Esiste una medicina di genere nel Parkinson? · Bradicinesia Tremore Rigidità Instabilità...
26
Esiste una medicina di genere nel Parkinson? MARTINA GIUNTINI U.O. NEUROLOGIA AZIENDA OSPEDALIERO-UNIVERSITARIA PISANA
Transcript of Esiste una medicina di genere nel Parkinson? · Bradicinesia Tremore Rigidità Instabilità...

Esiste una medicina di genere nel Parkinson?
MARTINA GIUNTINI U.O. NEUROLOGIA
AZIENDA OSPEDALIERO-UNIVERSITARIA PISANA

1
5 4 4 3
8 7 6 5
9
13 13 16
21
9
23 24
34
20
27
32
41
29
59
48 50
67
45
9
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
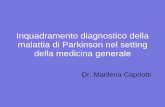
Gender difference Parkinson's Disease 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
J Neurol. 2017 Aug

•EPIDEMIOLOGIA
•SINTOMI MOTORI E NON MOTORI
•DISTURBI COGNITIVI
• IMPLICAZIONI E PROSPETTIVE FUTURE

Incidenza: Meta-analisi include > 2500 pazienti con MP da 17 studi
47 studi
(21 studi)
(4 studi)
(17 studi)

Studio nazionale francese: comprende 188.562 persone trattate per MP
Meta-analisi tra cui 22 studi che coinvolgono 7616 Uomini e 6510 donne con MP≥40 anni

Il contributo genetico nella MP è maggiore in età più
giovanile. Le forme genetiche
(non X-linked) hanno un'età di insorgenza più giovane
Il rischio di MP non genetico o i fattori protettivi sono
distribuiti in modo diverso negli uomini e nelle donne e il loro
ruolo aumenta con l'età.
Fattori di rischio: fattori chimici o
tossici
Fattori protettivi: estrogeni
MASCHI FEMMINE
Spiegazione possibile

Experimental Neurology 259 (2014) 44–56

•EPIDEMIOLOGIA
•SINTOMI MOTORI E NON MOTORI
•DISTURBI COGNITIVI
• IMPLICAZIONI E PROSPETTIVE FUTURE

Sintomi motori classici
Bradicinesia
Tremore
Rigidità
Instabilità posturale
MALATTIA DI PARKINSON: una patologia complessa
+
Sintomi non motori
Disfunzione autonomica
Disturbi gastrointestinali
Disturbi del sonno
Disturbi dell'umore
Difetto cognitivo
alcuni di questi sintomi spesso precedono le manifestazioni motorie della MP

COMPLESSO DEI SINTOMI NON MOTORI
Sintomi Neuropsichiatrici
Disturbi dell’umore
depressione, ansia, apatia
Psicosi
allucinazioni, deliri
Disturbi del comportamento
Impulsivo, ripetitivo
Disturbi cognitivi
deficit selettivi,
Demenza, Delirium
Disturbi del sonno
Restless Legs
Periodic Limb Movements
REM Sleep Behavior Disorder
Non-REM Sleep Mvt Disorders
Insonnia, EDS, Sogni vividi
OSAS
Sintomi autonomici
Urgenza vescicale, Nicturia,
Iperidrosi, scialorrea
Ipotensione ortostatica
Disfunzione sessuale
Dry eyes
Ageusia, disfagia, reflusso,
Stipsi, Incontinenza
Altri sintomi
Dolore, parestesie,
Iposmia
Fatigue
Seborrea
Visione annebbiata, Diplopia
Chaudhuri KR, Lancet Neurology, 2006

STORIA NATURALE DELLA MP
Postuma RB et al., Nat Rev Neurol 2016

COMPLICANZE MOTORIE DELLA MP

Oestrogen status
Several oestrogen status items were associated with age at
onset. Parity correlated positively with age at onset: the more
children a woman had before PD onset, the higher the age at
onset (2.7 years later onset per child; 95% CI 0.8 to 4.6;
p = 0.007) (fig 5A), the only exception being women without
children. These women may have a different basal oestrogen
status than women with children. Furthermore, in women with
an early PD onset, the choice to have (fewer) children might be
influenced by the burden of PD, thereby possibly inverting the
relationship between age at onset and parity. To control for this,
we repeated the analyses for the subgroup of women with
children (n = 67) and for the subgroup of women with an age
at onset > 40 years (n = 67) and found the same results.
Combining both selection criteria (n = 58) did not change theseresults. Age at menopause correlated with the age at onset
when taking those women with symptom onset after
menopause (0.5 years later onset per year; 95% CI 0.1 to 0.8;
p = 0.009). In these women, the duration of the fertile life spanwas associated with a 0.5 year later onset per year (95% CI 0.2
to 0.9; p = 0.001) (fig 5B). Without the selection based on theorder of menopause and symptom onset, the correlation of age
at menopause (p = 0.02) and of duration of the fertile life span(p = 0.05) with age at onset remained significant. Age at
menarche did not correlate with age at onset (p = 0.2). Noassociation was found for any of the oestrogen status items
with presenting symptom, sUPDRS-III or SPECT results.
DISCUSSIONSeveral findings in this study suggested a more benign PDphenotype in women compared with men. The benefits for
women seemed to apply mainly to the events preceding overtPD. Firstly, women tended to be older than men at symptom
onset. Secondly, women presented more often than men with atremor dominant form of PD, which in turn was associated
with a slower disease progression. Thirdly, at onset of the
disease, women had higher levels of striatal dopamine bindingthan men. These benefits in the preclinical phase could be
related to oestrogen status, because parity (number ofchildren), age at menopause and duration of the fertile life
span were all associated with a later age at onset of PD.However, women seemed to have no further advantage over
men once PD had become clinically manifest. Thus the rates ofdisease progression—as indexed by both clinical scores and
measurements of striatal dopamine binding—were comparablebetween men and women with overt symptoms. In the next
paragraphs, we discuss these findings in more detail.
Gender di f ferences preceding cl inical PD
The 2 year difference in age at PD onset between men andwomen observed here is comparable with the difference found
in most epidemiological studies.7 It suggests that the develop-ment of symptomatic PD is slightly delayed in women
compared with men. This could be explained by higher initialstriatal dopamine levels in women compared with men, asnoted in this study. Those higher initial dopamine levels could
delay the moment of reaching a critical threshold of striataldopamine depletion and hence postpone the development ofparkinsonian symptoms.
Several observations support this explanation. In our study,at symptom onset and throughout the course of the disease,
women had 16%higher striatal [ 123I]FP-CIT binding than men.This suggests that the critical threshold of dopamine depletion
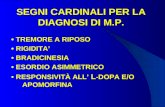
Figure 4 Mean striatal [123I]-FP-CITbinding. The lines show the estimateddecrease in mean tracer binding for men and women with age at onset of50 years. A higher age at onset was accompanied by lower initial striataltracer binding in both men and women. Women had 16%higher [123I]FP-CITbinding than men. The plotted observed values are those of all patientsin the study, irrespective of age at onset.
60
p = 0.007
A B
40
20
00 1 2 3 4
Ag
e a
t o
nse
t+1
SE (
yea
rs)
Ag
e a
t o
nse
t (y
ea
rs)
Parity
70
60
50
40
15 20 25 35 4530 40
Fertile life span (years)
Figure 5 Oestrogen status and age at onset. (A) The more children a woman had before the onset of Parkinson’s disease, the higher the age at onset. (B) Alonger fertile life span led to a higher age at onset: 0.5 year delay/ year.
822 Haaxma, Bloem, Borm, et al
www.jnnp.com
Le F hanno un uptake striatale più elevato
Questo fenotipo più benigno appare in relazione con lo stato estrogenico: età della menopausa, numero di figli, durata della vita fertile
253 MP de novo (156M / 97F)
• All’esordio le F sono 2.1 aa più anziane rispetto ai M
• Le F presentano più frequentemente un fenotipo tremorigeno
FENOTIPO CLINICO PIU’ BENIGNO

ETA’ ALL’ESORDIO COMPLICANZE MOTORIE:
• FLUTTUAZIONI MOTORIE
• DISCINESIE
GENERE

NMS valutati mediante NMS-Questionnaire (NMS-Q)
93 soggetti sani di controllo M/F:60/33
200 pazienti MP M/F:126/74
SINTOMI NON MOTORI

PD vs HC
M: MP vs Controlli Sani F: MP vs Controlli Sani
I SINTOMI NON MOTORI PRODROMICI DELLA MALATTIA
DI PARKINSON SEMBRANO SEGREGARE PIU’
FREQUENTEMENTE NEGLI UOMINI
93 soggetti sani di controllo M/F:60/33
200 pazienti MP M/F:126/74

• 47 PD (16F/31M) seguiti per 4 anni dalla diagnosi • Fluttuazioni non motorie valutate mediante WOQ-19
FLUTTUAZIONI NON MOTORIE MAGGIORI COMPLICANZE MOTORIE IN TERMINI
DI DISCINESIE
FLUTTUAZIONI SI PRESENTANO SPESSO CON
SINTOMI NON MOTORI NELLE DONNE CHE NON VENGONO INDAGATI

•EPIDEMIOLOGIA
•SINTOMI MOTORI E NON MOTORI
•DISTURBI COGNITIVI
• IMPLICAZIONI E PROSPETTIVE FUTURE

Pigott et al
• 55 (63% M) pazienti con MP cognitivamente intatti seguiti per 6 anni • Circa il 50% ha sviluppato deterioramento cognitivo entro la fine dello studio
Il genere maschile è un fattore di rischio per il deterioramento cognitivo nella MP

Il genere è un fattore di rischio età-dipendente per la demenza nella MP

•EPIDEMIOLOGIA
•SINTOMI MOTORI E NON MOTORI
•DISTURBI COGNITIVI
• IMPLICAZIONI E PROSPETTIVE FUTURE
• MIGLIOR IDENTIFICAZIONE DEI CASI PRODROMICI • MIGLIORAMENTO DELLE STRATEGIE TERAPEUTICHE

Liu et al
PPMI (Parkinson Progression Markers Initiative - PPMI) COORTE: 414 MP (269M/145F) e 188 controlli sani (121M/67F)

MASCHI
FEMMINE
Take-home message
Per essere efficaci, le strategie volte a differenziare la MP rispetto ai controlli sani in fase prodromica dovrebbero considerare il genere
Liu et al
PPMI (Parkinson Progression Markers Initiative - PPMI) COORTE: 414 MP (269M/145F) e 188 controlli sani (121M/67F)

Migliorare il management terapeutico
Il genere dovrebbe essere considerato per migliorare il trattamento su misura nei pazienti
con MP Differenze nel menagement medico
Differenze nell’approccio alla Deep Brain Stimulation surgery


J Neurol 2016
FENOTIPO CLINICO PIU’ BENIGNO?