APPROCCIO MULTIDISCIPLINARE ALL’ENDOMETRIOSI PELVICA: ENDOMETRIOSI ... · APPROCCIO...
45
APPROCCIO MULTIDISCIPLINARE ALL’ ENDOMETRIOSI PELVICA: ENDOMETRIOSI INTESTINALE Dott. G. Moretto Casa di Cura Polispecialistica dott. Pederzoli Peschiera del Garda (Verona) Castelmella (Bs) 08 nov 2014
Transcript of APPROCCIO MULTIDISCIPLINARE ALL’ENDOMETRIOSI PELVICA: ENDOMETRIOSI ... · APPROCCIO...

APPROCCIO MULTIDISCIPLINARE ALL’ENDOMETRIOSI
PELVICA:ENDOMETRIOSI INTESTINALE
Dott. G. Moretto Casa di Cura Polispecialistica dott. Pederzoli
Peschiera del Garda (Verona)Castelmella (Bs) 08 nov 2014
ENDOMETRIOSI:
◆ Endometriosi: condizione in cui tessuto analogo a quello endometriale si localizza in siti al di fuori dell’utero.
◆ Tale malattia interessa generalmente le donne nel loro periodo riproduttivo
ENDOMETRIOSI
◆ LOCALIZZAZIONI PIU’ FREQUENTI: Ovaie, tube, legamenti utero-sacrali,
peritoneo, setto retto-vaginale, sigma-retto.
◆ MENO FREQUENTI / RARE: Appendice, cervice, vagina, ombelico,
regione inguinale, uretere, pleura, polmone e cervello.
DPE (Endometriosi Pelvica Profonda)
◆ In deep pelvic endometriosis (DPE) the lesions are found more than 5 mm below the pelvic peritoneal surface.
SINTOMI:◆ La sintomatologia appare non specifica
(overlap con patologie benigne e maligne) e variabile.
◆ Circa ¾ delle pazienti sintomatiche lamentano dolore pelvico ciclico o cronico e/o dismenorrea
◆ Altri sintomi: dispareunia, tenesmo, dolore defecatorio, proctorragia.
◆ NB: necessario conoscere l’esistenza di tale patologia

DIAGNOSI:◆ ESAME FISICO ◆ DIAGNOSTICA STUMENTALE: ecografia
addominale e transvaginale: esami iniziali, sufficienti se trattamento medico.
◆ In caso di necessità di più precisa definizione estensione malattia, in previsione di ottica chirurgica: Ecografia transrettale e MRI permettono idonea valutazione con assenza di esposizione ad irradiazione

Il trattamento è in funzione delle dimensioni, localizzazione, estensione delle lesioni, severità dei sintomi, età, desiderio di gravidanza ed associata infertilità.
Lo scopo è di migliorare i sintomi e la fertilità della paziente.
TRATTAMENTO ENDOMETRIOSI
Il trattamento chirurgico prevede la rimozione delle lesioni al fine di migliorare i sintomi lamentati dalle pazienti
TRATTAMENTO CHIRURGICO:
COINVOLGIMENTO INTESTINALE
◆ 3-36% delle donne presentano un certo grado di endometriosi (Cattel N Engl J Med ’87; Forsgren Acta Chir Scand ’83; Prystwosky Arch Surge
’88;Samper South Med J, ‘84)
◆ il retto ed il colon sigmoideo risultano interessati nel 72%-85% dei casi (Fagan Radiol Clin North Am ’74; Macafee Br J Obstet Gynaecol ’60, Jenkinson
JAMA ’43)
There is a general consensus that surgical
resection is the treatment of choice for DPE
infiltrating the bowel wall.
One peculiar feature of this form of DPE is that
even though the activity of the disease may be
controlled by medical treatment, the regression
of the nodule in the muscular tissue will
eventually cause fibrosis and scar tissue that
result in narrowing and distortion of the bowel
lumen, leading to persistence or even worsening
of intestinal symptoms.

IN CONSIDERAZIONE DEL VASTO RANGE DI QUADRI ANATOMICI POSSIBILI, IL TRATTAMENTO RISULTA ESTREMAMENTE FLESSIBILE E DEVE ESSERE ADATTATO AI SINGOLI CASI
UNA VOLTA STABILITO IL TRATTAMENTO CHIRURGICO, SI POSSONO PRESENTARE TRE OPZIONI: ➢ESCISSIONE SUPERFICIALE, ➢RESEZIONE DISCOIDE, ➢RESEZIONE INTESTINALE SEGMENTARIA
The choice is based mainly on the extent of bowel involvement; the treatment of all
endometriotic lesions should be preferably achieved by a single operation
with the cooperation of different specialists)

SURGICAL TECHNIQUE: OPTIONS
Superficial excision Superficial lesions involving only the serosa can be "shaved off",
better by scissor to avoid thermal damage to the bowel wall
causing delayed fistula. Superficial excision has the advantage of
preventing intestinal opening however carries the risk of possible
micro- perforation with subsequent pelvic sepsis
Bowel discoid resection
It consists of using a circular stapling device (CEEA) to excise completely a full thickness lesion situated on the anterior rectal wall that otherwise would have required an ultra-low rectal resection (within 6 cm from the anal verge) and anastomose
◆ Limit: it removes lesions < 3 cm
However the studies by Remorgida, Anaf, Abrao, and Kavallaris demonstrated that disc excision leads to incomplete disease removal in a high percentage of cases, due to multifocal lesions that can be found at distance from the principal nodule.
Segmental bowel resection
When the bowel lesion involves more than
50% of the bowel circumference, is larger
than 3 cm or when multiple nodules are
present. (Redwine & Sharpe,
Baillere’s Clinical Obstetrics and Gynecol ’95)
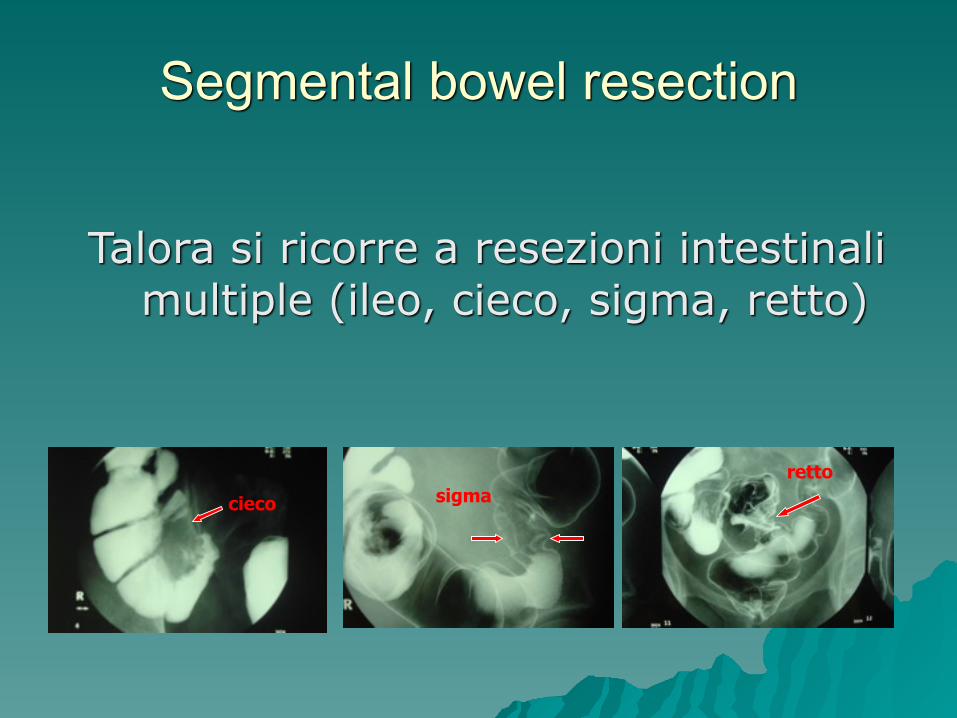
Segmental bowel resection
Talora si ricorre a resezioni intestinali multiple (ileo, cieco, sigma, retto)
cieco sigmaretto
Recto-sigmoid resection for endometriosis is acknowledged to be very challenging and
radicality has always to be balanced with the risk of complications.
Many retrospective studies have demonstrated the symptomatic beneficial effect of
bowel resection in 60-100% of patients.
Laparoscopy
Laparotomy
Segmental bowel resection
Main ly co lo rec ta l surgeons , consider laparoscopic resection as first line treatment even if difficult and time consuming.
Patients treated Laparoscopically show less pain, fastest post operative recovery, less complications, higher pregnancy rate.
Laparoscopy carries the risk of conversion that can be as high as 20% and depends from experience and skills of the surgeons, body mass index of the patient, intraoperative complications and difficult dissection for adhesion or previous surgical operations,
COMPLICANZE POST RESEZIONE INTESTINALE:
◆Sanguinamento ◆Deiscenza anastomotica ◆Fistola retto-vaginale ◆Ascessi pelvici …
Most of them require surgical management !

Risk of postoperative complications after laparoscopic colorectal resection for endometriosis
It depends on
• the type of surgery.
Superficial resection: 3.8%
Segmental resection: 11.1%
Segmental resection: 15.5%
• experience of the surgeon
• level of the resection (lower level – higher c.r.)
(Duepree, JM Coll Surg ‘02)
(Dubernard, Hum Reprod ‘06)
FATTORI DI RISCHIO X FISTOLA INTESTINALE
◆ Resezione bassa del retto ◆ Resezione vaginale associata ◆ Multiple resezioni intestinali ◆ Altri interventi maggiori (reimpianto
ureterale)
Dysfunctional digestive symptoms are rarely studied,
however they should be a major concern in young
and otherwise healthy women. Functional
problems are not infrequent being reported in up
to 55% of cases and, although they may improve
with time, tend to be permanent in a large
percentage of patients.
Di fondamentale importanza è giungere ad un preciso inquadramento preoperatorio della paziente, al fine di poter così programmare un corretto approccio chirurgico ed acquisire un adeguato e consenso informato.
Da qui la necessità di un approccio multidisciplinare al problema identificando le rispettive competenze.

GRAZIE PER L’ATTENZIONE

CONCLUSIONIHow can we change the surgical strategy to decrease the rate of intestinal
complications related to surgery?
Today we offer some proposals that are still not yet validated by international studies but seem interesting in our experience.
✓close the vagina by the vaginal route✓put an omental flap between the rectum and the vaginal suture✓pose a barrier system on the vaginal suture✓discoid resection whenever possible✓consider the ileostomy or colostomy colon protection

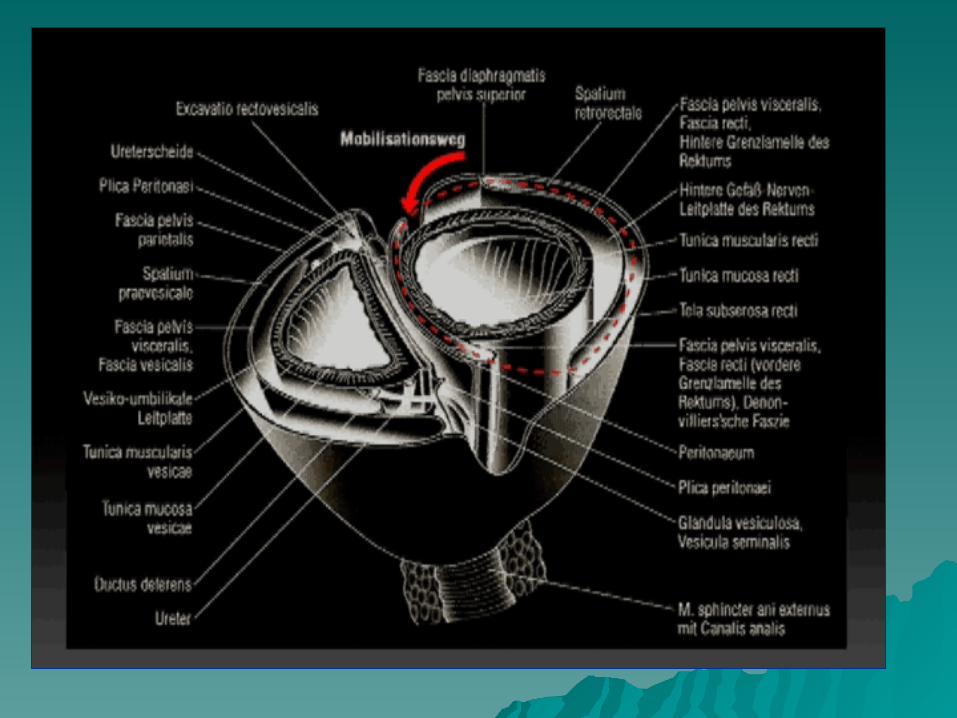
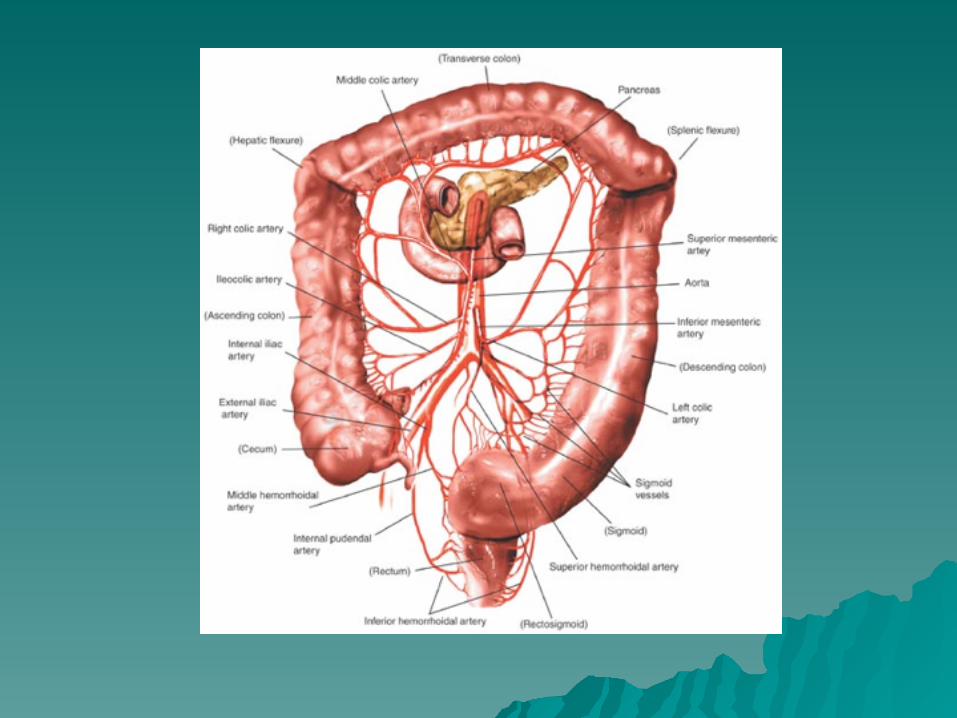
ANATOMIA
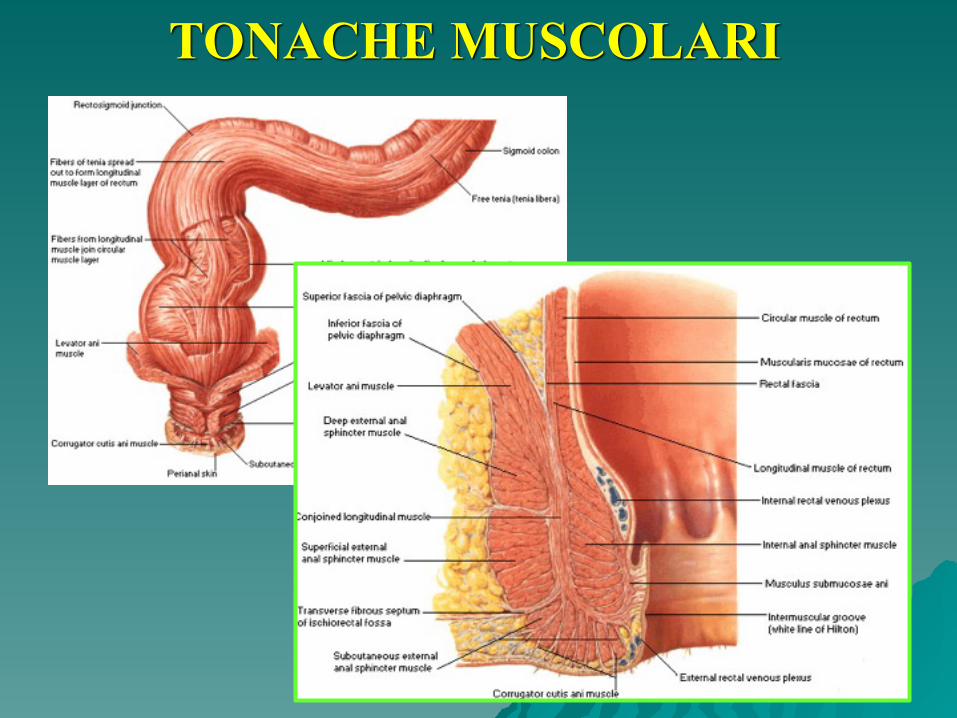
TONACHE MUSCOLARI
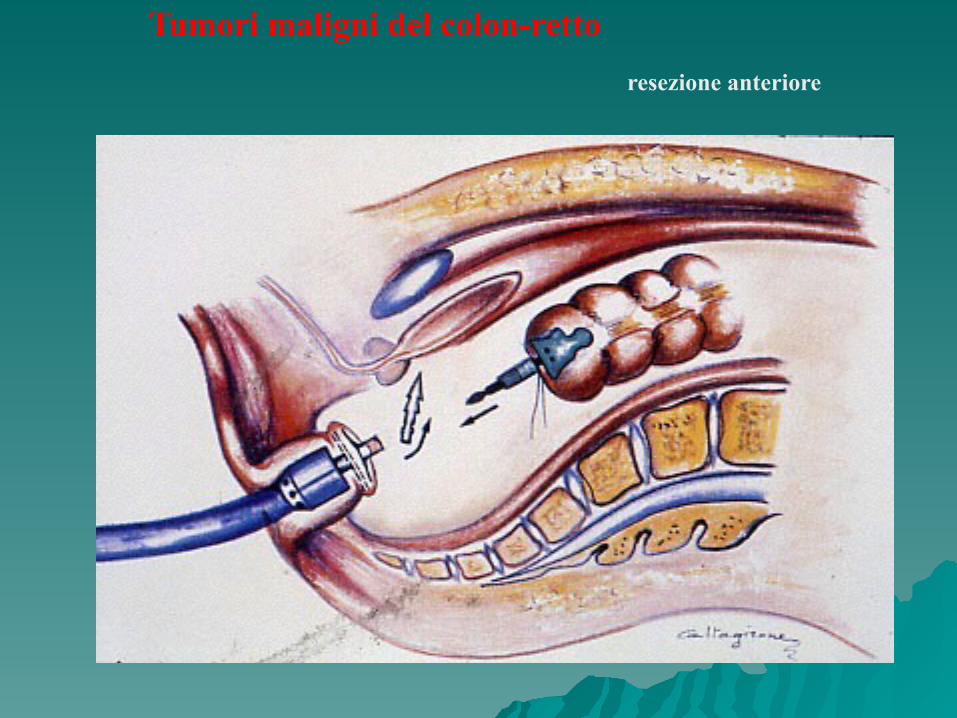
Tumori maligni del colon-rettoresezione anteriore
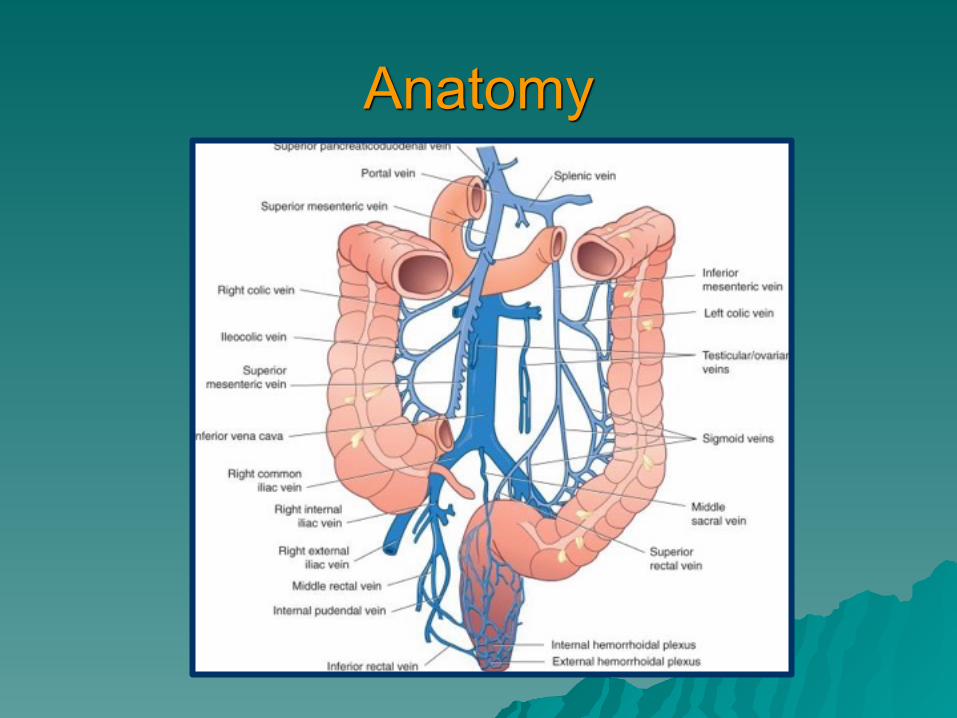
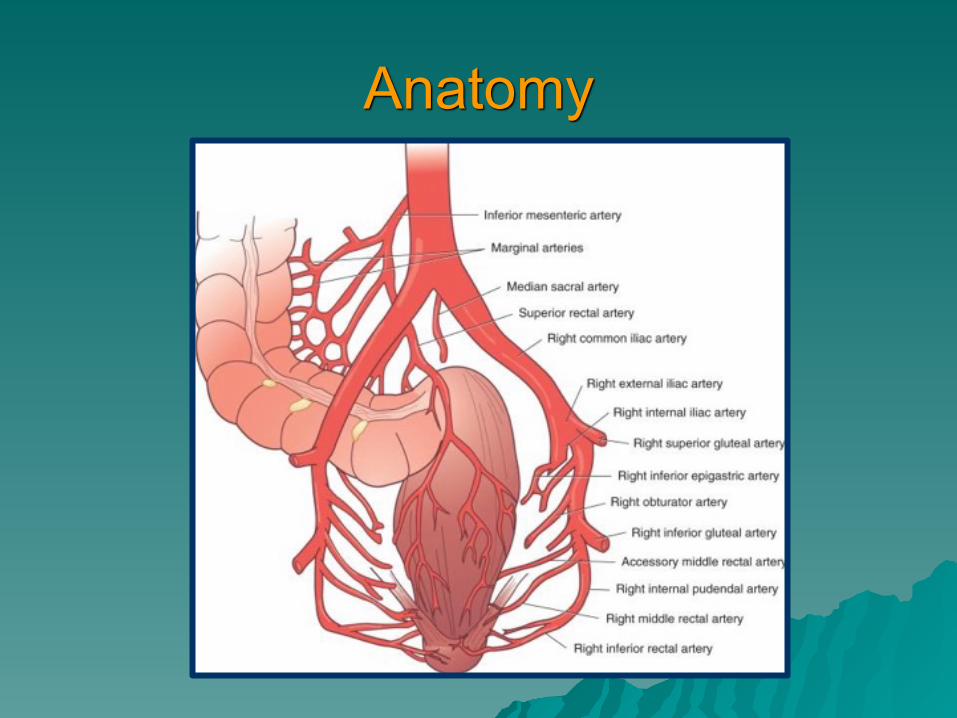
Anatomy
Anatomy
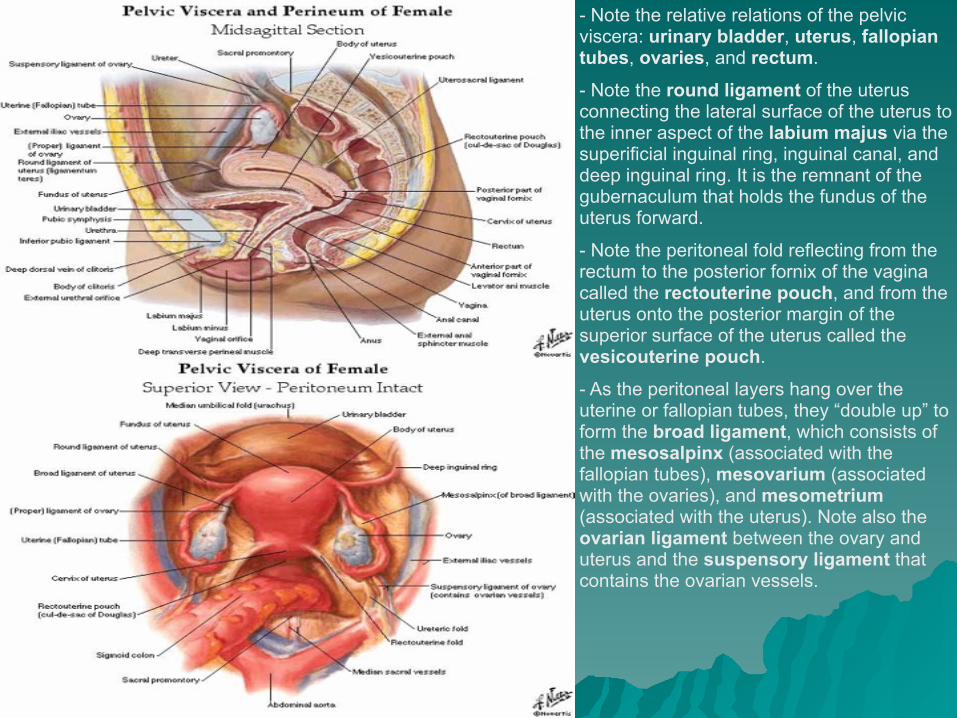
- Note the relative relations of the pelvic viscera: urinary bladder, uterus, fallopian tubes, ovaries, and rectum.
- Note the round ligament of the uterus connecting the lateral surface of the uterus to the inner aspect of the labium majus via the superificial inguinal ring, inguinal canal, and deep inguinal ring. It is the remnant of the gubernaculum that holds the fundus of the uterus forward.
- Note the peritoneal fold reflecting from the rectum to the posterior fornix of the vagina called the rectouterine pouch, and from the uterus onto the posterior margin of the superior surface of the uterus called the vesicouterine pouch.
- As the peritoneal layers hang over the uterine or fallopian tubes, they “double up” to form the broad ligament, which consists of the mesosalpinx (associated with the fallopian tubes), mesovarium (associated with the ovaries), and mesometrium (associated with the uterus). Note also the ovarian ligament between the ovary and uterus and the suspensory ligament that contains the ovarian vessels.
NOTE:
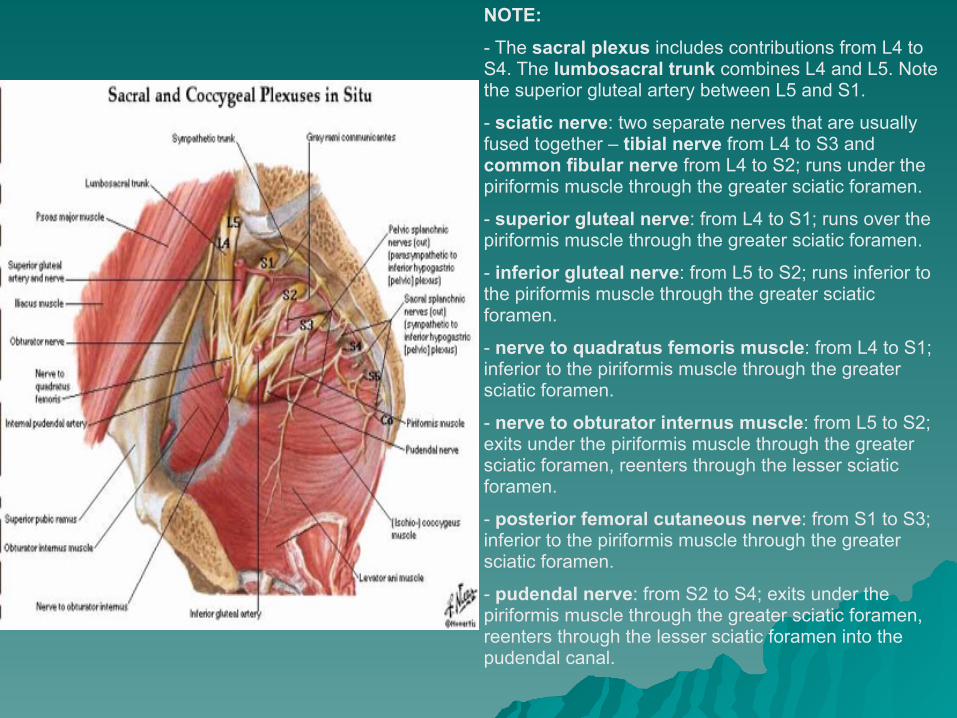
- The sacral plexus includes contributions from L4 to S4. The lumbosacral trunk combines L4 and L5. Note the superior gluteal artery between L5 and S1.
- sciatic nerve: two separate nerves that are usually fused together – tibial nerve from L4 to S3 and common fibular nerve from L4 to S2; runs under the piriformis muscle through the greater sciatic foramen.
- superior gluteal nerve: from L4 to S1; runs over the piriformis muscle through the greater sciatic foramen.
- inferior gluteal nerve: from L5 to S2; runs inferior to the piriformis muscle through the greater sciatic foramen.
- nerve to quadratus femoris muscle: from L4 to S1; inferior to the piriformis muscle through the greater sciatic foramen.
- nerve to obturator internus muscle: from L5 to S2; exits under the piriformis muscle through the greater sciatic foramen, reenters through the lesser sciatic foramen.
- posterior femoral cutaneous nerve: from S1 to S3; inferior to the piriformis muscle through the greater sciatic foramen.
- pudendal nerve: from S2 to S4; exits under the piriformis muscle through the greater sciatic foramen, reenters through the lesser sciatic foramen into the pudendal canal.
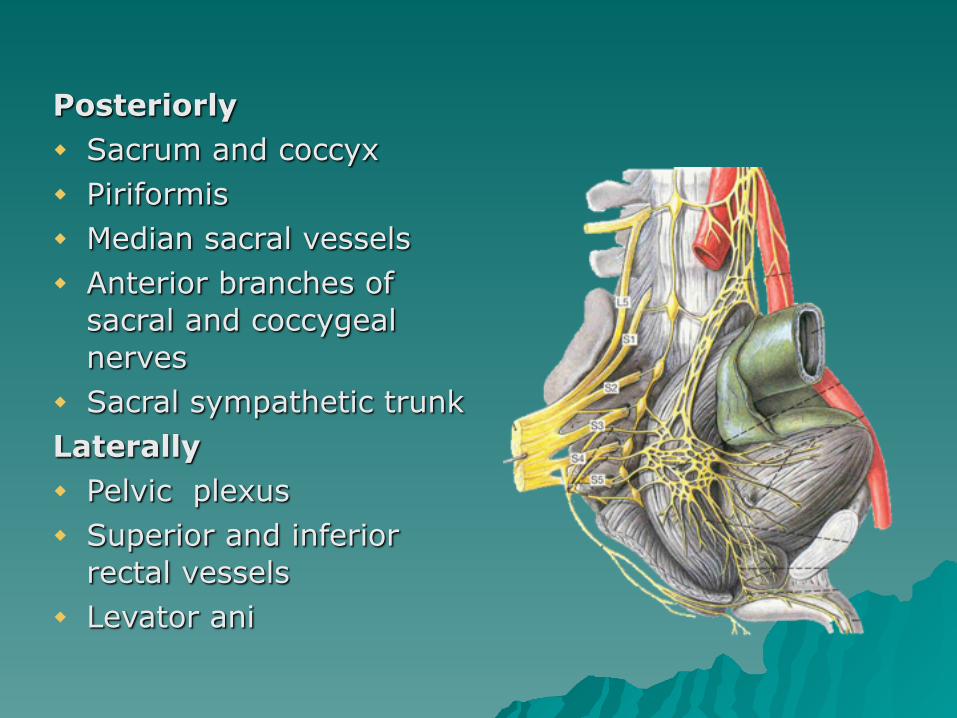
Posteriorly ◆ Sacrum and coccyx ◆ Piriformis ◆ Median sacral vessels ◆ Anterior branches of
sacral and coccygeal nerves
◆ Sacral sympathetic trunk Laterally ◆ Pelvic plexus ◆ Superior and inferior
rectal vessels ◆ Levator ani

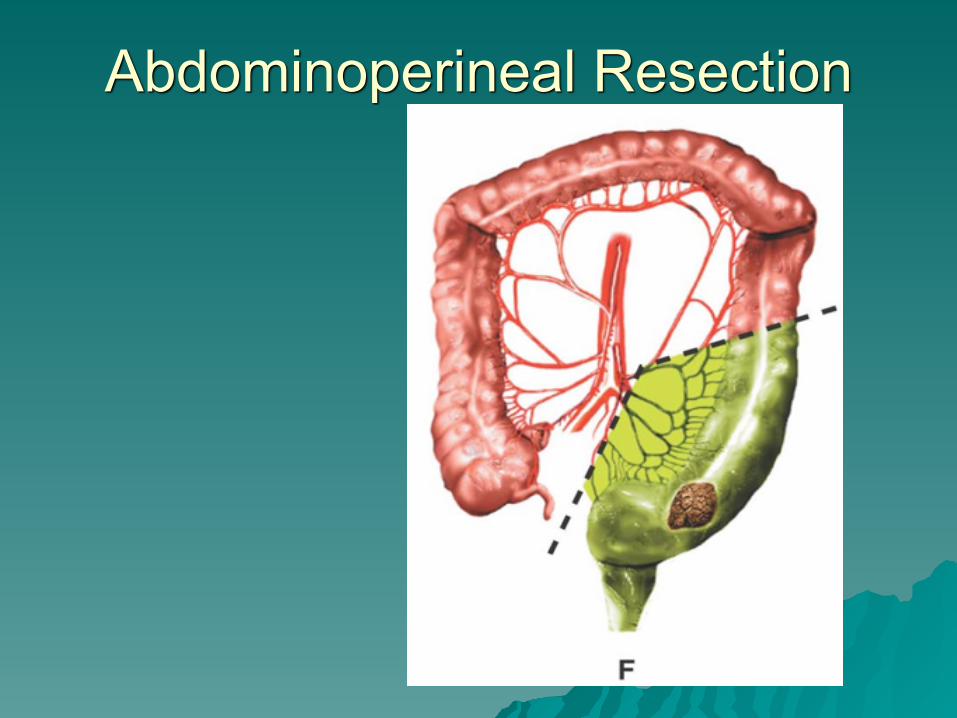
Abdominoperineal Resection

Left Hemicolectomy
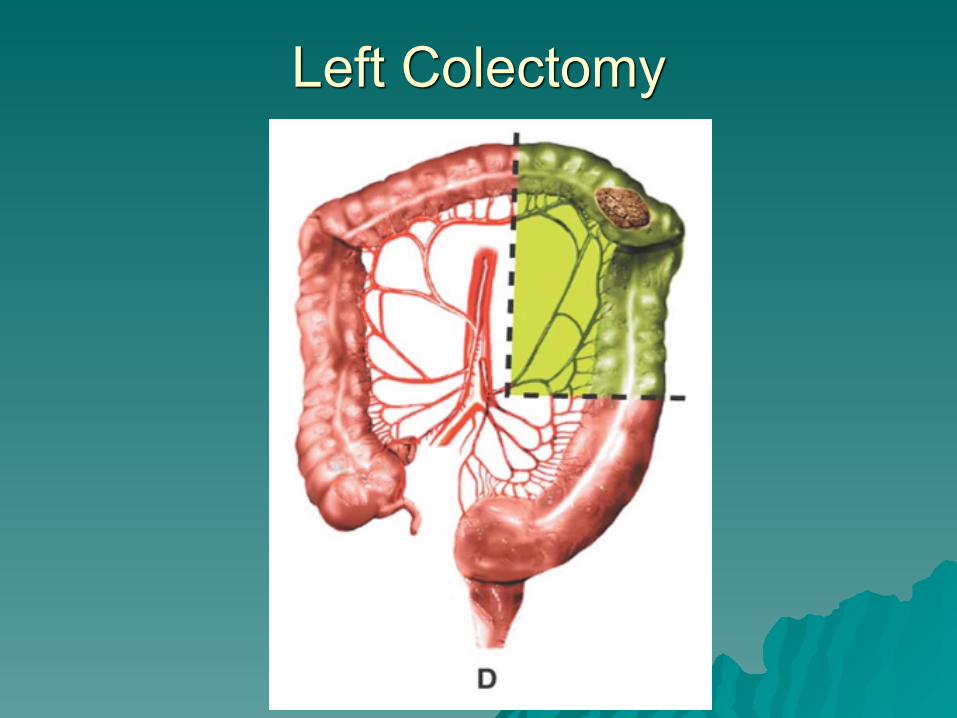
Left Colectomy
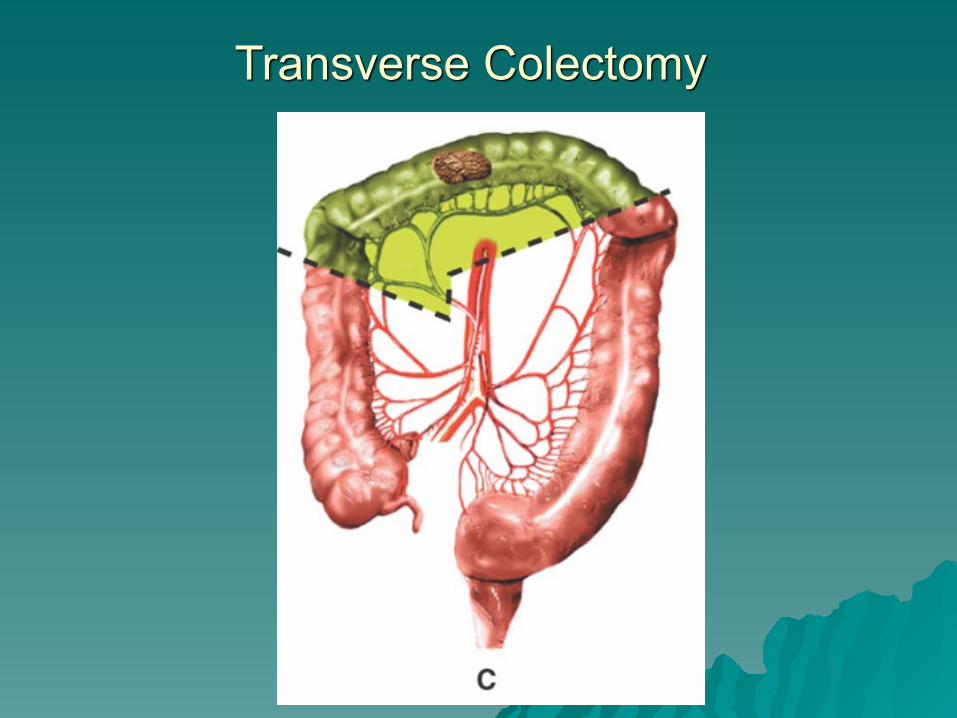
Transverse Colectomy

Right Hemicolectomy
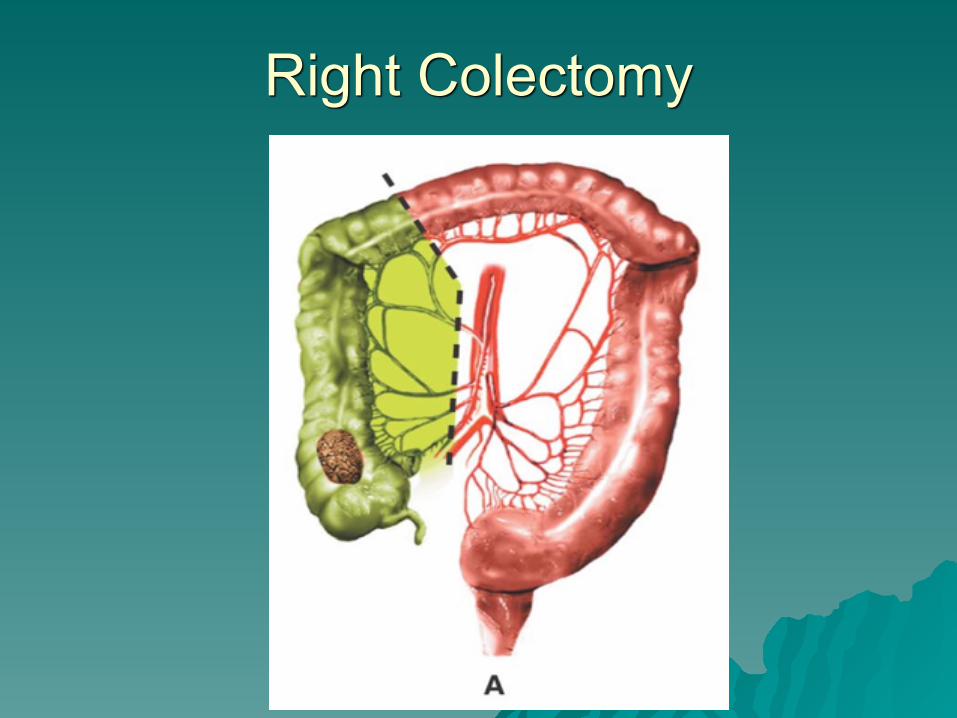
Right Colectomy
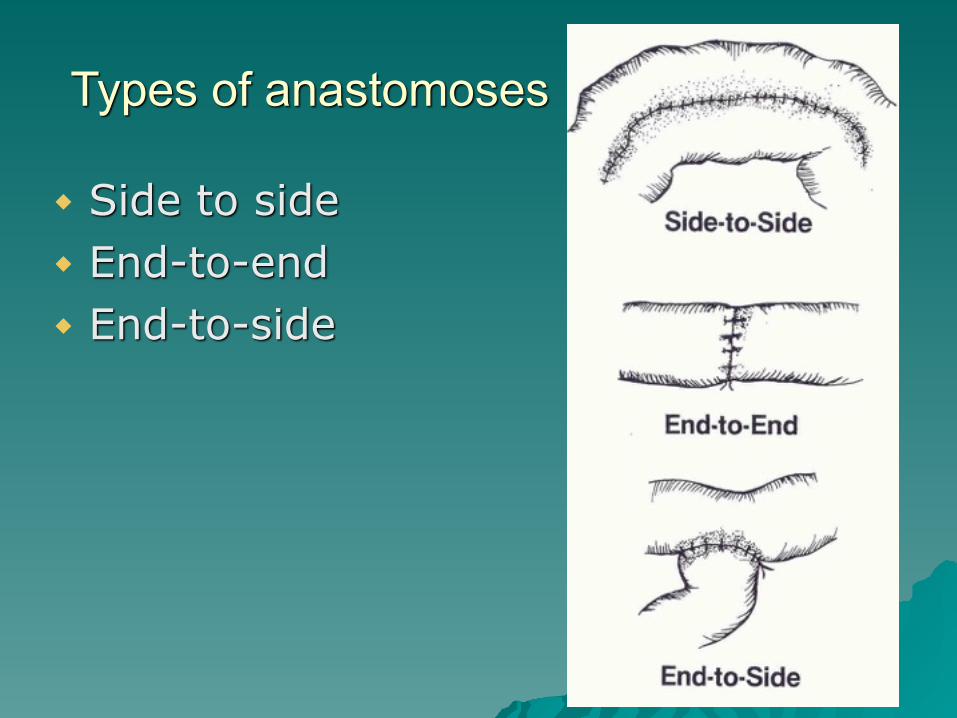
Types of anastomoses
◆ Side to side ◆ End-to-end ◆ End-to-side