Palermo assessment neuropsicologico della consapevolezza di malattia
Upload
nguyenthuyCategory
view
222download
0
Disturbi Cognitivi nella SM
Problemi e Soluzioni Maria Pia Amato
Maria Pia Amato
Centro SM, SOD Neurologia 1, AOU Careggi
Dipartimento NEUROFARBA, Sezione Neuroscienze
Università degli Studi di Firenze
Firenze, 13 Marzo 2015

Agenda
• Informazioni generali – Prevalenza
– Profilo neuropsicologico
– Impatto funzionale
– Informazioni dagli studi RM
• Approcci alla valutazione – Screening
– Brevi batterie
• Strategie di trattamento – Approcci farmacologici
– Riabilitazione cognitiva

• Dopo l’iniziale descrizione di Charcot, 1887, i DC sono stati
storicamente sottostimati e descritti nei vecchi testi come
–Relativamente rari
–Associati alle fasi più avanzate della malattia
“ [In] most of the patients
… there is marked
enfeeblement of the
memory;
conceptions are formed
slowly; the intellectual
and
emotional faculties are
blunted in their totality. “
• La risposta fornita ai pazienti con DC è oggi considerata un indicatore della qualità dell’assistenza fornita alle persone con SM (Cheng, 2010)
Paradigmi che cambiano
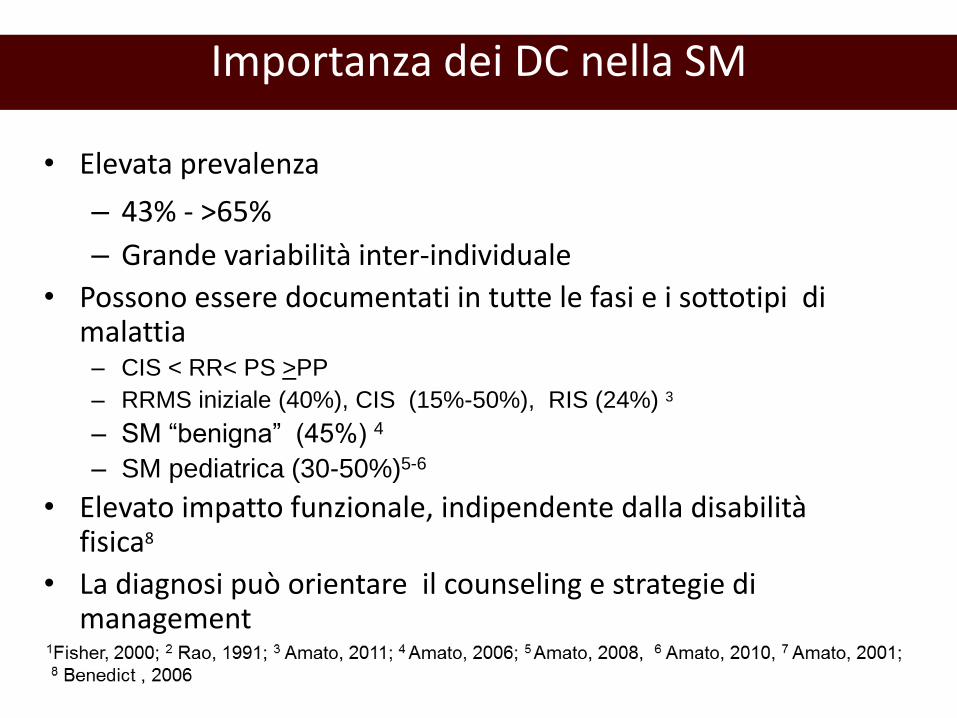
Importanza dei DC nella SM
• Elevata prevalenza
– 43% - >65% – Grande variabilità inter-individuale
• Possono essere documentati in tutte le fasi e i sottotipi di malattia – CIS < RR< PS >PP
– RRMS iniziale (40%), CIS (15%-50%), RIS (24%) 3
– SM “benigna” (45%) 4
– SM pediatrica (30-50%)5-6
• Elevato impatto funzionale, indipendente dalla disabilità fisica8
• La diagnosi può orientare il counseling e strategie di management
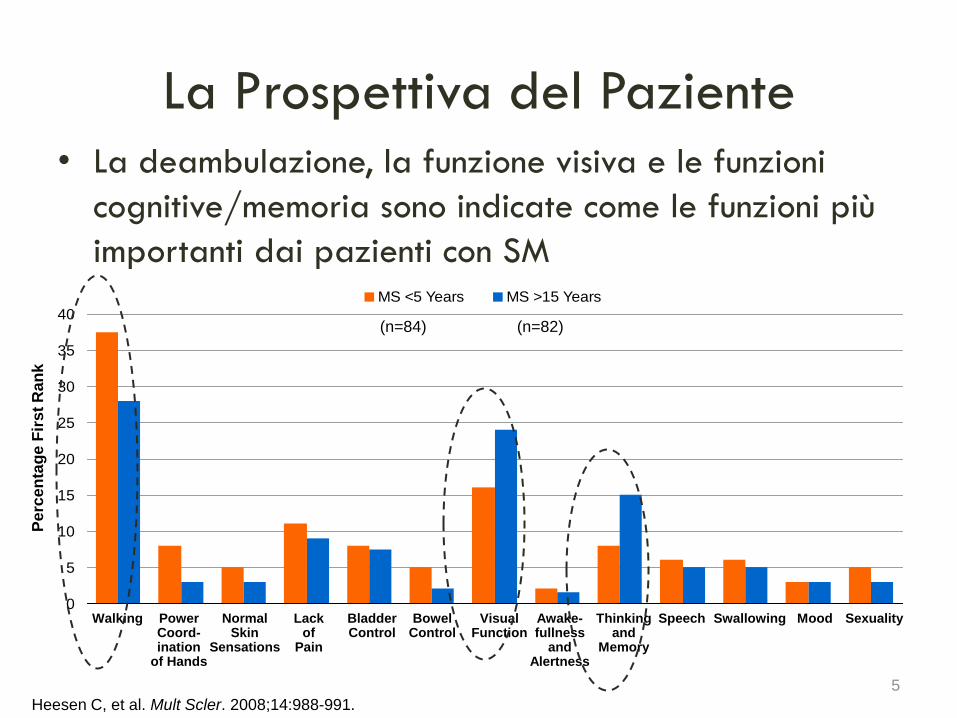
La Prospettiva del Paziente • La deambulazione, la funzione visiva e le funzioni
cognitive/memoria sono indicate come le funzioni più
importanti dai pazienti con SM
5
Heesen C, et al. Mult Scler. 2008;14:988-991.
0
5
10
15
20
25
30
35
40
MS <5 Years MS >15 Years
Pe
rce
nta
ge F
irs
t R
an
k
Walking Power Coord- ination
of Hands
Normal Skin
Sensations
Lack of
Pain
Bladder Control
Bowel Control
Visual Function
Awake- fullness
and Alertness
Thinking and
Memory
Speech Swallowing Mood Sexuality
(n=84) (n=82)
Profilo Neuropsicologico
• Velocità di elaborazione delle informazioni • “Memoria di lavoro” (“Working memory”) • Attenzione complessa (sostenuta, selettiva, divisa,
alternata) • Memoria a lungo termine: acquisizione e richiamo di
nuove informazioni • Funzioni esecutive ― Concettualizzazione astratta ― Soluzione di problemi ― Pianificazione ― Seguire contemporaneamente più compiti ― Fluenza verbale
Deficit focali: coinvolte selettivamente alcune funzioni cognitive

Inizio 4.5 aa. 10 aa.
Patients
Durata media malattia 1.6 aa.
EDSS media 1.9
No DC (0-2 subtest fallliti)
Lieve DC (3-5 subtest falliti)
Moderato DC (>5 subtest falliti)
Amato et al. Arch Neurol. 1995, 2001
DC 26% CI= 49% CI= 56%
Predittori di un esito cognitivo peggiore
• Età più avanzata
• EDSS più elevata
•Passaggio dalla fase RR allla fase SP
La frequenza dei DC tende a aumentare nel decorso della
malattia- Uno studio longitudinale in 10 anni 50 pazienti con diagnosi iniziale (non trattati) confrontati con 70 CS
DC 49% DC 56%

La frequenza dei DC tende a aumentare nel decorso della malattia
RIS, radiologically isolated syndrome; CIS, clinically isolated syndrome 1 Amato, Neurology 2012; 2 Potagas, J Neurol Sci 2008
1
%

-63 patients and 57 Controlli sani (CS)
-Al baseline, prevalenza di DC 31%, con impatto negativo sullo stile di vita e le
funzioni scolastiche
-Linguaggio coinvolto nel 30-40% dei casi
-IQ ridotto(<70) nel 6%, specie nei casi ad esordio più precoce
Nello studio a 5 anni, chiare possibilità di recupero, nell’ambito di grande
variabilità inter-individuale: circa il 50% mostra comunque un peggioramento

Individual changes in cognitive performance: year 0-5
56.3% dei bambini/adolescenti con SM presentano un peggioramento del CCI, a fronte di una relativa stabilità del punteggio EDSS Funzioni più soggette al deterioramento: -memoria visuo-spaziale -fluenza verbale -linguaggio espressivo Il DC era significativamente associato con: -esordio più precoce della SM -sesso maschile -scolarità più bassa
Amato et al, Neurology 2014

Impatto funzionale
• Comportamento
• Vita sociale
• Relazioni familiari
• Stress del CG
• Competenza in materie legali e
finanziarie
• Guida: > rischio incidenti
• Coping
• Aderenza ai trattamenti
• Capacità di beneficiare di
trattamenti riabilitativi
Un predittore dello stato
lavorativo (presente e
futuro) del soggetto
Studi trasversali
Rao et al. 1991
Beatty et al. 1995
Studi longitudinali
Amato et al. 2001
Morrow et al., 2010
Ruet et al., 2013
Un fattore prognostico
Costi indiretti di malattia

MRIV MTr DTI MRSI FMRI MRI-LV
Lesioni in T2 e T1 nella SB
Atrofia cerebrale
globale
Atrofia della SG
-neocorteccia
-ippocampo
-sottocorticale
(talamo)
Modificazini del tessuto cerebrale «apparentemente normale»
Fisiopatologia: Informazioni dagli studi RM
Lesioni nella SG
corticale
NCV (
cc3)
400
500
600
700
800
NC RR MS NC MS Preservati
-15
-10
-5
0
5
ZN
CV
MS deficit cogniitvo
Whole Groups
p=0.001
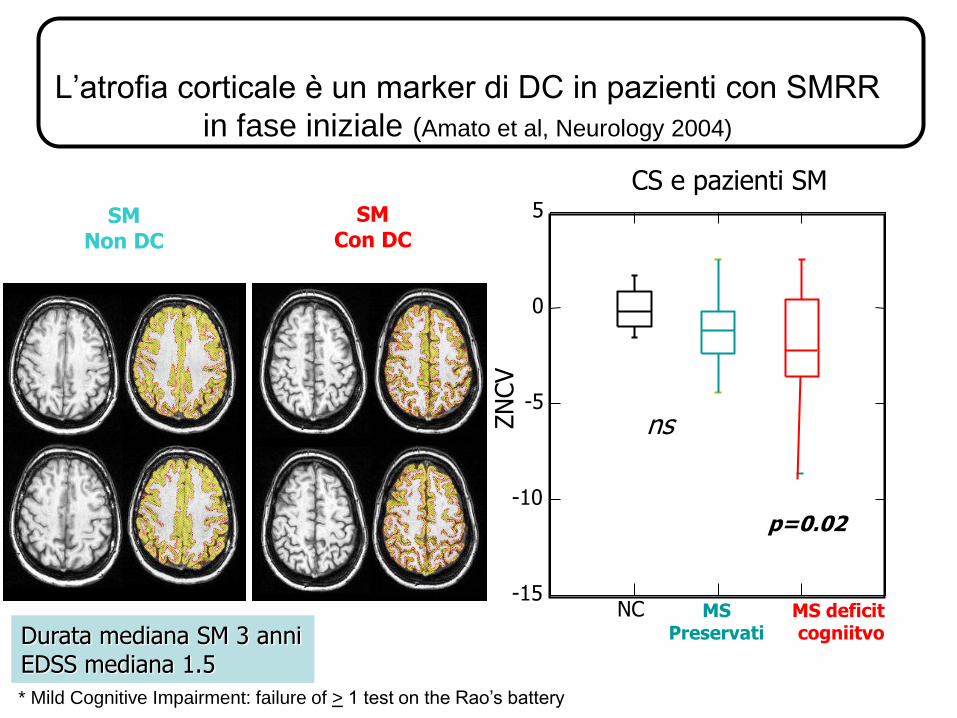
CS e pazienti SM
p=0.02
ns
Amato et al, Neurology 2004
SM Con DC
SM Non DC
L’atrofia corticale è un marker di DC in pazienti con SMRR
in fase iniziale (Amato et al, Neurology 2004)
Durata mediana SM 3 anni EDSS mediana 1.5
* Mild Cognitive Impairment: failure of > 1 test on the Rao’s battery

La disconnessione è un meccanismo importante ma correla solo in parte con il carico lesionale, confermando il ruolo del danno all sostanza bianca e grigia «apparentemente normali»

DTI e network strutturali nella SM
«connettomica»
Shu et al., Cereb Cortex 2011; Filippi et al., Lancet Neurol 2013
Ridotta efficienza dei network strutturali della SB

Pardini et al., JNNP, 2014
I DC possono persistere
a 6 e 12 mesi
• “RCI”, identificate da una riduzione dei punteggi al
test SDMT >4 punti, in assenza di nuovi segni/sintomi
neurologici, modificazioni della depressione e fatica
– associate a lesioni RM gd+ generalmente nei lobi fronto-parietali
Il ruolo dell’infiammazione
Ricadute Cognitive Isolate (RCI)

Il Paradosso Clinico-radiologico
• Nonostante correlazioni multi-parametriche la relazione
tra RM e DC resta sub-ottimale
• Grande variabilità inter-individuale
• Progressione lenta dei DC nonostante il danno cerebrale
progressivo
Capacità di compenso e «plasticità cerebrale»

CS
SM
Performance normale: compenso cerebrale attraverso il
reclutamento di aree supplementari normalmente
attivate dai soggetti sani
Performance ridotta: fallimento del reclutamento
(o pattern abnorme)
Sottogruppo SM
con performance
normale
Sottogruppo SM
con performance
ridotta
Compenso Cerebrale: fMRI e performance al test PASAT Mainero et al, Neuroimage 2004

• I pazienti con una maggiore efficienza cerebrale (RC) possono tollerare gradi più avanzati di danno cerebrale prima di presentare clinicamente DC. Y. Stern et al., (2005), Cereb. Cortex
• L’arricchimento intellettivo può associarsi con una maggiore efficienza cerebrale e fornire una “riserva conitiva (RC)” contro il DC.
Y. Stern, (2002), J. Int. Neuropsych. Soc.
L’ipotesi della “Riserva Cognitiva”
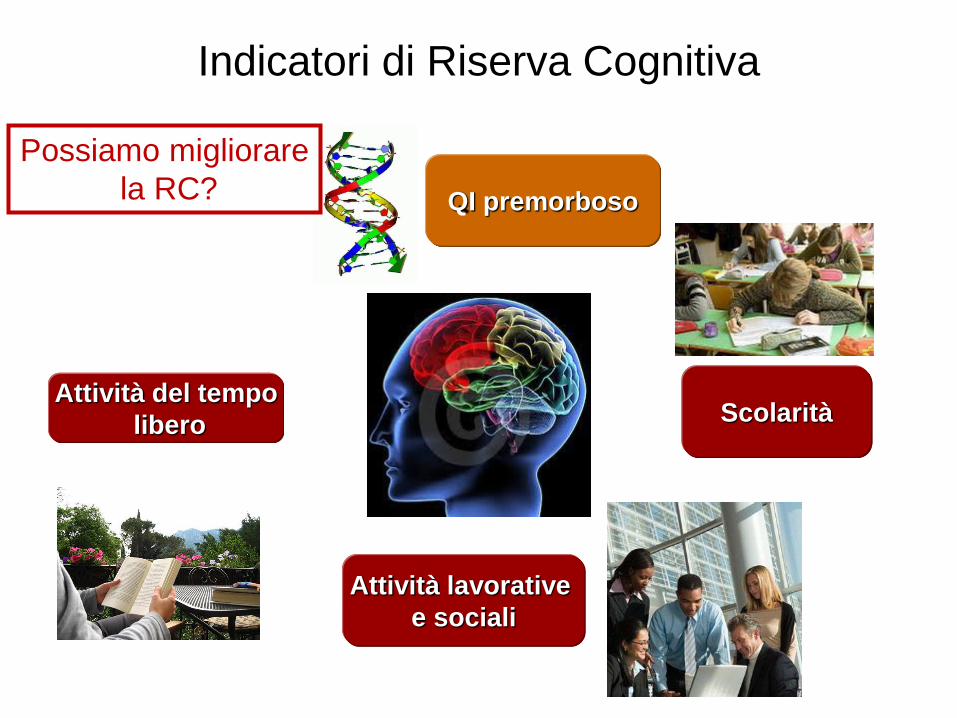
Indicatori di Riserva Cognitiva
Attività del tempo
libero
Scolarità
Attività lavorative
e sociali
QI premorboso
Possiamo migliorare
la RC?

Riserva Cognitiva nella SM
L’arricchimento intellettivo protegge i soggetti con
SM dal DC Sumowski et al., J. Clin. Exp. Neuropsyc. 2009
Sumowski et al., J. Int. Neuropsych. Soc. 2009
Sumowski et al., Neurology 2014 , 4.5 year follow-up
RC più alta
RC normale
RC più bassa

Riserva Cognitiva e Atrofia Cerebrale Progressiva (Amato et al, Neurology 2013)
52 paz. RR, valutazione NP sulla batteria di Rao
Follow-up 1.5 aa: l’età più avanzata e la progressione
dell’atrofia neocorticale si associvano con un
peggioramento del DC, indipendentemente dalla RC
la RC è un fattore protettivo ma solo entro certi
limiti di atrofia neocorticale:
Importanza del TRATTAMENTO PRECOCE:
Follow-up
assessment
NCV > 494 mm 3
Significant
relationship
NCV < 494: no
relationship with
cognitive performance
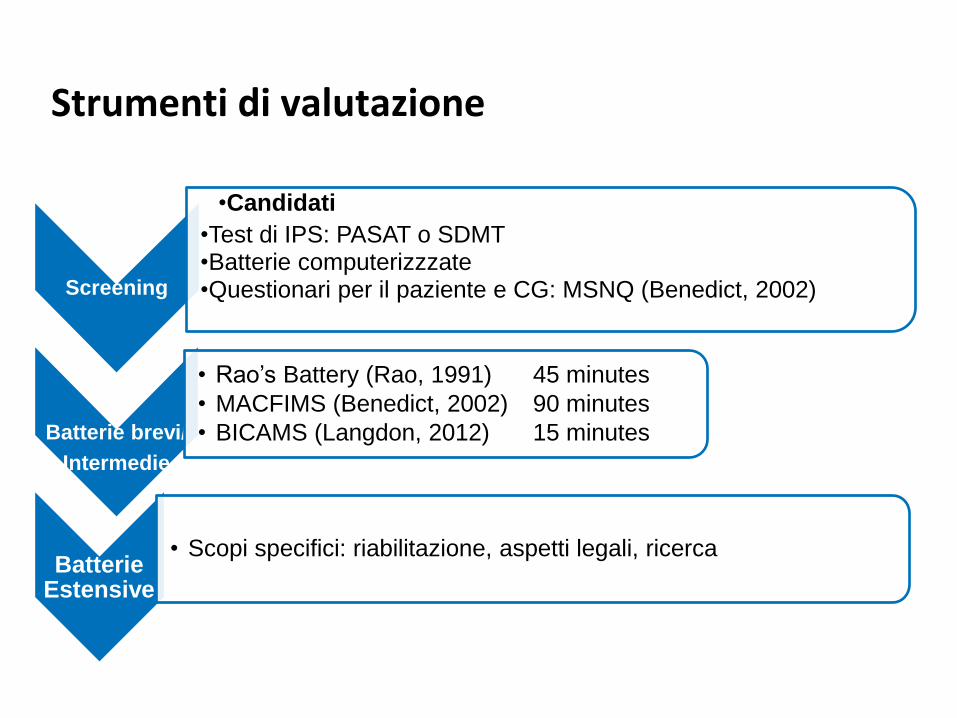
Strumenti di valutazione
Screening
•Candidati
•Test di IPS: PASAT o SDMT •Batterie computerizzzate •Questionari per il paziente e CG: MSNQ (Benedict, 2002)
Batterie brevi/
Intermedie
• Rao’s Battery (Rao, 1991) 45 minutes
• MACFIMS (Benedict, 2002) 90 minutes
• BICAMS (Langdon, 2012) 15 minutes
Batterie Estensive
• Scopi specifici: riabilitazione, aspetti legali, ricerca

Recommendations for a
Brief International Cognitive Assessment for MS
(BICAMS)
Langdon DW, Amato MP, Boringa J, Brochet B, Foley F, Fredrikson S,
Hamalainen P, Hartung HP, Krupp L, Penner IK; Reder AT, Benedict RHB
MSJ, 2012
Requirements: 15 minutes, no specific equipment, no specific assessor training
Methods: literature review and expert opinion, ratings of candidate tests on psychometric and pragmatic standards
• SDMT
with more time
• CVLT –II (first 5 recall trials)
• BVMT-R (first 3 recall trials)
Standard guidelines for
translations and
validation protocols
(Benedict, 2012)
SDMT: Symbol Digit Modalities Test; CVLT: California Verbal Learning Test; BVMT-R: Brief Visuospatial Memry Test-Revised
Access
The brief international cognitive assessment for
multiple sclerosis (BICAMS): normative values with
gender, age and education corrections in the
Italian population
Benedetta Goretti1, Claudia Niccolai1, Bahia Hakiki1,2, Andrea Sturchio1, Monica Falautano3, Eleonora
Minacapelli3,Vittorio Martinelli3, Chiara Incerti4, Ugo Nocentini4, Monica Murgia5, Giuseppe Fenu5, Eleonora
Cocco5,Maria Giovanna Marrosu5, Elisabetta Garofalo6, Ferdinando Ivano Ambra6, Maurizio Maddestra7, Marilena
Consalvo7,Rosa Gemma Viterbo8, Maria Trojano8, Nunzia Alessandra Losignore9, Giovanni Bosco Zimatore9,
Erika Pietrolongo10,Alessandra Lugaresi10, Dawn Langdon11, Emilio Portaccio1,2 and Maria Pia Amato
BMC Neurology 2014

Confonditori
Depressione e ansia
Fatica
Deficit neurologici
Dolore
Co-morbidità
Effetti collaterali delle terapie
modificato da Benedict et al., 2002
Approcci terapeutici
• Farmacologici
1.DMDs
–Per prevenire/rallentare lo sviluppo di DC
2. Sintomatici
- Per migliorare una funzione cognitiva già compromessa
• Riabilitazione cognitiva

Approcci farmacologi: DMDs
• I DMDs hanno effetti ben documentati su altri outcome clinici
(ricadute, disabilità)
• Il loro uso è supportato dai risultati RM che documentano un
impatto sull’infiammazione, il carico di lesioni e l’atrofia
cerebrale
• Alcuni di essi possono anche esercitare effetti neuroprotettivi
diretti (es. via BDNF, NGF, nuovi meccanismi d’azione)
RAZIONALE

Importanza del trattamento precoce: IFNβ1b nelle CIS
BENEFIT: Effetto sul PASAT
-0,1
0
0,1
0,2
0,3
0,4
0,5
BL Year
1
Year
2
Year
3
Year
4
Year
5
PA
SA
T Z
-sco
re
At Year 3:
P=0.064*
At Year 5:
P=0.0045*
Early treatment
Delayed treatment
P=0.0045*
I
mp
rove
men
t
*Non-parametric analysis of covariance. Penner, MSJ 2012
n=464 n=413 n=404 n=374 n=361 n=349
No significant difference
between the two treatment
groups for the other
Multiple Sclerosis
Functional Composite
(MSFC) subscales (25-
Foot Walk, 9-Hole Peg
Test) or the overall MSFC.
INFβ1b

• I dati della letteratura sono carenti
• La maggioranza degli studi sui DMD, comunque, ha riportato
qualche effetto positivo anche sul DC
• Il trattamento precoce è in principio il metodo più efficace per prevenire /rallentare l’avvento di un significativo DC
• E’ essenziale che d’ora in poi una breve valutazione delle funzioni cognitive sia inserita sistematicamente nei TC futuri sulla SM
DMTs: Messaggio da portare a casa
Amato et al., J Neurol 2012

Terapie sintomatiche per la Fatica
• Trial pilota, risultati negativi con
– 4-aminopiridina
– 3-4 diaminopiridina
– Rinnovato interesse con fampridina
– Amantadina
• Risultati preliminari positivi con modafinil (Wilken 2008)

Terapie sintomatiche: Stimolanti
• Trial pilota, risultati preliminari positivi con
– metilfenidato (Harel 2009)
– L –anfetamina (Benedict 2008; Sumouski 2010)
Terapie sintomatiche farmaci per la malattia di Alzheimer
• Risultati negativi con
– Rivastigmina
– Memantina
• Risultati controversi /negativi con
• Donepezil (Krupp 2004; Krupp 2011)
– Non effetti collaterali gravi
– Variabilità nella risposta • In una analisi post hoc risultati positivi sulla memoria verbale in
pazienti con gradi più marcati di deficit di memoria

• Enhancing plasticity processes in the brain, as suggested by f-MRI studies (Penner 2007, Sastre-Garriga, 2010, Chiaravalloti, 2012, Filippi, 2012, Leavitt, 2013).
Preventive
• Reducing cognitive deficits through cognitive retraining as best shown in the models of traumatic brain injury and stroke (Cicerone 2000).
Restorative
Compensatory/
Maintenance
•Improving coping strategies to deal with existing cognitive problems (eg internal strategies for memory problems) (Wilson 2008) and teaching compensatory strategies (eg external aids: notebooks, calendars, lists, computer-assisted aids…) (Wilson 2008).
Palliative Providing neuropsychological support to help patients to understand and accept their cognitive problems and increase
psychological well-being (Mateer 2005).
Rosti-Hotajarvi, Hamalainen, 2012
Come può funzionare la riabilitazione cognitiva
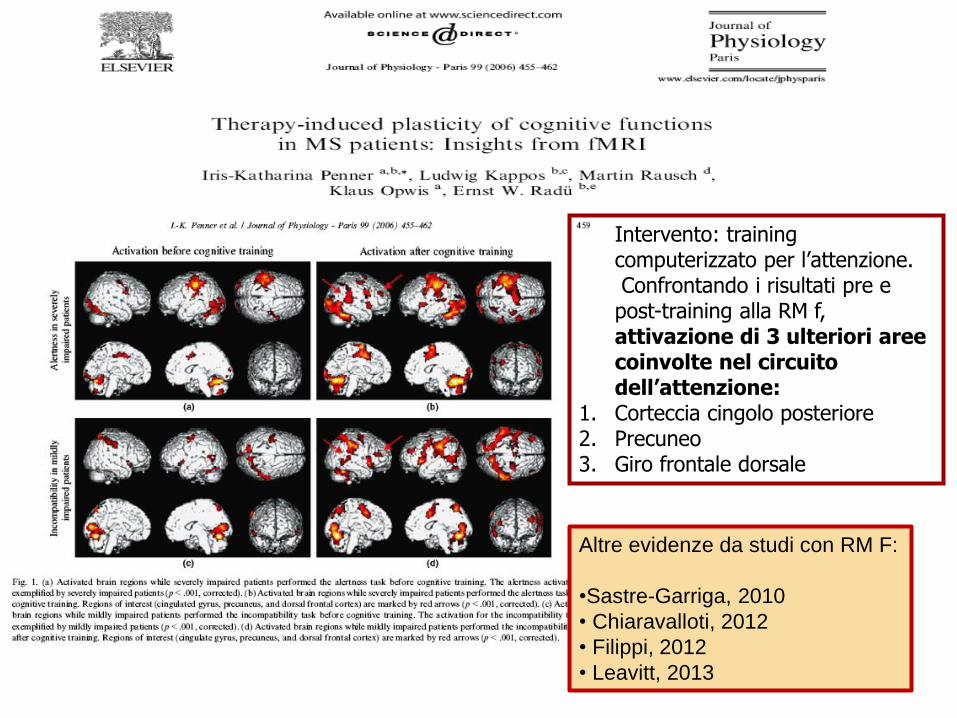
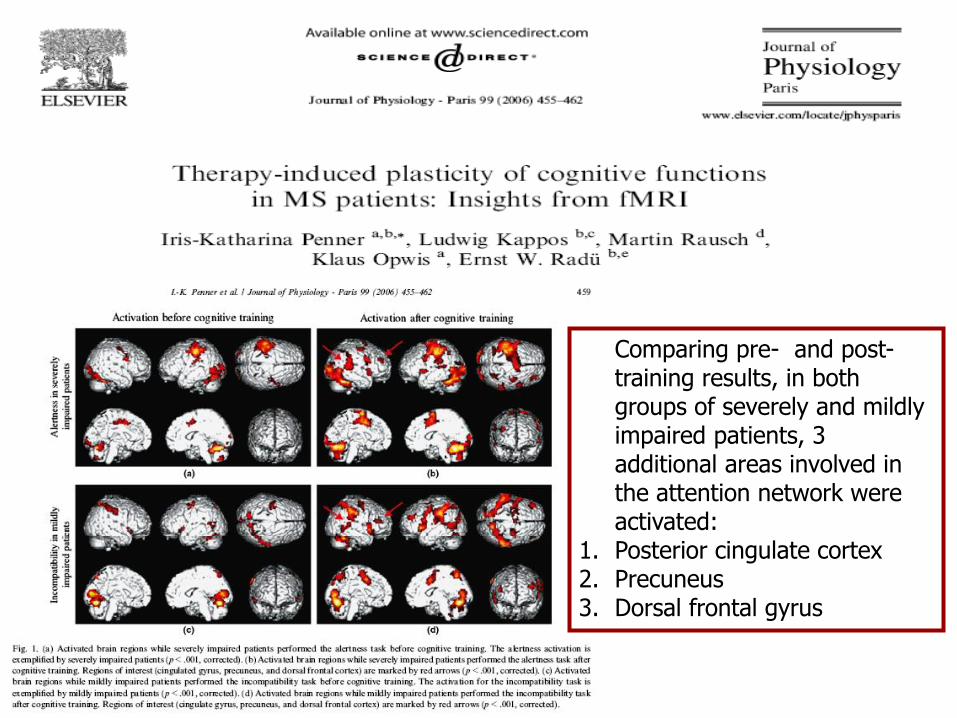
Intervento: training computerizzato per l’attenzione.
Confrontando i risultati pre e post-training alla RM f, attivazione di 3 ulteriori aree coinvolte nel circuito dell’attenzione:
1. Corteccia cingolo posteriore 2. Precuneo 3. Giro frontale dorsale
Altre evidenze da studi con RM F:
•Sastre-Garriga, 2010
• Chiaravalloti, 2012
• Filippi, 2012
• Leavitt, 2013
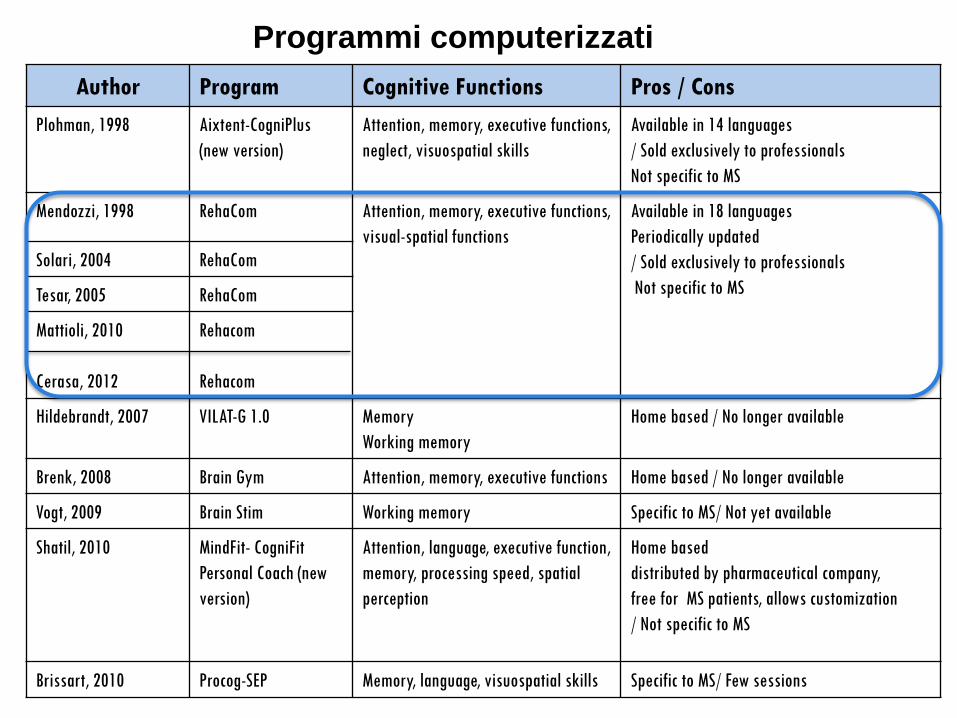
Author Program Cognitive Functions Pros / Cons
Plohman, 1998 Aixtent-CogniPlus
(new version)
Attention, memory, executive functions,
neglect, visuospatial skills
Available in 14 languages
/ Sold exclusively to professionals
Not specific to MS
Mendozzi, 1998 RehaCom Attention, memory, executive functions,
visual-spatial functions
Available in 18 languages
Periodically updated
/ Sold exclusively to professionals
Not specific to MS
Solari, 2004 RehaCom
Tesar, 2005 RehaCom
Mattioli, 2010
Cerasa, 2012
Rehacom
Rehacom
Hildebrandt, 2007 VILAT-G 1.0 Memory
Working memory
Home based / No longer available
Brenk, 2008 Brain Gym Attention, memory, executive functions Home based / No longer available
Vogt, 2009 Brain Stim Working memory Specific to MS/ Not yet available
Shatil, 2010 MindFit- CogniFit
Personal Coach (new
version)
Attention, language, executive function,
memory, processing speed, spatial
perception
Home based
distributed by pharmaceutical company,
free for MS patients, allows customization
/ Not specific to MS
Brissart, 2010 Procog-SEP Memory, language, visuospatial skills Specific to MS/ Few sessions
Programmi computerizzati
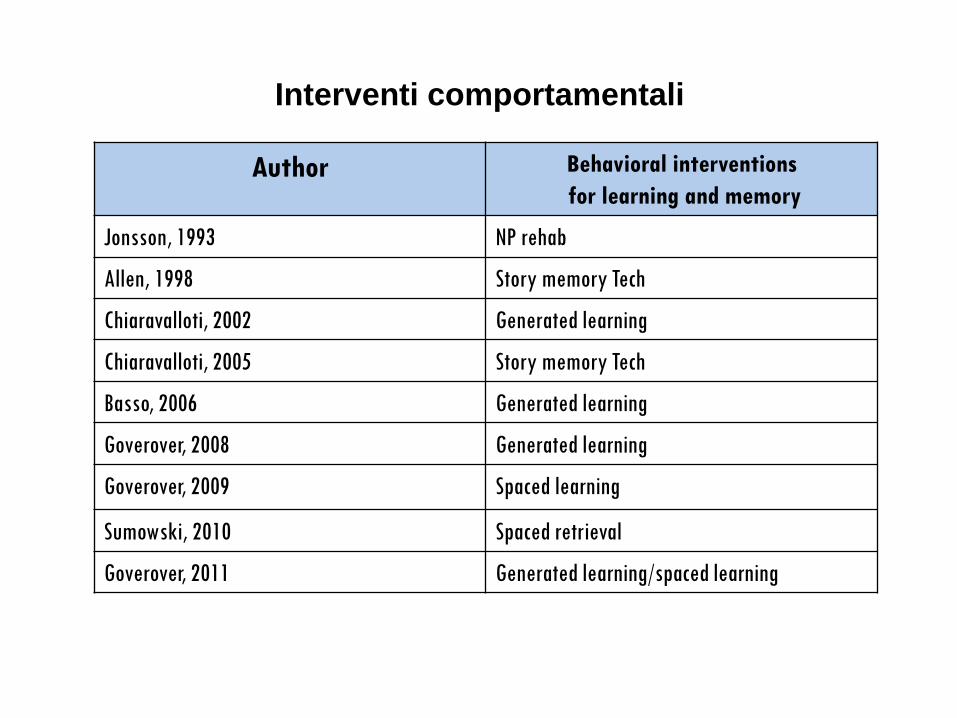
Author Behavioral interventions
for learning and memory
Jonsson, 1993 NP rehab
Allen, 1998 Story memory Tech
Chiaravalloti, 2002 Generated learning
Chiaravalloti, 2005 Story memory Tech
Basso, 2006 Generated learning
Goverover, 2008 Generated learning
Goverover, 2009 Spaced learning
Sumowski, 2010 Spaced retrieval
Goverover, 2011 Generated learning/spaced learning
Interventi comportamentali

─Modified story memory technique (MST)
─ Use of context and imagery to improve learning of new materials
─ Self-generation effect
─ The generation effect is the observation that items generated by subjects are remembered
better than items simply presented
─Spacing effect
─ The spacing effect is the observation that learning trials spaced over time result in significantly
better performance than if trials are “massed” (e.g. consecutive trials)
─Testing effect
─ The testing effect is the observation that testing (e.g. quiz) improves subsequent recall more
than restudying the material again
Interventi comportamentali per migliorare
l’apprendimento e la memoria
O’ Brien, 2008; DeLuca 2011

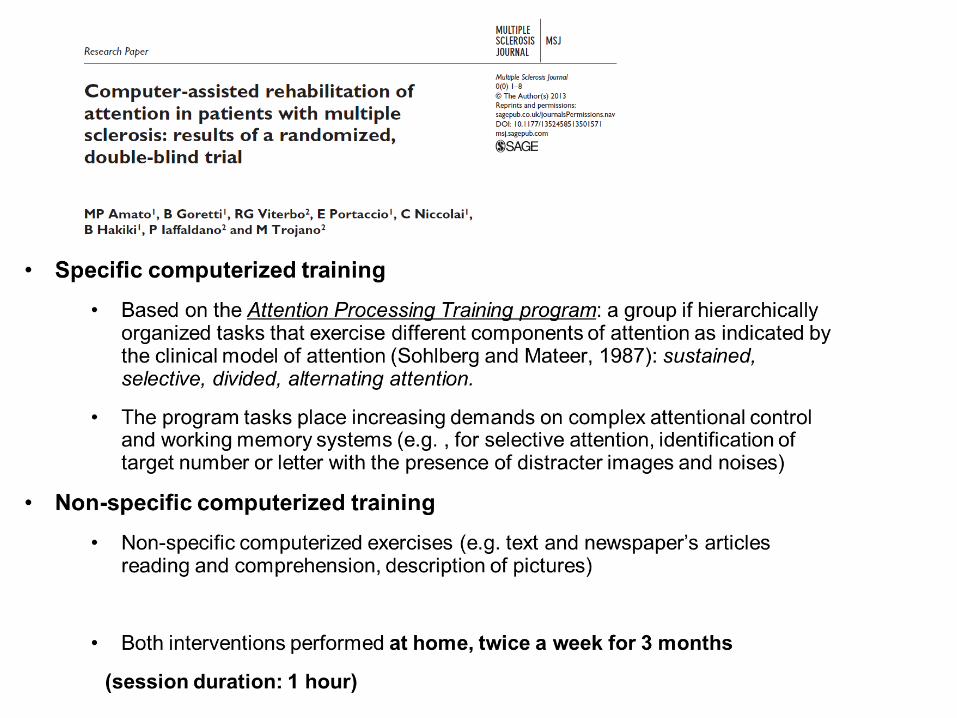
Intervention:
1. m-Story Memory Technique
2. Non specific intervention
―10 sessions
―2 times per week for 5
weeks
― each session 45 to 60
minutes
―The treatment group was
randomized to monthly booster
session or placebo booster
session group
Assessment:
―At baseline
―Immediately after the
treatment
―At 6 months
Neurology 2013

• Analisi RMf in 16 pazienti:
• Maggiore attivazione,
specifica dei soggetti
sottoposti alla
riabilitazione, di aree
cerebrali coinvolte nel
network della memoria
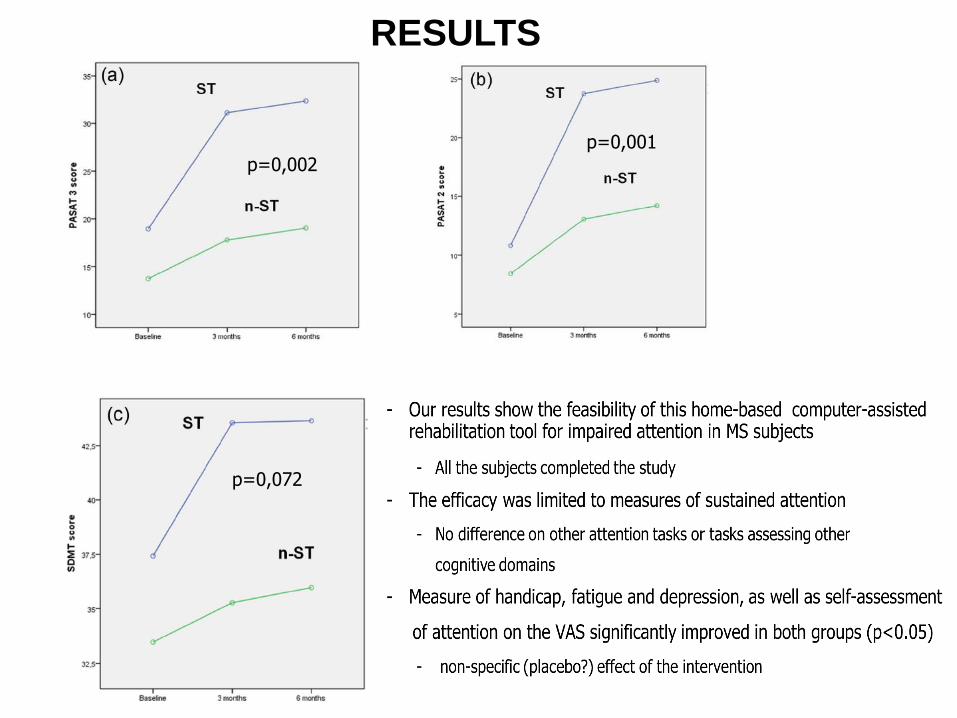
p=0,002 p=0,001
p=0,072
RESULTS

2011: Non effetti significativi nella metanalisi , MA 12/14 studi erano positivi
2012: Non evidenze a supporto …la conclusione è legata alla limitata qualità
metodologica degli studi
2014: C’è qualche evidenza che il training cognitivo possa migliorare la
memoria
Alcune revisioni delle evidenze
2011 2012 2014

―Pochi studi, molti limiti metodologici
―Il numero degli studi è aumentato/la qualità migliorata nell’arco degli ultimi anni
―Alcune questioni aperte: • Quali pazienti siano i migliori candidati • Quale profilo o livello di DC sia più opportuno affrontare • Quale formato sia ottimale • Frequenza e durata delle sedute
Riabilitazione Cognitiva: stato dell’arte

• Recenti studi rigorosamente disegnati mostrano effetti positivi della riabilitazione: “riabilitiamo la riabilitazione cognitiva nella SM!” – Memoria
– Attenzione
– Funzioni esecutive
• L’efficacia è supportata dagli studi di RM funzionale
• Nonostante quest’area debba rimanere un obiettivo primario della ricerca, tecniche di riabilitazione cognitiva sono oggi disponibili ed efficaci e dovrebbero essere offerte ai pazienti con SM
Riabilitazione Cognitiva: stato dell’arte
COS’ALTRO?
Training aerobico
Arricchimento intellettivo
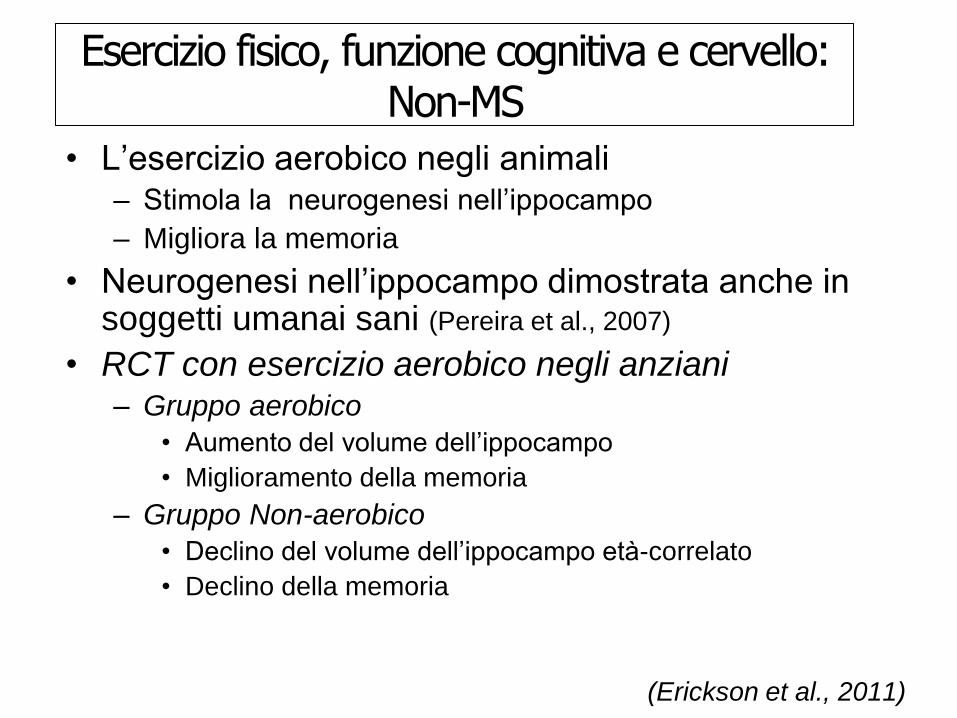
Esercizio fisico, funzione cognitiva e cervello: Non-MS
• L’esercizio aerobico negli animali – Stimola la neurogenesi nell’ippocampo
– Migliora la memoria
• Neurogenesi nell’ippocampo dimostrata anche in soggetti umanai sani (Pereira et al., 2007)
• RCT con esercizio aerobico negli anziani – Gruppo aerobico
• Aumento del volume dell’ippocampo
• Miglioramento della memoria
– Gruppo Non-aerobico
• Declino del volume dell’ippocampo età-correlato
• Declino della memoria
(Erickson et al., 2011)

G. Siracusa, MD M. Giannini, MD B. Goretti, PhD C. Niccolai, PhD B. Hakiki, MD L. Pastò, MD I. Righini, MD
E. Portaccio, MD L. Razzolini, MD
Prof. S. Sorbi, MD
Grazie!

Fratiglioni et al., 2004
Uno stile di vita attivo protegge dalla demenza
Att.. fisica.
Att. mentale.
Att. sociale.
Att. fisica.
Att. mentale.
Att. sociale
Att. fisica.
Att. mentale.
Att. sociale.
Phys. Act.= Pysical Activites Ment. Act.= Mental Activities Soc. Act.= Social Activities
Numero di studi che non riportano associazione
Numero di studi che riportano un’associazione

Alcuni suggerimenti
• Informazione/educazione del paziente e dei familiari
• Approccio inter-disciplinare e Counselling • Uso di ausilii (calendari, diari, strumenti computerizzati)
• Dare una priorità e distribuire nel tempo le attività
• Trovare gli appropriati adattamenti ambientali a casa /scuola/lavoro
Alcuni suggerimenti • Individualizzare l’approccio
• Coinvolgere i membri della famiglia/altre persone significative
• Affrontare possibili comorbidità e fattori di peggioramento – Fatica
– Depressione/Ansia
– Effetti collaterali delle terapie
– Stile di vita (sonno, alcol, fumo)
• Incoraggiare l’attività fisica
• Mantenere il più possibile l’inserimento nelle attività familiari/sociali/lavorative
• Esercizio (mentale e fisico): il cervello può migliorare!

Grazie!
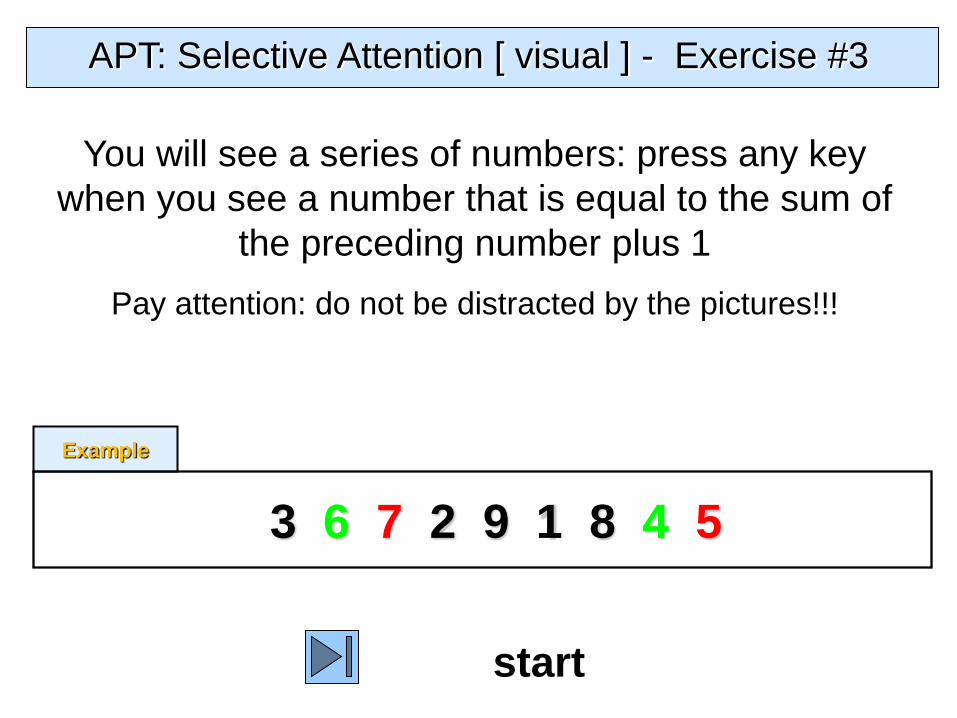
APT: Selective Attention [ visual ] - Exercise #3
start
You will see a series of numbers: press any key
when you see a number that is equal to the sum of
the preceding number plus 1
Pay attention: do not be distracted by the pictures!!!
3 6 7 2 9 1 8 4 5
Example
9

6

7
Comparing pre- and post- training results, in both groups of severely and mildly impaired patients, 3 additional areas involved in the attention network were activated:
1. Posterior cingulate cortex 2. Precuneus 3. Dorsal frontal gyrus

Thank you!
Emilio Portaccio
Benedetta Goretti
Bahia Hakiki
Marta Giannini
Luisa Pastò
Lorenzo Razzolini
Professor Sandro Sorbi
University of Florence, IT

A few “red flags” for CI
• Clinical • Report of difficulties from the patient/caregiver
• Prominent fatigue
• Withdrawal from hobbies and social activities that is not completely justified on the basis of physical disability
MRI • Increasing lesion load
• Persistent activity
• Lesion location involving critical regions and pathways (e.g. corpus callosum, cortex, thalami, basal ganglia)
• Brain atrophy

Modified Story Technique Percent Improvement in New Learning
after Treatment in MS subjects with Moderate/Severe CI
p <.05
Chiaravalloti et al., 2005
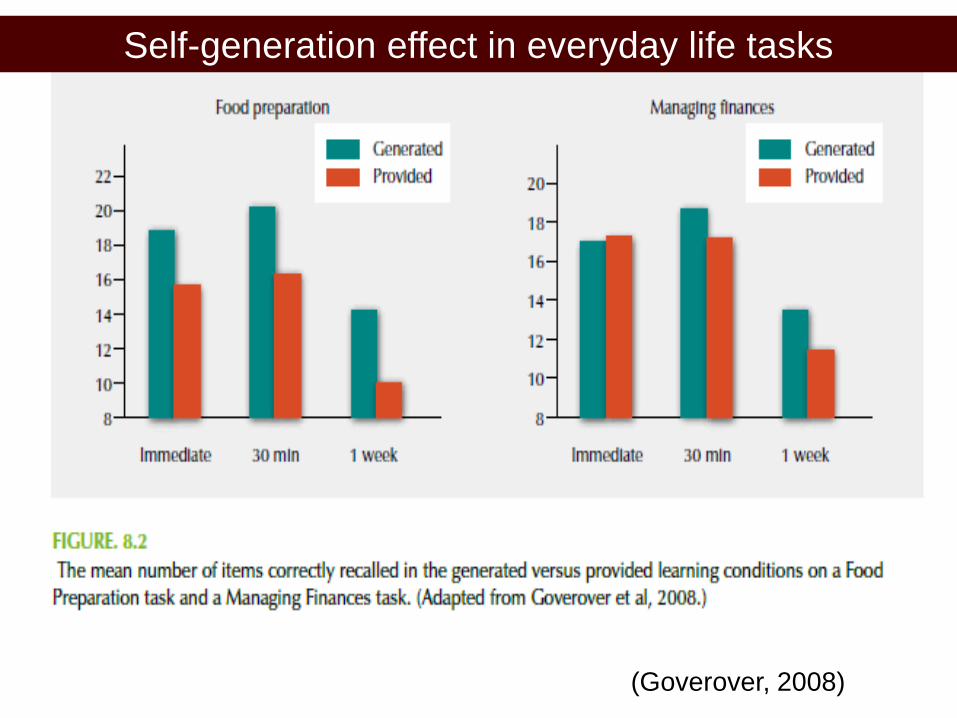
Self-generation effect in everyday life tasks
(Goverover, 2008)
• A few well-conducted studies show positive effects of rehabilitation approaches in the area of learning / memory and attention
• The efficacy is supported by preliminary findings of fMRI studies
• While cognitive rehabilitation is an option in practice, further,
more rigorous proof-of-concept studies are needed to develop standards and guidelines
Cognitive Rehabilitation: In Summary
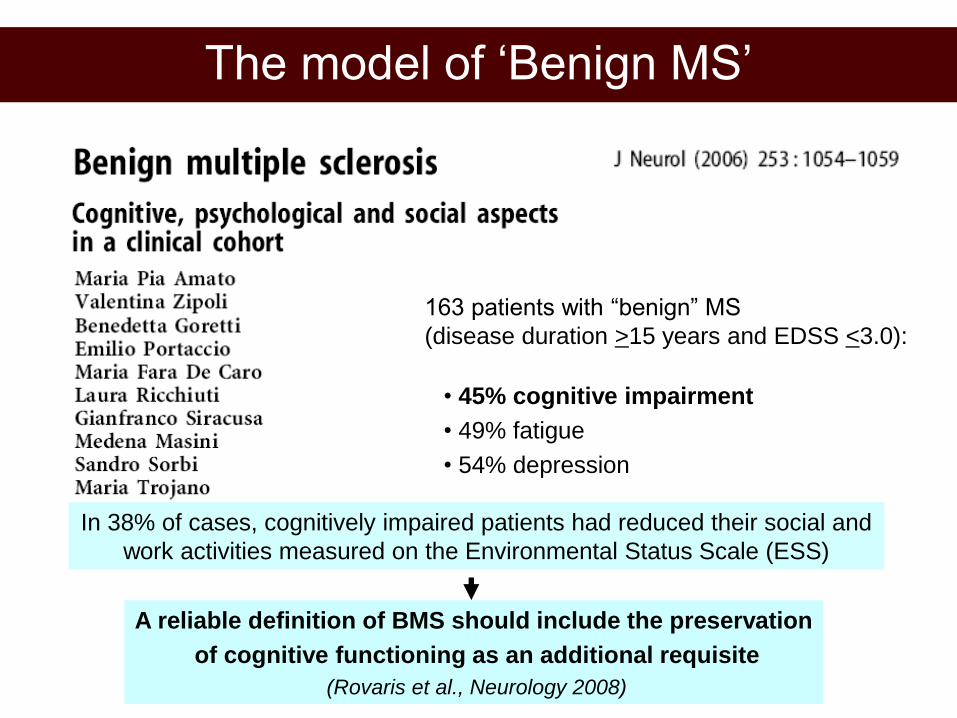
163 patients with “benign” MS
(disease duration >15 years and EDSS <3.0):
• 45% cognitive impairment
• 49% fatigue
• 54% depression
In 38% of cases, cognitively impaired patients had reduced their social and
work activities measured on the Environmental Status Scale (ESS)
A reliable definition of BMS should include the preservation
of cognitive functioning as an additional requisite
(Rovaris et al., Neurology 2008)
The model of ‘Benign MS’

Amato et al., 2008, Portaccio et al., 2009
“Pseudo-benign”, cognitively impaired patients, compared with “truly benign”, cognitively preserved subjects were characterized by – Greater T1 lesion loads in the white matter – Cortical tissue changes (reduced volumes, total and regional MTR values) – After 5 years, significantly higher probability of progressing to a no longer
benign status
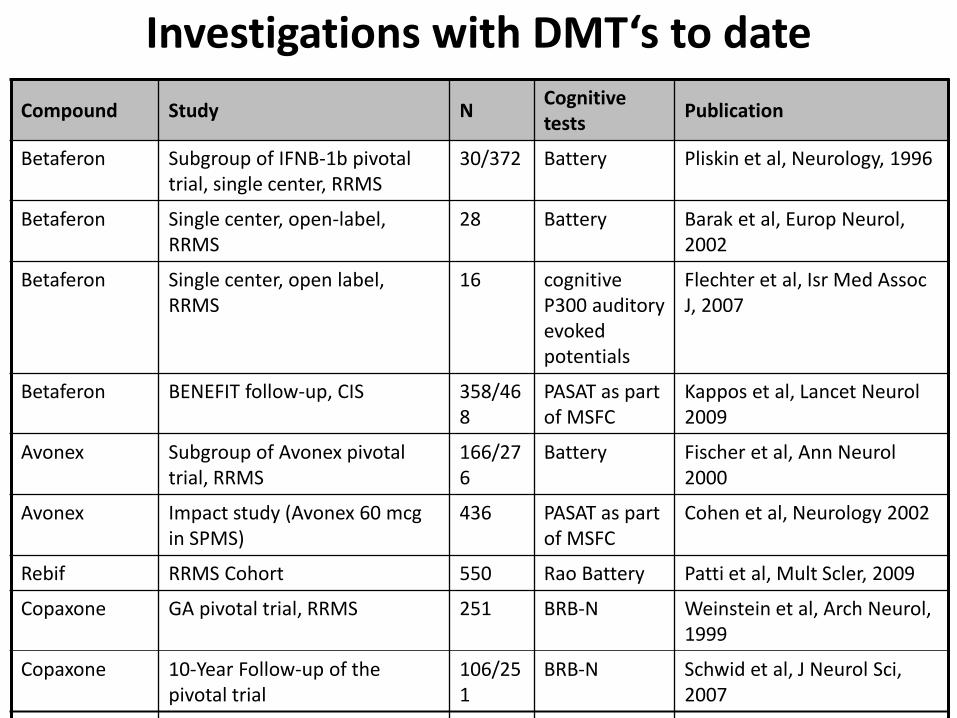
Compound Study N Cognitive tests
Publication
Betaferon Subgroup of IFNB-1b pivotal trial, single center, RRMS
30/372 Battery Pliskin et al, Neurology, 1996
Betaferon Single center, open-label, RRMS
28 Battery Barak et al, Europ Neurol, 2002
Betaferon Single center, open label, RRMS
16 cognitive P300 auditory evoked potentials
Flechter et al, Isr Med Assoc J, 2007
Betaferon BENEFIT follow-up, CIS 358/468
PASAT as part of MSFC
Kappos et al, Lancet Neurol 2009
Avonex Subgroup of Avonex pivotal trial, RRMS
166/276
Battery Fischer et al, Ann Neurol 2000
Avonex Impact study (Avonex 60 mcg in SPMS)
436 PASAT as part of MSFC
Cohen et al, Neurology 2002
Rebif RRMS Cohort 550 Rao Battery Patti et al, Mult Scler, 2009
Copaxone GA pivotal trial, RRMS 251 BRB-N Weinstein et al, Arch Neurol, 1999
Copaxone 10-Year Follow-up of the pivotal trial
106/251
BRB-N Schwid et al, J Neurol Sci, 2007
Betaferon Subgroup of EU-SPMS study 196/718
BRB Unpublished, abstract by Langdon et al., ECTRIMS 2002
Betaferon 16 Year LTF 179 Battery Unpublished, abstract by Langdon et al., AAN 2008
Tysabri AFFIRM, RRMS 627 PASAT as part of MSFC
Unpublished, abstract by Galetta et al. WCN 2005
Avonex Cohort study, CIS and early MS 231 MUSIC Unpublished, abstract by Haas et al. WCTRIMS 2008
Investigations with DMT‘s to date

Assessment: Key Points and Future Directions
• Clinicians now have many assessment tools available to measure CI in MS patients
• Some of the tests require very little time, are reliable and well correlated with meaningful and relevant QOL standards (e.g.SDMT; PASAT; CVLTR)
• Some tests with very high reliability such as the PASAT, SDMT and measures of verbal and visual memory are good candidates for clinical trials.
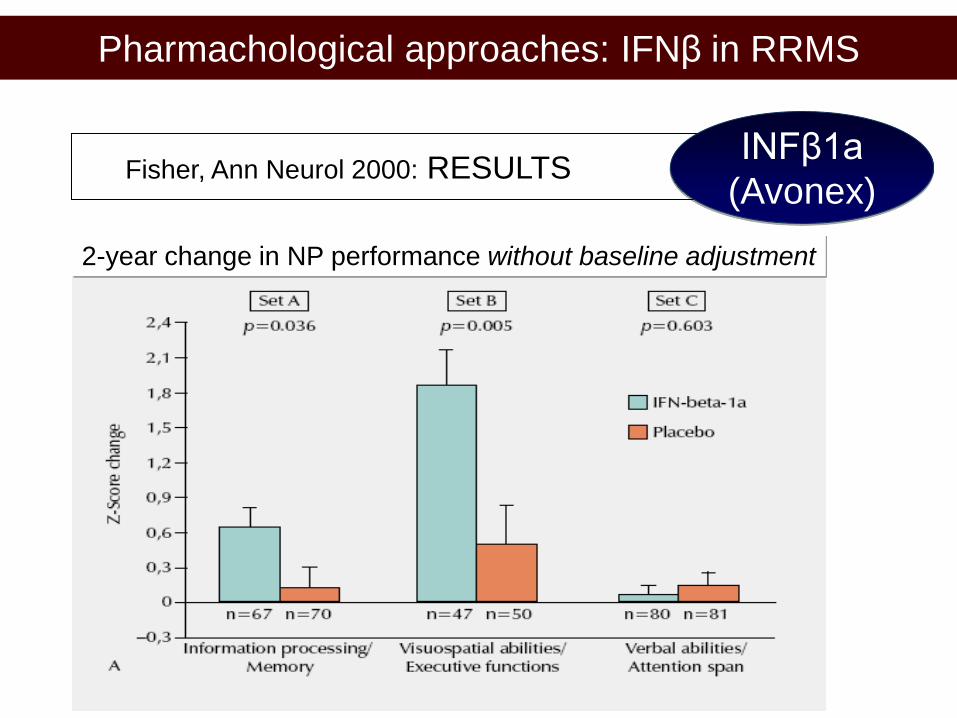
Pharmachological approaches: IFNβ in RRMS
Fisher, Ann Neurol 2000: RESULTS
INFβ1a
(Avonex)
2-year change in NP performance without baseline adjustment
Cognitive Rehabilitation - Key Principles
Restoration Complete or partial restitution of a disturbed function by
therapy, e.g. training exercises
Compensation Residual functions used as a basis for compensatory strategies,
e.g. coping strategies
Adaptation/accomodations
Changes in the shared environment of the individual which
allow functioning in spite of disabilities e.g. use of aids such as day planners, memory books
•

Amato et al., 2008, Portaccio et al., 2009
Truly “benign”, cognitively preserved patients were characterized by – Lower T1 lesion loads in the white matter
– Cortical tissue sparing (volumes, total and regional MTR values)
– Significantly higher probability of remaining benign after
5 years as compared with cognitively impaired subjects
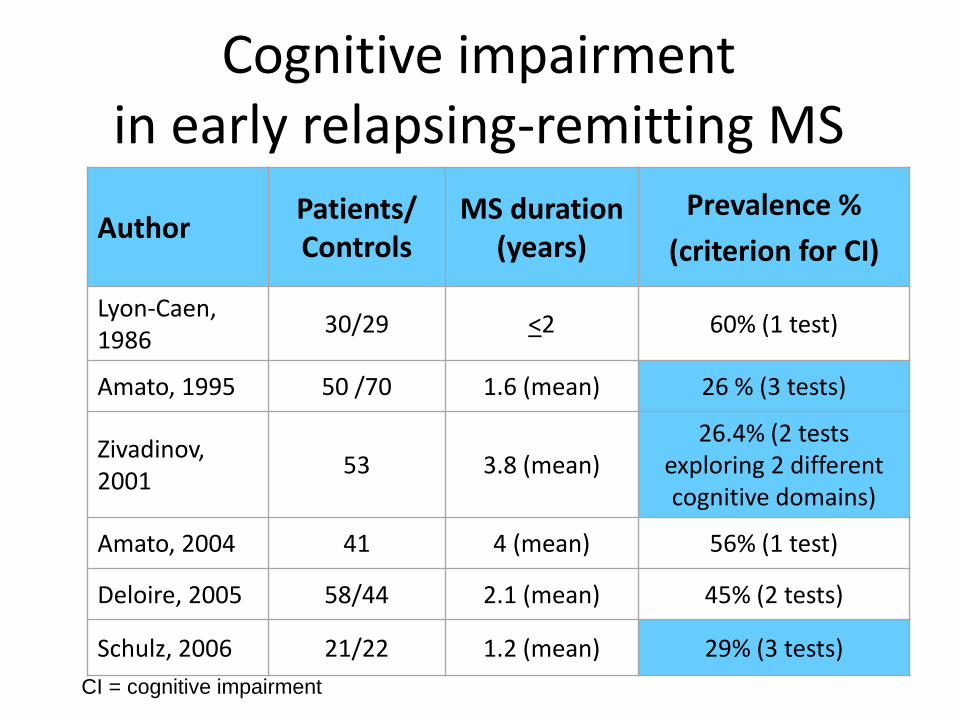
Cognitive impairment in early relapsing-remitting MS
Author Patients/ Controls
MS duration (years)
Prevalence %
(criterion for CI)
Lyon-Caen, 1986
30/29 <2 60% (1 test)
Amato, 1995 50 /70 1.6 (mean) 26 % (3 tests)
Zivadinov, 2001
53 3.8 (mean) 26.4% (2 tests
exploring 2 different cognitive domains)
Amato, 2004 41 4 (mean) 56% (1 test)
Deloire, 2005 58/44 2.1 (mean) 45% (2 tests)
Schulz, 2006 21/22 1.2 (mean) 29% (3 tests)
CI = cognitive impairment

•Study design: non-randomized double blind controlled
•Small sample size: reduced power, analyses of sub-groups impossible
•Absence of clear-cut inclusion criteria: objectively documented cognitive deficits
•Absence of description of clinical features
•Short follow-up period: evaluation of short and long-term benefits needed
•Confounders: effects of medications
•Possible role of aspecific learning or practice effects
•No assessment of functional impact on ADL
Cognitive Rehabilitation limitations of published studies
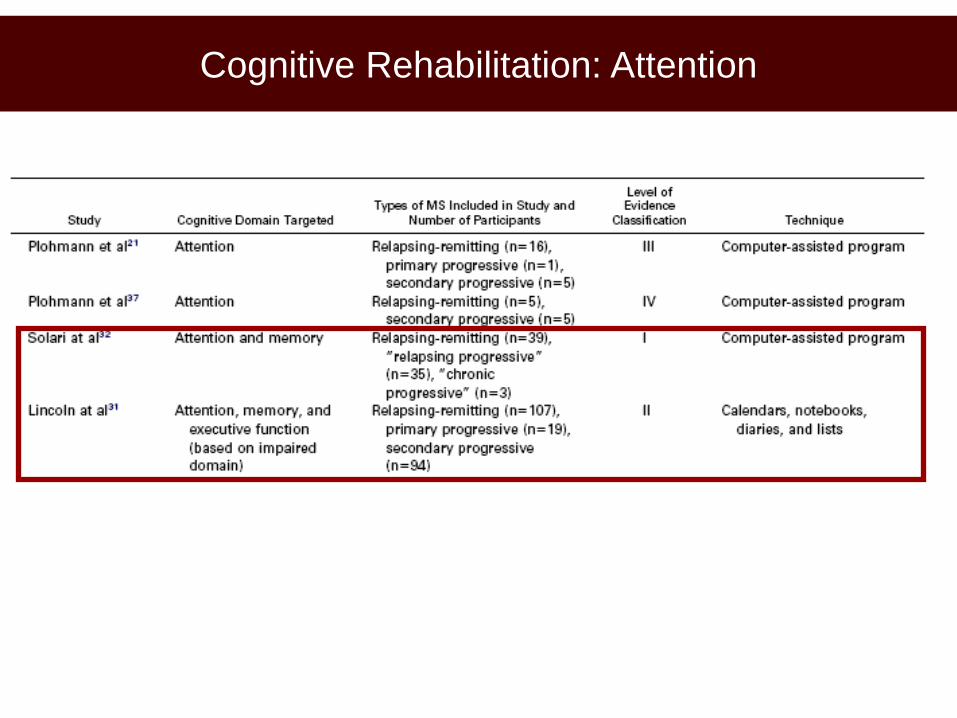
Cognitive Rehabilitation: Attention

Cognitive Rehabilitation: Executive Functioning

P<0.05
Comparison of mildly versus moderately impaired patients in the experimental group

Cognitive Rehabilitation:
Non specific rehabilitation interventions

*
*
*
20 pts. randomly assigned to
rehabilitation (RehaCom)
or no intervention

Pharmachological approaches: IFNβ in RRMS
Fisher, Ann Neurol 2000: METHODS
INFβ1a
(Avonex ®)
IFNB-1a 30 mcg
n=83
Placebo
n=83 Baseline Month 24
Comprehensive
Battery
Comprehensive
Battery
Brief
Battery
Month 6
Brief
Battery
Month 18
Brief
Battery
Month 12

Pharmachological approaches:
“Enhancers”
L-
amphetamine
Sumowski, MSJ 2011
─In memory imapired subjects delayed recall
improved by 48.5% in the LA group vs 1% in the PL group
─LA may act through enhanced hippocampal function
─A phase 3 trial focusing on memory functions is needed

Pathophysiology of CI in MS - Insights from MRI studies
• Sensory deafferentation
• Disconnession of associative areas: cortico-cortical and
cortico-thalamic
• Lesions affecting pathways / areas strategic for cognition
• Involvement of NABT
• Brain Atrophy: GM most important at both the cortical and
subcortical level
• Cortical lesions
• Effects of inflammation (NO, Cytokines etc.)
─ Suboptimal relationship between MRI and cognitive changes:
brain reserve and compensation

Pharmachological approaches:
Alzheimer’s Drugs
Rivastigmine

Pharmachological approaches: DMTs in RRMS
ITACA - STUDY SAMPLE
Glatiramer
vs IFNs
GA BIFNs
Mean age, ys. 36 36
Women 73% 72%
Mean MS duration, ys. 6.9 6.7
Mean EDSS 2.2 1.8
Treatment naive 72% 91%

Pharmachological approaches: DMTs in RRMS
AFFIRM: SF-36 at 2 years Tysabri ®
monotherapy

Kappos L et al. Neurology. 2006;67(7):1242-1249; Kappos L et al. Lancet. 2007;370(9585):389-397;
Kappos et al., Lancet Neurology 2009, EPAHD
//
Follow-up
2 years
CDMS
Placebo (N=176)
Betaferon (N=292)
24 months
Betaferon
Double Blind
Early Betaferon
Delayed Betaferon
5 years
Extension
up to 9 years
Observational
36 months
5 year results
Pharmachological approaches: IFNβ in CIS
BENEFIT: Study Design INFβ1b
(Betaferon ®)

Pharmachological approaches: IFNβ in CIS
BENEFIT: Effect on PASAT
107
*non parametric ANCOVA
LOCF= last observation carried forward n=273 n=166
Me
an
(S
EM
)
Post-hoc analysis, Data on file
p=0.021*
PASAT change from baseline to last visit (LOCF) of the placebo period
Kappos at al. Lancet Neurology 2009; 8: 987–997
INFβ1b
(Betaferon ®)
Pharmachological approaches: IFNβ in CIS
BENEFIT: post-hoc analyses
108
INFβ1b
(Betaferon ®)
– There was a link between PASAT performance and EDSS at CIS status and at year 5
– No link between PASAT performance and CDMS
– No link between PASAT performance and MRI indicators of disease activity (Gd-enhancement, T2-volume) or axonal/neuronal loss (T1 black hole, total brain volume)
Post-hoc analysis, Data on file

Pharmachological approaches: DMTs in RRMS
FREEDOMS: PASAT Results Fingolimod
0
2,5
5
7,5
10
12,5
Placebo FTY 0.5mg FTY 1.25mg
nu
mb
er
of
co
rrect
an
sw
ers
baseline
6 months
12 months
18 months
24 months
42.5
45
p = 0.014
p = 0.013
47.5
50
52.5
(n = 425)
(n = 429)
(n = 418)
(number of correct answers)