Dalla monoterapiaalla polipillolatigulliocardio.com/2018/Orlandini.pdf · • Una metanalisi di...
52
Ipertensione ed ipotensione Dalla monoterapia alla polipillola Orlandini Francesco Direttore Sanitario ASL 4 Regione Liguria
Transcript of Dalla monoterapiaalla polipillolatigulliocardio.com/2018/Orlandini.pdf · • Una metanalisi di...

Ipertensione ed ipotensione
Dalla monoterapia alla polipillola
Orlandini FrancescoDirettore Sanitario
ASL 4 Regione Liguria
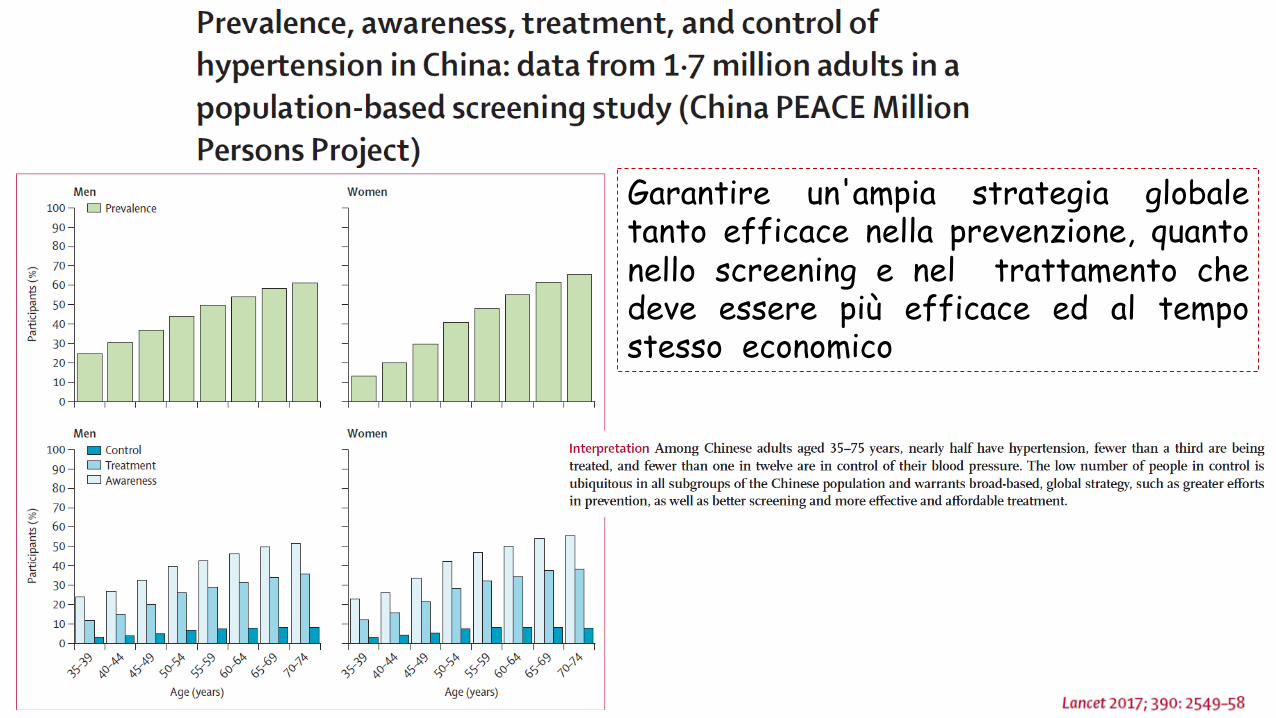
Garantire un'ampia strategia globaletanto efficace nella prevenzione, quantonello screening e nel trattamento chedeve essere più efficace ed al tempostesso economico
Cosa dicono le linee guida
Linee guida ESH-ESC 2013
ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults 2017
GuidelinesHypertension Canada’s 2017 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults
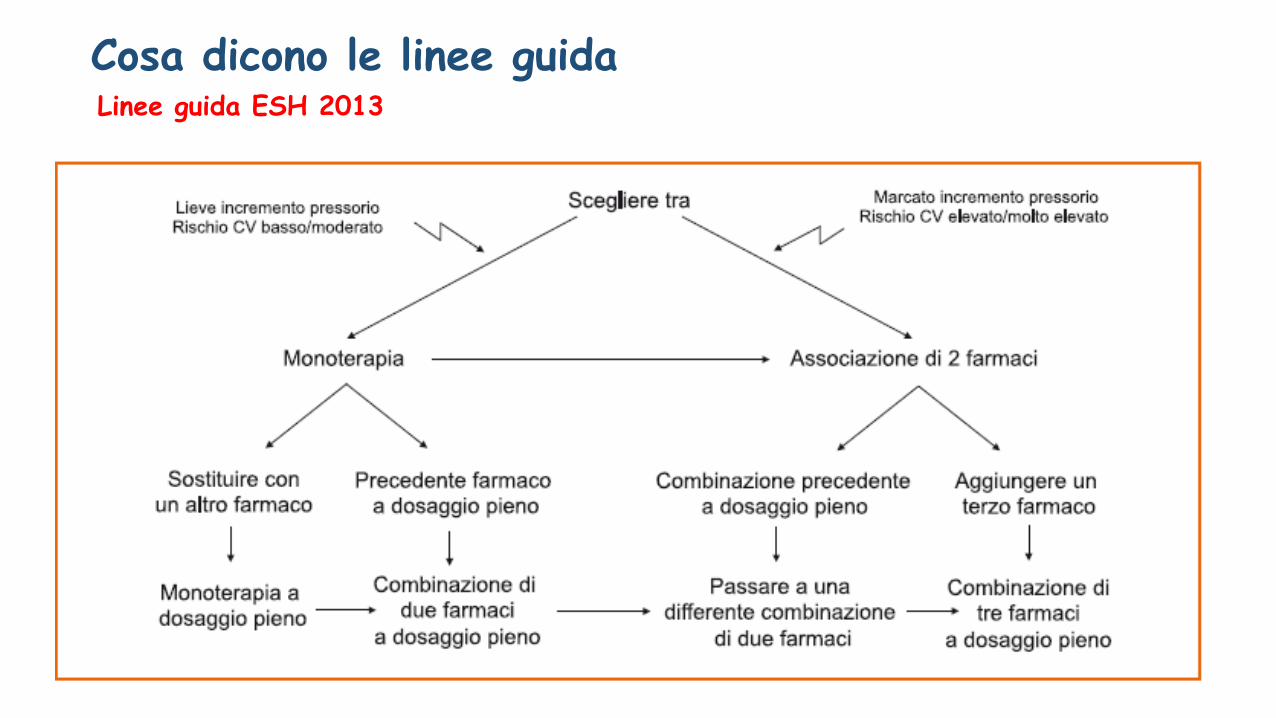
Linee guida ESH 2013Cosa dicono le linee guida
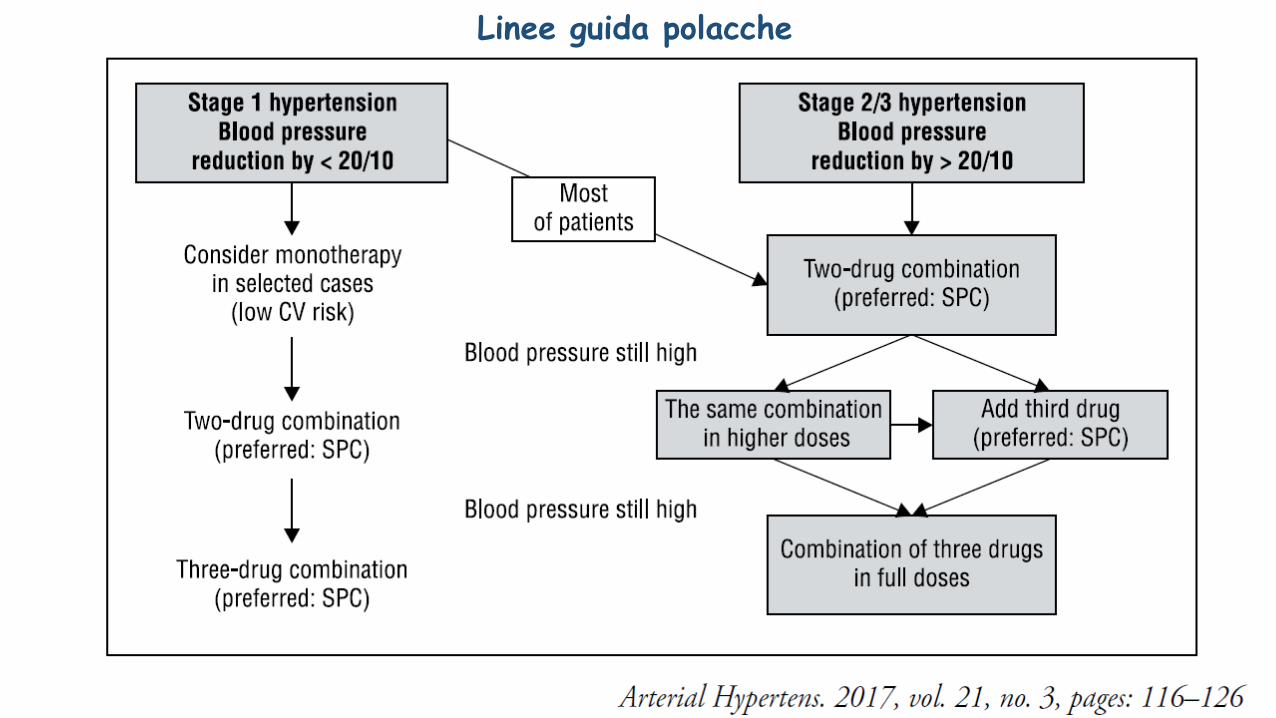
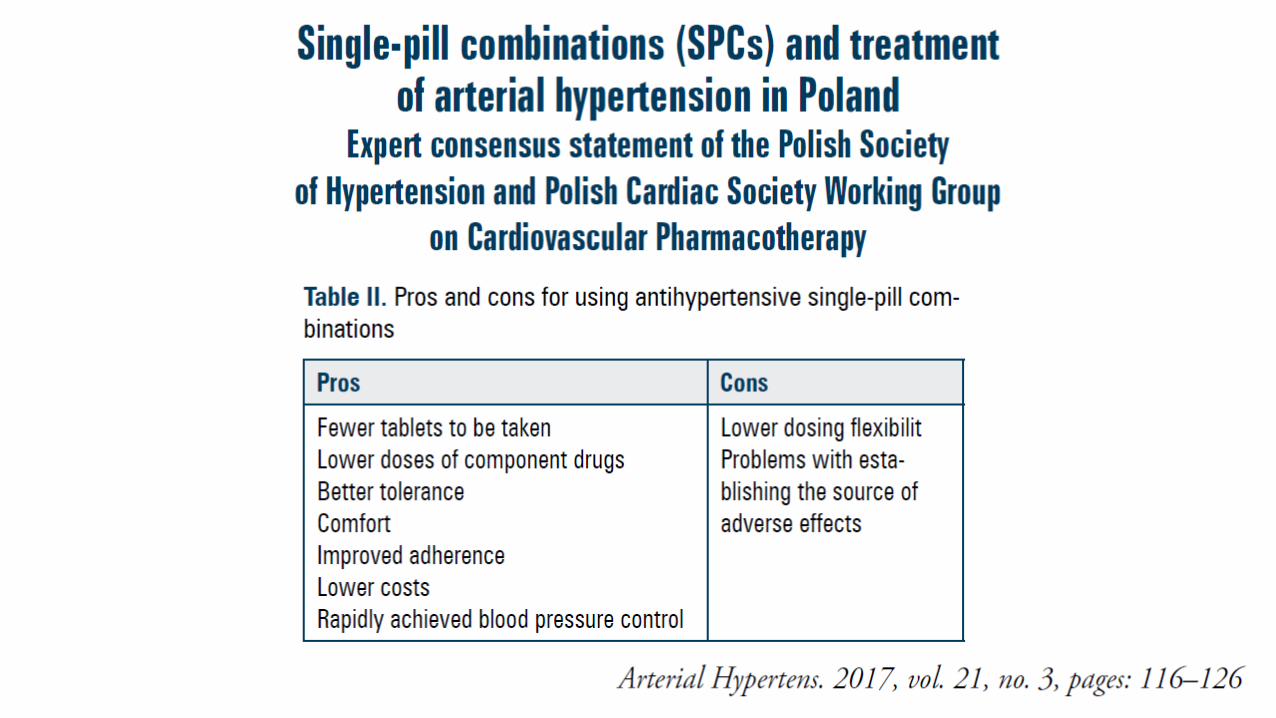
Linee guida polacche
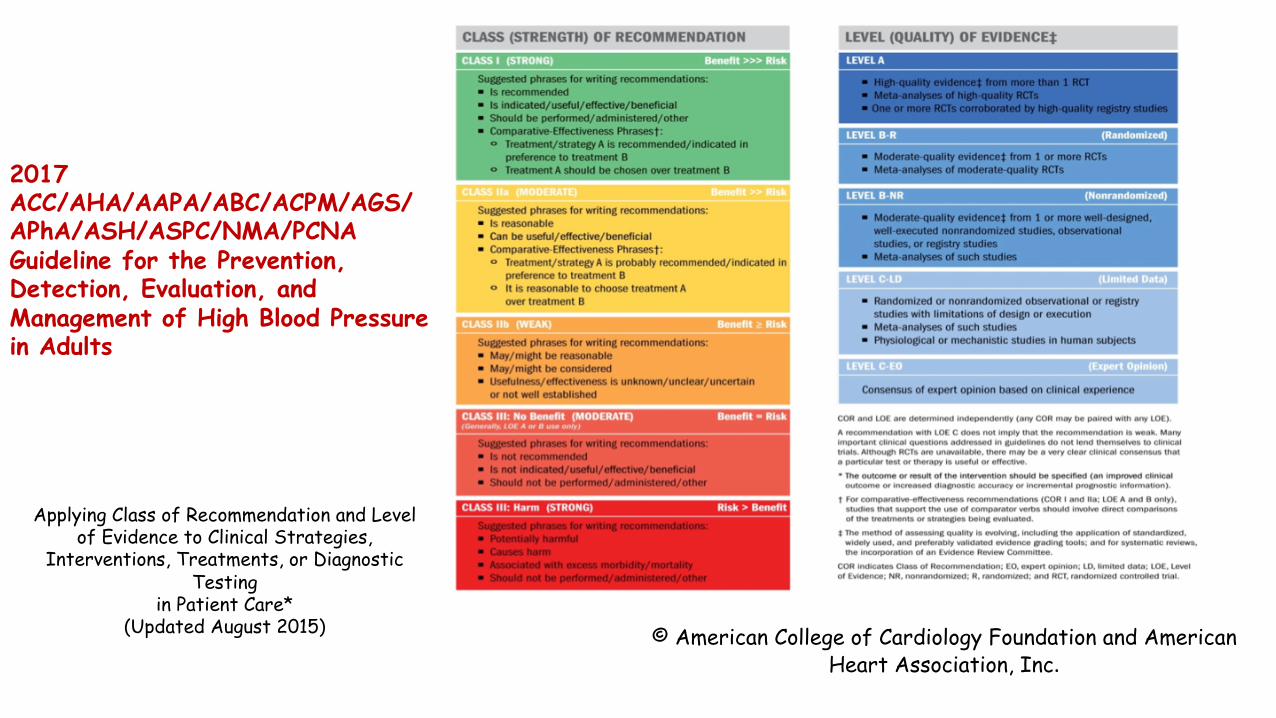
Applying Class of Recommendation and Level of Evidence to Clinical Strategies,
Interventions, Treatments, or Diagnostic Testing
in Patient Care* (Updated August 2015)
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults
© American College of Cardiology Foundation and American Heart Association, Inc.
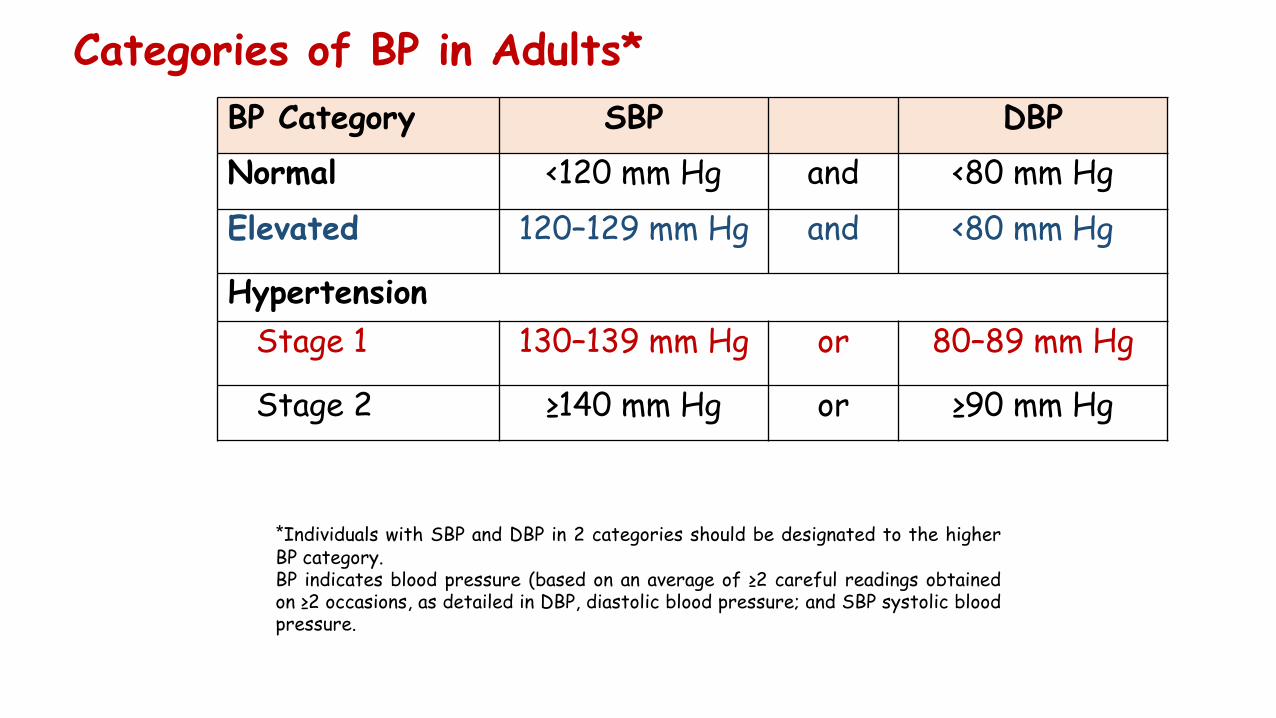
Categories of BP in Adults*
*Individuals with SBP and DBP in 2 categories should be designated to the higherBP category.BP indicates blood pressure (based on an average of ≥2 careful readings obtainedon ≥2 occasions, as detailed in DBP, diastolic blood pressure; and SBP systolic bloodpressure.
BP Category SBP DBPNormal <120 mm Hg and <80 mm HgElevated 120–129 mm Hg and <80 mm Hg
HypertensionStage 1 130–139 mm Hg or 80–89 mm Hg
Stage 2 ≥140 mm Hg or ≥90 mm Hg
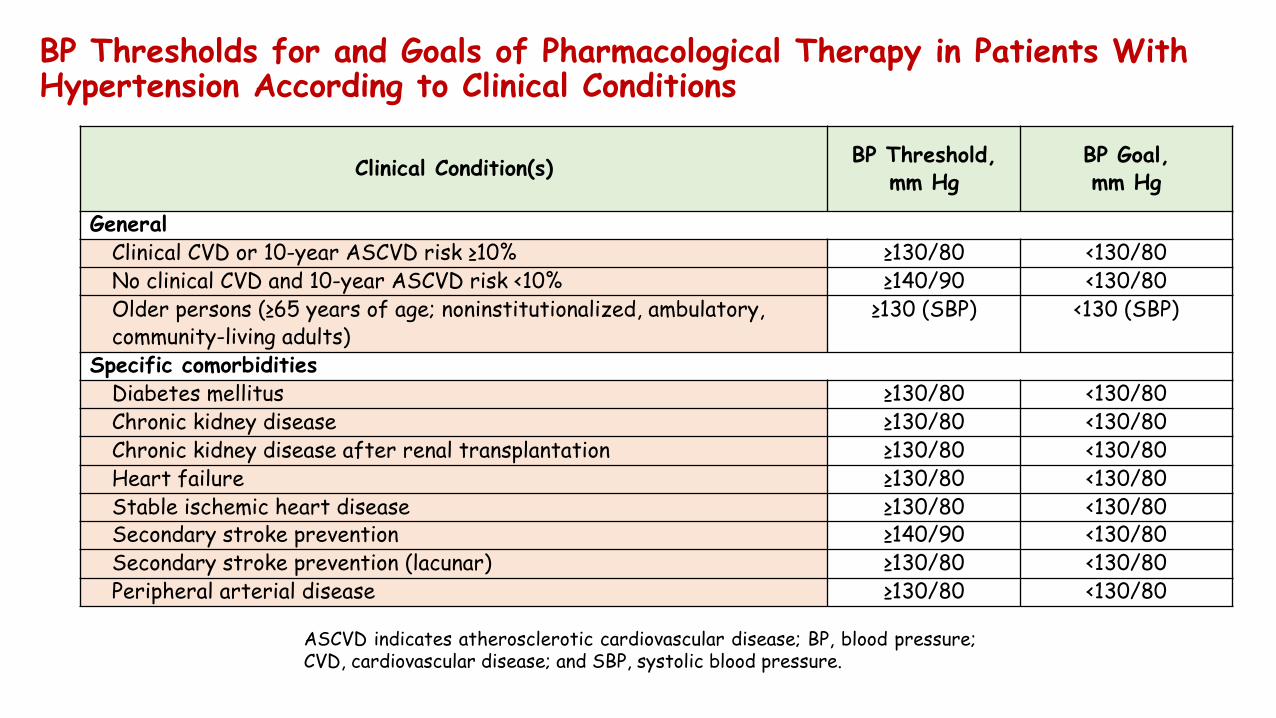
BP Thresholds for and Goals of Pharmacological Therapy in Patients With Hypertension According to Clinical Conditions
Clinical Condition(s) BP Threshold, mm Hg
BP Goal, mm Hg
GeneralClinical CVD or 10-year ASCVD risk ≥10% ≥130/80 <130/80No clinical CVD and 10-year ASCVD risk <10% ≥140/90 <130/80Older persons (≥65 years of age; noninstitutionalized, ambulatory, community-living adults)
≥130 (SBP) <130 (SBP)
Specific comorbiditiesDiabetes mellitus ≥130/80 <130/80Chronic kidney disease ≥130/80 <130/80Chronic kidney disease after renal transplantation ≥130/80 <130/80Heart failure ≥130/80 <130/80Stable ischemic heart disease ≥130/80 <130/80Secondary stroke prevention ≥140/90 <130/80Secondary stroke prevention (lacunar) ≥130/80 <130/80Peripheral arterial disease ≥130/80 <130/80
ASCVD indicates atherosclerotic cardiovascular disease; BP, blood pressure;CVD, cardiovascular disease; and SBP, systolic blood pressure.
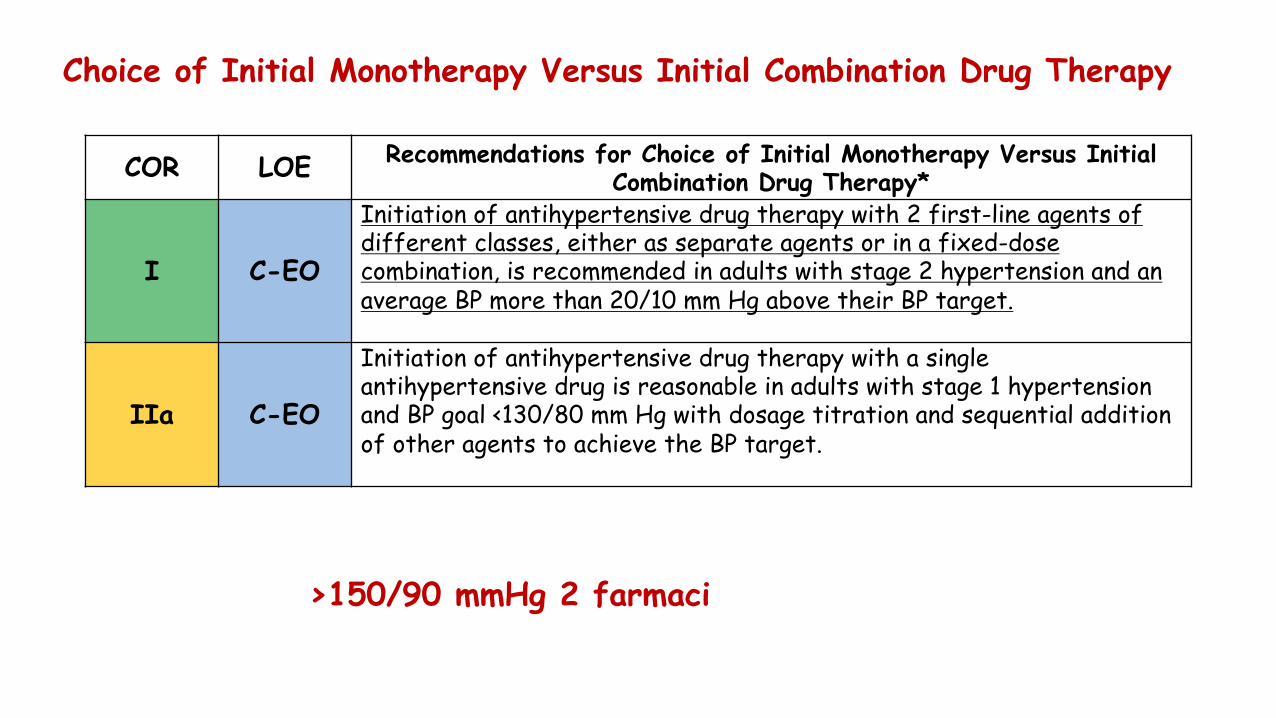
Choice of Initial Monotherapy Versus Initial Combination Drug Therapy
COR LOE Recommendations for Choice of Initial Monotherapy Versus Initial Combination Drug Therapy*
I C-EO
Initiation of antihypertensive drug therapy with 2 first-line agents of different classes, either as separate agents or in a fixed-dose combination, is recommended in adults with stage 2 hypertension and an average BP more than 20/10 mm Hg above their BP target.
IIa C-EO
Initiation of antihypertensive drug therapy with a single antihypertensive drug is reasonable in adults with stage 1 hypertension and BP goal <130/80 mm Hg with dosage titration and sequential addition of other agents to achieve the BP target.
>150/90 mmHg 2 farmaci
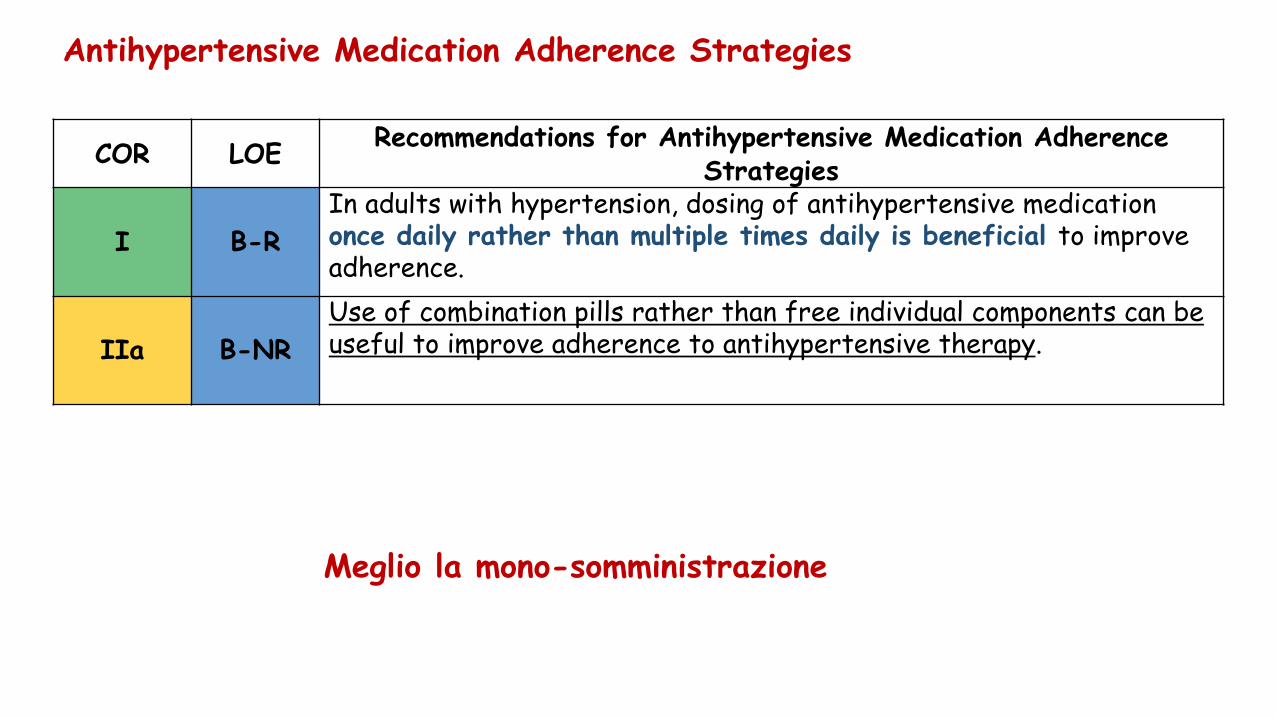
Antihypertensive Medication Adherence Strategies
COR LOE Recommendations for Antihypertensive Medication Adherence Strategies
I B-RIn adults with hypertension, dosing of antihypertensive medication once daily rather than multiple times daily is beneficial to improve adherence.
IIa B-NRUse of combination pills rather than free individual components can be useful to improve adherence to antihypertensive therapy.
Meglio la mono-somministrazione
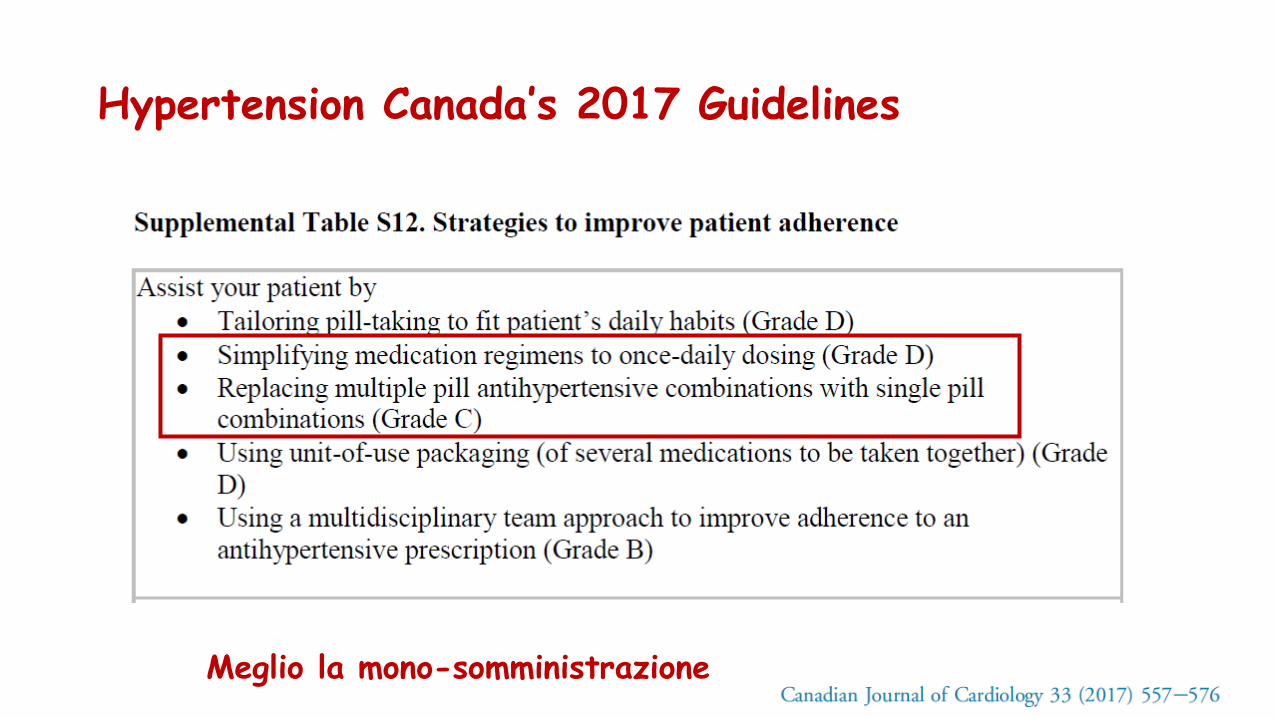
Hypertension Canada’s 2017 Guidelines
Meglio la mono-somministrazione
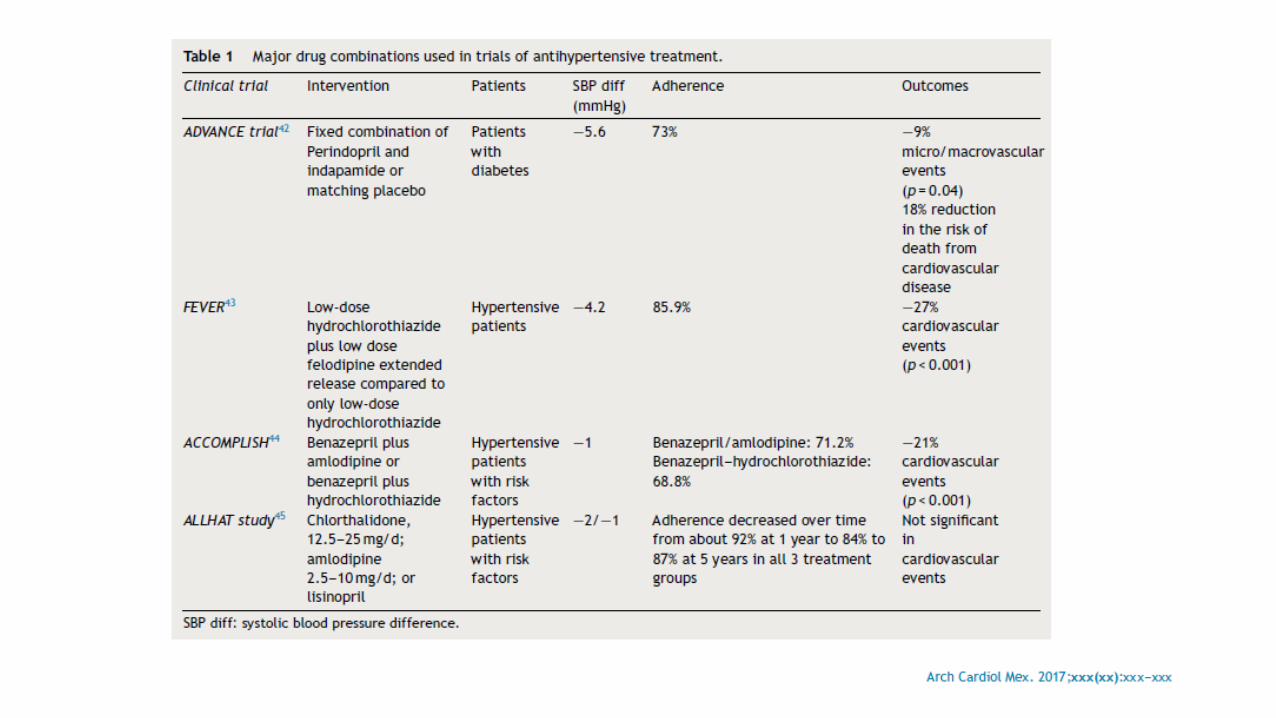
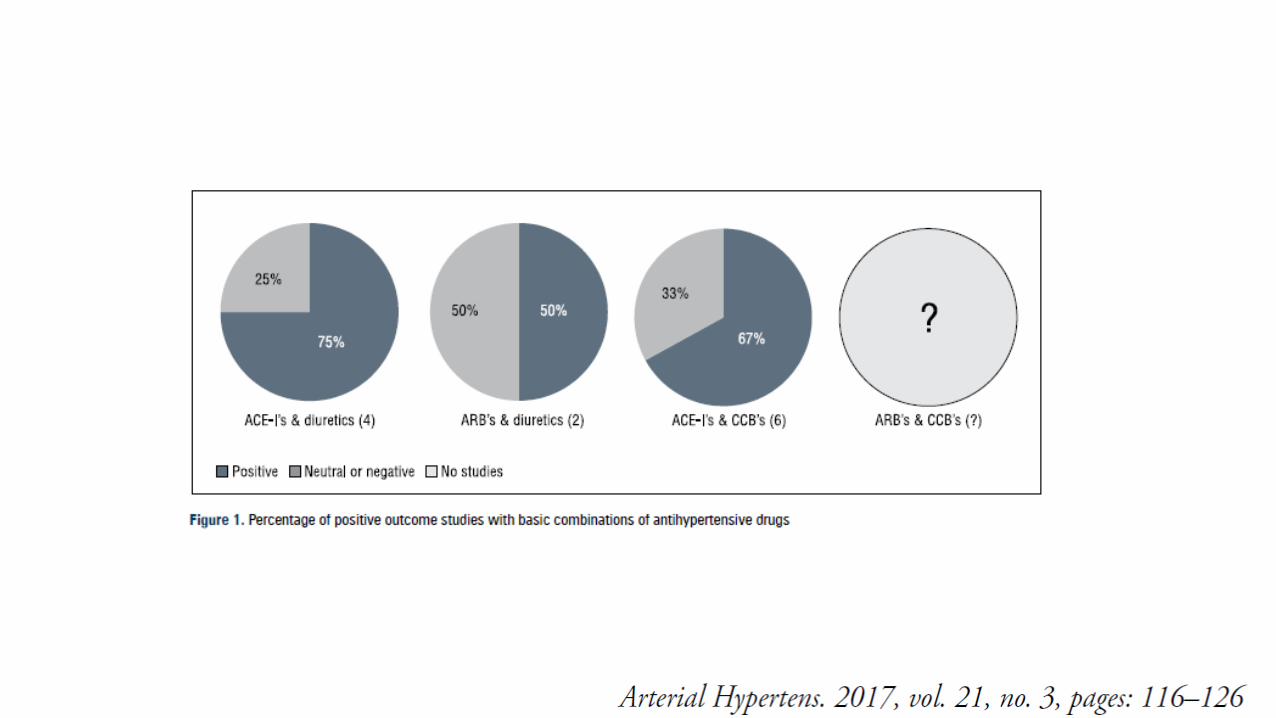
I vantaggi della terapia di associazione
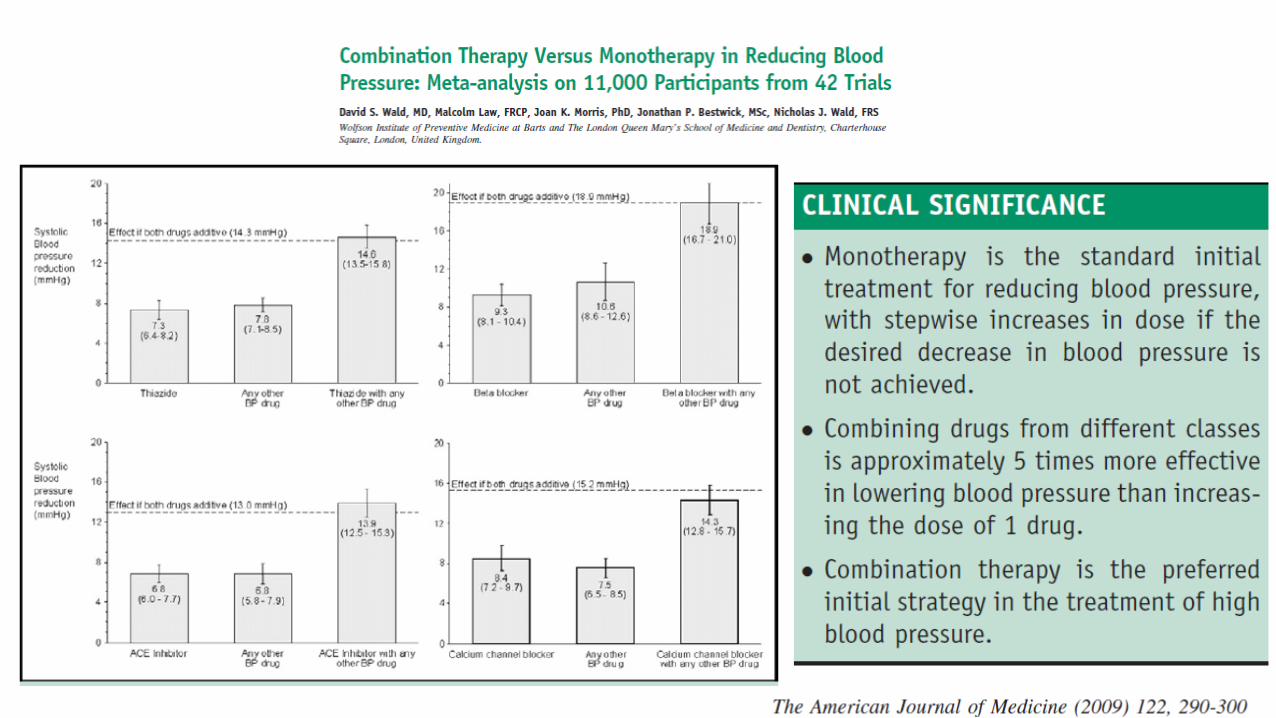
• Una metanalisi di più di 40 studi ha dimostrato che la combinazione di due farmaci
antipertensivi ha un’efficacia superiore a quanto ottenuto con l’incremento del dosaggio
di un singolo farmaco.
• Il vantaggio di iniziare la terapia con l’impiego di un’associazione risiede nel fatto che è
possibile ottenere una pronta risposta in un gran numero di pazienti (con un potenziale
beneficio nei pazienti ad alto rischio), una maggiore probabilità di raggiungere il target
pressorio in pazienti con elevati valori di partenza, e una minor probabilità di ridurre la
compliance dei pazienti con molte modifiche terapeutiche.
• E’ stato dimostrato che i pazienti che assumono una terapia di associazione hanno una
minor probabilità di andare incontro all’interruzione del trattamento
Altri potenziali vantaggi
• Attivazione di multipli meccanismi nel determinismo della riduzione
pressoria
• Evitare l’effetto ottundimento legato a meccanismi di compenso
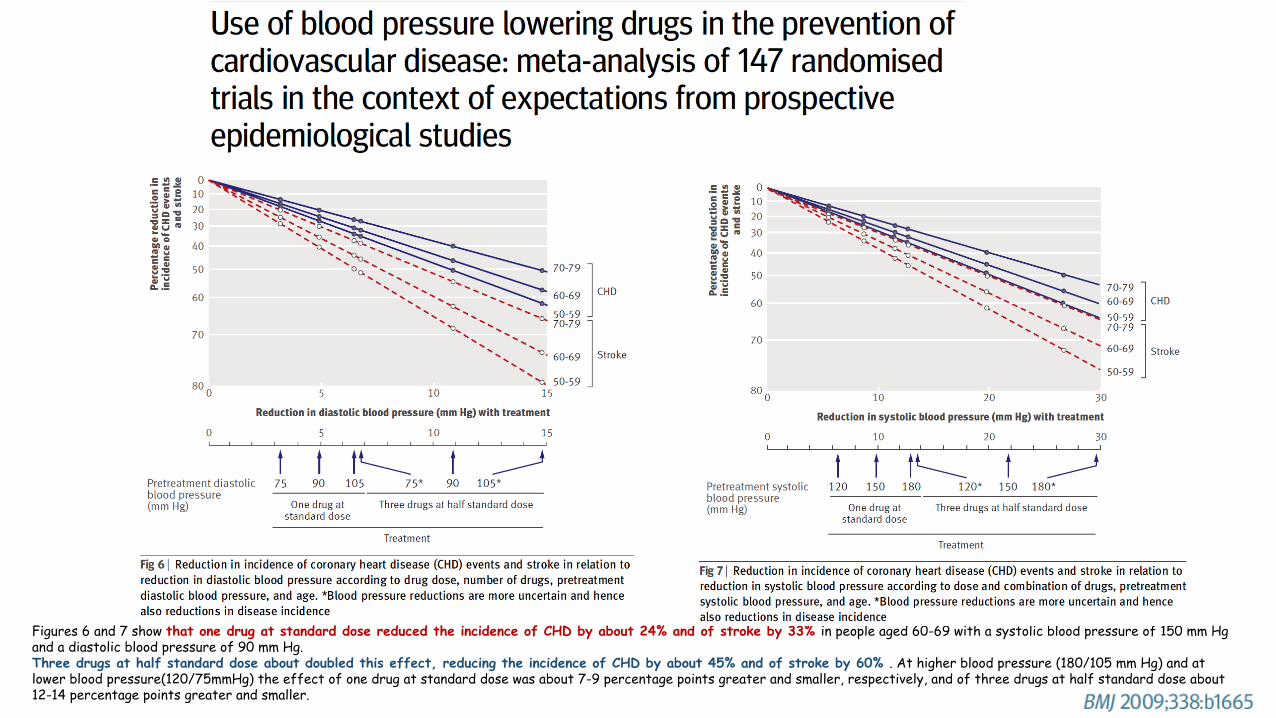
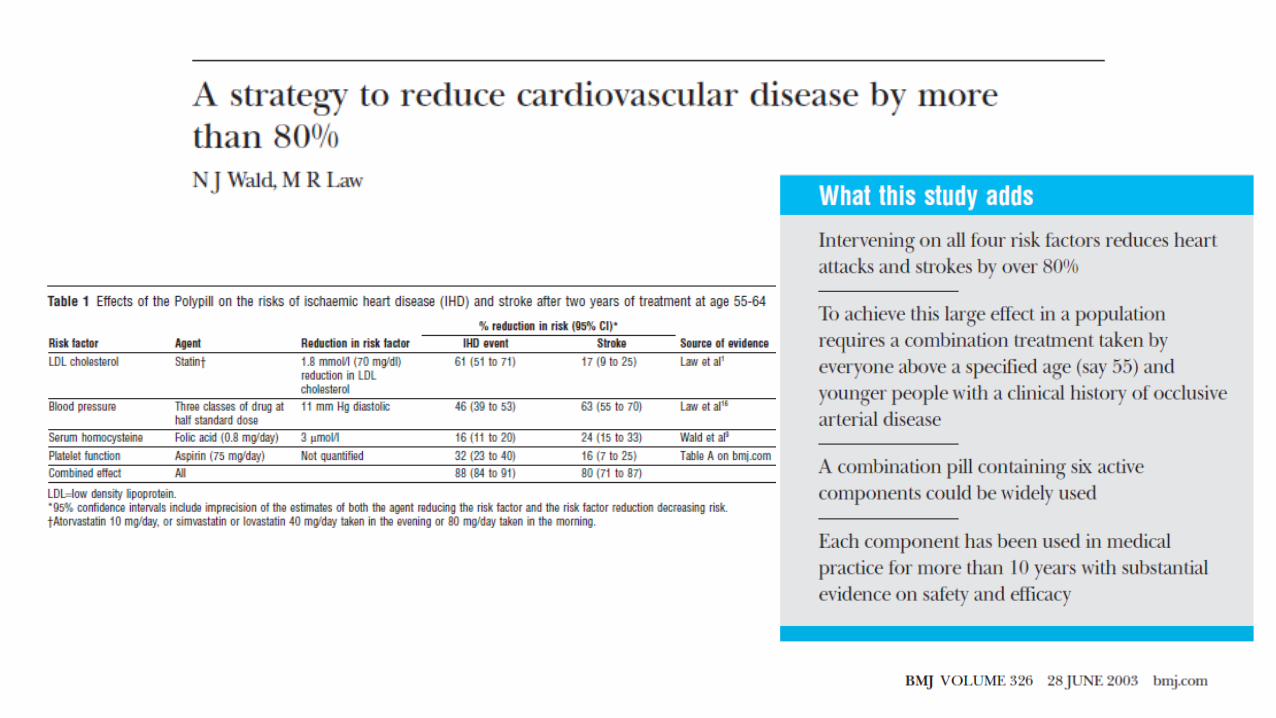
Figures 6 and 7 show that one drug at standard dose reduced the incidence of CHD by about 24% and of stroke by 33% in people aged 60-69 with a systolic blood pressure of 150 mm Hg and a diastolic blood pressure of 90 mm Hg. Three drugs at half standard dose about doubled this effect, reducing the incidence of CHD by about 45% and of stroke by 60% . At higher blood pressure (180/105 mm Hg) and atlower blood pressure(120/75mmHg) the effect of one drug at standard dose was about 7-9 percentage points greater and smaller, respectively, and of three drugs at half standard dose about12-14 percentage points greater and smaller.
Gli svantaggi della terapia di associazione
• Il vantaggio di iniziare il trattamento con la monoterapia risiede nel
fatto che usando un singolo farmaco si è in grado di valutarne
l’efficacia e gli aventi avversi
• Lo svantaggio di iniziare con una terapia di associazione è
rappresentato dal fatto che uno dei due farmaci impiegati può essere
inefficace
• L’aderenza alla terapia nel mondo è generalmente bassa e questo rappresenta ilmaggior determinante all’incremento del rischio cardio-vascolare
• L’aderenza è inversamente proporzionale alla complessità dei trattamentifarmacologici e migliora notevolmente dalla semplificazione degli stessi
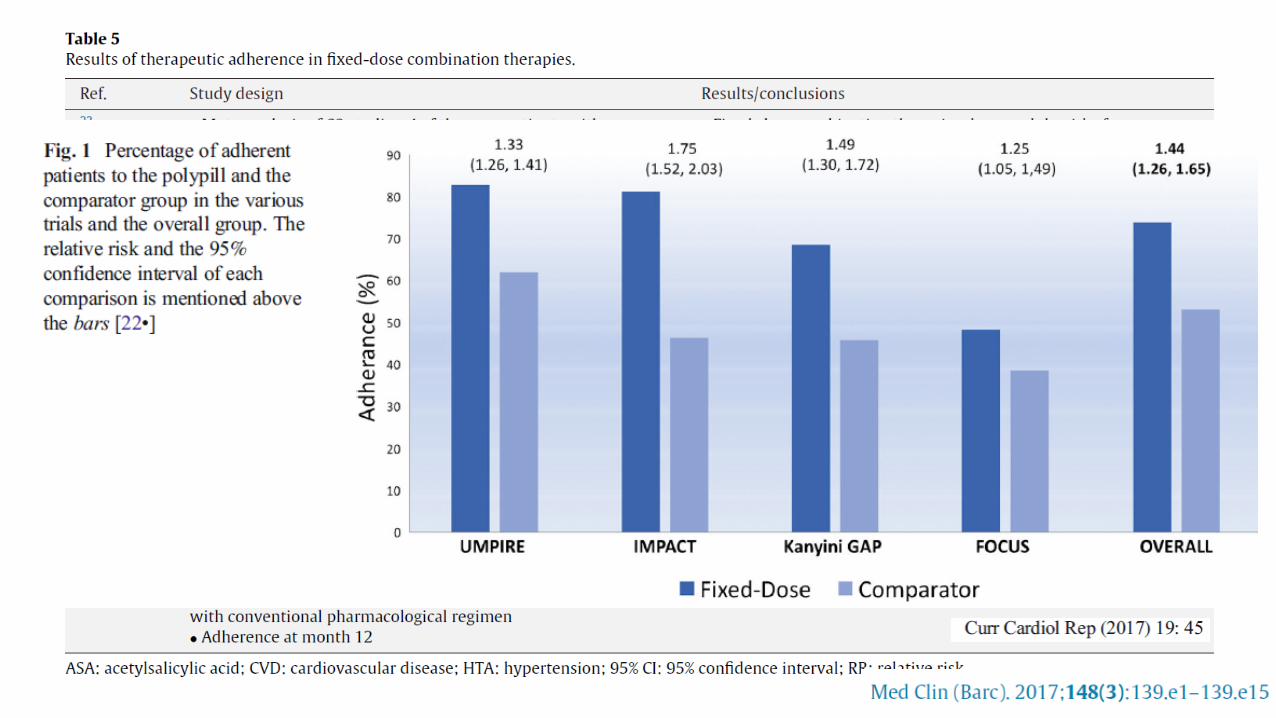
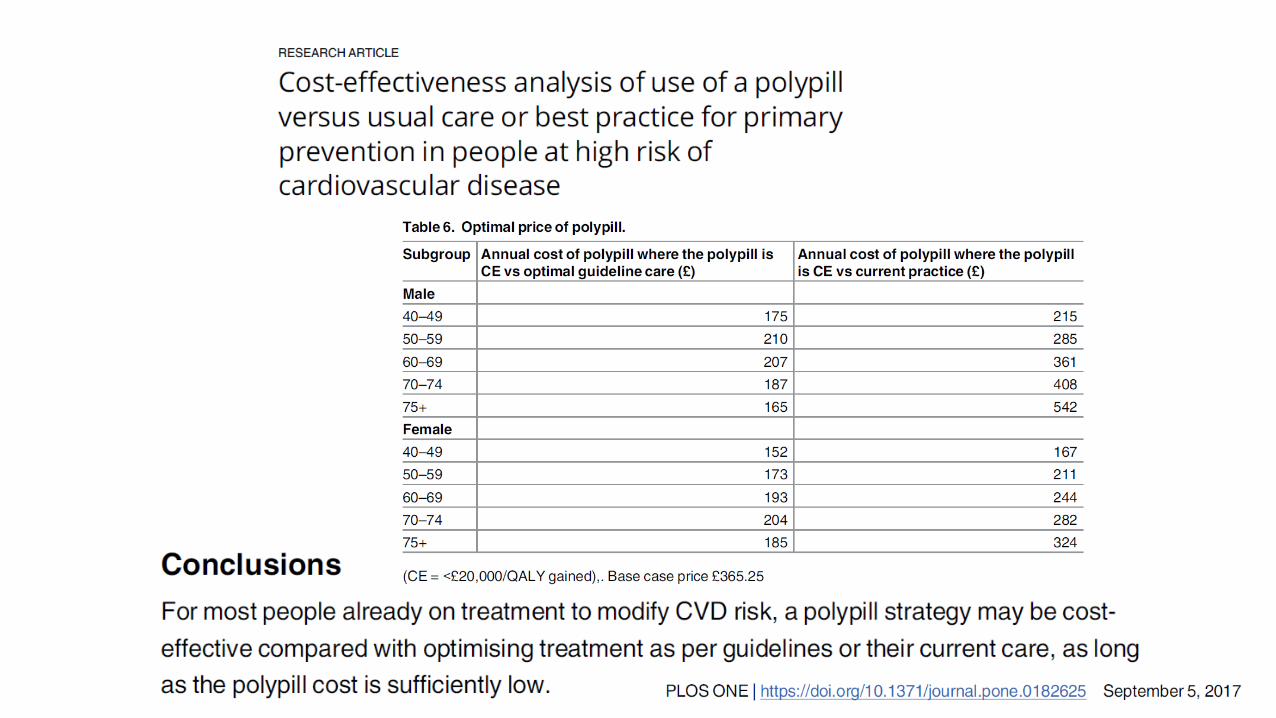
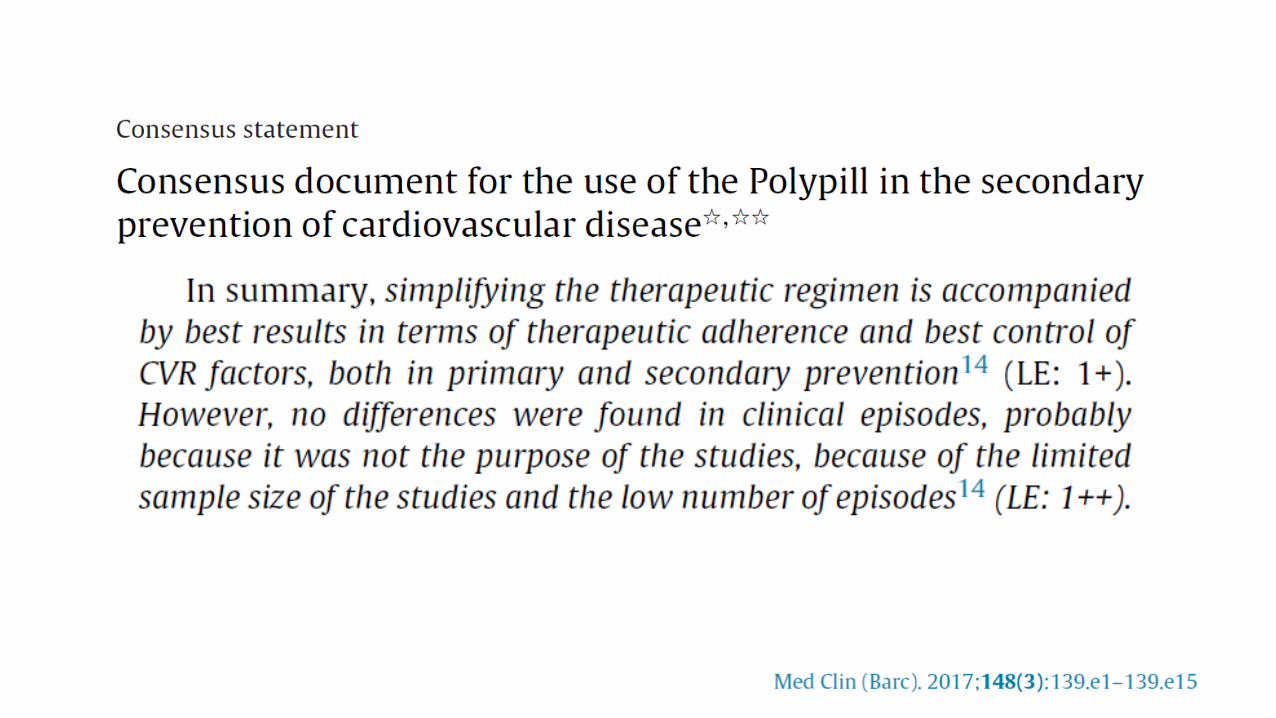
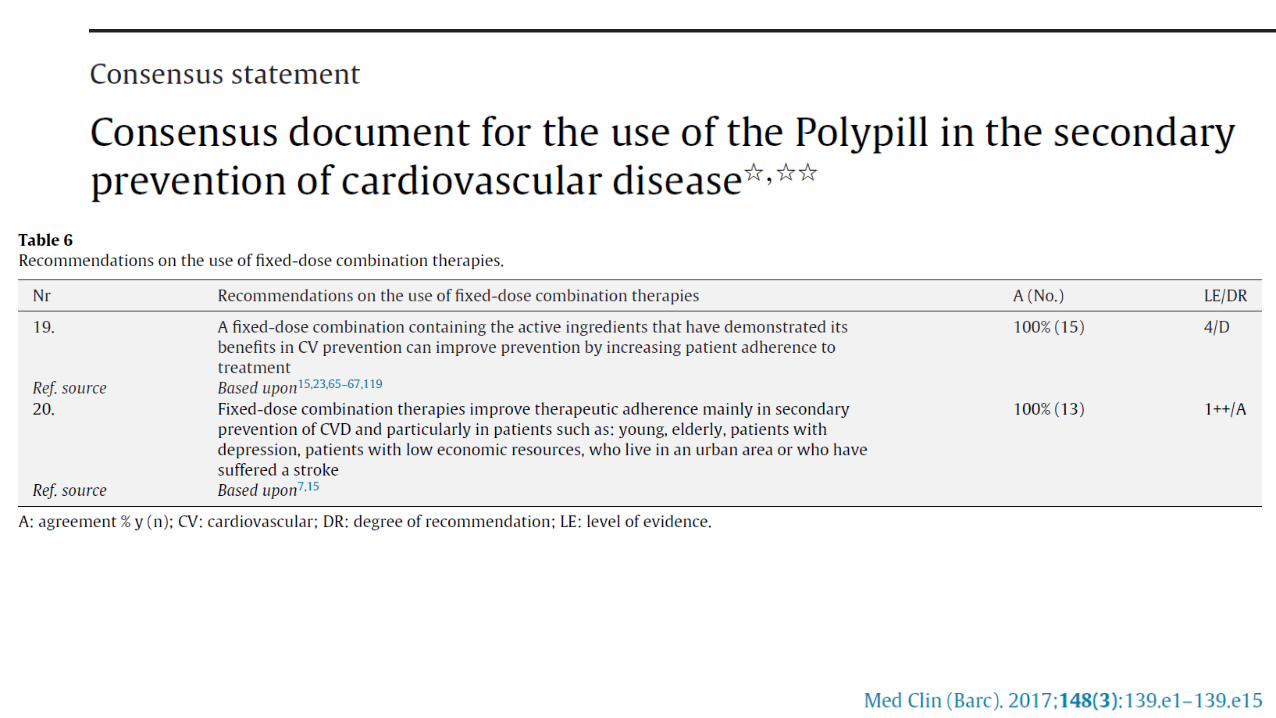
• Recenti studi hanno dimostrato che differenti farmaci cardiovascolari combinati inun’unica compressa, non perdono la loro efficacia individuale o non presentanoinconvenienti inattesi e questo aumenta l’aderenza al trattamento e il controllo dimultipli fattori di rischio, supportando l’uso della polipillola nella prevenzionecardiovascolare secondaria
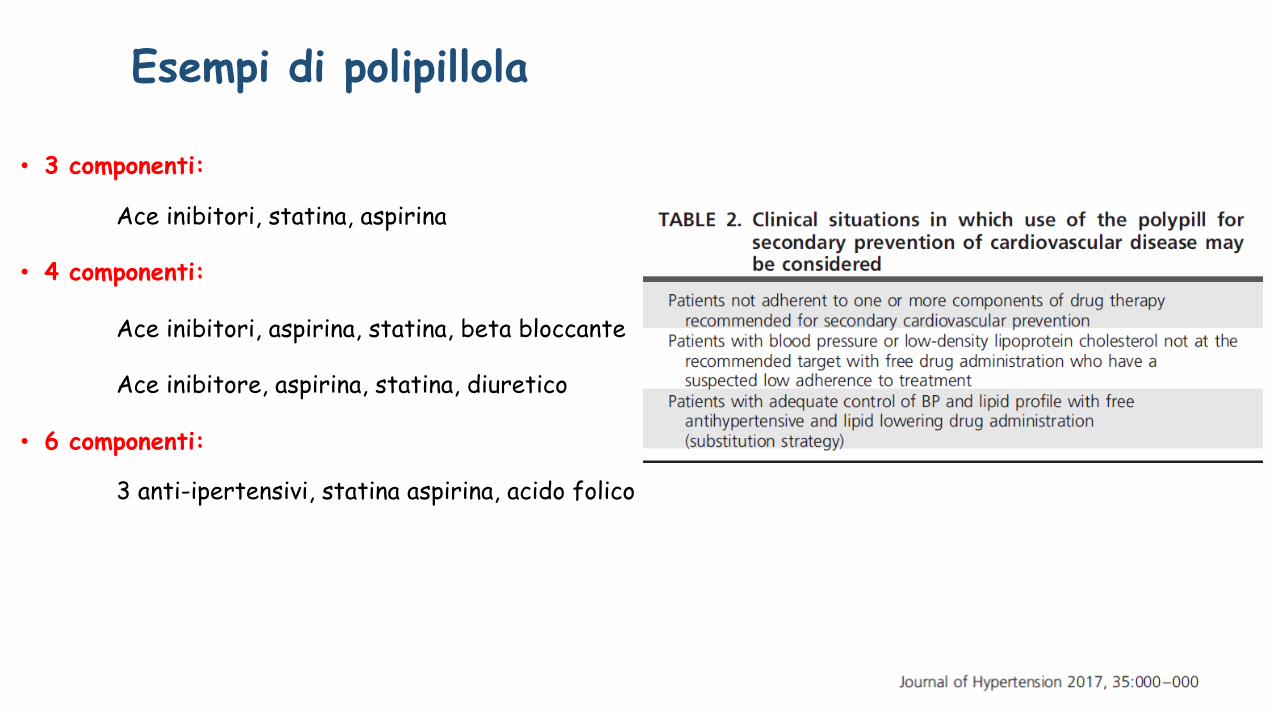
Esempi di polipillola
• 3 componenti:
Ace inibitori, statina, aspirina
• 4 componenti:
Ace inibitori, aspirina, statina, beta bloccante
Ace inibitore, aspirina, statina, diuretico
• 6 componenti:
3 anti-ipertensivi, statina aspirina, acido folico
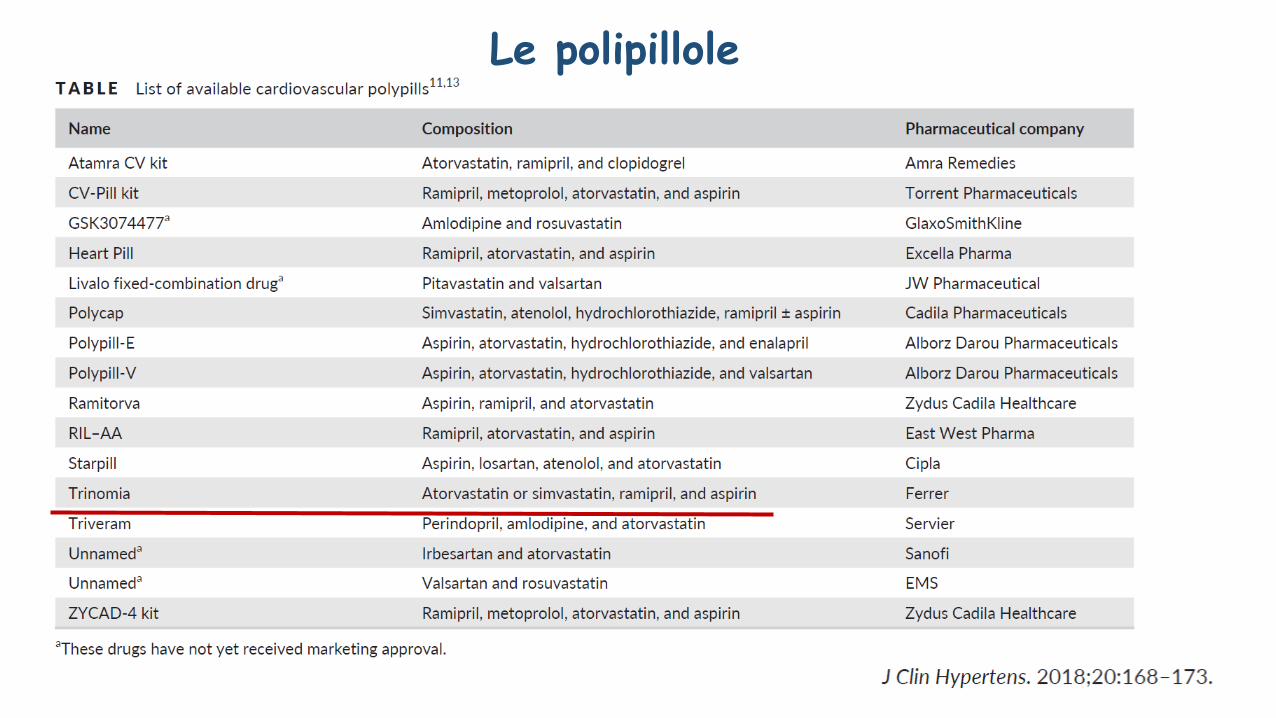
Le polipillole
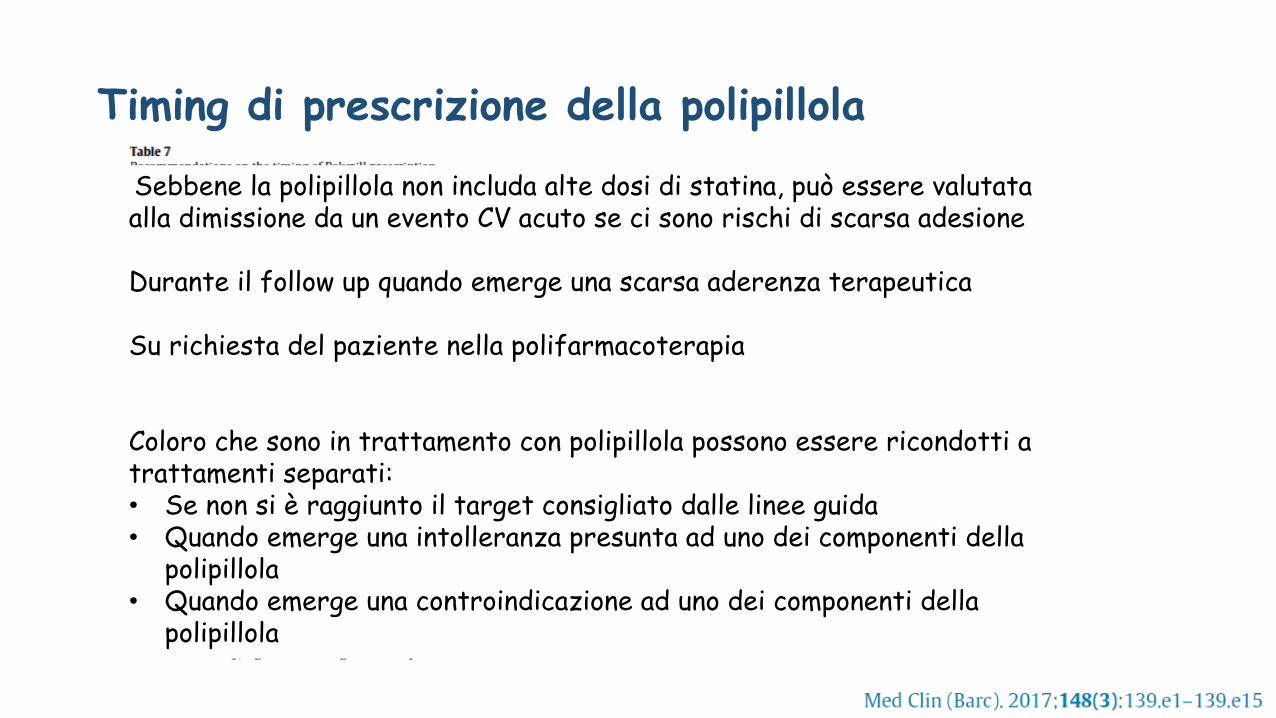
Timing di prescrizione della polipillola
Sebbene la polipillola non includa alte dosi di statina, può essere valutataalla dimissione da un evento CV acuto se ci sono rischi di scarsa adesione
Durante il follow up quando emerge una scarsa aderenza terapeutica
Su richiesta del paziente nella polifarmacoterapia
Coloro che sono in trattamento con polipillola possono essere ricondotti a trattamenti separati:• Se non si è raggiunto il target consigliato dalle linee guida• Quando emerge una intolleranza presunta ad uno dei componenti della
polipillola• Quando emerge una controindicazione ad uno dei componenti della
polipillola
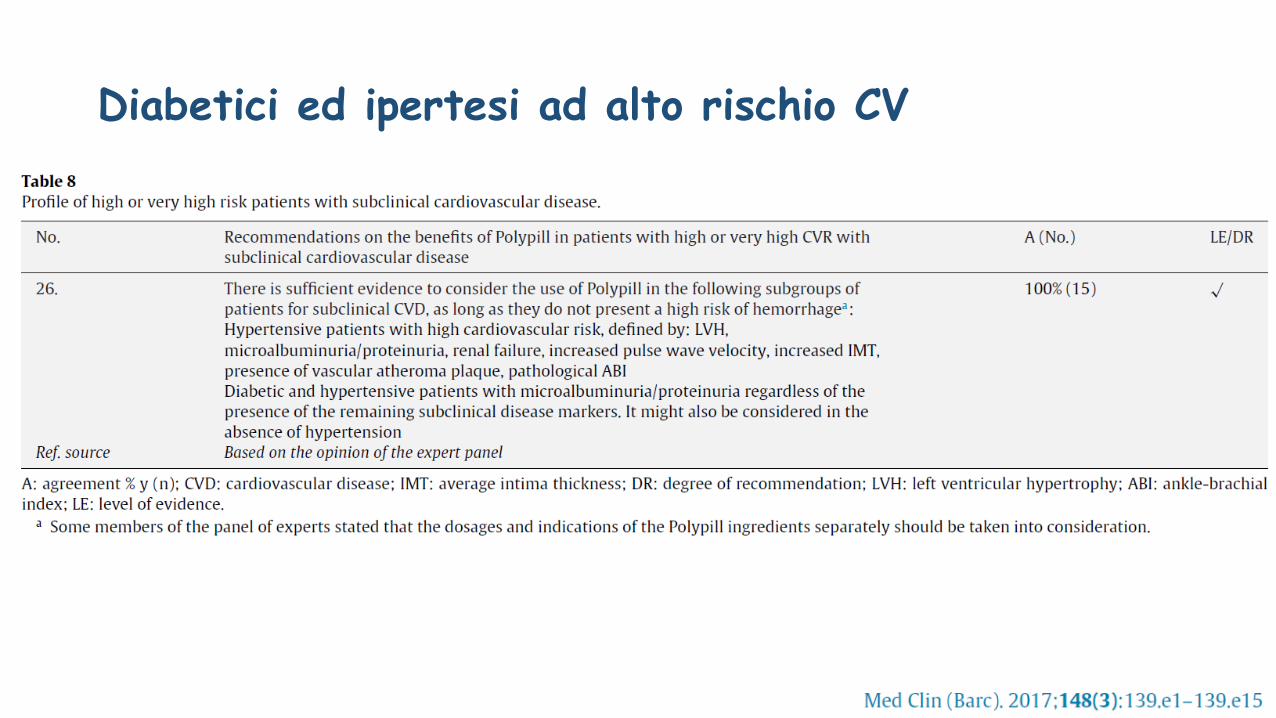
Diabetici ed ipertesi ad alto rischio CV
Contro la polipillola
• Titolazione della dose
• Intolleranza ad uno dei componenti
• Scarsa adesione da parte dei clinici
• Rischio di medicalizzazione di massa
Conclusioni
• L’aderenza alla terapia antipertensiva continua ad essere bassa soprattutto nei
paesi meno sviluppati
• La combinazione di più farmaci è spesso la strategia iniziale per raggiungere
rapidamente il target pressorio
• La terapia di combinazione in una unica compressa, oltre a non perdere l’efficacia
del singolo componente, migliora significativamente la aderenza
• In prevenzione secondaria la polipillola, che contiene principi attivi verso i
principali fattori di rischio CV, migliora la compliance e si suppone possa
migliorare la prognosi

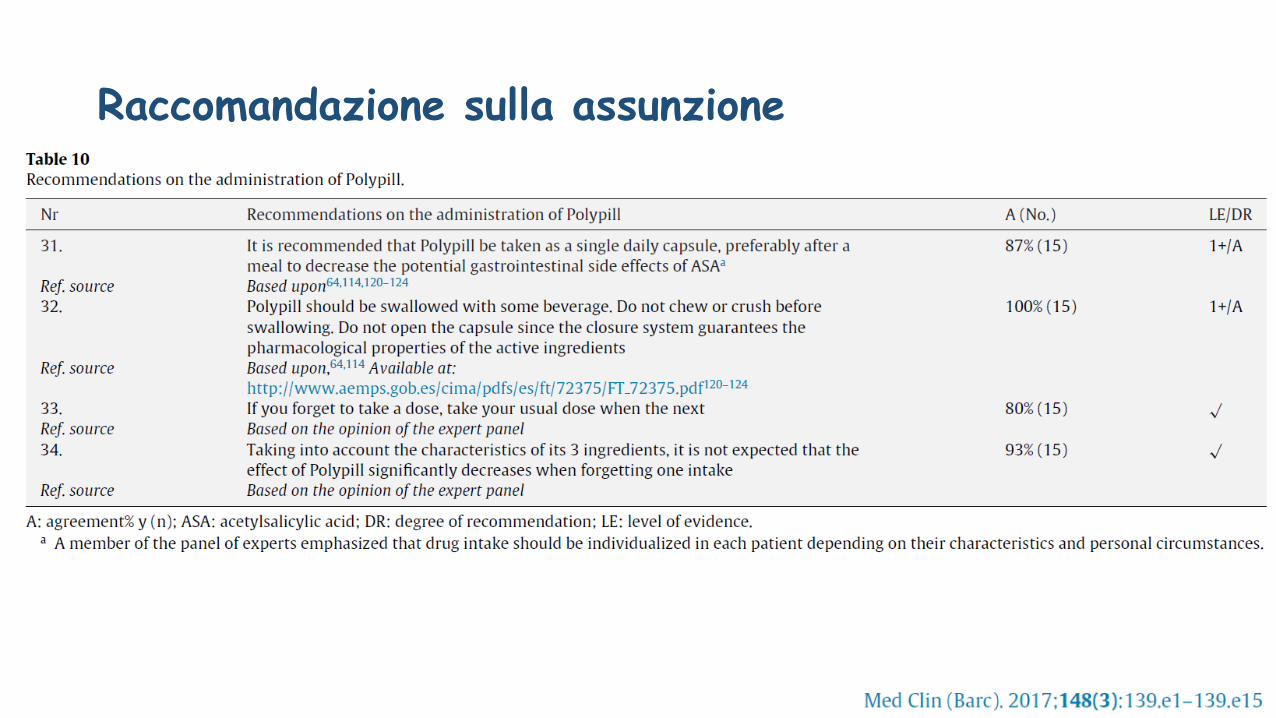
Raccomandazione sulla assunzione
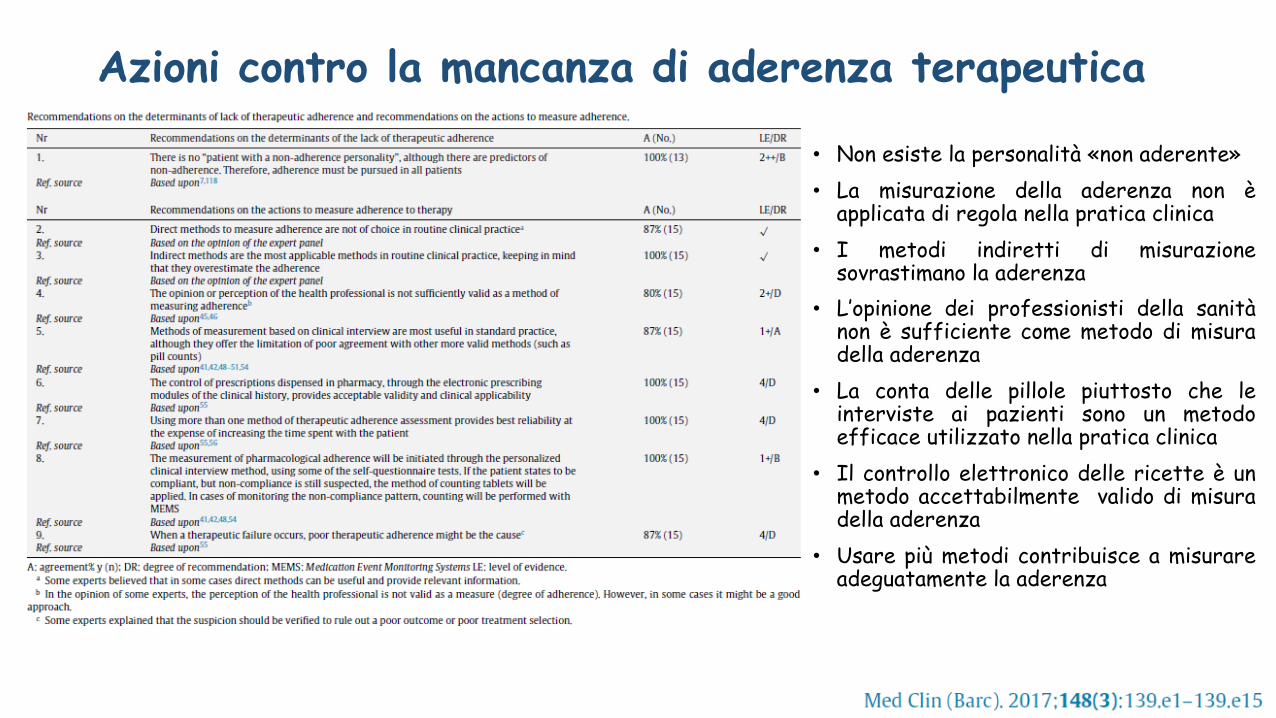
Azioni contro la mancanza di aderenza terapeutica
• Non esiste la personalità «non aderente»• La misurazione della aderenza non è
applicata di regola nella pratica clinica• I metodi indiretti di misurazione
sovrastimano la aderenza• L’opinione dei professionisti della sanità
non è sufficiente come metodo di misuradella aderenza
• La conta delle pillole piuttosto che leinterviste ai pazienti sono un metodoefficace utilizzato nella pratica clinica
• Il controllo elettronico delle ricette è unmetodo accettabilmente valido di misuradella aderenza
• Usare più metodi contribuisce a misurareadeguatamente la aderenza
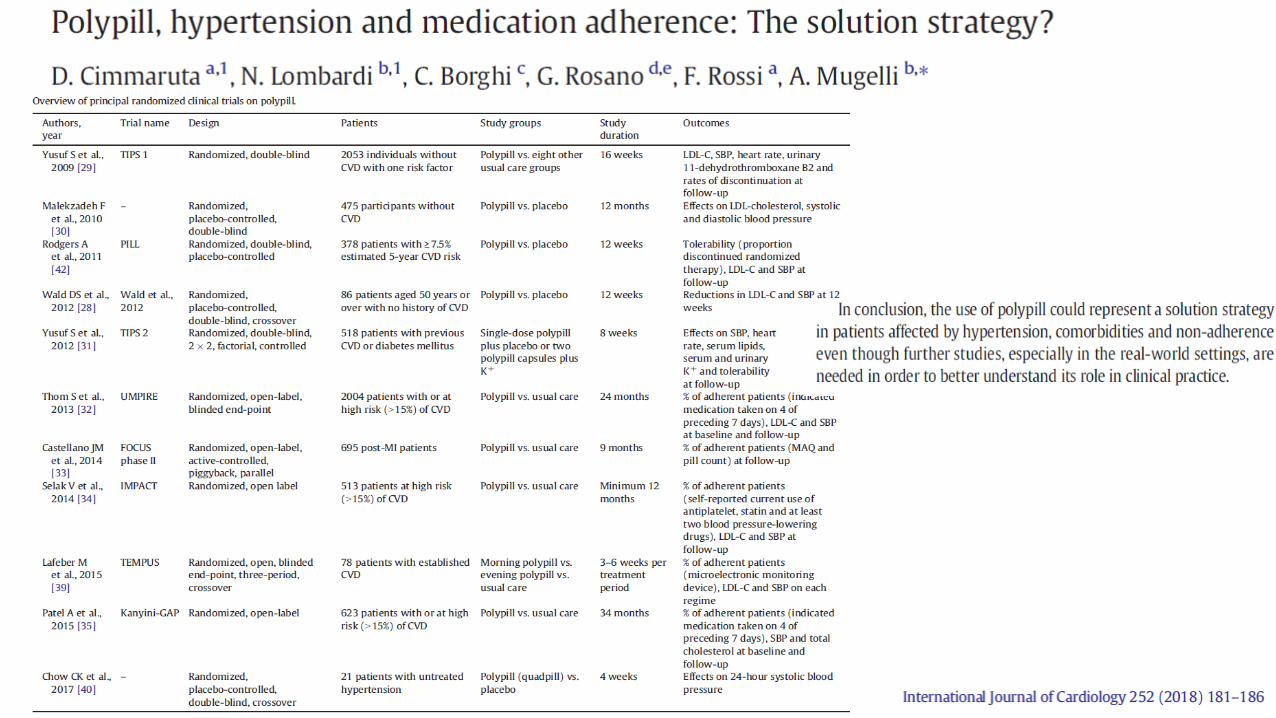
Dalla terapia di associazione alla polipillola
• La cosiddetta polipillola (cioè una combinazione fissa di alcuni antipertensivi
con una statina, una bassa dose di aspirina e talvolta l’acido folico), trova il
razionale nel fatto che il paziente iperteso spesso presenta anche dislipidemia
e frequentemente ha un elevato rischio.
• E’ stato dimostrato che ciascun farmaco, fra quelli associati nella polipillola,
mantiene la maggior parte, se non tutti, gli effetti attesi .
• Si può considerare l’impiego della polipillola una volta che sia stabilita la
necessita di utilizzo di ogni suo componente
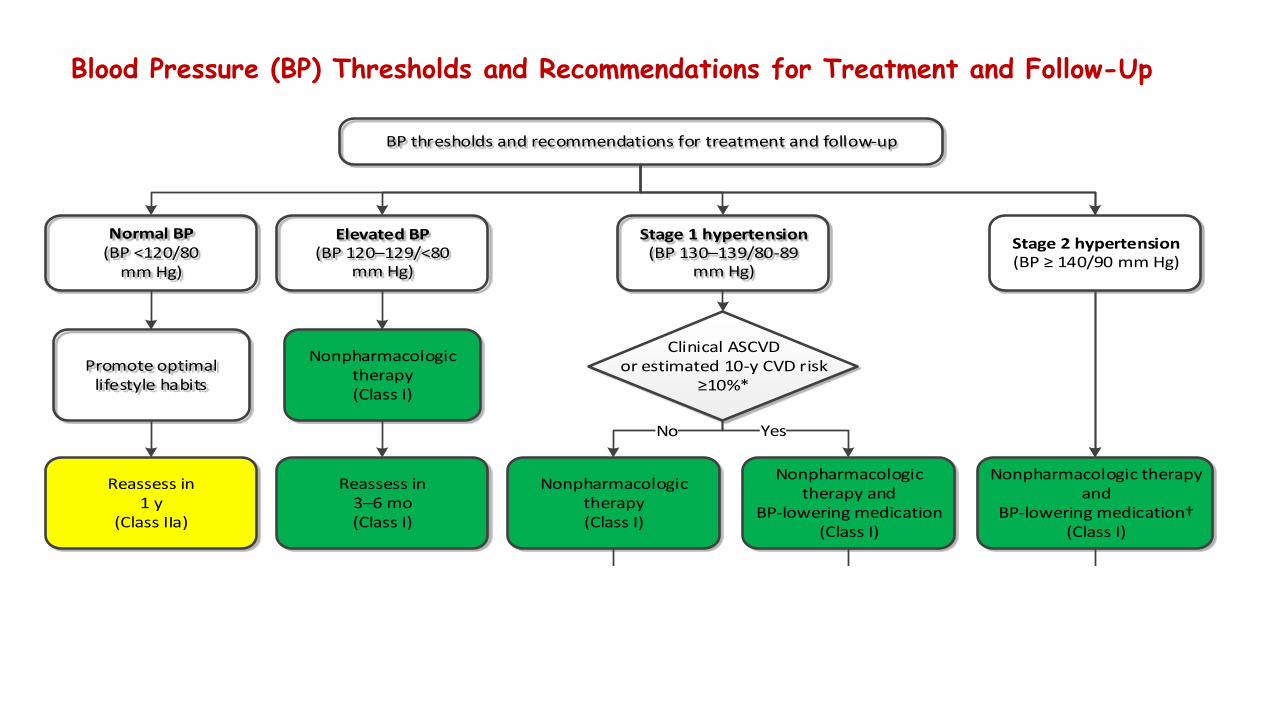
Blood Pressure (BP) Thresholds and Recommendations for Treatment and Follow-Up
Normal BP(BP <120/80
mm Hg)
Promote optimal lifestyle habits
Elevated BP(BP 120–129/<80
mm Hg)
Stage 1 hypertension(BP 130–139/80-89
mm Hg)
Nonpharmacologic therapy(Class I)
Reassess in 3–6 mo(Class I)
BP goal met
No Yes
Reassess in 3–6 mo(Class I)
Assess and optimize
adherence to therapy
Consider intensification of
therapy
Reassess in 1 mo
(Class I)
Nonpharmacologic therapy and
BP-lowering medication(Class I)
Reassess in 1 y
(Class IIa)
Clinical ASCVD or estimated 10-y CVD risk
≥10%*
YesNo
Nonpharmacologic therapy (Class I)
BP thresholds and recommendations for treatment and follow-up
Nonpharmacologic therapy and
BP-lowering medication†(Class I)
Reassess in 3–6 mo(Class I)
Stage 2 hypertension(BP ≥ 140/90 mm Hg)
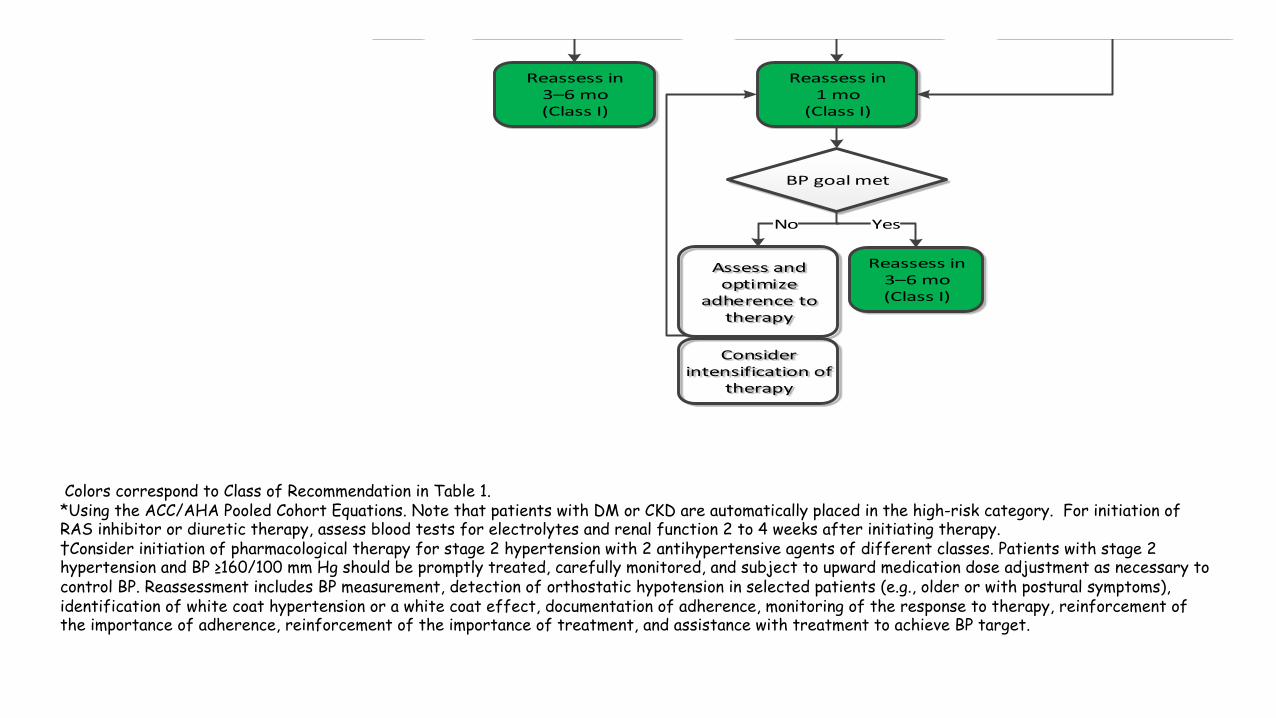
Colors correspond to Class of Recommendation in Table 1.*Using the ACC/AHA Pooled Cohort Equations. Note that patients with DM or CKD are automatically placed in the high-risk category. For initiation of RAS inhibitor or diuretic therapy, assess blood tests for electrolytes and renal function 2 to 4 weeks after initiating therapy.†Consider initiation of pharmacological therapy for stage 2 hypertension with 2 antihypertensive agents of different classes. Patients with stage 2 hypertension and BP ≥160/100 mm Hg should be promptly treated, carefully monitored, and subject to upward medication dose adjustment as necessary to control BP. Reassessment includes BP measurement, detection of orthostatic hypotension in selected patients (e.g., older or with postural symptoms), identification of white coat hypertension or a white coat effect, documentation of adherence, monitoring of the response to therapy, reinforcement of the importance of adherence, reinforcement of the importance of treatment, and assistance with treatment to achieve BP target.
Normal BP(BP <120/80
mm Hg)
Promote optimal lifestyle habits
Elevated BP(BP 120–129/<80
mm Hg)
Stage 1 hypertension(BP 130–139/80-89
mm Hg)
Nonpharmacologic therapy(Class I)
Reassess in 3–6 mo(Class I)
BP goal met
No Yes
Reassess in 3–6 mo(Class I)
Assess and optimize
adherence to therapy
Consider intensification of
therapy
Reassess in 1 mo
(Class I)
Nonpharmacologic therapy and
BP-lowering medication(Class I)
Reassess in 1 y
(Class IIa)
Clinical ASCVD or estimated 10-y CVD risk
≥10%*
YesNo
Nonpharmacologic therapy (Class I)
BP thresholds and recommendations for treatment and follow-up
Nonpharmacologic therapy and
BP-lowering medication†(Class I)
Reassess in 3–6 mo(Class I)
Stage 2 hypertension(BP ≥ 140/90 mm Hg)
Linee guida ESH/ESC 2013
• Sono a favore dell’impiego delle associazioni di due farmaci antipertensivi a dosaggio
fisso in una singola compressa, in modo che sia possibile ridurre il numero di
compresse che devono essere assunte giornalmente, aumentando l’aderenza alla
terapia, che nell’ipertensione è di solito modesta, consentendo così di aumentare la
percentuale di controllo della PA.
• Questo approccio è facilitato dalla disponibilità di differenti combinazioni a
dosaggio fisso degli stessi farmaci compresa l’associazione fissa di tre farmaci
(solitamente un bloccante del RAS, un calcioantagonista e un diuretico.)
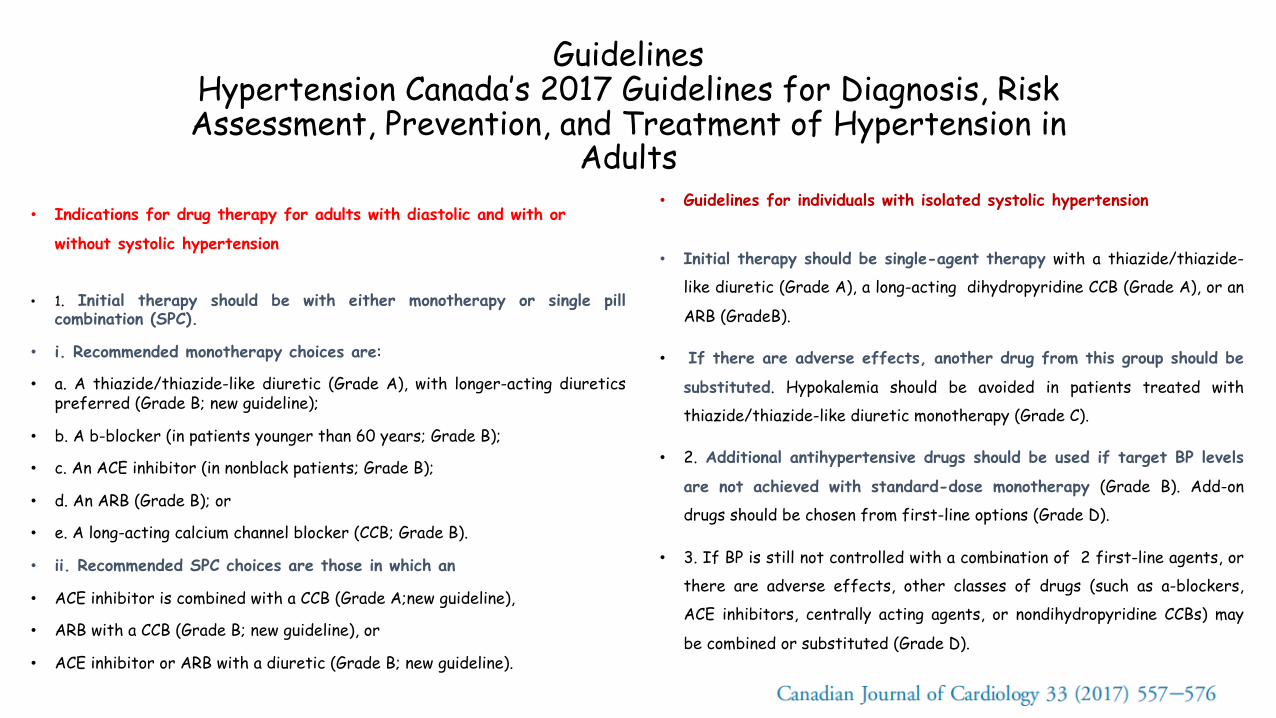
GuidelinesHypertension Canada’s 2017 Guidelines for Diagnosis, RiskAssessment, Prevention, and Treatment of Hypertension in
Adults• Indications for drug therapy for adults with diastolic and with or
without systolic hypertension
• 1. Initial therapy should be with either monotherapy or single pillcombination (SPC).
• i. Recommended monotherapy choices are:
• a. A thiazide/thiazide-like diuretic (Grade A), with longer-acting diureticspreferred (Grade B; new guideline);
• b. A b-blocker (in patients younger than 60 years; Grade B);
• c. An ACE inhibitor (in nonblack patients; Grade B);
• d. An ARB (Grade B); or
• e. A long-acting calcium channel blocker (CCB; Grade B).
• ii. Recommended SPC choices are those in which an
• ACE inhibitor is combined with a CCB (Grade A;new guideline),
• ARB with a CCB (Grade B; new guideline), or
• ACE inhibitor or ARB with a diuretic (Grade B; new guideline).
• Guidelines for individuals with isolated systolic hypertension
• Initial therapy should be single-agent therapy with a thiazide/thiazide-
like diuretic (Grade A), a long-acting dihydropyridine CCB (Grade A), or an
ARB (GradeB).
• If there are adverse effects, another drug from this group should be
substituted. Hypokalemia should be avoided in patients treated with
thiazide/thiazide-like diuretic monotherapy (Grade C).
• 2. Additional antihypertensive drugs should be used if target BP levels
are not achieved with standard-dose monotherapy (Grade B). Add-on
drugs should be chosen from first-line options (Grade D).
• 3. If BP is still not controlled with a combination of 2 first-line agents, or
there are adverse effects, other classes of drugs (such as a-blockers,
ACE inhibitors, centrally acting agents, or nondihydropyridine CCBs) may
be combined or substituted (Grade D).
• ◆ Improved adherence and reduced therapeutic inertiaThe use of single-pill combinations in the treatment of cardiovascular disease has been shown to markedly improve patient adherence,27-31
and improved adherence is associated with greater BP control32,33 and reduced cardiovascular events.34-36 Patients’ perceptions of adverse effects contribute significantly to decisions regarding medication adherence and are frequently listed as the most common concern among patients who are nonadherent to their antihypertensive medication.37 The potential to use lower doses in combination therapy than in monotherapy may help to reduce adverse events and increase adherence to medication regimens.
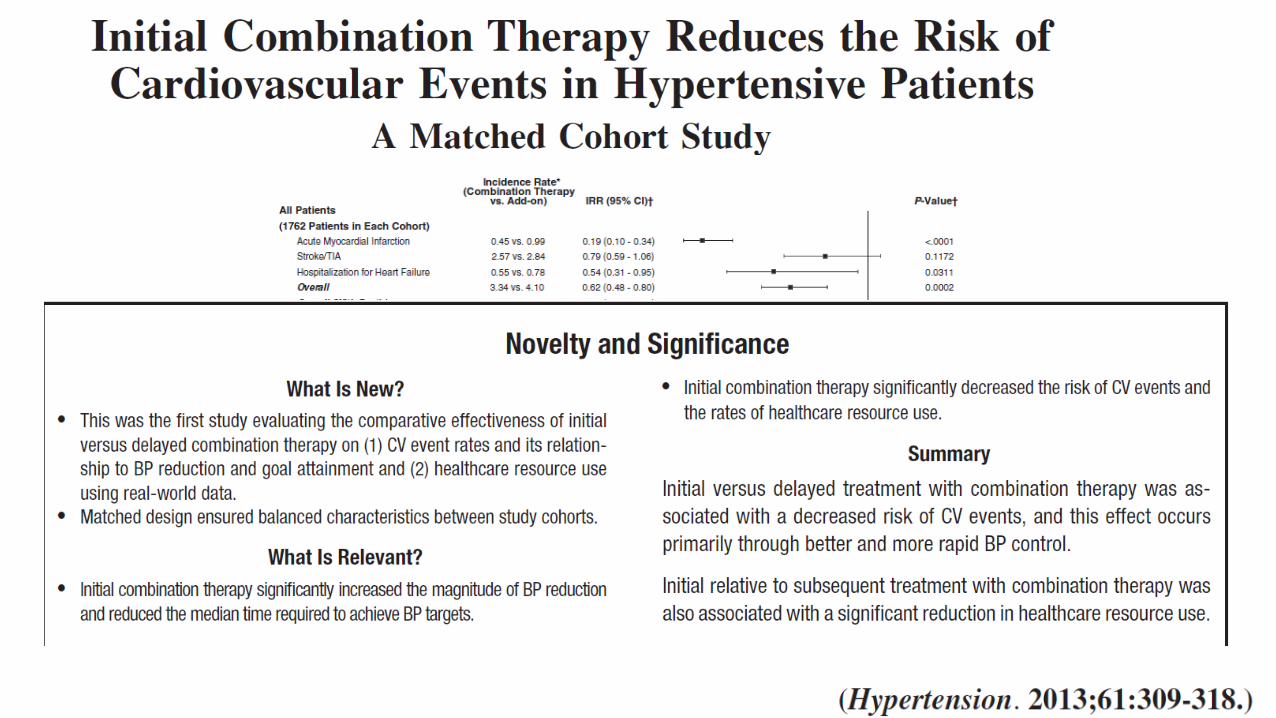
• The findings of Corrao et al are supported by a more recent matched cohort analysis of 1762 adult patients with hypertension, who were either prescribed initial combination therapy or initial monotherapy and later switched to combination therapy.12 Initiation with combination therapy versus monotherapy not only led to faster achievement of BP target (9.7 versus 11.9 months) and more effective BP control (40.3% versus 32.6%), but it was also linked to a 34% reduction in cardiovascular events or death.
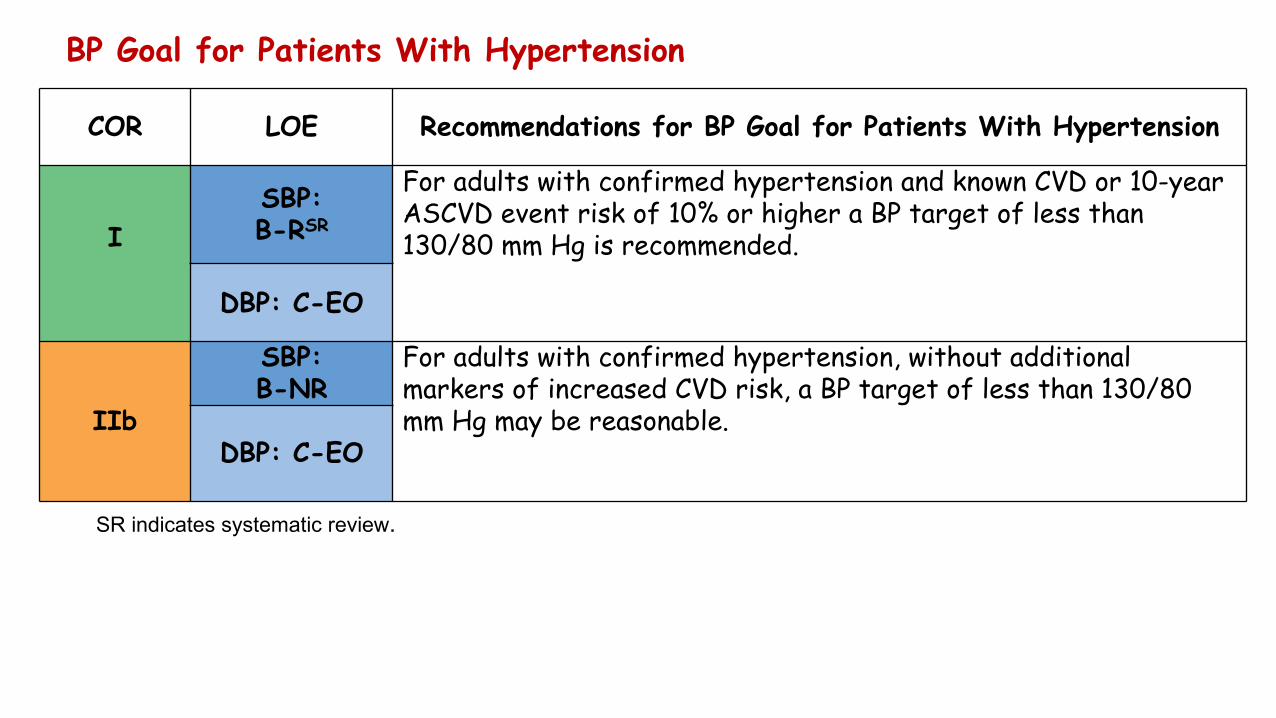
BP Goal for Patients With Hypertension
COR LOE Recommendations for BP Goal for Patients With Hypertension
ISBP:B-RSR
For adults with confirmed hypertension and known CVD or 10-year ASCVD event risk of 10% or higher a BP target of less than 130/80 mm Hg is recommended.
DBP: C-EO
IIb
SBP:B-NR
For adults with confirmed hypertension, without additional markers of increased CVD risk, a BP target of less than 130/80 mm Hg may be reasonable.
DBP: C-EO
SR indicates systematic review.
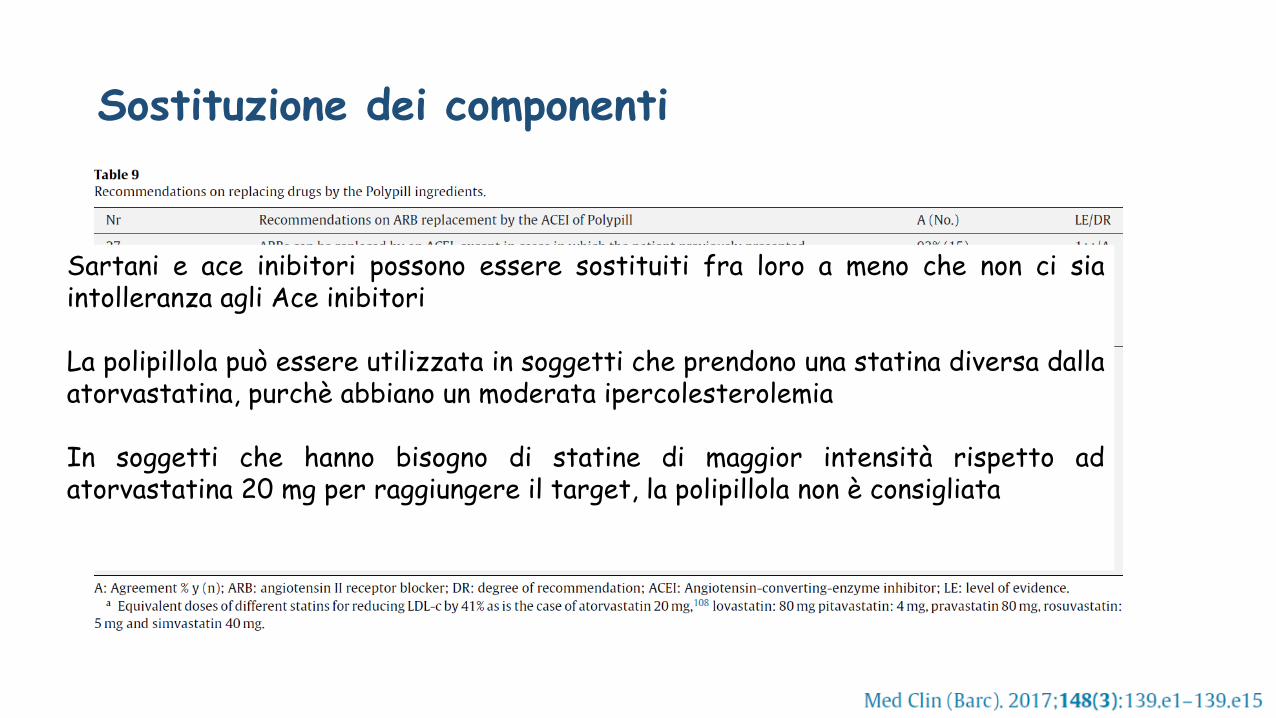
Sostituzione dei componenti
Sartani e ace inibitori possono essere sostituiti fra loro a meno che non ci siaintolleranza agli Ace inibitori
La polipillola può essere utilizzata in soggetti che prendono una statina diversa dallaatorvastatina, purchè abbiano un moderata ipercolesterolemia
In soggetti che hanno bisogno di statine di maggior intensità rispetto adatorvastatina 20 mg per raggiungere il target, la polipillola non è consigliata