Introduzione alla Evidence-based Medicine Fabrizio Faggiano.

Evidence Based Practice
Gabriele ManziAzienda U.S.L. di Bologna
GIMBEGIMBE®®

The The EvolutionEvolution ofof HealthHealth CareCare
DOING THINGS
CHEAPER
DOING THINGS BETTER
DOING THINGS RIGHT
DOING THE
RIGHT THINGS
DOING THE
RIGHT THINGS RIGHT
Efficiency EffectivenessQuality
Improvement
1970s 1980s 1990s 21st Century
GIMBEGIMBE®®

Evidence Based MedicineEvidence Based Medicine
L’EBM costituisce un approccio alla pratica clinica dove le decisioni cliniche risultano dall'integrazione tra l'esperienza del medico e l'utilizzo conscenzioso, esplitico e giudizioso delle migliori evidenze scientifiche disponibili, mediate dalle preferenze del paziente.
David Sackett
GIMBEGIMBE®®

Evidence Based MedicineEvidence Based MedicineWhat it is and what it isn’t
Researchevidence
Patientpreferences
Clinical expertise
Sackett et al, BMJ 1996
GIMBEGIMBE®®

Evidence Based MedicineEvidence Based MedicineWhat it is and what it isn’t
Modificato da Haynes RB et al, BMJ 2002
Clinical state and circumstances
Research evidence
Patients’ preferences and actions
Clinical expertise
GIMBEGIMBE®®
Health Care Resurces

Clinical Governance
Evidence Based Health Care
Evidence Based Practice
EBM EBPHEBN
GIMBEGIMBE®®
E.B. Pharmacy E.B. Midwifery

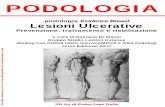
ANATOMIA DELLANATOMIA DELL’’INFORMAZIONE INFORMAZIONE BIOMEDICABIOMEDICA
RICERCA PRIMARIA
• Studi Osservazionali• Studi Sperimentali
RICERCA SECONDARIA
• Revisioni Sistematiche• Linee Guida• Analisi economiche• Analisi decisionali
FONTI TERZIARIE
• Revisioni tradizionali• Trattati• Editoriali• Parere degli esperti
Distorsione dei risultati
GIMBEGIMBE®®

I principi dellI principi dell’’evidence evidence based practicebased practice
GIMBEGIMBE®®

Componente essenziale: attitudine ad avvertire il bisogno di informazioneComponente tecnica: abilità pratiche per effettuare le ricerche e valutare criticamenteGiudizio clinico: pesare, valutare e integrare le evidenze nel processo decisionale.
Cartabellotta A. Rec Prog Med 2002
PREREQUISITI
GIMBEGIMBE®®

• Scegliere tra due interventi assistenziali (quale medicazione posizionare),
• Decidere la tipologia di paziente su cui intraprendere un intervento (su quali pazienti applico le strategie di prevenzione delle lesioni da decubito),
• La tempistica delle prestazioni (ogni quanto realizzare la medicazione di un CVC)
• Cosa e come comunicare con i pazienti e le loro famiglie (comunicare il rischio di caduta),
• Come organizzare l’assistenza (modalità di consegna)
• …
Come prendiamo le decisioni nella pratica professionale?
GIMBEGIMBE®®

• Insegnamento scolastico• Tradizioni/abitudini di reparto• Esperienza• Autoreferenzialità• Prescrizioni di …• Libri, riviste, …• …
Come prendiamo le decisioni nella pratica professionale?
GIMBEGIMBE®®

Difformità della praticaErogazione di prestazioni non ottimaliScarsa crescita professionaleEsposizione dei pazienti a rischi non necessariDeterminazione di costi non giustificati…
Le conseguenze di ciò
GIMBEGIMBE®®

Prostatecmia radicale
Clinica Urologica Divisione Urologia
Due giorni prima
Dieta senza scorie* 3 per 2 cp Humatin* 2 buste Selg (e/o Isocolan)
-
Giorno prima Dieta* Pranzo senza scorie Cena liquida; 3 per 2 cp HumatinClisma con Neomicina 1%Tricotomia ampia (dai capezzoli fino a metà coscia)Doccia con betadineDigiuno dalla mezzanotte
Purgante
Tricotomia xifopubica e scrotale
Digiuno dalla mezzanotteCalze antiembolo
Giorno dell’intervento
Digiuno totaleClisma ore 6.00 con neomicina 1%Doccia con BetadineAntibiotico profilassi
Doccia con betadine
Un esempio:da “Le basi scientifiche dell’assistenza infermieristica” di Paola di Giulio
GIMBEGIMBE®®

…una considerazione
“Meno del 20 % di ciò che i medici fanno ogni giorno possiede almeno uno studio clinico ben disegnato a sostegno della sua utilità.”
Cochrane A.L. ” Effectiveness and Efficiency. Random reflection on Health. Service” Nuffield Provincial hospital trust, London, 1972.
E quello che fanno gli infermieri?
GIMBEGIMBE®®

Le origini dellLe origini dell’’evidence evidence based practicebased practice
GIMBEGIMBE®®

Archibald L. Cochrane(1909-1988)
GIMBEGIMBE®®

Evidence-based Medicine: la storia 1972
Archibald L. Cochrane, un epidemiologo inglese, sosteneva che i risultati della ricerca avevano un impatto molto limitato sulla pratica clinica.“E’ causa di grande preoccupazione constatare come la professione medica non abbia saputo organizzare un sistema in grado di rendere disponibili, e costantemente aggiornate, delle revisioni critiche sugli effetti dell'assistenza sanitaria".In altre parole Cochrane, suggeriva di rendere disponibili a tutti i pazienti solo gli interventi sanitari di documentata efficacia.
GIMBEGIMBE®®

Evidence-based Medicine: la storia 1986
L'attenzione di Sackett e coll. si sposta progressivamente da “come leggere la letteratura biomedica” a “come utilizzare la letteratura biomedica per risolvere i problemi clinici”.
David Sackett
GIMBEGIMBE®®

EvidenceEvidence BasedBased NursingNursing
GIMBEGIMBE®®

Evidenza = Prova di efficacia ?
In Italiano– È evidenza qualsiasi cosa che sia palese e
chiara, per la quale non è necessaria qualsiasi ulteriore dimostrazione.
In Inglese– È evidenza qualsiasi cosa che ha provato la
propria validità mediante il metodo scientifico. È evidenza ciò che è stato dimostrato.
Evidence = Evidenza ?
GIMBEGIMBE®®

Evidence-Based Nursing (EBN)
Processo per mezzo del quale le infermiere e gli infermieri assumono le decisioni cliniche utilizzando le migliori ricerche disponibili, la loro esperienza clinica e le preferenze del paziente, in un contesto di risorse disponibili.
Di Censo A, Cullum N, Ciliska D.“Implementing evidence based nursing: some misconceptions”
Evidence Based Nursing 1998; 1:38-40
GIMBEGIMBE®®

Evidence-Based Nursing (EBN)
Opinion Based Nursing – O.B.N.
Evidence Based Nursing – E.B.N.
GIMBEGIMBE®®

• Individuare gli ambiti dove c’è variabilità• Dove c’è variabilità, c’è incertezza• Incertezza = area dove è necessario
fare chiarezza• Per fare chiarezza bisogna attivare la
ricerca• La ricerca è il motore che produce
conoscenza quale riferimento per guidare la pratica professionale
Paolo Chiari - Centro Studi EBNS.Orsola-Malpighi - Bologna
Perché la ricercaAttività
clinica
Attività
clinica
GIMBEGIMBE®®

Quando la ricerca e quando l’EBN
Quando abbiamo un dubbio ricorrere all’EBN, prima di pensare alla conduzione di uno studio, è senz’altro una precauzione che può farci risparmiare molto tempo ed energie a patto che non siamo nell’area grigia.
GIMBEGIMBE®®

Avere chiaro rispetto ad un problema assistenziale cosa voglio cercare, perché, e quali risultati devo andare a misurare (aree di incertezza)Porre le proprie domande alle banche dati, ricercando quelle che sono le conoscenze scientifiche disponibiliValutare criticamente i risultatiApplicazione delle conoscenze acquisite al problema originario
Il processo dell’EBN
GIMBEGIMBE®®

Selezionare un aspetto del proprio lavoro da mettere in discussione (bisogno di informazione)Trasformare il bisogno di informazione in quesiti clinici ben definitiRicercare con la massima efficienza, attraverso le fonti bibliografiche ed elettroniche le migliori evidenze disponibiliValutare criticamente le evidenze trovate, la loro validità ed applicabilitàDiffondere ed integrare le evidenze trovateMiglioramento continuo della pratica professionale
EBN – Strumento & Processo
GIMBEGIMBE®®

I limiti dellI limiti dell’’EvidenceEvidenceBasedBased PracticePractice
GIMBEGIMBE®®

I limiti della EBM
Esistenza di “zone grigie”:Zone in cui vi è incertezza sull’efficacia.EBM si basa sulle migliori evidenze “disponibili”, non sulle migliori evidenze “possibili”.
GIMBEGIMBE®®

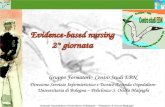
Le “aree grigie”: lo spazio dell’opinion based
Interventiinefficaci
Interventiefficaci Area grigia
PRATICA CLINICA
EBP
RICERCARICERCA
Copyright © 1996-2007 - GIMBE®
GIMBEGIMBE®®

Necessità di acquisire nuove competenzeMancanza di tempoScarsa attitudine a mettere in discussione le proprie conoscenze e a generare quesiti clinico-assistenziali.Barriere linguistiche Limitata diffusione/accesso agli strumenti informatici (computer, internet) Scarsa familiarità informaticaResistenza al cambiamentoScarsa disponibilità di riviste
I limiti dell’EBP nella realtà italiana
GIMBEGIMBE®®

Le caratteristiche della Le caratteristiche della letteratura letteratura biomedicabiomedica
GIMBEGIMBE®®

The The AscentAscent ofof EvidenceEvidence(and the (and the exhaustionexhaustion ofof man)man)
Clarke M.J. BMJ 1998Copyright © 1996-2007 - GIMBE®
GIMBEGIMBE®®

Le caratteristiche dell’informazione biomedica
Crescita esponenziale:circa 2.000.000 di articoli pubblicati ogni anno in oltre 20.000 rivistesino a 400.000 citazioni aggiunte annualmente au MEDLINE
GIMBEGIMBE®®

Le caratteristiche dell’informazione biomedica
Obsolescenza: Progresso scientifico e tecnologico.Ritardo nella disseminazione ed utilizzazione delle conoscenze.
Frammentazione:Articoli che trattano lo stesso argomento sono pubblicati in riviste ed annate diverse.
Basso rapporto segnale/rumore:La maggior parte della produzione scientifica èirrilevante per la pratica clinica.
GIMBEGIMBE®®

WARNING !!!
Trials are conducted and published without a systematic review of existing evidence, meaning that trials are conducted unnecessarily or don't address the most important questionsResults are selectively published with positive results emphasised or published more than once, and negative results are ignoredTrials favourable to sponsors are published in major journals, and unfavourable trials are not published at all or are published in minor journals
Smith R, Roberts I. Patient Safety Requires a New Way to Publish Clinical Trials. PLoS Clinical Trials (2006)1(1)
GIMBEGIMBE®®

WARNING !!!
Una ricerca effettuata su 3.600 ricercatori e 4.000 borsisti ha dimostrato che:0,3% ha inventato o falsificato dati6% non ha pubblicato dati che erano in contrasto con le
sue ricerche precedenti15,5% ha cambiato il disegno della ricerca per
accontentare lo sponsor4,7% ha pubblicato più volte gli stessi risultati15,3% non ha utilizzato tutti i risultati ottenuti
Nature 2005; 435: 718-9
GIMBEGIMBE®®

EBNFasi del processo:
Conversione del bisogno di informazione in quesiti clinici ben definiti.Ricerca con la massima efficienza delle migliori evidenze disponibili.Valutazione della loro validità ed applicabilitàclinica.Integrazione delle evidenze nella pratica clinica.Rivalutazione continua della propria performance professionale.
GIMBEGIMBE®®

Approcci di ricerca
Cercare attivamente nelle banche dati rispetto ad un quesito formulato (SEARCHING).Consultare periodicamente alcune riviste per individuare novità sui temi di abituale interesse (SCANNING).
GIMBEGIMBE®®

SCANNING
SEARCHING
sorveglianza cerco ciò che
mi serve
Gestione dell’informazione
GIMBEGIMBE®®

Seleziono alcune riviste e le leggo in modo regolare•che cosa trovo?
– abstract– full text
•problemi– time consuming– aspecificità
GIMBEGIMBE®®
SCANNING

• Risorse primarie– B.D. generali: Medline, Embase, …– B.D. specialistiche: Cinhal, Pedro,
Joanna Briggs, …• Risorse secondarie:informazioni predigerite
– B.D. revisione sistematiche: Cochranelibrary, Joanna Briggs, …
– B.D. linee guida: New Zeland guidelinegroup, Sign, National GuidelineClearinghouse, …
GIMBEGIMBE®®
SEARCHING

IL QUESITOovvero
Come definire un quesito clinico che ci permetta di ricercare la risposta nella letteratura
GIMBEGIMBE®®

Focalizzando la domanda si:
chiarisce l’obiettivo della ricerca
facilita l’utilizzo di regole appropriate nella scelta dei titoli e dei riassunti degli articoli che sono stati individuati
GIMBEGIMBE®®

FORMULARE DOMANDE PERTINENTI FORMULARE DOMANDE PERTINENTI ALLE QUALI SIA POSSIBILE ALLE QUALI SIA POSSIBILE
RISPONDERERISPONDERE
GIMBEGIMBE®®

I quesiti clinico-assistenzialiappartengono a due categorie principali
Background
Foreground
Conoscenza, esperienza
Modificato da: Guyatt GH, et al. AMA Press, 2001
GIMBEGIMBE®®

PerchPerchéé ci interessa questa distinzione? ci interessa questa distinzione? Per orientare diversamente la ricercaPer orientare diversamente la ricerca
Verso linee guida
Background Background questionsquestionsSono i quesiti di base che vengono formulati nelle situazioni in cui l'argomento è poco, o per nulla, conosciuto. E' un "bisogno di informazione" caratteristico del giovane professionista.Il professionista esperto, peraltro, formula quesiti di base quando la malattia/condizione/tecnologia è: – estranea al proprio settore professionale/specialistico– di recente introduzione (tecnologia) o descrizione (malattia)– rara
GIMBEGIMBE®®

PerchPerchéé ci interessa questa distinzione? ci interessa questa distinzione? Per orientare diversamente la ricercaPer orientare diversamente la ricerca
Verso la letteratura secondaria: Revisioni sistematiche
Verso la letteratura primaria: Medline, Cinahl, Embase
ForegroundForeground questionsquestions
Sono quesiti specifici, generalmente formulati dal professionista esperto.
GIMBEGIMBE®®

Quando nasce un quesito di foreground?
Categoria Quesito ed esempio
Eziologia/RischioQual'è la responsabilità eziologica del fattore di rischio X nell'insorgenza della malattia Y?
L'utilizzo del telefono cellulare aumenta il rischio di neoplasia cerebrale?
Diagnosi
Qual'è l’accuratezza del test diagnostico X (rispetto al gold-standard Y) nella diagnosi della malattia Z?
Qual'è l'accuratezza diagnostica della risonanza magnetica nucleare nei pazienti con sospetta lesione del menisco?
Prognosi
Qual'è la storia naturale della malattia X e la potenza dei fattori prognostici?
In un paziente con neurite ottica, quali sotto i fattori prognostici (favorevoli e sfavorevoli) che condizionano l'evoluzione in sclerosi multipla?
Trattamento
Qual'è l'efficacia del trattamento X (preventivo, terapeutico o riabilitativo), rispetto al trattamento Y, nella malattia Z?
In un paziente con osteoartrosi in trattamento cronico con FANS (malattia/condizione), l'omeprazolo (intervento), rispetto al misoprostolo (confronto) è in grado di prevenire l'ulcera da FANS sintomatica e le sue complicanze (evento)?
Copyright © 1996-2007 - GIMBE®
GIMBEGIMBE®®

formulare il quesito in modo preciso ed
articolato (es PICOM)
P patientI interventionC comparisonO outcomeM metodology
Quesito di foreground
GIMBEGIMBE®®

Esempio di ricerca
Punto di partenza: quesito in forma “narrativa”:
“Il saccarosio può essere impiegato come analgesico per i neonati che devono essere sottoposti a procedure dolorose
(es.: puntura del calcagno …)?”
GIMBEGIMBE®®

Patient: neonati da sottoporre a procedure dolorose.Intervention: analgesia con saccarosio.Comparison: altri trattamenti non farmacologici (“pacifiers”, ecc.).Outcome: ridotta percezione del dolore da parte del neonato.Metodology: Randomized Controlled Trial
Trasformazione con PICOM
GIMBEGIMBE®®

QUESITO DISEGNO DELLO STUDIO
EZIOLOGIA• COORTE• CASO CONTROLLO• REVISIONI SISTEMATICHE
PROGNOSI• STUDI LONGITUDINALI DI COORTE(SENZA COORTE CONCORRENTE)
DIAGNOSI
• STUDI TRASVERSALI DI CONFRONTOINDIPENDENTE E CIECO CON IL GOLD STANDARD DIAGNOSTICO
• REVISIONI SISTEMATICHE
TRATTAMENTO• RCT• REVISIONI SISTEMATICHE
PER OGNI DOMANDA UN DISEGNO
GIMBEGIMBE®®

Paziente o
problema
Chiedersi: “come descriverei un gruppo di pazienti
simili al mio?”
Bilanciare la precisione con la brevità
Quesito di foreground
GIMBEGIMBE®®

Intervento o
esposizione(una causa, un
fattore prognostico, un trattamento)
Chiedersi “Quale intervento principale/fattore di
rischio sto prendendo in considerazione?”
Essere specifici
Quesito di foreground
GIMBEGIMBE®®

Intervento di controllo
(se necessario e/o possibile)
Chiedersi “Qual’è la principale alternativa da comparare all’intervento prescelto?”
Essere specifici
Quesito di foreground
GIMBEGIMBE®®

Outcome
Chiedersi “Che cosa spero di ottenere?”
o“Che cosa questo intervento può
realmente produrre?”
Essere specifici
Quesito di foreground
GIMBEGIMBE®®

MetodologyChiedersi
“Quale disegno di studio costituisceil gold standard per il mio quesito?”
Quesito di foreground
GIMBEGIMBE®®

Perché è importante chiarire bene il quesito?
Per due motivi fondamentali:
– dal quesito vengono estratte le parole chiave che useremo nella ricerca.
– dalla chiara espressione del quesito possiamo definire i criteri di inclusione o di esclusione, tra i quali capire quale tipo di studio dobbiamo cercare.
GIMBEGIMBE®®

Esercitazione del quesito: diagnosi
Lavori come infermiere all’interno di un ambulatorio di assistenza di base. Usi abitualmente diversi strumenti validati per la diagnosi di depressione. Una collega ti parla di uno strumento analogo, ma composto da due sole domande, che secondo lei èefficace per la individuazione della depressione maggiore ed il cui uso, essendo così semplice, permetterebbe di risparmiare molto tempo. Decidi quindi di compiere una ricerca su diversi strumenti per la diagnosi di depressione e sulle loro proprietà.
GIMBEGIMBE®®

Esercitazione del quesito
Popolazione Intervento Comparazione Outcome
In pazienti con sospetta depressione
L’uso di uno strumento a due domande
Rispetto ad altri strumenti validati
Che livello di accuratezza permette?
GIMBEGIMBE®®

Stai assistendo una paziente di 28 anni che è appena stata sottoposta a dilatazione e curettage dopo aborto spontaneo. Era di 10 settimane ed era alla sua prima gravidanza. In un incontro di team, uno dei tuoi colleghi ricorda vagamente di aver letto un articolo inerente la depressione dopo l’aborto. Decidi di compiere una ricerca per verificare se nella tua paziente sono riscontrabili i fattori prognostici di severa e prolungata depressione.
Esercitazione del quesito: prognosi
GIMBEGIMBE®®

Popolazione Intervento Comparazio-ne
Outcome
In una paziente sana che ha recentemen-te subito un aborto
L’individua-zione di quali fattori prognostici
Consente di individuare uno stato depressivo non fisiologico
Esercitazione del quesito: prognosi
GIMBEGIMBE®®

Lavori come infermiere scolastico e visiti quotidianamente molti bambini delle scuole elementari e medie (di età compresa tra i 5 ed i 13 anni). Èinverno, per cui sono molto diffusi influenza e raffreddore. Una delle insegnanti ti ferma nell’atrio della scuola e ti chiede un consiglio per la sua bambina di 10 anni che è raffreddata. L’insegnante ha sentito dire che lo zinco in compresse può aiutare ad alleviare i sintomi del raffreddore: ti chiede se èrealmente efficace e se è opportuno darlo ai bambini.
Esercitazione del quesito: terapia
GIMBEGIMBE®®

Popolazione Intervento Comparazio-ne
Outcome
Nei bambini con raffreddore
L’assunzio-ne di compresse di zinco
?Sono efficaci e sicure per alleviare i sintomi del raffreddore?
Esercitazione del quesito: terapia
GIMBEGIMBE®®

Sei un infermiere territoriale. Una tua paziente èuna donna di 29 anni che ha assunto contraccettivi orali negli ultimi 6 anni. Ti telefona per chiederti un consiglio: è molto in ansia dopo avere letto che l’assunzione degli estroprogestinici aumenta il rischio di malattie cardiovascolari. Lei non ha mai fumato, è in buona salute e non ci sono casi di malattie cardiache nella sua famiglia. Chiede di vederti per discutere se è il caso di sospendere l’assunzione della pillola e passare all’uso di un altro metodo anticoncezionale. Nel prepararti all’incontro decidi di eseguire una ricerca.
Esercitazione del quesito: eziologia
GIMBEGIMBE®®

Popolazione Intervento Compara-zione
Outcome
Nelle donne in età fertile
L’assunzione di contraccettivi orali a base di estroprogestinici
Rispetto ad altri metodi contraccettivi non estroprogestinici
Aumenta il rischio di insorgenza di malattie cardiovasco-lari?
Esercitazione del quesito: eziologia
GIMBEGIMBE®®

GIMBEGIMBE®
THE END
GIMBEGIMBE®®

GIMBEGIMBE®®
Gabriele ManziAzienda U.S.L. di Bologna
Evidence Based Practice

Architettura della ricerca clinica
Studi Epidemiologici
GIMBEGIMBE®®

ANATOMIA DELLANATOMIA DELL’’INFORMAZIONE INFORMAZIONE BIOMEDICABIOMEDICA
RICERCA PRIMARIA
• Studi Osservazionali• Studi Sperimentali
RICERCA SECONDARIA
• Revisioni Sistematiche• Linee Guida• Analisi economiche• Analisi decisionali
FONTI TERZIARIE
• Revisioni tradizionali• Trattati• Editoriali• Parere degli esperti
Distorsione dei risultati
GIMBEGIMBE®®

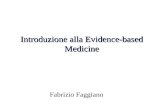
The 6S hierarchy ofThe 6S hierarchy ofprepre--appraised evidenceappraised evidence
DiCenso A, Bayley L, Haynes RB. Evid. Based Nurs. 2009;12;99-101
Original jourmal articles
Evidence based abstraction jourmal
Systematic reviews
Evidence based abstraction jourmal
Evidence based clinical practice guideline / textbooks
Computerized decision support systems

Non evidence
Evidence
Cohort StudiesCohort Studies
Case Control StudiesCase Control Studies
Case SeriesCase Series
Case ReportsCase Reports
Ideas, Editorials, OpinionsIdeas, Editorials, Opinions
Animal researchAnimal research
In vitro (In vitro (‘‘test tubetest tube’’) research) research
Mega TrialMega TrialRandomized Randomized Controlled Controlled
StudiesStudies
Systematic ReviewSystematic Review
GIMBEGIMBE®®
Ricerca sanitaria

• Studi osservazionali–descrittivi
• case report• case series
Architettura della ricerca clinica
GIMBEGIMBE®®

• Studi osservazionali–Analitici
• Studi caso controllo• Studi di coorte
–Con coorte parallela»Prospettici
–Senza coorte parallela»Prospettici retrospettivi
• Studi trasversali/cross sectional
Architettura della ricerca clinica
GIMBEGIMBE®®

QUESITO DISEGNO DELLO STUDIO
EZIOLOGIACOORTECASO CONTROLLOREVISIONI SISTEMATICHE
PROGNOSISTUDI LONGITUDINALI DI COORTE(SENZA COORTE CONCORRENTE)
DIAGNOSI
STUDI TRASVERSALI DI CONFRONTOINDIPENDENTE E CIECO CON IL GOLD STANDARD DIAGNOSTICOREVISIONI SISTEMATICHE
TRATTAMENTORCTREVISIONI SISTEMATICHE
Per ogni domanda un disegnoGIMBEGIMBE®®
Quali sono?

• Es: vogliamo verificare se avere un indice di massa corporea basso (BMI) (esposizione) è un fattore di rischio per le lesioni da decubito (esito).
GIMBEGIMBE®®
Studi che verificano l’eziologia

Come posso rispondere a questa domanda?
Attraverso tre disegni di studio:studi trasvesrale/cross sectionalstudi caso controllostudi di coorte
GIMBEGIMBE®®

Studio che raccoglie informazioni relative all’esposizione ai fattori di rischio ed ai loro esiti (positivi o negativi) NELLO STESSO MOMENTO e sullo stesso paziente.
GIMBEGIMBE®®
Studio Cross Sectional

Sono studi che rilevando i dati in un preciso momento realizzano la fotografia del fenomeno. Attraverso questi studi si rileva la PREVALENZA di una patologia, ossia l’insieme di tutti i casi esistenti in un determinato momento, in una determinata popolazione.
GIMBEGIMBE®®
Studio Cross Sectional

Sono studi retrospettivi che partendo dalla presenza, o meno, dell’esito (endpoint) raccolgono informazioni relative all’esposizione ai fattori di rischio.
Fattori di rischio
End point sì
End point no
Oggi
GIMBEGIMBE®®
Studio Caso-Controllo

Sono studi prospettici che partendo dall’esposizione ai fattori di rischio o meno, verificano se insorge l’esito.
End point
Fattori di rischio sìFattori di rischio no
Oggi
GIMBEGIMBE®®
Studio di Coorte

Soggettidello studio
CASI
CONTROLLI
esposti
non esposti
esposti
non esposti
ESPOSTI
NON ESPOSTI
outcome +
outcome -
outcome +
outcome -
CASO-CONTROLLO COORTE PROSPETTICA
direzione dell’osservazione
Studi osservazionali analitici

Cosa ci serve sapere per leggere gli studi osservazionali?
Dove può essere l’errore/imbroglio?
GIMBEGIMBE®®

In uno studio il termine bias si riferisce a qualsiasi errore sistematico che porti ad una stima errata dell’associazione tra l’esposizione e l’esito.In uno studio osservazionale i puùfrequenti bias che possiamo incontrare sono:– Information bias– Recall bias (studi caso controllo)– Selection bias– Fattori di confondimento
GIMBEGIMBE®®
Individuare i bias

Information bias/misclassification – si realizza tutte le volte in cui il paziente è posto nel gruppo sbagliato a causa della errata rilevazione del parametro considerato (es. misurazione errata di peso ed altezza e collocazione erronea nel gruppo sbagliato).
GIMBEGIMBE®®
Information bias

Esso si riduce in due modi:– Utilizzando misure di rilevazione oggettive.– Facendo in modo che chi effettua la
rilevazione dell’esposizione non sia a conoscenza dell’esito (studio caso controllo) e che chi rileva l’esito non sia a conoscenza della condizione di esposizione all’agente indagato (studio di coorte).
GIMBEGIMBE®®
Information bias

E’ proprio degli studi caso controllo e si verifica a causa dell’errato ricordo dei soggetti coinvolti nello studio.
GIMBEGIMBE®®
Recall bias

Coloro che non hanno sviluppato ldp hanno un ricordo meno accurato e
più positivo rispetto la durata della propria
degenza (in realtà 13 anziché 10 hanno avuto
degenze >10 gg).
Esempio : confronto tra quanto riferito dai pazienti e quanto rilevato dalla documentazione clinica.
GIMBEGIMBE®®

Esempio: confronto tra quanto riferito dai pazienti e quanto rilevato dalla documentazione clinica.
Questo tipo di biasmodifica in modo consistente i risultati della associazione, spostandola dall’ipotesi nulla!
GIMBEGIMBE®®

I soggetti selezionati devono essere identici ad eccezione dell’esposizione all’agente eziologico. Quando questo non si realizza siamo in presenza del SELECTION BIAS. In uno studio caso controllo, in cui si parte da due gruppi con e senza l’esito, cosa accadrebbe se si fossero scelte solo persone non esposte al reale agente eziologico?In uno studio di coorte, l’allocazione alla condizione di esposizione si riferisce allo sviluppo dell’esito (o nei due gruppi ci sono altre differenze non considerate)?
GIMBEGIMBE®®
Selection bias

Negli studi di coorte i soggetti inclusi nei gruppi devono essere seguiti per un periodo di tempo sufficientemente lungo.Cosa accadrebbe se il follow up fosse troppo breve, o in esso fossero persi molti soggetti?Una perdita nel follow up superiore al 20% compromette i risultati dello studio.
GIMBEGIMBE®®
Follow up

Se nel compimento di uno studio è stato effettuato un bias i suoi risultati possono essere definitivamente compromessi.Gli studi di coorte da questo punto di vista sono più sicuri per qul che riguarda l’information bias o il recall bias, ma non sempre sono realizzabili (condizioni rare o a lentissimo decorso).
GIMBEGIMBE®®

Errors in epidemiological studies
Study size
Error
Systematic error (bias)
Random error (chance)
Rothman, 2002
GIMBEGIMBE®®

Esiste una relazione tra l’assunzione di caffè e l’insorgenza del tumore del polmone?
GIMBEGIMBE®®
Fattori di confondimento

I fattori di confondimento sono le variabili associate sia all’esposizione, sia all’esito, che potrebbero spiegare qualsiasi relazione osservata tra questi due fattori.
Esposizione Esito
Fattore di confondimento
GIMBEGIMBE®®
Fattori di confondimento

Al contrario dei bias, i fattori di confondimento possono essere corretti cercando di escludere dal campione coloro che possono recarli con sé.Purtroppo però i fattori di confondimentosono numerosi, per cui è difficile escluderli completamente dagli studi (e non è detto che possano essere identificati).
GIMBEGIMBE®®
Fattori di confondimento

Per ridurre l’effetto delle variabili di confondimento esistono diverse tecniche in fase di campionamento o in fase di analisi.
GIMBEGIMBE®®
Fattori di confondimento

Accorgimenti in fase di campionamento
Esclusione dei soggetti che presentano variabili di confondimento.Matching negli studi caso controllo, che consiste nell’introdurre nel gruppo di controllo persone con le stesse variabili di confondimento presenti nel gruppo dei casi.Stratificazione, che consiste nell’esaminare l’associazione in modo separato nei diversi gruppi.
GIMBEGIMBE®®

Accorgimenti in fase di analisi
Regressione.Si tratta di un’elaborazione statistica che
ricalcola le associazioni tenendo conto dell’effetto delle variabili di confondimento.
GIMBE® Centro Studi EBN - BolognaGIMBEGIMBE®®

Esempio Esiste una relazione tra il sesso maschile e l’insorgenza delle lesioni da decubito?Lo studio di Margolis e al, rispetto al genere maschile e le lesioni da decubito, presenta un rischio relativo non adattato pari a 0,78, (CI 95% 0,70-0,88), quindi per gli uomini esisterebbe il 22% in meno di rischio di sviluppare lesioni da decubito.
GIMBEGIMBE®®

Esempio Tuttavia, considerando i fattori potenziali di confondimento, quali l’età e le patologie concomitanti, il rischio relativo diventa 1,01 (CI 95% 0,89-1,15).
Quindi, cosa si può concludere?
GIMBEGIMBE®®

• Negli studi sulle cause, vogliamo conoscere la relazione tra alcuni fattori di rischio dei pazienti (le esposizioni) e una particolare condizione o patologia (l’esito).
• La relazione tra i fattori di rischio e gli esiti viene generalmente presentata come rischio relativo, negli studi di coorte, o come odds ratio negli studi caso controllo.
GIMBEGIMBE®®
Misure di associazione

Tabellare i dati
a b
c d
Evento Sì Evento No
Gruppo E a + b
Gruppo C c + d
a + c b + d
Rischio Relativo (RR)a
EER ----------a + b
RR = ------------ = -------------c
CER ----------c + d
L’odds ratio (OR)
a/b OR = ------------
c/d
GIMBEGIMBE®®

Esempio ipotetico
Rischio Relativo (RR)a
EER ----------- 0,073a + b
RR = ------------ = --------------- = ----------- = 1,37c
CER ---------- 0,053c + d
Un risk ratio di 1,37 indica che le persone con un BMI basso hanno un rischio di 1,37 volte maggiore (o del 37%) di presentare l’esito, rispetto a quelli con elevato BMI.
GIMBEGIMBE®®

Esempio ipotetico
Odds Ratio (OR)
a/b 0,078OR = ------------ = ----------------- = 1,39
c/d 0,056
Un odds ratio di 1,39 indica che le persone con un BMI basso hanno una probabilitàdi 1,39 volte maggiore (o del 39%) di presentare l’esito, rispetto a quelli con elevato BMI.
GIMBEGIMBE®®

• Il RR si utilizza negli studi di coorte.• L’OR si utilizza negli studi caso controllo.• Non è tanto importante capire quando
bisogna usare l’uno o l’altro, ma sapere che cosa indicano.
GIMBEGIMBE®®
Misure di associazione

• RR/OR<1 - l’esposizione protegge rispetto l’insorgenza del danno
• RR/OR>1 – l’esposizione favorisce l’insorgenza del danno
• RR/OR=1 – l’esposizione non produce effetti
GIMBEGIMBE®®
Interpretazione

GIMBEGIMBE®®
Intervallo di confidenza (IC)

Si verifica quando i parametri di associazione (RR o OR) assumono valore uguale a 1 o quando l’intervallo di confidenza comprende il valore 1.
GIMBEGIMBE®®
Ipotesi nulla

Per valutare la validità di uno studio sull’eziologia (danno) di una particolare condizione, abbiamo bisogno di valutare quanto abbiano influito, sui risultati dello studio, 3 fattori:
il casoi biasi fattori di
confondimentoGIMBEGIMBE®®
I risultati sono validi?

Oltre a verificare i valori delle misure di associazione, e del loro IC, occorre osservare il valore assunto da “p”, che ci dice quale sia la significativitàstatistica dei risultati ottenuti.
GIMBEGIMBE®®
Test di significatività statistica… lo zampino del caso

GIMBEGIMBE®®
Significatività statistica

Per ogni quesito un disegno di studio ideale
QUESITO DISEGNO DELLO STUDIO
EZIOLOGIACOORTECASO CONTROLLOREVISIONI SISTEMATICHE
PROGNOSISTUDI LONGITUDINALI DI COORTE(SENZA COORTE CONCORRENTE)
DIAGNOSI
STUDI TRASVERSALI DI CONFRONTOINDIPENDENTE E CIECO CON IL GOLD STANDARD DIAGNOSTICO
REVISIONI SISTEMATICHE
TERAPIARCTREVISIONI SISTEMATICHE
GIMBEGIMBE®®

Non evidence
Evidence
CohortCohort StudiesStudies
Case Case ControlControl StudiesStudies
Case SeriesCase Series
Case ReportsCase Reports
Ideas, Editorials, OpinionsIdeas, Editorials, Opinions
Animal researchAnimal research
In vitro (In vitro (‘‘test tubetest tube’’) research) research
Mega TrialMega TrialRandomized Randomized Controlled Controlled
StudiesStudies
Systematic ReviewSystematic Review
GIMBEGIMBE®®
Ricerca sanitaria

• Studi sperimentali–Non controllati–Controllati
• Non randomizzati• Randomizzati
Architettura della ricerca clinica
GIMBEGIMBE®®

Il campione viene definito individuando criteri di inclusione e di esclusione. Essi sono utilizzati per selezionare il campione dall’insieme di tutte le unità.
Popolazione e campione
GIMBEGIMBE®®

Il campione deve essere corrispondente alle caratteristiche definite dal ricercatore e deve essere rappresentativo in termini quali-quantitativi della popolazione.Solo in questo modo sarà possibile trarre inferenze (generalizzazioni) sulle popolazione dallo studio effettuato su una piccola parte di essa.
GIMBEGIMBE®®
Campione

Un campione statisticamente rappresentativo deve essere sufficientemente numeroso, omogeneo e scelto a caso.
GIMBEGIMBE®®
Campione

Per ottenere delle informazioni attendibili su una popolazione utilizzando un campione, ènecessario che il campione sia ottenuto in modo casuale. Perché un campione possa essere considerato casuale, è indispensabile che ogni membro della popolazione in oggetto abbia la stessa probabilità di essere selezionato. Un campione non casuale non dà alcun affidamento: in altre parole tutte le inferenze da esso tratte non sono da prendersi sul serio.
GIMBEGIMBE®®
Campionamento casuale

Al fine di realizzare un campionamento casuale occorre ricorrere alla randomizzazione.Essa può essere realizzata in diversi modi:– Randomizzazione semplice– Randomizzazione stratificata– Randomizzazione a grappolo– Randomizzazione sistematica
GIMBEGIMBE®®
Campionamento casuale

• Studi sperimentali–Non controllati–Controllati
• Non randomizzati• Randomizzati
Architettura della ricerca clinica
GIMBEGIMBE®®

Direzione della raccolta dati
OutcomeEsposizione
Campione di
popolazioneRandomizzazione
Gruppo sperimentale
Gruppocontrollo
Esposizione
Outcome
No outcome
Outcome
No outcome
GIMBEGIMBE®®
Trial Randomizzati Controllati

Anatomiadell’RCT
Gruppo SperimentaleGruppo Sperimentale
Gruppo di ControlloGruppo di Controllo
OutcomeOutcome
No No OutcomeOutcome
OutcomeOutcome
No No OutcomeOutcome
GIMBEGIMBE®®

Singolo cieco: solo il soggetto sotto sperimentazione non sa quale trattamento sta ricevendo
Doppio cieco: sia il soggetto sotto sperimentazione che gli sperimentatori non sanno quale trattamento si assume/somministra
Doppio simulato: metodica utilizzata per mantenere la cecità quando si confrontano farmaci somministrati per vie diverse tra di loro
In aperto: sperimentazione senza cecità. Accettabile quando si confrontano terapie diverse e/o complesse
GIMBEGIMBE®®
La cecità per vedere bene

Non conoscere il trattamento che si riceve (paziente) o che si somministra (sperimentatore) impedisce di essere influenzati dalle aspettative che si hanno rispetto al trattamento
Altrettanto importante è essere ciechi nella valutazione dei risultati della sperimentazione, soprattutto se gli end-points sono sfumati o di difficle interpretazione (triplo cieco)
GIMBEGIMBE®®
La cecità per vedere bene

I RCTs rappresentano lo standard sperimentale per valutare l'efficacia dei trattamenti, grazie alla loro capacità di minimizzare i bias rispetto ad altri disegni sperimentali
L'elemento che contraddistingue i RCTs è l'assegnazione casuale dei pazienti al trattamento da sperimentare o al trattamento di controllo, attraverso le procedure di randomizzazione.
Questa assicura che tutti i fattori prognostici - sia noti che non conosciuti - vengono equamente distribuiti nei due gruppi di pazienti, tra i quali l’unica differenza risulta essere l’intervento terapeutico in studio.
Trial Randomizzati Controllati
GIMBEGIMBE®®

Se lo studio è condotto ed analizzato in maniera adeguata, l’eventuale differenza di esiti tra i due gruppi può essere attribuita all’effetto del trattamento in studio.
Esistono alcune condizioni per cui i RCTs non costituiscono il miglior disegno sperimentale:
- storia naturale delle malattie studi di coorte - eziologia, fattori di rischio studi di coorte, studi caso-controllo- accuratezza diagnostica studi trasversali
Trial Randomizzati Controllati
GIMBEGIMBE®®

Fasi degli studi sui farmaci
Da dove nascono gli RCTs
GIMBEGIMBE®®

• Nella fase I viene definita la massima dose tollerata e gli effetti tossici di un nuovo farmaco già sperimentato in laboratorio su animali (si svolgono pochi pazienti, <30).
• Lo scopo della fase II è stabilire l’efficacia del farmaco in un gruppo maggiore e mirato di pazienti (massimo 100).
GIMBEGIMBE®®
Fasi degli studi farmacologici

• La fase III rappresenta i tipici effettivi trials, in quanto si cerca di comparare il nuovo farmaco con un farmaco esistente o un intervento ritenuto efficace.
• La fase IV riguarda gli studi che cercano di monitorare gli effetti indesiderati di un nuovo farmaco dopo che è stato approvato per il marketing.
GIMBEGIMBE®®
Fasi degli studi farmacologici

Necessità di ricorrere agli RCTs
Ma è proprio indispensabile confrontare i risultati di due
gruppi?
GIMBEGIMBE®®

Il trattamento sperimentale viene assegnato a tutti i pazienti eleggibili consecutivamente osservati. Sono ad esempio le serie di casi o gli studi di fase I e II.
GIMBEGIMBE®®
Trial non controllati

In assenza del gruppo di controllo, i benefici del trattamento sperimentale vengono misurati confrontando i risultati ottenuti al decorso della malattia non trattata (o trattata con terapia standard).I benefici del trattamento sperimentale vengono misurati riportando i benefici assoluti del trattamento (ad es. il 98% dei pazienti con polmonite trattati con l’antibiotico X è guarito)
GIMBEGIMBE®®
Trial non controllati

OutcomeEsposizione:Intervento sperimentale
Pazienti eleggibiliFollow up
GIMBEGIMBE®®
Trial non controllati

• Principali fonti bias sono:- variabilità prognostica e di decorso della malattia.- effetto placebo.- aspettative ottimistiche del medico e del paziente.
GIMBEGIMBE®®
Trial non controllati

L’effetto totale del trattamento è la somma del miglioramento spontaneo, delle risposte
aspecifiche e della risposta specifica
Miglioramento spontaneo
Effetto Hawthorne
Aspettative ottimistiche
Effetto placebo
Effetto reale del trattamento
Copyright © 1996-2007 - GIMBE®
GIMBEGIMBE®®

Effetto reale del trattamento
Dipende dai benefici o dai danni indotti dal trattamento in uso, può essere influenzato anche dalla storia naturale della malattia che porterà il paziente a migliorare o peggiorare comunque
Effetto reale del trattamento
GIMBEGIMBE®®

Induce il paziente a stare meglio per la consapevolezza di essere trattato
L’effetto placebo può essere maggiore se il paziente ha fiducia nel medico o nella struttura sanitaria a cui si rivolge o se ha grande speranza che il nuovo trattamento sia efficace
GIMBEGIMBE®®
Effetto placebo

Le aspettative ottimistiche del medico derivano dalla sua fiducia nel trattamento che sta sperimentando e che lo inducono a interpretare ottimisticamente i risultati terapeutici accentuando l’effetto placebo
GIMBEGIMBE®®
Apettative ottimistiche

Induce il paziente a stare meglio per la consapevolezza di essere parte di uno studio
GIMBEGIMBE®®
Effetto Hawthorne

In una certa epoca storica hanno prodotto evidenze inconfutabili per trattamento drammatica efficacia in condizioni ad esito invariabilmente fatale/sfavorele:
– insulina nel coma diabetico.– penicillina nella polmonite pneumococcica (o
nella endocardite batterica).– vitamina B12 nell’anemia perniciosa.– appendicectomia nell’appendicite acuta.
GIMBEGIMBE®®
Trial non controllati

Oggi si utilizzano per:– efficacia del nuovo trattamento
drammaticamente evidente in osservazioni iniziali.
– patologie a decorso sfavorevole (arresto cardiaco, epatite fulminante, …).
– patologie rare.– studi di fase I e II.– assenza di trattamenti alternativi di confronto.– presupposti fisiopatologici convincenti.
Byar DP. NEJM 1990; 323: 1343GIMBEGIMBE®®
Trial non controllati

• Smith GC, Jill JP.Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ, Dec 2003; 327: 1459 - 1461.
GIMBEGIMBE®®
Trial non controllati

As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials.Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute.
Parachutes reduce the risk of injury after gravitational challenge, but their effectiveness has not been proved with randomized contolled trials.
GIMBEGIMBE®®

• Sempre più frequenti• Dimensione del campione > 1.000 - > 10.000• Multicentrici >100 - > 1.000• Criteri di inclusione larghi• Disegno semplice, registrati solo dati essenziali• End points non equivocabili (es: mortalità)• Grande potenza statistica: possono evidenziare differenze di efficacia minime fra i trattamenti a confronto.
Topol EJ & Califf RM. Br Heart J 1992; 68: 348
GIMBEGIMBE®®
Mega-Trial

Magnesio nell’infarto miocardicoRazionale: variazione nell’andamento di patologie cardiache in funzione della quantità di magnesio nell’acqua
Studi su animali hanno mostrato l’attività antiaritmica, antiaggregante e coronarodilatatrice del magnesio
Piccoli trials positivi sull’uso del magnesio nell’infarto
Una review informale dei risultati ha mostrato una riduzione della mortalità da IMA (infarto acuto del miocardio)
Una meta-analisi formale su 1300 pazienti con un totale di 78 decessi ha mostrato una riduzione del 55% nel rischio di morte (p=0.001)
Studio LIMIT-1 su 100 paz. - diminuzione delle aritmie (1986)
Studio LIMIT-2 su 2300 paz. - diminuzione dell’incidenza di insuff. ventricolare sinistra (1994)
GIMBEGIMBE®®
Dai trial clinici ai mega-trial

58.050 pazienti entro 24 ore dall’infarto in 1086 ospedali
- captopril per 1 mese vs placebo
- nitoderivati per un mese vs placebo
- magnesio solfato IV 24 h vs controllo
Risultati
Il captopril previene 5 morti su 1000, i nitroderivati e il magnesio sono inefficaci
GIMBEGIMBE®®
Il mega-trial ISIS-4 (1995)

Lancet, 1995 Mar 18;345(8951):669-85.
GIMBEGIMBE®®

Sono caratterizzati dalla presenza di un gruppo di pazienti di controllo, i cui esiti vengono confrontati con quelli del gruppo dei pazienti trattati
L'assegnazione dei pazienti all'uno o all'altro gruppo avviene con una delle seguenti procedure:
‐ controlli paralleli (contemporanei) ‐ controlli storici‐ controlli da banche dati
Trial controllati non randomizzati
GIMBEGIMBE®®

Copyright © - GIMBE®
I limiti comuni a tutti i CCTs sono:• lo sbilanciamento dei fattori prognostici tra i due gruppi di pazienti• la tendenza ad assegnare al trattamento sperimentale i pazienti a prognosi più favorevole• la sovrastima dell'efficacia del trattamento sperimentale, accentuata nelle CCTs con controlli storici dal miglioramento delle condizioni assistenziali
Per tali ragioni le CCTs, non dovrebbero più occupare alcun ruolo nella moderna ricerca clinica (vedi Consort Statement II)Costituiscono a tutti gli effetti una frode scientifica

Cosa dobbiamo sapere quando leggiamo gli
RCT
Dove può essere l’imbroglio?
GIMBEGIMBE®®

• Benchè costituiscano gli studi più rigorosi, in essi la presenza di errori sistematici (bias), compromette la credibilità e l’autorevolezza dei risultati.
• I più comuni bias possono essere:– bias di selezione– bias di accertamento– bias di violazione del protocollo– bias di pubblicazione– bias temporali
GIMBEGIMBE®®
Bias negli RCTs

• Accade quando gli outcome di uno studio sono influenzati dalle differenze sistematiche (reali e non casuali) dei due gruppi di studio, che dipendono dalle modalità con cui le persone sono state selezionate a partecipare al trial o con cui sono state assegnate ai due gruppi.
• La prevenzione di questo tipo di bias si realizza con una corretta randomizzazione.
GIMBEGIMBE®®
Selection bias

• Se uno studio è realmente randomizzato, l’allocazione ai gruppi non può essere influenzata dai ricercatori o dai partecipanti allo studio.
• Con la randomizzazione a tutti i partecipanti dello studio sono date le stesse opportunità di essere assegnati ad ognuno dei gruppi di studio.
GIMBEGIMBE®®
Selection bias

• Questo tipo di bias accade quando i risultati o le conclusioni di un trial sono distorte dalla conoscenza relativa all’intervento a cui ogni partecipante è stato sottoposto. Questo tipo di errore può essere determinato da chi eroga l’intervento, dai soggetti studiati, dai ricercatori che valutano o analizzano gli outcome e coloro che scrivono l’articolo descrivente il trial.
• Il miglior modo per evitare questo bias è mantenere le persone, coinvolte nello studio, non a conoscenza dell’identità dell’intervento il più a lungo possibile, realizzando quella che è detta CECITA’.
GIMBEGIMBE®®
Ascertainment bias

GIMBEGIMBE®®
Bias di violazione di protocollo
Lost to follow‐up (persi al follow up)
Withdrawal (sospendono il trattamento)
Crossover (passano all’altro gruppo)

GIMBEGIMBE®®
Bias di violazione di protocollo
Tutti i pazienti randomizzati devono essere inclusi nell’analisi alla fine dello studio (sia i persi al follow‐up, sia quelli che hanno sospeso il trattamento)
Ciascun paziente deve essere analizzato nel gruppo originale di randomizzazione, anche se poi ha ricevuto il trattamento dell’altro braccio (cross‐over)

• Ciò si giustifica con il fatto che, se il trattamento procura effetti indesiderati tali da non consentire al soggetto di seguire correttamente la terapia, considerare il suo esito negativo nel gruppo di controllo, ne accrescerebbe l’efficacia.
• Questo tipo di elaborazione dei dati si chiama analisi secondo “intention to treat”.
GIMBEGIMBE®®
Bias di violazione di protocollo

• Ogni paziente reclutato dovrebbe essere considerato fino alla fine, ma purtroppo non è sempre così, a causa, ad esempio del ritiro del pz dallo studio.
• L’abbandono degli studi non avviene per caso. Addirittura esso potrebbe essere determinato dal trattamento stesso.
• Per questo quando il numero dei persi al follow up non è uguale nei due gruppi, èlegittimo nutrire qualche sospetto.
GIMBEGIMBE®®
Follow up

• Dato che studiare solo coloro che sono rimasti nello studio può portare a sovrastimare l’efficacia del trattamento, gli autori dello studio devono riportare nelle conclusioni tutti coloro che erano stati reclutati, assegnando ai soggetti persi del gruppo di trattamento l’esito peggiore ed ai soggetti persi del gruppo di controllo l’esito migliore.
• In questo caso il rischio è di sottostimare l’efficacia del trattamento, il che è sicuramente più accettabile del contrario.
GIMBEGIMBE®®
Follow up

Il limite tollerabile di persi durante il follow up èdel 20%: difficilmente uno studio che ha dimostrato l’efficacia del trattamento, rimane tale attribuendo un esito negativo a più del 20% dei pazienti.
GIMBEGIMBE®®
Follow up

• Alcune evidenze dimostrano la probabilitàdi trovare pubblicato uno studio, non ècasuale ma dipende dalla direzione e dalla forza dei risultati della ricerca, per cui i lavori con risultati statisticamente significativi (positivi) sono pubblicati con maggiore facilità rispetto a quelli con risultati non significativi.
• Questa tendenza, che appare favorire i trials con risultati positivi, è stata chiamata pubblication bias.
GIMBEGIMBE®®
Publication bias

Uno studio randomizzato sulla lorcainide(antiaritmico di classe I), dove si osservava un aumento di morti fra i pazienti trattati, non venne pubblicato per 13 anni.
Negli anni 80 questi farmaci causarono fra 20.000 e 70.000 morti premature negli USA
Tonks, BMJ dicembre 1999
GIMBEGIMBE®®
Publication bias

Lo studio VIGOR che ha promosso il VIOXX èstato pubblicato nel novembre 2000 sul New England Journal of Medicine
Bombardier C. et al. “Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis.” VIGOR Study Group. N Engl J Med. 2000 Nov 23;343(21):1520-8
Nel dicembre 2005 il NEJM informa i lettori che gli autori dello studio VIGOR avevano manipolato i dati dei risultati della ricerca omettendo casi di gravi effetti avversi
Gregory D. et al. “Expression of Concern: Bombardier et al., ‘Comparison of Upper Gastrointestinal Toxicity of Refecoxib and Naproxen in Patients with Rheumatoid Arthritis’ N Engl J Med 2000 Nov 23;343(21):1520-8”
N Engl J Med. 2005 Dec 29;353(26):2813-4.
GIMBEGIMBE®®
Publication bias

GIMBEGIMBE®®
Publication bias

Dal 1999 al 2004 il VIOXX ha indotto negli USA circa 38.000 decessi supplementari (Lancet 2005)
Stima per i paesi industrializzati: 140-160.000 decessi supplementari
GIMBEGIMBE®®
Publication bias

Nel maggio del 2006 il Wall Street Journal informa che l’editore del NEJM era già a conoscenza nell’agosto 2001 della manipolazione.
La ditta produttrice del VIOXX (Merck) aveva acquistato nel novembre 2000 per la campagna pubblicitaria 900.000 ristampe dell’articolo del NEJM per circa 700-830.000 $
Il profitto per il NEJM si aggirava intorno ai 500.000$
Smith R. “Lapses at the new England journal of medicine.” J R Soc Med. 2006 Aug;99(8):380-2
GIMBEGIMBE®®
Publication bias

• Questo tipo di errore accade in quanto la velocità di pubblicazione dipende dalla direzione e dalla forza dei risultati del trial. In generale sembra che uno studio con risultati negativi impieghi il doppio del tempo per essere pubblicato rispetto ad uno con risultati positivi.
• Inoltre possono passare anni dal momento in cui lo studio è stato completato a quello in cui èpubblicato, tanto che il tempo per realizzalo sembra uguale a quello necessario per pubblicarlo e ciò riguarda allo stesso modo gli studi grandi e gli studi piccoli.
GIMBEGIMBE®®
Bias temporali – Time lag bias

Possiamo quindi fidarci della generalizzabilità degli RCTs?
In letteratura sono segnalati alcuni aspetti che devono portarci a considerare gli RCTs sempre con spirito critico. In particolare sono segnalati:
– Popolazioni estremanente selezionate (Gurwitz JH. Jama 1992).
– Competenza, motivazioni e condizioni organizzativo-assistenziali ideali (Grilli R. Et al, Il Pensiero Scientifico Editore,1995).
GIMBEGIMBE®®

– Risultati “medi” che non prevedono la risposta nel paziente individuale (Rothweel PM. Lancet 1995).
– End point misurati (surrogati vs clinicamente significativi) (Fleming TR,et al. Ann.Inter.Med. 1996).
– Misure utilizzate per riportare i risultati (relative vs assolute) (Bobbio M, et al. Lancet 1994).
GIMBEGIMBE®®
Possiamo quindi fidarci della generalizzabilità degli RCTs?

Clinicamente rilevanti - comprendono, oltre la mortalità, tutti gli eventi clinici morbosi che possono essere rilevati nella storia naturale/post-terapeutica di una malattia
Surrogati – sono variabili anatomico-fisiologico-metaboliche misurate con test di laboratorio/strumentali
Hard - di sicura determinazione, per la verifica dei quali l’errore èminimo (mortalità)
Soft - possono essere influenzati da imprecisioni o soggettività(es. miglioramento di un quadro sintomatologico, lettura di un ECG/Rx)
GIMBEGIMBE®®
End point

Trattamento End point surrogatoEnd pointrilevante
Encainide, Flecainide, Moricizina: extrasistolia ventricolare post-IMA (1)
extrasistolia mortalità
Milrinone: insufficienza eardiaca (2)
portata circolatoria mortalità
NaF: osteoporosi (2)densità minerale
osseaincidenza fratture
(1) Epstein AE & al. JAMA 1993; 270:2451(2) Da: Fleming TR & al Ann Intern Med 1996;125:605
GIMBEGIMBE®®
End point

Misure di efficacia negli RCTs
GIMBEGIMBE®®

Nella lettura degli studi troveremo indicate diverse misure di efficacia.La comprensione del loro significato, l’interpretazione del loro valore e della loro precisione ci servono per capire la forza e la direzione della associazione che vi è tra trattamento e outcome (e quindi di capire se l’intervento è efficace e in che misura).
GIMBEGIMBE®®
Misure di efficacia

Esempio
Cullen l, et al. Nebulized lidocaine decrease the discomfort of nasogastric tube insertion: a randomized, doubleblind trial. Ann Emerg Med 2004; 44: 131-7.La somministrazione di lidocaina nebulizzata prima dell’inserimento del sondino naso gastrico riduce il disagio del paziente?P: Adulti da sottoporre a posizionamento del SNG in pronto soccorso.I: nebulizzazione di lidocaina nella narice da utilizzare.C: nebulizzazione di soluzione fisiologica.O: disagio misurato attraverso una scala visuale analogica (misura continua), difficoltà di inserimento del sondino (misura continua), complicanze (sanguinamento, vomito, impossibilità di passaggio, dispnea – misure discrete).
GIMBEGIMBE®®

Esempio
Outcome Lidocaina Placebo Differenza (IC 95%)
Disagio riferito (media dei punteggi della scala visuale analogica)
37.7 59.3 26.6 (5.3 a 38.0)
Difficoltàpercepita dall’infermiere nell’inserimento del SNG
2 2 0 (-1 a 1)
Sanguinamento nasale 17% 0 17% (3,5-31)
Vomito 10% 0 10%(-0,7-21)
GIMBEGIMBE®®

Il primo passaggio per capire le diverse misure di efficacia consiste nel tabellare i dati.
a b
c d
Evento Sì Evento No
Gruppo S a + b
Gruppo C c + d
a + c b + d
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

Experimental Event Rate - Frequenza (o rischio) nel gruppo sperimentale
aEER =
a + b
Control Event Rate -Frequenza (o rischio) nel gruppo di controllo
cCER =
c + d
La EER ci dice con che frequenza l’evento
indesiderato si è verificato
nel gruppo sperimentale
La CER ci dice con che frequenza l’evento
indesiderato si è verificato
nel gruppo sperimentale
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

Dal rapporto tra EER e CER individuiamo il rischio relativoche ci dice qual è il rischio di manifestare l’evento negativo
nel gruppo sperimentale rispettoa quello del gruppo di controllo.
Se l’intervento ha un effetto benefico
RR<1Se peggiora l’esito RR>1
Se non c’è differenza RR=1
Rischio Relativo / RR
aEER
a + bRR = =
cCER
c + d
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

A volte per motivi statisticianziché essere calcolato il RRtroviamo indicato l’odds ratio
che non confronta le frequenze
(rischio) degli eventi, ma le loro probabilità.
se l’intervento ha un effetto benefico
OR<1Se peggiora l’esito OR>1
Se non c’è differenza OR=1
Odds ratio / OR
a/b OR =
c/d
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

Sia il RR che l’OR sono misure della forza dell’associazione tra trattamento ed esito RELATIVE. Esse, cioè, non ci danno espressione della importanza clinica degli eventi nei due gruppi.Per questo motivo, per comprendere la rilevanza clinica degli effetti, vengono calcolate altre misure di efficacia.
GIMBEGIMBE®®
Il difetto di RR e OR

Riduzione Assoluta del Rischio
ARR = CER _ EER
La riduzione del rischio assoluto ci dà l’esatta
espressionedi quanto si riduca la frequenza
degli eventi negativi con il trattamentosperimentato.
La riduzione del rischio relativo dice con che
proporzione diminuisce il rischio con
il trattamento sperimentato.
Riduzione Relativa del Rischio
ARRRRR =
CER
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

La RRR è di nuovo una misura relativa, che non ci dà idea della frequenza, e quindi dell’importanza, dell’evento negativo.Al contrario ARR è proprio espressione di questa misura, ma essendo un numero decimale non è facile da ricordare.Per questo motivo la misura che rende al meglio l’importanza clinica dell’associazione tra trattamento ed outcome è il NNT.
GIMBEGIMBE®®
I difetti di RRR e ARR

Number Needed to Treat 1
NNT = ARR
Il numero dei pazienti da trattare ci dice il numero di
quante persone è necessariotrattare per evitare un
evento negativo. Si tratta diun valore espresso con
numeri interi (e quindi è piùfacile da ricordare)
tanto più è piccolo tanto maggiore è l’efficacia clinica
del trattamento.Tanto più è grande
tanto più è modesta l’efficaciadel trattamento.
GIMBEGIMBE®®
Misure di efficacia per gli esisti discreti

Trivedi DP, Doll R, Khaw KT. Effect of four montly oral vitamin D3 supplementation on fracutres and mortality in men and women living in the community: randomised double blind controlled trial. BMJ 2003; 326:469-72. La somministrazione di un integratore di Vitamina D3 per via orale riduce l’incidenza di fratture negli anziani (65-85) residenti al domicilio?P: anziani residenti al domicilio.I: somministrazione di un integratore di Vit D3.C: somministrazione di un placebo.O: Incidenza di fratture e mortalità da tutte le cause.
GIMBEGIMBE®®
Un esempio realeUn esempio reale

Rischio Relativo Riduzione Assoluta del RischioEER 0,088
RR = = = 0,8 ARR= CER - EER= 0,11 – 0,088 = 0,022 CER 0,11
Riduzione relativa del rischio = di quanto si riduce il rischio nel gruppo sperimentale?Riduzione assoluta del rischio = differenza (%) fra controllo e sperimentale
Gruppo intervento
Frattura Non frattura
N. Tot.
Trattamento sperimentale 119 1226 1345
Trattamento controllo 149 1192 1341
Riduzione Relativa del Rischio Number Needed to TreatARR 0,022 1 1
RRR = = = 20% NNT = = = 44CER 0,11 ARR 0,022
GIMBEGIMBE®®

RCT a doppio cieco della durata di 5 anni sulla riduzione del rischio di malattie coronariche con la somministrazione di gemfibrozil.
Pazienti arruolati: 4081gruppo sperimentale (gemfibrozil) 2051 pz.gruppo controllo (placebo) 2030 pz.
gruppo sperimentale eventi cardiaci 56 morti 45
gruppo controllo eventi cardiaci 84 morti 42
HELSINKI HEART STUDYNew England Journal of Medicine 1987;
317:1237-45
Calcolare RR, ARR, RRR, NNTGIMBEGIMBE®®
Un esempio realeUn esempio reale

Spesso i risultati degli studi clinici sono presentati in termini di riduzione relativa del rischio (RRR) espressa come percentuale. RRR è un indicatore che, se non completato da ulteriori elementi, può enfatizzare l’efficacia di un trattamento, in particolare può far credere che il risultato sia piùrilevante del reale nella pratica medica.
GIMBEGIMBE®®

Studio B: 10.000 pazienti per gruppo; EER= 0,01 (1%); CER=0,02 (2%); RRR= 0,5 (50%)
Studio A: 10.000 pazienti per gruppo; EER= 0,1 (10%); CER=0,2 (20%); RRR= 0,5 (50%)
Studio C: 10.000 pazienti per gruppo; EER= 0,001 (0,1%); CER=0,002 (0,2%); RRR= 0,5 (50%)
ARRStudio A: 0,1 (10%); Studio B: 0,01 (1%); Studio C: 0,001 (0,1%)
NNTStudio A: 10 soggetti; Studio B: 100 soggetti; Studio C: 1000 soggetti
GIMBEGIMBE®®

GIMBEGIMBE®®
La curva gaussiana

Quando valutiamo l’efficacia di un trattamento, oltre ad osservare il valore della misura di efficacia, dobbiamo valutarne la sua precisione.Ciò si effettua considerando l’intervallo di confidenza (IC).
GIMBEGIMBE®®
Intervallo di confidenza (IC)

L’intervallo di confidenza (IC) fornisce la misura della precisione dei risultati di una ricerca, così da poter trarre deduzioni sulla popolazione da cui sono tratti quei pazienti.
Per convenzione si è stabilito che la precisione dell’intervallo di confidenza sia al 95%, lasciando sempre un piccolo - 5% -margine di errore dovuto al caso.
GIMBEGIMBE®®
Intervallo di confidenza (IC)

Stima l’intervallo dei valori all’interno del quale, con una probabilità del 95%, partendo dal risultato conseguito nel campione, cade il reale valore della popolazione studiata.
L’IC si fonda sull’idea che lo stesso studio, condotto su differenti campioni di pazienti, non porterebbe a risultati identici, ma questi sarebbero distribuiti intorno al risultato vero che resta sconosciuto.
GIMBEGIMBE®®
Intervallo di confidenza (IC)

In particolare dobbiamo verificare:– Quanto è ampio l’intervallo di confidenza.– Che i suoi limiti non vadano oltre il valore che
conferma l’ipotesi nulla (assenza di associazione).
GIMBEGIMBE®®
Intervallo di confidenza (IC)

Tanto più è ampio l’intervallo di confidenza, tanto meno precisa è la stima dell’associazione tra fattori di rischio e condizione (e meno dobbiamo fidarci del risultato dello studio).L’ampiezza dell’IC è inversamente proporzionale alla dimensione del campione (se sono stati inclusi pochi soggetti il risultato ottenuto ènecessariamente poco preciso).
GIMBEGIMBE®®
Intervallo di confidenza (IC)

Coloro che eseguono lo studio mirano a dimostrare l’esistenza di una relazione tra il trattamento ed il miglioramento dell’outcome, cercando di dimostrare l’inesistenza dell’ipotesi nulla.L’ipotesi nulla sussiste tutte le volte in cui non vi è alcuna relazione tra il miglioramento dell’esito ed il trattamento studiato.
GIMBEGIMBE®®
Ipotesi nulla

Ipotesi nulla - H0 Ipotesi alternativa - H1
Non esiste una reale differenza tra le variabili studiate: le differenze osservate sono dovute la caso.
Le differenze osservate sono troppo grandi per essere dovute al caso.
GIMBEGIMBE®®
Ipotesi nulla

Come faccio a verificare che l’ipotesi nulla si è verificata o meno?Attraverso l’esame dei valori delle misure di efficacia, che non devono esprimere specifici valori.
GIMBEGIMBE®®
Ipotesi nulla

Parametro Valore nullo
RRR, RR, OR 1
ARR 0
NNT Infinito
Se questo valore è 1, il rischio o la
probabilità di incorrere
nell’evento avverso sono
Uguali, sia che si faccia il
trattamento o meno
ARR non deve essere 0, perchésignificherebbe che il beneficio ottenuto in termini di riduzione assoluta del rischio è 0, nel qual caso NNT diventerebbe un valore tendente ad infinito.
GIMBEGIMBE®®
Ipotesi nulla nei parametri discreti

Nel caso in cui lo studio misuri parametri continui, mediante la dimostrazione della differenza della media, essa non deve essere 0.
GIMBEGIMBE®®
Ipotesi nulla nei parametri continui

Oltre a verificare i valori delle misure di efficacia, e del loro IC, vi è anche un altro parametro che occorre osservare che ci dice quale sia la significatività statistica dei risultati ottenuti.Si tratta del test di significatività che attribuisce il valore ad una variabile detta “p”.
GIMBEGIMBE®®
Significatività statistica

Il valore di “p” misura la probabilità che la associazione osservata possa essere dovuta a fluttuazioni casuali, ossia alla possibile variabilità tra campioni, e possa quindi non corrispondere a fenomeni reali. Quanto deve essere il valore di “p” per poter escludere l’ipotesi nulla?
GIMBEGIMBE®®
Significatività statistica

Viene deciso dei ricercatori che indicano il livello di significatività statistica stabilito.Il livello di significatività per convenzione è0,05. Si conclude cioè che una differenza non è dovuta al caso se “p” è uguale o inferiore a 0,05.Nel caso i ricercatori vogliano darsi una maggiore rigorosità statistica possono portare tale valore soglia a 0,01.
GIMBEGIMBE®®
Significatività statistica

È chiaro quindi che – "Significativo" non è sinonimo di "importante“– "Significativo" = difficilmente dovuto al puro
caso.
GIMBEGIMBE®®
Significatività statistica

La significatività statistica non è l’unico criterio utile per decidere se utilizzare i risultati di uno studio. La significatività statistica dipende dalla numerosità del campione e dall’entità dell’efficacia del trattamento (differenze degli esiti). Differenze clinicamente irrilevanti possono divenire statisticamente significative se le dimensioni dei campioni sono sufficientemente grandi. Al contrario, differenze clinicamente rilevanti possono essere statisticamente non significative se i campioni sono troppo piccoli (in gergo statistico, se lo studio manca di potenza statistica).
GIMBEGIMBE®®
Significatività statistica

Randomized Controlled Trials - Critical Appraisal
Come si valutano i Trial Randomizzati Controllati.
GIMBEGIMBE®®

Durante la lettura di una pubblicazione si devono trovare informazioni sufficienti, presentate chiaramente e coerentemente, affinché si possa decidere, in base alle evidenze fornite dagli autori, se le conclusioni a cui arrivano sono logiche e credibili.
GIMBEGIMBE®®
Critical appraisal

1. Validità interna2. Rilevanza clinica
3. Applicabilità
4. Consistenza
Critical appraisal
GIMBEGIMBE®®

E’ diretta funzione del rigore metodologico seguito dai ricercatori nelle fasi di:
pianificazione e conduzione dello studioanalisi dei risultati
La validità interna ha l’obiettivo di minimizzare i bias che possono “distorcere” la validità interna della ricerca
I criteri di validità interna variano con il disegno dello studio correlato agli obiettivi (eziologia, diagnosi, prognosi, trattamento)
GIMBEGIMBE®®
Validità interna

A. I risultati dello studio sono validi?Domande preliminari
Lo studio si basa su una domanda di ricerca chiaramente formulata? – Una domanda di ricerca è chiaramente formulata se sono
indicati la popolazione studiata, l’intervento erogato, l’outcome considerato
Gli autori hanno utilizzato il tipo giusto di studio?– Deve esserci coerenza tra il disegno dello studio ed il
quesito.
Vale la pena continuare?GIMBEGIMBE®®
Validità interna

A. I risultati dello studio sono validi?Domande specifiche
L’assegnazione dei pazienti al trattamento èrandomizzato?– I migliori metodi di randomizzazione sono
quelli realizzati con il computer o con le tabelle dei numeri random; sistemi più deboli sono rappresentati dalla assegnazione alternata, secondo l’ordine di arrivo o del giorno, settimana o mese.Se non c’è stata randomizzazione
si può anche lasciare perdere l’articolo in esame.
GIMBEGIMBE®®
Validità interna

Tutti i pazienti ammessi a partecipare allo studio sono stati considerati in modo appropriato nella formulazione delle conclusioni?– La percentuale dei pazienti persi al follow up
non può essere superiore al 20%.– L’analisi dei risultati deve essere effettuata
secondo l’intention to treat.
GIMBEGIMBE®®
Validità interna

Vi era cecità rispetto al trattamento? A che livelli?
– Considera che questo non è sempre possibile, ma valuta se sono stati compiuti tutti gli sforzi per assicurare la cecità. In generale coloro che analizzano i dati possono sempre non essere resi a conoscenza a che gruppo si riferiscono i dati che stanno analizzando.
GIMBEGIMBE®®
Validità interna

I gruppi erano simili all’inizio dello studio?– Valuta l’eventuale presenza di fattori di
confondimento che possono avere influito sugli esiti.
Al di là dell’intervento sperimentale i partecipanti sono stati assistiti nello stesso modo?– Ad esempio verifica se sono stati valutati agli
stessi intervalli.
GIMBEGIMBE®®
Validità interna

1. Validità interna
2. Rilevanza clinica3. Applicabilità
4. Consistenza
GIMBEGIMBE®®
Critical appraisal

Misura, oltre la significatività statistica, l’entità e la precisione dei risultati dello studio
Corrisponde alla fase di analisi dei risultati
Gli elementi che influenzano la rilevanza clinica sono diversi per gli studi di:
• trattamento• diagnosi• eziologia e prognosi
GIMBEGIMBE®®
Rilevanza clinica

Copyright © - GIMBE®
Studi di eziologia e prognosi‐ Rilevanza clinica del danno o fattore prognostico‐ RR (studi di coorte), OR (studi caso‐controllo)‐ Ampiezza limiti di confidenza
Rilevanza clinica

Studi su trattamenti‐ Rilevanza clinica dell’end‐point (surrogato vs significativo)‐ NNT‐ Ampiezza limiti di confidenza
GIMBEGIMBE®®
Rilevanza clinica

B. Quali sono i risultati?Quanto è grande l’effetto del trattamento?– Verificare che i parametri di efficacia non
corrispondano al valore dell’ipotesi nulla.– Quanto precisa è la stima dell’effetto del
trattamento?– Valutare gli intervalli di confidenza ed il valore
di “p”.
GIMBEGIMBE®®
Rilevanza clinica

1. Validità interna
2. Rilevanza clinica
3. Applicabilità4. Consistenza
GIMBEGIMBE®®
Critical appraisal

E’ il grado con cui i risultati dello studio possono essere applicati al paziente individuale
Sinonimi: validità esterna, generalizzabilità
E’ condizionata da: criteri di selezione dei pazienti: inclusione, esclusionesetting assistenziale: aspetti strutturali‐organizzativi,
tecnologie, “competence” professionaledescrizione accurata e completa delle modalità di
erogazione degli interventi sanitari
GIMBEGIMBE®®
Applicabilità

C. Il risultato potrà aiutarti a livello locale?I risultati possono essere applicati alla popolazione locale?– Considera se i pazienti considerati nel trial
sono così diversi da quelli da te assistiti.
GIMBEGIMBE®®
Applicabilità

ExplanatoryRCTs
Ideal condition
Routine clinical practice
Internal validity(efficacy)
Generalizzability(effectiveness)
Pragmatic RCTs
GIMBEGIMBE®®

1. Validità interna
2. Rilevanza clinica
3. Applicabilità
4. Consistenza
GIMBEGIMBE®®
Critical appraisal

Si riferisce al fatto che i risultati di uno studio vengano confermati da altri studi
Sinonimi: riproducibilità della ricerca
Lo strumento ideale per verificare la consistenza della ricerca è rappresentato dalle revisioni sistematiche con meta‐analisi di più studi
N.B. Il bias di pubblicazione, oltre a sovrastimare l’efficacia dei trattamenti, influenza la consistenza della ricerca
GIMBEGIMBE®®
Consistenza

Mortality in the placebo and beta-blocker groups of 22 RCTs
Brophy JM, et al. Ann Intern Med 200GIMBEGIMBE®®

no
no
no
Presenza di bias che compromettono la validità dei risultati
Lo studio è valido?
sì
I risultati dello studio sono clinicamente rilevanti?
sì
Risultati validi, ma irrilevanti: end points surrogati, NNT elevato, ampi limiti di confidenza
Risultati validi e clinicamente rilevanti, ma non applicabili nel mio contesto assistenziale
I risultati dello studio sono applicabili?
sì
Best evidence for patients
GIMBEGIMBE®®

GIMBEGIMBE®
THE END
GIMBEGIMBE®®

GIMBEGIMBE®®
Gabriele ManziAzienda U.S.L. di Bologna
Evidence Based Practice

Modificato da Haynes RB et al ACP J Club. 2002; 136:A11-14.
Clinical state, settingand circumstances
Patientpreferences
Researchevidence
Health care resources
Clinicalexpertise
GIMBEGIMBE®®

“…E’ causa di grande preoccupazione constatare come la professione medica non abbia saputo organizzare un sistema in grado di rendere
disponibili e costantemente aggiornate, revisioni critiche sugli effetti dell’assistenza sanitaria”
Archibald Cochrane, 1972
GIMBEGIMBE®®

ANATOMIA DELLANATOMIA DELL’’INFORMAZIONE INFORMAZIONE BIOMEDICABIOMEDICA
RICERCA PRIMARIA
• Studi Osservazionali• Studi Sperimentali
RICERCA SECONDARIA
• Revisioni Sistematiche• Linee Guida• Analisi economiche• Analisi decisionali
FONTI TERZIARIE
• Revisioni tradizionali• Trattati• Editoriali• Parere degli esperti
Distorsione dei risultati
GIMBEGIMBE®®

Hanno lo scopo di rendere più“maneggevole” una enorme quantità di informazioni
• revisioni tradizionali• revisioni sistematiche
GIMBEGIMBE®®
Reviews

Le revisioni tradizionali, oltre ad avere obiettivi molto ampi, non sono basate su una ricerca sistematica delle evidenze disponibili, ma su una loro selezione legata a diversi fattori: reperibilità, accessibilità linguistica, sintonia con le idee dell’autore
Nelle revisioni sistematiche esiste un protocollo che definisce un preciso obiettivo e descrive fonti e metodi utilizzati per ricercare, selezionare e sintetizzare gli studi primari.
Cartabellotta A. Rec Prog Med 1998
Narrative reviews vs Systematic reviews
GIMBEGIMBE®®

Paragonabile al capitolo di un libroNon esplicitato il metodo di selezione, sintesi e interpretazione delle evidenzeImpossibilità di fare una valutazione criticaObiettivi molto ampiSpesso fatte su commissione
GIMBEGIMBE®®
Narrative reviews

E’ una ricerca scientifica vera e propriaEsplicitato il protocollo metodologicoPossibilità di fare una valutazione critica (definizione di obiettivi, fonti, criteri…)Sintesi dei risultati spesso fatta con metodo meta analitico
GIMBEGIMBE®®
Systematic reviews

Narrative vs Systematic ReviewCaratteristica Revisione
narrativaRevisione sistematica
Domande Molto vasta Focalizzate su problemi clinici
Risorse e ricerca Non specificate Complete ed esplicite
Selezione Non specificate Basato su criteri espliciti
Critical appraisal Variabile Rigoroso
Sistesi Qualitativa Qualitativa/quantitativa *meta-analisis
GIMBEGIMBE®®

E’ uno strumento capace di risolvere alcuni problemi legati alla ricerca e alla
interpretazione delle migliori evidenze
Ha un ruolo sempre crescente per la pratica clinica,
per la formazione permanente, per le decisioni di politica sanitaria
GIMBEGIMBE®®
Systematic reviews

Processo di sviluppo delle RS
Nel loro approccio, i ricercatori, usano metodi che sono pianificati e documentati in un protocollo di revisione sistematica
Il protocollo di revisione sistematica assicura che la revisione sia condotta con lo stesso rigore che ci si aspetta da una ricerca
GIMBEGIMBE®®
Systematic reviews

Definizione del quesitoStrategia di ricercaDefinizione dei criteri di inclusione/esclusioneValutazione qualità degli studiEstrapolazione dei datiAnalisi dei dati
GIMBEGIMBE®®
Componenti essenziali del processo
Systematic reviews

GIMBEGIMBE®®

E’ un momento fondamentale del processo di una revisione sistematica
Deve definire i partecipanti, gli interventi da valutare, gli esiti da misurare
Quesiti poco chiari e troppo generici portano a revisioni di qualità scadente
GIMBEGIMBE®®
Quesito

GIMBEGIMBE®®

Devono essere sempre definiti prima di iniziare la ricerca degli studi in letteraturaDevono riflettere direttamente il quesito della ricerca (partecipanti, interventi, risultati)Devono indicare che tipo di studi verranno selezionati
GIMBEGIMBE®®
Definizione dei criteri di inclusione/esclusione

GIMBEGIMBE®®

DatabaseRicerca manualeRicerca bibliograficaContatti con i ricercatoriRicerca di letteratura non pubblicata
GIMBEGIMBE®®
Elementi per la strategia di ricerca

Lo scopo è di identificare quanti più studi ragionevolmente possibili sull’argomento;Anche i lavori non pubblicati devono essere richiesti per aiutare a minimizzare i rischi di pubblicazione. Le riviste tendono ad accettare e pubblicare più facilmente le ricerche che dimostrano un esito positivo.Includere, quando è possibile, anche le pubblicazioni non in inglese
Elementi per la strategia di ricerca
GIMBEGIMBE®®

GIMBEGIMBE®®

Una RS di buona qualità dipende soprattutto dalla qualità degli studi inclusiLa valutazione dello studio deve essere condotta sulla metodologia della ricerca utilizzata per condurre lo studio stessoEsistono numerosi strumenti per effettuare una valutazione criticaVa definito il metodo usato per la valutazione e per l’analisi delle informazioni per farli conoscere ai fruitori della RS
GIMBEGIMBE®®
Valutazione della qualità degli studi

GIMBEGIMBE®®

Definizione dei risultati importanti per le proprie necessitàEstrapolare i dati nel modo più accurato possibile, tale che siano di facile utilizzo quando si affronta l’analisi dei dati stessiCreare uno strumento (es. una griglia) dove registrare le informazioni che servono, relative ad ogni studio incluso nella RS
GIMBEGIMBE®®
Sintesi degli studi

GIMBEGIMBE®®

L’obiettivo di una revisione sistematica è di riassumere i risultati di differenti studi per ottenere una valutazione totale dell’efficacia di un intervento o di un trattamento. Per un buon livello qualitativo, l’analisi dei dati va definita nel protocollo della RS.
GIMBEGIMBE®®
Sintesi dei dati

L’obiettivo di una revisione sistematica è di riassumere i risultati di differenti studi per ottenere una valutazione totale dell’efficacia di un intervento o di un trattamento.
Sintesi dei dati

I dati di una revisione si possono analizzare in modi differenti: se quantitativi si prestano al metodo statistico della meta-analisi, se qualitativi possono essere presentati in forma narrativaIn entrambi i casi è opportuno definire a priori la metodologia che si intende seguire
GIMBEGIMBE®®
Sintesi dei dati

GIMBEGIMBE®®

La RS presenta un quesito ben definito? (partecipanti, interventi, outcomes)E’ stato fatto un lavoro sostanziale per la ricerca della letteratura? (database appropriati, key words adeguate, letteratura non pubblicata)E’ stata data una corretta e chiara definizione dei criteri di inclusione/esclusione? Questi sono adeguati?
GIMBEGIMBE®®
Systematic reviews critical appraisal

E’ stata valutata dagli autori la qualità degli studi inclusi nella RS?Gli autori forniscono sufficienti informazioni sui singoli studi? (progetto di ricerca, dimensione del campione, descrizione dell’intervento, risultati ottenuti)Gli studi sono stati assemblati in modo appropriato? (test di eterogeneità)
GIMBEGIMBE®®
Systematic reviews critical appraisal

Metodo per combinare i risultati di più studi indipendenti in modo da poter calcolare un valore statistico riassuntivo totale (cumula insieme più studi per ottenere un risultato unico)Consente una stima più precisa dell’efficacia di un trattamentoLa validità di una MA dipende anche dalla qualità della RS su cui si basa
GIMBEGIMBE®®
Meta-analisi

Systematic review analisi metodologica
Meta – analisi analisi statistica
GIMBEGIMBE®®

Revisioni sistematiche (qualitative)
***
Meta – analisi (non sistematiche)
Revisioni sistematiche (quantitative)
GIMBEGIMBE®®

E’ utilizzata nei casi di incertezza nella valutazione di efficacia di un trattamentoquando i risultati dei singoli studi non sono univociquando singoli studi sono effettuati su un campione di pazienti numericamente scarso (poco affidabili)
LA COMBINAZIONE DEI DATI DIMINUISCE L’IMPRECISIONE DEI RISULTATI DEI SINGOLI STUDI
GIMBEGIMBE®®
Meta-analisi

GIMBEGIMBE®® Antmann EM, et al. JAMA 1992

GIMBEGIMBE®®

The Cochrane Library
GIMBEGIMBE®®

Nel 1993 nasce la fondazione CochraneCollaboration, un network internazionale con l’obiettico di “preparare, aggiornare e disseminare revisioni sistematiche degli studi clinici controllati sugli effetti dell’assistenza sanitaria e, laddove non disponibili studi clinici controllati, revisioni sistematiche delle evidenze comunque esistenti.”
Chalmers I., 1993
GIMBEGIMBE®®
Cochrane Collaboration

• Tuttavia:- il n° totale di revisioni sistematiche (RS) èancora modesto (poco più di 1.800 ripetto alle 30-35 mila previste)- la maggior parte di RS riguarda 5-6 specialitàcliniche- molte RS non sono conclusive (aree grigie)
• Rappresenta la prima fonte di consultazione se il “bisogno d’informazione” riguarda l’efficacia dei trattamenti
Cochrane Library
GIMBEGIMBE®®

Rappresenta la prima fonte di consultazione se il “bisogno d’informazione” riguarda l’efficacia dei trattamenti Nonostante sia la fonte di elezione dispone di un numero di revisioni sistematiche ancora limitato (circa 4200 vs 35000 previste)Molte RS in essa contenute riguardano un numero esiguo di specialità clinichemolte RS non sono conclusive (aree grigie)
GIMBEGIMBE®®
Cochrane Library

È il database principale:
raccoglie le revisioni sistematiche realizzate dai gruppi di revisione Cochrane (circa 4200)
raccoglie i protocolli di quelle in corso di realizzazione (circa 1900)
abstracts delle revisioni e titoli dei protocolli sono disponibili gratuitamente on-line.
GIMBEGIMBE®®
Cochrane Database of Systematic Reviews(CDRS)

Contiene circa 12.000 abstract di revisioni sistematiche pubblicate in letteratura e valutate criticamente a cura del NHS Centre for Review and Dissemination.
Accessibile gratuitamente on-line
GIMBEGIMBE®®
Database of Abstract of Reviews ofEffectiveness - (DARE)

E’ un registro creato dopo una ricerca manuale delle riviste pubblicate dal 1945 ad oggi per identificare tutti i RCTs pubblicati; include più di 608.000 RCTs(molti non indicizzati nelle banche dati tradizionali)
GIMBEGIMBE®®
Cochrane Controlled Trial Register(CCTR)

The Cochrane Methodology Register (CMR)
Health Technology Assessment Database
NHS Economic Evaluation Database
GIMBEGIMBE®®
altre risorse

www.evidencebasednursing.it GIMBEGIMBE®®

Mappa della ricerca
FOREGROUND - PICO
E’ meglio posizionare il paziente con Braden <13 su materasso a cessione d’aria o a pressione alternata?
QUESITO
BACKGROUND
Cos’è il TIA o come si assiste il paziente con TIA
TESTO o E-BOOK!
LGRS Studi Primari
ESPERIENZA - RICERCA
GIMBEGIMBE®®

Revisioni sistematiche
Mappa della ricerca
QUESITO
Studi Primari
E’ un trattamento? Trial randomizzto e controllato
Ricerca una causa? Studio di coorte o Caso controllo
Vuole conoscere una prognosi? Studio di coorte
Vuole valutare un test Studio di sensibilitàdiagnostico? e specificità
GIMBEGIMBE®®

GIMBEGIMBE®
THE END
GIMBEGIMBE®®

GIMBEGIMBE®®
Gabriele ManziAzienda U.S.L. di Bologna
Evidence Based Practice

Conoscenze che derivano dalle prove di efficacia, ossia dalle sperimentazioni cliniche.Esse permettono l’acquisizione di nuove informazioni partendo dal dato empirico derivante da esse.
Non è evidenza ciò che èesplicito, ma ciò che èdimostrato.
GIMBEGIMBE®®
Cosa sono le evidenze scientifiche?

Garantire un livello omogeneo di assistenza su obiettivi prioritari di prevenzione, diagnosi, terapia, riabilitazione
Utilizzare criteri scientifici, oggettivi, riproducibili per decidere come impiegare le risorse economiche.
Cartabellotta, 1998
GIMBEGIMBE®®
Obiettivi di un sistema sanitario impossibilitato a soddisfare tutte le
domande di salute

•PSN 1998-2000•DLGs 229/99
GIMBEGIMBE®®
Come è arrivata l’EBHC in Italia?

Il Piano Sanitario Nazionale 1998-2000 definisce i livelli di assistenza alla luce di principi ispiratori del Servizio Sanitario Nazionale.
GIMBEGIMBE®®
Il PSN 1998-2000

Principio dell'efficacia e dell'appropriatezza degli
interventi:le risorse devono essere indirizzate verso le prestazioni la cui efficacia é riconosciuta in base alle evidenze scientifiche e verso i soggetti che maggiormente ne possono trarre beneficio.
GIMBEGIMBE®®
Principi ispiratori del SSN

Appropriatezza clinicaMisura in cui un particolare intervento è sia efficace sia indicato per la persona che lo
riceve. - benefici > effetti negativi e disagi
- benefici/danni > con = costi- è relativa solo alla fase decisionale
GIMBEGIMBE®®
Appropriatezza

Appropriatezza organizzativao generica
Misura in cui un intervento viene erogato al livello più gradito all’utente e/o meno costoso
(ad es. domicilio, ambulatorio, day-hospital, ricovero)
PSN 1998-2000appropriatezza = efficacia
GIMBEGIMBE®®
Appropriatezza

Coordinato dall’Istituto Superiore di Sanità in collaborazione con l’ASL 6 di Livorno, l'Agenzia di sanitàpubblica della regione Lazio, CeVEAS di Modenae il Centro Cochrane Italiano.
http://www.snlg-iss.it/GIMBEGIMBE®®

GIMBEGIMBE®®
Linee Guida
Raccomandazioni di comportamento clinico, prodotte attraverso un metodo sistematico di revisione della letteratura, che informano tutti gli attori di un sistema sanitario (professionisti, manager, utenti) sulle modalità più appropriate per la gestione di presentazioni cliniche e malattie.

GIMBEGIMBE®®
Contesto Locale
Insieme delle variabili (strutturali, organizzative, tecnologiche, professionali) in grado di condizionare l’applicazione locale di singole raccomandazioni delle LG.

GIMBEGIMBE®®
Percorso Assistenziale*• Strumento finalizzato all’implementazione delle LG• In relazione al contesto locale il PA:
- adatta le raccomandazioni delle LG- definisce:
- procedure (how)- professionisti (who)- setting (where)- tempistiche (when)
• In altri termini: PA= LG + CL
* da preferire a “percorso diagnostico-terapeutico”, termine più riduttivo

GIMBEGIMBE®®
Processo (assistenziale)• Rappresenta l’unità elementare del PA (costituito da N processi)• In funzione del numero di strutture e di professionisti coinvolti nella sua erogazione il processo può essere:
- molto semplice, talora sino ad identificarsi con la procedura (vedi) - estremamente complesso
• L’appropriatezza dei processi è correlata al grado di aderenza alle raccomandazioni cliniche.

GIMBEGIMBE®®
Procedura (operativa)• Sequenza di azioni tecnico-operative attraverso cui il professionista eroga gli interventi assistenziali.• Rappresenta l’unità elementare del processo (costituito da N procedure) • Può essere molto semplice (cateterismo vescicale) o estremamente complessa (chirurgia dell’aorta addominale).• La conformità della procedura dovrebbe essere definita da standard di competence professionale (accreditamento?) • Sinomini: istruzione operativa

GIMBEGIMBE®®
A B C D
Percorso assistenzialeProcessoProcedura operativa

GIMBEGIMBE®®
Protocollo
• Può indicare, indifferentemente, un processo o una procedura.• Nella letteratura giuridica il termine protocollo viene interpretato come “vincolante” (mandatory) per i professionisti.• Questo termine, in disuso nella letteratura internazionale, dovrebbe essere limitato, anche per i potenziali rischi medico-legali.

Basate sull’evidenza Non basate sull’evidenza
GIMBEGIMBE®®
Linee Guida

Le non non evidenceevidence basedbased guide guide lineline erano diffuse soprattutto qualche anno fa, erano fatte in casa (senza l’ausilio di revisioni sistematiche) ed avevano come risultato quello di validare i comportamenti giàin atto.
GIMBEGIMBE®®

Le evidenceevidence basedbased guide guide lineline si caratterizzano per:la multidisciplinarietmultidisciplinarietàà del gruppo responsabile
della produzione della linea guidala valutazione sistematicavalutazione sistematica delle prove scientifiche
disponibili quale base per le raccomandazioni formulate
la classificazioneclassificazione delle raccomandazioni in base alla qualità delle prove scientifiche che le sostengono
Grilli et al, Lancet 2000
GIMBEGIMBE®®

• Deve dichiarare la qualità delle informazioni utilizzate (livello di evidenzalivello di evidenza) e l’importanza/rilevanza/fattibilità/priorità della loro implementazione (forza delle forza delle raccomandazioniraccomandazioni).
• Deve essere prodotta attraverso un processo processo multidisciplinaremultidisciplinare (cittadini/pazienti): ciò migliora la qualità delle linee guida e favorisce la sua adozione nella pratica.
GIMBEGIMBE®®
Requisiti per lo sviluppo e l’applicabilità di una EBGL

• Deve esplicitare le alternativeesplicitare le alternative di trattamento e i loro effetti sugli esiti.
• Deve essere flessibile e adattabileflessibile e adattabile alle mutevoli condizioni locali.
• Nel produrre una linea guida dovrebbero essere esplicitati i possibili indicatori di monitoraggioindicatori di monitoraggioutili a valutarne l’effettiva applicazione.
GIMBEGIMBE®®
Requisiti per lo sviluppo e l’applicabilità di una EBGL

• Una linea guida dovrebbe essere aggiornata aggiornata con regolaritcon regolaritàà per evitare che le raccomandazioni divengano obsolete.
• Una linea guida deve essere chiaradeve essere chiara, dotata di una struttura semplice e di un linguaggio comprensibile, esplicitando in modo inequivocabile i punti ritenuti fondamentali e le aree di incertezza.
GIMBEGIMBE®®
Requisiti per lo sviluppo e l’applicabilità di una EBGL

Le tecnologie sanitarie sono l’insieme delle risorse materiali e delle conoscenze indispensabili per l’erogazione delle prestazioni sanitarie. La valutazione delle tecnologie sanitarie (technology assessment) consiste nella valutazione di benefici, rischi e costi (clinici, sociali, economici, di sistema) del trasferimento delle tecnologie sanitarie nella pratica clinica.
GIMBEGIMBE®®
Technology Assessment

Si pone ad un livello di complessità superiore occupandosi non solo di aspetti clinici, ma anche organizzativi, gestionali, economici e sociali. Mira fornire ad amministratori e decisori della sanità le informazioni necessarie per fare scelte appropriate sul piano dell’efficienza allocativa.
GIMBEGIMBE®®
Technology Assessment

GIMBEGIMBE®®

• Agenzie internazionali
• Agenzie nazionali
• Agenzie governative
• Agenzie regionali
• Aziende sanitarie
GIMBEGIMBE®®
Chi produce linee guida?

variabilità degli interventi professionali;
esigenza di confronto tra attori diversi con differenti punti di vista (amministratori, pazienti, operatori);
crescente complessità ed aumentata insorgenza di obsolescenza delle tecnologie sanitarie;
aumentate aspettative da parte della popolazione.
GIMBEGIMBE®®
Perché?

Le linee guida riassumono in modo sistematico le migliori modalità assistenziali, attualmente riconosciute, relative ad una patologia o condizione.
Esse vengono assunte come “regole d’arte” e nelle controversie giudiziarie costituiscono il criterio per valutare la correttezza tecnica della condotta del professionista sanitario nella cura del paziente.
GIMBEGIMBE®®
Aspetti legali

La dottrina medico-legale, pur affermando che per valutare la condotta professionale dei professionisti si deve fare riferimento anche a questi documenti, nella stesura vigente sottolinea correttamente “il valore relativo” delle linee guida “per i singoli casi”.
GIMBE®
GIMBEGIMBE®®
Aspetti legali

Le linee guida, infatti, fanno riferimento a un paziente astratto, non a “quel particolare paziente” che il professionista deve in concreto curare, con la sua complessità clinica e la sua specificità patologica.
GIMBEGIMBE®®
Aspetti legali

La diligenza deve essere valutata in relazione alle circostanze concrete nelle quali il professionista si è trovato a operare e, quindi, la giurisprudenza riconosce al sanitario pur sempre uno spazio di discrezionalità tecnica nella scelta del metodo di cura da proporre al singolo paziente, purché fondata correttamente su dati oggettivi riscontrati durante il processo di cura.
GIMBEGIMBE®®
Aspetti legali

In definitiva il professionista nella sua pratica clinica deve confrontarsi con il contenuto di una linea guida che, se correttamente elaborata e aggiornata, può contenere le “regole dell’arte”astrattamente applicabili. Peraltro la responsabilità della scelta del trattamento da praticare compete al professionista che ha in cura il paziente e, quindi, spetta al sanitario verificare se nel caso di specie si deve seguire l’indicazione contenuta nella linea guida ovvero èopportuno discostarsene a ragion veduta.
GIMBEGIMBE®®
Aspetti legali

Le linee guida non sono infatti vincolanti per legge e, quindi, non sussiste alcun obbligo di automatica applicazione. Le linee guida, se correttamente interpretate, non deresponsabilizzano quindi il professionista, ma rendono invece più evidente il suo dovere di motivare e documentare le scelte dei comportamenti di cura.
GIMBEGIMBE®®
Aspetti legali

E’ opportuno infine ricordare che la responsabilità professionale presuppone l’accertamento non solo della colpa, ma anche della sussistenza del rapporto di causalità tra comportamento del sanitario ed evento dannoso per il paziente.
GIMBEGIMBE®®
Aspetti legali

GIMBEGIMBE®®

Il livello delle prove (LdP) indica che la raccomandazione è derivata da studi pianificatie condotti in modo tale da produrre informazionivalide e prive di errori sistematici.
GIMBEGIMBE®®
Livello delle prove

Complessivamente, quindi, si può affermare chel’LdP dipende da:
appropriatezza del disegno di studio utilizzato(qualità metodologica a priori);rigore e qualità di conduzione e analisi dello studio
(controllo dell’errore sistematico);dimensione dell’effetto clinico/epidemiologico
misurato (controllo dell’errore casuale);appropriatezza e rilevanza degli indicatori di esito
utilizzati (rilevanza clinico-epidemiologica).
GIMBEGIMBE®®
Livello delle prove

La forza della raccomandazione (FdR) siriferisce alla probabilità che l’applicazione nellapratica di una raccomandazione determini un miglioramento dello stato di salute dellapopolazione.
GIMBEGIMBE®®
Forza delle raccomandazioni

Livello delle evidenze
Forza delle raccomandazioni
GIMBEGIMBE®®
Forza delle raccomandazioni

GIMBEGIMBE®®

GIMBEGIMBE®®

GIMBEGIMBE®®
Ceveas

Ceveas
GIMBEGIMBE®®

Più volte sono state prodotte per consenso, attraverso una riunione di un gruppo di esperti nel corso di un convegno per discutere e concordare quale sia il comportamento ottimale da tenere per affrontare un determinato problema.
GIMBEGIMBE®®
Come nasce una LG

Questo processo presenta molti limiti:
non sempre l’opinione degli esperti riflette lo stato delle conoscenze mediche!
l’analisi della letteratura scientifica potrebbe non essere eseguita in modo sistematico!
le conclusioni a cui si arriva possono non essere valide da un punto di vista scientifico!
GIMBEGIMBE®®

Gli esperti si confrontano nel corso di una o piùdiscussioni non strutturate e infine arrivano a un consenso sulle raccomandazioni.Questo tipo di consenso viene definito informale in quanto i criteri di scelta non sono fissati a priori e le raccomandazioni espresse possono riflettere l’opinione dei più esperti o di coloro che hanno maggiore autorevolezza o potere.E’ il metodo più semplice, pratico e utilizzato, ma èanche quello scientificamente meno valido.
GIMBEGIMBE®®
Consenso informale

Il confronto in questo caso è più strutturato, in modo che tutte le posizioni espresse all’interno del gruppo possano essere rappresentate e discusse.Il metodo più noto è il Metodo” Delphi”: a tutti i partecipanti viene inviato un questionario con le domande principali sulle quali si vuole trovare un consenso.I partecipanti rispondono e si arriva via via a discutere le risposte-comportamenti piùraccomandati.
GIMBEGIMBE®®
Consenso formale

Ideato dalla Rand Corporation negli anni Ottanta, prevede gruppi di 10-11 esperti che vengono chiamati a definire i criteri di utilizzo appropriato di una procedura o di un trattamento, avendo come riferimento non il paziente medio, ma specifiche categorie di pazienti.Il suo limite è che nonostante si combinino le opinioni degli esperti con le indicazioni della letteratura, la valutazione resta sempre soggettiva.E’ difficile coinvolgere più figure professionali, con diverso potere.
GIMBEGIMBE®®
Metodo Rand

Prevede momenti di discussione e verifica delle informazioni disponibili sui diversi aspetti di una tecnologia sanitaria, in modo da definire lo stato dell’arte e produrre raccomandazioni per la pratica clinica.
GIMBEGIMBE®®
Consensus Conference

NICE National Institute of Clinical Excellence
http://www.nice.org.ukOrganizzazione creata dal governo inglese all’interno del suo servizio sanitario nazionaleValuta l’efficacia degli interventi medici, rappresentati da farmaci, dispositivi medici, procedure fisioterapiche e chirurgiche allo scopo di orientare una corretta utilizzazione delle risorse da parte del National Health Service ingleseProduce linee guida cliniche e rapporti di valutazione tecnologica
GIMBEGIMBE®®

GIMBEGIMBE®
THE END
GIMBEGIMBE®®

Endoscopic cyanoacrylate injection versus b-blockerfor secondary prophylaxis of gastric variceal bleed:a randomised controlled trial
Smruti Ranjan Mishra,1 Barjesh Chander Sharma,1 Ashish Kumar,2
Shiv Kumar Sarin1,2
ABSTRACTBackground and aims Bleeding from gastric varices isoften severe and difficult to manage. Endoscopicinjection of gastric varices with cyanoacrylate is effectivein prevention of rebleeding. The efficacy of b-blockers insecondary prophylaxis of gastric variceal bleed has notbeen well studied. A comparison of the efficacy of b-blocker treatment and cyanoacrylate injection for theprevention of gastric variceal rebleeding was carried out.Methods Patients with gastro-oesophageal varices type2 (GOV2) with eradicated oesophageal varices orisolated gastric varices type 1 (IGV1) who had bled fromgastric varices were randomised to cyanoacrylateinjection (n¼33) or b-blocker treatment (n¼34).Baseline and follow-up upper gastrointestinal endoscopyand hepatic venous pressure gradient (HVPG)measurements were performed. Primary end points weregastric variceal rebleeding or death.Results The probability of gastric variceal rebleedingrate in the cyanoacrylate group was significantly lowerthan in the b-blocker group (15% vs 55%, p¼0.004) andthe mortality rate was lower (3% vs 25%, p¼0.026)during a median follow-up of 26 months. The medianbaseline and follow-up HVPG in the cyanoacrylate groupwere 15 (10e23) and 17 (11e24) mm Hg (p¼0.001)and for the b-blocker group 14 (11e24) and 13(8e25) mm Hg (p¼0.003). While no patient showedreduction of HVPG in the cyanoacrylate group, in the b-blocker group 12 of 28 (42%) patients were responders,of which 5 (41% of responders) bled. On multivariateanalysis, treatment method, portal hypertensivegastropathy and size of the gastric varix >20 mmindependently correlated with gastric variceal rebleeding.Gastric variceal rebleeding independently correlated withmortality.Conclusions Cyanoacrylate injection is more effectivethan b-blocker treatment for the prevention of gastricvariceal rebleeding and improving survival.Clinical trial number NCT00888784.
INTRODUCTIONGastric varices (GVs) are less common than oeso-phageal varices, occurring in w20% of patientswith portal hypertension.1 GVs bleed lessfrequently than oesophageal varices1; howeverbleeding tends to be more severe, requires moretransfusions and has a higher mortality rate thanoesophageal variceal bleeding.1e3 After control ofacute bleeding, GVs have a high rebleeding rate(34e89%) and treatment options to preventrebleeding are not optimised.2 4 5 The frequency
and severity of bleeding from GVs depends on theirlocation (figure 1). GVs could be associated withoesophageal varices (gastro-oesophageal varicestype 1 along the lesser curve, or type 2 (GOV2),along the fundus) or are present in isolation(isolated gastric varix type 1 (IGV1), in the fundusor at ectopic sites in the stomach or the first part ofthe duodenum (isolated gastric varix type 2)).1
b-Blockers have been reported to reduce the riskof rebleeding of oesophageal varices by w40% andrisk of death by 20%.6e11 A small open-label trial ofb-blocker and nitrate treatment in patients withGVs reported no significant benefit for rebleeding orsurvival, but there was a trend towards lowerrebleeding.12 Endoscopic injection of cyanoacrylate
Significance of this study
What is already known about this subject?< The efficacy of b-blockers in secondary prophy-
laxis of gastric variceal bleeding has not beenwell studied.
< Endoscopic injection of cyanoacrylate has beenproven to be effective in the prevention ofgastric variceal rebleeding.
< b-Blockers have been recommended empiricallyfor prophylaxis of gastric variceal bleedingwithout proof.
What are the new findings?< The probability of rebleeding from large gastro-
oesophageal varices type 2 (GOV2) or isolatedgastric varices type 1 (IGV1) was significantlylower in the cyanoacrylate group (15%)compared with the b-blocker group (55%).
< The majority of patients with such gastricvarices have baseline HVPG >12 mm Hg.
< Cyanoacrylate injection increases the hepaticvenous pressure gradient (HVPG), and b-blockerdecreases HVPG significantly on follow-up.
< Mortality in patients treated with a b-blocker ishigher than with cyanoacrylate injection.
How might it impact on clinical practice in theforeseeable future?< Endoscopic injection of cyanoacrylate should be
used to prevent rebleeding from large GOV2 andIGV1 and improve survival.
< b-Blockers are not effective in prevention ofrebleeding from such gastric varices, althoughthey decrease HVPG in these patients.
1Department ofGastroenterology, G B PantHospital, New Delhi, India2Department of Hepatology,Institute of Liver & BiliarySciences (ILBS), New Delhi,India
Correspondence toDr S K Sarin, Department ofGastroenterology, G B PantHospital, 201 Academic Block,New Delhi 110002, India;[email protected]
Revised 1 February 2010Accepted 7 February 2010
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 729
Stomach

has been proven to be effective in the prevention of GVrebleeding.13e17 However, cyanoacrylate injection is associatedwith a risk of cerebral or pulmonary embolism and damage tothe endoscope.18
Results on the long-term efficacy of gastric variceal obturationwith cyanoacrylate injection are variable, with eradication ratesbetween 50% and 100% and a rebleeding rate of 23e50%, withthe majority occurring in the first year.13 16 19e21 Due to the highrate of primary haemostasis and lower rebleeding rate, GVobturation with cyanoacrylate injection is used as the first-linetreatment for bleeding GVs and secondary prophylaxis of GVbleed.
For patients who have bled from IGV1 or GOV2, N-butyl-cyanoacrylate, transjugular intrahepatic portosystemic shunt(TIPS) or b-blockers have been recommended.22 Endoscopicinjection of thrombin has also been tried for secondaryprophylaxis of bleeding from GVs.23e26 b-Blockers have beenrecommended empirically for GVs since they have been found tobe quite effective in patients who have bled from oesophagealvarices. However, there is no randomised controlled trial availablecomparing b-blocker treatment with endoscopic cyanoacrylateinjection for prevention of rebleeding from GVs. We conducteda randomised controlled trial to study the efficacy of endoscopiccyanoacrylate injection versus b-blockers in the prevention ofgastric variceal (GOV2 or IGV1) rebleeding and improvement insurvival. We also investigated the predictors of rebleeding andmortality in patients who had previously bled from GVs.
Patients and methodsPatients with portal hypertension with upper gastrointestinalbleed were assessed. All consecutive patients with cirrhosis withGVs (GOV2 with eradicated oesophageal varices or IGV1)admitted to our hospital from August 2006 to March 2009 wereenrolled. The study was approved by our institutional reviewboard, and written informed consent was obtained from allpatients. Parents gave the written consent for children. Patientswho had bled from GOV2 or IGV1 were included. The exclusioncriteria were non-cirrhotic portal hypertension, presence of
oesophageal varices, contraindications to b-blockers and cyano-acrylate injection, patients already on b-blockers, past history ofcyanoacrylate injection or sclerotherapy for GVs or GV ligation,TIPS, balloon-occluded retrograde transvenous obliteration(BRTO), balloon-occluded endoscopic injection sclerotherapy,shunt operation, undetermined origin of bleeding, hepaticencephalopathy grade III/IV, hepatorenal syndrome, hepatocel-lular carcinoma, presence of deep jaundice (serum bilirubin>10 mg/dl), cardiorespiratory failure, age >75 years, pregnancyor patients who did not give informed consent.After assessing eligibility with initial endoscopy and subse-
quently obtaining informed consent patients were randomised,using a sealed envelope technique, to receive cyanoacrylateinjection (Nectacryl, Nectar Laboratories, Medak, India) or b-blocker (propranolol). The allocation sequence remained withthe statistician and the sequence remained concealed from theinvestigators until the intervention was assigned. The doctorswho evaluated the outcomes were blinded to group assignment.According to the Baveno IV consensus on portal hypertension,22
secondary prophylaxis starts from the sixth day of acute varicealbleed. For patients presenting with acute GV bleeding, anemergency endoscopy was done and, if the bleeding was foundto be from GOV2 or IGV1, one cyanoacrylate injection wasgiven to control acute GV haemorrhage (not with the intentionof obliterating the GV). The patients were randomised and thefollow-up started from day 6 after occurrence of acute bleeding.None of the patients presenting with acute GV bleeding receivedb-blocker or endoscopic treatment for secondary prophylaxisfrom day 0 till day 6. Patients with a previous bleed wererandomised after control endoscopy. For patients randomised tothe propranolol group, control endoscopy was completed andpropranolol was started on the same day. For patients rando-mised to the cyanoacrylate group, a second endoscopy withcyanoacrylate injection was performed on the same day. Inpatients with a history of past bleeding, the follow-up startedimmediately after randomisation. The follow-up period wasterminated at 3 months after enrolment of the last patient.Upper gastrointestinal endoscopy was done to determine the
variceal status at baseline and repeated at 3 month intervals orduring rebleeding. The size of the GV, recurrence of oesophagealvarices and portal hypertensive gastropathy (PHG) wererecorded. An attempt was made to localise the source of bleedingat the time of emergency endoscopy. The size of the GV wascalculated by a zebra guide wire with markings made at 5 mmintervals, and we classified the fundal varix as small (<10 mm),medium (10e20 mm) or large (>20 mm). The colour of the GVwas observed as red or blue. The recent signs of haemorrhageover the GV were the presence of a clot or blackish spot localisedover the GV.1 The presence or absence of oesophageal varices andPHG were also evaluated. Concurrence of two independentobservers was required before characterising the type of GV andits size. Rebleeding from GVs was managed with a cyanoacry-late injection in the b-blocker group and TIPS or surgery in thecyanoacrylate group.The primary end points of the study were rebleeding from
GVs or death. The actuarial probability of rebleeding from GVsand mortality were calculated. Secondary end points wereincrease or decrease in the size of GVs, appearance of newoesophageal varices and appearance or worsening of PHG andcomplications.The diagnosis of cirrhosis was based on clinical, biochemical,
radiological and histological findings. Ultrasonography of theabdomen with Doppler of splenoportal axis, CT angiography ormagnetic resonance (MR) angiography was done to diagnose
Figure 1 Classification of gastric varices.
730 Gut 2010;59:729e735. doi:10.1136/gut.2009.192039
Stomach

cirrhosis and assess spontaneous shunts. Model for end-stageliver disease (MELD) and ChildeTurcotteePugh (CTP) scoreswere calculated at baseline and serial intervals.
Technique of cyanoacrylate injectionEndoscopic injection was performed intravariceally usinga therapeutic endoscope and a transparent Teflon injector, witha 6e8 mm long, 21-gauge needle, with N-butyl-2-cyanoacrylate.The cyanoacrylate was injected without dilution with lipiodol.The maximum amount of cyanoacrylate injected per site was2 ml, and the total amount of cyanoacrylate required to oblit-erate the GVs completely was recorded. An attempt was madeto obturate the GVs completely at one session by injectingcyanoacrylate at multiple sites. If a second session was required,it was done within a week of the initial session. The injected GVwas palpated using the hub of the injector with the needleretracted to look for solidification and obliteration of the GV. Ifthe GV was not completely obturated, cyanoacrylate was rein-jected till the whole GV became solidified.
b-Blocker treatmentPropranolol was started at a dose of 20 mg twice daily. The dosewas increased every alternate day by 20 mg to achieve targeta heart rate of 55/min or to the maximal dose of 360 mg/day ifthe medication was well tolerated and the systolic blood pres-sure was >90 mm Hg. On the occurrence of intolerable adverseeffects, systolic blood pressure <90 mm Hg or pulse rate <55/min, the dose of the medication was decreased step-wise, andeventually stopped if these adverse events were disabling andpersisted. Reintroduction of the medication was attempted ifcessation of the drug resulted in improvement of the reportedside effect. Compliance was assessed by pill count, and moni-toring the heart rate and blood pressure. Patients were moni-tored every day until adequate b-blockade was achieved, thenevery month for the first 3 months and subsequently every3 months. Patients were advised to refrain from consumingalcohol and from taking non-steroidal anti-inflammatory drugs.
HVPG measurementAfter an overnight fast, HVPG measurement was performed aspreviously described.27 HVPG was measured and repeated after1 year in both groups. In patients who presented with GVbleeding, HVPG was measured within 24 h. Patients were cate-gorised into responders ($20% reduction in HVPG or HVPG<12 mm Hg) and non-responders (<20% reduction in HVPG),and the primary end points were calculated.
Statistical analysesThe rebleeding rates following cyanoacrylate injection have beenreported to be in the range of 15e25%.13e18 We hypothesisedthat the rate of GV rebleeding would be more in the b-blockergroup (50%) in comparison with the cyanoacrylate group (15%).Thus, to achieve a statistical power of 80% with an error of 5%and drop-out rate of 20%, a sample size of 32 patients in eachgroup was calculated.
Fisher exact test was used to compare categorical groups.Student t test and ManneWhitney U test were used for theparametric and non-parametric data, respectively. For compar-ison of pretreatment and post-treatment parameters, pairedStudent t test was used. The KaplaneMeier analyses and log-rank test were applied to compare the cumulative probability ofrebleeding from the GV, and death. Each patient was analysed inan intention to treat manner. A p value of <0.05 was consideredsignificant. Statistical analysis was done using SPSS, version 15.0(SPSS, Chicago, Illinois, USA).
RESULTSA total of 1005 consecutive patients with portal hypertensionand upper gastrointestinal bleeding presented to our hospitalbetween August 2006 and March 2009 (figure 2). Inclusioncriteria were not fulfilled in 938 patients. Sixty-seven (6.6%)patients with cirrhosis who were enrolled in the study had GVs(GOV2/IGV1) without oesophageal varices with a history of GVbleed, and were randomised to receive either cyanoacrylateinjection (n¼33) or b-blocker (n¼34). One patient in thecyanoacrylate group and two patients in the b-blocker grouprefused the allocated intervention, so 32 patients with cirrhosisreceived the allocated treatment in each group. One patient whowas lost to follow-up in the b-blocker group was included in thefinal analysis.Of the 64 patients, 15 presented with active bleeding from
GVs and were treated with a combination of vasoactive drugsalong with an emergency single injection of cyanoacrylate afterendoscopic confirmation of the source of bleed from GVs asrevealed by active ooze of blood (n¼6), spurt (n¼5) or presenceof a clot (n¼4). Of 15 patients presenting with acute gastricvariceal bleed, eight patients were randomised to the cyanoac-rylate group and seven to the b-blocker group. Of the 64patients, 49 had a history of bleed from GVs within a 15 dayperiod from the time of enrolment. These patients had under-gone diagnostic endoscopy at the time of acute bleeding atperipheral hospitals which confirmed bleeding from GVs asshown by evidence of spurt (n¼7), ooze (n¼17) or presence ofa clot (n¼14) on GVs, and only large GVs (n¼11) without anyother obvious source of bleeding, such as oesophageal varices,portal hypertensive gastropathy, gastric antral vascular ectasia,gastric ulcer, gastric erosions and duodenal ulcer. However, thesepatients did not receive endoscopic injection of cyanoacrylate.They were managed with blood transfusions or infusion of freshfrozen plasma, and some patients received vasoactive drugs.Bleeding stopped in all the patients without endoscopic
Figure 2 Trial profile.
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 731
Stomach

treatment. Upper gastrointestinal endoscopy performed aftera median period of 7 (4e15) days showed maroon-black spots(n¼26), a nipple (n¼9) on GVs and only large GVs (n¼14)without other obvious source of bleeding.
Baseline characteristics of both groups of patients werecomparable (table 1). The median follow-up period was 26(range 3e34) months in both the groups. The most commonaetiology of cirrhosis was alcohol or cryptogenic (table 1). Fourpatients in the b-blocker and six patients in the cyanoacrylategroup had IGV1; the rest of the patients had GOV2. The size,colour of GVs and PHG between the two groups were similar(table 1). MR portovenography and Doppler ultrasounddemonstrated spontaneous lienorenal shunt in the cyanoacrylategroup (n¼8) and in the b-blocker group (n¼11).
Gastric variceal obturationEndoscopic intervention could be performed with 100% tech-nical success. Complete obturation of GVs was achieved in all.The mean number of sessions required to achieve obliterationwas 1.760.4 (range 1e2). The mean volume of cyanoacrylaterequired was 6.061.7 (range 3e9) ml. Mean time to obturationwas 2.060.6 (range 1e3) days.
b-Blocker treatmentAll patients were compliant to b-blocker treatment. The meandaily dose was 160 (range 80e320) mg. The median timeinterval to achieve the desired heart rate was 15 (range 5e20)days, and during this period no patient bled from GVs.
Gastric variceal rebleedingOver a median follow-up period of 26 (3e34) months, in thecyanoacrylate group 3 (9%) (GOV2 (n¼2), IGV1 (n¼1)) patientsbled, in contrast to 15 (44%) (GOV2 (n¼12), IGV1 (n¼3)) in theb-blocker group. The probability of GV rebleeding was signifi-cantly lower in the cyanoacrylate group (15%) compared with
the b-blocker group (55%) (p¼0.004, log rank 8.466, figure 3A).The difference was also significant in the frequency of bleedingover a median follow-up period of 26 months from GOV2between the two groups (p¼0.005) (table 2). Of 34 patients inthe b-blocker group 15 had rebleed, and cyanoacrylate injectionwas used to control rebleeding in 13 patients. In two patients,bleeding from GVs was torrential and cyanoacrylate injectioncould not be performed, and they were subjected to surgery. Of33 patients in the cyanoacrylate group, two patients hada rebleed and were managed by surgery.
Size of gastric varixOver a median follow-up period of 26 (3e34) months in thecyanoacrylate group all patients had a decrease in GV size(table 2) and the median size of GVs decreased from w25(10e35) to w5 (0e10) mm (p<0.01). In the b-blocker group, 15of 34 (44%) patients had an increase in size of GVs and the sizeof GVs increased from a median of 25 (10e35) to 30 (15e40)mm (p<0.01). All patients bleeding from GVs in the b-blockergroup had an increase in size of at least 5 mm.
Appearance of oesophageal varices and PHGOver a median follow-up period of 26 (3e34) months in thecyanoacrylate group, 7 of 33 (21%) and in b-blocker group 4 of34 (11%) patients developed oesophageal varices on follow-up(p¼0.302). All patients had small oesophageal varices and didnot bleed. No significant difference was noted between thecyanoacrylate group (24%) and the b-blocker (21%) groupregarding appearance or worsening of PHG (table 2).
Hepatic venous pressure gradientBaseline HVPG was measured in 27 patients in the cyanoacry-late group (three patients refused and, in another two patients,the hepatic vein could not be cannulated) and in 28 patients inthe b-blocker group (three patients refused and in another one
Table 1 Baseline characteristics of study group patients
Parameters Cyanoacrylate (n[33) b-Blocker (n[34) p Value
Age (median, range) years 40 (6e70) 39 (6e70) 0.702
Sex (male:female) 19:14 26:8 0.109
Aetiology of cirrhosis (alcohol/cryptogenic/viral and others)
12/14/7 11/15/8 0.779
Previous gastric variceal bleed 4/33 3/34 1
Ascites 15/33 15/34 1
Hepatic encephalopathy (grade I/II) 3/33 3/34 1
Serum bilirubin (median, range) mg/dl 1.6 (0.4e6.9) 1.6 (0.3e5.9) 0.756
Serum albumin (median, range) g/dl 2.8 (1.2e3.7) 2.9 (2e3.7) 0.782
INR (median, range) 1.6 (1.1e3.2) 1.5 (1.1e3.1) 0.812
Platelets (median, range) 105/ml 1.1 (0.4e2.1) 1.1 (0.5e3.2) 0.695
Serum creatinine (median, range) mg/dl 0.7 (0.2e1.5) 0.7 (0.3e1.5) 0.818
ChildePugh score (median, range) 9 (6e12) 9 (6e12) 0.753
ChildePugh class (A/B/C) 4/12/17 5/13/16 0.970
MELD score (median, range) 15 (8e35) 15 (8e35) 0.360
HVPG (median, range) mm Hg 15 (10e23) 14 (11e24) 0.894
Time interval between index bleed andrandomisation (median, range) days
7 (4e15) 7 (4e14) 1
Follow-up (median, range) months 26 (3e34) 26 (3e34) 0.947
Gastro-oesophageal varix type2 26/33 28/34 0.495
Isolated gastric varix type 1 6/33 4/34 0.495
Size of gastric varix (median, range) mm 25 (10e35) 25 (10e35) 0.202
Portal hypertensive gastropathy 12/33 17/34 0.213
Colour of gastric varix (red/blue) 25/8 23/11 0.572
Spontaneous shunts 11/33 10/34 0.791
HVPG, hepatic venous pressure gradient; INR, international normalised ratio; MELD, model for end-stage liver disease.
732 Gut 2010;59:729e735. doi:10.1136/gut.2009.192039
Stomach

patient the hepatic vein could not be cannulated). Follow-upHVPG was measured in 23 patients in the cyanoacrylate group(three patients refused HVPG measurement and in one patientthe hepatic vein could not be cannulated) and in 28 patients inthe b-blocker group. Median baseline HVPG was 15 (10e23)mm Hg and follow-up HVPG was 17 (11e24) mm Hg in thecyanoacrylate group. The increase in HVPG on follow-up in thecyanoacrylate group was significant (p¼0.001). The medianbaseline HVPG was 14 (11e24) mm Hg and follow-up HVPGwas 13 (8e25) mm Hg in the b-blocker group. The decrease in
HVPG on follow-up in the b-blocker group was significant(p¼0.003). In the cyanoacrylate group, 22 of 27 (81%) patientshad HVPG >12 mm Hg at baseline and 22 of 23 (91%) patientshad HVPG >12 mm Hg on follow-up. In the b-blocker group, 24of 28 (85%) patients had HVPG >12 mm Hg at baseline and 18of 28 (64%) patients had HVPG >12 mm Hg on follow-up.
Response to treatment and rebleedingIn the cyanoacrylate group, none of the patients responded totreatment in the form of reduction in HVPG. In the b-blockergroup, 12 of the 28 (42%) patients were responders. However, 5(41%) responders bled during follow-up. Of the non-responders,2 of 23 (8%) patients in the cyanoacrylate group and 8 of 16(50%) patients in the b-blocker group bled. In responders, themedian baseline HVPG was 16 (12e22) mm Hg and the follow-up HVPG was 12 (8e16) mm Hg. A >20% reduction in HVPGwas achieved in 12 of 28 (42%) patients in the b-blocker group.In non-responders in the b-blocker group, the median baselineHVPG was 14 (11e24) mm Hg and the follow-up HVPG was13.5 (10e25) mm Hg. Of the responders who bled, one hadIGV1 and the other four had GOV2. Those responders who didnot bleed had a mean decrease in HVPG from baseline of 30% incomparison with a 22% decrease in those who bled. In patientswith IGV1, the baseline median HVPG was 13 (11e17) mm Hgand in patients with GOV2 the baseline median HVPG was 14(10e24) mm Hg.Since all the patients were bleeders, it was interesting to note
that patients with spontaneous shunt (n¼21) at baseline hada lower median HVPG (13 (10e15) mm Hg) than patientswithout spontaneous shunt (n¼43) (18 (13e24) mm Hg(p¼0.001)). Thus, the HVPG levels which predict the likelihoodof rebleeding in patients with or without shunt are 13 and18 mm Hg, respectively. In patients with spontaneous shunt, 6of 21 (28%) patients had a HVPG value of <12 mm Hg. Inpatients without spontaneous shunt, all had HVPG >12 mmHg. Overall, 20% of patients who bled had a HVPG <12 mmHg.Patients with cirrhosis who bled had a median HVPG of 15(11e24) mm Hg at baseline and 14 (9e25) mm Hg (p¼0.715) atfollow-up. In non-bleeders, the median HVPG at baseline was 14(10e23) mm Hg and follow-up HVPG was 13.5 (8e22) mm Hg(p¼0.031). HVPG decreased in 5 of 10 (50%) patients in theb-blocker group with spontaneous shunt.
ComplicationsNo significant difference in the frequency of complications wasobserved between the two groups. One (3%) patient in the
Figure 3 Probability of freedom from gastric variceal rebleeding (A)and survival (B) in the cyanoacrylate and b-blocker group.
Table 2 Results of treatment in the cyanoacrylate and b-blocker groups
CharacteristicsCyanoacrylate group (n[33) b-Blocker group (n[34)
p Value(n, %) (n, %)
Follow-up (months) 26 (3e34) 26 (3e34)
Rebleeding 3/33 (10%) 15/34 (44%) 0.004
Bleed from GOV2 2/26 (8%) 12/28 (36%) 0.005
Bleed from IGV1 1/6 (16%) 3/4 (75%) 0.190
Increase in size of GV 0 15/34 (44%) 0.001
Decrease in size of GV 33/33 (100%) 0 0.001
Appearance of oesophageal varix 7/33 (21%) 4/34 (11%) 0.302
Aggravation/appearance of PHG 8/33 (24%) 7/34 (21%) 1
Bleed-related mortality 0/33 6/34 (17%) 0.024
Overall mortality 1/33 (3%) 8/34 (23%) 0.046
GOV2 0/26 6/28 (21%) 0.023
IGV1 1/6 (16%) 2/4 (50%) 0.5
Complications 1 (3%) 2 (6%) 1
GOV2, gastro-oesophageal varix type 2; GV, gastric varix; IGV1, isolated gastric varix type 1; PHG, portal hypertensive gastropathy.
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 733
Stomach

cyanoacrylate and 2 (6%) patients in the b-blocker groupdeveloped spontaneous bacterial peritonitis, and improved ontreatment (table 2). Four patients in the b-blocker group devel-oped headache and generalised weakness which was controlledwith dose reduction, and after 2e3 weeks the desired dose wasachieved. No serious adverse effects were noticed which requiredstoppage of b-blocker.
MortalityOver amedian follow-upperiod of 26 (3e34)months, a significantdifference in the overall mortality was observed between thecyanoacrylate (n¼1, 3%) and the b-blocker (n¼8, 25%) group(p¼0.016, log rank¼5.808, figure 3B). Of 15 patients withrebleeding in the b-blocker group, treated with cyanoacrylateinjection, 6 (19%) patients died in comparison with none in threeof 33 patients in the cyanoacrylate group (p¼0.024) who weremanaged with surgery at the time of rebleeding. In the b-blockergroup, one patient died of hepatic encephalopathy and one patientdied of spontaneous bacterial peritonitis and hepatorenalsyndrome. In the cyanoacrylate group, one patient died of hepaticencephalopathy. The cumulative 2-year survival rate was 90% inthe cyanoacrylate group and 52% in the b-blocker group. In theb-blocker group, only one patient died among responderscompared with seven patients among non-responders (p¼0.077).
Predictors of GV rebleed and mortalityOn univariate analysis, the variables which influenced GVrebleeding were size of the GV >20 mm, a red or black spot overthe GV, blue colour of the GV, presence of PHG, internationalnormalised ratio (INR) $1.6, serum creatinine >1 mg/dl, CTPscore $9, MELD score $17 and the treatment method. Onmultivariate analysis, the treatment method (p¼0.006), PHG(p¼0.029) and size of the GV >20 mm (p¼0.002) independentlycorrelated with GV rebleeding. Variables which influencesurvival on univariate analysis included GV rebleeding, presenceof PHG, CTP $9, MELD score $17 and the treatment method.On multivariate analysis, GV rebleeding (p¼0.003) indepen-dently correlated with mortality.
DISCUSSIONThe results of this large prospective randomised controlledclinical trial comparing the efficacy of cyanoacrylate andb-blocker treatmjent clearly demonstrate that endoscopic injec-tion of cyanoacrylate is significantly more effective than b-blocker treatment for the prevention of rebleeding from GVs.
Small studies have reported that drug treatment is effective inthe prevention of GV rebleeding after successful endoscopicinjection of the bleeding varix with tissue adhesives.12 28 A smallopen-label trial of b-blocker and nitrate treatment reported nosignificant benefit in terms of risk of rebleeding or survival.12
This study had several limitations such as a small sample size,retrospective analysis, fixed and low doses of drug and lack ofhaemodynamic monitoring. In another study, Evrard et alrandomised patients to receive 160 mg/day of propranolol(n¼20) or histoacryl injection (n¼21) for secondary prophylaxisof gastro-oesophageal variceal bleed.28 The rebleeding andmortality rates were similar in the b-blocker and endoscopictreatment groups, with a higher complication rate in the latter(10% vs 47%). This study had limitations of early terminationdue to increased complications in the histoacryl arm, nohaemodynamic monitoring and inclusion of patients with co-existing oesophageal varices. In fact, all patients had oesophagealvarices, and 17 had GVs (12 with GOV1 and 5 with GOV2).
The median baseline HVPG was 14.5 (10e24) mm Hg. Of 55patients with bleeding from gastric varices, 16% had baselineHVPG <12 mm Hg. Patients with gastric variceal bleed havebeen shown to have lower HVPG than patients with bleedingfrom oesophageal varices.29 In addition, w35% of patients withgastric variceal bleed have portal pressure <12 mm Hg.29
Spontaneous splenorenal or gastrorenal shunts commonlydevelop between the splenic vein (splenorenal shunt) and gastricvarices, respectively, and connect via the inferior phrenic orsuprarenal vein to the left renal vein.30 These shunts are seen inup to 60% of patients with GVs.30 31 We found spontaneousshunts in 33% of our patients. Median HVPG in patients withspontaneous shunts was lower in comparison with thosewithout shunts (13 vs 18 mm Hg). In fact, HVPG was high inpatients with both GOV2 and IGV1 types of varices. Of the 15patients who bled, 20% had HVPG of <12 mm Hg.There are limited data on the efficacy of b-blockers in reduc-
tion of portal pressure in patients with GVs. Keeping this inview, HVPG was measured to assess the response to b-blockertreatment in all our patients with GVs. The median HVPG wassignificantly reduced on follow-up; however, this could notprevent GV rebleeding or mortality. Of the 12 responders to b-blocker, five patients who rebled had a median decrease in HVPGof 22% compared with 30% in seven patients who did notrebleed. This raises the question of whether a 20% reduction inHVPG is adequate to define a response to b-blocker in patientswith GVs, or whether it should be a >25% reduction. In thecyanoacrylate group, HVPG increased on follow-up, howeverwithout an increase in the frequency of rebleeding. This increasein HVPG could be attributed to redistribution of blood flow inthe portal system and indirectly suggests adequacy of GVobturation. Whether addition of a b-blocker to prevent the risein HVPG by cyanoacrylate injection will be helpful needs furtherstudies.BRTO and balloon-occluded endoscopic injection scle-
rotherapy have shown good results for prophylaxis of high riskfundal variceal bleed.31 32 In a prospective trial, Hong et al showedthat the therapeutic efficacies of glue and BRTO for the treatmentof active gastric variceal haemorrhage and/or high-risk GVappeared to be similar. However, glue might be associated witha higher rebleeding rate than BRTO, and BRTO could be aneffective rescue treatment for patients with gastric varicealhaemorrhage after initial treatment with glue.32 TIPS has beenfound to be quite effective in the prevention of GV rebleeding, notonly by reducing the portal pressure, but also by allowing thepossibility of obliterating gastric variceal channels. In a rando-mised controlled trial (patients with both oesophageal varices andGVs), Lo et al showed that TIPS was more effective than glueinjection in preventing rebleeding fromGVs, with similar survivaland frequency of complications.33 However, all these proceduresare quite expensive, need expertise and are associated withcomplications over time.18 29 32e35 Cyanoacrylate injection, onthe other hand, is easily available, rapid, cost-effective, requiresless expertise, is less invasive and has been shown to be veryeffective in preventing GV rebleeding.13 16 19e21 34
Endoscopic variceal sclerotherapy is inappropriate for patientswith fundal varices.5 19 The randomised trials by Tan et al and Loet al compared histoacryl injection and variceal band ligation andreported a rebleeding rate almost twice higher with ligation forsecondary prevention of bleeding from GVs.13 36
Generally not more than 2 ml of cyanoacrylate should beinjected at a single site to prevent embolic and thromboticcomplications.37 38 Precautions to prevent damage to the endo-scope must be taken during cyanoacrylate injection. By avoiding
734 Gut 2010;59:729e735. doi:10.1136/gut.2009.192039
Stomach

lipiodol use, limiting the total volume per injection and byproper monitoring, no embolic complication was observed in ourstudy population. Dilution of cyanoacrylate with lipiodol delayssolidification by 15e20 s, thus increasing the chances of distalembolisation. In the undiluted form, it solidifies within 5e7 s,and thus the chances of distal embolisation become almostnegligible. However, with undiluted cyanoacrylate injection,there is a risk of needle impaction in GVs at the time ofinjection.39
b-Blocker treatment was well tolerated and none of ourpatients required withdrawal of treatment. In the cyanoacrylategroup, 21% of patients had appearance of new oesophagealvarices in comparison with 11% in the b-blocker group, althoughnone of the patients bled from oesophageal varices. Thefrequency of PHG in both the groups was similar (24% vs 21%).
Survival in the cyanoacrylate group was better because ofa low frequency of rebleeding compared with the b-blockergroup. In both the groups, differences in mortality were due torebleed-related deaths. However, mortality due to other causes(not rebleed related) was similar in both the groups. Morefavourable survival in our patients could be due to close follow-up during the study period and the fact that w50% of thepatients with cirrhosis in both the groups were Child A and B.
The stronger aspects of our trial are that it was a randomisedcontrolled study and had a large sample size, a longer follow-upperiod and a minimal drop-out rate. The weaker aspect of thisstudy is inclusion of only a selective patient group with IGV1and GOV2 types of GVs. The applicability of the present studyis related only to patients with bleeding GVs of GOV2 and IGV1types. GVs of GOV2 and IGV1 types are more common, andassociated with more frequent and more severe bleeds withhigher mortality rates as compared with other types of gastricvarices.1
In conclusion, the results of our study clearly demonstratethat cyanoacrylate injection is more effective in the preventionof rebleeding from GVs and improving patient survival ascompared with b-blocker treatment. Propranolol is not effectivein preventing gastric variceal rebleeding despite reduction inHVPG.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the MAMC EthicalCommittee, New Delhi.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Sarin SK, Lahoti D, Saxena SP, et al. Prevalence, classification and natural history of
gastric varices: a long-term follow-up study in 568 portal hypertension patients.Hepatology 1992;16:1343e9.
2. Trudeau W, Prindiville T. Endoscopic injection sclerosis in bleeding gastric varices.Gastrointest Endosc 1986;32:264e8.
3. Thakeb F, Salem SA, Abdallah M, et al. Endoscopic diagnosis of gastric varices.Endoscopy 1994;26:287e91.
4. Bretagne JF, Dudicourt JC, Morisot D, et al. Is endoscopic variceal sclerotherapyeffective for the treatment of gastric varices? [abstract]. Dig Dis Sci 1986;31:505S.
5. Sarin SK. Long-term follow-up of gastric variceal sclerotherapy: an eleven-yearexperience. Gastrointest Endosc 1997;46:8e14.
6. Lebrec D. Pharmacological treatment of portal hypertension: hemodynamic effectsand prevention of bleeding. Pharmacol Ther 1994;61:65e107.
7. Hayes PC, Davis JM, Lewis JA, et al. Meta-analysis of value of propranolol inprevention of variceal haemorrhage. Lancet 1990;336:153e6.
8. Lin HC, Soubrane O, Lebrec O. Prevention of portal hypertension and portosystemicshunts by early chronic administration of clonidine in conscious portal vein-stenosedrats. Hepatology 1991;14:325e30.
9. Sarin SK, Groszmann RJ, Mosca PG, et al. Propranolol ameliorates the developmentof portal-systemic shunting in a chronic murine schistosomiasis model of portalhypertension. J Clin Invest 1991;87:1032e6.
10. Ideo G, Bellati G, Fesce E, et al. Nadolol can prevent the first gastrointestinalbleeding in cirrhotics: a prospective, randomized study. Hepatology 1988;8:6e9.
11. The Italian Multicenter Project for Propranolol in Prevention of Bleeding.Propranolol prevents first gastrointestinal bleeding in non-ascitic cirrhotic patients.Final report of a multicenter randomized trial. J Hepatol 1989;9:75e83.
12. Wu CY, Yeh HZ, Chen GH. Pharmacologic efficacy in gastric varicealrebleeding and survival: including multivariate analysis. J Clin Gastroenterol2002;35:127e32.
13. Lo GH, Lai KH, Cheng JS, et al. A prospective, randomized trial of butylcyanoacrylate injection versus band ligation in the management of bleeding gastricvarices. Hepatology 2001;33:1060e4.
14. Soehendra N, Nam VC, Grimm H, et al. Endoscopic obliteration of largeesophagogastric varices with bucrylate. Endoscopy 1986;18:25e6.
15. Ramond MJ, Valla D, Mosnier JF, et al. Successful endoscopic obliteration ofgastric varices with butyl cyanoacrylate. Hepatology 1989;10:488e93.
16. Huang YH, Yeh HZ, Chen GH, et al. Endoscopic treatment of bleeding gastric varicesby N-butyl-2-cyanoacrylate (Histoacryl) injection: long-term efficacy and safety.Gastrointest Endosc 2000;52:160e7.
17. Binmoeller KF, Soehendra N. “Superglue”: the answer to variceal bleeding andfundal varices? Endoscopy 1995;27:392e6.
18. Ryan BM, Stockbrugger RW, Ryan JM. A pathophysiologic, gastroenterologic, andradiologic approach to the management of gastric varices. Gastroenterology2004;126:1175e89.
19. Sarin SK, Jain AK, Jain M, et al. A randomized controlled trial of cyanoacrylateversus alcohol injection in patients with isolated fundic varices. Am J Gastroenterol2002;97:1010e15.
20. Akahoshi T, Hashizume M, Shimabukuro R, et al. Long-term results of endoscopichistoacryl injection sclerotherapy for gastric variceal bleeding: a 10-year experience.Surgery 2002;131:S176e81.
21. Kim JW, Baik SK, Kim KH, et al. Effect of endoscopic sclerotherapy using N-butyl-2-cyanoacrylate in patients with gastric variceal bleeding. Korean J Hepatol2006;12:394e403.
22. de Franchis R. Evolving consensus in portal hypertension report of the BavenoIV consensus workshop on methodology of diagnosis and therapy in portalhypertension. J Hepatol 2005;43:167e76.
23. Ramesh J, Limdi JK, Sharma V, et al. The use of thrombin injections in themanagement of bleeding gastric varices: a single center experience. GastrointestEndosc 2008;68:877e82.
24. Yang WL, Tripathi D, Therapondos G, et al. Endoscopic use of human thrombin inbleeding gastric varices. Am J Gastroenterol 2002;97:1381e5.
25. Datta D, Vlavianos P, Alisa A, et al. Use of fibrin glue (beriplast) in the managementof bleeding gastric varices. Endoscopy 2003;35:675e8.
26. Tripathi D, Hayes PC. Endoscopic therapy for bleeding gastric varices: to clot orglue? Gastrointest Endosc 2008;68:883e6.
27. Wadhawan M, Dubey S, Sharma BC, et al. Hepatic venous pressure gradient incirrhosis: correlation with the size of varices, bleeding, ascites, and Child’s status.Dig Dis Sci 2006;51:2264e9.
28. Evrard S, Dumonceau JM, Delhaye M, et al. Endoscopic histoacryl obliteration vs.propranolol in the prevention of esophagogastric variceal rebleeding: a randomizedtrial. Endoscopy 2003;35:729e35.
29. Tripathi D, Therapondos G, Jackson E, et al. The role of the transjugular intrahepaticportosystemic stent shunt (TIPSS) in the management of bleeding gastric varices:clinical and haemodynamic correlations. Gut 2002;51:270e4.
30. Watanabe K, Kimura K, Matsutani S, et al. Portal hemodynamics in patients withgastric varices. A study in 230 patients with esophageal and/or gastric varices usingportal vein catheterization. Gastroenterology 1988;95:434e40.
31. Matsumoto A, Hamamoto N, Nomura T, et al. Balloon-occluded retrogradetransvenous obliteration of high-risk gastric fundal varices. Am J Gastroenterol1999;94:643e9.
32. Hong CH, Kim HJ, Park JH. Treatment of patients with gastric variceal hemorrhage:endoscopic N-butyl-2-cyanoacrylate injection versus balloon-occluded retrogradetransvenous obliteration. J Gastroenterol Hepatol 2009;24:372e8.
33. Lo GH, Liang HL, Chen WC, et al. A prospective, randomized controlled trial oftransjugular intrahepatic portosystemic shunt vs. cyanoacrylate injection in theprevention of gastric variceal rebleeding. Endoscopy 2007;39:679e85.
34. Marques P, Maluf-Filho F, Kumar A, et al. Long-term outcomes of acute gastricvariceal bleeding in 48 patients following treatment with cyanoacrylate. Dig Dis Sci2008;53:544e50.
35. Tripathi D, Ferguson JW, Therapondos G, et al. Review article: recent advancesin the management of bleeding gastric varices. Aliment Pharmacol Ther2006;24:1e17.
36. Tan PC, Hou MC, Lin HC, et al. A randomized trial of endoscopic treatment of acutegastric variceal hemorrhage: N-butyl-2-cyanoacrylate injection versus band ligation.Hepatology 2006;43:690e7.
37. Hwang SS, Kim HH, Park SH, et al. N-butyl-2-cyanoacrylate pulmonary embolismafter endoscopic injection sclerotherapy for gastric variceal bleeding. J Comput AssistTomogr 2001;25:16e22.
38. Yoshida H, Onda M, Tajiri T, et al. Endoscopic findings of bleeding esophagogastricvarices. Hepatogastroenterology 2002;49:1287e9.
39. Bhasin DK, Sharma BC, Prasad H, et al. Endoscopic removal of sclerotherapy needlefrom gastric varix after N-butyl-2-cyanoacrylate injection. Gastrointest Endosc2000;51:497e8.
Gut 2010;59:729e735. doi:10.1136/gut.2009.192039 735
Stomach

Stretching to prevent or reduce muscle soreness after
exercise (Review)
Herbert RD, de Noronha M
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2008, Issue 4
http://www.thecochranelibrary.com
Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Pre-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise). 20
Analysis 1.2. Comparison 1 Pre-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours post-exercise). 21
Analysis 1.3. Comparison 1 Pre-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise). 21
Analysis 1.4. Comparison 1 Pre-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours post-exercise). 22
Analysis 1.5. Comparison 1 Pre-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise). 22
Analysis 1.6. Comparison 1 Pre-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours post-exercise). 23
Analysis 2.1. Comparison 2 Post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise). 23
Analysis 2.2. Comparison 2 Post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours post-exercise). 24
Analysis 2.3. Comparison 2 Post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise). 24
Analysis 2.4. Comparison 2 Post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours post-exercise). 25
Analysis 2.5. Comparison 2 Post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise). 25
Analysis 2.6. Comparison 2 Post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours post-exercise). 26
Analysis 3.1. Comparison 3 Either pre- or post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Analysis 3.2. Comparison 3 Either pre- or post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Analysis 3.3. Comparison 3 Either pre- or post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Analysis 3.4. Comparison 3 Either pre- or post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Analysis 3.5. Comparison 3 Either pre- or post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Analysis 3.6. Comparison 3 Either pre- or post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours
post-exercise). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
29APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iStretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Stretching to prevent or reduce muscle soreness afterexercise
Robert D Herbert1, Marcos de Noronha2
1The George Institute for International Health, Camperdown, Australia. 2School of Physiotherapy, University of Sydney, Lidcombe,
Australia
Contact address: Robert D Herbert, The George Institute for International Health, PO Box M201, Missendown Road, Camperdown,
New South Wales, 2050, Australia. [email protected].
Editorial group: Cochrane Bone, Joint and Muscle Trauma Group.
Publication status and date: Edited (no change to conclusions), published in Issue 4, 2008.
Review content assessed as up-to-date: 15 August 2006.
Citation: Herbert RD, de Noronha M. Stretching to prevent or reduce muscle soreness after exercise. Cochrane Database of SystematicReviews 2007, Issue 4. Art. No.: CD004577. DOI: 10.1002/14651858.CD004577.pub2.
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Many people stretch before or after (or both) engaging in athletic activity. Usually the purpose is to reduce risk of injury, reduce soreness
after exercise, or enhance athletic performance.
Objectives
The aim of this review was to determine effects of stretching before or after exercise on the development of post-exercise muscle soreness.
Search strategy
We searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (to April 2006), the Cochrane Central Register
of Controlled Trials (The Cochrane Library 2006, Issue 2), MEDLINE (1966 to May 2006), EMBASE (1988 to May 2006), CINAHL
(1982 to May 2006), SPORTDiscus (1949 to May 2006), PEDro (to May 2006) and reference lists of articles.
Selection criteria
Eligible studies were randomised or quasi-randomised studies of any pre-or post-exercise stretching technique designed to prevent or
treat delayed-onset muscle soreness (DOMS), provided the stretching was conducted soon before or soon after exercise. To be eligible
studies must have assessed muscle soreness or tenderness.
Data collection and analysis
Methodological quality of the studies was assessed using the Cochrane Bone, Joint and Muscle Trauma Group’s methodological quality
assessment tool. Estimates of effects of stretching were converted to a common 100-point scale. Outcomes were pooled in a fixed-effect
meta-analysis.
Main results
Of the 10 included studies, nine were carried out in laboratory settings using standardised exercise protocols and one involved post-
exercise stretching in footballers. All participants were young healthy adults. Three studies examined the effects of stretching before
exercise and seven studies investigated the effects of stretching after exercise. Two studies, both of stretching after exercise, involved
1Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

repeated stretching sessions at intervals of greater than two hours. The duration of stretching applied in a single session ranged from
40 to 600 seconds.
All studies were small (between 10 and 30 participants received the stretch condition) and of questionable quality.
The effects of stretching reported in individual studies were very small and there was a high degree of consistency of results across
studies. The pooled estimate showed that pre-exercise stretching reduced soreness one day after exercise by, on average, 0.5 points on a
100-point scale (95% CI -11.3 to 10.3; 3 studies). Post-exercise stretching reduced soreness one day after exercise by, on average, 1.0
points on a 100-point scale (95% CI -6.9 to 4.8; 4 studies). Similar effects were evident between half a day and three days after exercise.
Authors’ conclusions
The evidence derived from mainly laboratory-based studies of stretching indicate that muscle stretching does not reduce delayed-onset
muscle soreness in young healthy adults.
P L A I N L A N G U A G E S U M M A R Y
Stretching to prevent or reduce muscle soreness after exercise
Many people stretch prior to or after engaging in physical activities such as sport. Usually the purpose is to reduce the risk of injury,
reduce soreness after exercise, or enhance athletic performance.
The review located 10 relevant randomised trials looking at the effect of stretching before or after physical activity on muscle soreness.
The trials were mostly small and of questionable quality. Nine were conducted in laboratories using standardised exercises. Only one
study examined the effect of stretching on muscle soreness after sport. Three of the studies examined the effects of stretching before
physical activity and seven examined effects of stretching after physical activity.
The 10 studies produced very consistent findings. They showed there was minimal or no effect on the muscle soreness experienced
between half a day and three days after the physical activity. Effects of stretching on effect on other outcomes such as injury and
performance were not examined in this review.
B A C K G R O U N D
Many people stretch before or after (or before and after) engaging
in athletic activity. Usually the purpose is to reduce the risk of
injury, reduce soreness after exercise, or enhance athletic perfor-
mance (Cross 1999; de Vries 1961; Gleim 1990; Gleim 1997).
This review focuses on the effects of muscle stretching on muscle
soreness. Another Cochrane review (Yeung 2003) has examined
whether stretching prevents injury, and several non-Cochrane sys-
tematic reviews have examined whether stretching prevents mus-
cle soreness or injury, or enhances performance (Herbert 2002;
Shrier 2004; Thacker 2004; Weldon 2003).
The muscle soreness that is the focus of this review is sometimes
called delayed-onset muscle soreness to differentiate it from sore-
ness that occurs as muscle fatigue, or immediately after muscles
have been fatigued. Delayed-onset muscle soreness (hereafter re-
ferred to simply as muscle soreness) is usually caused by unaccus-
tomed exercise, particularly exercise that requires primarily eccen-
tric muscle contraction. Eccentric contractions occur when the
muscle lengthens as it contracts. Typically the soreness arises within
the first day after exercise and peaks in intensity at around 48
hours (Balnave 1993; Bobbert 1986; Wessel 1994). The soreness
is usually associated with tenderness and may be associated with
swelling (Bobbert 1986; Wessel 1994).
The series of events that ultimately cause muscle soreness are only
partly understood. The initial event is probably mechanical disrup-
tion of sarcomeres (contractile units within muscle fibres; Proske
2001). This causes swelling of damaged muscle fibres and initiates
an inflammatory response, which could excite nociceptors (recep-
tors capable of transmitting information about pain; Lieber 2002).
2Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Muscle soreness is usually only experienced when the muscle con-
tracts or is stretched. This indicates that, while swelling of muscle
fibres and inflammation may be necessary for muscle soreness to
occur, swelling and inflammation are not sufficient to cause sore-
ness on their own. Muscle soreness is exacerbated by vibration over
the belly of the muscle, and pressure thresholds increase when large
diameter afferents are blocked (large diameter afferents are nerve
cells that conduct information about touch and limb position),
indicating that excitation of large diameter muscle afferents, prob-
ably primary spindle afferents from stretch receptors in muscles,
is involved in generating the sensation of soreness (Weerakkody
2001).
The practice of stretching to prevent muscle soreness was encour-
aged by early investigators of muscle soreness who thought that
unaccustomed exercise caused muscle spasm (de Vries 1961). Mus-
cle spasm was believed to impede blood flow to the muscle, caus-
ing ischaemic pain and further spasm. Stretching the muscle was
thought to restore blood flow to the muscle and interrupt the pain-
spasm-pain cycle. The muscle spasm theory of muscle soreness has
since been discredited (Bobbert 1986), but the practice of stretch-
ing persists.
Typically people who stretch to prevent muscle soreness do so prior
to exercise, but some people stretch after exercise. Usually each at-
risk muscle is stretched for between 15 seconds and 2 minutes,
once or several times. Some proponents of stretching recommend
applying a sustained stretch to the relaxed muscle (de Vries 1961;
this is called static stretching), but others recommend more elabo-
rate techniques such as the ’contract-relax-agonist contract’ tech-
nique (Feland 2001). This technique and related techniques (col-
lectively called proprioceptive neuromuscular facilitation (PNF)
techniques) involve contracting the muscle strongly before apply-
ing a stretch.
O B J E C T I V E S
This review aims to determine the effect of stretching before or
after exercise on the development of post-exercise muscle soreness.
M E T H O D S
Criteria for considering studies for this review
Types of studies
We considered any randomised or quasi-randomised (method of
allocating participants to a treatment that is not strictly random
e.g. by date of birth, hospital record number and alternation)
clinical trials of pre-or post-exercise stretching techniques designed
to prevent or treat delayed-onset muscle soreness.
Types of participants
Trials involving participants of any age group, and of either sex.
Types of interventions
Any pre-or post-exercise stretching technique designed to prevent
or treat delayed-onset muscle soreness, provided the stretching was
conducted soon before or soon after exercise of any type.
Types of outcome measures
Measures of muscle soreness (pain) or tenderness (pain on palpa-
tion of the muscle).
Search methods for identification of studies
We searched the Cochrane Bone, Joint and Muscle Trauma Group
Specialised Register (12 April 2006), the Cochrane Central Reg-
ister of Controlled Trials (The Cochrane Library 2006, Issue 2)
(see Appendix 1), MEDLINE (OVID WEB; 1966 to 16 May
2006), EMBASE (OVID WEB; 1988 to 16 May 2006), CINAHL
(OVID WEB; 1982 to 16 May 2006), SPORTDiscus (OVID
WEB; 1949 to 16 May 2006), PEDro - Physiotherapy Evidence
Database (www.pedro.fhs.usyd.edu.au/accessed 16 May 2006)
and reference lists of articles.
In MEDLINE (OVID WEB) the subject-specific search in
Appendix 2 was used. As it was anticipated that only a small
number of references would be identified, the results were not
combined with a trial search strategy. This strategy was modified
slightly for use in the other OVID databases.
In PEDro, two searches were conducted (see Appendix 3).
Data collection and analysis
Selection of trials
The two authors screened search results for potentially eligible
studies. When titles and abstracts suggested a study was potentially
eligible for inclusion a paper copy of the report was obtained. Dis-
agreements between the two people regarding a study’s eligibility
were resolved by discussion or, where necessary, by a third person.
Assessment of methodological quality
The methodological quality of the studies was assessed using the
Cochrane Bone, Joint and Muscle Trauma Group quality assess-
ment tool (Table 1). Two people independently assessed study
quality in this way. Disagreements were resolved by discussion.
Where necessary, a third person was consulted. It was anticipated
that several of the included studies would be laboratory-based stud-
ies which were unlikely to describe elements thought important
3Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

in clinical trials. These studies may appear methodologically weak
when assessed with a tool designed for clinical trials. Nonetheless
it was thought useful to document the degree to which they con-
form with best practice clinical trial design.
Table 1. Bone, Joint and Muscle Trauma Group methodological quality assessment tool
Item Criterion
A Was the assigned treatment adequately concealed prior to allocation?
2 = clearly yes (method did not allow disclosure of assignment).
1 = not sure (small but possible chance of disclosure of assignment or unclear).
0 = clearly no (quasi-randomised or open list/tables).
B Were the outcomes of patients/participants who withdrew described and included in the analysis (intention to treat)?
2 = withdrawals well described and accounted for in analysis.
1 = withdrawals described and analysis not possible.
0 = no mention, inadequate mention, or obvious differences and no adjustment.
C Were the outcome assessors blinded to treatment status?
2 = effective action taken to blind assessors.
1 = small or moderate chance of unblinding of assessors.
0 = not mentioned or not possible.
D Were the treatment and control group comparable at entry?
2 = good comparability of groups, or confounding adjusted for in analysis.
1 = confounding small; mentioned but not adjusted for.
0 = large potential for confounding, or not discussed.
E Were the participants blind to assignment status after allocation?
2 = effective action taken to blind participants.
1 = small or moderate chance of unblinding of participants.
0 = not possible, or not mentioned (unless double-blind), or possible but not done.
F Were the treatment providers blind to assignment status?
2 = effective action taken to blind treatment providers.
1 = small or moderate chance of unblinding of treatment providers.
0 = not possible, or not mentioned (unless double-blind), or possible but not done.
G Were care programmes, other than the trial options, identical?
2 = care programmes clearly identical.
1 = clear but trivial differences.
0 = not mentioned or clear and important differences in care programmes.
H Were the inclusion and exclusion criteria clearly defined?
2 = clearly defined.
1 = inadequately defined.
0 = not defined.
4Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Bone, Joint and Muscle Trauma Group methodological quality assessment tool (Continued)
I Were the interventions clearly defined? (This item was optional)
2 = clearly defined interventions are applied with a standardised protocol.
1 = clearly defined interventions are applied but the application protocol is not standardised.
0 = intervention and/or application protocol are poorly or not defined.
J Were the outcome measures used clearly defined? (by outcome)
2 = clearly defined.
1 = inadequately defined.
0 = not defined.
K Were diagnostic tests used in outcome assessment clinically useful? (by outcome)
2 = optimal.
1 = adequate.
0 = not defined, not adequate.
L Was the surveillance active, and of clinically appropriate duration?
2 = active surveillance and appropriate duration.
1 = active surveillance, but inadequate duration.
0 = surveillance not active or not defined.
Data extraction
Soreness or tenderness data from stretch and comparison groups
were extracted from study reports using a pro forma. This was
done by the authors; again, disagreements were resolved by dis-
cussion or a third person. It was expected that some studies would
report soreness data and some would report tenderness data. Some
studies reported raw scores, whereas others report change scores
or covariance-adjusted scores. It was also expected that outcomes
would usually be measured at a series of times following exercise.
Where available, data were extracted for each of a series of 12-hour
intervals following exercise (6-17 hours, 18-29 hours, 30-41 hours,
etc). Only one outcome was recorded from each study for each
time. Where multiple outcomes were available, soreness data was
preferred to tenderness data. Covariate-adjusted data were most
preferred, then change scores, then raw scores. Where within-sub-
ject studies (studies in which participants’ limbs were allocated to
stretch and control conditions) or cross-over studies (studies in
which each participant was sequentially exposed to both stretch
and control conditions) did not provide estimates of the variance
of differences between conditions or of the correlations between
outcomes under the two conditions being compared (Elbourne
2002) the variance of the difference between conditions was esti-
mated by assuming the data were independent.
Analysis
Pain and tenderness data were typically reported on 100 mm visual
analogue scales or 10 point scales. To facilitate pooling, data were
converted to a common 100-point scale. The effect of stretch-
ing was estimated from each study using the difference between
mean pain levels in stretch and comparison groups. Where there
was apparent qualitative homogeneity in participants, interven-
tions and outcome measures, meta-analysis was considered. Meta-
analysis was conducted using the RevMan Analysis program in
Review Manager (RevMan 2003). The effects of stretching was
described as a weighted mean difference. Data were inspected for
statistical heterogeneity. As there was no evidence of heterogeneity
of effect (Cochran Q, P < 0.1; Fleiss 1993), a fixed-effect model
was used to pool findings across studies. Effects of pre- and post-
exercise stretching were initially estimated separately but, as there
was no evidence of heterogeneity, they were combined in a sec-
ondary analysis. A post-hoc analysis was conducted to obtain sepa-
rate estimates from laboratory-based studies and the one commu-
nity-based study. An additional post-hoc analysis was conducted
to obtain separate estimates from studies of static stretch and the
one study that used another method of stretching.
R E S U L T S
5Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
The search retrieved 25 potentially eligible studies of which 10
were included (Buroker 1989; Dawson 2005; Gulick 1996; High
1989; Johansson 1999; Maxwell 1988; McGlynn 1979; Terry
1985; Wessel 1994a; Wessel 1994b). The titles or abstracts of a
further four papers appeared potentially eligible but could not be
retrieved (Costa 1997; Buckenmeyer 1998; Lin 1999; Lu 1992)
and still await assessment.
Included studies
Participants of all included studies were young healthy adults (age
less than 40 years or mean age less than 26 years); no studies in-
vestigated effects of stretching on muscle soreness in children or
middle-aged or older adults. All but one of the studies were car-
ried out in laboratory settings and involved standardised exercise.
The exception (Dawson 2005) investigated the effect of post-game
stretching on muscle soreness in Australian rules football players.
Three studies examined the effect of stretching before exercise (
High 1989; Johansson 1999; Wessel 1994a); the remaining seven
studies investigated the effects of stretching after exercise. The
stretch was of the knee extensor muscles (Buroker 1989; High
1989; Maxwell 1988; Terry 1985), hamstring muscles (Johansson
1999; Wessel 1994a; Wessel 1994b), ankle plantarflexor muscles (
Buroker 1989), wrist extensor muscles (Gulick 1996), elbow flexor
muscles (McGlynn 1979), or “legs and back” muscles (Dawson
2005). All but one of the studies examined the effects of static
stretching; one study examined the effects of a PNF technique
(“hold-relax”; Terry 1985). Two studies, both of stretching after
exercise, involved repeated stretching sessions (Buroker 1989: 12
sessions; McGlynn 1979: 5 sessions). The duration of stretching
applied in a single session ranged from 40 seconds (Terry 1985)
to 600 seconds (Gulick 1996), with a median of 390 seconds.
In six studies (Buroker 1989; Dawson 2005; Gulick 1996; High
1989; Maxwell 1988; McGlynn 1979) participants were randomly
allocated to stretch and control conditions. One of these (Dawson
2005) was a cross-over study in which each subject experienced
both the stretch and control conditions. The remaining four stud-
ies (Johansson 1999; Terry 1985; Wessel 1994a; Wessel 1994b)
stratified by participant and randomised legs to stretch and con-
trol conditions. Thus five studies (the single cross-over study and
the four studies that compared right and left legs) provided paired
comparisons. In all but two of these sufficient data were supplied
to take account of the paired nature of the data. In the studies
by Wessell and Wan (Wessel 1994a; Wessel 1994b) the estimates
from an analysis which accounted for the paired nature of the data
were less precise (Wessel 1994a) or had similar precision (Wessel
1994b) to estimates obtained by ignoring the paired nature of the
data, so the data were treated as if they were independent. Data
from the other two studies (Dawson 2005; Johansson 1999) were
treated as independent. See ’Characteristics of included studies’
for further details.
One study (Gulick 1996) reported only pooled data from all
groups and another (Maxwell 1988) did not provide any data
that could be used to calculate precison. (Both studies concluded
stretching had no effect.) Consequently these studies did not con-
tribute to the meta-analysis.
Excluded studies
Eleven studies were excluded (see ’Characteristics of excluded stud-
ies’).
Risk of bias in included studies
Table 2 summarises the methodological quality assessments. The
reviewers were not always able to agree on how particular items
were rated; these items are marked as “No consensus” in Table
2. All included studies were apparently randomised. None of the
studies described if the allocation schedule was concealed. There
was no blinding in any studies: this is because it is difficult or
impossible in studies of stretching to blind the person supervising
the stretching exercises and the person doing the stretches and, as
the outcome (soreness) must be self-reported, the assessor cannot
be blinded. None of the studies clearly indicated that analysis was
by intention to treat and in one study (Dawson 2005) analysis
was explicitly not by intention to treat. Only one study explicitly
reported completeness of follow up (Dawson 2005 reported data
were available for 31 of 34 player-conditions), although two fur-
ther studies (High 1989; Terry 1985) provided data that implied
follow up was complete. It is likely that follow up was complete
or nearly complete in most or all studies because the follow-up
period was very short (three days or less) and outcome measures
were not onerous.
Table 2. Quality of trials. Rows correspond to those in Table 01
Buroker
1989
Dawson
2005
Gulick
1996
High
1989
Johansson
1999
Maxwell
1988
McGlynn
1979
Terry
1985
Wessel
1994a
Wessel
1994b
1 0 1 1 1 1 1 1 1 1
6Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Quality of trials. Rows correspond to those in Table 01 (Continued)
0 0 0 0 No
consensus
0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 2 0 0 0 0 0 0 2 2
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0
2 2 2 2 2 2 2 2 2 2
2 0 No
consensus
1 2 0 2 2 0 0
2 1 2 2 2 2 2 2 2 2
2 2 2 2 2 2 2 2 2 2
2 2 2 2 2 2 2 2 2 2
2 2 2 2 2 2 2 2 2 2
Effects of interventions
One study (Gulick 1996) reported only pooled data from all
groups and another (Maxwell 1988) did not provide any data that
could be used to calculate precision. Consequently these studies
did not contribute to the meta-analysis. (Both studies concluded
stretching had no effect.) The following results are based on data
from the remaining studies.
The mean effects of stretching reported in individual studies were
too small to be of clinical relevance. There was a remarkable de-
gree of consistency (homogeneity) of results across studies (I2 for
all pooled estimates was 0%). The pooled estimate was that pre-
exercise stretching reduced soreness one day after exercise by, on
average, 0.5 points on a 100-point scale (95% CI -11.3 to 10.3; 3
studies; Analysis 01.02). Post-exercise stretching reduced soreness
one day after exercise by, on average, 1.0 points on a 100-point
scale (95% CI -6.9 to 4.8; 4 studies; Analysis 02.02). Similar ef-
fects were evident between half a day and three days after exercise.
As there was no sign of statistical heterogeneity we pooled the pre-
exercise and post-exercise studies. The pooled estimates are that
pre- and post-exercise stretching reduces soreness, on average, by
0.9 points on a 100-point scale at one day (95% CI -6.1 to 4.2; 7
studies; Analysis 03.02), increases soreness by 1.0 points on a 100-
point scale at two days (95% CI -4.1 to 6.2; 7 studies; Analysis
03.04) and decreases soreness by 0.3 points on a 100-point scale
at three days (95% CI -6.8 to 6.2; 5 studies; Analysis 03.06).
Similar estimates of effects were obtained in the only study that
tested PNF stretching. Terry 1985 showed the effect of PNF
stretching was to reduce soreness by 1.1 points on a 100-point
scale at both one and two days after exercise (95% CIs of -13.0
to 10.8; and -13.3 to 11.1 respectively). Also similar effects were
obtained in the one study of stretching after sport. Dawson 2005
showed that stretching increased muscle soreness by 3.0 points on
a 100-point scale (95% CI -7.1 to 13.1) at 15 hours and by 4.0
points (95% CI -5.2 to 13.2) at 48 hours after an Australian rule
football match.
D I S C U S S I O N
The evidence from randomised studies indicates that stretching
soon before or soon after exercise does not lessen muscle soreness
on subsequent days.
7Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

This conclusion is based on studies that rate poorly on conven-
tional scales of study quality. None of the reviewed studies explic-
itly concealed allocation, none were blinded, and none explicitly
analysed by intention to treat. Nonetheless there are some reasons
to believe that the findings may not be seriously biased: First, there
is a high degree of consistency across studies in estimates of the
effect of stretching. Also, biases due to non-concealment, lack of
blinding and failure to analyse by intention to treat typically pro-
duce exaggerated effects (Chalmers 1983; Colditz 1989; Moher
1998; Schulz 1995), yet this review found consistent evidence of
near-zero effects. The high degree of consistency of estimates across
studies suggests that alternative weightings (based, for example,
on different approaches to estimating precision from studies that
used within-subject designs) would produce very similar pooled
estimates of effects.
All but one of the eligible studies were laboratory-based stud-
ies. These studies assessed whether supervised stretching reduced
the soreness produced by standardised exercise involving eccen-
tric contractions of a particular muscle group. Such studies can be
considered to have an “explanatory” orientation because they tell
us about what the effects of stretching could be when adminis-
tered under ideal conditions. It might have been expected that the
effects of stretching would be smaller in community settings. In
community settings, unlike the laboratory settings of these stud-
ies, stretching is not usually supervised, so it may be carried out
sub-optimally. Also, the everyday experience of muscle soreness
may be of soreness in many muscle groups, and it may be diffi-
cult to effectively stretch all of the muscle groups that might be-
come sore. These considerations suggest the effects of stretching
might be smaller in community settings than in laboratory set-
tings. However the estimates from nine laboratory-based studies
and one community-based study suggest there are similar (near-
zero) effects in both settings.
The practice of stretching before or after exercise may have been
arisen because of the mistaken belief, prevalent in the 1960s and
1970s, that muscle soreness was due to muscle spasm (de Vries
1961). This view has since been discredited (Bobbert 1986). Con-
temporary beliefs about the mechanisms of muscle soreness do
not suggest any means by which stretching before or after exercise
could reduce the soreness that follows that exercise session. How-
ever if, as has been proposed, muscle soreness is due to excessive
elongation of some sarcomeres within muscle fibres (Proske 2001),
it is conceivable that any intervention which increased the num-
ber of sarcomeres in series in muscle fibres, or which increased the
length or compliance of tendons, could reduce sarcomere strains
and lessen muscle damage associated with unaccustomed eccentric
muscle contractions. This suggests the possibility that stretching
may be more effective for people who have very short muscles, or
if the stretching is repeated for weeks or months or years. To date,
however, randomised trials have only examined the short-term ef-
fects of one or a few sessions of stretching, and no randomised
trials have specifically investigated interactions between effects of
stretching and flexibility.
The best available evidence indicates stretching does not reduce
muscle soreness. However there are other justifications for stretch-
ing. Some evidence suggests that once muscle soreness has devel-
oped stretching may provide a transient relief of soreness (Reisman
2005): some people stretch to reduce risk of injury, others stretch
to enhance athletic or sporting performance, and yet others stretch
because it gives them a sense of well-being. The current review
does not provide any evidence of an effect or otherwise of stretch-
ing on risk of injury, performance or well-being.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
The available evidence from randomised trials carried out mainly
in laboratory settings consistently suggests that stretching before
or after exercise does not prevent muscle soreness in young healthy
adults.
Implications for research
Arguably the findings of this review are clear enough that further
research into the effects of stretching on muscle soreness is not
necessary. We see some merit in this view. However, in our opinion
it would be useful to conduct further trials of the effects of longer-
term stretching programs, in community-based populations and
for people with reduced flexibility.
A C K N O W L E D G E M E N T S
This review is based on an earlier “non-Cochrane” review con-
ducted by Rob Herbert and Michael Gabriel and published in
2002 (Herbert RD, Gabriel M. BMJ 2002;325(7362):468-72).
Through that earlier work Michael Gabriel indirectly contributed
to the current review. His contribution is gratefully acknowledged.
The authors thank Helen Handoll, Vicki Livingstone, Janet Wale,
Gisela Sole and Lindsey Shaw for helpful comments on the review,
and Lisa Harvey for assistance with data extraction.
8Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Buroker 1989 {published data only}
Buroker KC, Schwane JA. Does postexercise static stretching
alleviate delayed muscle soreness?. Physician and Sportsmedicine1989;17(6):65–83.
Dawson 2005 {published data only}
Dawson B, Gow S, Modra S, Bishop D, Stewart G. Effects of
immediate post-game recovery procedures on muscle soreness,
power and flexibility levels over the next 48 hours. Journal ofScience and Medicine in Sport 2005;8(2):210–21.
Gulick 1996 {published data only}
Gulick DT, Kimura IF, Sitler M, Paolone A, Kelly JD. Various
treatment techniques on signs and symptoms of delayed onset
muscle soreness. Journal of Athletic Training 1996;31(2):145–52.
High 1989 {published data only}
High DM, Howley ET, Franks BD. The effects of static stretching
and warm-up on prevention of delayed-onset muscle soreness.
Research Quarterly for Exercise and Sport 1989;60(4):357–61.
Johansson 1999 {published data only}
Johansson PH, Lindström L, Sundelin G, Lindström B. The effects
of preexercise stretching on muscular soreness, tenderness and force
loss following heavy eccentric exercise. Scandinavian Journal ofMedicine and Science in Sports 1999;9(4):219–25.
Maxwell 1988 {published data only}
Maxwell S, Kohn S, Watson A, Balnave RJ. Is stretching effective in
the prevention of or amelioration of delayed-onset muscle soreness?.
In: Torode M editor(s). The athlete maximising participation and
minimising risk. Sydney: Cumberland College of Health Sciences,
1988:109–18.
McGlynn 1979 {published data only}
McGlynn GH, Laughlin NT, Rowe V. Effect of electromyographic
feedback and static stretching on artificially induced muscle
soreness. American Journal of Physical Medicine 1979;58(3):139–48.
Terry 1985 {published data only}∗ Terry L. Stretching and muscle soreness. An investigation into the
effects of hold-relax stretch on delayed post-exercise soreness in thequadriceps muscle - a pilot study [thesis]. Adelaide (Australia): South
Australian Institute of Technology, 1985.
Terry L. Stretching and muscle soreness: an investigation into the
effects of a hold-relax stretch on delayed post-exercise soreness in
the quadriceps muscle: a pilot study [abstract]. Australian Journal of
Physiotherapy Australian Journal of Physiotherapy 1987;33(1):69.
Wessel 1994a {published data only}
Wessel J, Wan A. Effect of stretching on the intensity of delayed-
onset muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):
83–7.
Wessel 1994b {published data only}
Wessel J, Wan A. Effect of stretching on the intensity of delayed-
onset muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):
83–7.
References to studies excluded from this review
Abraham 1977 {published data only}
Abraham WM. Factors in delayed muscle soreness. Medicine and
Science in Sports 1997;9(1):11–20.
Bale 1991 {published data only}
Bale P, James H. Massage, warmdown and rest as recuperative
measures after short term intense exercise. Physiotherapy in Sport1991;13(2):4–7.
de Vries 1966 {published data only}
de Vries HA. Quantitative electromyographic investigation of the
spasm theory of muscle pain. American Journal of Physical Medicine1966;45(3):119–34.
Jayaraman 2004 {published data only}
Jayaraman RC, Reid RW, Foley JM, Prior BM, Dudley GA,
Weingand KW, et al.MRI evaluation of topical heat and static
stretching as therapeutic modalities for the treatment of eccentric
exercise-induced muscle damage. European Journal of AppliedPhysiology 2004;93(1-2):30–8.
Lightfoot 1997 {published data only}
Lightfoot JT, Char D, McDermott J, Goya C. Immediate
postexercise massage does not attenuate delayed onset muscle
soreness. Journal of Strength and Conditioning Research 1997;11:
119–24.
Lund 1998 {published data only}
Lund H, Vestergaard-Poulsen, Kanstrup I-L, Sejrsen P. The effect of
passive stretching on delayed onset muscle soreness, and other
detrimental effects following exercise. Scandinavian Journal of
Medicine and Science in Sports 1998;8:216–21.
Prentice 1982 {published data only}
Prentice WE. Electromyographic analysis of the effectiveness of
heat or cold and stretching for inducing relaxation in injured
muscle. Journal of Orthopaedic and Sports Physical Therapy 1982;3
(3):133–40.
Rahnama 2005 {published data only}
Rahnama N. Rahmani-Nia F. Ebrahim K. The isolated and
combined effects of selected physical activity and ibuprofen on
delayed-onset muscle soreness. Journal of Sports Sciences 2005;23
(8):843–850.
Reilly 2002 {published data only}
Reilly T, Rigby M. Effect of an active warm-down following
competitive soccer. In: Spinks W, Reilly T, Murphy A editor(s).
Science and Football IV. Proceedings of the 4th World Congress ofScience and Football; 1999 Feb 22-26; Sydney, NSW. London:
Routledge, 2002:226–9.
Rodenburg 1994 {published data only}
Rodenburg JB, Steenbeek, Schiereck P, Bar PR. Warm-up,
stretching and massage diminish harmful effects of eccentric
exercise. International Journal of Sports Medicine 1994;15(7):414–9.
Smith 1993 {published data only}
Smith LL, Brunetz MH, Chenier TC, McCammon MR, Houmard
JA, Franklin ME, et al.The effects of static and ballistic stretching
on delayed onset muscle soreness. Research Quarterly for Exercise
and Sport 1993;1:103–7.
9Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

References to studies awaiting assessment
Buckenmeyer 1998 {published data only}
Buckenmeyer P, Kokkinidis E. Machairidou M, Tsamourtas A. The
effect of static stretching and cryotherapy on the recovery of
delayed muscle soreness [Greek]. Exercise & Society Journal of SportScience (Komotini) 1998;(19):45–53.
Costa 1997 {published data only}
Costa MC, Cabral JG, Muniz GMA, Silva EF, Silva MG, Duarte
JAR, et al.Effects of stretching after exercise on some indirect
markers muscle damage. 9th European Congress on Sports
Medicine; 1997 Sept 23-26; Porto, Portugal. 1997:1.
Lin 1999 {published data only}
Lin WH. The effects of massage, stretch and meloxicam on delayed
onset muscle soreness [Masters thesis]. Taiwan: National College of
Physical Education and Sports Taoyuan, 1999.
Lu 1992 {published data only}∗ Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of
the effect of acupuncture and static stretch on contractile structural
alteration of skeletal muscle after strenuous exercise. Sport Science(Beijing) 1992;12(6):47–51.
Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of the
effect of acupuncture and static stretch on ultrastructural alteration
of M-line of skeletal muscle after strenuous exercise. Sports Science(Beijing) 1992;12(6):52–9.
Lu D, Fan JY, Qu Z. An immuno-electron microscopic study of the
effect of acupuncture and static stretch on ultrastructural alteration
of Z-band in human skeletal muscle after strenuous exercise. SportsScience (Beijing) 1992;12(6):60–5.
Additional references
Balnave 1993
Balnave CD, Thomson MW. Effect of training on eccentric
exercise-induced muscle damage. Journal of Applied Physiology
1993;75(4):1545–51.
Bobbert 1986
Bobbert MF, Hollander AP, Huijing PA. Factors in delayed onset
muscle sorenesss of man. Medicine and Science in Sports and Exercise1986;18(1):75–81.
Chalmers 1983
Chalmers TC, Celano P, Sacks HS, Smith H. Bias in treatment
assignment in controlled clinical trials. New England Journal ofMedicine 1983;309(22):1358–61.
Colditz 1989
Colditz GA, Miller JN, Mosteller F. How study design affects
outcomes in comparisons of therapy. I: Medical. Statistics in
Medicine 1989;8(4):441–54.
Cross 1999
Cross KM, Worrell TW. Effects of a static stretching program on
the incidence of lower extremity musculotendinous strains. Journalof Athletic Training 1999;34:11–4.
de Vries 1961
de Vries HA. Prevention of muscular distress after exercise. ResearchQuarterly 1961;32:177–85.
Elbourne 2002
Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington
HV, Vail A. Meta-analyses involving cross-over trials:
methodological issues. International Journal of Epidemiology 2002;
31(1):140–9.
Feland 2001
Feland JB, Myrer JW, Merrill RM. Acute changes in hamstring
flexibility: PNF versus static stretch in senior athletes. PhysicalTherapy in Sport 2001;2(4):186–93.
Fleiss 1993
Fleiss JL. The statistical basis of meta-analysis. Statistical Methods inMedical Research 1993;2:121–45.
Gleim 1990
Gleim GW, Stachenfeld NS, Nicholas JA. The influence of
flexibility on the economy of walking and jogging. Journal ofOrthopedic Research 1990;8:814–23.
Gleim 1997
Gleim GW, McHugh MP. Flexibility and its effects on sports injury
and performance. Sports Medicine 1997;24:289–99.
Lieber 2002
Lieber RL, Friden J. Morphologic and mechanical basis of delayed-
onset muscle soreness. Journal of the American Academy ofOrthopaedic Surgeons 2002;10(1):67–73.
Moher 1998
Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et
al.Does quality of reports of randomised trials affect estimates of
intervention efficacy reported in meta-analyses?. Lancet 1995;352
(9128):609–13.
Proske 2001
Proske U, Morgan DL. Muscle damage from eccentric exercise:
mechanism, mechanical signs, adaptation and clinical applications.
Journal of Physiology 2001;537(2):333–45.
Reisman 2005
Reisman S, Walsh LD, Proske U. Warm-up stretches reduce
sensations of stiffness and soreness after eccentric exercise. Medicineand Science in Sports and Exercise 2005;37(6):929–36.
RevMan 2003
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 4.2 for Windows. Copenhagen: The
Nordic Cochrane Centre, The Cochrane Collaboration, 2003.
Schulz 1995
Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence
of bias. Dimensions of methodological quality associated with
estimates of treatment effects in controlled trials. JAMA 1995;273
(5):408–12.
Shrier 2004
Shrier I. Does stretching improve performance?A systematic and
critical review of the literature. Clinical Journal of Sport Medicine2004;14(5):267–73.
Thacker 2004
Thacker SB, Gilchrist J, Stroup DF, Kimsey CD. The impact of
stretching on sports injury risk: a systematic review of the literature.
Medicine and Science in Sports and Exercise 2004;36(3):371–8.
10Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Weerakkody 2001
Weerakkody NS, Whitehead NP, Canny BJ, Gregory JE, Proske U.
Large-fibre mechanoreceptors contribute to muscle soreness after
eccentric exercise. Journal of Pain 2001;2(4):209–19.
Weldon 2003
Weldon SM, Hill RH. The efficacy of stretching for prevention of
exercise-related injury: a systematic review of the literature. Manual
Therapy 2003;8(3):141–50.
Wessel 1994
Wessel J, Wan A. Effect of stretching on the intensity of delayed-
onset muscle soreness. Clinical Journal of Sport Medicine 1994;4(2):
82–7.
Yeung 2003
Yeung EW, Yeung SS. Interventions for preventing lower limb soft-
tissue injuries in runners. Cochrane Database of Systematic Reviews2003, Issue 4. [DOI: 10.1002/14651858.CD001256]
References to other published versions of this review
Herbert 2002
Herbert RD, Gabriel M. Effects of pre- and post-exercise stretching
on muscle soreness, risk of injury and athletic performance: a
systematic review. BMJ 2002;325(7362):468–72.∗ Indicates the major publication for the study
11Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Buroker 1989
Methods Randomised (between subjects) design
Participants 23 participants (16 men and 7 women) aged 18-33 years with no known contraindications to exercise.
None was highly physically trained and none were extremely active in the six weeks preceding the study.
Interventions Control group (N = 8): no stretching.
One stretch group 1 (N = 7): stretched left knee extensors after exercise.
A second stretch group (N = 8): stretched left knee extensors and right plantarflexors after exercise.
Stretches (10 30-second static stretches, each separated by 10 seconds rest, to noticeable tension or slight
discomfort)were performed at 2-hour intervals for the first 24 hours and 4-hour intervals for the following
48 hours except that participants were allowed to sleep for 8 hours each night.
Outcomes The following measures were taken on days 1, 2 and 3:
1. Soreness on a 0-6 scale (0 = no pain, light pain only on palpation, 4 = moderate pain, stiffness and/or
weakness, especially on movement, 6 = severe pain limiting range of movement)
2. Force required to invoke tenderness (sum of measures at 9 sites)
3. Force required to invoke tenderness (highest value from 9 or 10 sites)
Notes Data from the two stretch groups were pooled.
Stretched after exercise.
Soreness induced with 20 minutes of step-down exercise.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Dawson 2005
Methods Randomised (within subjects, cross-over)design
Participants 17 semi-professional Australian rules football players.
Interventions Stretch condition: 15 minutes of supervised gentle stretching of the legs and back. This involved “2-3
repeats of 30 s held stretches across several muscle groups and joints”.
Control condition: no recovery procedures.
Outcomes The following measures were taken at 15 and 48 hours:
1. Soreness (“how do you feel today?”) measured on a 1-7 scale anchored at “very, very good” and “very,
very sore”.
12Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dawson 2005 (Continued)
Notes Part of a larger study in which each subject was exposed on 12 occasions, each separated by one week, to
one of four interventions (control, stretch, pool walking, hot-cold regimen).
Initial condition was allocated randomly and subsequent conditions by alternation. Stretch was before
exercise.
Soreness was induced by playing football.
All participants underwent a “pool recovery program” on the two days following exercise.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Gulick 1996
Methods Randomised (between subjects) design
Participants ~22 untrained participants randomly drawn from a larger sample of 35 men and 38 women aged 21 to
40 years.
Interventions Stretch group (N ~ 11): static stretches of the wrist extensor muscles to “end range” for 10 minutes soon
after exercise.
Control group (N ~ 11): two placebo tablets after exercise and one further placebo tablet 24 hours later.
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:
1. On a 10 cm visual analogue scale anchored at “no soreness at all” and “soreness as bad as it could be”
2. Force required to invoke tenderness (sum of measures at 9 sites).
Notes Part of a larger study in which subjects were randomised to seven interventions (control, stretch, anti-
inflammatory drug, intense exercise, ice massage, herbal ointment).
Stretch was after exercise.
Soreness was induced by 15 sets of 15 isokinetic eccentric wrist extensor contractions.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
High 1989
Methods Randomised (between subjects) design
Participants 30 untrained participants (stretch group, 7 men and 7 women, mean age 19.4 years; control group, 8
men and 8 women, mean age 20.4 years)
13Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

High 1989 (Continued)
Interventions Stretch group: stretched the quadriceps muscles (5 stretches, twice each on each leg for 50 seconds) of
both legs prior to exercise. Control group: did not stretch.
Outcomes The following measures were taken at 24 hour intervals for 5 days:
1. Soreness on a 0-6 scale (0 = “absence of soreness”, 6 = “most severe pain possible from soreness”.
Notes Part of a larger study in which subjects were randomised to four interventions (control, stretch, warm-up,
warm-up and stretch).
Stretch was before exercise.
Soreness was induced by 80 up to minutes of step-down exercise.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Johansson 1999
Methods Randomised (between legs) design
Participants 10 health female physiotherapy students (24 (SD 3) years, 62 (SD 3) kg, 169 (SD 5) cm), not taking anti-
inflammatory medication, with no lower limb musculoskeletal symptoms, had not participated in weight
training for more than 3 hours per week, and were not experiencing DOMS at the time of testing.
Interventions Stretch leg: four 20-second “hamstring hurdle” stretches, with 20 second rests between stretches. Stretch
intensity was sufficient to induce a strong feeling of stretch but not pain.
Control leg: the hamstring muscles on the other side of the body were not stretched.
Outcomes The following measures were taken 24, 48 and 96 hours after exercise:
1. Hamstring muscle soreness on a 100 mm visual analogue scale (0 = “no soreness”, 100 = “worst possible
soreness”).
2. Tenderness measured with an algometer at 5 locations.
Notes Stretch was before exercise.
Soreness was induced with 10 sets of 10 isokinetic knee flexor contractions.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
14Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Maxwell 1988
Methods Randomised (between subjects) design
Participants ~14 female first-year college students randomly drawn from a larger sample of 20 participants aged 18-
25 years (mean 19.4) and with varying histories of physical activity
Interventions Stretch group (N ~ 6): participants lay in prone with the hips in a neutral position. A static stretch was
applied to the quadriceps to the point of discomfort and held for 15 seconds.
Control group (N ~ 6): participants did not stretch.
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:
1. Pain experienced in the quadriceps muscle whilst descending a flight of stairs rated on a 10 cm visual
analogue scale anchored at 0 (“no pain”) and 10 (“severe pain”).
Notes Stretch was after exercise.
Soreness was induced with 15 minutes of step-down exercise.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
McGlynn 1979
Methods Randomised (between subjects) design
Participants 24 men aged 18-26 years who had not engaged in any systematic activity with their non-dominant arms
in the past 30 days
Interventions Stretch group (N ~ 12): participants “hyperextended” the “forearm” for two minutes before releasing the
stretch for one minute. This sequence was repeated four times each at 6, 25, 30, 49 and 54 hours after
exercise.
Control group (N ~12): participants did not stretch.
Outcomes The following measures were taken 24, 48 and 72 hours after exercise:
1. Pain rated on a 30-point scale, where 0-10 was “mild” pain, 11-20 was “moderate” pain, and 21-30
was “severe” pain.
Notes Part of a larger study in which subjects were randomised to three interventions (control, stretch, biofeed-
back).
Strech was after exercise.
Soreness was induced with eccentric elbow flexor exercises perfomed to failure.
Risk of bias
Item Authors’ judgement Description
15Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

McGlynn 1979 (Continued)
Allocation concealment? Unclear B - Unclear
Terry 1985
Methods Randomised (between legs) design
Participants 30 healthy participants, 15 men and 15 women, aged between 18 and 35 years. The modal level of exercise
was three times per week.
Interventions Stretch (hold-relax)leg: participants lay prone with a wedge under the thigh and the knee was actively
flexed as far as possible. Then the participant performed an isometric contraction against manual resistance
for 4-6 seconds. This was followed by two seconds of relaxation and then an 8 second passive stretch. This
was repeated 5 times.
Control leg: the other leg was not stretched.
Outcomes The following measures were taken on days 2 and 3:
1. “Pain” (or, variably, “pain, soreness or stiffness” or “soreness”)experienced that day during functional
movements rated on a scale of 0 (“no pain”) to 7 (“unbearably painful”).
Notes Stretching was after exercise.
Soreness was induced with 20 minutes of step-up and step-down exercise.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Wessel 1994a
Methods Randomised (between legs) design
Participants 10 sedentary adults (5 women and 5 men) with no history of back or lower limb injury or disease, mean
age 24.2 (SD 5.37), mean height 175.5 cm (SD 7.6) and mean mass 66.3 kg (8.9)
Interventions Stretch leg: ten 60-second stretches of the hamstring muscles prior to exercise.
Control leg: not stretched.
Outcomes The following measures were taken at 12 hour intervals to 72 hours after exercise:
1. Pain on a 10 cm visual analogue scale while walking on an “even” surface.
Notes Randomisation was by toss of a coin.
Stretching was before exercise.
Soreness was induced by 3 sets of 20 isokinetic eccentric knee flexor contractions.
Risk of bias
16Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wessel 1994a (Continued)
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Wessel 1994b
Methods Randomised (between legs) design
Participants 10 sedentary adults (2 women and 8 men) with no history of back or lower limb injury or disease, mean
age 25.2 (SD 3.36), mean height 171.2 cm (SD 7.29) and mean mass 61.3 kg (7.12)
Interventions Stretch leg: ten 60-second stretches of the hamstring muscles after exercise.
Control leg: not stretched.
Outcomes The following measures were taken at 12 hour intervals to 72 hours after exercise:
1. Pain on a 10 cm visual analogue scale while walking on an “even” surface.
Notes Randomisation was by toss of a coin.
Stretching was after exercise.
Soreness was induced by 3 sets of 20 isokinetic eccentric knee flexor contractions.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
DOMS: delayed onset muscle soreness
s: second
SD: standard deviation
~: approximately
The numbers of participants given in the Participants and Interventions columns are the number of participants who received the
stretch or control intervention. Thus, in studies with three or more arms the number of participants given is less than the total number
of participants in the study. In Gulick 1996, 73 participants were randomised to 7 groups but the size of each group is not given, so
sample sizes are given as “~11”. In Maxwell 1988, 20 participants were randomised to 3 groups but the size of each group is not given,
so sample sizes are given as “~6”. In McGlynn 1979, 36 participants were randomised to 3 groups but the size of each group is not
given, so sample sizes are given as “~12”.
17Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of excluded studies [ordered by study ID]
Abraham 1977 Stretching occurred 24 hours after exercise; not clear if conditions (stretch/flex) were randomised.
Bale 1991 No stretch condition.
de Vries 1966 Not randomised (compared before and after stretch).
Jayaraman 2004 Stretching did not begin until 36 hours after exercise.
Lightfoot 1997 Plantarflexors were sore, but quadriceps and hamstring muscles were stretched (fails criterion of “stretching
technique designed to prevent or treat delayed-onset muscle soreness”).
Lund 1998 Not randomised (used historical controls).
Prentice 1982 Stretch combined with heat or cold; interventions 24 hours after exercise; did not measure soreness.
Rahnama 2005 Stretching combined with jogging and walking and submaximal concentric contractions.
Reilly 2002 Not clearly randomised; stretch combined with jogging and “shake-down”.
Rodenburg 1994 Intervention was a combination of warm-up, stretch and massage.
Smith 1993 Compares effects of static and ballistic stretching.
18Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Pre-exercise stretching
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Soreness on day 0.5 (assessed 6-
17 hours post-exercise)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 Soreness on day 1 (assessed 18-
29 hours post-exercise)
3 70 Mean Difference (IV, Fixed, 95% CI) -0.52 [-11.30,
10.26]
3 Soreness on day 1.5 (assessed 30-
41 hours post-exercise)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
4 Soreness on day 2 (assessed 42-
53 hours post-exercise)
2 40 Mean Difference (IV, Fixed, 95% CI) 0.72 [-11.20, 12.64]
5 Soreness on day 2.5 (assessed 54-
65 hours post-exercise)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
6 Soreness on day 3 (assessed 66-
77 hours post-exercise)
2 40 Mean Difference (IV, Fixed, 95% CI) -2.50 [-15.82,
10.82]
Comparison 2. Post-exercise stretching
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Soreness on day 0.5 (assessed 6-
17 hours post-exercise)
2 51 Mean Difference (IV, Fixed, 95% CI) -0.47 [-6.05, 5.12]
2 Soreness on day 1 (assessed 18-
29 hours post-exercise)
4 127 Mean Difference (IV, Fixed, 95% CI) -1.04 [-6.88, 4.79]
3 Soreness on day 1.5 (assessed 30-
41 hours post-exercise)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
4 Soreness on day 2 (assessed 42-
53 hours post-exercise)
5 158 Mean Difference (IV, Fixed, 95% CI) 1.12 [-4.63, 6.87]
5 Soreness on day 2.5 (assessed 54-
65 hours post-exercise)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
6 Soreness on day 3 (assessed 66-
77 hours post-exercise)
3 67 Mean Difference (IV, Fixed, 95% CI) -0.03 [-7.49, 7.43]
19Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 3. Either pre- or post-exercise stretching
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Soreness on day 0.5 (assessed 6-
17 hours post-exercise)
3 71 Mean Difference (IV, Fixed, 95% CI) -0.97 [-6.24, 4.29]
2 Soreness on day 1 (assessed 18-
29 hours post-exercise)
7 197 Mean Difference (IV, Fixed, 95% CI) -0.93 [-6.05, 4.20]
3 Soreness on day 1.5 (assessed 30-
41 hours post-exercise)
2 40 Mean Difference (IV, Fixed, 95% CI) 1.0 [-14.37, 16.37]
4 Soreness on day 2 (assessed 42-
53 hours post-exercise)
7 198 Mean Difference (IV, Fixed, 95% CI) 1.04 [-4.14, 6.22]
5 Soreness on day 2.5 (assessed 54-
65 hours post-exercise)
2 40 Mean Difference (IV, Fixed, 95% CI) -0.75 [-13.25,
11.76]
6 Soreness on day 3 (assessed 66-
77 hours post-exercise)
5 107 Mean Difference (IV, Fixed, 95% CI) -0.28 [-6.79, 6.22]
Analysis 1.1. Comparison 1 Pre-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 4 (5) 10 9 (25) -5.00 [ -20.80, 10.80 ]
-100 -50 0 50 100
Favours stretch Favours control
20Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 Pre-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
High 1989 14 63.2 (37.5) 16 66.9 (37.5) 16.1 % -3.70 [ -30.60, 23.20 ]
Johansson 1999 10 52.2 (15.5) 10 51 (15.8) 61.7 % 1.20 [ -12.52, 14.92 ]
Wessel 1994a 10 14 (24) 10 17 (28) 22.2 % -3.00 [ -25.86, 19.86 ]
Total (95% CI) 34 36 100.0 % -0.52 [ -11.30, 10.26 ]
Heterogeneity: Chi2 = 0.16, df = 2 (P = 0.92); I2 =0.0%
Test for overall effect: Z = 0.09 (P = 0.92)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 1.3. Comparison 1 Pre-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 27 (30) 10 26 (28) 1.00 [ -24.43, 26.43 ]
-100 -50 0 50 100
Favours stretch Favours control
21Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 Pre-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Johansson 1999 10 70.5 (16.6) 10 69.4 (17.1) 65.1 % 1.10 [ -13.67, 15.87 ]
Wessel 1994a 10 32 (24) 10 32 (22) 34.9 % 0.0 [ -20.18, 20.18 ]
Total (95% CI) 20 20 100.0 % 0.72 [ -11.20, 12.64 ]
Heterogeneity: Chi2 = 0.01, df = 1 (P = 0.93); I2 =0.0%
Test for overall effect: Z = 0.12 (P = 0.91)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 1.5. Comparison 1 Pre-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 27 (19) 10 29 (27) -2.00 [ -22.46, 18.46 ]
-100 -50 0 50 100
Favours stretch Favours control
22Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 Pre-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 1 Pre-exercise stretching
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Johansson 1999 10 39.4 (23.8) 10 38.2 (24.1) 40.3 % 1.20 [ -19.79, 22.19 ]
Wessel 1994a 10 13 (17) 10 18 (22) 59.7 % -5.00 [ -22.23, 12.23 ]
Total (95% CI) 20 20 100.0 % -2.50 [ -15.82, 10.82 ]
Heterogeneity: Chi2 = 0.20, df = 1 (P = 0.65); I2 =0.0%
Test for overall effect: Z = 0.37 (P = 0.71)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 2.1. Comparison 2 Post-exercise stretching, Outcome 1 Soreness on day 0.5 (assessed 6-17 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Dawson 2005 14 60 (17) 17 57 (10) 30.6 % 3.00 [ -7.09, 13.09 ]
Wessel 1994b 10 4 (6) 10 6 (9) 69.4 % -2.00 [ -8.70, 4.70 ]
Total (95% CI) 24 27 100.0 % -0.47 [ -6.05, 5.12 ]
Heterogeneity: Chi2 = 0.65, df = 1 (P = 0.42); I2 =0.0%
Test for overall effect: Z = 0.16 (P = 0.87)
-100 -50 0 50 100
Favours stretch Favours control
23Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Post-exercise stretching, Outcome 2 Soreness on day 1 (assessed 18-29 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 61.7 (15.1) 8 64 (5.9) 45.3 % -2.30 [ -10.97, 6.37 ]
McGlynn 1979 12 29.4 (20) 12 27.5 (19.5) 13.6 % 1.90 [ -13.90, 17.70 ]
Terry 1985 30 23.6 (23.6) 30 24.7 (23.6) 23.8 % -1.10 [ -13.04, 10.84 ]
Wessel 1994b 10 13 (16) 10 13 (16) 17.3 % 0.0 [ -14.02, 14.02 ]
Total (95% CI) 67 60 100.0 % -1.04 [ -6.88, 4.79 ]
Heterogeneity: Chi2 = 0.24, df = 3 (P = 0.97); I2 =0.0%
Test for overall effect: Z = 0.35 (P = 0.73)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 2.3. Comparison 2 Post-exercise stretching, Outcome 3 Soreness on day 1.5 (assessed 30-41 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994b 10 22 (22) 10 21 (22) 1.00 [ -18.28, 20.28 ]
-100 -50 0 50 100
Favours stretch Favours control
24Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.4. Comparison 2 Post-exercise stretching, Outcome 4 Soreness on day 2 (assessed 42-53 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 65.2 (23.1) 8 68.5 (13.7) 14.6 % -3.30 [ -18.36, 11.76 ]
Dawson 2005 14 52 (15) 17 48 (10) 39.2 % 4.00 [ -5.18, 13.18 ]
McGlynn 1979 12 29.4 (20) 12 27.2 (20.4) 12.7 % 2.20 [ -13.96, 18.36 ]
Terry 1985 30 23.3 (24) 30 24.4 (24) 22.4 % -1.10 [ -13.25, 11.05 ]
Wessel 1994b 10 26 (22) 10 26 (17) 11.1 % 0.0 [ -17.23, 17.23 ]
Total (95% CI) 81 77 100.0 % 1.12 [ -4.63, 6.87 ]
Heterogeneity: Chi2 = 0.87, df = 4 (P = 0.93); I2 =0.0%
Test for overall effect: Z = 0.38 (P = 0.70)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 2.5. Comparison 2 Post-exercise stretching, Outcome 5 Soreness on day 2.5 (assessed 54-65 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994b 10 24 (19) 10 24 (17) 0.0 [ -15.80, 15.80 ]
-100 -50 0 50 100
Favours stretch Favours control
25Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.6. Comparison 2 Post-exercise stretching, Outcome 6 Soreness on day 3 (assessed 66-77 hours
post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 2 Post-exercise stretching
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 51.8 (20.2) 8 50.3 (26.5) 12.6 % 1.50 [ -19.52, 22.52 ]
McGlynn 1979 12 11.4 (9.9) 12 11.4 (13) 65.1 % 0.0 [ -9.25, 9.25 ]
Wessel 1994b 10 17 (17) 10 18 (19) 22.3 % -1.00 [ -16.80, 14.80 ]
Total (95% CI) 37 30 100.0 % -0.03 [ -7.49, 7.43 ]
Heterogeneity: Chi2 = 0.03, df = 2 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 0.01 (P = 0.99)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 3.1. Comparison 3 Either pre- or post-exercise stretching, Outcome 1 Soreness on day 0.5
(assessed 6-17 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 1 Soreness on day 0.5 (assessed 6-17 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 4 (5) 10 9 (25) 11.1 % -5.00 [ -20.80, 10.80 ]
Dawson 2005 14 60 (17) 17 57 (10) 27.2 % 3.00 [ -7.09, 13.09 ]
Wessel 1994b 10 4 (6) 10 6 (9) 61.7 % -2.00 [ -8.70, 4.70 ]
Total (95% CI) 34 37 100.0 % -0.97 [ -6.24, 4.29 ]
Heterogeneity: Chi2 = 0.93, df = 2 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 0.36 (P = 0.72)
-100 -50 0 50 100
Favours stretch Favours control
26Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Either pre- or post-exercise stretching, Outcome 2 Soreness on day 1 (assessed
18-29 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 2 Soreness on day 1 (assessed 18-29 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 61.7 (15.1) 8 64 (5.9) 35.0 % -2.30 [ -10.97, 6.37 ]
High 1989 14 63.2 (37.5) 16 66.9 (37.5) 3.6 % -3.70 [ -30.60, 23.20 ]
Johansson 1999 10 52.2 (15.5) 10 51 (15.8) 14.0 % 1.20 [ -12.52, 14.92 ]
McGlynn 1979 12 29.4 (20) 12 27.5 (19.5) 10.5 % 1.90 [ -13.90, 17.70 ]
Terry 1985 30 23.6 (23.6) 30 24.7 (23.6) 18.4 % -1.10 [ -13.04, 10.84 ]
Wessel 1994a 10 14 (24) 10 17 (28) 5.0 % -3.00 [ -25.86, 19.86 ]
Wessel 1994b 10 13 (16) 10 13 (16) 13.4 % 0.0 [ -14.02, 14.02 ]
Total (95% CI) 101 96 100.0 % -0.93 [ -6.05, 4.20 ]
Heterogeneity: Chi2 = 0.40, df = 6 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.35 (P = 0.72)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 3.3. Comparison 3 Either pre- or post-exercise stretching, Outcome 3 Soreness on day 1.5
(assessed 30-41 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 3 Soreness on day 1.5 (assessed 30-41 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 27 (30) 10 26 (28) 36.5 % 1.00 [ -24.43, 26.43 ]
Wessel 1994b 10 22 (22) 10 21 (22) 63.5 % 1.00 [ -18.28, 20.28 ]
Total (95% CI) 20 20 100.0 % 1.00 [ -14.37, 16.37 ]
Heterogeneity: Chi2 = 0.0, df = 1 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.13 (P = 0.90)
-100 -50 0 50 100
Favours stretch Favours control
27Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.4. Comparison 3 Either pre- or post-exercise stretching, Outcome 4 Soreness on day 2 (assessed
42-53 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 4 Soreness on day 2 (assessed 42-53 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 65.2 (23.1) 8 68.5 (13.7) 11.8 % -3.30 [ -18.36, 11.76 ]
Johansson 1999 10 70.5 (16.6) 10 69.4 (17.1) 12.3 % 1.10 [ -13.67, 15.87 ]
Dawson 2005 14 52 (15) 17 48 (10) 31.8 % 4.00 [ -5.18, 13.18 ]
McGlynn 1979 12 29.4 (20) 12 27.2 (20.4) 10.3 % 2.20 [ -13.96, 18.36 ]
Terry 1985 30 23.3 (24) 30 24.4 (24) 18.2 % -1.10 [ -13.25, 11.05 ]
Wessel 1994a 10 32 (24) 10 32 (22) 6.6 % 0.0 [ -20.18, 20.18 ]
Wessel 1994b 10 26 (22) 10 26 (17) 9.0 % 0.0 [ -17.23, 17.23 ]
Total (95% CI) 101 97 100.0 % 1.04 [ -4.14, 6.22 ]
Heterogeneity: Chi2 = 0.88, df = 6 (P = 0.99); I2 =0.0%
Test for overall effect: Z = 0.39 (P = 0.69)
-100 -50 0 50 100
Favours stretch Favours control
28Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.5. Comparison 3 Either pre- or post-exercise stretching, Outcome 5 Soreness on day 2.5
(assessed 54-65 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 5 Soreness on day 2.5 (assessed 54-65 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Wessel 1994a 10 27 (19) 10 29 (27) 37.4 % -2.00 [ -22.46, 18.46 ]
Wessel 1994b 10 24 (19) 10 24 (17) 62.6 % 0.0 [ -15.80, 15.80 ]
Total (95% CI) 20 20 100.0 % -0.75 [ -13.25, 11.76 ]
Heterogeneity: Chi2 = 0.02, df = 1 (P = 0.88); I2 =0.0%
Test for overall effect: Z = 0.12 (P = 0.91)
-100 -50 0 50 100
Favours stretch Favours control
Analysis 3.6. Comparison 3 Either pre- or post-exercise stretching, Outcome 6 Soreness on day 3 (assessed
66-77 hours post-exercise).
Review: Stretching to prevent or reduce muscle soreness after exercise
Comparison: 3 Either pre- or post-exercise stretching
Outcome: 6 Soreness on day 3 (assessed 66-77 hours post-exercise)
Study or subgroup Stretch Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Buroker 1989 15 51.8 (20.2) 8 50.3 (26.5) 9.6 % 1.50 [ -19.52, 22.52 ]
Johansson 1999 10 39.4 (23.8) 10 38.2 (24.1) 9.6 % 1.20 [ -19.79, 22.19 ]
McGlynn 1979 12 11.4 (9.9) 12 11.4 (13) 49.6 % 0.0 [ -9.25, 9.25 ]
Wessel 1994a 10 13 (17) 10 18 (22) 14.3 % -5.00 [ -22.23, 12.23 ]
Wessel 1994b 10 18 (19) 10 17 (17) 17.0 % 1.00 [ -14.80, 16.80 ]
Total (95% CI) 57 50 100.0 % -0.28 [ -6.79, 6.22 ]
Heterogeneity: Chi2 = 0.36, df = 4 (P = 0.99); I2 =0.0%
Test for overall effect: Z = 0.09 (P = 0.93)
-100 -50 0 50 100
Favours stretch Favours control
29Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A P P E N D I C E S
Appendix 1. Search strategy for The Cochrane Library
#1. stretch*
#2. flexib*
#3. PLIABILITY single term (MeSH)
#4. (range near motion)
#5. (((((warmup or warm-up) or (warm next down)) or cooldown) or cool-down) or (cool next down))
#6. ((((#1 or #2) or #3) or #4) or #5)
#7. (sore* near musc*)
#8. doms
#9. MUSCLE CONTRACTION explode all trees (MeSH)
#10. MUSCLE SKELETAL single term (MeSH)
#11. (#9 or #10)
#12. PAIN single term (MeSH)
#13. (#11 and #12)
#14. (#7 or #8 or #13)
#15. (#6 and #14)
Appendix 2. Search strategy for MEDLINE (OVID WEB)
1. stretch$.tw.
2. flexib$.tw.
3. Pliability/
4. (range adj3 motion).tw.
5. Range of Motion, Articular/
6. (warmup or warm-up or warm up or cooldown or cool-down or cool down).tw.
7. or/1-6
8. (sore$ adj3 musc$).tw.
9. DOMS.tw.
10. exp Muscle Contraction/
11. Muscle, Skeletal/
12. or/10-11
13. Pain/
14. and/12-13
15. or/8-9,14
16. and/7,15
Appendix 3. Search strategy for PEDro
The first search combined the following terms with “OR”:
[in the Title/abstract field] stretch*, sore*, DOMS
The second search combined the following terms with “AND”:
[in the Therapy field] stretching, mobilisation, manipulation, massage
[in the Subdiscipline field] sports
[in the Problem field] pain
30Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

W H A T ’ S N E W
Last assessed as up-to-date: 15 August 2006.
4 July 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 1, 2004
Review first published: Issue 4, 2007
C O N T R I B U T I O N S O F A U T H O R S
The protocol for the current review was written by Rob Herbert. Data collection, data extraction, quality assessment, data analysis
and interpretation were carried out by Marcos de Noronha and Rob Herbert. Rob Herbert wrote the review. Marcos de Noronha
commented on drafts and approved the final version. Rob Herbert is guarantor for the review.
D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
Internal sources
• University of Sydney, Australia.
External sources
• No sources of support supplied
I N D E X T E R M S
31Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Medical Subject Headings (MeSH)
∗Exercise; Muscle Stretching Exercises; Muscular Diseases [∗prevention & control]; Pain [∗prevention & control]; Randomized Con-
trolled Trials as Topic
MeSH check words
Humans
32Stretching to prevent or reduce muscle soreness after exercise (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.