Convegno regionale AES 2015 Alghero 22 maggio - Pangea Etica · Convegno regionale AES 2015 Alghero...
44
Alfredo Marzano Gastroepatologia Ospedale San Giovanni Battista Università di Torino Convegno regionale AES 2015 Alghero 22 maggio Epatite B Gestione della cirrosi scompensata
Transcript of Convegno regionale AES 2015 Alghero 22 maggio - Pangea Etica · Convegno regionale AES 2015 Alghero...

Alfredo Marzano
Gastroepatologia
Ospedale San Giovanni Battista
Università di Torino
Convegno regionale AES 2015
Alghero 22 maggio
Epatite B
Gestione della cirrosi scompensata

Caso clinicoPresentazione
• Ricovero reparto ottobre 2014• C.A., uomo, 63 anni, Domodossola, guardia giurata;• Potus (1L/die); fumo (20/die)• ECA HBV nota dal 1981. Mai trattato• 2004 ECT (non lesioni focali, IP ND); EGDS: no varici;• 2004-5-6 exeresi polipi colon; dolicocolon;• 2014: diagnosi cirrosi compensatano terapia
• Ricovero 17/10/2014 altro Osp. per febbricola, ascite, ittero(wbc 4600, hb 12.1, mcv 98, plts 64000, INR 2.69, ast 768, alt589, ggt 196, BT 13.34, BD 10.36), alb 2.7, HBsAg+ 0.49 UI ,antiHBs 7.5 UI, IgM HBc pos, antiHBe+, HCV-, HIV -;
• TC : ascite in cirrosi, VP pervia. No terapia antivirale.
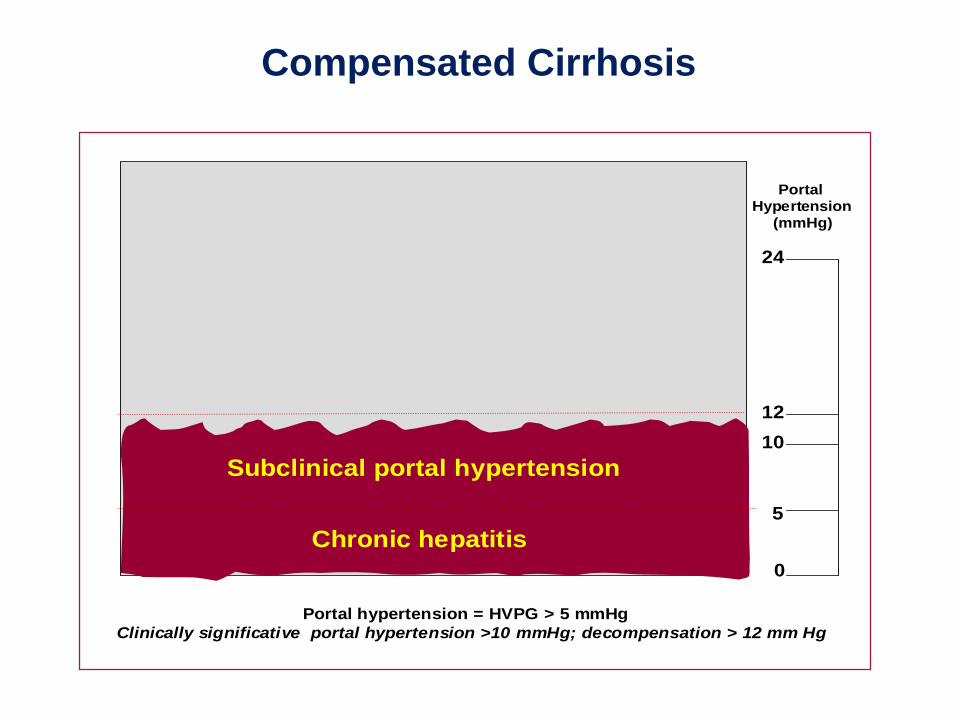
Subclinical portal hypertension
0
12
10
5
24
PortalHypertension
(mmHg)
Portal hypertension = HVPG > 5 mmHg
Clinically significative portal hypertension >10 mmHg; decompensation > 12 mm Hg
Chronic hepatitis
Compensated Cirrhosis
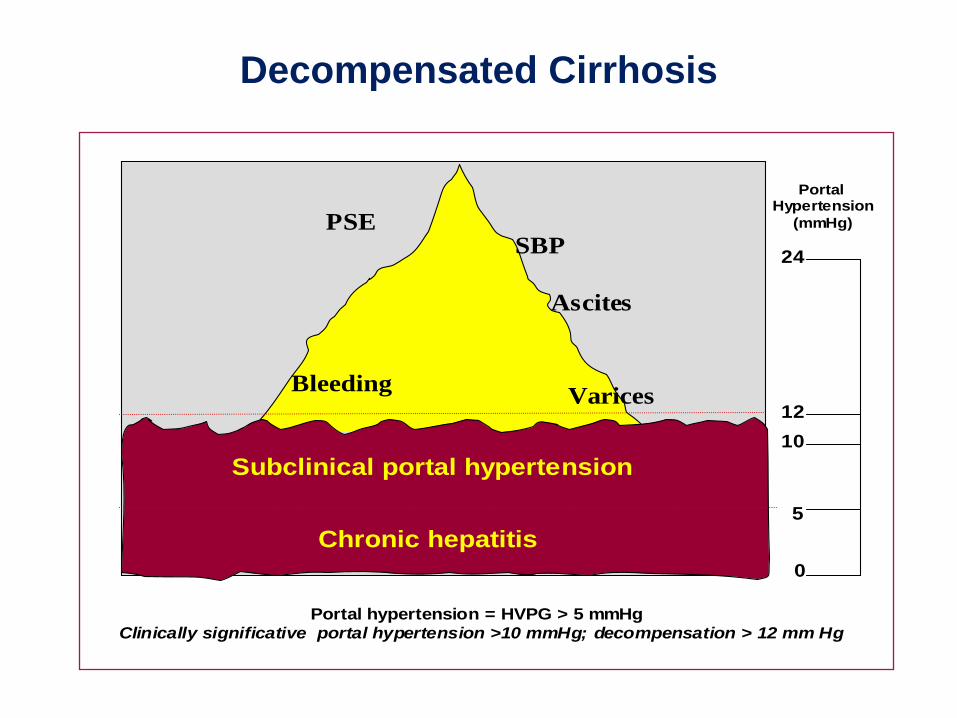
Subclinical portal hypertension
VaricesBleeding
PSE
Ascites
SBP
0
12
10
5
24
PortalHypertension
(mmHg)
Portal hypertension = HVPG > 5 mmHg
Clinically significative portal hypertension >10 mmHg; decompensation > 12 mm Hg
Chronic hepatitis
Decompensated Cirrhosis
Varices Bleeding
PSE
Ascites
SBP
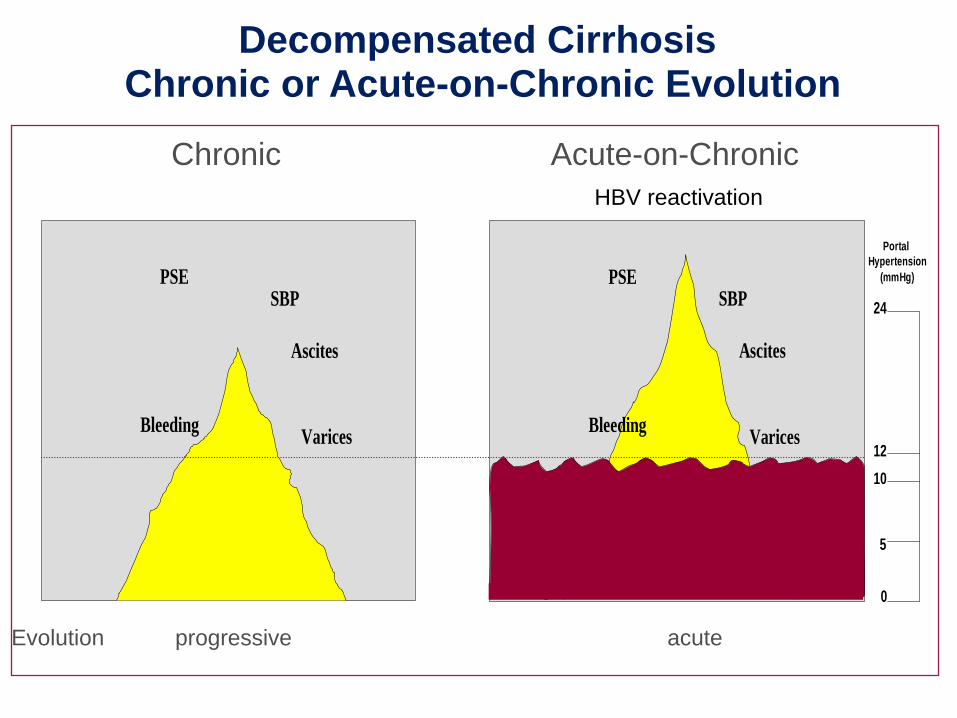
Decompensated CirrhosisChronic or Acute-on-Chronic Evolution
VaricesBleeding
PSE
Ascites
SBP
0
12
10
5
24
Portal
Hypertension
(mmHg)
Chronic Acute-on-Chronic
HBV reactivation
Evolution progressive acute
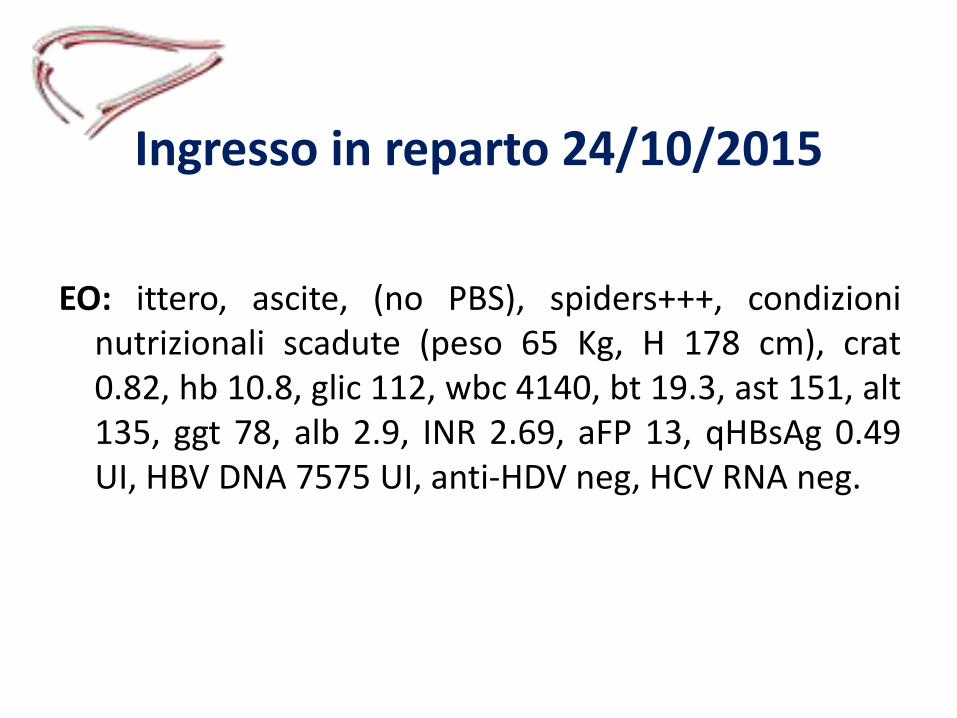
Ingresso in reparto 24/10/2015
EO: ittero, ascite, (no PBS), spiders+++, condizioninutrizionali scadute (peso 65 Kg, H 178 cm), crat0.82, hb 10.8, glic 112, wbc 4140, bt 19.3, ast 151, alt135, ggt 78, alb 2.9, INR 2.69, aFP 13, qHBsAg 0.49UI, HBV DNA 7575 UI, anti-HDV neg, HCV RNA neg.

Decorso
MELD 28
• Valutazione preliminare chirurgo OLT;• Gruppo A-• TC con ricostruzione vascolare (non trombosi portale, non
lesioni focali)• EGDS: GC severa• Entecavir 0.5 mg 1 co/die (24/10)• Bilancio OLT• Plasma, albumina, compenso dell’ascite (- 5 Kg 1/11)
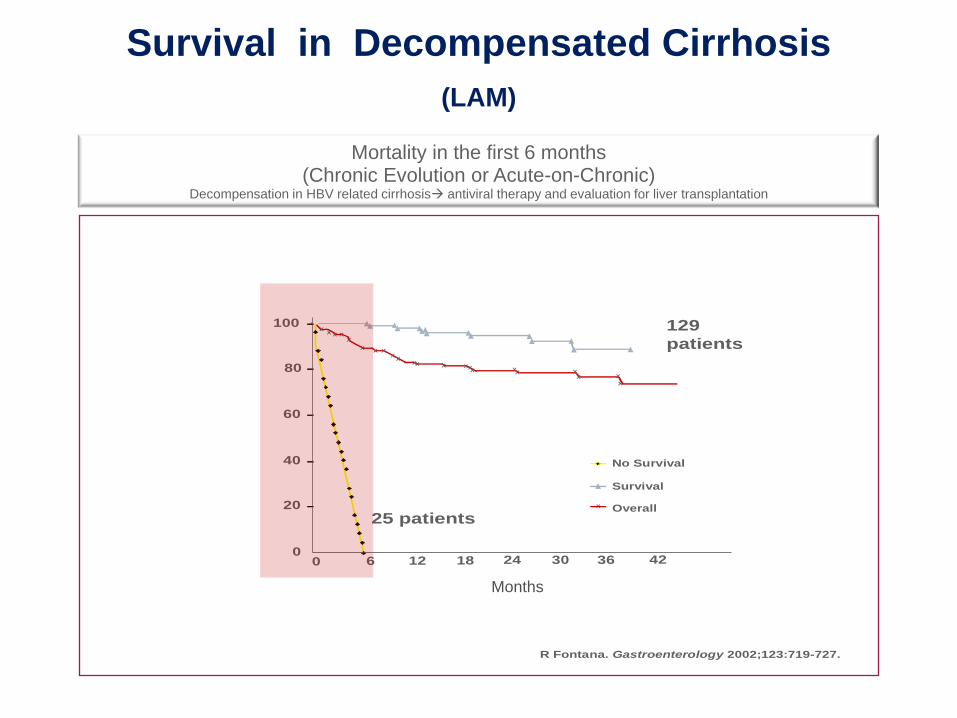
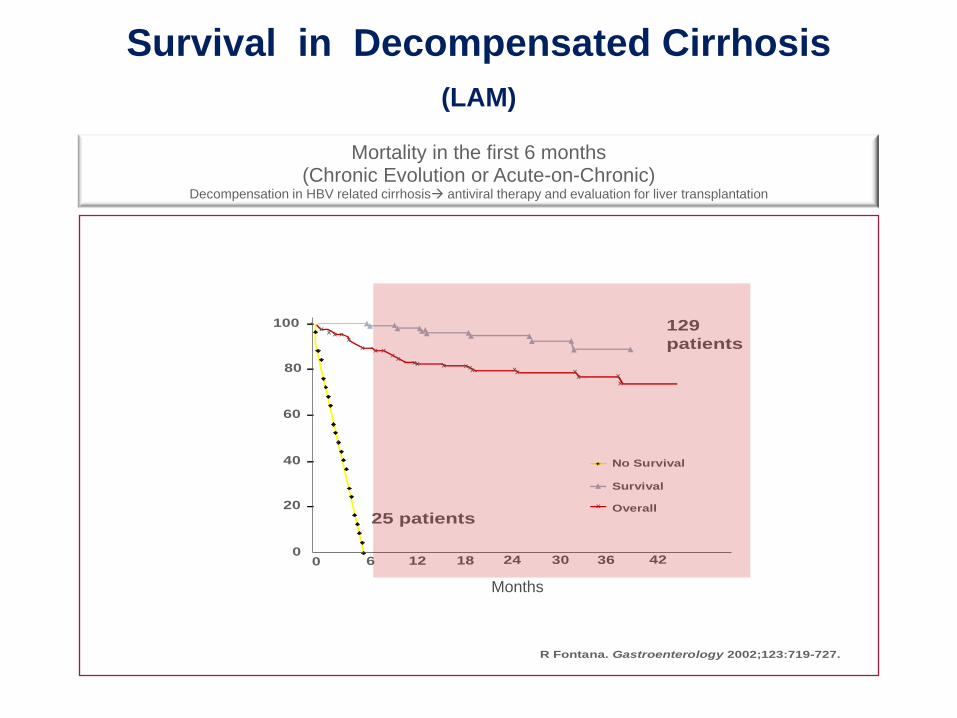
R Fontana. Gastroenterology 2002;123:719-727.
25 patients
129
patients
0
20
40
60
80
100X
X XXX
XX X
XX
XXX
XXX
XXXX X
X
X
0 6 12 18 24 30 36 42
No Survival
Survival
Overall
Survival in Decompensated Cirrhosis
(LAM)
Mortality in the first 6 months(Chronic Evolution or Acute-on-Chronic)
Decompensation in HBV related cirrhosis antiviral therapy and evaluation for liver transplantation
Months
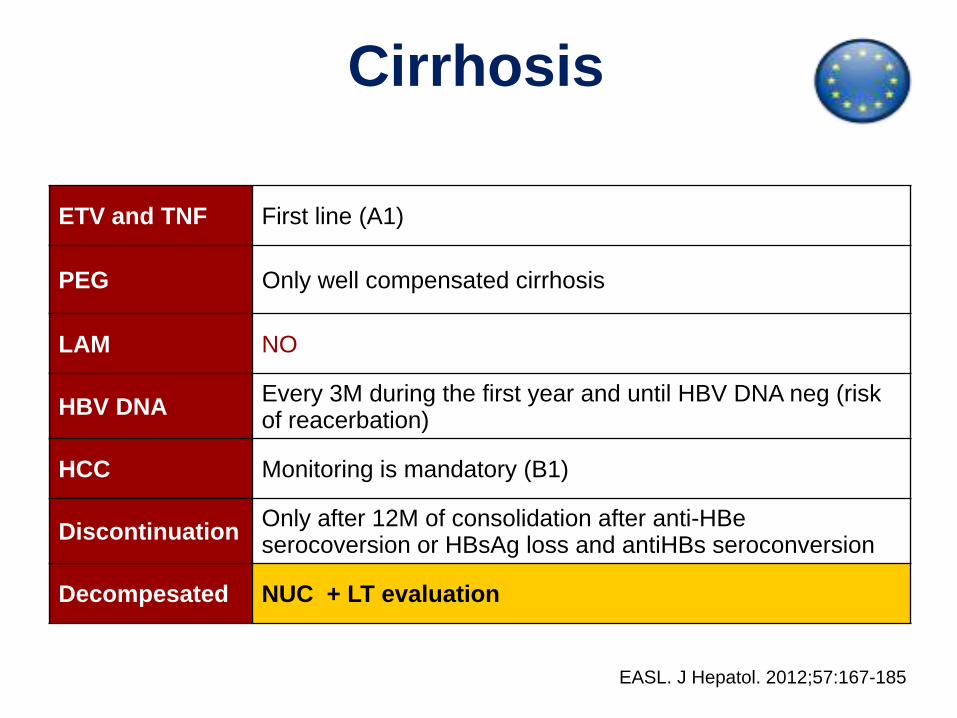
Cirrhosis
ETV and TNF First line (A1)
PEG Only well compensated cirrhosis
LAM NO
HBV DNAEvery 3M during the first year and until HBV DNA neg (risk of reacerbation)
HCC Monitoring is mandatory (B1)
DiscontinuationOnly after 12M of consolidation after anti-HBe serocoversion or HBsAg loss and antiHBs seroconversion
Decompesated NUC + LT evaluation
EASL. J Hepatol. 2012;57:167-185
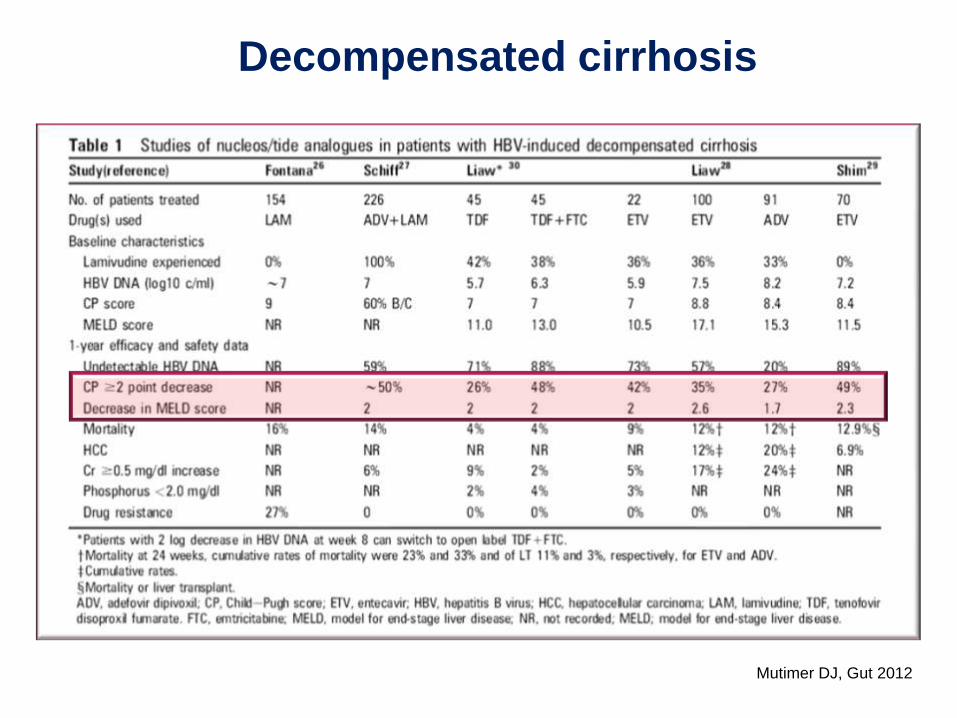
Decompensated cirrhosis
Mutimer DJ, Gut 2012
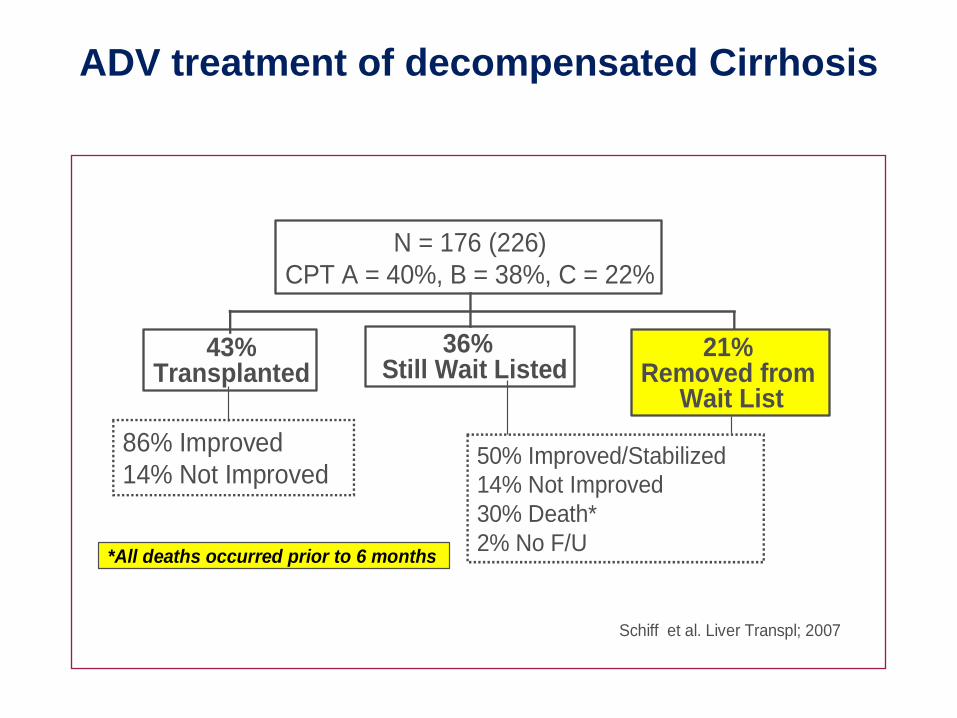
86% Improved
14% Not Improved50% Improved/Stabilized
14% Not Improved
30% Death*
2% No F/U
N = 176 (226)
CPT A = 40%, B = 38%, C = 22%
43%Transplanted
21% Removed from
Wait List
36% Still Wait Listed
*All deaths occurred prior to 6 months
Schiff et al. Liver Transpl; 2007
ADV treatment of decompensated Cirrhosis
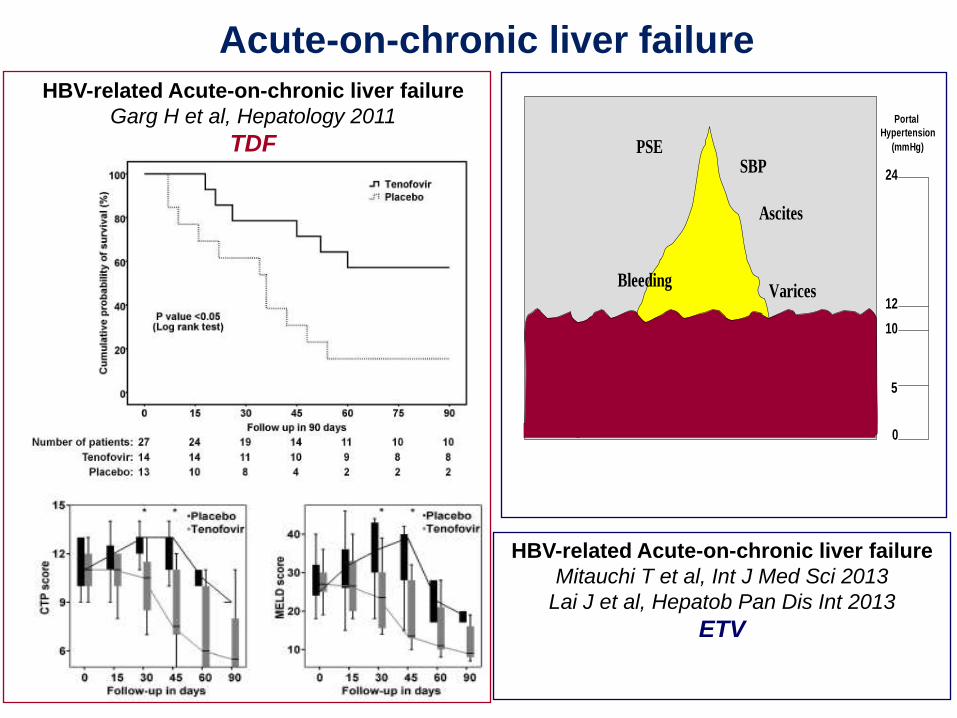
HBV-related Acute-on-chronic liver failure
Garg H et al, Hepatology 2011
TDF
VaricesBleeding
PSE
Ascites
SBP
0
12
10
5
24
Portal
Hypertension
(mmHg)
HBV-related Acute-on-chronic liver failure
Mitauchi T et al, Int J Med Sci 2013
Lai J et al, Hepatob Pan Dis Int 2013
ETV
Acute-on-chronic liver failure
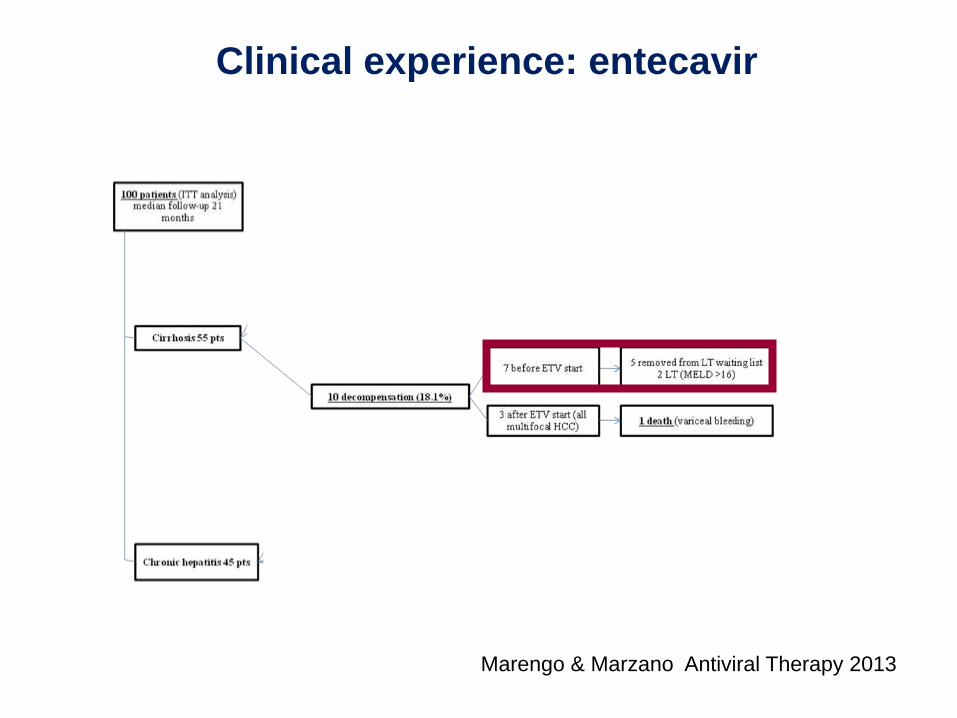
Clinical experience: entecavir
Marengo & Marzano Antiviral Therapy 2013
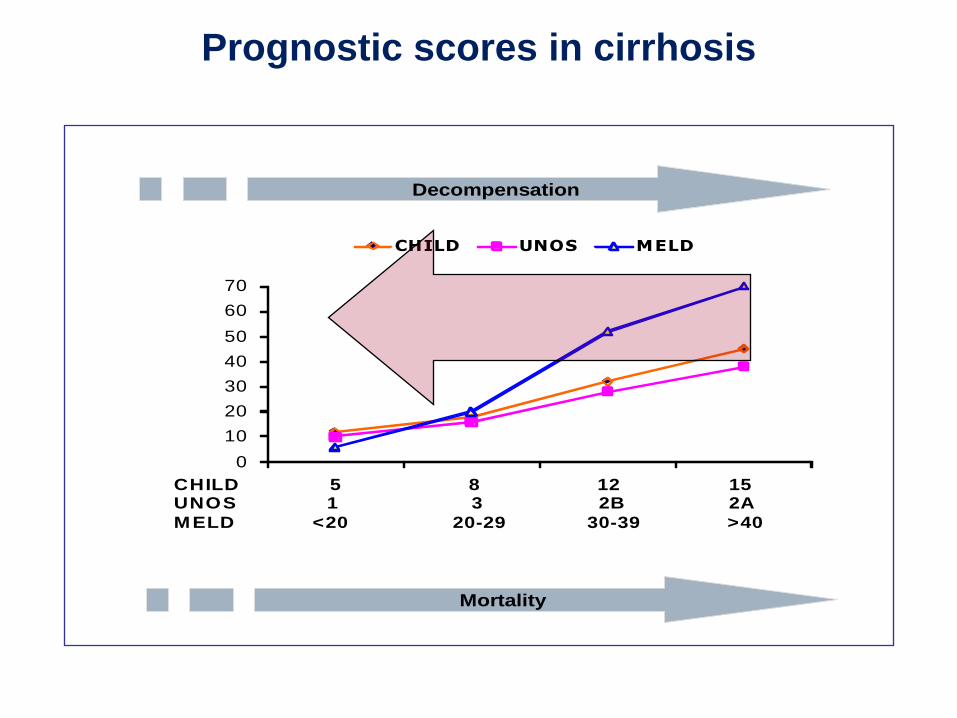
Prognostic scores in cirrhosis
Post-
Liv
er
Tra
nspla
nta
tion
mort
alit
y
*
0
10
20
30
40
50
60
70
CHILD UNOS MELD
CHILD 5 8 12 15UNOS 1 3 2B 2A
MELD <20 20-29 30-39 >40
Decompensation
Mortality
R Fontana. Gastroenterology 2002;123:719-727.
25 patients
129
patients
0
20
40
60
80
100X
X XXX
XX X
XX
XXX
XXX
XXXX X
X
X
0 6 12 18 24 30 36 42
No Survival
Survival
Overall
Survival in Decompensated Cirrhosis
(LAM)
Mortality in the first 6 months(Chronic Evolution or Acute-on-Chronic)
Decompensation in HBV related cirrhosis antiviral therapy and evaluation for liver transplantation
Months
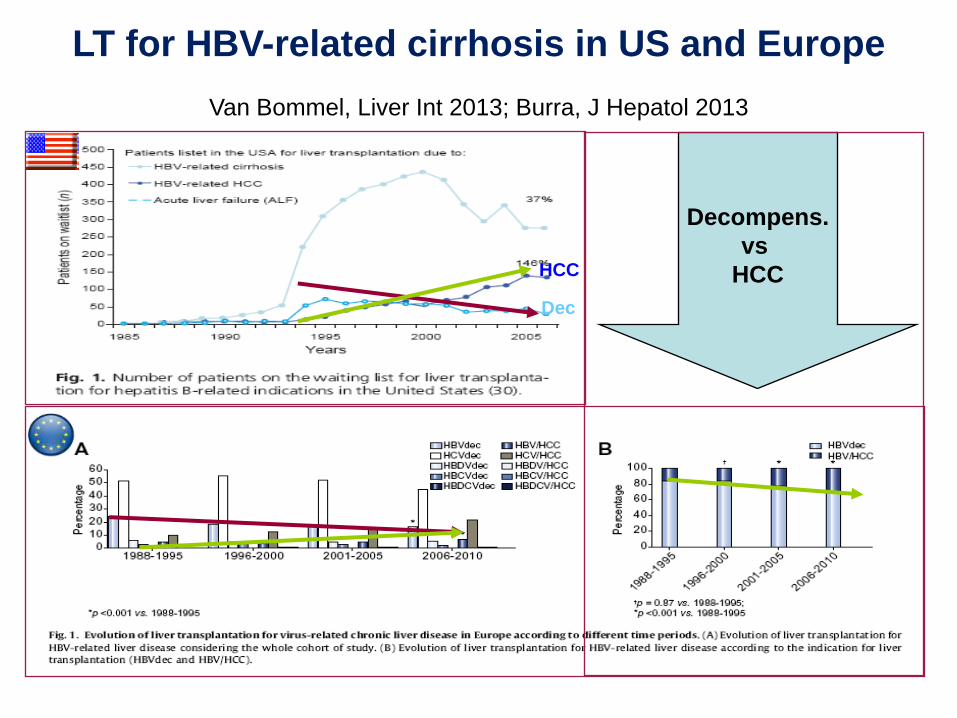
LT for HBV-related cirrhosis in US and Europe
Decompens.
vs
HCC
Van Bommel, Liver Int 2013; Burra, J Hepatol 2013
HCC
Dec
Decorso 1
• Riduzione HBV DNA (1065 UI il 6/11), incrementoBT (21) e INR (3.19); episodio di EPS risolto conriduzione diuretici e idratazione
MELD 31• Dimesso 11/11/2015 con indicazione al
completamento del bilancio in ambulatorio OLT.Inserito in LAT 17/11/2015
MELD 28 BT 5.5, creat 0.94, INR 1.59

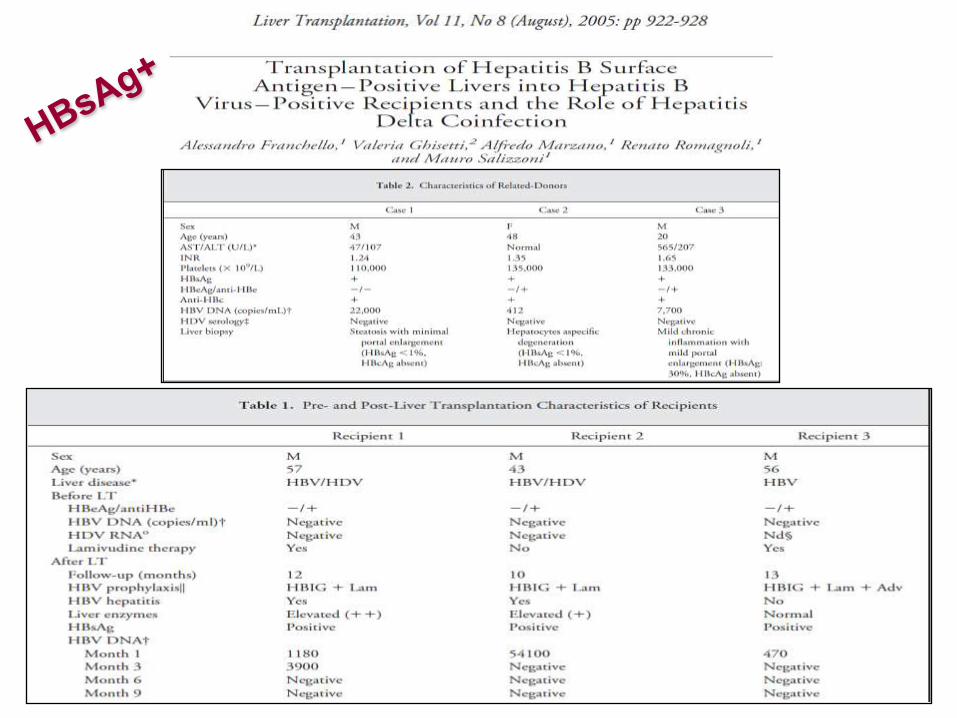
OLT 2666 (!) 16/12/2014
Donatore 0+; HBsAg+
• Estubato G1;
• Rigetto 27/12;
• Anemia da autoanticorpi (siero Antilinfocitario);CMV (terapia), colangite (EC,SH)stop 30/1/2015;
• EBV alto titolo (2.044.600 cp/ml 13/1)TCPTLD(RTX);
• Chiusura Kehr 28/1;
• PPD+piraldina
Profilassi post-OLT
• HBIG 20,000 UIStop G7
• ETV 0.5 mg/die
Decorso post-OLT
• Dimesso 6/2/2015 (52 gg degenza): wbc 3850, hb9.5, plts 115, BT 5.1, ast 76, alt 108, ggt 562, aph268;
• 17/3/2015: non sintomi; funzione midollare nn, EBVDNA neg, CMV neg, colangio-RMN stenosianastomotica;
• 4/5/2015 ERCP: sfinterotomia e protesi.
• In programma biliodigestiva.
• HBsAg+
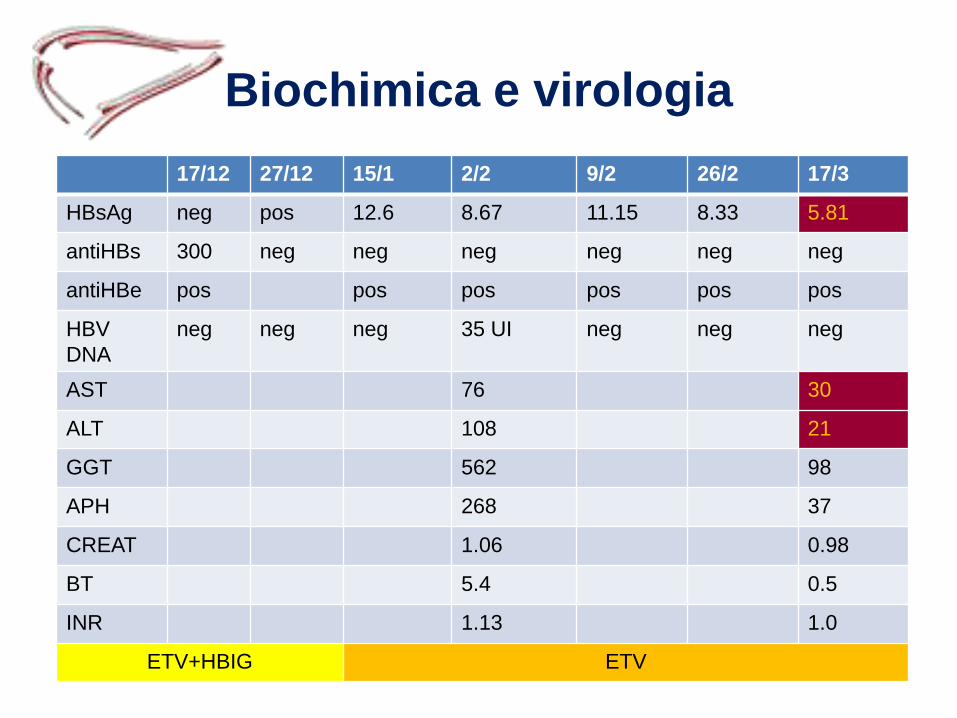
Biochimica e virologia
17/12 27/12 15/1 2/2 9/2 26/2 17/3
HBsAg neg pos 12.6 8.67 11.15 8.33 5.81
antiHBs 300 neg neg neg neg neg neg
antiHBe pos pos pos pos pos pos
HBV
DNA
neg neg neg 35 UI neg neg neg
AST 76 30
ALT 108 21
GGT 562 98
APH 268 37
CREAT 1.06 0.98
BT 5.4 0.5
INR 1.13 1.0
ETV+HBIG ETV
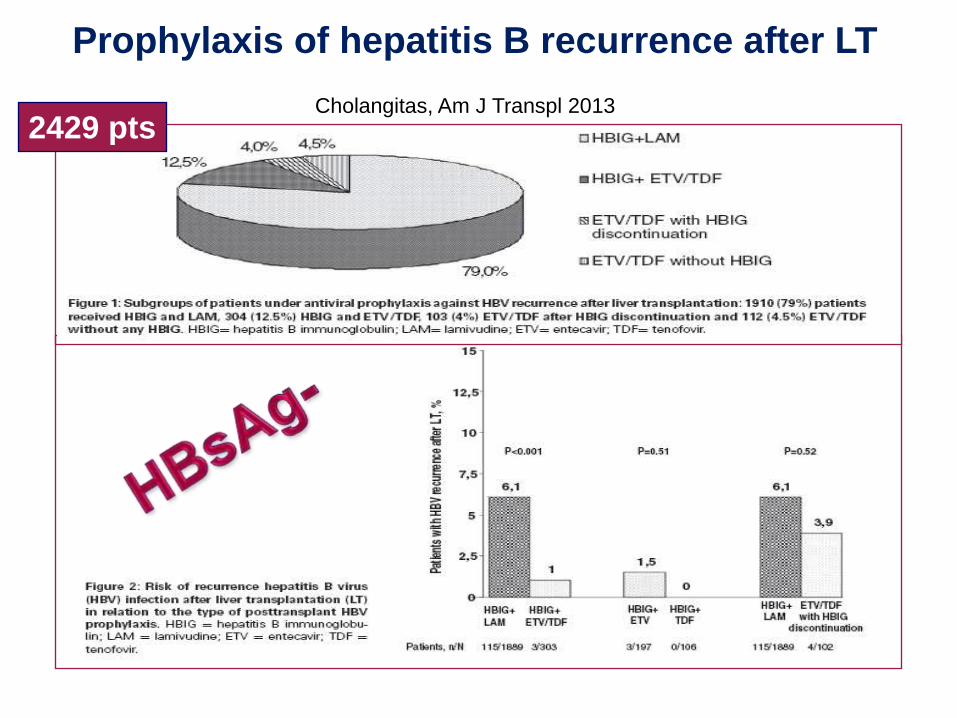
2429 pts
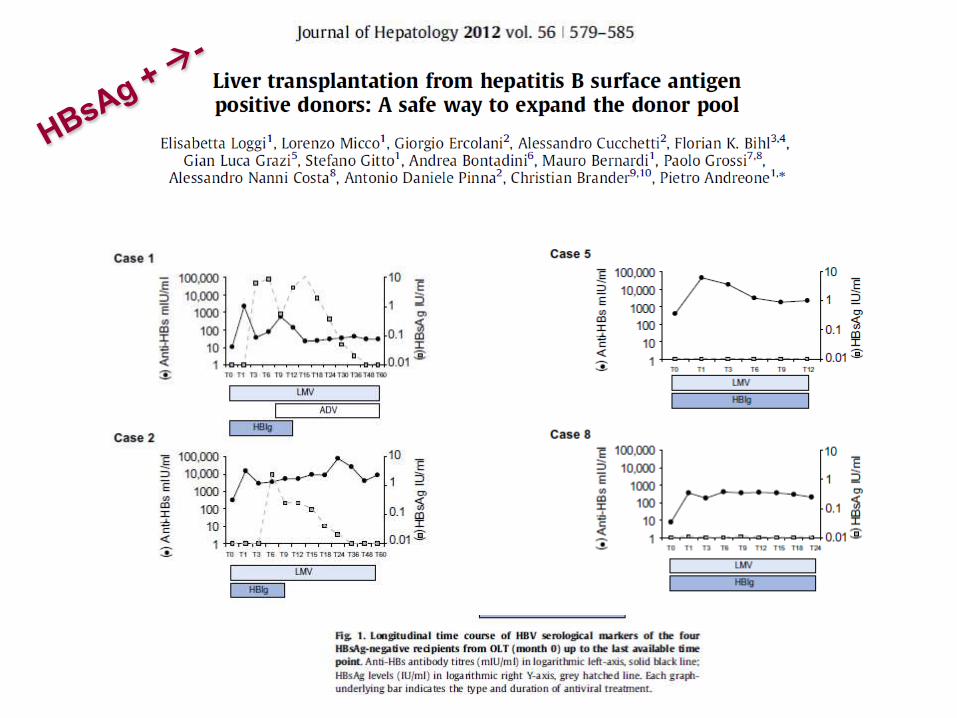
Prophylaxis of hepatitis B recurrence after LT
Cholangitas, Am J Transpl 2013
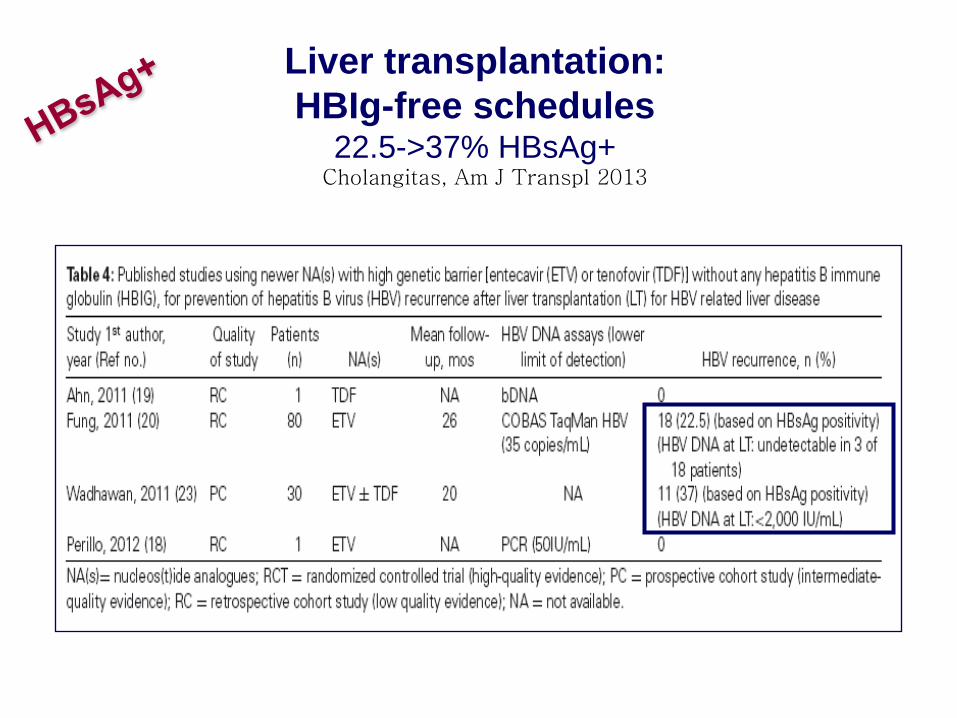
Liver transplantation:
HBIg-free schedules22.5->37% HBsAg+
Cholangitas, Am J Transpl 2013
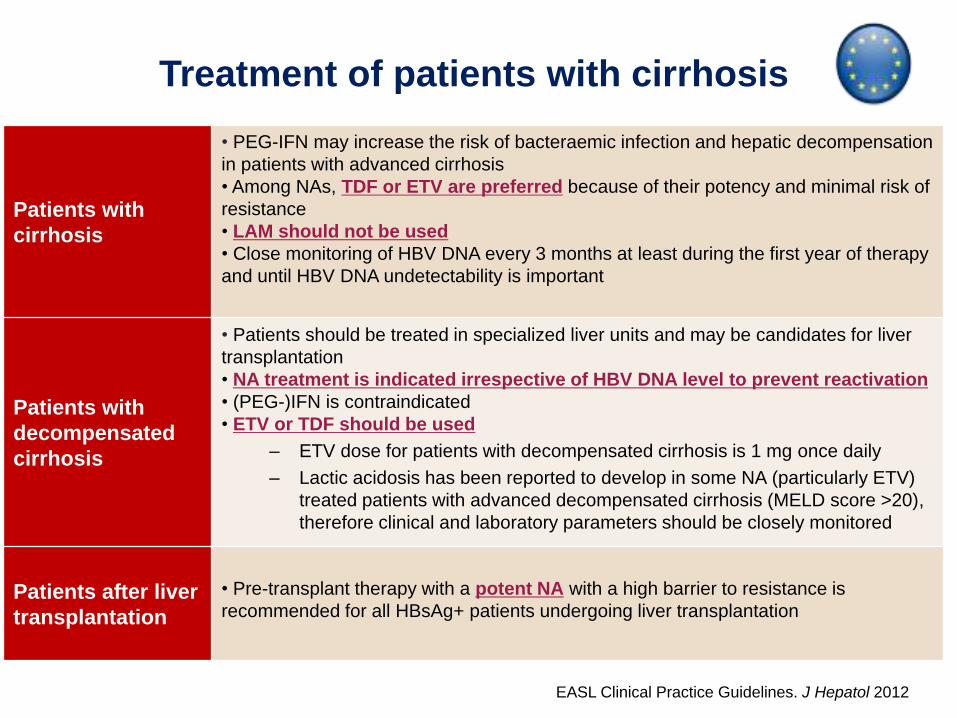
Treatment of patients with cirrhosis
Patients with
cirrhosis
• PEG-IFN may increase the risk of bacteraemic infection and hepatic decompensation
in patients with advanced cirrhosis
• Among NAs, TDF or ETV are preferred because of their potency and minimal risk of
resistance
• LAM should not be used
• Close monitoring of HBV DNA every 3 months at least during the first year of therapy
and until HBV DNA undetectability is important
Patients with
decompensated
cirrhosis
• Patients should be treated in specialized liver units and may be candidates for liver
transplantation
• NA treatment is indicated irrespective of HBV DNA level to prevent reactivation
• (PEG-)IFN is contraindicated
• ETV or TDF should be used
– ETV dose for patients with decompensated cirrhosis is 1 mg once daily
– Lactic acidosis has been reported to develop in some NA (particularly ETV)
treated patients with advanced decompensated cirrhosis (MELD score >20),
therefore clinical and laboratory parameters should be closely monitored
Patients after liver
transplantation
• Pre-transplant therapy with a potent NA with a high barrier to resistance is
recommended for all HBsAg+ patients undergoing liver transplantation
EASL Clinical Practice Guidelines. J Hepatol 2012
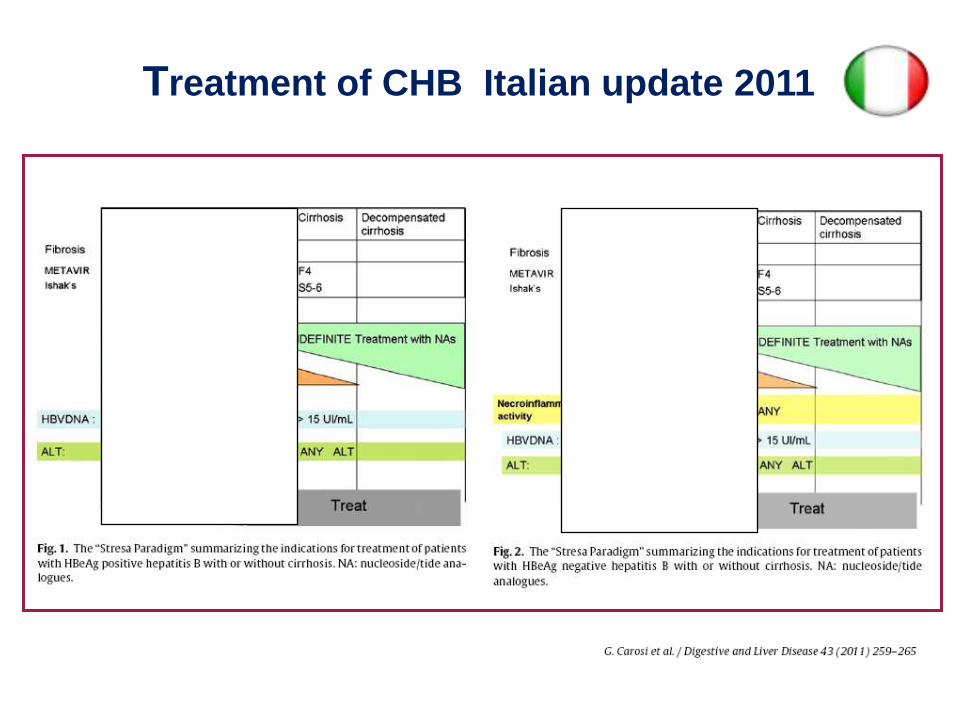
Treatment of CHB Italian update 2011
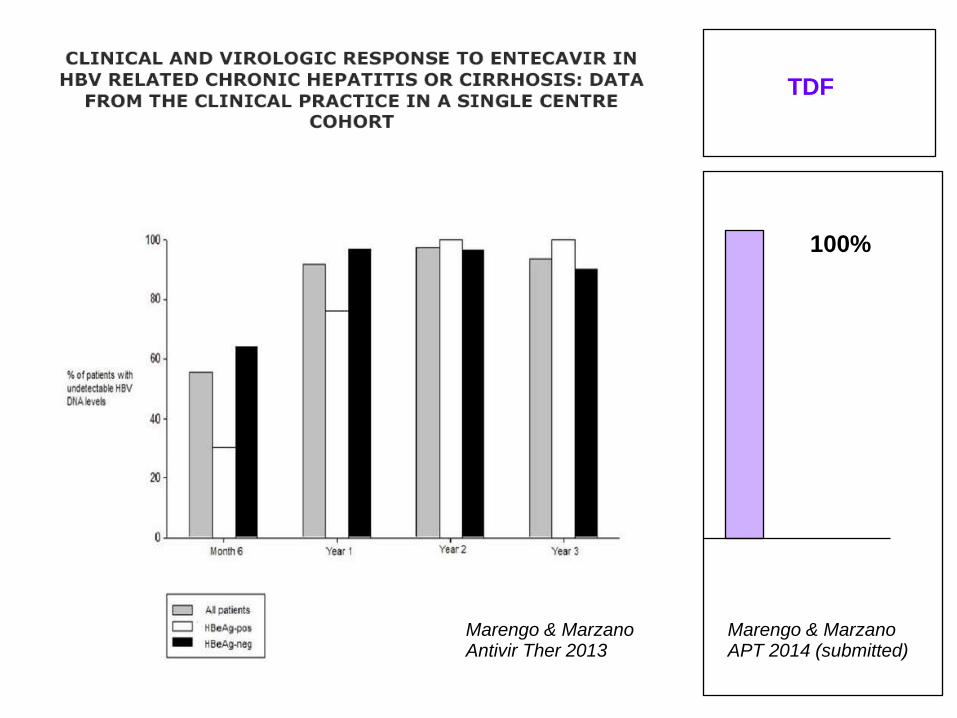
Marengo & Marzano Antivir Ther 2013
100%
TDF
Marengo & Marzano APT 2014 (submitted)
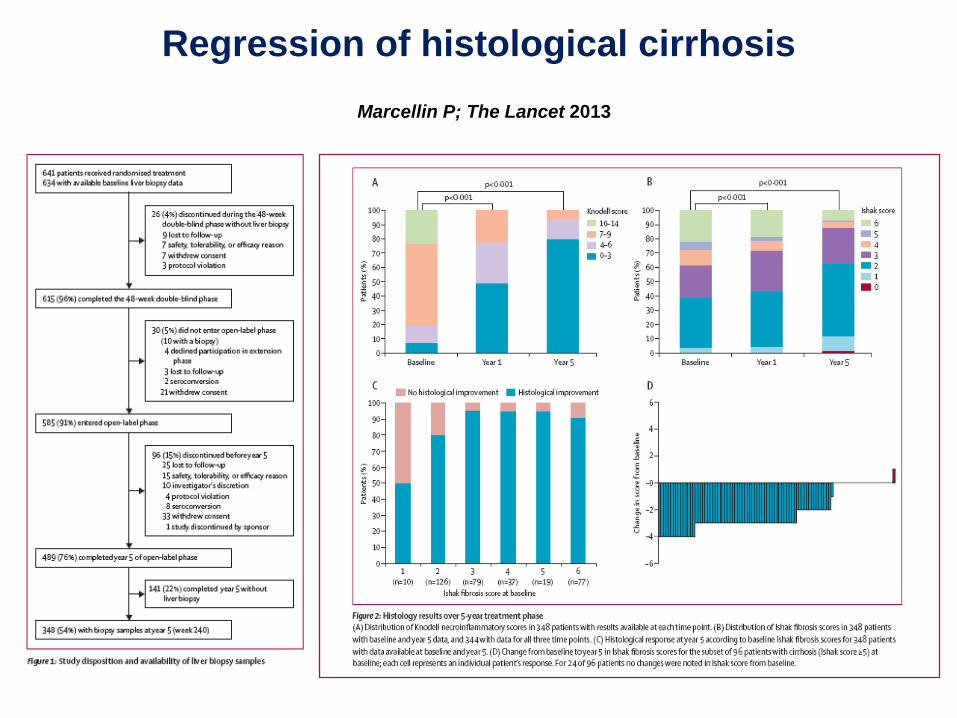
Marcellin P; The Lancet 2013
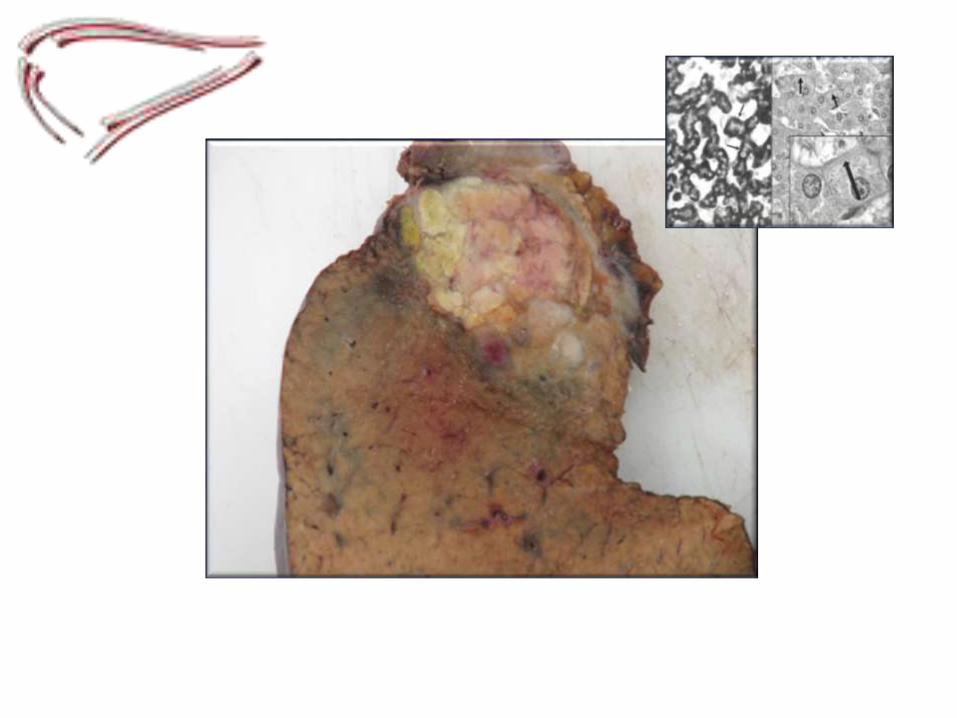
Regression of histological cirrhosis
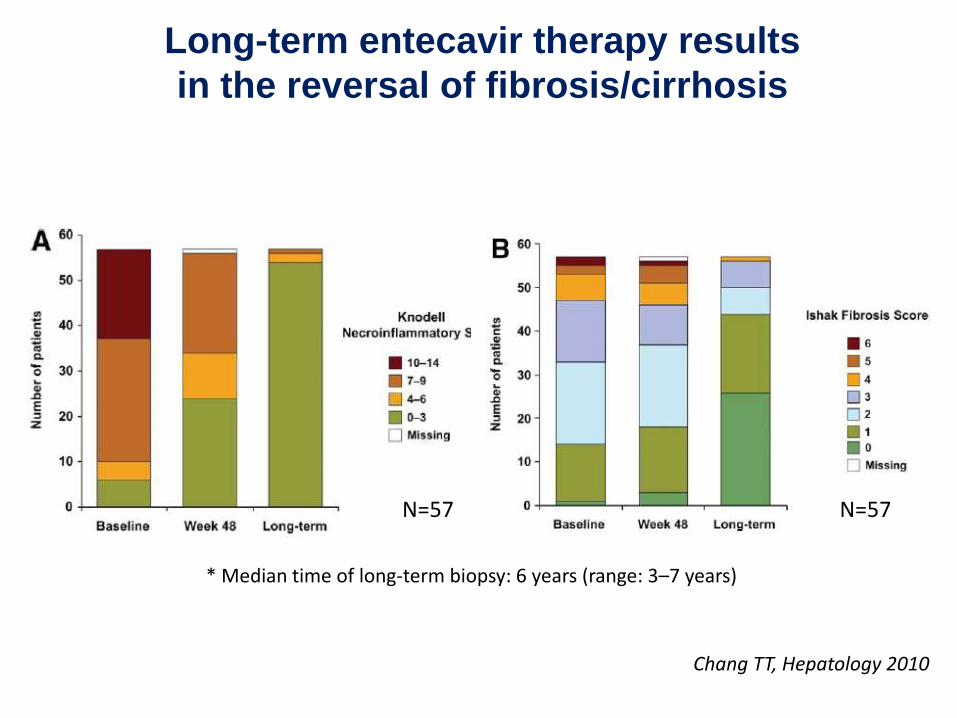
N=57N=57
* Median time of long-term biopsy: 6 years (range: 3–7 years)
Long-term entecavir therapy results
in the reversal of fibrosis/cirrhosis
Chang TT, Hepatology 2010
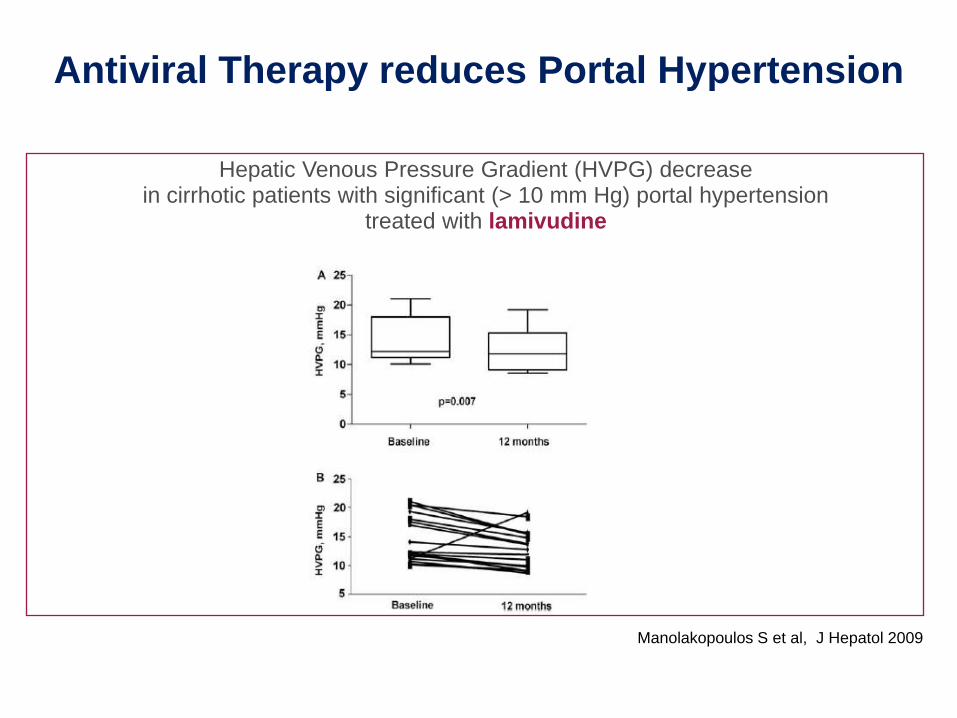
Antiviral Therapy reduces Portal Hypertension
Hepatic Venous Pressure Gradient (HVPG) decreasein cirrhotic patients with significant (> 10 mm Hg) portal hypertension
treated with lamivudine
Manolakopoulos S et al, J Hepatol 2009
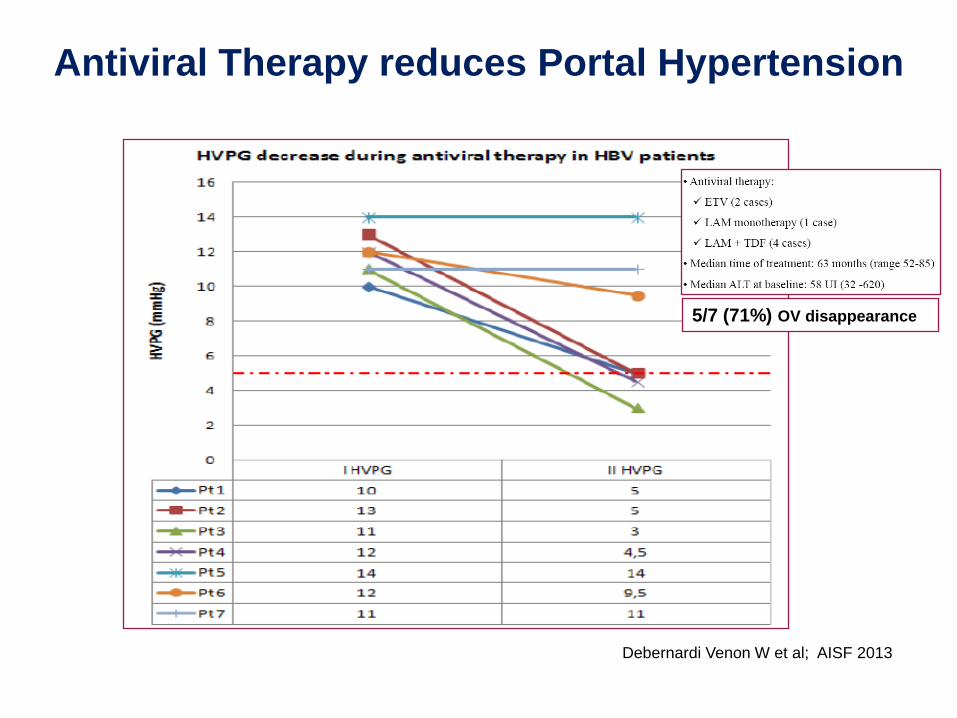
Antiviral Therapy reduces Portal Hypertension
Debernardi Venon W et al; AISF 2013
5/7 (71%) OV disappearance
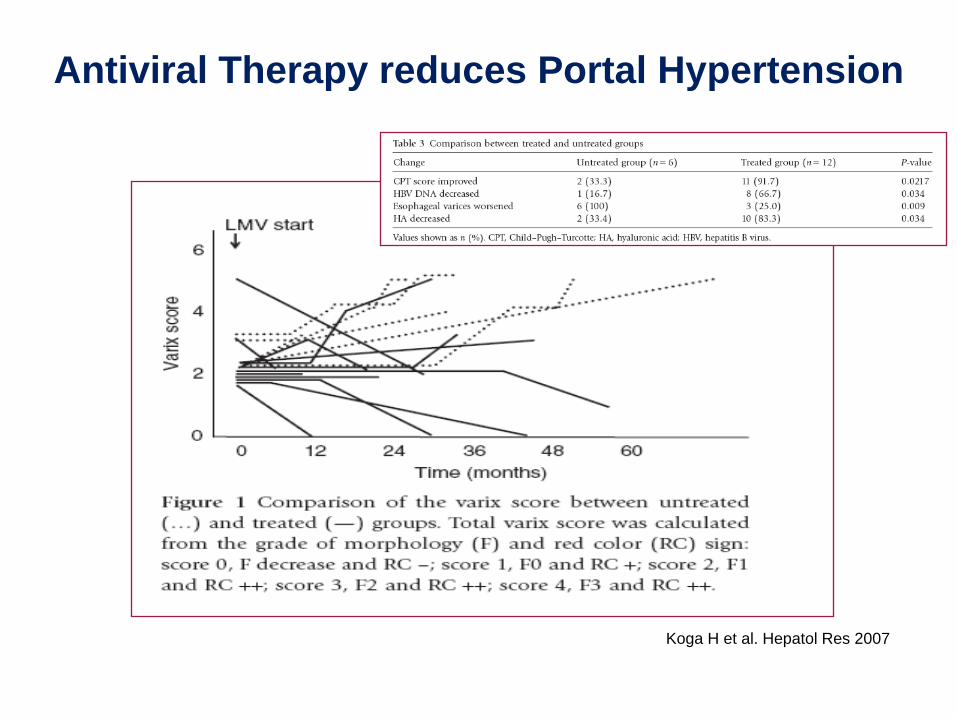
Antiviral Therapy reduces Portal Hypertension
Koga H et al. Hepatol Res 2007
0
20
40
60
80
100
0 12 24 36 48 60 72 84 96 108 120 Months
27 24 19 9 4 3
80%
2127 15 8 4
27 26 23 2
0
14 92427 21 18 14
12%
EV progression
EV regression
0
20
40
60
80
100
0 12 24 36 48 60 72 84 96 108 120
Patients
at risk80 78 74 62 45 3380 6778 56 39
8%
EV progression
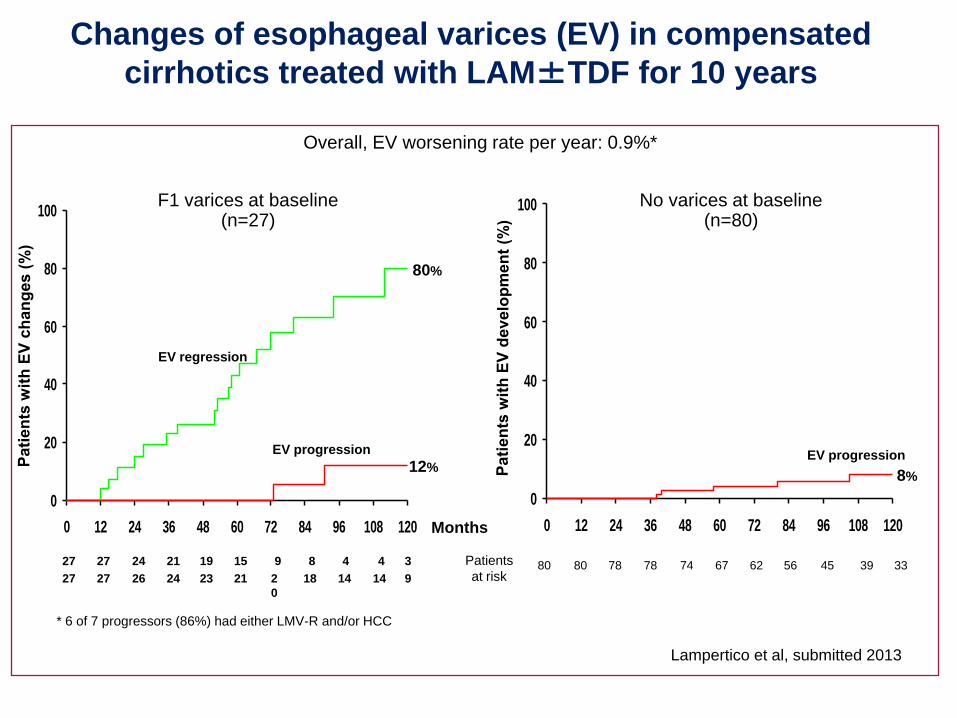
Changes of esophageal varices (EV) in compensated
cirrhotics treated with LAM±TDF for 10 years
No varices at baseline (n=80)
Lampertico et al, submitted 2013
F1 varices at baseline (n=27)
Overall, EV worsening rate per year: 0.9%*
* 6 of 7 progressors (86%) had either LMV-R and/or HCC
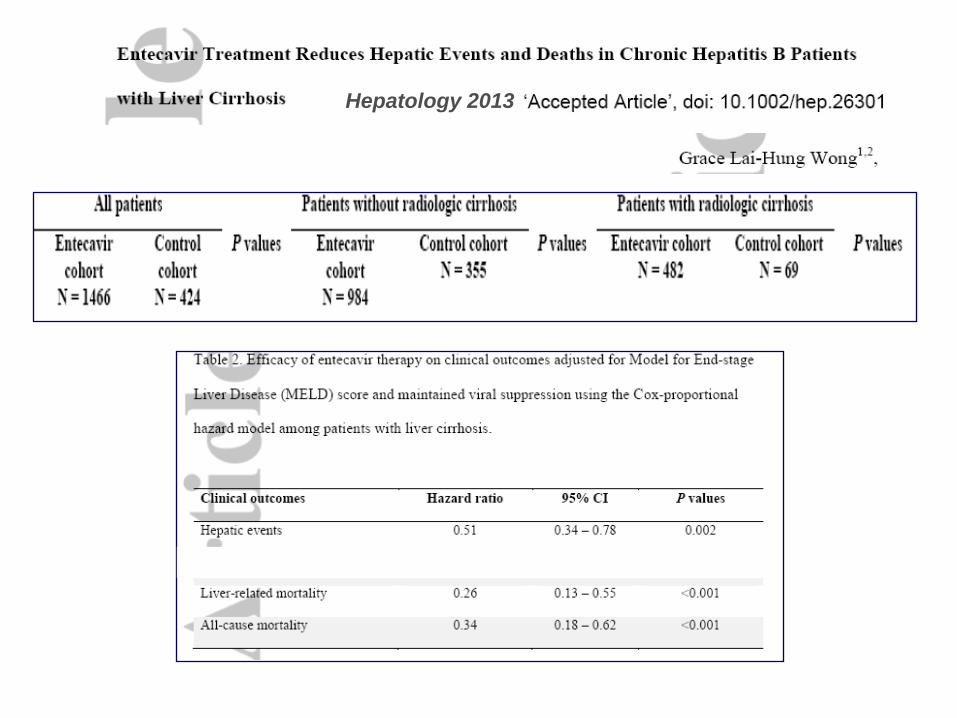
Hepatology 2013
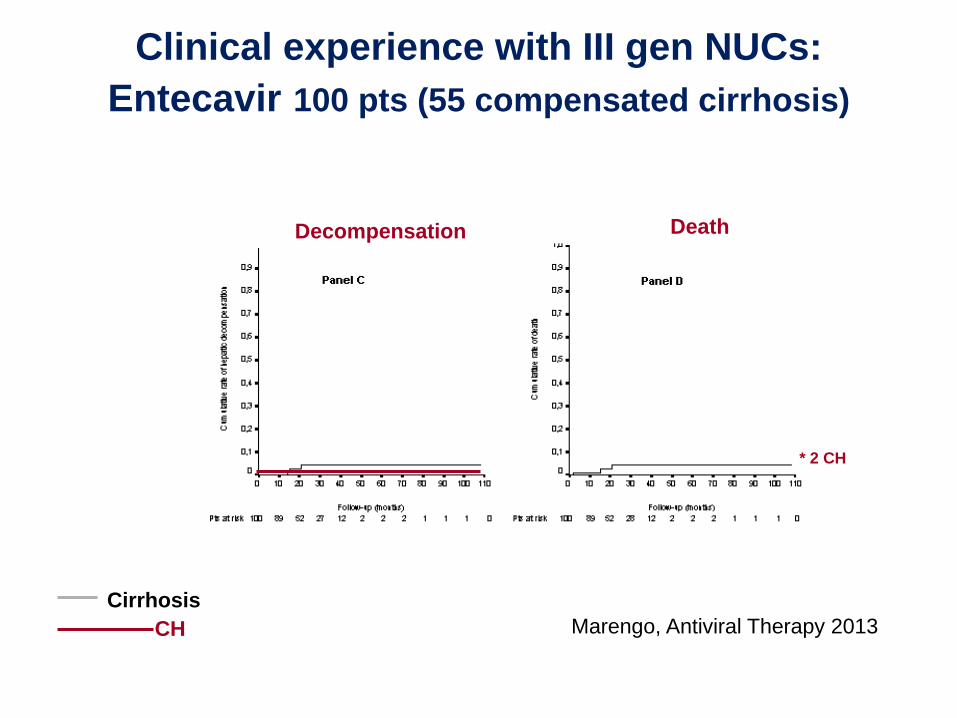
Marengo, Antiviral Therapy 2013
Decompensation Death
* 2 CH
CH
Cirrhosis
Clinical experience with III gen NUCs:
Entecavir 100 pts (55 compensated cirrhosis)
HCC
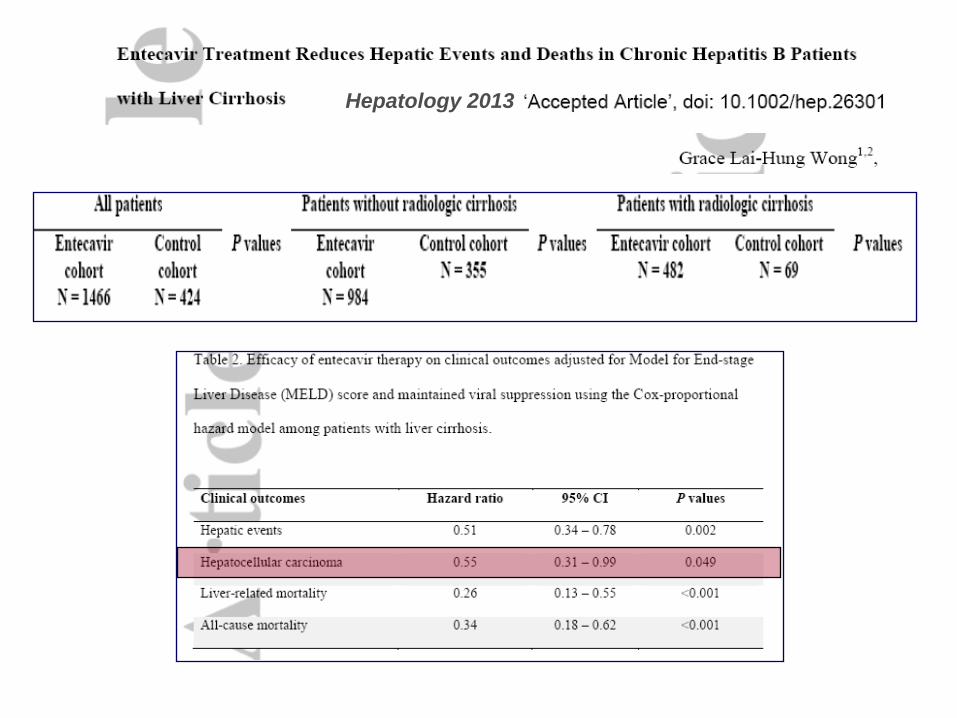
Hepatology 2013

Results
0
5
10
15
20
HVPG basal
HVPG aftertherapy
mmHg
P< 0.02
Debernardi V & Marzano.
Personal data
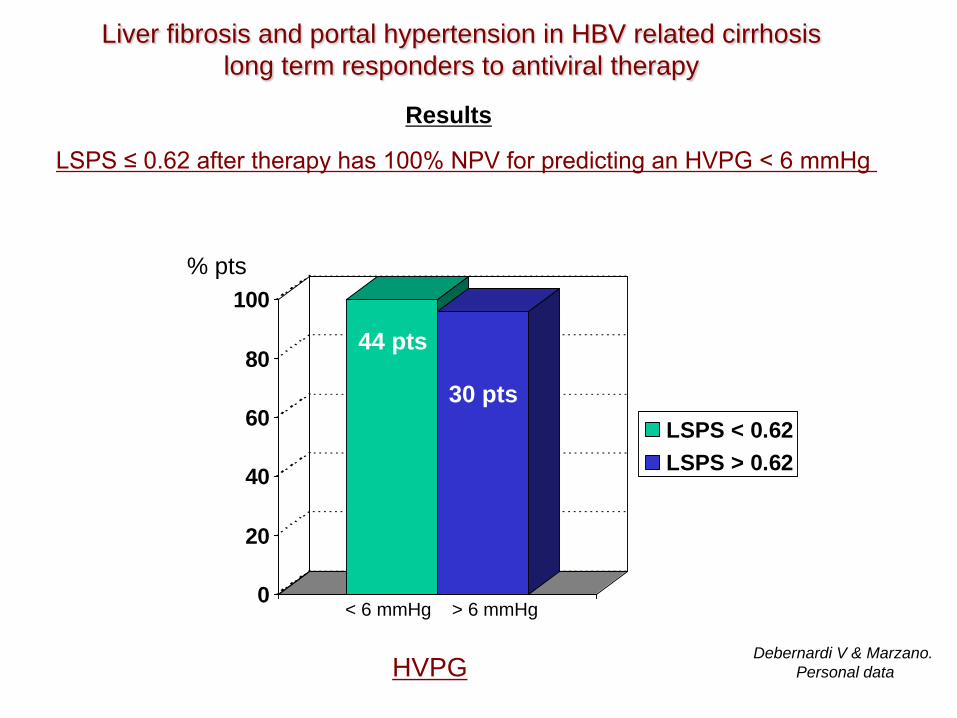
Liver fibrosis and portal hypertension in HBV related cirrhosis
long term responders to antiviral therapy
Mean
0
20
40
60
80
100
LSPS < 0.62
LSPS > 0.62
LSPS ≤ 0.62 after therapy has 100% NPV for predicting an HVPG < 6 mmHg
HVPG
< 6 mmHg > 6 mmHg
% pts
44 pts
30 pts
Results
Liver fibrosis and portal hypertension in HBV related cirrhosis
long term responders to antiviral therapy
Debernardi V & Marzano.
Personal data

Incidence of HCC: 14.8%
HCC vs no HCC: no significant difference in ALT, LS, Ø spleen, PLTS, qHBsAg
≤ 0.62 > 0.62
HCC 4/11 (36%) 7/11 (63%)*
qHBsAg (mean) 147.09 909.92*
LS ≥ 11 0/4 (mean 5.8) 6/7 (mean 16.3)*
ALT (mean) 23 42*
Ø spleen (cm) 10.1 13.4*
PLTS 185000 116000*
* p < 0.05 vs patients group with LSPS ≤0.62
Liver fibrosis and portal hypertension in HBV related cirrhosis
long term responders to antiviral therapy
Debernardi V & Marzano.
Personal data

LSPS

Epatite B
Gestione della cirrosi scompensata
Conclusioni
• tutti i cirrotici vanno trattati con NUC
• in caso di scompenso: NUC, trattamento delle
complicanze legate all’ipertensioine portale ed al
profilo emodinamico + bilancio OLT