Farmaci antifunginei
66
Farmaci antifunginei 1] Dermatophytes Microsporum , Epidermophyton e Trichophyton 2] Candida 3] Aspergillus 4] Cryptococcus 5] Rhizopus ... Funghi patogeni per l‘uomo Un fungo è un organismo appartenente alla famiglia degli eucarioti quali la famiglia dei lieviti, muffe ed i caratteristici funghi edili e tossici Microsporum canis Candida albicans
description
Farmaci antifunginei. Un fungo è un organismo appartenente alla famiglia degli eucarioti quali la famiglia dei lieviti, muffe ed i caratteristici funghi edili e tossici. Funghi patogeni per l ‘ uomo. 1] Dermatophytes Microsporum , Epidermophyton e Trichophyton 2] Candida - PowerPoint PPT Presentation
Transcript of Farmaci antifunginei

Farmaci antifunginei
1] DermatophytesMicrosporum, Epidermophyton e Trichophyton
2] Candida3] Aspergillus4] Cryptococcus5] Rhizopus...
Funghi patogeni per l‘uomo
Un fungo è un organismo appartenente alla famiglia degli eucarioti quali la famiglia dei lieviti, muffe ed i caratteristici funghi edili e tossici
Microsporum canis
Candida albicans


Aspergillus fumigatus is a saprophytic fungus that plays anessential role in recycling environmental carbon and nitrogen.
It sporulates abundantly, with every conidial head producing thousands of conidia. The conidia released into the atmosphere have a diameter small enough (2 to 3 mm) to reach the lung alveoli. A. fumigatus does not have an elaborate mechanism for releasing its conidia into the air.
Over the past 10 years, A.fumigatus has become the most prevalent airborne fungal pathogen, causing severe and usually fatal invasive infectionsin immunocompromised hosts in developed countries.

For most patients, the main portal of entry and site of infection for A. fumigatus is the respiratory tract.
Sites of infections have been described in the normal or immunocompromised host, such as the skin, peritoneum, kidneys, bones, eyes, and gastrointestinal tract.
At present, only AmB and itraconazole are available to treat aspergillosis. In spite of their activity in vitro, the efficacy of these drugs in vivo against A. fumigatus remains low, and as a consequence, mortality from IA remainshigh.
Detection of galactomannan in bronchoalveolar lavage fluid seems to be a promising tool for rapid diagnosis in the critical care setting.




CATHETER-RELATED BLOODSTREAM INFECTIONS AND CANDIDA BIOFILMSCandida species are the fourth leading cause of health care-associated infections and the third most common cause of central line-associated bloodstream infections. Candida species are associated with the highest overall crude mortality of all nosocomial bloodstream infections, comparable to that of Pseudomonas and exceeding that of Staphylococcus aureus infections.Candida albicans is the most common fungal species associated with biofilm-related infections.In addition to device- and catheter-related infections, endocarditis and other prosthetic infections have also been associated with biofilm formation. In patients with candidemia, biofilm-producing strains of Candida species have been associated with increased morbidity and mortality compared to non-biofilm-producing strains.



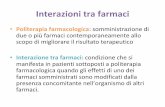
Infezioni cutanee da funghi
Trichophyton mentagrophytes
Microsporum canis (Tinea capitis)
http://nedo.gumed.edu.pl/wszpziu/skrypty/Atlas%20Dermatol/I_Derma/000IM02.pdf

Tinea corporis
Tinea faciei Tinea cruris

Candidiosi, Stomatite, Mughetto Intertrigine da candida (ascelle)
Candidiosi da pannolino

Oncimicosi





POLIENIAmphotericina B, Nistatina
AZOLIImidazoles:
Ketoconazolo..Triazoles: Fluconazolo,
itraconazolo, voriconazolo, posaconazolo, ravuconazolo
ALLILAMMINETerbinafina, butenafina
MORFOLINEAmorolfine
PIRIMIDINE FLUORINATEFlucitosina
Farmaci antifunginei suddivisi per classi

ECHINOCANDINECaspofungin, anidulafungin, micafungin
PEPTIDE-NUCLEOSIDENikkomicina Z
DERIVATI TETRAIDROFURANICISordarine,
azasordarine ALTRI
Griseofulvina
Farmaci antifunginei suddivisi per classi

Nature Reviews Drug Discovery | AOP, published online 20 August 2010; doi:10.1038/nrd3074


1] Agenti che interferiscono con l ‘ integrita’della membrana
Amphotericina B, Nistatina
2] Inibitori della sintesi dell ‘ ergosterolo
Azoli, allilamine, morfoline
3] Inibitori degli acidi nucleiciFlucitosina
4] AntimitoticiGriseofulvina
5] Inibitori della sintesi del glucano
Echinocandine
6] Inibitori della sintesi della chitina
Nikkomicina
MECCANISMO DI AZIONE
7] Inibitori della sintesi proteica
Sordarine, azasordarine

naftifina clotrimazoloeconazoloketoconazolooxiconazolosertaconazolosulconazolo
butenafina
ciclopiroxclotrimazole-betamethasone
Topical allylamines Topical azoles
Other topical antifungals

AMFOTERICINA B genera dei pori nella membrana
Usi terapeutici :
- Leishemaniosi mucocutanea americana- Aspergillosi invasiva- Blastomicosi- Candidiosi ( E’ presente per il 60% nei pazienti affetti da HIV e in più dell’80% in sogggetti con AIDS.)- Meningite criptococcica in pazienti con HIV- Criptococcosi polmonare- Infezioni funginee del SNC

Effetti collaterali generali :
Perdita di peso corporeoDiarrea, indigestione, perdita dell’appetito, nausea, vomitoFebbre, mal di testa
Effetti collaterali gravi :
Aritmia cardiaca, ipotensione tromboflebitiIpocaliemiaAnafilassiNefrotossicitàconvulsioni
Effetti collaterali Amfotericina B

In addition to infusion-related adverse effects, Amphotericin B ( AmB) may be associated with considerable cumulative toxicity like cardiotoxicity, neurotoxicity and, most notably, nephrotoxicity (60–80% of patients), the latter manifesting in tubular injury and a poorly understood renal vasoconstriction. Although AmB’s nephrotoxic effects are to a certain extent preventable (e.g. by sodium supplementation) and reversible, they represent the main dose-limiting determinants. Fortunately, all approved lipid-based formulations were shown to significantly reduce t he likelihood of severe azotaemia compared to conventional D-AmB, even in patients treated concomitantly with other nephrotoxic drugs. Thus, in many hospitals, conventional D-AmB, despite its lower cost, is largely abandoned as a therapeutic agent against IA . Despite its unfavourable safety profile, AmB still represents the best proven and most important therapeutic option in salvage situations and in the management of breakthrough infections.

Treatment and follow-up
Treatment regimen consisted of griseofulvin at the dose of 15 mg/kg/d for 6-12 weeks, associated with antifungal topicals for all infants except five (less than 6 months of age), which were treated just by antifungal topicals.
The tolerance of treatment was excellent and no side effects or abnormal results in blood chemistry tests were observed.
The follow-up in 30 infants showed complete hair re-growth in 28 cases; 2 cases of kerion showed persistent alopecia.

Interazione tra farmaciGriseofulvin has long been a concern in its interaction with anticoagulants, hormone replacement therapy agents, sedatives, and anticonvulsants.
FarmacocineticaThe antifungal agent griseofulvin is also poorly water soluble drug, and its absorption from oral route is also poor, as a result, failure in providing effective plasma drug profile on conventional oral administration.
GRISEOFULVINA
Meccanismo di azioneGF is known to inhibit the growth of fungal, plant and mammalian cells mainly by inducing abnormal mitosis and blocking the cells at G2/M phase of cell cycle.


Case report

Ketoconazolo
TERB
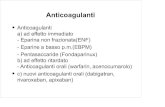
Lo Squalene è il precursore di tutte le famiglie di steroidi

Classification of triazoles
First generation of triazoles• Fluconazole• Itraconazole
Second generation of triazoles• Voriconazole • Posaconazole • Ravuconazole

Fluconazole was discovered by Richardson et al. working atPfizer in Sandwich, UK in a programme initiated in 1978. Theoriginal patent covering its structure had been filed by Riley andcolleagues at ICI Pharmaceuticals, who discontinued antifungalresearch prior to fluconazole’s launch. Fluconazole was identifiedbecause of its in vivo activity, and only many years later werein vitro systems found to measure in vitro activity. Phase 2 studiescommenced in 1988 and were focused on Candida, cryptococcaland coccidioidal infections, initially using doses of 50 mg daily.3–6Prophylaxis studies in neutropenia followed. The increasing needfor orally active azoles because of the AIDS epidemic, andrespectable efficacy despite low doses of the drug, led to rapid Foods and Drugs Administration and European licensures in 1990.

Il ketoconazolo può essere micostatico o fungicida a seconda delle dosi. Inibisce la sintesi dell’ergosterolo che porta come risultato il danno della membrana cellulare con fuoriscita degli elementi intracellulari necessari per la vita del fungo. Inibisce la sintesi dei trigliceridi e dei fosfolipidi dei funghi.
Il fluconazolo è un inibitore del CYP450 umano particolarmente degli isoenzimi CYP2C9 e CYP3A4.
Meccanismo di azione


Fluconazole: Fluconazole is an oral and parenteral agent. It readily penetrates into tissues due to its low lipophilic nature and limited protein binding; it is approximately 90% bioavailable. Concentrations in urine are several fold greater than in blood (10- to 20-fold greater) (11,12). Rare, but serious, hepatotoxicity may be associated with fluconazole. Drug interactions are possible because fluconazole is an inducer of cytochrome P450 isoenzymes. Clinical use in paediatrics: Fluconazole, the azole that is most widely used in paediatrics, is often used in the treatment of Candida and cryptococcal infections. It is more active against Candida albicans compared with other candidial strains (eg, Candida parapsilosis, Candida glabrata, Candida krusei and Candida tropicalis).

Voriconazole (VRC) is a triazole antifungal agent, which demonstrated good activity against Aspergillus strains, even when resistant to AmB and itraconazole (ITC). As is the case for all triazole antifungal agents, VRC inhibits the fungal enzyme 14 alfa-lanosterol demethylase, which catalyses a key step in the membrane synthesis, namely the conversion of lanosterol to ergosterol.
Voriconazole
Although all the antifungals have some hepatotoxic potential, the imidazoles seem to have a higher incidence; therefore, it is important to determine liver status before prescribing. Of greater concern is the large list of interactions mostly related to cytochrome P450 metabolism, a very long list of prominent drugs, including the statins.
TRIAZOLI

Inibizione deglienzimi coinvolti nellasintesi di ergosteroloda parte dei farmaciAntifunginei azolici, morfolinici e allilaminici.

Meccanismo di resistenza dei funghi agli azoli
1) Alterazione della 14 alfa demetilasi
2) Sovraespressione della lanosterolo demetilasi
3) Alterazione dei sistemi di efflusso
4) Cambiamento della composizione degli steroli di
membrana della cellula funginea


FLUCITOSINA(5-fluorocitosina)
Flucitosinacytosine deaminase
5 fluorouracile
5 fluorouracile 5-fluorodeo5-fluorodeossissiuridinuridinaa monomonoffososffatatoo
InInibizione sintesi DNAibizione sintesi DNA
5 fluorouracileUracil fosforibosil trasferasi
Acido 5 fluoro uridilico
Acido 5 fluoro uridilicoFosforilazione
5-fluoro-UTP5-fluoro-UTP
Incorporato nella sintesi dell‘RNA con risultato di inibizione della sintesi proteica

The final milestone of antifungal drug discovery in the 20th century was the identification and development of echinocandin antifungal agents.
Echinocandins are semisynthetic lipopeptides that inhibit synthesis of β-1,3-d-glucan in susceptible fungi, leading to damage of the fungal cell wall. Because a glucan-rich cell wall is a target not found in mammalian cells, these agents were predicted to be effective antifungal agents with very little collateral toxicity in mammalian cells—a prediction that has been proven true in clinical trials of patients with invasive candidiasis15-17 and aspergillosis.
However, echinocandins still lack activity against some common opportunistic yeasts (Cryptococcus species) and less common molds (ie, Fusarium, Scedosporium, and Mucorales) that often develop as breakthrough infections in severely immunocompromised patients.
ECHINOCANDINE

Echinocandine
Inibizione della sintesi del glucano componente della membrana cellulare
1) caspofungin, 2) micafungin 3) anidulafungin
Echinocandina BMicafungin was introduced into the market in 2005


Fks1p and Fks2p involvement in the synthesis of beta1:3 glucan in the cell walls.

Caspofungina
Viene somministrata per via endovenosa
CaspofunginEfficacy of Caspofungin in Invasive Aspergillosi (IA)
Caspofungin (CPF) is the first approved member of the class of echinocandins and the only member currently licensed for the therapy of Invasive Aspergillosi.
Echinocandins act as non-competitive inhibitors of the UDP-glucose- (1,3)-D -glucan- (3)- D -glucosyltransferase, commonly referred to as (1,3)-glucan synthase.
This enzyme is especially important in the cell wall synthesis of yeasts and molds . CPF is active against pathogenic Aspergillus and Candida species. Like all echinocandins, CPF is a high-molecular-weight lipoprotein and can thus be administered by intravenous infusion only.

MECHANISM OF ACTION AND IN VITRO ACTIVITY
In common with other echinocandins, micafungin inhibits the synthesis of 1,3-b-D-glucan, a major component of fungal cell wall, in a non-competitive, concentration-dependent manner. Micafungin has potent and fungicidal activity against a wide range of Candida spp. in vitro, including fluconazole-resistant Candida spp. and multidrug-resistant Candida spp. residing in biofilms .
Micafungin has poor oral bioavailability and is only available for intravenous administration. The compound is extensively (>99%) bound to plasma proteins, metabolized by the liver, and excretion predominantly occurs via the fecal route.

Meccanismo di resistenza alle echinocandine
Nel gene FKS1 è codificato l’enzima glucano sintasi mentre nel gene GNS1 è codificato un enzima che prende parte alla sintesi (estensione) degli acidi grassi.
Mutazioni genetiche di laboratorio hanno messo in evidenza che la mutazione di questi enzimi porta alla comparsa di resistenza alle echinocandine

Eur J Med Res (2011) 16: 159-166

http://infection.thelancet.com Vol 6 April 2006

La Chitina è un polimero della N-acetilglucosamina, costituente principale della parete cellulare dei funghi
La Nikkomicina è un inibitore della sintesi della chitina
Chitin—the term comes from a Greek word for tunic, a form of clothing worn in ancient Greece—was first discovered in 1811 by Henri Braconnot as a substance occurring in mushrooms (Braconnot 1811). Nowadays, it is known that chitin is highly abundant in nature. There are two allomorphic forms of chitin, namely, α-chitin and β-chitin, which differ in packing and polarities of adjacent chains in successive sheets (Aam et al. 2010; Chen et al. 2010).Fungal cell walls contain α-chitin.
Nikkomicina

Chitin is made by chitin synthases requiring specific microvesicles, the chitosomes, for intracellular transport. Fungi contain several chitin synthases, some of which may be essential at a certain stage. The most widely studied chitin synthase inhibitors are polyoxins and nikkomycins that probably bind to the catalytic site of chitin synthases.

Sir,Until the last decade, antifungal therapy was based mostly on drugs acting on the fungal membrane, such as amphotericin B and azoles, and the rationale for the use of combination therapy remained questionable. Thus, the only drug combination of two antifungals with two modes of activity used clinically, primarily in cryptococcosis, was amphotericin B and 5-fluorocytosine. The introduction of echinocandins, which act on the fungal cell wall by inhibiting glucan synthesis, opened the approach to explore different drug combinations, such as echinocandins and polyenes, or echinocandins and azoles, for various mycoses. Nikkomycin Z inhibits chitin synthesis, by acting as a competitive analogue of chitin synthase substrate UDP-N-acetylglucosamine. Since chitin is found in most fungal cell walls, inhibition of its synthesis may be considered as a potentialmeans for antifungal therapy.


Voriconazole is a second-generation triazole with broad spectrum of antifungal activity. the most important therapeutic impact is related to its activity against all common aspergillus spp. It is considered the first-line drug for the treatment of invasive aspergillosis.
VORICONAZOLO


Voriconazole is a triazole antifungal agent and is a second generation synthetic derivative of fuconazole; it is effective against yeast and lamentous fungi. The primary mode of action of voriconazole is the inhibition of cytochrome P-450- mediated 14-α-lanosterol demethylation, an essential step in fungal ergosterol biosynthesis and the resulting ergosterol depletion causes fungal cell wall destruction.

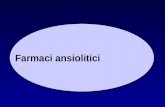
Common toxicities of antifungal agents. CNS = central nervous system; 5-FC = flucytosine; GI = gastrointestinal; IV = intravenous; QTc = corrected QT interval.

J Dtsch Dermatol Ges. 2011 Apr;9(4):274-6. doi: 10.1111/j.1610-0387.2010.07563.x. Epub 2010 Nov 3.
Severe phototoxicity associated with long-term voriconazole treatment.Vöhringer S, Schrum J, Ott H, Höger PH.Department of Pediatric Dermatology, Catholic Children's Hospital Wilhelmstift, Hamburg, Germany.Abstract
Voriconazole is a second-generation triazole antifungal approved for the treatment of invasive fungal infections, particularly with Aspergillus, Candida, Fusarium, and Scedosporium spp. Frequently reported adverse effects of voriconazole include visual disturbance (21 %), elevated liver enzymes (15.6 %) and rashes (7 %), which are largely attributable to drug-induced photosensitivity. We report a case of serious phototoxicity in a 8 year old boy who underwent chemotherapy for AML. He received voriconazole for the treatment and subsequent re-infection prophylaxis after pulmonary aspergillosis. One year after the start of therapy he developed blistering eruptions on his face after minimal sunlight exposure. Recent reports about the development of squamous cell carcinoma and melanoma, respectively, in children during and after oral therapy with voriconazole seem to warrant systematic follow-up investigations of all voriconazole-treated patients.

Expert Rev Pharmacoecon Outcomes Res. 2010 Dec;10(6):623-36.
Pharmacoeconomics of voriconazole in the management of invasive fungal infections.Al-Badriyeh D, Heng SC, Neoh CF, Slavin M, Stewart K, Kong DC.College of Pharmacy, Qatar University, Doha, Qatar.
AbstractThe incidence of invasive fungal infection has risen in recent years with the introduction of more intensive chemotherapy regimens and the advent of stem cell and solid-organ transplants. In patients undergoing chemotherapy, mortality rates ranging from 50 to 90% have been associated with documented invasive fungal infection. Voriconazole is a second-generation triazole, which is a synthesized derivative of fluconazole. It was first approved for marketing in the USA in 2002.Voriconazole has excellent bioavailability and is available in oral and intravenous dosage form. It has extended-spectrum antifungal activity whereby it is highly effective against a variety of fungal organisms, including Candida, Fusarium, Paecilomyces and Scedosporium species, but it is especially known for its activity against the Aspergillu s species.Voriconazole has become widely used for three types of treatment strategies (i.e., targeted, empirical and prophylactic).
However, voriconazole is a high-cost antifungal agent and, therefore, its effectiveness should be scrutinized, taking into consideration its cost in relation to the costs of other comparable antifungal agents.

Major information on the best therapeutic strategies for
cryptococcal meningoencephalitis derives from therapeutic trials involving HIV-positive [1,2,3] or HIV-negative patients [4].According to the current Infectious Diseases Society of America(IDSA) guidelines, the treatment should depend on anatomic siteand host’s immunological status. Induction therapy using acombination of amphotericin B (AMB, 0.7–1 mg/kg/d) andflucytosine (5FC, 100 mg/kg/d) for 2 weeks followed by aconsolidation phase of 10 weeks by fluconazole (FCZ, 400 mg/d) should be prescribed for central nervous system infection (CNS) in both HIV-positive and -negative patients, based mostly on data extrapolated from trials in HIV-infected patients [5] and retrospective studies onHIV-negative patients [6,7].
Conclusion: Our results support the conclusion that induction therapy with AMB+5FC for at least 14 days should be prescribed rather than any other induction treatments in all patients with high fungal burden at baseline regardless of their HIV serostatus and of the presence of proven meningoencephalitis.

Objectives: Invasive fungal infections are a major cause of mortality among patients at risk. Treatmentguidelines vary on optimal treatment strategies. We aimed to determine the effects of different antifungal therapies on global response rates, mortality and safety.Results: Our analysis included 11 studies enrolling a total of 965 patients. For our primary analysis of global response rates, we pooled 7 trials comparing azoles to amphotericin B, Relative Risk [RR] 0.87 (95% Confidence
Interval [CI], 0.78–0.96, P = 0.007, I2 = 43%, P = 0.09. We also pooled 2 trials of echinocandins versus amphotericin B and found a pooled RR of 1.10 (95% CI, 0.99–1.23, P = 0.08). One study compared anidulafungin to fluconazole and yielded a RR of 1.26 (95% CI, 1.06–1.51) in favor of anidulafungin. We pooled 7 trials assessing azoles versus amphotericin B for all-cause mortality, resulting in a pooled RR of 0.88 (95% CI, 0.74–1.05, P = 0.17, I2 = 0%, P = 0.96). Echinocandins versus amphotericin B (2 trials) for all causemortality resulted in a pooled RR of 1.01 (95% CI, 0.84–1.20, P = 0.93). Anidulafungin versusfluconazole resulted in a RR of 0.73 (95% CI, 0.48–1.10, P = 0.34). Our mixed treatment comparison analysis found
similar within-class effects across all interventions. Adverse event profiles differed, with amphotericin B exhibiting larger adverse event effects.Conclusion: Treatment options appear to offer preferential effects on response rates and mortality.
When mycologic data are available, therapy should be tailored.

Invasive candidiasis has emerged as an important nosocomial infection, especially in critically ill patients.We review the epidemiology of invasive candidiasis with an emphasis on data from Taiwan. An increasing incidence of candidemia became apparent from 1980 to the end of the 1990s, followed by relative stability.Crude mortality rates of patients with candidemia were in the range of 35% to 60%. Candida albicans remains the predominant cause of invasive candidiasis in Taiwan and accounts for more than 50% of all cases. Candida tropicalis, Candida glabrata and Candida parapsilosis are the three most common nonalbicans Candida species that cause invasive candidiasis. The above four Candida species account for more than 90% of invasive candidiasis in Taiwan. Overall, invasive Candida isolates have remained highly susceptible to fluconazole (> 90% susceptibility) over the past two decades. However, periodic surveillance is needed to monitor antifungal resistance because reduced fluconazole susceptibility in non-albicans
Candida is not an uncommon trend. Voriconazole and echinocandins continue to exhibit excellent in vitro activity against invasive Candida isolates. [J Formos Med Assoc 2009;108(6):443–451]

Topical polyene or azole antifungal agents are effective in most cases. Drug choice is dictated by several factors, including the patient’s medical history, oral symptoms and predicted compliance with application method. Some common regimes are given below.Nystatin oral suspension (100 000 units ⁄mL – 1 mL topically), or nystatin pastilles (100 000 IU) four times daily for 7 to 14 days should resolve most local candidal infections. Note that some studies indicate nystatin to be ineffective for Candidal lesions in cancer patients.

Protein inhibitors: The sordarins
The sordarin are protein synthesis inhibitors with a mode of action that blocks the function of fungal but not human translation elongation factor 2 (39, 56). Different sordarin derivatives have different spectra of susceptible species for reasons that are not yet clear but may be related to the problems of penetration of these agents into target fungi (56, 81). Nevertheless, their high specificity for the fungal target and the relative way to obtain new sordarin variants hold promise for positive future developments with this series of antifungal drugs.
TRENDS in Microbiology Vol.11 No.6 June 2003