changes due to ageing.
• …a limited number of centres have reported their data, resulting in a low number of evaluable patients with a follow-up duration of >5 years of rhGH replacement with half of the long-term studies describing (part of) the same patient cohort. (The course of QoL during ongoing therapy is unestablished).
• …metabolic profile, rhGH therapy has shown prolonged, beneficial effects in the long-term for body composition, lipid profile, carotid IMT and BMD, but overall cardiovascular risk, as assessed by the prevalence of the MS, glucose levels and BMI appeared not to be influenced or was even negatively affected.
• …the benefit of long-term rhGH treatment should be a matter of ongoing research to enable adequate risk benefit analyses and, in clinical daily practice, the benefits of rhGH should be considered carefully in each patient.

Occurrence of impaired fasting glucose in GH-deficient adults receiving GH replacement compared with untreated subjects
• There were no significant differences in the distribution of FPG elevation between GH-treated and untreated groups (P = 1.00)
• GH replacement therapy in our adult subjects with GH deficiency was associated with a mild increase in Fasting Plasma Glucose levels. This increase most frequently occurred within the first year of therapy, was usually in the range of impaired fasting glucose rather than diabetes mellitus and often spontaneously normalized
Woodmansee W. Occurrence of impaired fasting glucose in GH-deficient adults receiving GH replacement compared with untreated subjects. Clinical Endocrinology (2010) 72, 59–69
US HypoCCS study, 572 subjects
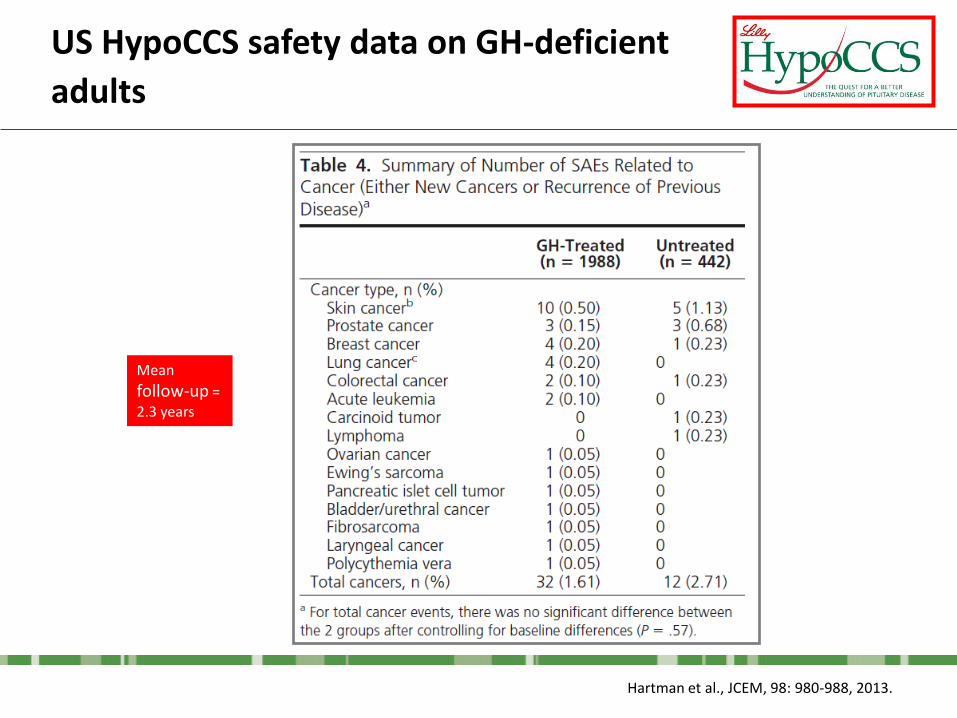
Hartman et al., JCEM, 98: 980-988, 2013.
US HypoCCS safety data on GH-deficient
adults
Mean
follow-up = 2.3 years
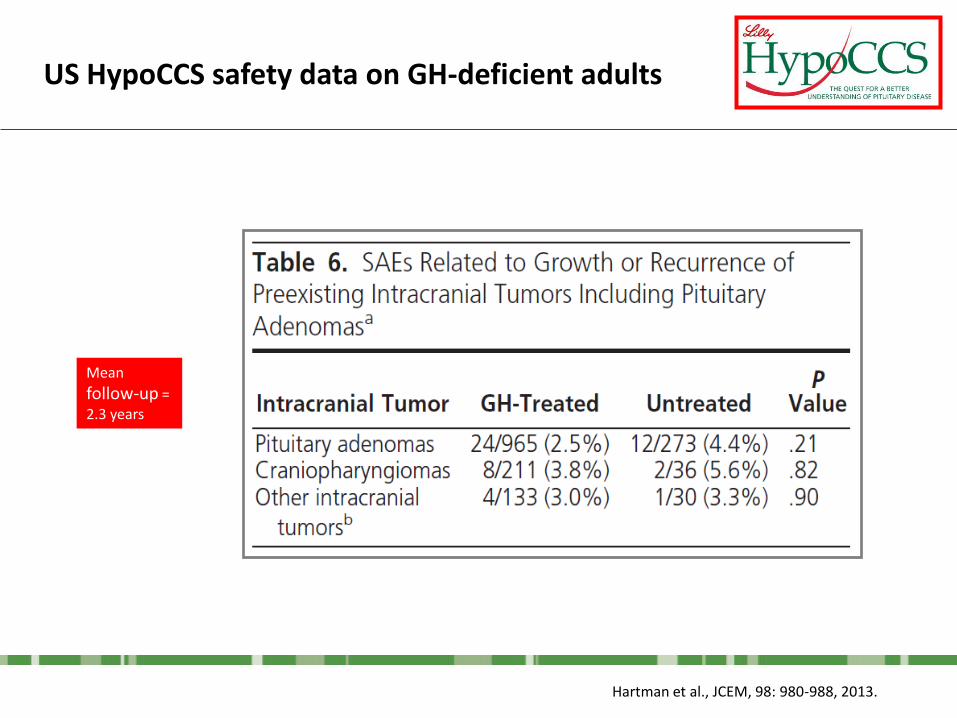
Hartman et al., JCEM, 98: 980-988, 2013.
US HypoCCS safety data on GH-deficient adults
Mean
follow-up = 2.3 years
The aim of the present analysis was to describe the characteristics and outcomes of the Italian adult
patients with hypopituitarism/GHD who are participating in HypoCCS.
Italian HypoCCS population
AIM of the study
Data were assessed for Italian patients in the HypoCCS database for the data lock of July 2010. Patients with evaluable data were grouped according to tertiles (Group A ≤33%,Group B >33-≤66%, Group C >66%) of maximum GH peak concentration reported from stimulation testing at the time of entry to the study. Patients were also assessed according to body mass index category (BMI: ≤25, >25-≤30, >30 kg/m2). Demographic and other patient characteristics were analyzed for baseline determinations. GH dose, BMI, serum lipid concentrations, smoking status and CVD risk according to the Framingham index were analyzed at baseline and over time of GH treatment, at yearly intervals.
PATIENTS and METHODS
RESULTS
The HypoCCS database included 1025 patients in Italy with data available for analysis. The most frequent cause of hypopituitarism/GHD was pituitary adenoma reported for 40% of patients, with craniopharyngiomas reported for 14% and idiopathic GHD reported for 13% (34% in CO and 6% in AO patients).
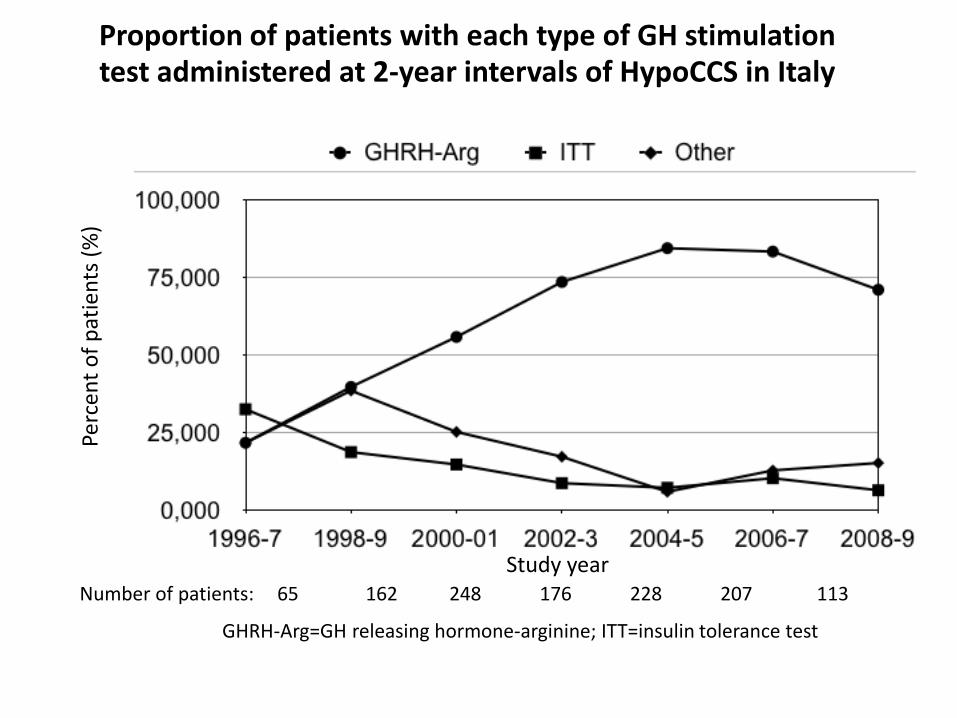
Proportion of patients with each type of GH stimulation test administered at 2-year intervals of HypoCCS in Italy
Study year
Perc
ent
of
pat
ien
ts (
%)
GHRH-Arg=GH releasing hormone-arginine; ITT=insulin tolerance test
Number of patients: 65 162 248 176 228 207 113
Group A Group B Group C P
N=342 N=345 N=338
Age, yearsa 44 ± 16 45 ± 16 43 ± 15 0.231
Female, n (%) 148 (43.3) 132 (38.3) 144 (42.6) 0.350
Male, n (%) 194 (56.7) 213 (61.7) 194 (57.4)
Adult onset, n (%) 258 (75.9) 266 (77.1) 265 (78.4) 0.737
Childhood onset, n (%) 82 (24.1) 79 (22.9) 73 (21.6)
Serum IGF-I, µg/L 78.0 ± 66.5 101.6 ± 65.6 139.3 ± 77.5 <0.001
Starting GH dose, µg/kg/dayb 311 (291-331) 356 (330-383) 392 ± 323 <0.001
GH treatment duration, yearsa 7.2 ± 9.2 5.5 ± 8.2 5.0 ± 7.6 0.001
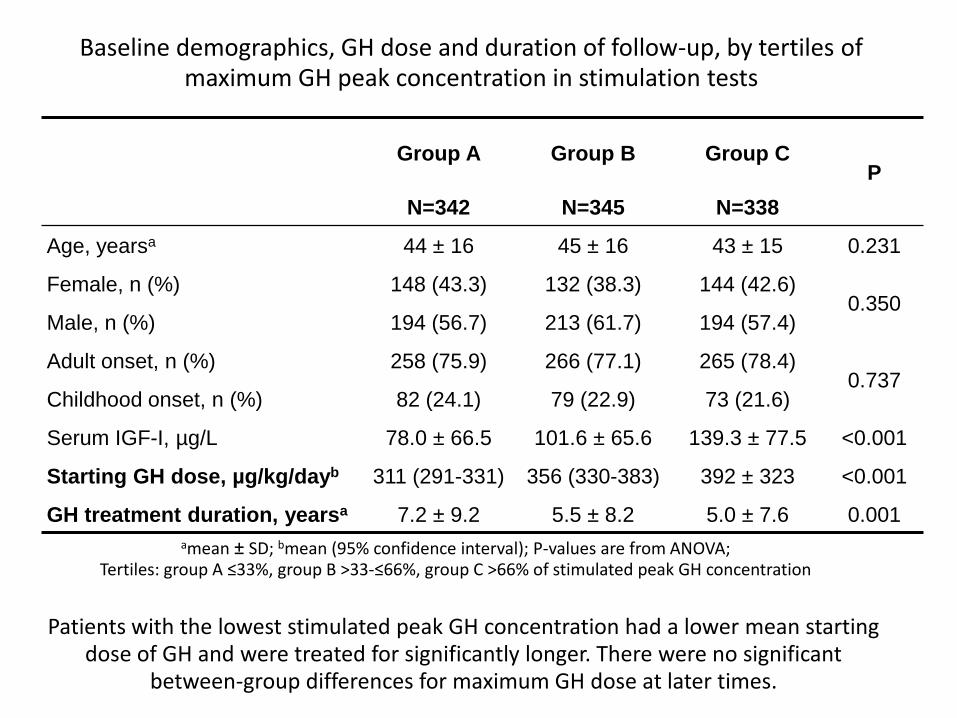
Baseline demographics, GH dose and duration of follow-up, by tertiles of maximum GH peak concentration in stimulation tests
amean ± SD; bmean (95% confidence interval); P-values are from ANOVA; Tertiles: group A ≤33%, group B >33-≤66%, group C >66% of stimulated peak GH concentration
Patients with the lowest stimulated peak GH concentration had a lower mean starting dose of GH and were treated for significantly longer. There were no significant
between-group differences for maximum GH dose at later times.
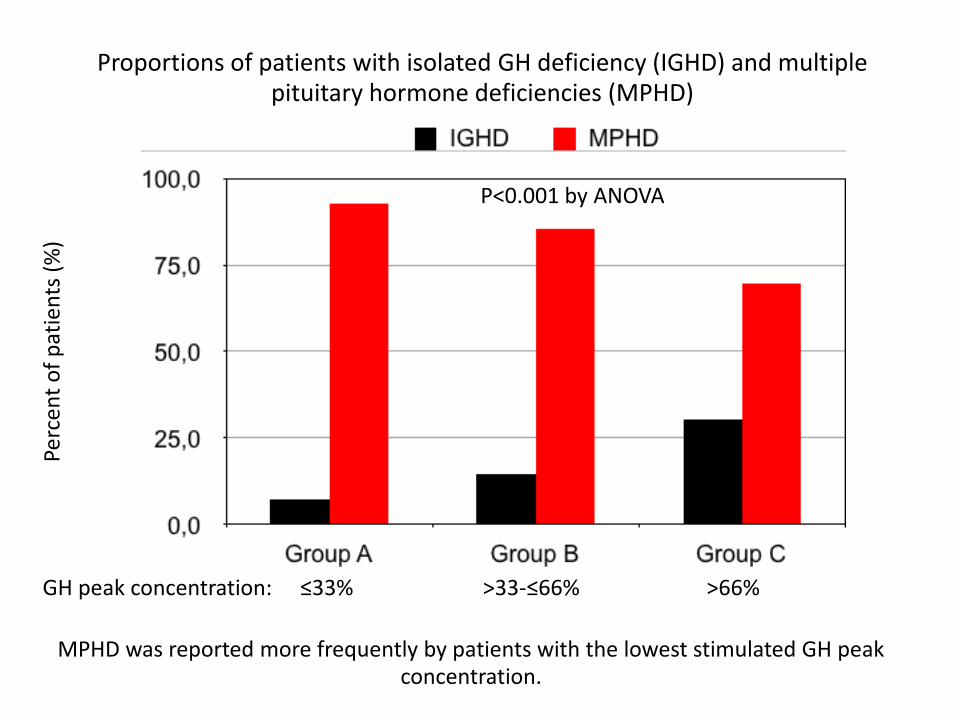
Proportions of patients with isolated GH deficiency (IGHD) and multiple pituitary hormone deficiencies (MPHD)
Perc
ent
of
pat
ien
ts (
%)
GH peak concentration: ≤33% >33-≤66% >66%
P<0.001 by ANOVA
MPHD was reported more frequently by patients with the lowest stimulated GH peak concentration.
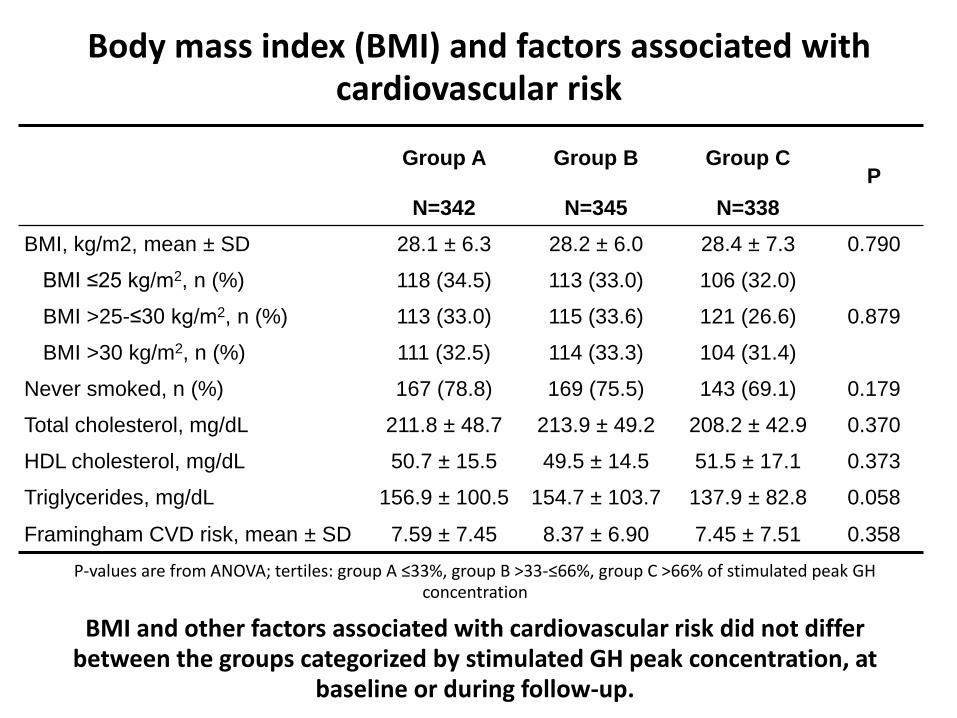
Group A Group B Group C P
N=342 N=345 N=338
BMI, kg/m2, mean ± SD 28.1 ± 6.3 28.2 ± 6.0 28.4 ± 7.3 0.790
BMI ≤25 kg/m2, n (%) 118 (34.5) 113 (33.0) 106 (32.0)
0.879 BMI >25-≤30 kg/m2, n (%) 113 (33.0) 115 (33.6) 121 (26.6)
BMI >30 kg/m2, n (%) 111 (32.5) 114 (33.3) 104 (31.4)
Never smoked, n (%) 167 (78.8) 169 (75.5) 143 (69.1) 0.179
Total cholesterol, mg/dL 211.8 ± 48.7 213.9 ± 49.2 208.2 ± 42.9 0.370
HDL cholesterol, mg/dL 50.7 ± 15.5 49.5 ± 14.5 51.5 ± 17.1 0.373
Triglycerides, mg/dL 156.9 ± 100.5 154.7 ± 103.7 137.9 ± 82.8 0.058
Framingham CVD risk, mean ± SD 7.59 ± 7.45 8.37 ± 6.90 7.45 ± 7.51 0.358
Body mass index (BMI) and factors associated with cardiovascular risk
BMI and other factors associated with cardiovascular risk did not differ between the groups categorized by stimulated GH peak concentration, at
baseline or during follow-up.
P-values are from ANOVA; tertiles: group A ≤33%, group B >33-≤66%, group C >66% of stimulated peak GH concentration
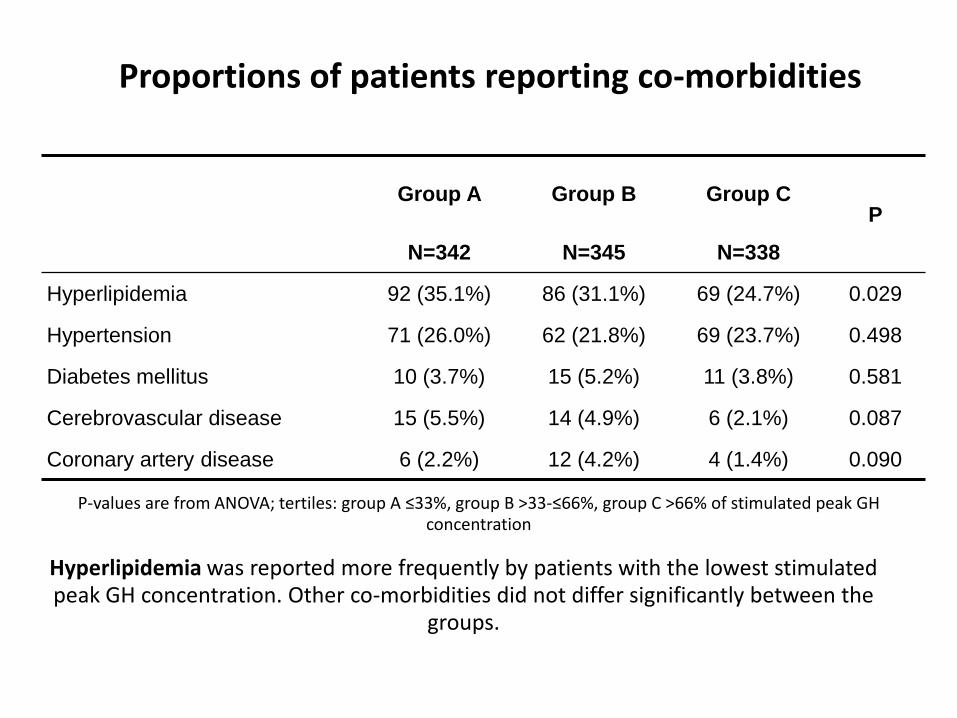
Group A Group B Group C P
N=342 N=345 N=338
Hyperlipidemia 92 (35.1%) 86 (31.1%) 69 (24.7%) 0.029
Hypertension 71 (26.0%) 62 (21.8%) 69 (23.7%) 0.498
Diabetes mellitus 10 (3.7%) 15 (5.2%) 11 (3.8%) 0.581
Cerebrovascular disease 15 (5.5%) 14 (4.9%) 6 (2.1%) 0.087
Coronary artery disease 6 (2.2%) 12 (4.2%) 4 (1.4%) 0.090
Proportions of patients reporting co-morbidities
Hyperlipidemia was reported more frequently by patients with the lowest stimulated peak GH concentration. Other co-morbidities did not differ significantly between the
groups.
P-values are from ANOVA; tertiles: group A ≤33%, group B >33-≤66%, group C >66% of stimulated peak GH concentration
Group A Group B Group C P
N=342 N=345 N=338
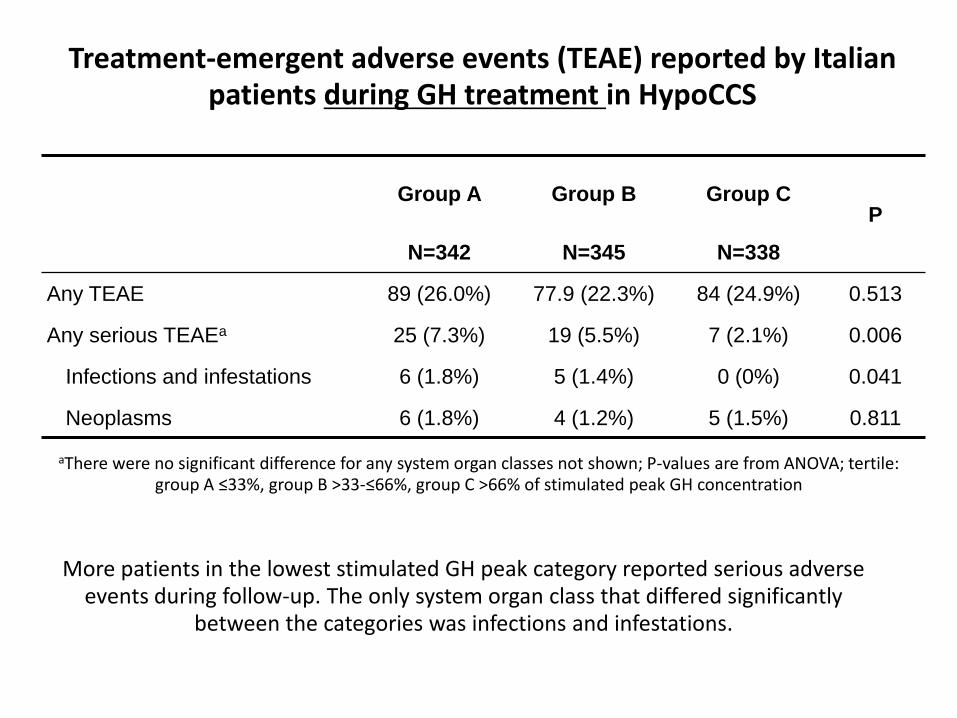
Any TEAE 89 (26.0%) 77.9 (22.3%) 84 (24.9%) 0.513
Any serious TEAEa 25 (7.3%) 19 (5.5%) 7 (2.1%) 0.006
Infections and infestations 6 (1.8%) 5 (1.4%) 0 (0%) 0.041
Neoplasms 6 (1.8%) 4 (1.2%) 5 (1.5%) 0.811
Treatment-emergent adverse events (TEAE) reported by Italian patients during GH treatment in HypoCCS
More patients in the lowest stimulated GH peak category reported serious adverse events during follow-up. The only system organ class that differed significantly
between the categories was infections and infestations.
aThere were no significant difference for any system organ classes not shown; P-values are from ANOVA; tertile: group A ≤33%, group B >33-≤66%, group C >66% of stimulated peak GH concentration
SUMMARY 1
In adult patients treated with GH in HypoCCS in Italy, the most frequent GH stimulation test used for diagnosis was GHRH-arginine and the majority of patients had stimulated GH peak below standard cut-off levels for GH deficiency.
Patients in the lowest GH peak concentration group started on a lower GH dose than the other groups, although there were no between-group differences at later times.
Patients with the lowest stimulated GH peak concentration were more likely to have multiple pituitary hormone deficiencies.
SUMMARY 2
Baseline means for BMI, serum lipids, smoking status and the Framingham CVD risk did not differ between the categories of stimulated GH peak concentration. Mean BMI, serum lipid values and Framingham CVD risk during follow-up did not differ between the GH peak concentration groups.
More patients in the lowest GH peak concentration group reported hyperlipidemia.
Treatment-emergent adverse events were reported by similar numbers of patients in each GH peak concentration group. Serious adverse events were reported more frequently in the patients with the lowest stimulated GH peak concentration, but the only system organ class that differed significantly between groups was infections and infestations.
Take Home messages
1) Terapia con rhGH: Effetti positivi long-term (>5 anni) su composizione corporea, profilo lipidico, IMT
carotidea, e massa osssea, ma su rischio CV (=SM, BMI, glicemia) non effetti positivi (forse anche negativi).
Però: Mancano gruppi di controllo long term di pazienti non trattati. 2) Terapia con rhGH: Aumentata incidenza di diabete (DM2 o secondario?) per un FU di 3.9 anni, in
pazienti anziani, con peggior quadro lipidico, più elevato BMI e più elevata PA prima del trattamento. Dato ancora controverso.
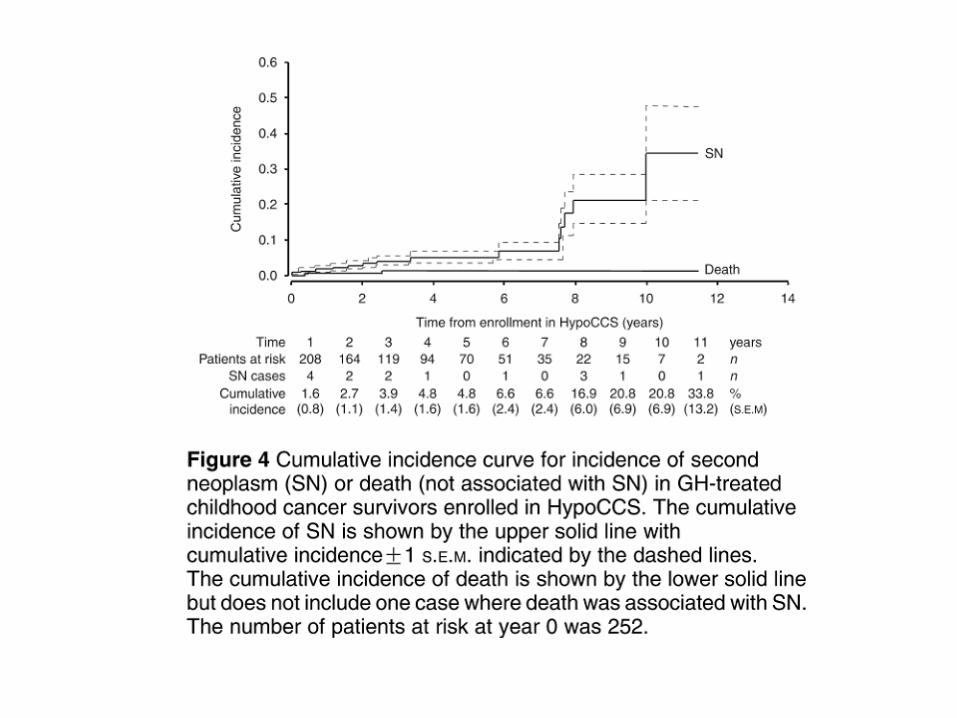
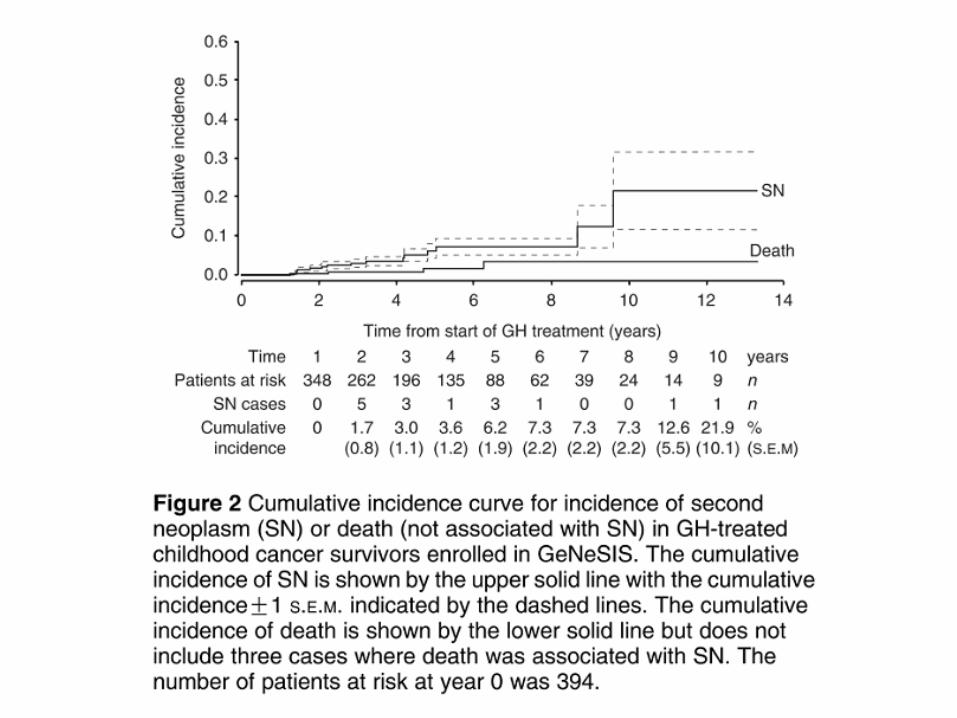
3) Terapia con rhGH: non rischio di II° tumore o incremento residuo tumorale, ma FU medio di 2.3 anni. Aumento incidenza di II° tumore per sopravissuti da neoplasia pediatrica, quando
trattati con rhGH (ma end point clinico forte: bassa statura se non trattati).

Endocrinology
University of Piemonte Orientale,
Novara
P. Marzullo
L. Pagano
S. Belcastro
A. Busti
M.T. Samà
M. Caputo
M. Zavattaro
Endocrinology and
Metabolism
University of Turin
E. Ghigo, F. Camanni
V. Gasco
L. Ghizzoni
S. Grottoli
E. Arvat
Metabolic Diseases
Maggiore della Carità Hospital, Novara
G. Allochis
G. Mauri
C. Ponziani
Pediatrics
University of Piemonte
Orientale, Novara
G. Bona
S. Bellone
F. Prodam
Grazie NoGeRo
Novara, Genova, Roma
D. Ferone
R. Baldelli
1. Proc Natl Acad Sci U S A. 2013 Nov 11. [Epub ahead of print]
Growth hormone prevents the development of autoimmune diabetes. Villares R, Kakabadse D, Juarranz Y, Gomariz RP, Martínez-A C, Mellado M. Department of Immunology and Oncology, Centro Nacional de Biotecnología, Consejo Superior de Investigaciones Científicas, E-28049 Madrid, Spain.
Evidence supports a relationship between the neuroendocrine and the immune systems. Data from mice that overexpress or are deficient in growth hormone (GH) indicate that GH stimulates T and B-cell proliferation and Ig synthesis, and enhances maturation of myeloid progenitor cells. The effect of GH on autoimmune pathologies has nonetheless been little studied. Using a murine model of type 1 diabetes, a T-cell-mediated autoimmune disease characterized by immune cell infiltration of pancreatic islets and destruction of insulin-producing β-cells, we observed that sustained GH expression reduced prodromal disease symptoms and eliminated progression to overt diabetes. The effect involves several GH-mediated mechanisms; GH altered the cytokine environment, triggered anti-inflammatory macrophage (M2) polarization, maintained activity of the suppressor T-cell population, and limited Th17 cell plasticity. In addition, GH reduced
apoptosis and/or increased the proliferative rate of β-cells. These results support a role for GH in immune response regulation and identify a unique target for therapeutic intervention in type 1 diabetes. PMID: 24218587 [PubMed - as supplied by publisher]
La terapia con ormone della crescita nei
soggetti con bassa statura non convenzionale (follow up a 2 anni in regione Piemonte)
Patrizia Matarazzo
Endocrinologia Pediatrica O.I.R.M. - Città della Salute e della Scienza-Torino
Gruppo Tecnico “Area Pediatrica” della Commissione GH Piemonte
BASSA STATURA NON CONVENZIONALE:
definizione
Condizioni per le quali il trattamento con rhGH NON è
convenzionale, cioè non previsto dalla Nota AIFA 39:
•BS idiopatica (Idiopatic Short Stature=ISS)
•BS in displasie scheletriche (Skeletal Dysplasia=SD)
(SHOX, ipocondroplasia, acondroplasia, DSE,...)
•BS sindromi/mal. genetiche
(Noonan, Silver Russell, Cornelia de Lange,...)
•BS in mal. croniche
(fibrosi cistica, celiachia, distrofie muscolari,...)
•BS in soggetti SGA normato ma trattamento su approvazione delle Commissioni Regionali
BASSA STATURA NON CONVENZIONALE:
motivazioni e
basi scientifiche per l'impiego di rhGH
La bassa statura è fattore di rischio per problemi psico-
sociali dimostrato per le gravi basse stature -4sds
Esistono dati di efficacia del trattamento nella ISS, SGA,
SHOX, Ipocondroplasia
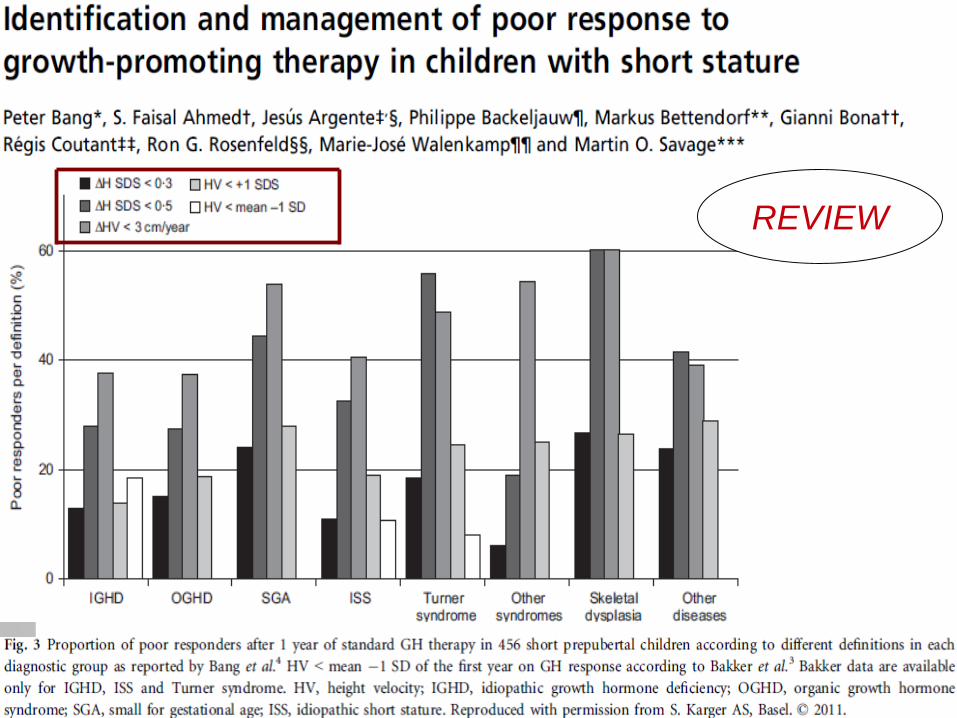
Nella Acondroplasia e nelle sindromi
- non ci sono dati definitivi sull'altezza adulta;
- il trattamento con rhGH sembra migliorare la velocità di
crescita a 1 -2 anni.
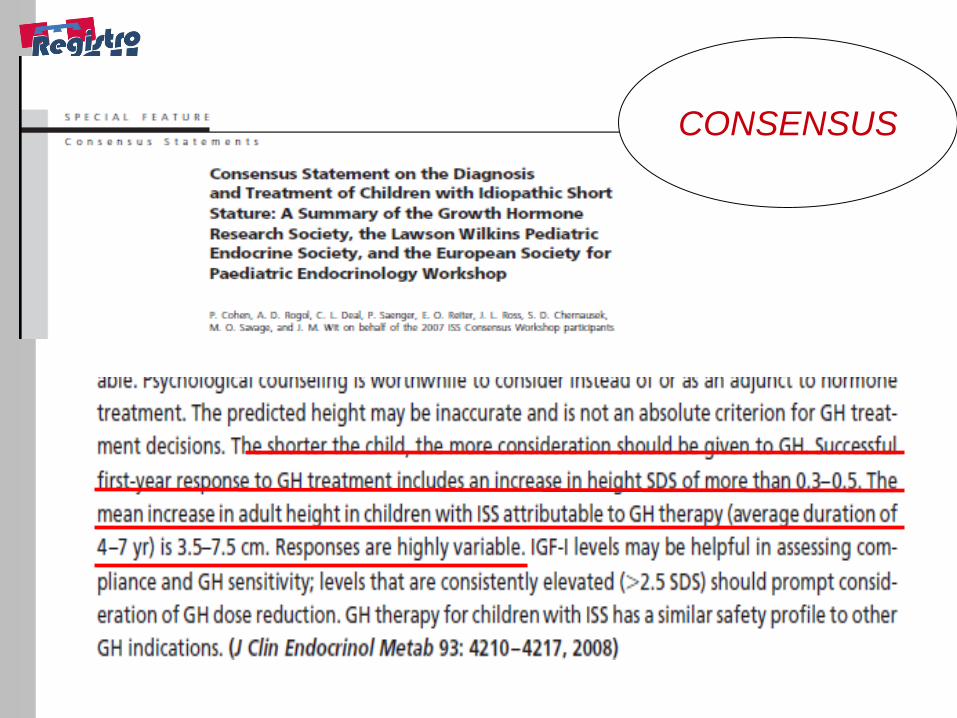
Negli Stati Uniti la ISS è tra le indicazioni “ufficiali” per il
trattamento con rhGH
CONSENSUS
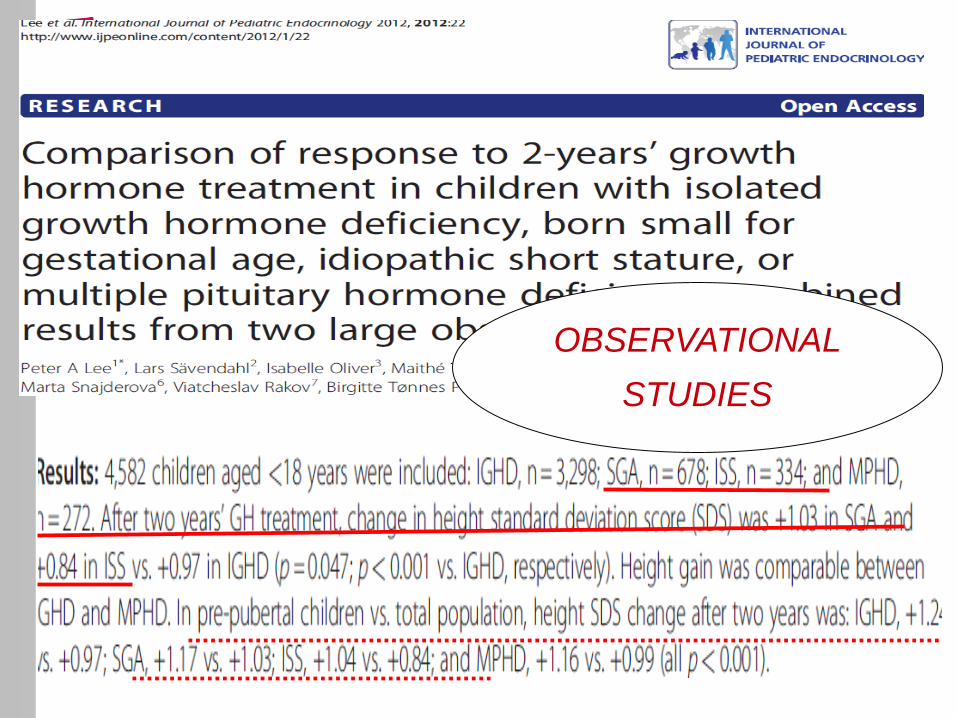
OBSERVATIONAL
STUDIES
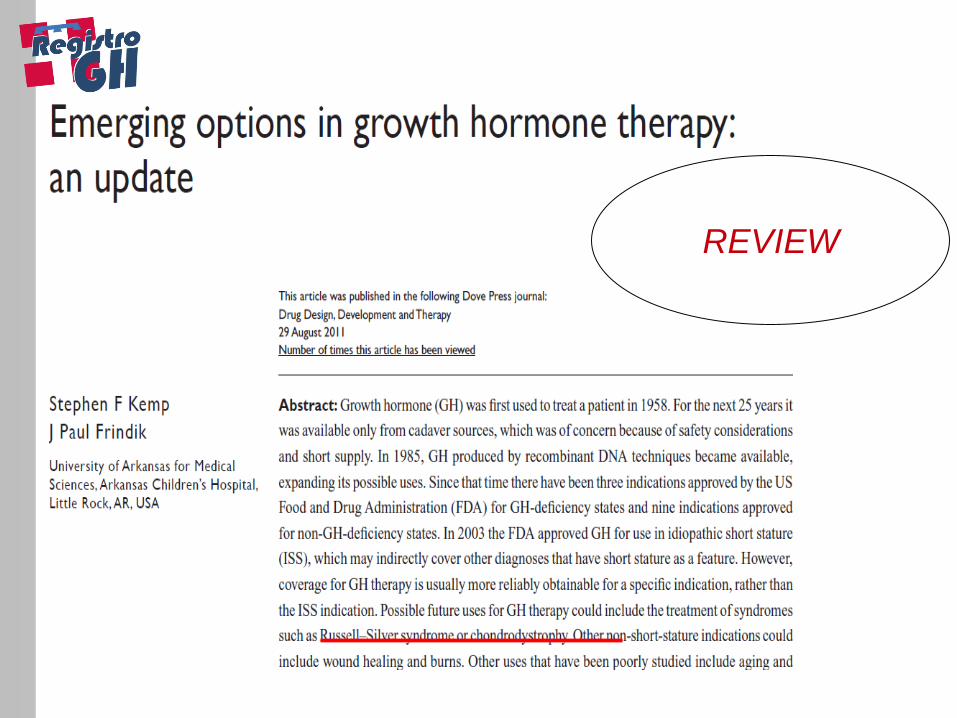
REVIEW
REVIEW
REVIEW
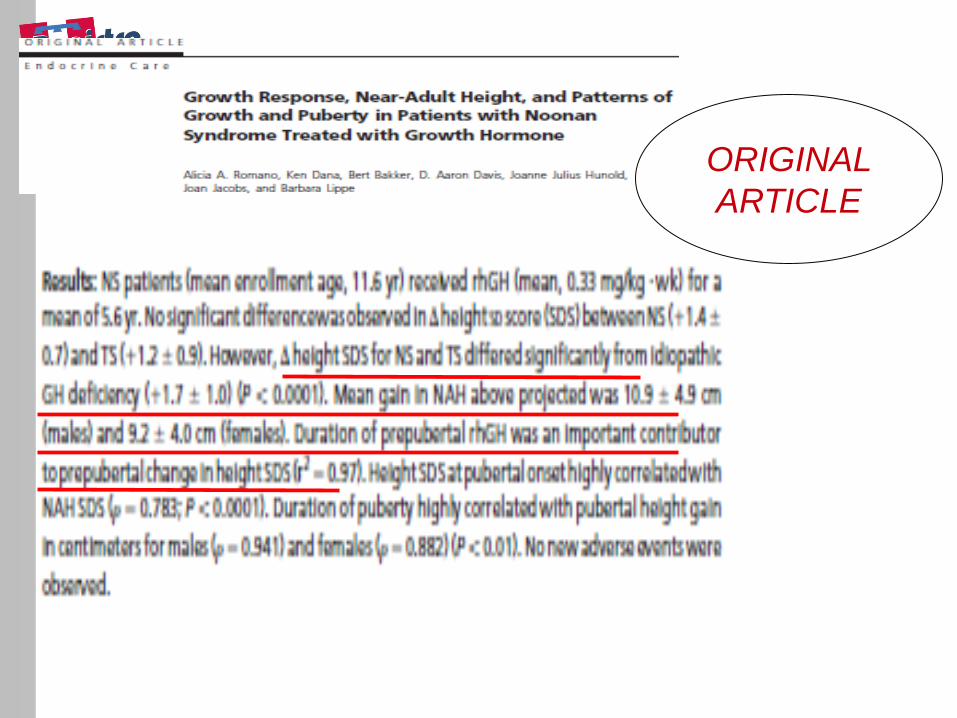
ORIGINAL
ARTICLE
Nota 39
- Determinazione 29 luglio 2010 (GU 18 novembre 2010, n. 270): modifica
alla nota AIFA 39 di cui alla determinazione del 26 novembre
2009.modifica alla nota AIFA 39 di cui alla determinazione del 26
novembre 2009.
Età evolutiva
In soggetti con caratteristiche clinico-auxologiche in accordo con il punto I e
con normale secrezione di GH (punto II), la terapia può essere effettuata solo
se autorizzata dalla Commissione Regionale preposta alla sorveglianza
epidemiologica ed al monitoraggio dell’appropriatezza del trattamento con
GH in base alle più recenti acquisizioni scientifiche in materia.
ma non specificava le tipologie di pazienti, la durata
dell'autorizzazione,
i criteri per la prosecuzione o per la sospensione del trattamento
Fonte dati: Registro GH Piemontese,
attivo dal 1999, dal 2010 strumento ufficiale di erogazione del P.T.
Elaborazione e supervisione dei dati:
BASSA STATURA: TRATTAMENTO CON GH NON
CONVENZIONALE:
Metodologia di lavoro
Area Pediatrica P. Matarazzo, S. Vannelli, S. Bellone
Registro GH A. Borraccino, G. Migliaretti
Formazione/comunicazione A. Ravaglia
(Area Adulti - G. Aimaretti)
Torino OIRM: Auxologia, S. Vannelli; Endocrinologia, P.
Matarazzo;
MOLINETTE: Endocrinologia, L. Ghizzoni;
MAURIZIANO: Pediatria, F. Massara
Orbassano: Pediatria, C. Montanari
Alessandria: Pediatria, F. Pesce,
Asti: Pediatria, L. Startari
Cuneo: Pediatria, V. De Donno
Novara: Pediatria, S. Bellone
Tortona: Pediatria, F. Fontana
Verbania: Pediatria, A. Sartorio, G. Mazzilli
Franco Cavallo, Gianni Bona, Roberto Lala, Lucia Ghizzoni, Aldo
Ravaglia, Michelangela Pozzetto, Jolanda Davletbaiev Commissione GH
REGISTRO PIEMONTESE GH:
criteri di inclusione al trattamento
con rhGH
1. Criteri auxologici conformi al punto I a della Nota AIFA 39
2. Valutazione diagnostica completa in base al PDTA della bassa statura della Regione Piemonte (farlo entrare)
3. Invio dati alla Commissione GH tramite il modulo “SUPERVISIONE” del Registro GH Piemontese
4. Approvazione della Commissione GH Piemonte:
per 2 anni nei soggetti < 10 anni con BSI, SGA, SHOX, Ipocondroplasia
per 1 anno nei soggetti < 10 anni con Acondroplasia, Sindromi, Malattie Croniche, e nei soggetti > 10 anni con ogni diagnosi precedente
11/10/13
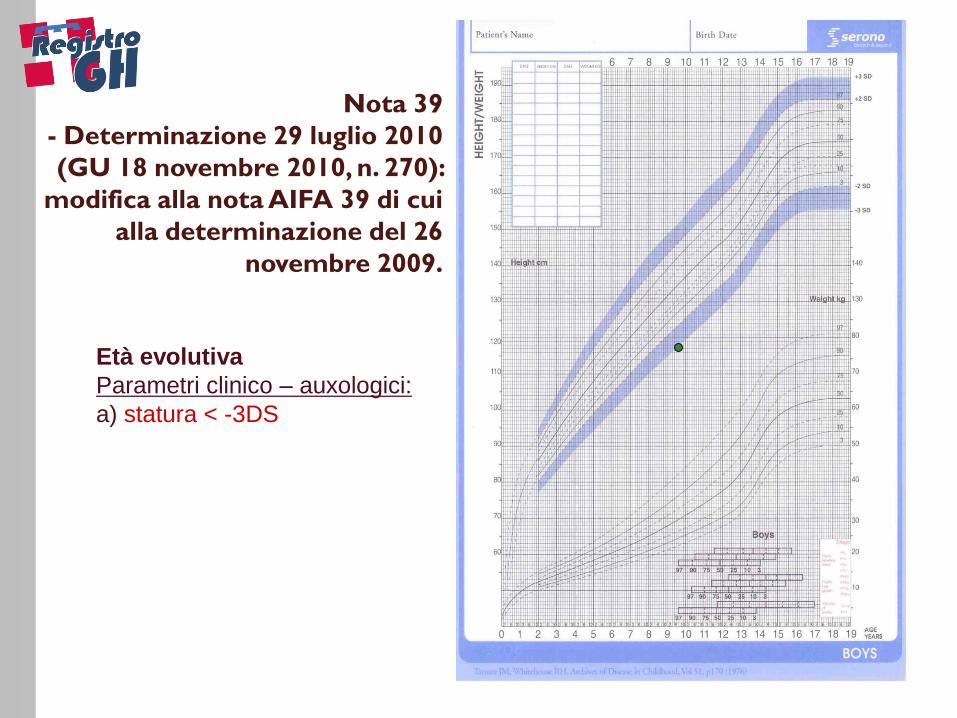
Età evolutiva
Parametri clinico – auxologici:
a) statura < -3DS
Nota 39
- Determinazione 29 luglio 2010
(GU 18 novembre 2010, n. 270):
modifica alla nota AIFA 39 di cui
alla determinazione del 26
novembre 2009.
11/10/13
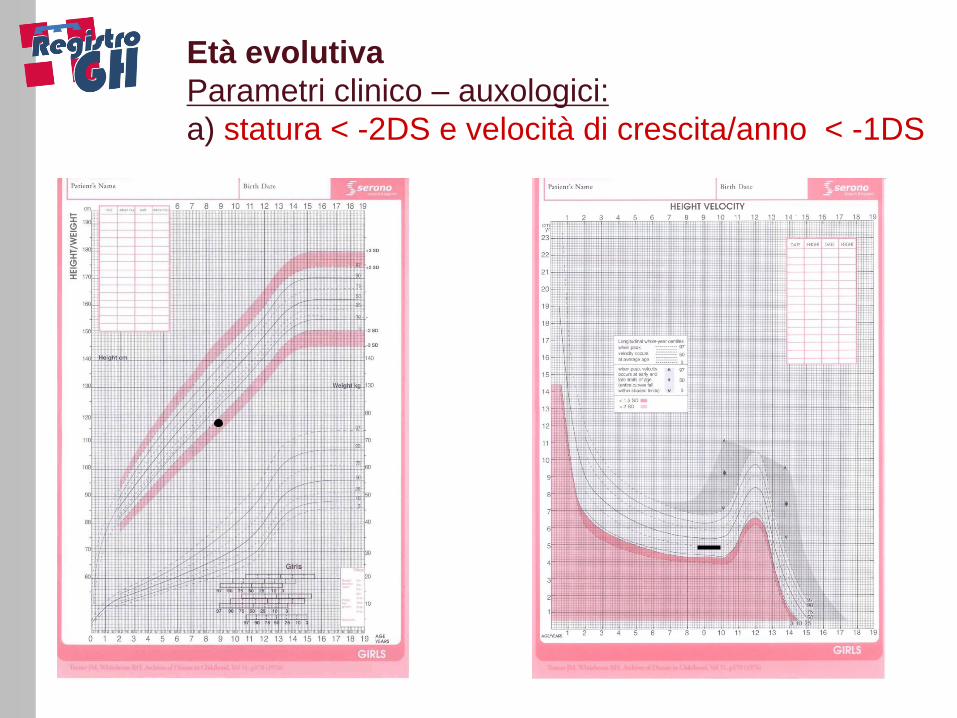
Età evolutiva
Parametri clinico – auxologici:
a) statura < -2DS e velocità di crescita/anno < -1DS
11/10/13
REGISTRO PIEMONTESE GH:
criteri di inclusione al trattamento
con rhGH
1. Criteri auxologici conformi al punto I a della Nota AIFA 39 (far entrare la nota oppure le curve di Tanner segnando i criteri della nota)
2. Valutazione diagnostica completa in base al PDTA della bassa statura della Regione Piemonte
3. Invio dati alla Commissione GH tramite il modulo “SUPERVISIONE” del Registro GH Piemontese
4. Approvazione della Commissione GH Piemonte:
per 2 anni nei soggetti < 10 anni con BSI, SGA, SHOX, Ipocondroplasia
per 1 anno nei soggetti < 10 anni con Acondroplasia, Sindromi, Malattie Croniche, e nei soggetti > 10 anni con ogni diagnosi precedente
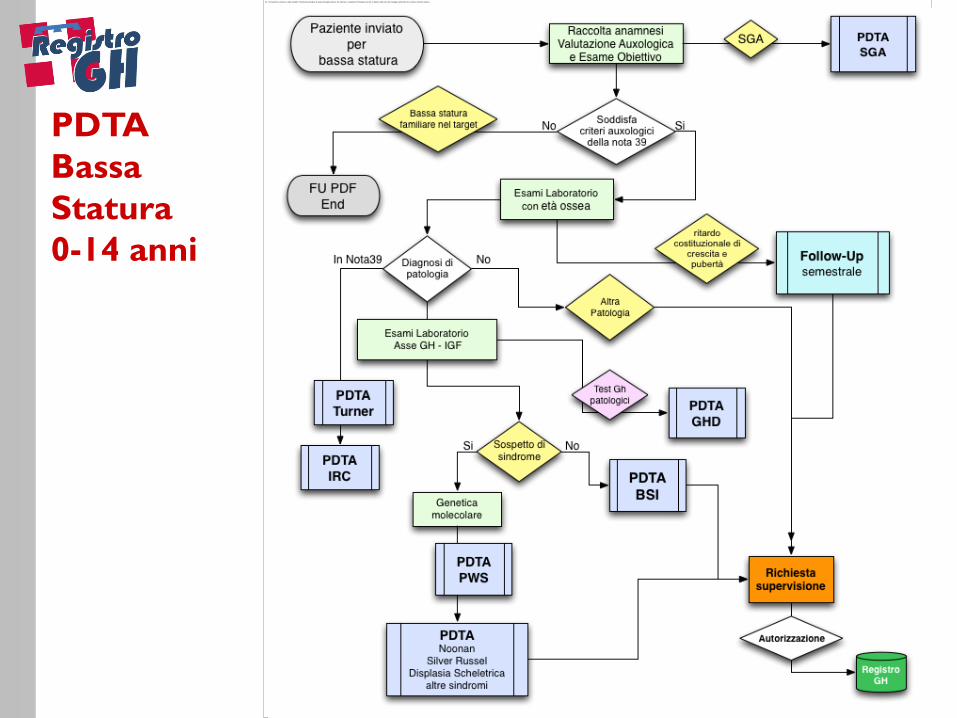
PDTA
Bassa
Statura
0-14 anni
REGISTRO PIEMONTESE GH:
criteri di inclusione al trattamento
con rhGH
1. Criteri auxologici conformi al punto I a della Nota AIFA 39 (far entrare la nota oppure le curve di Tanner segnando i criteri della nota)
2. Valutazione diagnostica completa in base al PDTA della bassa statura della Regione Piemonte
3. Invio dati alla Commissione GH tramite la sezione “SUPERVISIONE” del Registro GH Piemontese
4. Approvazione della Commissione GH Piemonte:
per 2 anni nei soggetti < 10 anni con BSI, SGA, SHOX, Ipocondroplasia
per 1 anno nei soggetti < 10 anni con Acondroplasia, Sindromi, Malattie Croniche, e nei soggetti > 10 anni con ogni diagnosi precedente
5. Rivalutazione al termine del periodo concesso di trattamento: criteri di efficacia
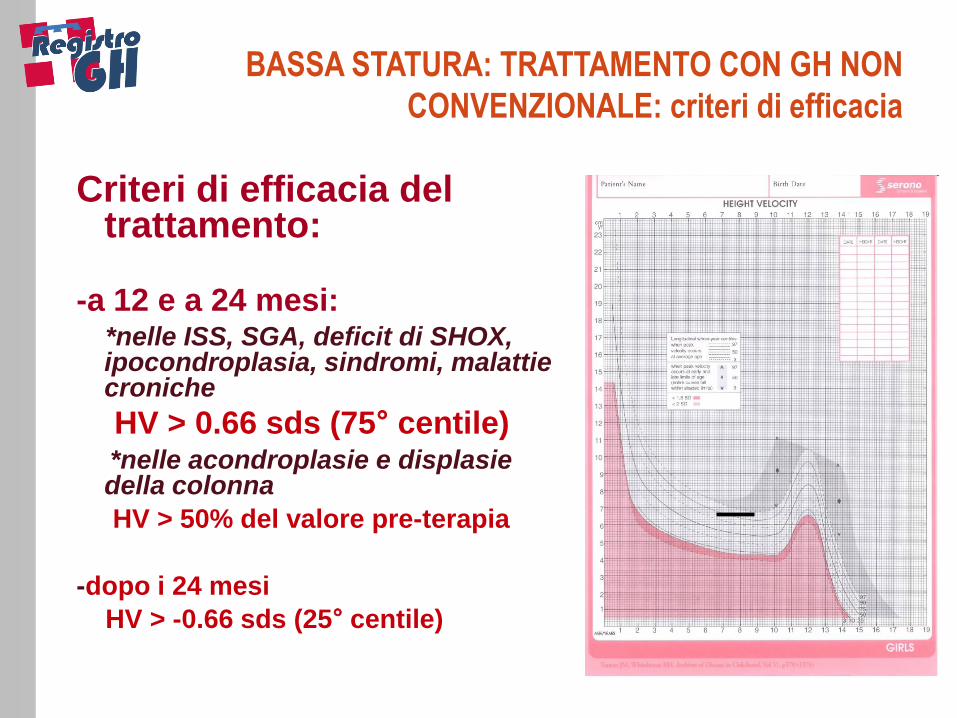
Criteri di efficacia del trattamento:
-a 12 e a 24 mesi: *nelle ISS, SGA, deficit di SHOX,
ipocondroplasia, sindromi, malattie croniche
HV > 0.66 sds (75° centile) *nelle acondroplasie e displasie
della colonna
HV > 50% del valore pre-terapia
-dopo i 24 mesi
HV > -0.66 sds (25° centile)
BASSA STATURA: TRATTAMENTO CON GH NON
CONVENZIONALE: criteri di efficacia
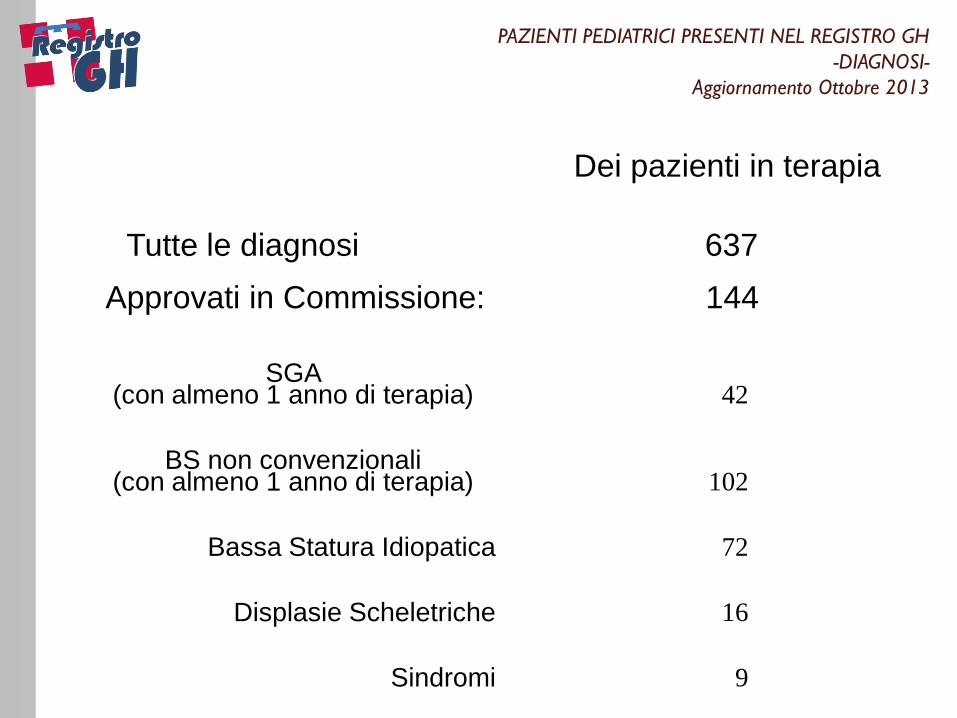
PAZIENTI PEDIATRICI PRESENTI NEL REGISTRO GH
-DIAGNOSI-
Aggiornamento Ottobre 2013
Dei pazienti in terapia
Tutte le diagnosi 637
SGA (con almeno 1 anno di terapia) 42
BS non convenzionali (con almeno 1 anno di terapia) 102
Bassa Statura Idiopatica 72
Displasie Scheletriche 16
Sindromi 9
Malattie croniche 5
Approvati in Commissione: 144
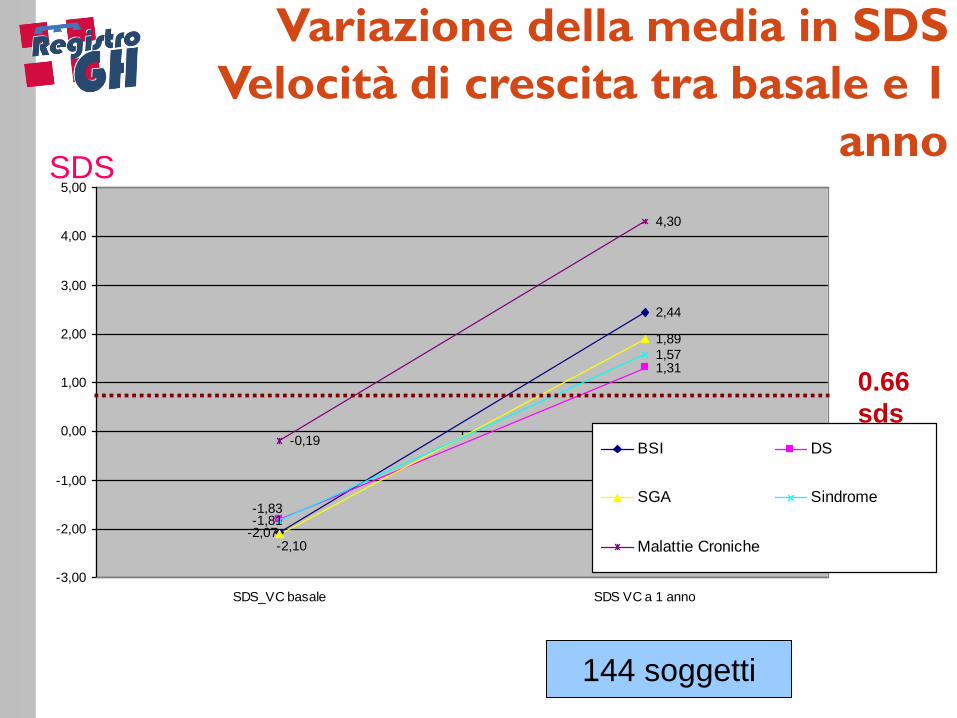
Variazione della media in SDS
Velocità di crescita tra basale e 1
anno SDS
2,44
1,31
1,89
1,57
-0,19
4,30
-2,07-1,81
-2,10
-1,83
-3,00
-2,00
-1,00
0,00
1,00
2,00
3,00
4,00
5,00
SDS_VC basale SDS VC a 1 anno
BSI DS
SGA Sindrome
Malattie Croniche
144 soggetti
0.66
sds
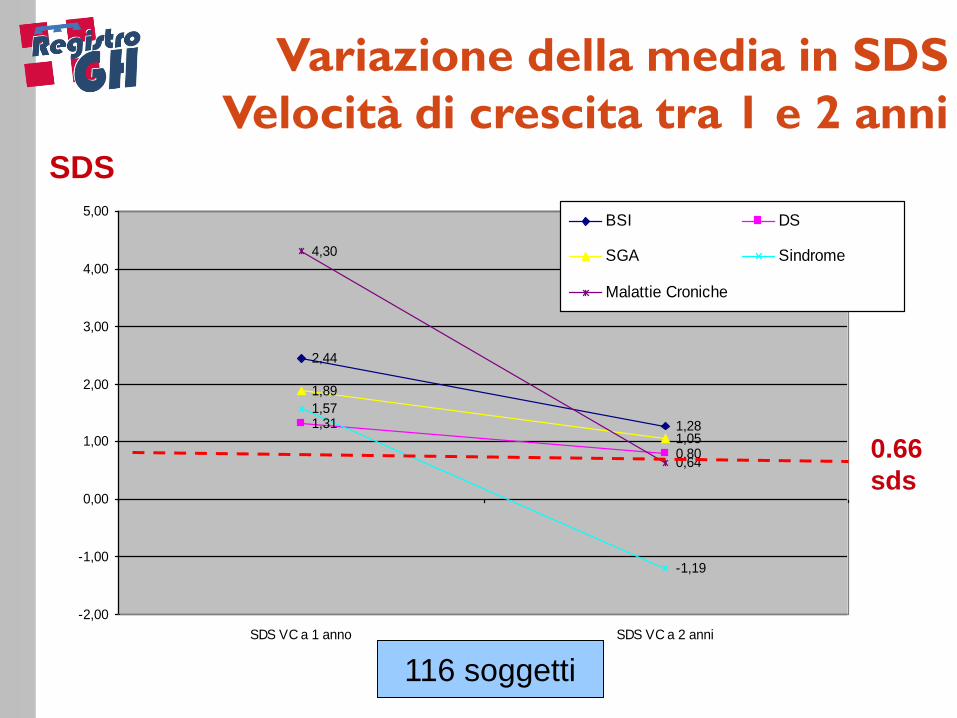
SDS
2,44
1,281,31
0,80
1,89
1,05
1,57
-1,19
4,30
0,64
-2,00
-1,00
0,00
1,00
2,00
3,00
4,00
5,00
SDS VC a 1 anno SDS VC a 2 anni
BSI DS
SGA Sindrome
Malattie Croniche
0.66
sds
Variazione della media in SDS
Velocità di crescita tra 1 e 2 anni
116 soggetti
I
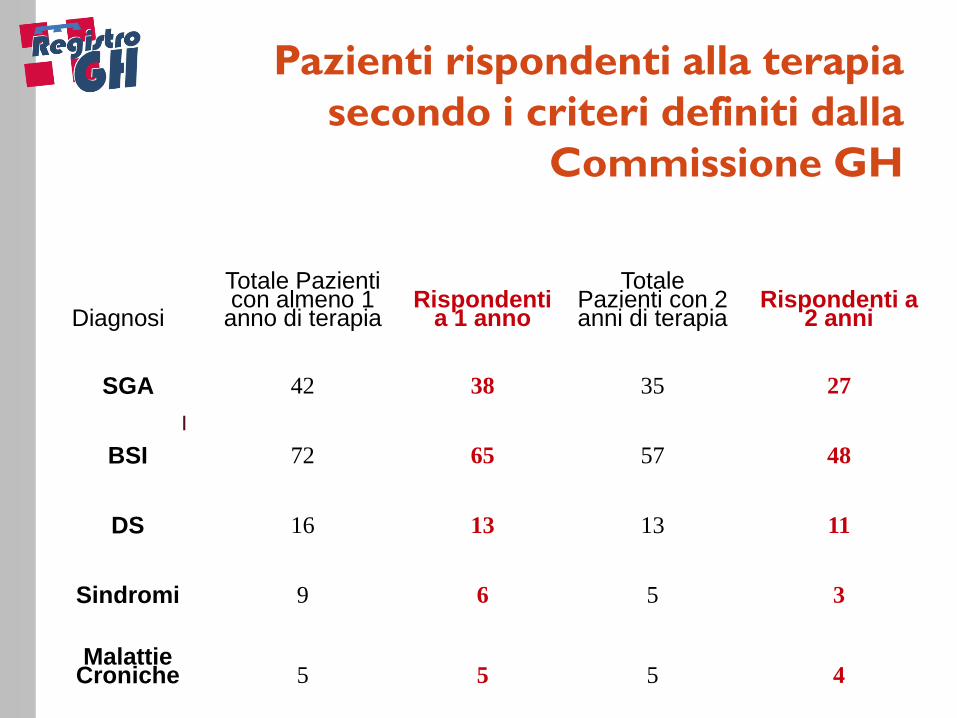
Pazienti rispondenti alla terapia
secondo i criteri definiti dalla
Commissione GH
Diagnosi
Totale Pazienti con almeno 1
anno di terapia Rispondenti
a 1 anno
Totale Pazienti con 2 anni di terapia
Rispondenti a 2 anni
SGA 42 38 35 27
BSI 72 65 57 48
DS 16 13 13 11
Sindromi 9 6 5 3
Malattie Croniche 5 5 5 4
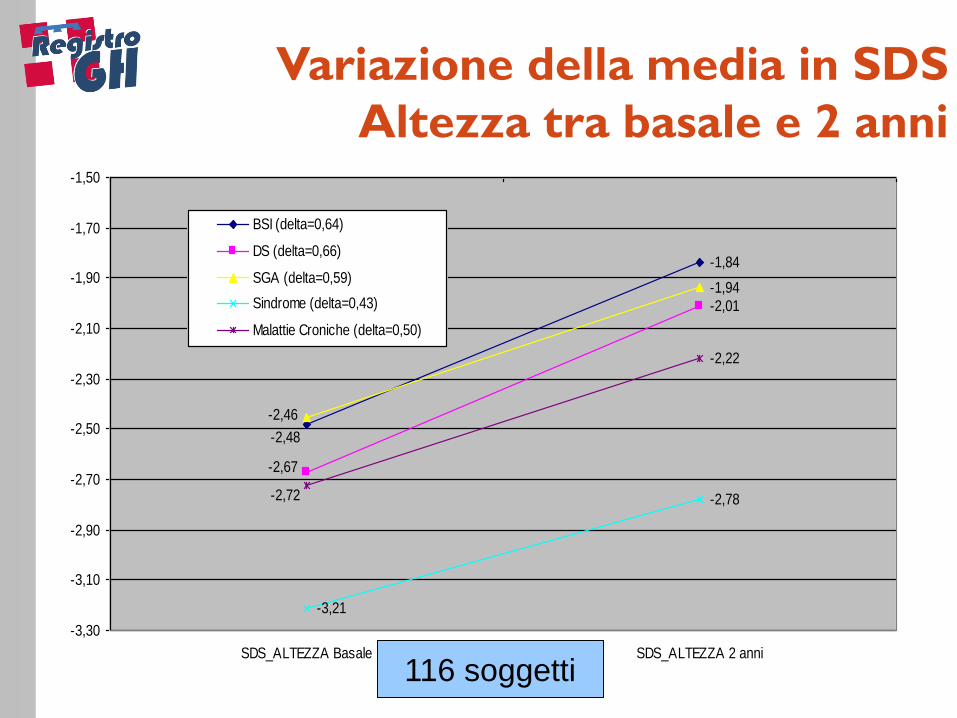
Variazione della media in SDS
Altezza tra basale e 2 anni
-1,84
-2,01
-1,94
-3,21
-2,78
-2,22
-2,48
-2,67
-2,46
-2,72
-3,30
-3,10
-2,90
-2,70
-2,50
-2,30
-2,10
-1,90
-1,70
-1,50
SDS_ALTEZZA Basale SDS_ALTEZZA 2 anni
BSI (delta=0,64)
DS (delta=0,66)
SGA (delta=0,59)
Sindrome (delta=0,43)
Malattie Croniche (delta=0,50)
116 soggetti
-Dose terapeutica: 0.22-0.28 mg/kg/sett. a seconda dell'età (prepubere/pubere), della patologia e dei livelli di IGF......senza mai superare la dose WARNING EMA di 50 mcg/kg/die
-Valutazione parametri metabolici e livelli di IGF per monitoraggio efficacy and safety
-Segnalazione puntuale effetti collaterali/eventi avversi
TRATTAMENTO NON CONVENZIONALE
CON GH NELLA BASSA STATURA: non solo
criteri di efficacia
-Il trattamento con rhGH non convenzionale in quadri di grave bassa statura è efficace.... ma occorrono criteri di efficacia condivisi.....e specifici per patologia
-La “good response” va correlata con i fattori predittivi noti: età inizio terapia, TH, IGF pre-terapia, HV pre-terapia..
-Il follow up va prolungato....fino alle altezze adulte definitive
-La casistica va ampliata (studio multicentrico con le altre Regioni...)
-Gli strumenti di valutazione e previsione della risposta terapeutica vanno implementati......(Prof. Migliaretti)
-Il miglioramento degli aspetti psicologici e di qualità di vita va considerato e “pesato”......dai dati di “patologia” al singolo individuo
TRATTAMENTO NON CONVENZIONALE
CON GH NELLA BASSA STATURA:
riflessioni e prospettive future.
BASSA STATURA NON
CONVENZIONALE:
proposta di curve di crescita
Giuseppe Migliaretti Dipartimento di Scienze Cliniche e Biologiche,
Università di Torino
11/10/13
Da letteratura sollecitazioni a proporre modelli
predittivi della crescita in pazienti trattati con
ormone somatotropo (GH)
1. Kaplowitz et al. International Journal of Pediatric Endocrinology
2013, 2013-9
2. Ranke et al. BMC Medical Informatics and Decision Making 2011,
11:38
3. Topor et al. Pediatrics. 2010 November ; 126(5): 938–944.
CURVA DI CRESCITA DEI PAZIENTI
BSI, SGA e SHOX.
Introduzione
11/10/13
Proposta di curva di crescita per i pazienti con diagnosi di BASSA STATURA NON CONVENZIONALE
in trattamento con GH
CURVA DI CRESCITA DEI PAZIENTI
BSI, SGA e SHOX.
Obiettivo
11/10/13
Follow-up completo dei pazienti
BSI, SGA e SHOX
con almeno 1 anno di terapia
(follow-up da 1 a 4 anni - media 3 anni)
CURVA DI CRESCITA DEI PAZIENTI
BSI, SGA e SHOX.
Base dati
11/10/13
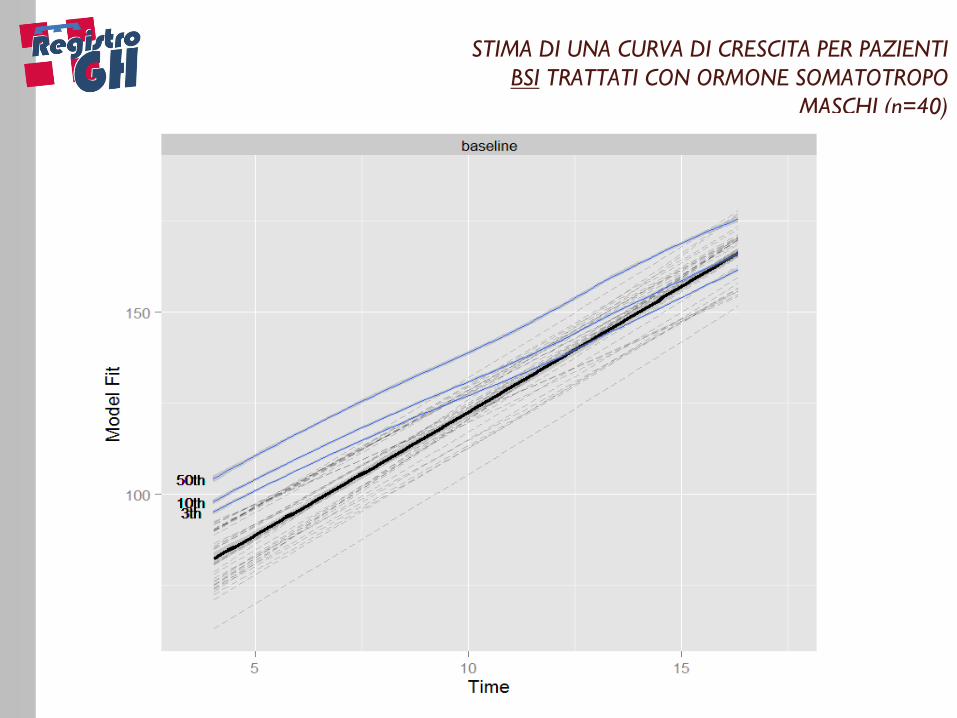
Per la stima della curva di crescita è stato
utilizzato un modello bayesiano gerarchico semiparametrico per dati longitudinali gia’
proposto in letteratura [4, 5]
CURVA DI CRESCITA DEI PAZIENTI
BSI, SGA e SHOX.
Metodi
4. T.D. Savitsky and S.M. Paddock. Bayesian Hierarchical Semiparametric Modeling of Longitudinal Post-treatment Outcomes from Open-enrolment Therapy Groups. Journal of the Royal Statistical Society: 2013. Series A 176(3):795-808
5. Migliaretti G, Berchialla P, Borraccino A, Gregori D, Cavallo F; Commissione GH Piemonte. A mathematical model in the analysis of the response to growth hormone treatment in pediatric patients with diagnosis of
growth hormone deficiency. J Endocrinol Invest. 2012 Feb;35(2):209-14.
11/10/13
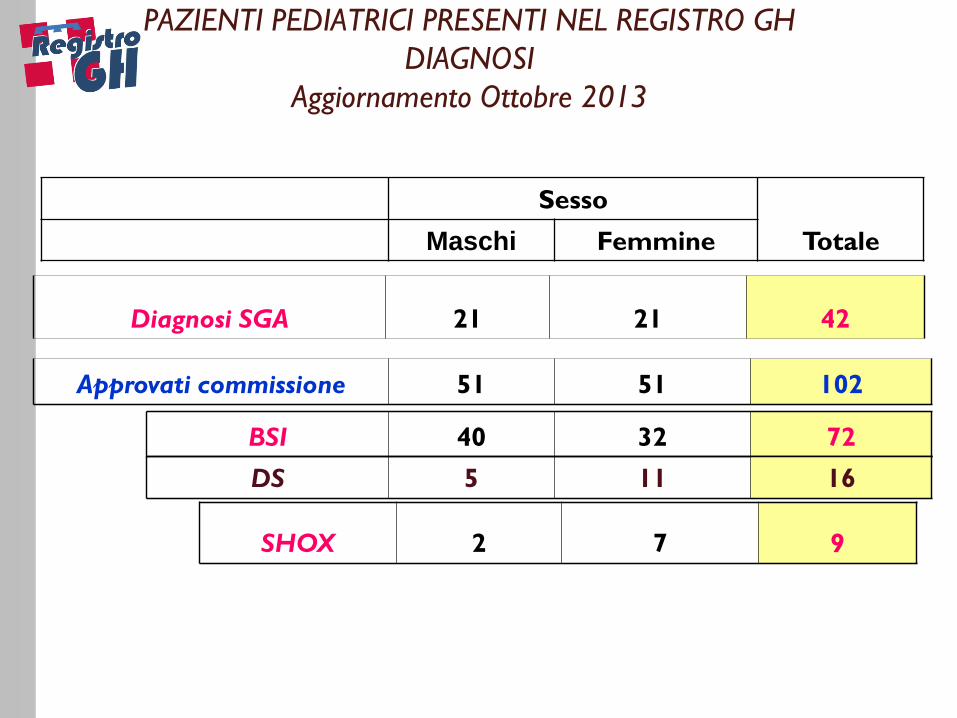
PAZIENTI PEDIATRICI PRESENTI NEL REGISTRO GH
DIAGNOSI
Aggiornamento Ottobre 2013
Diagnosi SGA 21 21 42
Approvati commissione 51 51 102
BSI 40 32 72
DS 5 11 16
SHOX 2 7 9
Sesso
Totale Maschi Femmine
11/10/13
STIMA DI UNA CURVA DI CRESCITA PER PAZIENTI
BSI TRATTATI CON ORMONE SOMATOTROPO
MASCHI (n=40)
11/10/13
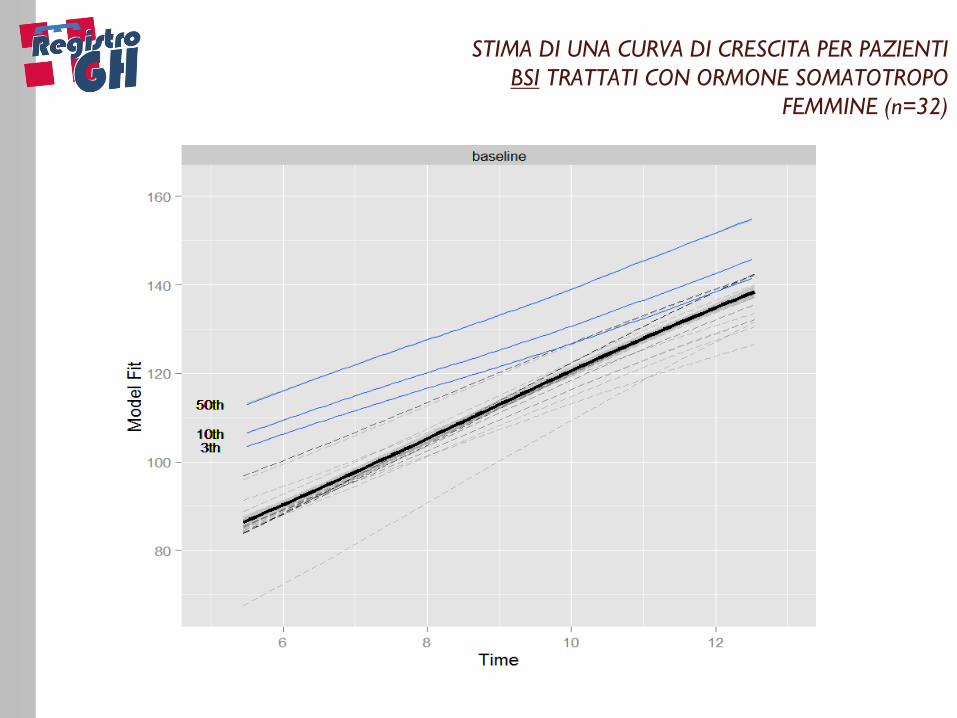
STIMA DI UNA CURVA DI CRESCITA PER PAZIENTI
BSI TRATTATI CON ORMONE SOMATOTROPO
FEMMINE (n=32)
11/10/13
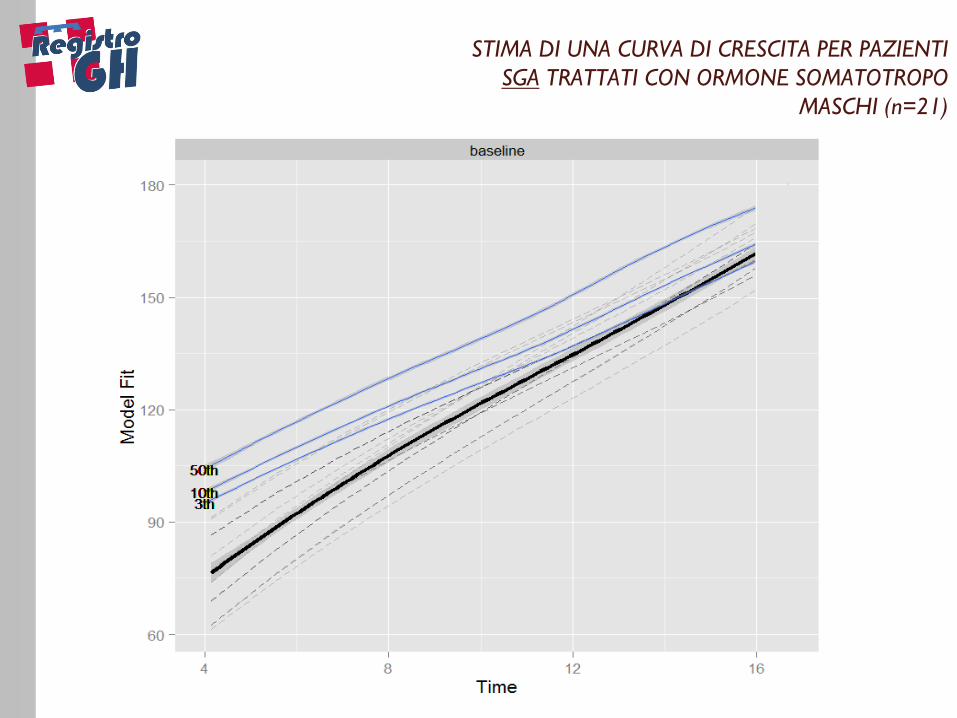
STIMA DI UNA CURVA DI CRESCITA PER PAZIENTI
SGA TRATTATI CON ORMONE SOMATOTROPO
MASCHI (n=21)
11/10/13
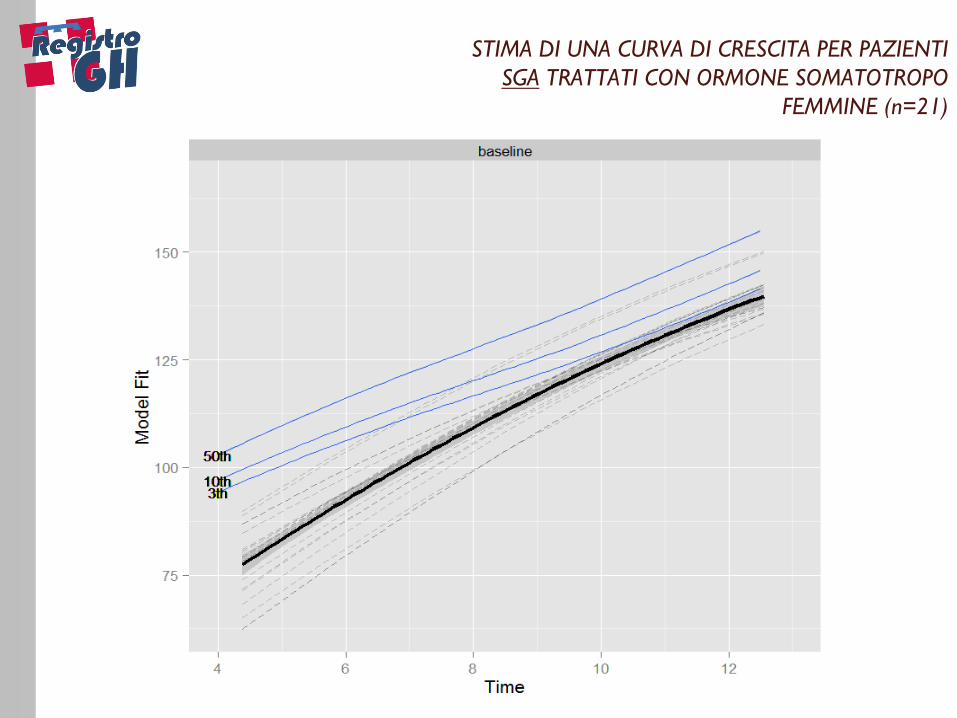
STIMA DI UNA CURVA DI CRESCITA PER PAZIENTI
SGA TRATTATI CON ORMONE SOMATOTROPO
FEMMINE (n=21)
11/10/13
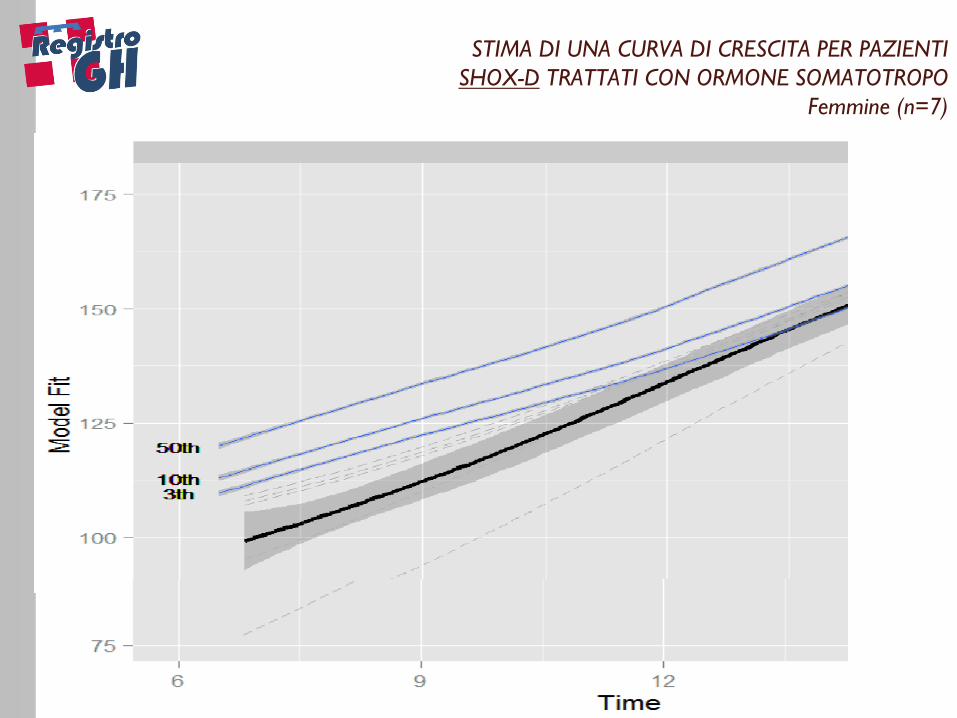
STIMA DI UNA CURVA DI CRESCITA PER PAZIENTI
SHOX-D TRATTATI CON ORMONE SOMATOTROPO
Femmine (n=7)
11/10/13
Conclusioni
VANTAGGI DEI MODELLI PRESENTATI:
1. Presentano una ipotesi di curva di crescita SPECIFICA per
diagnosi dei pazienti in trattamento con diagnosi ‘non
convenzionale’
2. Effetto del trattamento che, sotto l’ipotesi di una crescita attesa
lungo il centile di riferimento all’inizio della terapia (<3°),
sembrerebbe evidenziare un effetto a lungo termine che porta il
paziente a raggiungere (e superare) il 3° centile a fine crescita

11/10/13
Conclusioni
SVILUPPI
Perfezionamento dei modelli presentati, anche mediante un controllo
per i vari fattori di confondimento (per esempio il BG),
OBIETTIVO FUTURO
anche nell’ottica sempre più diffusa di una medicina personalizzata,,
costruire modelli che siano di ausilio nella previsione di crescita
‘individualizzata’ per il paziente a inizio terapia

11/10/13
Ringraziamenti
Paola Berchialla
Dip di Scienze Cliniche e Biologiche
Università di Torino












