Curiosare fra le raccomandazioni delle Linee Guida ESC ... · PDF fileLinee Guida ESC 2014...
23
Curiosare fra le raccomandazioni delle Linee Guida ESC 2014 sulla rivascolarizzazione miocardica Marco Comeglio UO Diagnostica e Interventistica Cardiovascolare Asl 3 Pistoia Curiosare fra le raccomandazioni delle Curiosare fra le raccomandazioni delle Linee Guida ESC 2014 Linee Guida ESC 2014 sulla rivascolarizzazione miocardica sulla rivascolarizzazione miocardica Marco Comeglio Marco Comeglio UO Diagnostica e Interventistica Cardiovascolare UO Diagnostica e Interventistica Cardiovascolare Asl 3 Pistoia Asl 3 Pistoia L’uomo ha un’insaziabile curiosità di conoscere og cosa, eccetto quelle che meritano di essere conosciute Oscar W L L ’ ’ uomo ha un uomo ha un ’ ’ insaziabile insaziabile curiosit curiosit à à di conoscere og di conoscere og cosa, eccetto quelle che cosa, eccetto quelle che meritano di essere meritano di essere conosciute conosciute Oscar W Oscar W
Transcript of Curiosare fra le raccomandazioni delle Linee Guida ESC ... · PDF fileLinee Guida ESC 2014...

Curiosare fra le raccomandazioni delle
Linee Guida ESC 2014
sulla rivascolarizzazione miocardica
Marco Comeglio
UO Diagnostica e Interventistica Cardiovascolare
Asl 3 Pistoia
Curiosare fra le raccomandazioni delleCuriosare fra le raccomandazioni delle
Linee Guida ESC 2014Linee Guida ESC 2014
sulla rivascolarizzazione miocardicasulla rivascolarizzazione miocardica
Marco ComeglioMarco Comeglio
UO Diagnostica e Interventistica CardiovascolareUO Diagnostica e Interventistica Cardiovascolare
Asl 3 PistoiaAsl 3 Pistoia
L’uomo ha un’insaziabile
curiosità di conoscere ogni
cosa, eccetto quelle che
meritano di essere
conosciuteOscar Wilde
LL’’uomo ha unuomo ha un’’insaziabile insaziabile
curiositcuriositàà di conoscere ogni di conoscere ogni
cosa, eccetto quelle che cosa, eccetto quelle che
meritano di essere meritano di essere
conosciuteconosciuteOscar WildeOscar Wilde
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
Guidelines and recommendations Guidelines and recommendations should should helphelp healthhealth
professionalsprofessionals to make decisions in their daily to make decisions in their daily
practice; however, the practice; however, the final decisions final decisions concerning an concerning an
individual patient individual patient must be made by the must be made by the responsible responsible
health professionalhealth professional(s), in consultation with the (s), in consultation with the
patientpatient……
PreamblePreamble
1.1. Scores and risk stratification Scores and risk stratification
2.2. Process for decisionProcess for decision--making and patient informationmaking and patient information
3.3. Strategies for diagnosis: functional testing and imagingStrategies for diagnosis: functional testing and imaging
4.4. Revascularization for stable coronary artery diseaseRevascularization for stable coronary artery disease
5.5. Revascularization in nonRevascularization in non--STST--segment elevation acute coronary segment elevation acute coronary syndromessyndromes
6.6. Revascularization in STRevascularization in ST--segment elevation myocardial infarctionsegment elevation myocardial infarction
7.7. Revascularization in patients with heart failure and cardiogenicRevascularization in patients with heart failure and cardiogenic shockshock
8.8. Revascularization in patients with diabetesRevascularization in patients with diabetes
9.9. Revascularization in patients with chronic kidney diseaseRevascularization in patients with chronic kidney disease
10.10. Revascularization in patients requiring valve interventionsRevascularization in patients requiring valve interventions
11.11. Associated carotid/peripheral artery diseaseAssociated carotid/peripheral artery disease
12.12. Repeat revascularization and hybrid proceduresRepeat revascularization and hybrid procedures
13.13. ArrhythmiasArrhythmias
14.14. Procedural aspects of coronary artery bypass graftingProcedural aspects of coronary artery bypass grafting
15.15. Procedural aspects of percutaneous coronary interventionProcedural aspects of percutaneous coronary intervention
16.16. Antithrombotic treatmentsAntithrombotic treatments
17.17. Points of interest and special conditionsPoints of interest and special conditions
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
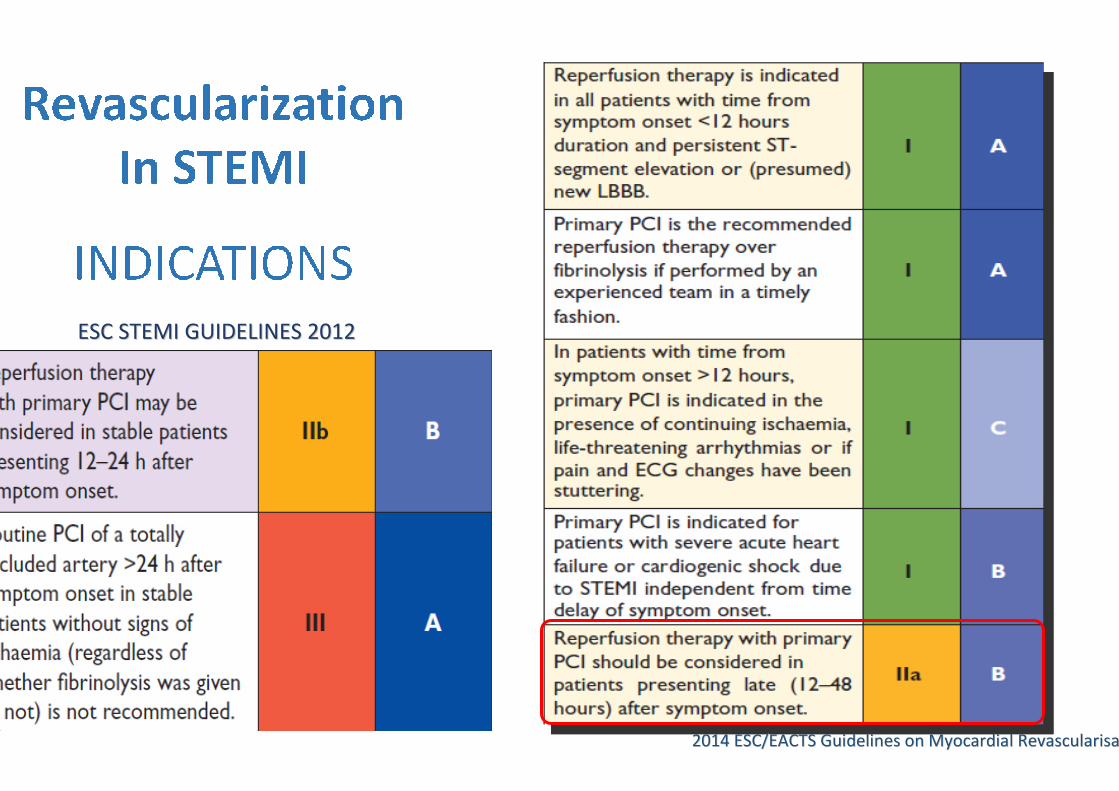
ESC STEMI GUIDELINES 2012ESC STEMI GUIDELINES 2012
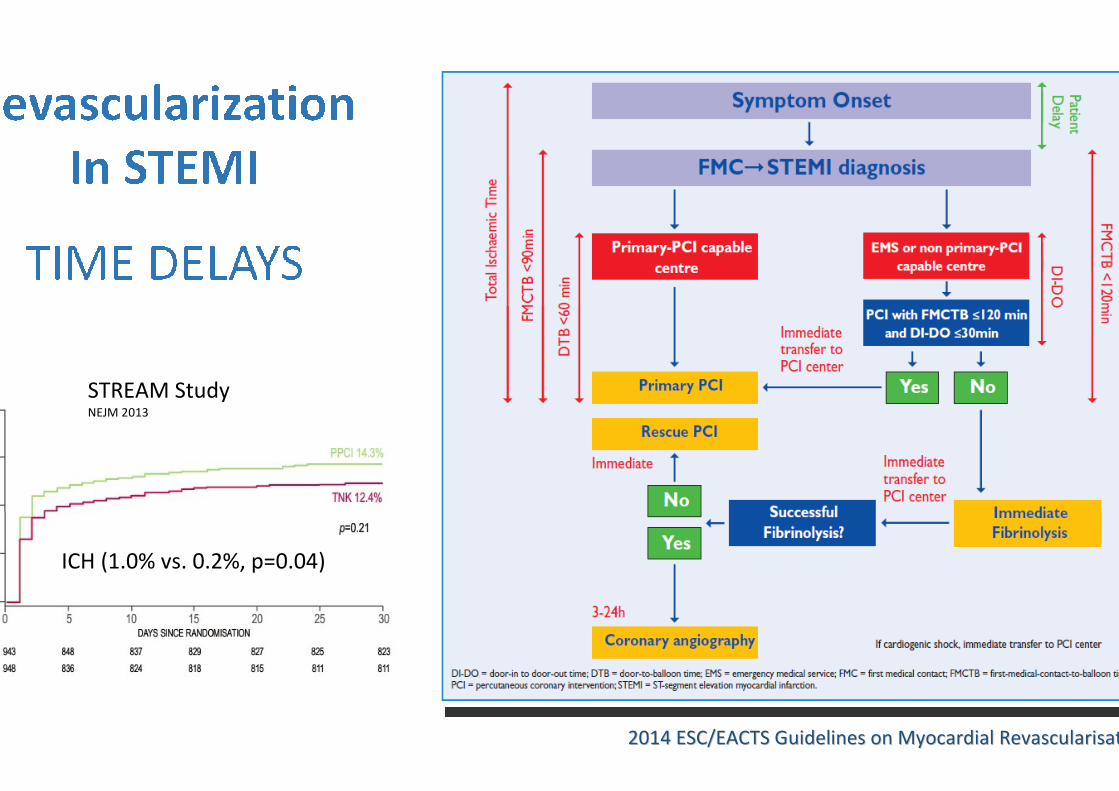
STREAM StudyNEJM 2013
ICH (1.0% vs. 0.2%, p=0.04)
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
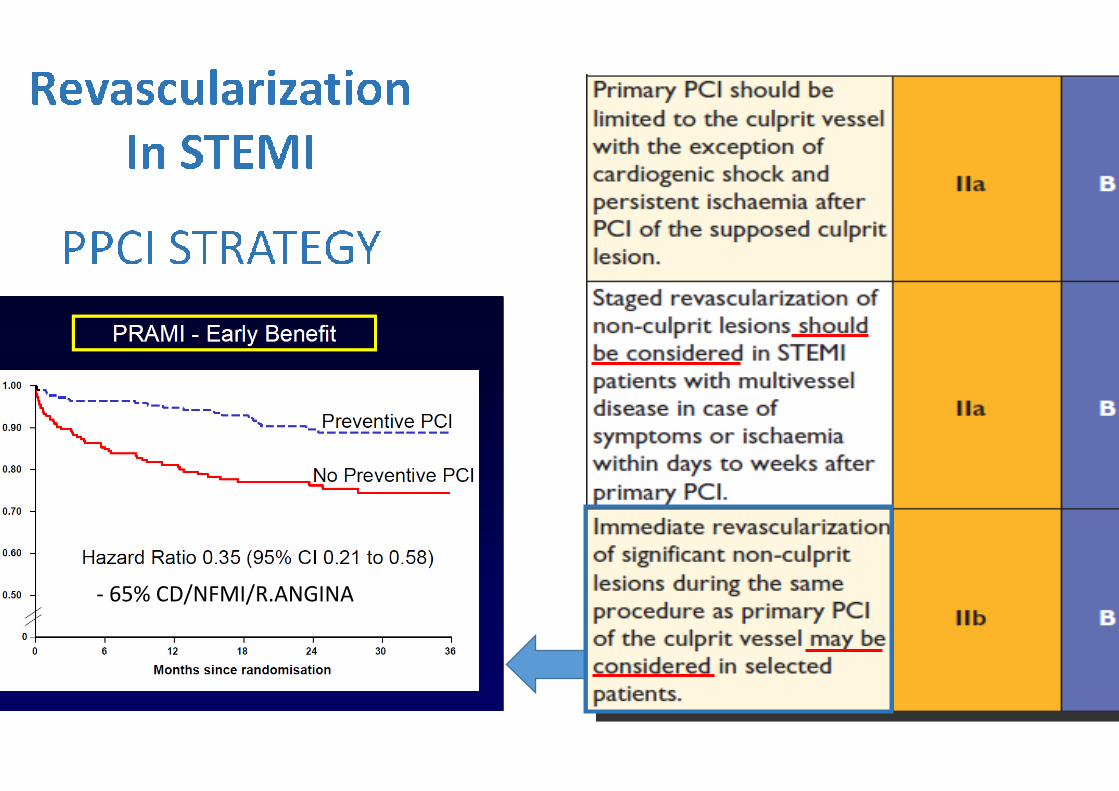
- 65% CD/NFMI/R.ANGINA
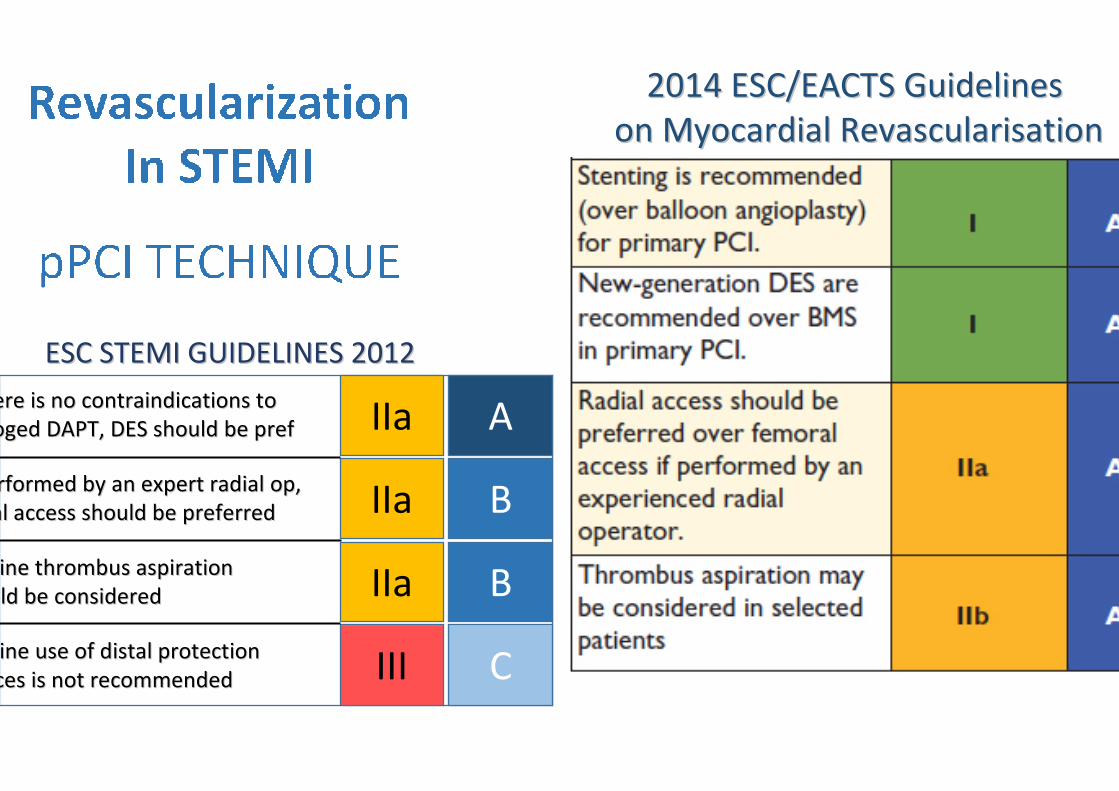
•• DES or BMS ?DES or BMS ?
•• Radial or Femoral ?Radial or Femoral ?
•• Thrombectomy or not ?Thrombectomy or not ?
If there is no contraindications to If there is no contraindications to
prologed DAPT, DES should be prefprologed DAPT, DES should be pref
If performed by an expert radial op, If performed by an expert radial op,
radial access should be preferredradial access should be preferred
Routine thrombus aspiration Routine thrombus aspiration
should be consideredshould be considered
Routine use of distal protection Routine use of distal protection
devices is not recommendeddevices is not recommended
IIa
IIa
IIa
III
B
A
B
C
ESC STEMI GUIDELINES 2012ESC STEMI GUIDELINES 2012
2014 ESC/EACTS Guidelines 2014 ESC/EACTS Guidelines
on Myocardial Revascularisationon Myocardial Revascularisation
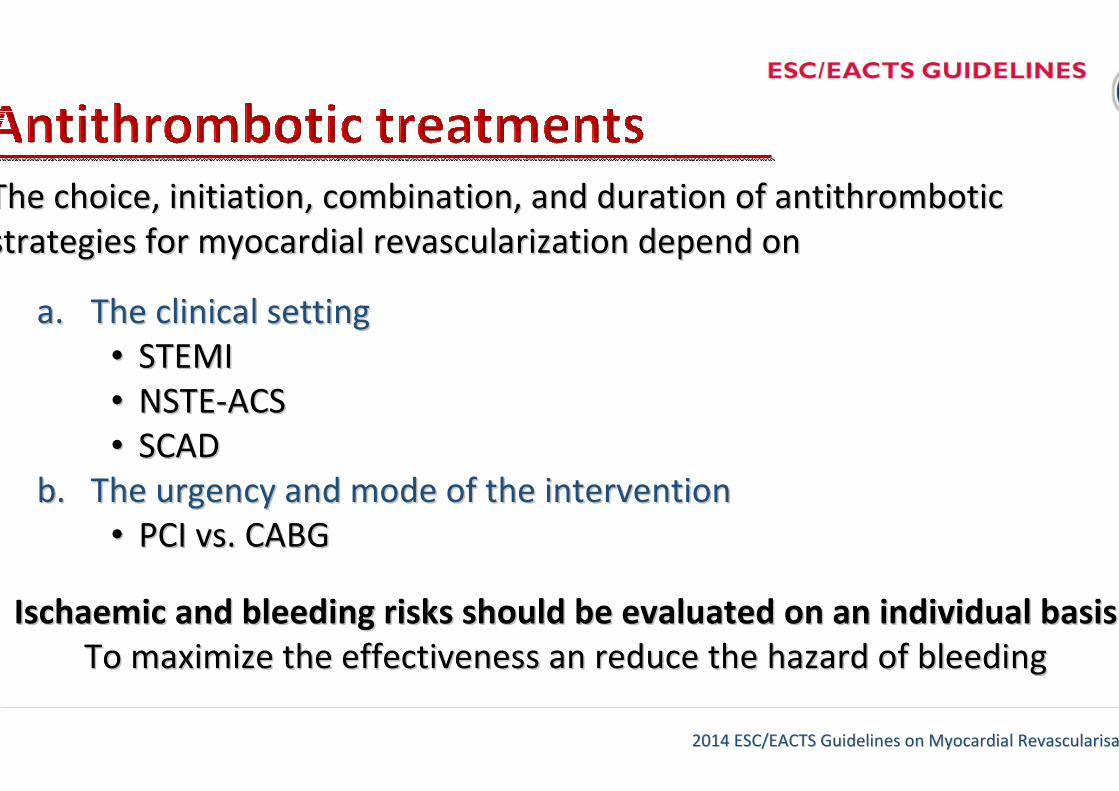
The choice, initiation, combination, and duration of antithromboThe choice, initiation, combination, and duration of antithrombotic tic
strategies for myocardial revascularization depend onstrategies for myocardial revascularization depend on
a.a. The clinical settingThe clinical setting
•• STEMISTEMI
•• NSTENSTE--ACSACS
•• SCADSCAD
b.b. The urgency and mode of the interventionThe urgency and mode of the intervention
•• PCI vs. CABGPCI vs. CABG
Ischaemic and bleeding risks should be evaluated on an individuaIschaemic and bleeding risks should be evaluated on an individual basisl basis
To maximize the effectiveness an reduce the hazard of bleedingTo maximize the effectiveness an reduce the hazard of bleeding
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
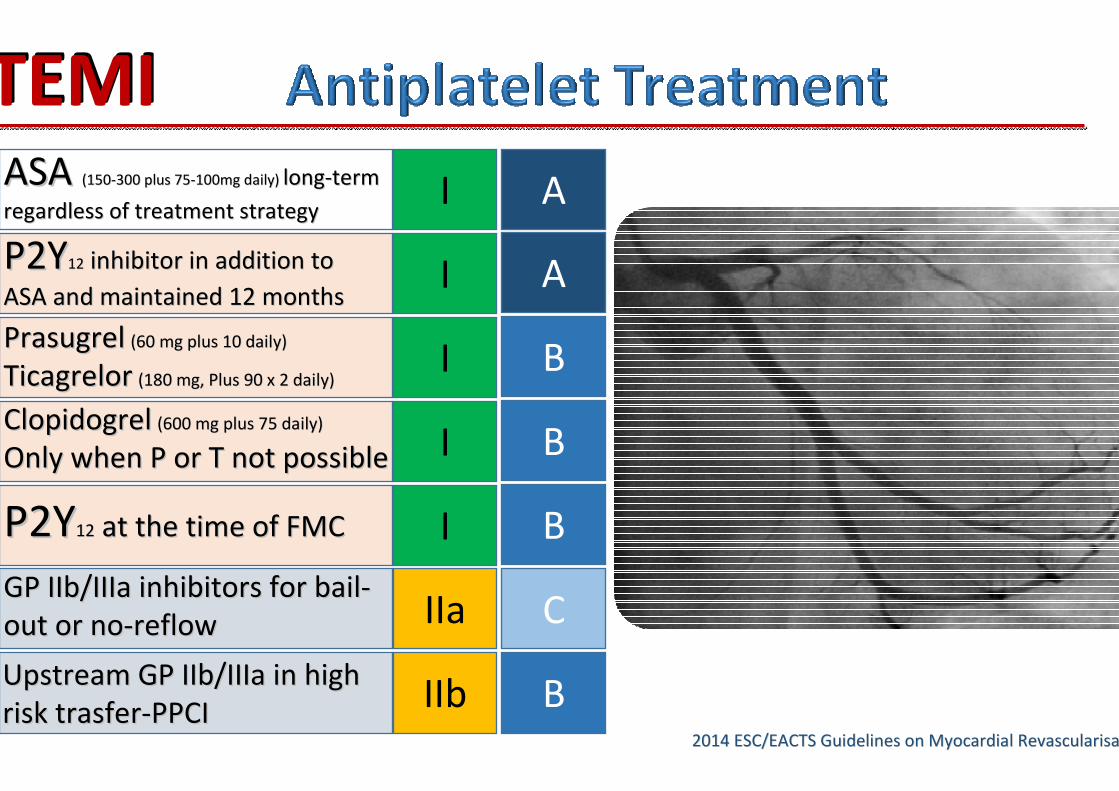
ASA ASA (150(150--300 plus 75300 plus 75--100mg daily) 100mg daily) longlong--term term
regardless of treatment strategyregardless of treatment strategyI A
P2YP2Y1212 inhibitor in addition to inhibitor in addition to
ASA and maintained 12 months ASA and maintained 12 months
PrasugrelPrasugrel (60 mg plus 10 daily)(60 mg plus 10 daily)
TicagrelorTicagrelor (180 mg, Plus 90 x 2 daily) (180 mg, Plus 90 x 2 daily)
I
I
I
A
B
BClopidogrelClopidogrel (600 mg plus 75 daily)(600 mg plus 75 daily)
Only when P or T not possibleOnly when P or T not possible
I BP2YP2Y1212 at the time of FMCat the time of FMC
IIa CGP IIb/IIIa inhibitors for bailGP IIb/IIIa inhibitors for bail--
out or noout or no--reflow reflow
IIb BUpstream GP IIb/IIIa in high Upstream GP IIb/IIIa in high
risk trasferrisk trasfer--PPCIPPCI
STEMISTEMI
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
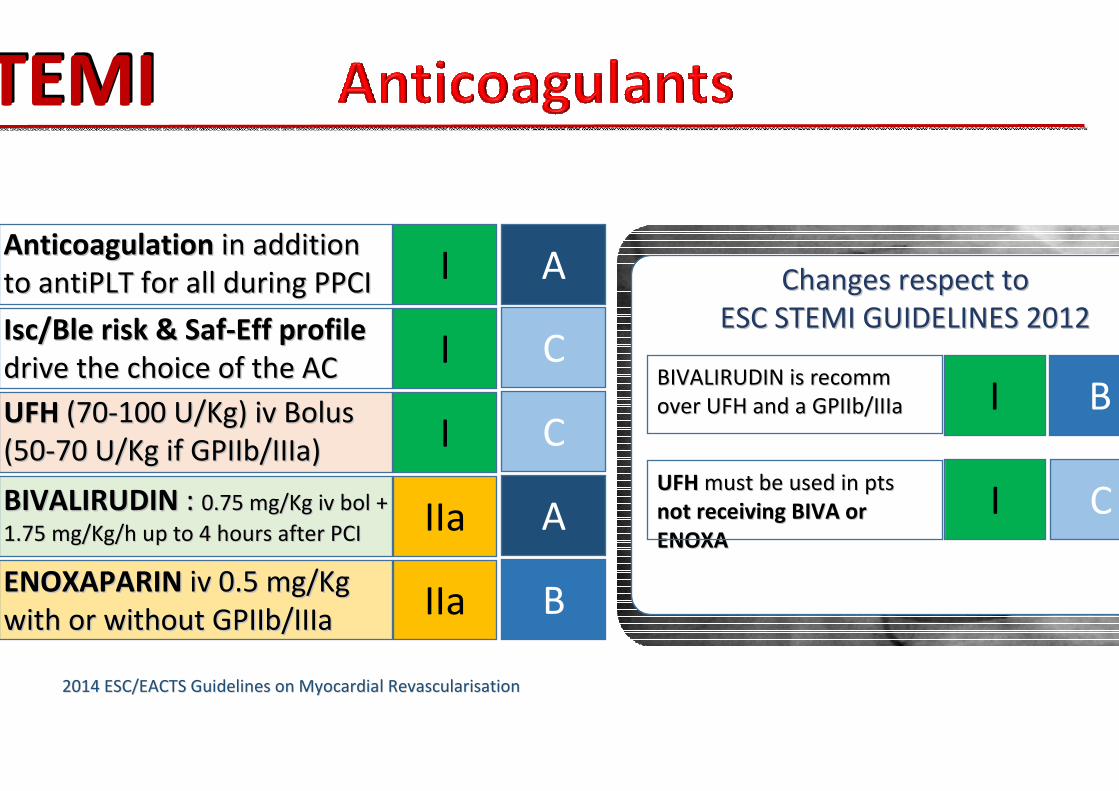
AnticoagulationAnticoagulation in addition in addition
to antiPLT for all during PPCI to antiPLT for all during PPCI I A
Isc/Ble risk & SafIsc/Ble risk & Saf--Eff profile Eff profile
drive the choice of the AC drive the choice of the AC I C
UFHUFH (70(70--100 U/Kg) iv Bolus100 U/Kg) iv Bolus
(50(50--70 U/Kg if GPIIb/IIIa)70 U/Kg if GPIIb/IIIa) I C
IIa ABIVALIRUDINBIVALIRUDIN : : 0.75 mg/Kg iv bol + 0.75 mg/Kg iv bol +
1.75 mg/Kg/h up to 4 hours after PCI1.75 mg/Kg/h up to 4 hours after PCI
IIa BENOXAPARINENOXAPARIN iv 0.5 mg/Kg iv 0.5 mg/Kg
with or without GPIIb/IIIawith or without GPIIb/IIIa
Changes respect toChanges respect to
ESC STEMI GUIDELINES 2012ESC STEMI GUIDELINES 2012
BIVALIRUDIN is recomm BIVALIRUDIN is recomm
over UFH and a GPIIb/IIIaover UFH and a GPIIb/IIIa I B
UFHUFH must be used in pts must be used in pts
not receiving BIVA or not receiving BIVA or
ENOXAENOXA
I C
STEMISTEMI
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
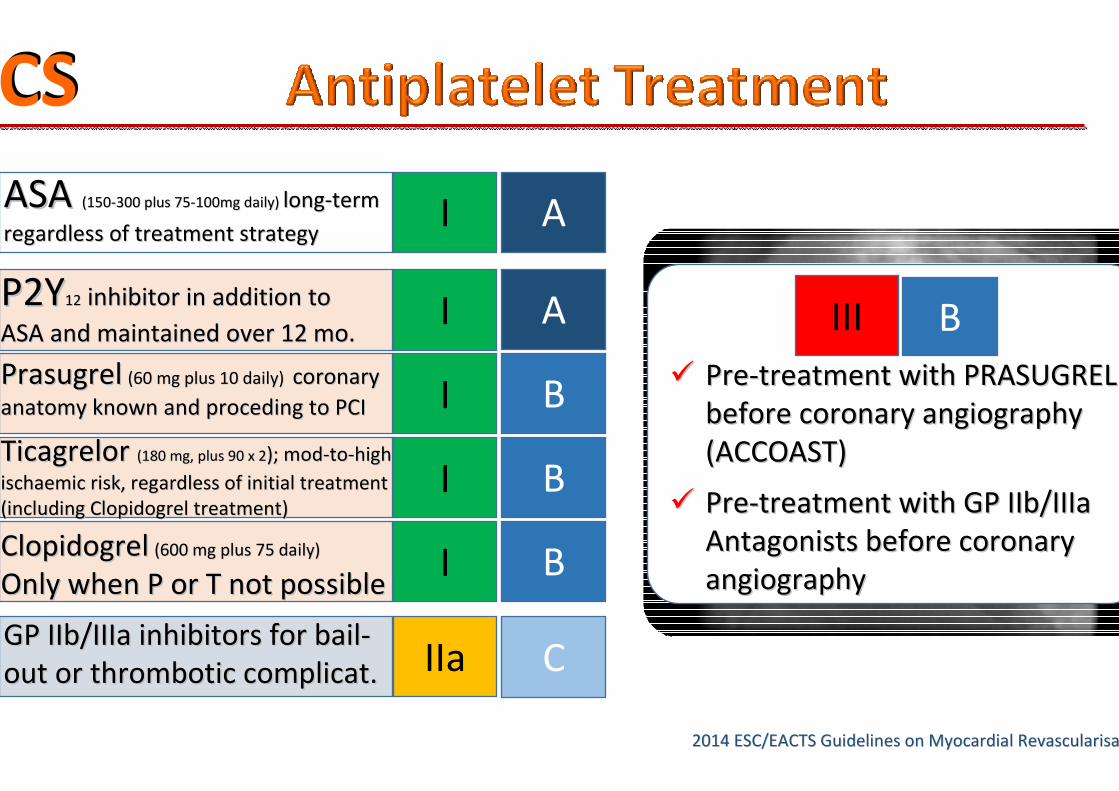
ASA ASA (150(150--300 plus 75300 plus 75--100mg daily) 100mg daily) longlong--term term
regardless of treatment strategyregardless of treatment strategyI A
P2YP2Y1212 inhibitor in addition to inhibitor in addition to
ASA and maintained over 12 mo.ASA and maintained over 12 mo.
PrasugrelPrasugrel (60 mg plus 10 daily) (60 mg plus 10 daily) coronary coronary
anatomy known and proceding to PCIanatomy known and proceding to PCI
I
I
I
A
B
B
ClopidogrelClopidogrel (600 mg plus 75 daily)(600 mg plus 75 daily)
Only when P or T not possibleOnly when P or T not possibleI B
Ticagrelor Ticagrelor (180 mg, plus 90 x 2(180 mg, plus 90 x 2); mod); mod--toto--high high
ischaemic risk, regardless of initial treatment ischaemic risk, regardless of initial treatment
(including Clopidogrel treatment)(including Clopidogrel treatment)
IIa CGP IIb/IIIa inhibitors for bailGP IIb/IIIa inhibitors for bail--
out or thrombotic complicat. out or thrombotic complicat.
ACSACS
III B
�� PrePre--treatment with PRASUGREL treatment with PRASUGREL
before coronary angiography before coronary angiography
(ACCOAST)(ACCOAST)
�� PrePre--treatment with GP IIb/IIIa treatment with GP IIb/IIIa
Antagonists before coronary Antagonists before coronary
angiographyangiography
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
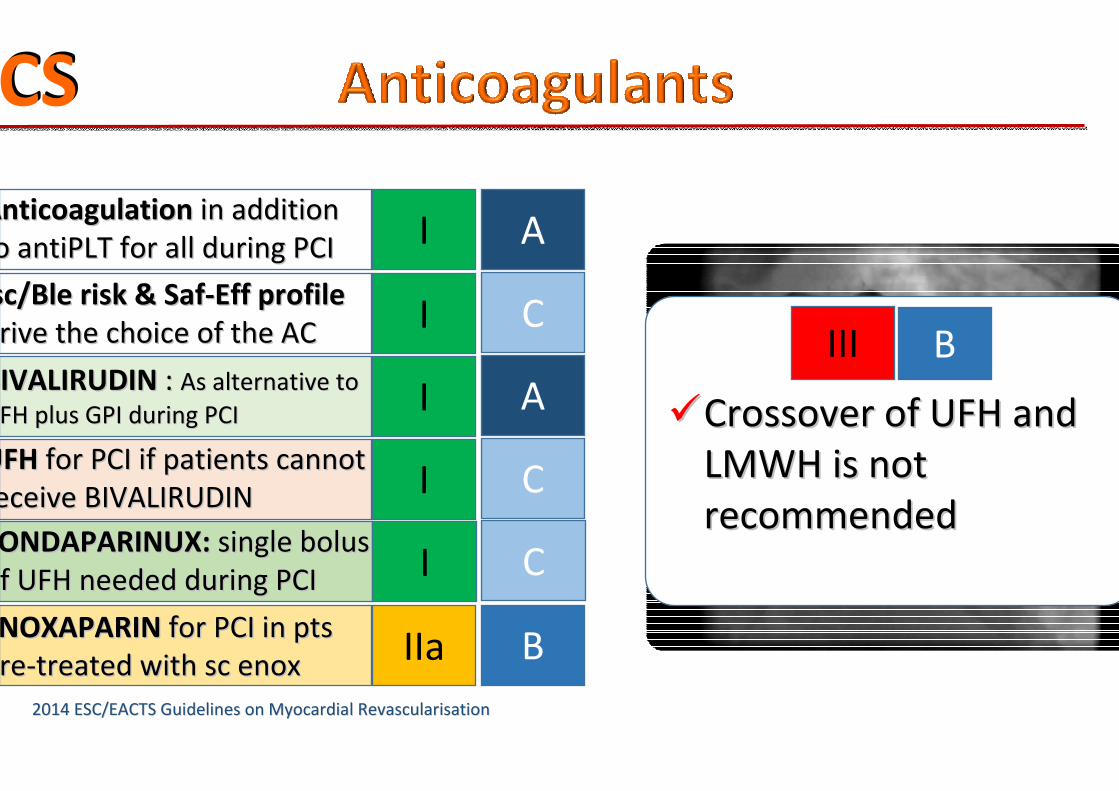
AnticoagulationAnticoagulation in addition in addition
to antiPLT for all during PCI to antiPLT for all during PCI I A
Isc/Ble risk & SafIsc/Ble risk & Saf--Eff profile Eff profile
drive the choice of the AC drive the choice of the AC I C
UFHUFH for PCI if patients cannot for PCI if patients cannot
receive BIVALIRUDINreceive BIVALIRUDIN I C
I ABIVALIRUDINBIVALIRUDIN : : As alternative to As alternative to
UFH plus GPI during PCIUFH plus GPI during PCI
IIa BENOXAPARINENOXAPARIN for PCI in pts for PCI in pts
prepre--treated with sc enoxtreated with sc enox
ACSACS
FONDAPARINUX: FONDAPARINUX: single bolus single bolus
of UFH needed during PCIof UFH needed during PCI I C
III B
��Crossover of UFH and Crossover of UFH and
LMWH is not LMWH is not
recommendedrecommended
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
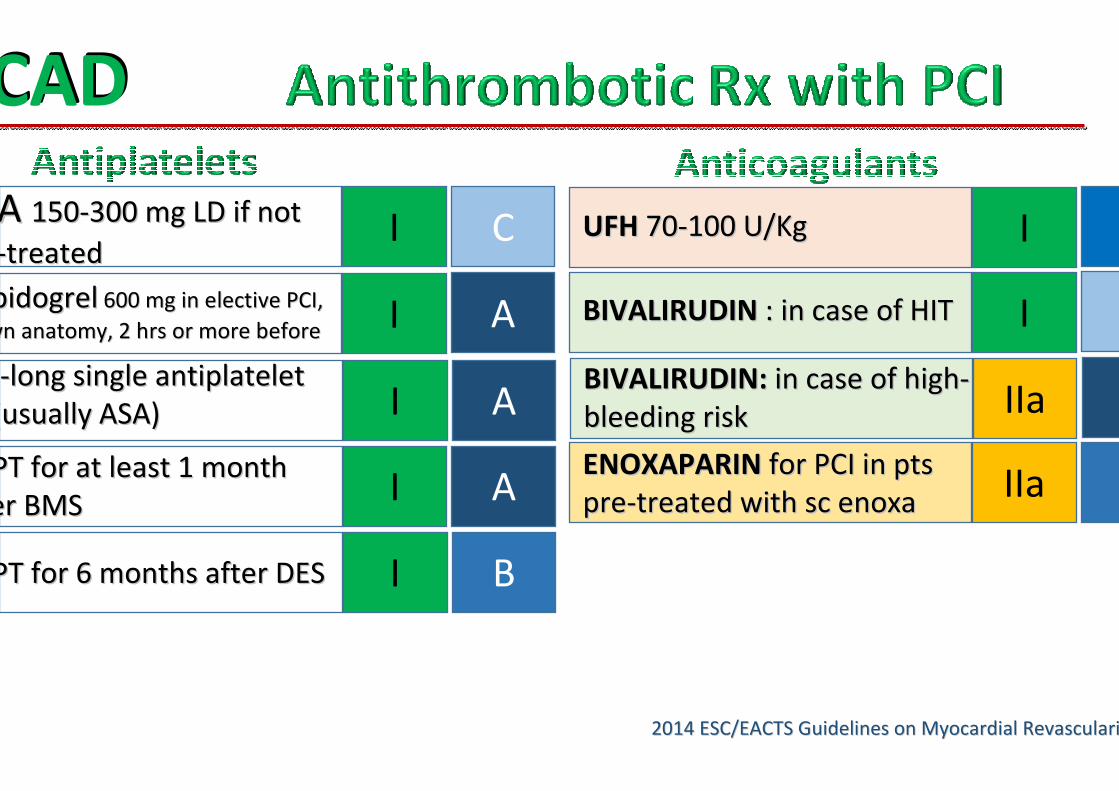
ASA ASA 150150--300 mg LD if not 300 mg LD if not
--treatedtreatedI C
ClopidogrelClopidogrel 600 mg in elective PCI, 600 mg in elective PCI,
known anatomy, 2 hrs or more beforeknown anatomy, 2 hrs or more before I A
SCADSCAD
Life--long single antiplatelet long single antiplatelet
Rx (usually ASA)Rx (usually ASA) I A
DAPT for at least 1 month DAPT for at least 1 month
after BMSafter BMSI A
DAPT for 6 months after DESDAPT for 6 months after DES I B
UFHUFH 7070--100 U/Kg100 U/Kg I
IBIVALIRUDINBIVALIRUDIN : in case of HIT: in case of HIT
IIaENOXAPARINENOXAPARIN for PCI in pts for PCI in pts
prepre--treated with sc enoxatreated with sc enoxa
BIVALIRUDIN: BIVALIRUDIN: in case of highin case of high--
bleeding riskbleeding risk IIa
EXCELLENTEXCELLENTIt is recommended that DAPT be administered
��SCADSCAD� for at least 1 month after BMS
� for 6 months after new-generation DES
��ACSACS� up to 1 year irrespective of
revascularization strategy (CURE; TRITON; PLATO)
2014 ESC/EACTS2014 ESC/EACTS
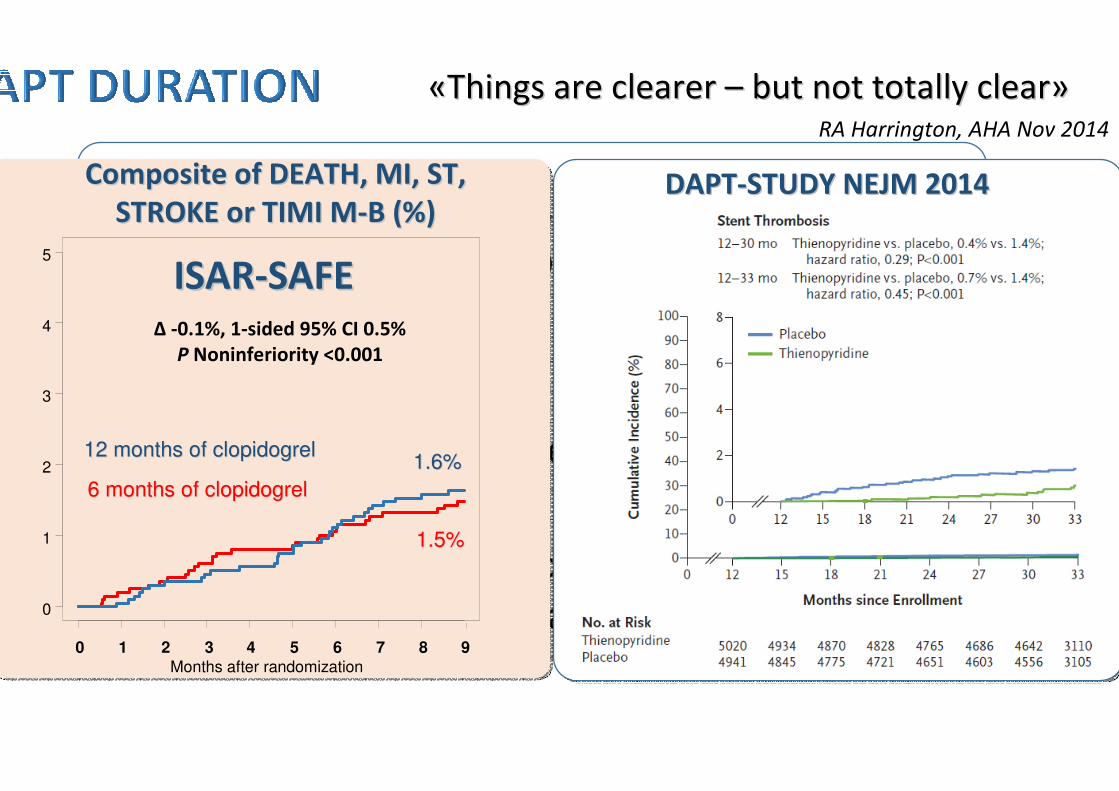
Guidelines on Myocardial RevascularisationGuidelines on Myocardial RevascularisationDAPTDAPT--STUDY NEJM 2014STUDY NEJM 2014
0
1
2
3
4
5
0 1 2 3 4 5 6 7 8 9
12 months of clopidogrel12 months of clopidogrel
6 months of clopidogrel6 months of clopidogrel
Months after randomization
Composite of DEATH, MI, ST,Composite of DEATH, MI, ST,
STROKE or TIMI MSTROKE or TIMI M--B (%)B (%)
1.6%1.6%
1.5%1.5%
Δ -0.1%, 1-sided 95% CI 0.5%
P Noninferiority <0.001
ISARISAR--SAFESAFE
RA Harrington, AHA Nov 2014
««Things are clearer Things are clearer –– but not totally clearbut not totally clear»»
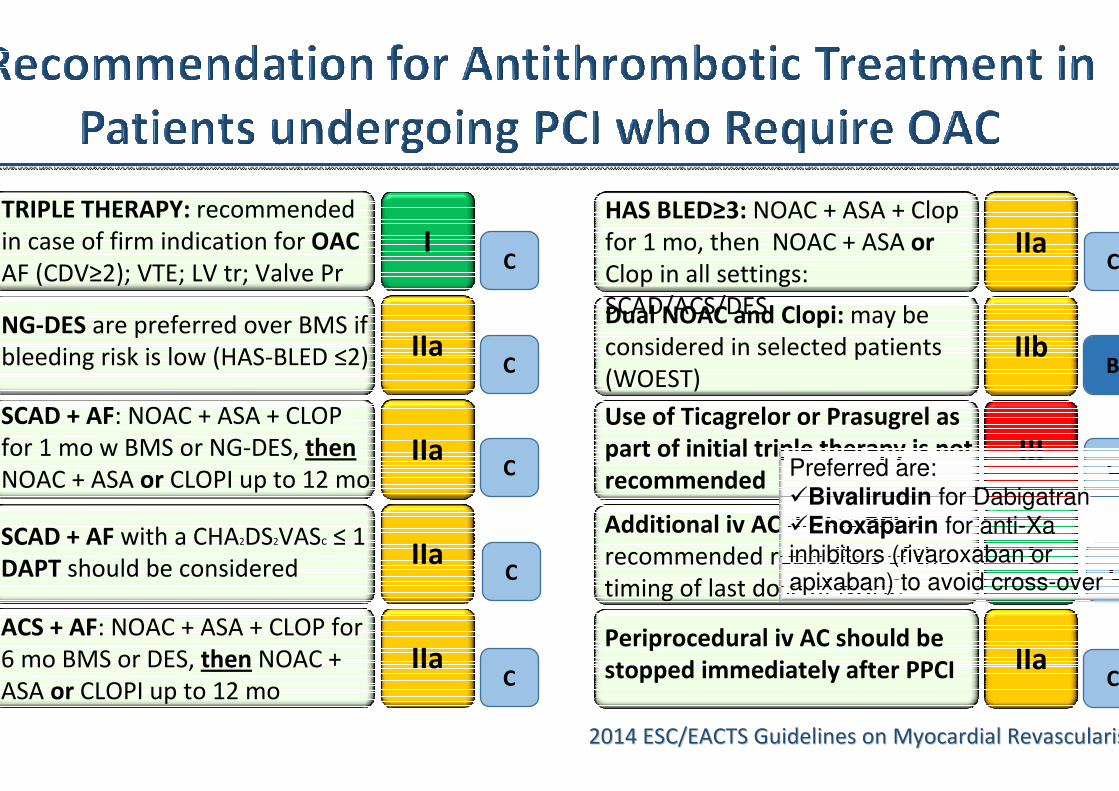
Dual NOAC and Clopi: may be
considered in selected patients
(WOEST)
Use of Ticagrelor or Prasugrel as
part of initial triple therapy is not
recommended
Additional iv AC during PCI is
recommended regardless of the
timing of last dose of NOAC
IIb
III
I
IIaPeriprocedural iv AC should be
stopped immediately after PPCI
HAS BLED≥3: NOAC + ASA + Clop
for 1 mo, then NOAC + ASA or
Clop in all settings:
SCAD/ACS/DES
IIaC
C
C
C
B
TRIPLE THERAPY: recommended
in case of firm indication for OAC
AF (CDV≥2); VTE; LV tr; Valve Pr I
C
SCAD + AF: NOAC + ASA + CLOP
for 1 mo w BMS or NG-DES, then
NOAC + ASA or CLOPI up to 12 mo IIa
C
IIaACS + AF: NOAC + ASA + CLOP for
6 mo BMS or DES, then NOAC +
ASA or CLOPI up to 12 mo C
SCAD + AF with a CHA2DS2VASc ≤ 1
DAPT should be consideredIIa
C
NG-DES are preferred over BMS if
bleeding risk is low (HAS-BLED ≤2) IIaC
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
Preferred are:
�Bivalirudin for Dabigatran
�Enoxaparin for anti-Xa
inhibitors (rivaroxaban or apixaban) to avoid cross-over
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
PCI or CABG, may be indicated to reduce myocardial ischaemia andPCI or CABG, may be indicated to reduce myocardial ischaemia and its its
adverse clinical adverse clinical manifestationsmanifestations
AnginaAngina: : associated with associated with impaired quality of life, reduced physical endurance, mental impaired quality of life, reduced physical endurance, mental
depression, and recurrent hospitalizations and outpatient visitsdepression, and recurrent hospitalizations and outpatient visits
�� Revascularization by PCI or CABG more effectively relieves anginRevascularization by PCI or CABG more effectively relieves angina, reduces the use a, reduces the use
of antiof anti--angina drugs, and improves exercise capacity and quality of lifeangina drugs, and improves exercise capacity and quality of life, compared , compared
with a strategy of OMT alonewith a strategy of OMT alone
IschaemiaIschaemia is of prognostic importance in patients with SCAD, particularly is of prognostic importance in patients with SCAD, particularly when when
occurring at low work loadoccurring at low work load
�� Revascularization relieves myocardial ischaemia more effectivelyRevascularization relieves myocardial ischaemia more effectively than OMT alonethan OMT alone
The extent, location, and severity of CAD are important prognostThe extent, location, and severity of CAD are important prognostic factors in addition to ic factors in addition to
ischaemia and left ventricular functionischaemia and left ventricular function
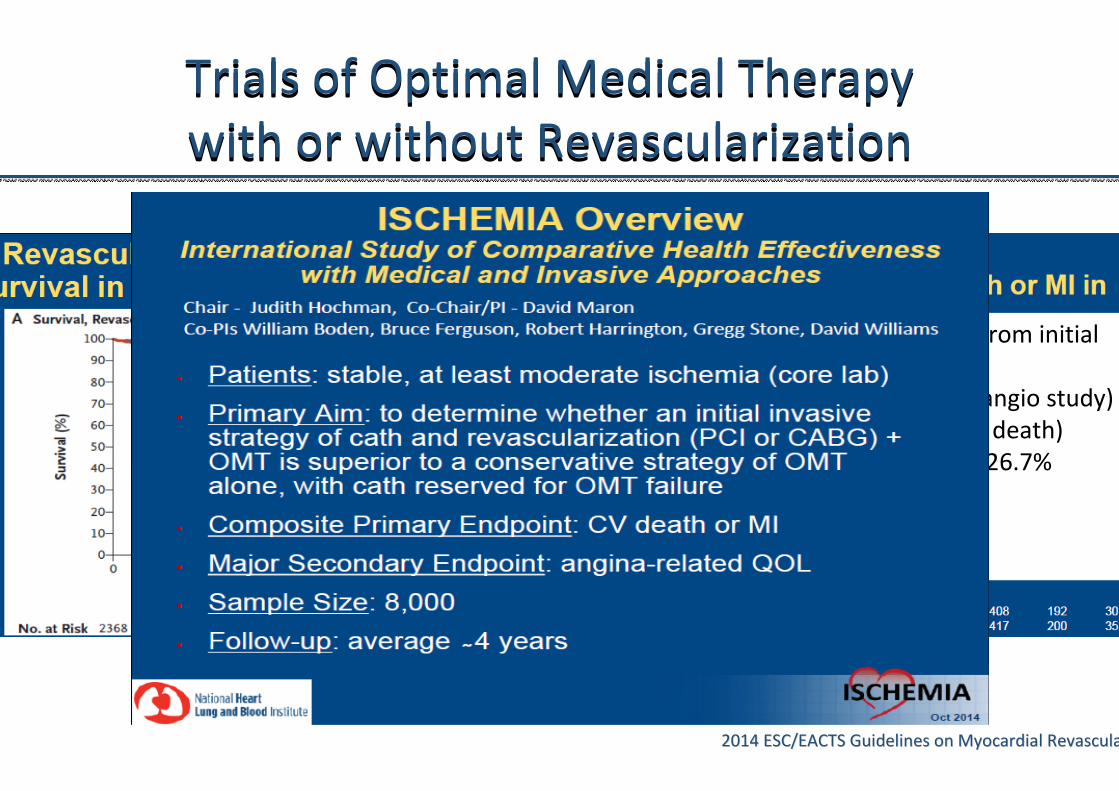
Trials of Optimal Medical Therapy
with or without Revascularization
Trials of Optimal Medical Therapy
with or without Revascularization
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
• Underpowered (many exclusion from initial
cohort)
• Investigator selection Bias (post-angio study)
• Low risk pts (0.4% annual cardiac death)
• End Point : all cause death - only 26.7%
confirmed Cardiac Death
• ITT … but huge cross-over
• …..etc…
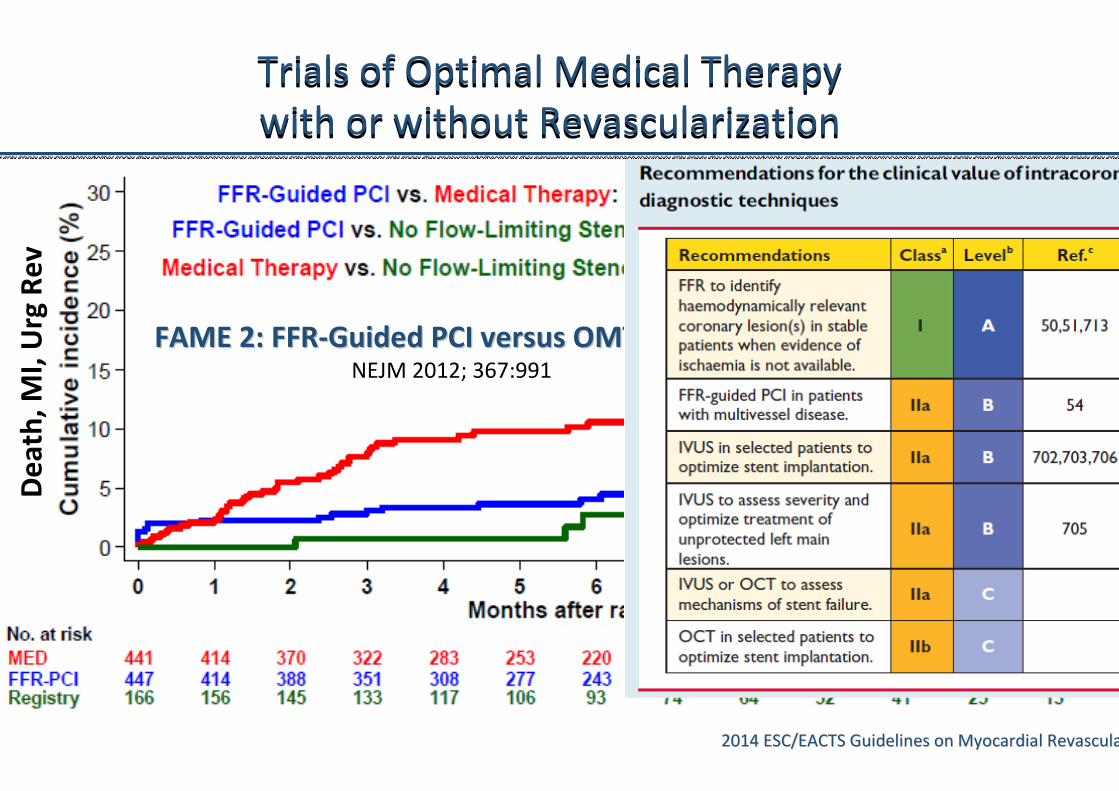
Trials of Optimal Medical Therapy
with or without Revascularization
Trials of Optimal Medical Therapy
with or without Revascularization
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
FAME 2: FFRFAME 2: FFR--Guided PCI versus OMT in SCADGuided PCI versus OMT in SCADNEJM 2012; 367:991
De
ath
, M
I, U
rg R
ev
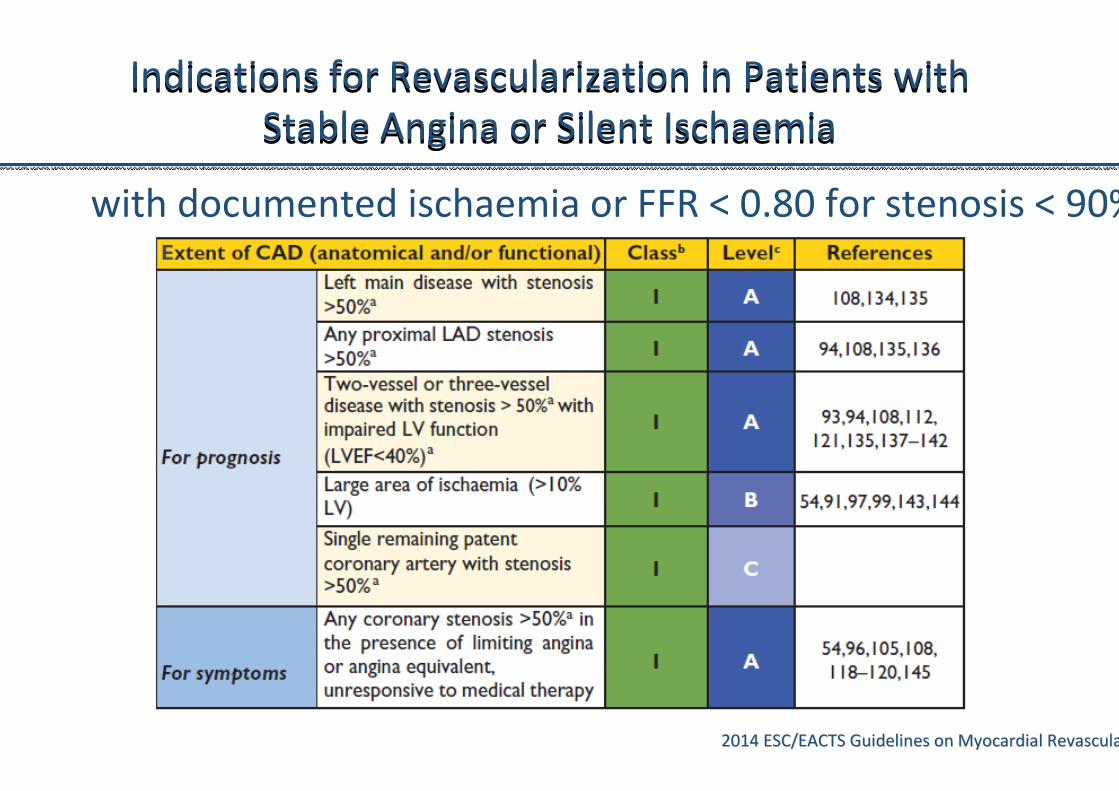
with documented ischaemia or FFR < 0.80 for stenosis < 90%
Indications for Revascularization in Patients with
Stable Angina or Silent Ischaemia
Indications for Revascularization in Patients with
Stable Angina or Silent Ischaemia
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
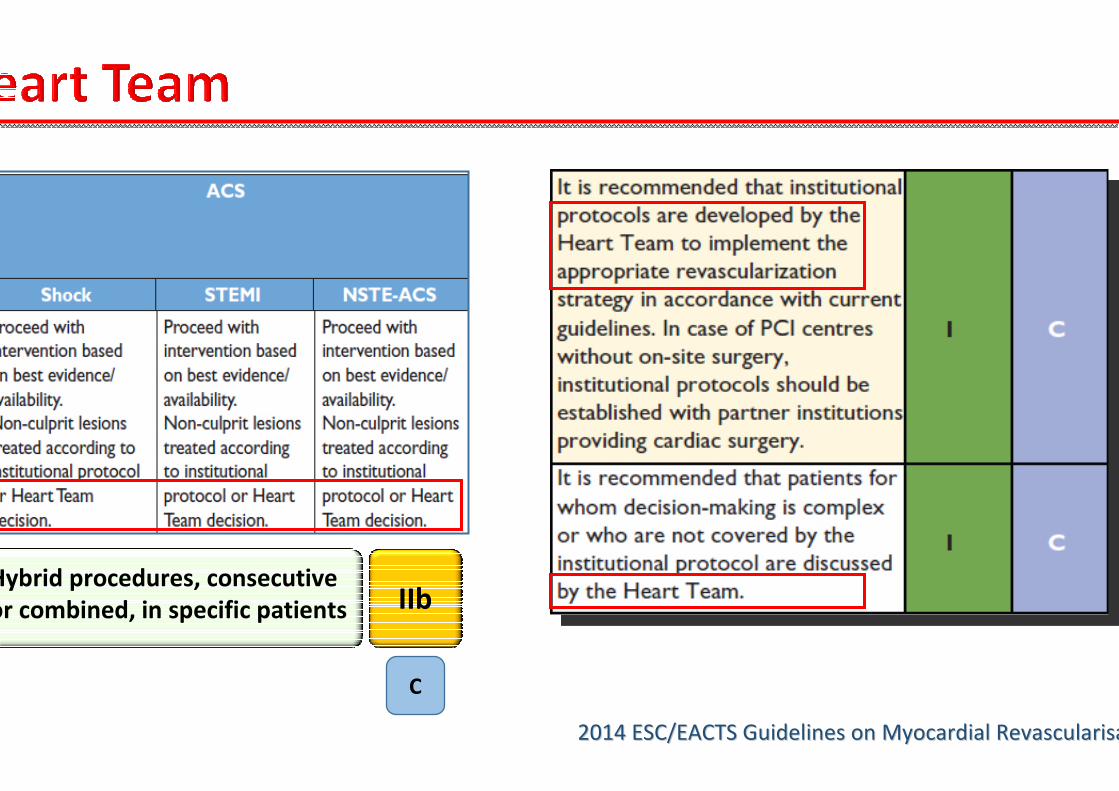
Hybrid procedures, consecutive
or combined, in specific patients IIb
C
2014 ESC/EACTS Guidelines on Myocardial Revascularisation2014 ESC/EACTS Guidelines on Myocardial Revascularisation
Heart team

Male, 55 yrsMale, 55 yrs
HPTN, DIABETESHPTN, DIABETES
ACS: ACS: TnI 1,5 ng/mlTnI 1,5 ng/ml
Cr 1.32 mg/dlCr 1.32 mg/dl
HbA1cHbA1c 7.10 %7.10 %
3V DIFFUSE DISEASE3V DIFFUSE DISEASE
SYNTAX SCORE: 30SYNTAX SCORE: 30
STS : STS : 0.632% mortality0.632% mortality
11.46% morb. mort.11.46% morb. mort.
0.93% perm. stroke0.93% perm. stroke