APPROCCIO TERAPEUTICO NELLE FORME · PDF filequestionnaire (MG-QOL15) Alberto Raggi1, PsyD;...
20
Bolzano, 12 Maggio 2017 SCALE DI VALUTAZIONE ED APPROCCIO TERAPEUTICO NELLE FORME ADULTE Dott. Mauro Scarpelli UOC Neurologia A AOUI Verona
Transcript of APPROCCIO TERAPEUTICO NELLE FORME · PDF filequestionnaire (MG-QOL15) Alberto Raggi1, PsyD;...

Bolzano, 12 Maggio 2017
SCALE DI VALUTAZIONE ED
APPROCCIO TERAPEUTICO NELLE
FORME ADULTE
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Dott. Mauro Scarpelli UOC Neurologia A AOUI Verona

Scale di valutazione
Necessarie per seguire il paziente nel tempo, ridurre la variabilità di giudizio tra i clinci, valutare l’efficacia degli interventi terapeutici
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Affinchè siano applicate correttamente, è spesso necessario un training di apprendimento
Affiancano, e non sostituiscono, la visita clinica

Scale di valutazione
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984

Scale di valutazione
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
The Quantitative Myasthenia Gravis (QMG) Test
The Manual
(This Manual is Designed to Accompany the Videotape)
Richard J.Barohn, M.D., Professor of Neurology Laura Herbelin, Clinical Evaluator
University of Texas Southwestern Medical Center Dallas, TX
Il paziente non deve avere assunto piridostigmina nelle 12 ore precedenti l’esecuzione del test

Scale di valutazione
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Classificazione MGFA (Jaretzi, Neurology 2000)Gravità clinica (Classe I-V) “Clinical score”Risposta alla terapia

Scale di valutazione
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
ORIGINAL COMMUNICATION
Validation of the MG-DIS: a disability assessment for myastheniagravis
Alberto Raggi1 • Matilde Leonardi1 • Silvia Schiavolin1 • Carlo Antozzi2 •
Greta Brenna2 • Lorenzo Maggi2 • Renato Mantegazza2
Received: 9 November 2015 / Revised: 12 February 2016 / Accepted: 15 February 2016 / Published online: 1 March 2016! Springer-Verlag Berlin Heidelberg 2016
Abstract This paper is aimed to present the validation ofthe myasthenia gravis disability assessment (MG-DIS), a
MG-specific patient-reported disability outcome measure.
Consecutive MG patients were enrolled, followed-up for12 months and administered the SF-36, the WHO disability
assessment schedule (WHODAS 2.0) and the preliminary
31-item MG-DIS addressing impairments and activitylimitations. Factor structure and metric properties were
assessed. In total, 109 patients were enrolled: 76 were
females, mean age 50, mean MG duration 10.4 years, 86were AChR-positive. The MG-DIS was reduced to 20
items, explaining 70.6 % of the original questionnaire
variance, four subscales (generalized impairment-relatedproblems; bulbar function-related problems; mental health
and fatigue-related problems; vision-related problems) and
an overall disability index. The MG-DIS has good metricproperties (Cronbach’s alpha ranging between .808 and
.930), is stable, showed to be more sensitive than the
WHODAS 2.0 and SF-36 to detect group differences andlongitudinal changes and was well correlated with the MG-
composite (.642). The MG-DIS includes items representingocular, generalized, bulbar and respiratory symptoms, and
is therefore well-built around MG-specific features. MG-DIS can be used in clinical trials as well as in observational
or epidemiological studies to characterize patients’ dis-
ability level and address the amount of improvement indisability. Further studies are needed to explore the pos-
sibility of a shorter disability scale.
Keywords Myasthenia gravis ! Disability evaluation !Factor analysis ! Validation study ! Patient-reportedoutcome
Introduction
Myasthenia gravis (MG) is an autoimmune disease caused
by autoantibodies to the post-synaptic site of the neuro-
muscular junction, whose main features are fluctuatingmuscle weakness and fatigability [1]. Typically, MG
affects women with a bimodal period of onset, around
20–40 and 60–80 years of age [2, 3]. Staging of MG rec-ognizes different forms, depending on the severity of
weakness and fatigability and on muscle involvement
(ocular, generalized, bulbar or respiratory). As shown in aliterature review, outcome measures for MG are mostly
focused on clinical manifestations that are deemed to beimmediately evident and relevant for clinicians dealing
with MG patients [4]. However, due to the unique char-
acteristics of MG (i.e. the fact that symptoms are evident tothe patient and can fluctuate during the day), it is important
that patient-reported outcomes measures (PROMs) are
incorporated in patient’s assessment. This was also one ofthe recommendations for clinical trials in MG, which
highlighted the need to incorporate subject responses into
trial outcome measures [5]. PROMs are increasingly usedin clinical trials and in descriptive studies, as they complete
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00415-016-8072-9) contains supplementarymaterial, which is available to authorized users.
& Alberto [email protected]
1 Neurology, Public Health and Disability Unit, NeurologicalInstitute C. Besta IRCCS Foundation, Via Celoria 11,20133 Milan, Italy
2 Department of Neuroimmunology and NeuromuscularDisorders, Neurological Institute C. Besta IRCCSFoundation, Milan, Italy
123
J Neurol (2016) 263:871–882
DOI 10.1007/s00415-016-8072-9
Scala che valuta la disabilità, composta da 20 items, compilata dal paziente
Validation of the Italian version of the 15-item Myasthenia Gravis Quality of Life
questionnaire (MG-QOL15)
Alberto Raggi1, PsyD; Matilde Leonardi1, MD; Roberta Ayadi1, MSc; Carlo Antozzi2, MD;
Lorenzo Maggi2, MSc; Fulvio Baggi2, MSc; Renato Mantegazza2, MD.
Neurological Institute C. Besta IRCCS Foundation: 1) Neurology, Public Health and Disability
Unit; 2) Department of Neuroimmunology and Neuromuscular Disorders
Acknowledgement: This study was supported by Besta Institute Foundation.
Corresponding Author
Alberto Raggi, PsyD
Neurology, Public Health and Disability Unit – Neurological Institute C. Besta IRCCS Foundation
Via Celoria 11, 20133 – Milan (Italy);
Phone, +39.02.2394.3105 (2521); fax, +39.02.2394.2442; e-mail: [email protected]
Running title: Italian MG-QOL15
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/mus.25545
This article is protected by copyright. All rights reserved.

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984 I farmaci cardine della terapia sono:
- piridostigmina: sintomatico, agisce a livello della trasmissione neuromuscolare
- steroide: interviene a livello patogenetico riducendo l’azione degli anticorpi
- immunosoppressore: riduce la produzione di autoanticorpi e permette di limitare l’utilizzo dello steroide (e i conseguenti effetti collaterali)

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984 Piridostigmina:
- inibitore dell’acetilcolinesterasi; dose incrementale (60 mg x5) fino alla tollerabilità del paziente. Rapidità d’azione, non effetti collaterali a lungo termine
- in genere poco efficace nelle forme oculari (ha più effetto sulla ptosi che sulla diplopia)
- in genere poco efficace nella MG da antcorpi anti-MuSK

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984 Steroide (prednisone):
- iniziale incremento graduale per evitare un transitorio peggioramento dei sintomi
- la somministrazione a giorni alterni non riduce significativamente l’insorgenza di effetti collaterali
- raggiunta la stabilizzazione clinica, riduzione alla dose minima efficace

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984 Immunosoppressore:
- azatioprina è la prima scelta (2-3 mg/kg)
- da evitare in soggetti con attività di tiopurina metiltransferasi ridotta/assente
- micofenolato mofetile, ciclosporina, metotrexate, tacrolimus sono seconde scelte equivalenti

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984 Immunosoppressore (anticorpi monoclonali):
- rituximab (anti-CD20) sempre più utilizzato; particolarmente efficace nelle forme anti MuSK
- ruxolitinib, eculizumab e altri, usati in maniera aneddotica
- trapianto autologo di staminali ematopoietiche ha dato buoni risultati (remissione farmacologica) in 7 pazienti

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
REVIEW
Efficacy and safety of rituximab for myasthenia gravis:a systematic review and meta-analysis
Raffaele Iorio • Valentina Damato •
Paolo Emilio Alboini • Amelia Evoli
Received: 2 September 2014 / Revised: 3 October 2014 / Accepted: 4 October 2014 / Published online: 12 October 2014! Springer-Verlag Berlin Heidelberg 2014
Abstract Myasthenia gravis is an autoimmune disorderof the neuromuscular junction caused by circulating anti-
bodies specific for the post-synaptic acetylcholine receptor
or, in a minority of cases, for the muscle-specific tyrosine-kinase and the low-density lipoprotein receptor-related
protein 4. A wide range of symptomatic and immunosup-
pressive treatments is currently available for MG patientswith variable outcome. However, most immunosuppressive
treatments are characterized by delayed onset of action and
in some cases are not sufficient to induce stable remissionof the disease. Rituximab (RTX) is a chimaeric monoclonal
antibody specific for the CD20 B-cell surface antigen.
Recent studies have provided evidence that RTX may be aneffective treatment for patients with myasthenia gravis
(MG) who are refractory to standardized immunosuppres-
sive therapy. We performed a systematic review and ameta-analysis of the efficacy and safety of RTX in myas-
thenia gravis considering the potential predictive factors
related to patients’ response to RTX in this disease.
Keywords Rituximab ! Myasthenia gravis !Immunotherapy ! Antibodies
Introduction
Myasthenia gravis (MG) is a rare disorder of the neuro-
muscular junction, caused by antibodies (Ab) against post-synaptic membrane proteins. The muscle acetylcholine
receptor (AChR) is the main antigen, as AChR-Ab can be
detected in up to 85–90 % of MG patients. AChR-Ab aremainly of IgG1 and IgG3 isotypes, and induce severe
alterations of the post-synaptic membrane through AChR
increased degradation and complement activation [1].Around 40 % of patients with AChR-negative MG have
serum Ab to the muscle-specific tyrosine-kinase (MuSK).
MuSK-Ab induce severe functional alteration of the neu-romuscular junction, although, being mostly IgG4, they do
not activate complement [2].
The aim of MG treatment is first to induce and thenmaintain remission, avoiding unnecessary toxicity. Cur-
rent treatment options include acetylcholinesterase inhib-
itors, short-term immune therapies such as plasmapheresisor intravenous immunoglobulin (IVIG), and long-term
treatment with corticosteroids, and immunosuppressiveagents including, but not exclusively, azathioprine (AZA),
mycophenolate mofetil (MMF) and cyclosporine (CYA)
[3]. Conventional treatment is effective, as it can controlsymptoms in most patients. However, this outcome often
requires prolonged and even life-long immunosuppres-
sion. Moreover, a proportion of patients have refractorydisease as they complain of disabling weakness or fre-
quent relapses and/or require too high doses of steroids
or other immunosuppressive agents with serious sideeffects [4].
Rituximab (RTX), is a mouse/human chimeric IgG1
monoclonal antibody that binds to CD20 B lymphocytessurface antigen, which is involved in B-cell activation, dif-
ferentiation and growth [5]. RTX was initially developed and
R. Iorio (&)Don Carlo Gnocchi ONLUS Foundation, Milan, Italye-mail: [email protected]
V. Damato ! P. E. Alboini ! A. EvoliInstitute of Neurology, Department of Geriatrics, Neurosciencesand Orthopedics, Catholic University, l.go Gemelli, 8,00168 Rome, Italy
123
J Neurol (2015) 262:1115–1119
DOI 10.1007/s00415-014-7532-3
REFERENCES
1. Jiang N, Nutter TJ, Cooper BY. Molecular and cellular influences ofpermethrin on mammalian nociceptors at physiological tempera-tures. Neurotoxicology 2013;37:207–219.
2. Narahashi T. Modification of nerve membrane sodium channels by theinsecticide pyrethroids. Comp Bicoehm Physiol C 1982;72:411–414.
3. Nutter TJ, Jiang N, Copper BY. Persistent Na 1 and K 1 channel dys-functions after chronic exposure to insecticides and pyridostigminebromide. Neurotoxicology 2013;39:72–83.
4. Abou-Donia MB, Wilmarth KR, Jensen KF, Oehme FW, Kurl TL. Neu-rotoxicity resulting from co-exposure to pyridostigmine bromide,deet, and permethrin: implications of Gulf War chemical exposures.J Toxicol Environ Health 1996;48:35–56.
5. Classes of Pesticides. (Vol. 3) In: Hayes WJ, Laws ER, editors. Handbookof pesticide toxicology. New York, NY: Academic Press, Inc; 1990.
6. Engel AG, Tsujihata M, Lindstrom JM, Lennon VA. The motor endplate in myasthenia gravis and in experimental autoimmune myasthe-nia gravis. Ann N Y Acad Sci 1976:274:60.
Published online 16 November 2016 in Wiley Online Library(wileyonlinelibrary.com). DOI 10.1002/mus.25434
---------------------------------------------------------
REMISSION OF MYASTHENIA GRAVIS WITHMuSK Antibodies During RuxolitinibTreatment
Myasthenia gravis (MG) with antibodies (Abs) to themuscle-specific tyrosine kinase receptor (MuSK-MG) is arare disease that accounts for 5–8% of all MG cases. InMuSK-MG, patients have increased frequency of Th1and Th17 subsets of CD41 T-cells.1 Differentiation ofCD41 T-lymphocytes is driven by activation of the Januskinase/signal transducer and activator of transcription(JAK/STAT) pathway,2 and cytokine-activated STAT pro-teins control the balance of different T-cell subsets.3
We report a MuSK-MG patient who achieved remis-sion after treatment with ruxolitinib for myelofibrosis. A70-year-old woman was referred with a diagnosis of ace-tylcholine receptor (AChR) Ab-negative MG. Neurologi-cal evaluation showed fluctuating diplopia, milddysphagia with chewing fatigability, and facial and neckmuscle weakness (MRC score 4); the quantitative MGscore was 7. Anti-AChR Abs were confirmed to be absent,and anti-MuSK Abs were detected (7.5 nMol/L; normal,< 0.05). Single fiber electromyography (SFEMG) of theorbicularis oculi muscle confirmed abnormal neuromus-cular transmission, showing 80% of pairs with increasedjitter, 40% of pairs with impulse blocking, and a meanconsecutive difference (MCD) of 89 ls (normal, < 36 ls).As the patient’s symptoms were moderate, immunosup-pressive treatment was not performed. MG statusremained more or less unchanged for years, with inter-
mittent pyridostigmine therapy (30 mg 3 times daily).MuSK Abs were re-tested in 2006 and in 2010 and againpositive (5.4 and 6.3 nMol/L, respectively).
In 1994, the patient was diagnosed with polycythemiavera. She was treated with piperazine (25 mg daily) andacetylsalicylic acid (ASA) (100 mg daily), with good con-trol until 2012, when it evolved in myelofibrosis. Pipera-zine and ASA were discontinued, and hydroxyurea(500 mg twice daily, orally) was prescribed. This treat-ment was not beneficial, and in the last months of 2014she needed transfusions every 30 days. Since February2015, she received ticlopidine (250 mg daily) and ruxoli-tinib (10 mg twice daily, orally), with improvement ofblood parameters. During the last follow-up visit inMarch 2016, she reported not taking pyridostigmine for6 months and had no MG symptoms. Clinical examina-tion detected no muscle weakness or fatigability, and theMuSK Ab assay was negative (0.03 nMol/L). SFEMG ofthe orbicularis oculi muscle showed no impulse block-ing, and MCD was normal (23.2 ls).
The JAK/STAT pathway constitutes the core of manycellular activities through cytokine activation. JAK/STATpathway inhibition reduces cell proliferation andSTAT3/STAT5 phosphorylation, thus decreasing circu-lating levels of inflammatory cytokines. This effect hasproven useful in cancer and autoimmune disease treat-ment. Two JAK/STAT blockers are currently available astherapeutics: tofacitinib and ruxolitinib.4
Tofacitinib is effective in inflammatory bowel disease,psoriasis, and rheumatoid arthritis.4 Ruxolitinib, a selec-tive inhibitor of JAK1 and JAK2, has been approved inthe United States and Europe for intermediate- or high-risk myelofibrosis.5 Associated side-effects are most com-monly hematologic (reversible myelosuppression); head-ache, vomiting, diarrhea, and opportunistic infectionshave also been reported.5
Ruxolitinib treatment has resulted in remission ofrefractory dermatomyositis when it was administered forconcomitant myelofibrosis,6 and it is a promisingapproach for alopecia areata7 and rheumatoid arthritis.4
Spontaneous MG recovery cannot be strictly ruledout in our patient, but ruxolitinib administration is likelyto have been directly therapeutic. It may be worthwhileto further assess the efficacy of JAK/STAT inhibition inMG as well as in other autoimmune diseases.
Author contributions: Dr. Alboini: data collection, drafting of themanuscript, interpretation of results. Dr. Evoli: study design, datacollection, interpretation of results, review of the manuscript forintellectual content. Dr. Damato: data collection, interpretation ofresults. Dr. Iorio: data collection, interpretation of results.Dr. Bartoccioni: data collection, interpretation of results.
Paolo E. Alboini, MD1
Amelia Evoli, MD1
Valentina Damato, MD1
Raffaele Iorio, MD, PhD1,*
Emanuela Bartoccioni, PhD 2
1Institute of Neurology, Largo F. Vito, 1 – 00168,Catholic University, Rome, Italy2General Pathology, Catholic University, Rome, Italy
Abbreviations: Abs, antibodies; AChR, anti-acetylcholine receptor; ASA,acetylsalicylic acid; EMG, electromyography; JAK/STAT, Janus kinase/signal transducer and activator of transcription; MCD, mean consecutivedifference; MG, myasthenia gravis; MuSK, muscle-specific tyrosine kinasereceptor; SFEMG, single fiber electromyographyKey words: JAK/STAT; JAK/STAT inhibitors; MuSK; myasthenia gravis;myelofibrosis; ruxolitinibCorrespondence to: A. Evoli; e-mail: [email protected]
Conflicts of Interest: Paolo E. Alboini declares no conflict of interests. AmeliaEvoli: advisory board for CSL Behring, scientific award jury member for Grifols.Valentina Damato declares no conflict of interests. Raffaele Iorio declares noconflict of interests. Emanuela Bartoccioni declares no conflict of interests.
VC 2016 Wiley Periodicals, Inc.
E12 Noteworthy Cases MUSCLE & NERVE March 2017
Marked Clinical and Jitter Improvement after Eculizumab in Refractory Myasthenia Vern C. Juel, M.D.,1 Donald B. Sanders, M.D.,1 Lisa D. Hobson-Webb, M.D.,1 Janice M. Massey, M.D.,1 Jeffrey T. Guptill, M.D.,1 Fanny O’Brien, Ph.D.,2 Jing Jing Wang, M.D.,2 James F. Howard, Jr., M.D.3 Author Affiliations:
1. Department of Neurology, Duke University Medical Center, Durham, NC, 27710, USA
2. Departments of Clinical Research and Global Medical Affairs, Alexion Pharmaceuticals, Cheshire, CT, 06410, USA
3. Department of Neurology, University of North Carolina, Chapel Hill, NC, 27599-7025,
USA Acknowledgments: We recognize Kate Beck, RN, clinical trials coordinator, for conducting clinical trial visits and assessments in the study subject. Words: 621 Figures: 1 References: 7 Corresponding author: Vern C. Juel, M.D. 200 Trent Drive, DUMC 3403 Duke University Medical Center Durham, NC 27710 Telephone: 919-684-4044 Fax: 919-660-3853 e-mail: [email protected] Running title: Eculizumab in Refractory MG
Abstract presented at the Myasthenia Gravis Foundation of America Scientific Session, Savannah, Georgia, November 1, 2014.
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/000.00000
This article is protected by copyright. All rights reserved.

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
n en
gl j m
ed 375;26
nejm
.org
D
ecember 29, 2016
2576
The n
ew
en
gl
an
d jo
ur
na
l of m
ed
icin
e
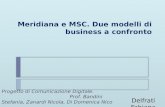
Table 2. Drugs Used Most Frequently for the Treatment of Myasthenia Gravis.
Drug Mode of Action Dose Side Effects Risks and Contraindications
Pyridostigmine Symptomatic; acetylcholinesterase inhibition
Single dose: 10–120 mg; daily dose: 40–600 mg
Cholinergic autonomic effects Cholinergic crisis
Prednisone or prednisolone
Immunomodulation Induction dose: 40–80 mg daily; stable dose: 5–20 mg daily; alternate-day treatment is an alternative
Widespread dose-dependent glucocorticoid effects
Gastrointestinal bleeding, cushingoid appearance
Azathioprine Suppression of B and T cells 50–250 mg daily Nausea, vomiting, tiredness, infections, night sweats
Leukopenia, liver toxicity
Mycophenolate mofetil Suppression of B and T cells 1.5–2 g daily Nausea, vomiting, diarrhea, joint pain, infections, tiredness
Leukopenia, progressive multifocal leukoencephalopathy; contraindi-cated during pregnancy
Rituximab Suppression of B cells 0.5–1 g, repeated after 2 wk; can be repeated at 6-mo intervals
Nausea, infections, infusion-related problems
Progressive multifocal leukoencepha-lopathy
Methotrexate Inhibition of folate metabolism Gradual increase to 20 mg/wk Nausea, infections, lung disease Leukopenia, liver toxicity; contraindicat-ed during pregnancy
Cyclosporine Suppression of T cells and natural killer cells
2.5–5 mg/kg of body weight daily Nausea, hypertension, infections, hypertrichosis
Kidney toxicity
Tacrolimus Suppression of T cells and natural killer cells
3 mg daily Nausea, infections, lung disease, hyperten-sion, neuropsychiatric problems
Liver and kidney toxicity
Cyclophosphamide Suppression of B and T cells 1–5 mg per kg administered by intravenous infusion every 4 wk for a limited period
Nausea, vomiting, alopecia, discoloration of nails and skin, infections
Leukopenia
Intravenous immune globulin
Suppression of B and T cells, neutralization of autoantibodies
2 g per kg administered over a period of 2 to 5 days
Nausea, headache, fever, hypotension or hypertension, local skin reactions
IgA deficiency, allergic reactions
The New
England Journal of Medicine
Dow
nloaded from nejm
.org by mauro scarpelli on D
ecember 29, 2016. For personal use only. N
o other uses without perm
ission. C
opyright © 2016 M
assachusetts Medical Society. A
ll rights reserved.

n engl j med 375;26 nejm.org December 29, 2016 2577
Myasthenia Gr avis
antibody binds specifically to the CD20 surface antigen on B lymphocytes and should therefore be effective in antibody-mediated diseases such as myasthenia gravis. T-cell responses are also influenced by rituximab. A group of experts who recently issued guidelines for the management of myasthenia gravis could not reach a consensus on the role of rituximab.11 Evidence from small case series indicates that two thirds of patients with severe myasthenia gravis and an insuffi-cient response to prednisolone and azathioprine
have a substantial improvement with rituximab.60 A recommended induction dose has not been established. The treatment should be repeated if the symptoms recur after several months. Con-cerns regarding rituximab are the risk of pre-cipitating additional autoimmune disorders and JC virus–related progressive multifocal leukoen-cephalopathy. The treatment scheme for general-ized myasthenia gravis is summarized in Fig-ure 3A.
A number of monoclonal antibody drugs have
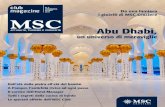
Figure 3. Proposed Treatment Algorithms for Generalized Myasthenia Gravis and for Severe Exacerbations of Generalized Disease.
Panel A shows treatments for generalized myasthenia gravis, and Panel B shows treatments for severe exacerbations. Both algorithms are from Gilhus and Verschuuren.2 IV denotes intravenous.
A Proposed Treatment for Generalized Myasthenia Gravis B Proposed Treatment for Severe Exacerbations of GeneralizedMyasthenia Gravis
Acetylcholinesterase inhibitor andthymectomy (if early onset or thymoma)
Diagnosis confirmed
Continue withacetylcholin-
esterase inhibitorClinical remission?
Prednisolone and azathioprine
No
Yes
Continue withlowest
possible doseAdequate effect?
Mycophenolate mofetil for mild or moderate symptoms
Rituximab for severe symptomsOther immunosuppressive drugs
No
Yes
ContinuetreatmentSufficient effect?
Other immunosuppressive drugs(methotrexate, cyclosporine, tacrolimus)
Reevaluation of diagnosisOff-label drugs
No
Yes
Intensive careIV immune globulin or plasma exchangeTreatment of infection and other
precipitating events
Intensify long-term immuno-suppression
Improvement?
Plasma exchange or IV immune globulinGlucocorticoids in megadoseIntensive care
No
Yes
Intensify long-term immuno-suppression
Improvement?
No
Yes
RituximabIntensive careTreatment of complicationsOther immunosuppressive drugsNever give up
The New England Journal of Medicine Downloaded from nejm.org by mauro scarpelli on December 29, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
n engl j med 375;26 nejm.org December 29, 20162572
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Clinic a l a nd Patho genic Va r i a n t s
Variants of myasthenia gravis are defined on the basis of autoimmune and antibody disease mech-anisms, target molecules of skeletal muscle, thymic status, genetic characteristics, response to therapy, and disease phenotype. Patients with myasthenia gravis should always be subgrouped on the basis of all these variables (Fig. 2A) and should be assigned to only one subgroup. To combine disparate clinical and nonclinical fea-tures in the classification of individual patients is a challenge (Table 1). Subgroups influence thera-peutic decisions and prognosis.
In 15% of all patients with myasthenia gravis, symptoms and signs are confined to ocular muscles. Only half of patients with ocular myas-thenia gravis have detectable muscle antibod-ies.13 Ptosis and diplopia are common initial symptoms, but the disease remains restricted to ocular muscles in only a minority of patients. In 90% of patients who continue to have purely ocular myasthenia gravis 2 years after the start of symptoms, the disease will persist as a focal eye-muscle weakness and never become general-ized. Myasthenia gravis with muscle-specific kinase antibodies is not manifested as ocular myasthenia, whereas both acetylcholine receptor and LRP4 antibodies can be found in the ocular subgroup.2 The presence of muscle antibodies increases the risk of subsequent generalized disease.
Ten percent of patients with myasthenia gra-vis have a thymoma, and the prevalence increases with increasing age. Two thirds of patients with myasthenia gravis have generalized early-onset or late-onset disease and no thymoma. Among patients who have myasthenia gravis with acetyl-choline receptor antibodies, the age at onset has a bimodal pattern, supporting the use of a cutoff age of 50 years to distinguish between early-onset and late-onset disease.14 Juvenile myasthe-nia gravis, which is included in the early-onset group and is defined as an onset before the age of 15 years, is much more common in East Asian populations than in whites.15,16 Early-onset myas-thenia gravis tends to be characterized by thymic hyperplasia, whereas thymic atrophy is charac-teristic of late-onset disease. Early-onset myasthe-nia gravis is associated with HLA-DR3, HLA-B8, and non-HLA genes that are known to influence
the immune system and probably the risks of autoimmune disease; late-onset disease is asso-ciated with HLA-DR2, HLA-B7, and HLA-DRB1 15.01.17,18 Thymic status and HLA pattern repre-sent strong subgroup markers, probably point-ing directly to variation in pathogenic pathways. Early-onset myasthenia gravis is three times as likely to be diagnosed in females as it is in males, whereas males slightly outnumber fe-males in the late-onset group. Coexisting auto-
Figure 2. Subgroups of Myasthenia Gravis and Coexisting Conditions.
Panel A shows myasthenia gravis subgroups defined on the basis of clinical, antibody, and thymic features. MuSK denotes muscle-specific kinase, and LRP4 lipo-protein receptor–related protein 4. As shown in Panel B, patients with myasthenia gravis commonly have coexist-ing conditions that are related to their disease (especially thymoma and other autoimmune conditions), induced by therapy, or unrelated to their disease.
B Coexisting Conditions
A Myasthenia Gravis Subgroups
Thymoma
CardiacdiseaseUnrelated
disorders
AutoimmunityTherapy-induced
disorders
Myastheniagravis
Early onset
Late onset
Ocular
Seronegative
Thymoma
LRP4MuSK
The New England Journal of Medicine Downloaded from nejm.org by mauro scarpelli on December 29, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
Terapia nell’adulto

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Remissione completa e duratura della MG in <10% dei casiRefrattarietà ai trattamenti convenzionali nel 10-15% dei casi
Gravità clinica dose dello steroide sono i fattori che più influenzano negativamente la qualità di vita
Miglior controllo della risposta autoimmune nelle fasi precoci di malattia modifica l’entità dell’attacco immunitario e riduce il rischio di danno d’organo permanente
EARLY FAST-ACTING TREATMENT STRATEGY AGAINST GENERALIZEDMYASTHENIA GRAVISKIMIAKI UTSUGISAWA, MD,1 YURIKO NAGANE, MD,1 TETSUYA AKAISHI, MD,2 YASUSHI SUZUKI, MD,3 TOMIHIRO IMAI, MD,4
EMIKO TSUDA, MD,4 NAOYA MINAMI, MD,5 AKIYUKI UZAWA, MD,6 NAOKI KAWAGUCHI, MD,7 MASAYUKI MASUDA, MD,8
SHINGO KONNO, MD,9 HIDEKAZU SUZUKI, MD,10 HIROYUKI MURAI, MD,11 and MASASHI AOKI, MD2
1 Department of Neurology, Hanamaki General Hospital, 4-28, Kajoh-chou, Hanamaki 025-0075, Japan2 Department of Neurology, Tohoku University Graduate School of Medicine, Sendai, Japan3 Department of Neurology, Sendai Medical Center, Sendai, Japan4 Department of Neurology, Sapporo Medical University Hospital, Sapporo, Japan5 Department of Neurology, Hokkaido Medical Center, Sapporo, Japan6 Department of Neurology, Chiba University School of Medicine, Chiba, Japan7 Chiba Neurology Clinic, Chiba, Japan8 Department of Neurology, Tokyo Medical University, Tokyo, Japan9 Department of Neurology, Toho University Oh-hashi Medical Center, Tokyo, Japan10 Department of Neurology, Kinki University School of Medicine, Osaka, Japan11 Department of Neurological therapeutics, Kyushu University Graduate School of Medicine, Fukuoka, Japan
Accepted 5 September 2016
ABSTRACT: Introduction: In this study we sought to clarify theeffects of early fast-acting treatment (EFT) strategies on the timecourse for achieving the treatment target in generalized myasthe-nia gravis (MG). Methods: This retrospective study of 923 con-secutive MG patients analyzed 688 generalized MG patientswho had received immunotherapy during the disease course.The time to first achieve minimal manifestations (MM) or betterwhile receiving prednisolone at !5 mg/day for "6 months (MM-or-better-5mg) up to 120 months after starting immunotherapywas compared between EFT and non-EFT patients. Results:Achievement of MM-or-better-5mg was more frequent and earli-er in the EFT group (P 5 0.0004, Wilcoxon test; P 5 0.0001,log-rank test). Multivariate Cox regression analysis calculated ahazard ratio of 1.98 (P < 0.0001) for utilization of EFT. Dosingregimens of oral steroids in EFT produced no differences in thetime course. Conclusions: EFT strategies are advantageous forearly achievement of MM-or-better-5mg.
Muscle Nerve 000:000–000, 2016
Long-term full remission without immune treat-ment is rare in myasthenia gravis (MG) patients,even though the frequency of patients with severeillness decreases during treatment.1–5 Many MG
patients are still burdened by both insufficientimprovement and long-term side effects of oralcorticosteroids.3–7 Disease severity and the dose oforal corticosteroids are major factors that negative-ly affect self-perceived health-related quality of life(HRQOL) in MG patients.5,6 Steroid-associateddepression has also been suggested to be a signifi-cant negative factor for HRQOL of patients.5,7
Therefore, greater effort is needed to reduce boththe severity of the illness and the dose of oralcorticosteroids.5,6
It is ideal but uncommon (<10% of totalpatients) for MG patients to achieve MyastheniaGravis Foundation of America (MGFA) completestable remission (CSR)8 status.4–6 The HRQOL ofMG patients who achieve minimal manifestations(MM)8 or better status on prednisolone (PSL) at!5 mg/day (MM-or-better-5mg) is good and atalmost an identical level to those who achieve CSRstatus.5,6 Moreover, comparisons of the relation-ship between patients’ HRQOL and clinical param-eters of MG with the associated treatment have ledto the proposal that achieving MM-or-better-5mgcan be a practical treatment target.5,6,9 By achiev-ing an early return to such a state, MG patients areenabled to live a normal lifestyle without worryabout corticosteroid complications.6
Because the percentage of patients who achieveMM-or-better-5mg is not high (<50% of subjects incross-sectional studies), changes in treatments areneeded to further increase treatment success.5,6
However, studies on the use of longer treatmentswith a higher dose of oral corticosteroids did notidentify better outcomes for MG patients.10,11
Therapeutic strategies have been reported thataggressively use non-oral fast-acting immunothera-pies, such as plasmapheresis, high-dose intravenousmethylprednisolone (HMP), and intravenousimmunoglobulin (IVIg) in the early stages of
Additional supporting information may be found in the online version ofthis article.
Abbreviations: AChR-Ab, autoantibodies against the acetylcholine recep-tor; CNI, calcineurin inhibitor; CSR, complete stable remission; EFT, earlyfast-acting treatment; HMP, high-dose intravenous methylprednisolone;HRQOL, health-related quality of life; IVIg, intravenous immunoglobulin;MG, myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America;MG-QOL15, 15-item MG-Specific QOL Scale; MG-QOL15-J, Japaneseversion of the MG-QOL15; MM, minimal manifestations; MuSK-Ab, auto-antibodies against muscle-specific tyrosine kinase; PSL, prednisolone;QMG, MGFA quantitative MG scoreKey words: Kaplan–Meier method; myasthenia; oral steroids; treatmentstrategies; treatment targetThis work was supported by the Japan MG Registry Study Group.
Correspondence to: K. Utsugisawa; e-mail: [email protected]
This is an open access article under the terms of the Creative CommonsAttribution-NonCommercial License, which permits use, distribution andreproduction in any medium, provided the original work is properly citedand is not used for commercial purposes.
VC 2016 The Authors. Muscle & Nerve Published by Wiley Periodicals, Inc.Published online 00 Month 2016 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/mus.25397
Early Treatment for MG MUSCLE & NERVE Month 2016 1

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Start High, Then Go Low: An Effective Strategy in the Treatment of Myasthenia Gravis.
Nicholas J. Silvestri, MD, and Gil I. Wolfe, MD
From the Department of Neurology, University at Buffalo Jacobs School of Medicine and Biomedical
Sciences, SUNY, Buffalo, NY.
Correspondence to:
Nicholas J. Silvestri, MD
Dept. of Neurology
Univ. at Buffalo Jacobs School of Medicine and Biomedical Sciences
100 High St.
Buffalo, NY 14203
The authors have read the Journal's position on issues involved in ethical publication and all
authors have read and approved the submitted manuscript.
Dr. Silvestri serves on the medical advisory board for OptionCare. Dr. Wolfe serves on the
medical advisory board for Grifols and Shire. The authors report no other relevant financial
disclosures or conflicts of interest.
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/mus.25654
This article is protected by copyright. All rights reserved.
use of CNIs in the EFT group may have promotedachievement of the treatment target. However, thebeneficial effects of CNIs were not detected in themultivariate analysis, suggesting that the effectswere not strong beyond the effects of EFT.
Figure 2B shows the baseline cumulative hazardcurves for both the EFT and non-EFT groups,excluding the effects of the covariables, as a func-tion of time.
Differences between Low-Dose and High-Dose PSL
Regimens in EFT Patients.
Differences in Background and Therapies Uti-lized. Table 3 shows comparisons of characteristicsand therapies utilized for the EFT-treated patientswhen combined with either the low- or high-dosePSL regimens. Symptoms at the time when condi-tions were at their worst (worst QMG) were moresevere (P < 0.0001), the duration of immune treat-ment was longer (P < 0.0001), and the frequencyof thymectomy was higher (P < 0.01) in the EFT-treated patients given the high-dose PSL regimen.Current severity (QMG), current MG-QOL15-Jscore, and percentage of patients who achieved
MM-or-better-5mg for !6 months at the presenttime were not different between the 2 groups.Although the maximum dose of PSL during thedisease course was much higher, and the durationof taking PSL at a dose of !20 mg was much lon-ger in the high-dose PSL group (P < 0.0001),there was no difference between the 2 groups withregard to current dose of oral PSL and frequencyof CNI use. In the low-dose PSL group, only 1patient received !20 mg for 3 months. Althoughthere were no differences between groups for fre-quencies of plasmapheresis and IVIg within 6months from starting the immune therapy, thedose of HMP was lower in the high-dose PSLgroup (P < 0.0001).
Differences in Time Course Required to AchieveTreatment Target. Figure 3A shows the Kaplan–Meier curves for first achievement of the treatmenttarget (MM-or-better-5mg for !6 months) in theEFT groups with the low- and high-dose PSL regi-mens. Achievement of the treatment targetappeared to be more frequent and occur earlier in
FIGURE 2. (A) Kaplan–Meier curves for the first achievementof the treatment target (MM or better-5mg for !6 months) inboth the EFT and non-EFT groups. (B) Baseline cumulativehazard curves for both the EFT and non-EFT groups, excludingthe effects of the covariables as a function of time. EFT, earlyfast-acting treatment; MM, minimal manifestations.
FIGURE 3. (A) Kaplan–Meier curves for first achievement ofthe treatment target (MM or better-5mg for !6 months) in bothgroups of the EFT with the low- and high-dose PSL regimens.(B) Time courses of the baseline cumulative hazard curves forboth the low-dose and high-dose PSL groups as a function oftime. EFT, early fast-acting treatment; MM, minimal manifesta-tions; PSL, prednisolone.
6 Early Treatment for MG MUSCLE & NERVE Month 2016
use of CNIs in the EFT group may have promotedachievement of the treatment target. However, thebeneficial effects of CNIs were not detected in themultivariate analysis, suggesting that the effectswere not strong beyond the effects of EFT.
Figure 2B shows the baseline cumulative hazardcurves for both the EFT and non-EFT groups,excluding the effects of the covariables, as a func-tion of time.
Differences between Low-Dose and High-Dose PSL
Regimens in EFT Patients.
Differences in Background and Therapies Uti-lized. Table 3 shows comparisons of characteristicsand therapies utilized for the EFT-treated patientswhen combined with either the low- or high-dosePSL regimens. Symptoms at the time when condi-tions were at their worst (worst QMG) were moresevere (P < 0.0001), the duration of immune treat-ment was longer (P < 0.0001), and the frequencyof thymectomy was higher (P < 0.01) in the EFT-treated patients given the high-dose PSL regimen.Current severity (QMG), current MG-QOL15-Jscore, and percentage of patients who achieved
MM-or-better-5mg for !6 months at the presenttime were not different between the 2 groups.Although the maximum dose of PSL during thedisease course was much higher, and the durationof taking PSL at a dose of !20 mg was much lon-ger in the high-dose PSL group (P < 0.0001),there was no difference between the 2 groups withregard to current dose of oral PSL and frequencyof CNI use. In the low-dose PSL group, only 1patient received !20 mg for 3 months. Althoughthere were no differences between groups for fre-quencies of plasmapheresis and IVIg within 6months from starting the immune therapy, thedose of HMP was lower in the high-dose PSLgroup (P < 0.0001).
Differences in Time Course Required to AchieveTreatment Target. Figure 3A shows the Kaplan–Meier curves for first achievement of the treatmenttarget (MM-or-better-5mg for !6 months) in theEFT groups with the low- and high-dose PSL regi-mens. Achievement of the treatment targetappeared to be more frequent and occur earlier in
FIGURE 2. (A) Kaplan–Meier curves for the first achievementof the treatment target (MM or better-5mg for !6 months) inboth the EFT and non-EFT groups. (B) Baseline cumulativehazard curves for both the EFT and non-EFT groups, excludingthe effects of the covariables as a function of time. EFT, earlyfast-acting treatment; MM, minimal manifestations.
FIGURE 3. (A) Kaplan–Meier curves for first achievement ofthe treatment target (MM or better-5mg for !6 months) in bothgroups of the EFT with the low- and high-dose PSL regimens.(B) Time courses of the baseline cumulative hazard curves forboth the low-dose and high-dose PSL groups as a function oftime. EFT, early fast-acting treatment; MM, minimal manifesta-tions; PSL, prednisolone.
6 Early Treatment for MG MUSCLE & NERVE Month 2016

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Early fast-acting treatment (EFT) strategies: plasmaferesi, Ig vena, metilprednisolone
MG generalizzata, entro 1 mese dall’esordio dei sintomi
Miglioramento dei sintomi a lungo termine e riduzione della dose di steroide di mantenimento
Anticorpi monoclonali da usare come EFT?Riduzione della dose di mantenimento anche di altri farmaci immunosoppressori dopo EFT?
Start High, Then Go Low: An Effective Strategy in the Treatment of Myasthenia Gravis.
Nicholas J. Silvestri, MD, and Gil I. Wolfe, MD
From the Department of Neurology, University at Buffalo Jacobs School of Medicine and Biomedical
Sciences, SUNY, Buffalo, NY.
Correspondence to:
Nicholas J. Silvestri, MD
Dept. of Neurology
Univ. at Buffalo Jacobs School of Medicine and Biomedical Sciences
100 High St.
Buffalo, NY 14203
The authors have read the Journal's position on issues involved in ethical publication and all
authors have read and approved the submitted manuscript.
Dr. Silvestri serves on the medical advisory board for OptionCare. Dr. Wolfe serves on the
medical advisory board for Grifols and Shire. The authors report no other relevant financial
disclosures or conflicts of interest.
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/mus.25654
This article is protected by copyright. All rights reserved.

Terapia nell’adulto
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
L’obiettivo della terapia nella MG deve essere la remissione clinica o lo stato di minima disabilità
Sebbene la terapia della miastenia continui a fondarsi sui 3 pilastri storici (piridostigmina, steroide, immunosoppressore), gli anticorpi monoclonali stanno assumendo un ruolo sempre più importante
E’ meglio essere aggressivi nelle prime fasi della malattia per non doverlo essere nelle ricadute
Adeguare l’utilizzo dei farmaci al singolo paziente ne mogliora significativamente la qualità di vita

Ringraziamenti
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Silvia RomitoGiovanna SquintaniMaria Rachele Bianchi

Ringraziamenti
www.assmiastenia.it
[email protected] [email protected]
Telefono segreteria: 333 333 2001 (dal lunedì al venerdì, dalle 15.00 alle 18.00)
Sostieni l’Associazione Miastenia Il tuo contributo è molto importante per noi!
UNITI SIAMO PIÙ FORTI
DELLA MIASTENIA Nella misura in cui PUOI, partecipa attivamente all’Associazione Miastenia di Padova: iscrivendoti all’A.M. donando un po’ del tuo tempo libero diventando
volontario A.M. aiutandoci a far conoscere l’A.M. attraverso donazioni in denaro, che sono
deducibili nella dichiarazione dei redditi:
c/c postale Banco Posta 15696354 IBAN: IT14 T076 0112 1000 0001 5696 354
c/c Banca Padovana Credito Cooperativo S.C. IBAN: IT96 V084 2962 9800 1901 0000 362
scegliendo di devolvere il “5x1000” all’A.M. non costa nulla ed è facilissimo!!!
Nella dichiarazione dei redditi PUOI destinare all’A.M. la quota del TUO 5x1000 IRPEF inserendo il codice fiscale 92085440284 nel riquadro “Sostegno delle organizzazioni non lucrative di utilità sociale, delle associazioni di promozione sociale, delle associazioni riconosciute che operano nei settori di cui all’art. 10 c.1, lett. A) del D. Lgs 460/1997”.
Visita il nostro sito direttamente dal tuo
smart-phone
Diventa NOSTRO AMICO in Facebook,
cerca Associazione Miastenia Padova
O.N.L.U.S. di diritto
Codice Fiscale 92085440284
Registro delle O.d.V. Regione Veneto: PD0707 Registro del Comune di Padova: 984
Silvia RomitoGiovanna SquintaniMaria Rachele Bianchi